
Abstract
Background
To provide estimates of cardiovascular disease burden to guide future health strategies and interventions and enable improvements in health and performance of the health care system to be monitored.
Design
A descriptive study.
Methods
The study was performed in Serbia without Kosovo and Metohia for the year 2000. Disability-adjusted life years (DALY) was used to provide a comprehensive assessment of premature mortality (years of life lost; YLL) and disability attributable (years lived with disability; YLD) to ischaemic heart disease (IHD) and cerebrovascular diseases, and to estimate the attributable and avoidable burden of these diseases caused by smoking, hypertension, overweight/obesity, physical inactivity, alcohol consumption and an inadequate consumption of fruit and vegetables.
Results
IHD was responsible for 150 889 DALY (16.28/1000 population), and cerebrovascular diseases were responsible for 136 090 DALY (14.49/1000 population). There were considerably more YLL for both IHD and stroke than YLD. For both diseases DALY rates increased with ageing in men and women. The risk factors most responsible for IHD and stroke burden were smoking, physical inactivity, hypertension and overweight/obesity. Sex and age differences were present in the burden attributable to various risk factors.
Conclusion
Despite limitations the DALY estimates represent a useful measure of the size of the health problem. The DALY and related estimates for cardiovascular disease can be used as a guide for the prevention of IHD and stroke as well as the evaluation of future health gains by reducing population exposure to lifestyle and related risk factors.
Introduction
In Europe, cardiovascular diseases (CVD) are the main cause of death (48% of all deaths) and the main cause of years of life lost (YLL) because of mortality (approximately 30% of the total YLL) [1]. As a cause of disability-adjusted life years (DALY) lost [2, 3], CVD are in second place in established market economies (18% of total DALY), and in first place in formerly socialistic economies (23% of total DALY) [2].
The population of Serbia without Kosovo and Metohia is in the third stage of the ‘epidemiological transition’ [4] with non-communicable diseases as a predominant cause of death and disability. CVD in Serbia have occupied the first place as a cause of death for decades [5–7]. In the year 2000 they were responsible for 62% of all causes of death (56% in men and 67% in women). Ischaemic heart disease (IHD) and cerebrovascular diseases were responsible for 58% of deaths caused by all CVD (64% in men and 54% in women). In both men and women, IHD and cerebrovascular diseases ranked first and second as a cause of death, and with a large proportion of deaths below the age of 70 years (43% of all IHD deaths and 32% of all stroke deaths).
The aim of the present study was to provide a comprehensive assessment of premature mortality and disability attributable to IHD and cerebrovascular diseases, and to estimate the burden of IHD and cerebrovascular diseases attributable to lifestyle and related risk factors.
Methods
The data presented in this paper are part of the Serbian Burden of Disease Study (SBDS), which was carried out by the European Agency for Reconstruction's Project Team. DALY, a summary measure of population health developed for the Global Burden of Disease (GBD) study [2], was used to estimate the burden caused by disease mortality and disability in the study. The project commenced in October 2002 and finished in September 2003.
The study was conducted in Serbia (a part of Serbia and Montenegro) without Kosovo and Metohia, which is in central Serbia and Vojvodina. The total number of the observed population was 7 551 000 (3 674 000 men and 3 877 000 women). The reference year for the analysis was 2000.
DALY combines a measurement of premature mortality and disability [2, 3, 8]. This indicator is the aggregation of YLL and years lived with disability (YLD) at the population level and thus reflects the ‘burden of disease’ in the population.
The population estimates used for the above indicators were from the census adjustments for years 1999, 2000 and 2001 (not including the migration component).
For the calculation of YLL, we considered all deaths of individuals resident in the Republic of Serbia that occurred anywhere in and outside of Serbia and were registered in 2000.
The completeness of the 2000 mortality database of the Serbian Statistical Office was 98%. Apart from some missing data, two other problems with the validity and reliability of cause of death data were also present: not assigning a specific code, but using senility or some other ill-defined code, and assigning the wrong code as a result of diagnostic methods, carelessness, etc. These problems were solved in the way recommended in the National Burden of Disease manual [9, 10].
