
Abstract
Background
Decreased exercise capacity is the main factor restricting the daily life of patients with chronic heart failure. N-terminal pro-brain natriuretic peptide (NT pro-BNP) is strongly related to the severity of and is an independent predictor of outcome in chronic heart failure.
Design
The study aimed to evaluate the effect of exercise training on functional capacity and on changes in NT pro-BNP levels and to assess the effect of exercise training on quality of life.
Materials and methods
Sixty patients (45 men/15 women, mean age 52.7 years; ±5.3 SD), with stable heart failure (45 ischaemic/hypertensive and 15 idiopathic patients), in New York Heart Association (NYHA) functional class II (n = 35) to III (n = 25), with an ejection fraction less than 40%, were randomly assigned to a training (n = 30) and a control group (n = 30). The training group (30 patients) performed 3 months of supervised physical training programme using a bicycle ergometer for 30 min three times a week at a load corresponding to 60–70% of their oxygen consumption (Vo2) peak. The control group did not change their previous physical activity. A graded maximal exercise test with respiratory gas analysis and an endurance test with constant workload corresponding to 85% of the peak oxygen load at the baseline and after 3 months were performed, and at the same times NT pro-BNP levels were measured.
Results
The exercise capacity increased from 15.8 (±2.3 SD) to 29.9 (±2.1 SD) min (P<0.0001) and the peak Vo2 tended to improve from 14.5 (±1.4 SD) to 17.7 (±2.6 SD) ml/kg per min (P<0.0001) during the supervised training period. Vo2 at the anaerobic threshold increased from 12.9 (±1.0 SD) to 15.5 (±1.7 SD) ml/kg per min (P<0.0001). NT pro-BNP levels decreased from 3376 (±3133 SD) to 1434 (±1673 SD) pg/ml (P=0.043). The positive training effects were associated with an improvement in the NYHA functional class.
Conclusion
Physical training of moderate intensity significantly improves the exercise capacity and neurohormonal modulation in patients with chronic heart failure. This is associated with an alleviation of symptoms and improvement in quality of life.
Introduction
Dyspnoea and muscle fatigue are the main limiting factors of exercise capacity in patients with chronic congestive heart failure. This reduced exercise capacity is more importantly influenced by skeletal muscle impairments than by abnormalities of cardiac function [1–3]. The skeletal muscle abnormalities are similar to those found with physical deconditioning [1, 2]. Skeletal muscle atrophy, a change in fibre type, bioenergetics favouring anaerobic metabolism and impaired skeletal muscle blood flow, also associated with other alterations such as apoptosis and chronic inflammation, suggest that peripheral factors may impair oxygen transport and utilization, and may limit exercise performance in congestive heart failure [4–7]. This vicious circle can be interrupted by discouraging a sedentary lifestyle and promoting physical activity. Controlled clinical studies have recently demonstrated that both in-hospital and home-based exercise training programmes of various intensities induce favourable clinical effects by significantly increasing aerobic capacity, delaying the onset of anaerobic metabolism, reducing the sympathetic drive, and increasing vagal tone [8–13]. In recent years, several studies have demonstrated that brain natriuretic peptide (BNP) was an independent predictor of cardiac survival in patients with congestive heart failure [14–17]. Because there is a correlation between BNP and exercise capacity, it has been suggested that BNP assay might be an easy alternative to peak oxygen consumption (Vo2) for the selection of high-risk patients [18]. A recent nonrandomized study showed that exercise training might offer additional non-pharmacological modulation of the activated neurohormonal pathways in the setting of congestive heart failure [19]. In that study after 4 months of training a significant reduction in N-terminal pro-brain natriuretic peptide (NT pro-BNP) plasma levels was observed. Accordingly, we designed a prospective and randomized study to evaluate the effect of exercise training on functional capacity and on changes in NT pro-BNP levels. Another objective of the study was to assess the effect of exercise training on quality of life.
Methods
Patients
Initially, 75 consecutive patients with chronic heart failure in stable condition were recruited. However, after the screening visit at baseline, 15 patients decided not to participate. Therefore, 60 patients (mean age 52.7 years; ± 5.3 SD) were studied. All patients were clinically stable on medical therapy (angiotensin-converting enzyme inhibitors, beta-blockers, nitrates, diuretics, and digoxin, as necessary) in the 3 months before the study. Criteria for eligibility were documented clinical signs and symptoms of heart failure, left ventricular ejection fraction less than 40%, New York Heart Association (NYHA) class II–III, and sinus rhythm. The clinical characteristics of the patients are summarized in Table 1. The cause of heart failure was ischaemic or hypertensive cardiomyopathy (75%) or idiopathic dilated cardiomyopathy (25%). Mitral insufficiency was present in 28 patients, and was mild in all. Exclusion criteria were unstable angina, recent acute myocardial infarction, decompensated congestive heart failure, haemodynamically significant valvular heart disease, poorly controlled cardiac arrhythmias, significant chronic pulmonary illness, renal insufficiency (serum creatinine > 2.5 mg/dl), inability to attend regular exercise training sessions, exercise testing limited by angina or leg claudication, abnormal blood pressure response to exercise testing (systolic blood pressure during exercise > 250 mmHg or diastolic blood pressure > 120 mmHg, systolic blood pressure response decrease > 20 mmHg after a normal increase or decrease below the resting level), and neurological or orthopaedic limitations.
Baseline patient characteristics