YLL was determined by the average life expectancy at the age of death while discounting future years by 3%. The life expectancy at birth was fixed at 82.5 years for women and 80.0 years for men [11].
The GBD study weighted a year of healthy life lived at young ages and older ages lower than for other ages [2]. In SBDS 2000 we decided to use this approach to be able to compare our results with other studies.
For the calculation of YLD, data for Serbia were available only for selected conditions, and consequently the estimation of the total burden (DALY) was possible only for these disorders. Among them were IHD and cerebrovascular diseases. YLD for IHD and cerebrovascular diseases were calculated on the basis of incidence data.
The IHD [International Classification of Disease, version 10 (ICD10) codes I20–I25] model assumed that disease might start as either angina pectoris or acute myocardial infarction (AMI). In this work the general term ‘stroke’ is used synonymously with the whole group of cerebrovascular diseases (ICD10 codes I60–I69).
All data on AMI and stroke were derived from the Registry of Myocardial Infarction and Stroke, Cindy and Monica Collaborative Center, Novi Sad, for 1998 (unpublished data). Incident cases experienced AMI or stroke for the first time in the course of the year.
With no appropriate data on angina pectoris, angina pectoris incidence was estimated to be 1.8 times higher than that for AMI. This estimate was based on data from hospitals in Belgrade (for the year 2000), as being more reliable in comparison with data from other parts of the country. According to these data, out of all hospitalized IHD cases, 64% were with angina pectoris and 36% with AMI.
The disability duration for AMI 28-day non-survivors was assessed on the basis of data from the register. The disability duration for AMI 28-day survivors was taken from the GBD study estimate for the former socialist economies of Europe [12]. For angina pectoris disability duration was taken from the Victorian Burden of Disease Study [13]. The duration of disability in stroke cases was assessed in the manner used in the South and West DALYs project [14].
The disability weights used for IHD and stroke were slightly modified GBD weights [2]. It was assumed that each of the non-survivors (AMI or stroke) suffered disability of the most severe category, similar to a terminal cancer [14, 15]. For the rest, disability weights were calculated from GBD weights assuming that, according to the GBD estimate for the former socialist economies of Europe, 20% of IHD and stroke incidence cases were untreated [2].
The standardization of IHD and stroke incidence, YLL, YLD and DALY rates was performed by the use of a direct method with the European population as the standard [16].
The population-attributable risks [17, 18] were applied to the YLL, YLD and DALY data, so allowing an estimate to be made of the burden attributable to some of the major risk factors. Seven risk factors were chosen for the analysis. For six of them: smoking cigarettes, alcohol consumption, physical inactivity, low vegetable and fruit intake, high blood pressure and obesity, the prevalence data were derived from the 2000 Population Health Survey, which comprised 9921 individuals, aged 20 years and older [19]. The health survey collected self-reported information from participants for the past 7 days. As there were no recent data on the blood cholesterol level in Serbia, data from the Population Health Survey Study in the Republic of Srpska [20] were used to estimate the prevalence of that risk factor in Serbia.
Data on smoking refer only to current smoking. The prevalence of each level of alcohol intake (low, hazardous, harmful) was estimated from weekly consumption by age group and sex, after conversion to standard drinks per day (10 ml of alcohol equals 7.9 g of alcohol). The consumption of 0–0.25 standard drinks per day was considered to be abstinence [18]. The analysed levels of inactivity were sedentary and low levels defined by an estimation based on the frequency and duration of physical activity. More than one serving of fruit and vegetables per day was considered as adequate consumption.
High blood pressure was defined as systolic blood pressure of 160 mmHg or greater or diastolic blood pressure of 95 mmHg or greater. ‘Hypertension’ was used as a term for those individuals with high blood pressure or receiving treatment for high blood pressure, or both.
A body mass index (kg/m2) of 25–29.9 was defined as overweight and a body mass index greater than 30 was regarded as obesity. A blood cholesterol level above 5.5 mmol/l was defined as a high level.
The relative risks associated with exposure to these seven factors were accepted from the following studies. For smoking, the age-adjusted relative risk estimated for individuals 35 years and over came from the second wave of the American Cancer Society's Cancer Prevention Study [21]. For alcohol consumption, physical inactivity, hypertension, obesity and high blood cholesterol, the relative risk was taken from the Australian Burden of Disease Study [22] and the Victoria Burden of Disease Study [13], and for inadequate fruit and vegetables intake, the relative risk was estimated by the New Zealand Ministry of Health [23].
Attributable fractions were calculated from the prevalence of risk factors in the population and the relative risk of dying if exposed to the risk factor [17, 18]. As prevalence data on risk factors were sufficiently detailed [19], it was possible to make the same category cutpoints for the risk factors as those categories used in studies from which the relative risks were accepted. The only exception was fruit and vegetables consumption. Instead of three to five servings of fruit and vegetables per day [23], in SBDS more than one serving per day was considered to be an adequate consumption because it better corresponds to our population's diet. For the attribution of disability burden to risk factors, it was assumed that relative risks apply equally to mortality and morbidity. The relative risks were not fully adjusted for important covariates, and the univariate population-attributable risks calculated did not allow for the clustering and interaction of risk factors.
Results
IHD was responsible for 150 889 DALY (96 023 in men and 54 866 in women), and stroke was responsible for 136 090 DALY (65 795 in men and 70 295 in women; Table 1). There were considerably more YLL lost for both IHD and stroke than YLD. The proportion of YLD in DALY for IHD was higher in women than in men (10.8 versus 9.2%). The opposite and more pronounced difference by sex was found for the YLD/DALY ratio of stroke (12.6% in men versus 8.0% in women).
For IHD and stroke the DALY rates per 1000 population increased with age in both men and women and peaked in the oldest, 75 years of age and older (Fig. 1) [24].
In Table 2 are presented YLD and DALY per 1000 population, as well as the YLD/DALY ratio (%) for IHD and stroke in Serbia without Kosovo and Metohia, and the EURO region [25]. The proportion of YLD in DALY for IHD was higher in Serbia compared with the EURO region. The same proportion of stroke in Serbia was half of that in EURO B. It was lower even when compared with EURO C.
The prevalence of observed risk factors and the burden of IHD and stroke attributable to them are presented in Table 3. Smoking, alcohol consumption, inadequate intake of fruit and vegetables, and overweight/besity were more prevalent in men. Physical inactivity, hypertension and high blood cholesterol were more prevalent in women. Out of these factors, for the IHD burden in men those most responsible were smoking, physical inactivity, hypertension and overweight/obesity. The same factors were responsible for most of the IHD in women, but their rank, according to their percentage of IHD total burden, differed from that in men; physical inactivity being in the first place followed by hypertension, overweight/obesity and smoking. In both sexes alcohol consumption had a protective effect. For stroke burden, the most responsible factors in both sexes were hypertension, physical inactivity, smoking and overweight/obesity. Whereas alcohol consumption was beneficial for stroke in women, it had a harmful effect for stroke in men. A high blood level of cholesterol may also be a risk factor for stroke, but the evidence is less clear and this association was not analysed. Besides differences between men and women in the effect of alcohol consumption on stroke, the greatest sex difference was found for IHD and stroke burden attributable to smoking; the burden attributable to tobacco was almost double in men compared with women.
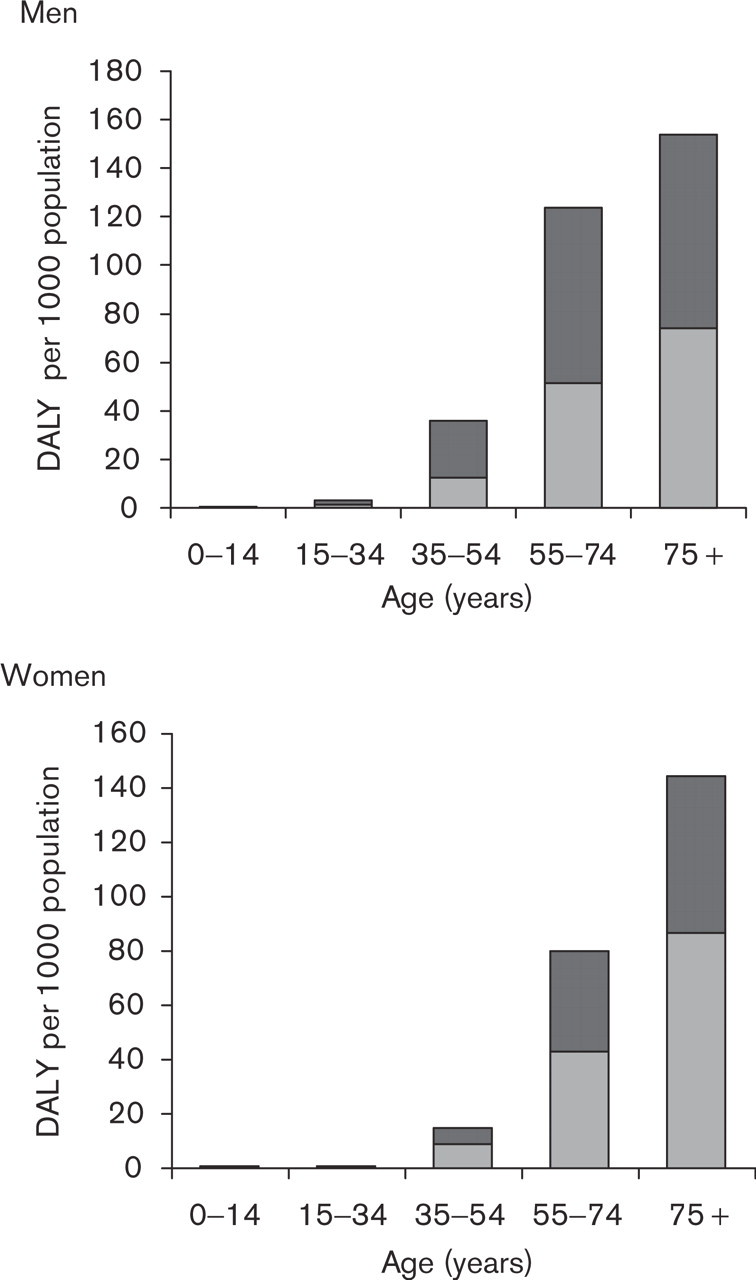
The burden of ischaemic heart disease and stroke by age, Serbia without Kosovo and Metohia, 2000. DALY, Disability-adjusted life years. ▪, Ischaemic heart disease; □, stroke. Reproduced with permission from the Serbian Burden of Disease Study Group [24].
There were also age differences in the burden attributable to various risk factors. The burden attributable to smoking was in both sexes the greatest in age groups 55–64 and 45–54 years. The benefits from alcohol were found in ages over 45 years and particularly over 65 years. The greatest burden attributable to physical inactivity was connected with older age groups in both sexes. The proportion of DALY attributable to an inadequate intake of fruit and vegetables was highest for men in the age group 55–64 years and for women in the age group 65–74 years of age. The hypertension burden grew with ageing. In younger age groups it was higher for men than for women, and the opposite was true in older age groups. The burden attributable to overweight/obesity increased with age, and was highest at age 55–64 years in both sexes. The burden attributable to a high blood cholesterol level was highest for the age group 55–64 years in men and for those 75 years and over in women.
Burden of ischaemic heart disease (IHD) and stroke in Serbia without Kosovo and Metohia, 2000
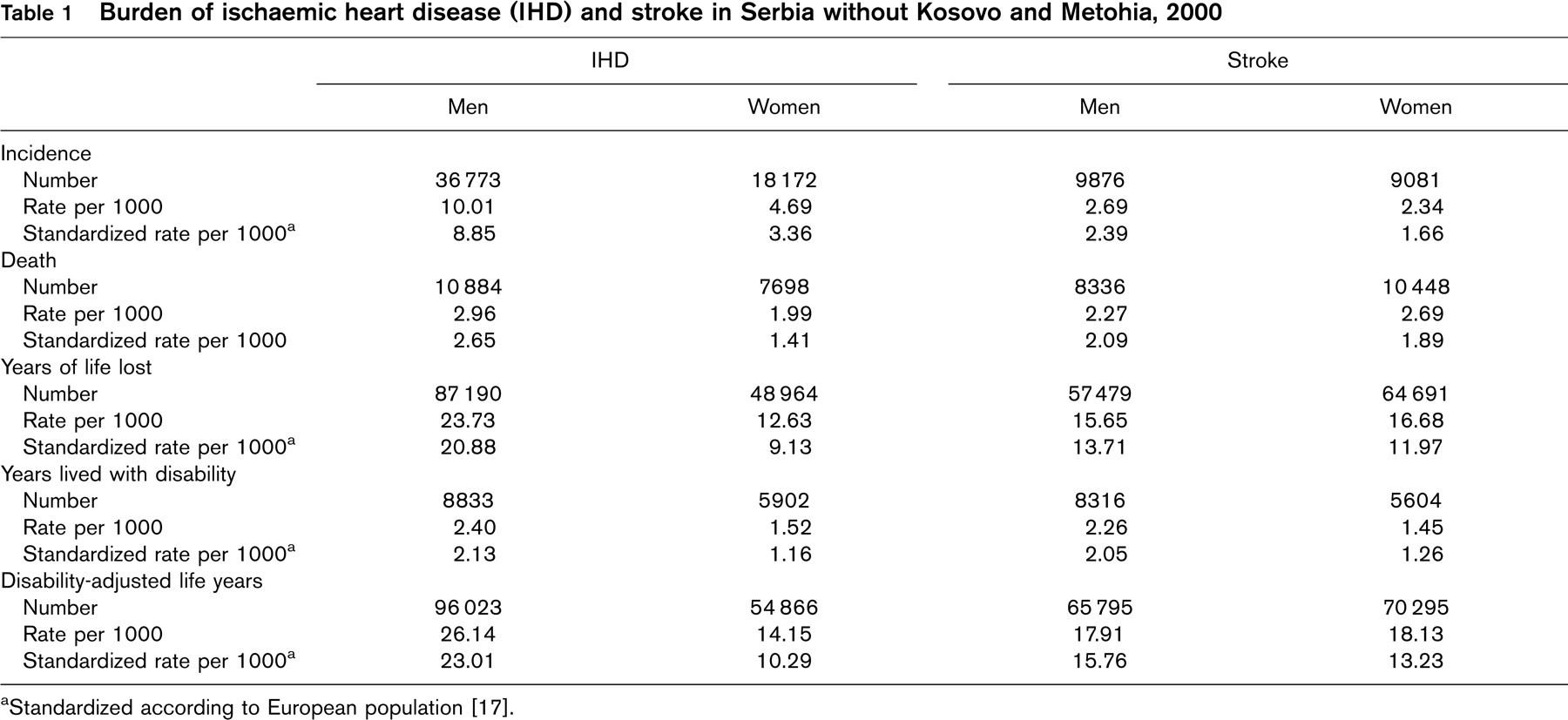
aStandardized according to European population [17].
Discussion
The precision of YLL estimates is almost entirely dependent on the quality of data on the underlying cause of death. Causes of death registration is reasonably accurate in Serbia, but as mentioned in the Methods section there were several ICD-10 categories (‘garbage’ codes and ill-defined or unknown categories) for which deaths were reallocated to disease and injury causes as proposed in the NBD manual [9]. After these reallocations, the distribution of death by age, sex and cause used to estimate the mortality burden differed slightly from cause of death data in the Serbian mortality database. However, these reallocations involved a considerable number of deaths and certainly had some effect on the precision of the YLL estimates.
Incidence data for stroke and myocardial infarction used for the estimation of YLD can be considered reliable because they were obtained from the Register of Myocardial Infarction and Stroke (Novi Sad), which was developed as a part of the known multicentric study (Cindy and Monica Collaborative Center), which provides the best estimates of CVD incidence in Europe [26]. As there were no significant differences in the risk factor prevalence between Vojvodina and central Serbia, it was assumed that incidence data for Novi Sad (Vojvodina), which is not the most complete data on CVD we have, could be extrapolated to the entire population.
Years lived with disability (YLD) and disability-adjusted life years (DALY) per 1000 population and years lived with disability/disability-adjusted life years ratio (%) for ischaemic heart disease (IHD) and stroke in Serbia without Kosovo and Metohia, and the EURO region a
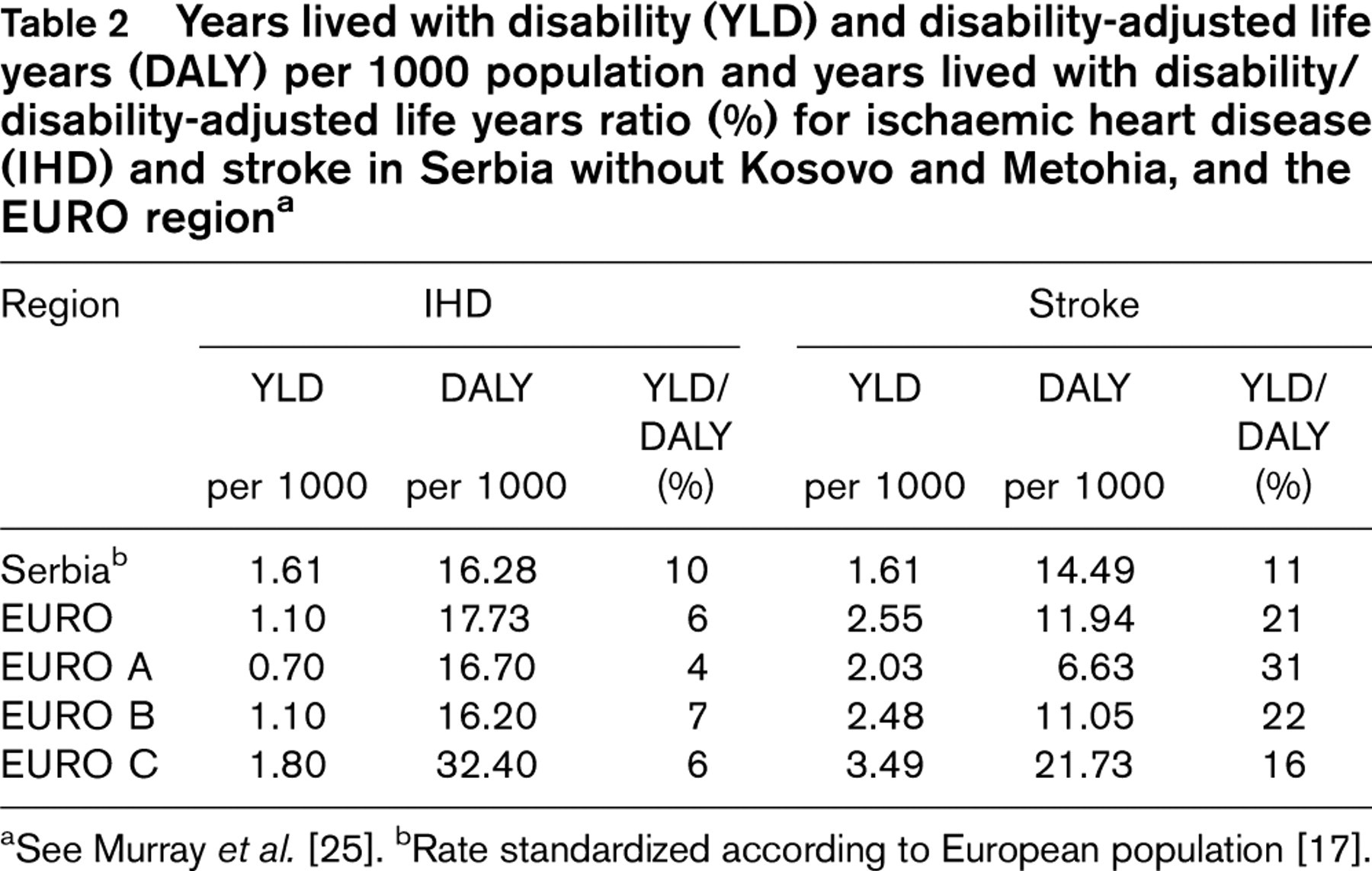
aSee Murray et al. [25].
bRate standardized according to European population [17].
However, as there was no appropriate data on angina pectoris, incidence for that condition was estimated on the basis of hospital utilization data in Belgrade. It can be assumed that the hospitalization of angina pectoris cases is less frequent in comparison with the hospitalization of myocardial infarction cases, and the incidence of angina pectoris was probably underestimated in spite of a number of myocardial infarction cases dying out of hospital. In addition, disability weights for IHD and stroke were accepted from other studies, not derived within a Serbian context. This approach is valuable for reasons of comparability with other populations but, on the other hand, these weights may not completely reflect local community preferences [27].
The model used for the estimation of the burden attributable to various risk factors is a simplified one. Data on risk prevalence in the SBDS study were available only for current exposure status, and may not reflect the level of the true exposure over a period of time. The prevalence of the majority of risk factors was based on self-reported data, and self-reported data may not always be completely valid. However, as the prevalence data for Serbia were very similar to data obtained for the same risk factors in the MONICA study [28] we can consider them to be reliable. The attribution of disease burden to a single risk factor is also a simplification, because several risk factors often occur simultaneously. The overall risk may be greater or smaller than the total for all risk factors. New models based on surveys that measure multiple risk factors in the same population are needed to do more justice to the interaction between risk factors and the effect on the calculation of the burden attributable to them.
Prevalence (%) of some risk factors and ischaemic heart diseases and stroke burden attributable to them, Serbia without Kosovo and Metohia, 2000
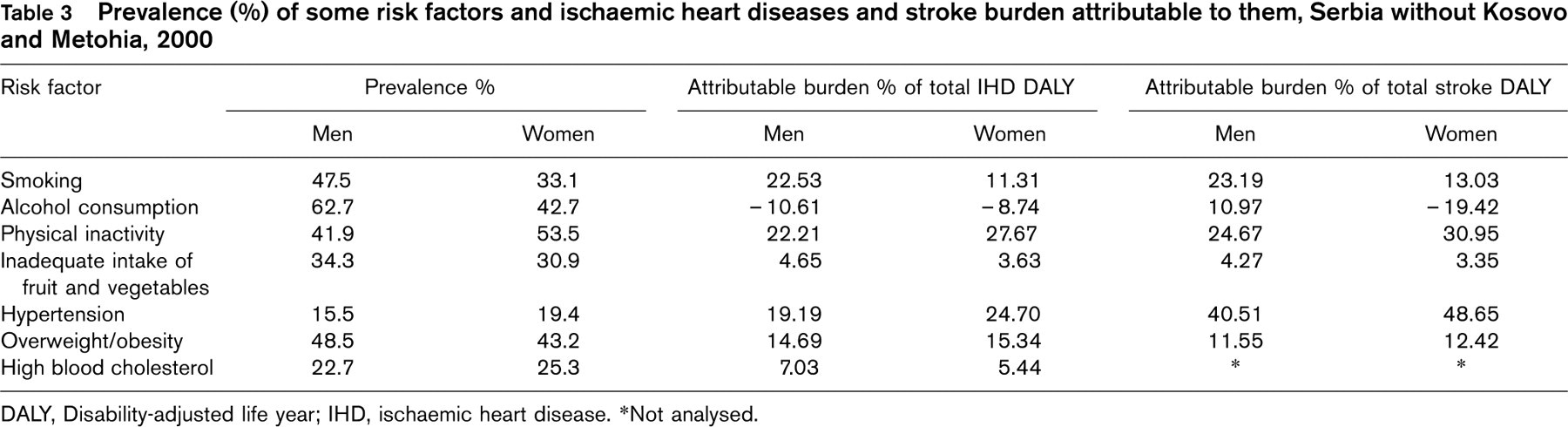
DALY, Disability-adjusted life year; IHD, ischaemic heart disease.
∗Not analysed.
The fact that in SBDS the total burden (DALY) was estimated for a limited number of disorders makes comparison with other populations more difficult, but not impossible. That is, the greatest part of the total burden caused by IHD and stroke was the result of premature death. In the Serbian population, as in populations of developed countries, IHD and stroke are the leading single causes of premature YLL for both sexes, being responsible for 16.7% (IHD) and 15.0% (stroke) of the total YLL [24]. It can be expected that they would be in the first two places had the total burden for all conditions been estimated. The proportion of YLD in DALY for IHD in Serbia was higher than in the EURO region [25], closer to that found in the Victoria study [13]. For an estimation of YLD caused by IHD, the disability duration of angina pectoris was taken from the Victoria study, because it was not available in the GBD study, which probably explains this finding. The proportion of YLD in DALY for stroke in Serbia was half of that in EURO B, and even lower when compared with EURO C. This finding cannot be explained by the method used for YLD calculation. Disability duration of stroke for the subjects surviving 28 days after stroke (approximately 50% of stroke cases) was taken from the South and West DALYs Project [14]. When the Australian model [21] was applied instead, almost the same results were obtained. The great proportion of YLL in the total stroke burden calls for efforts to be made to improve stroke therapy.
The association of IHD and stroke with observed risk factors is well known. The results obtained are close to those found in the GBD study [2] and the Australian study [22]. The main differences were found for sex and age distribution of the attributable burden related to age differences in disease morbidity and mortality, and age differences in the prevalence of exposure to risk factors.
The burden attributable to smoking was very high compared with some other populations [2, 22] as a result of the high prevalence of current smokers in Serbia, which is one of the highest in Europe. There is also a greater percentage of smokers among people younger than 35 years: 49.1% of the student population of Serbia and 27.0% of 15-year-old school children [29].
The main reason for the sex difference in the influence of alcohol on stroke burden is probably because the highest mortality rates for stroke were in the younger age groups among men, and in the old age groups among women. At the same time the harmful effect of alcohol intake for stroke was connected to younger age, whereas benefits were found in ages over 45 years and mostly in the elderly age group.
The main difference between SBDS results for DALY attributable to physical inactivity and the results of other studies [2, 22] is related to the age distribution of the prevalence of physical inactivity. The prevalence for younger age groups in Serbia was very high. For example, the prevalence of a sedentary level of physical inactivity in the age group of 35–39 years was nearly twice as high in Serbia than in the Australian study [22].
Because of the differences in the definition of an inadequate intake of fruit and vegetables, results from Serbia are not completely comparable with other studies, although they were similar to the results for New Zealand [23] and Australian [22] burden of disease studies.
The IHD burden attributable to a high cholesterol level was mainly caused by the increased risk of premature dying. It was lower in comparison with other studies because of the relatively low prevalence of high blood cholesterol. Prevalence data of blood cholesterol levels for Serbia were based on data for the Republic of Srpska [30], but these two populations are very similar in health status, lifestyle and social conditions.
Although these are obvious limitations, the attributable DALY estimates represent a useful measure of the size of the health problem presented by observed risk factors [22]. These estimates can be used as a guide for the prevention of IHD and stroke as well as for evaluating the scope of future health gains obtained by reducing population exposure to these hazards.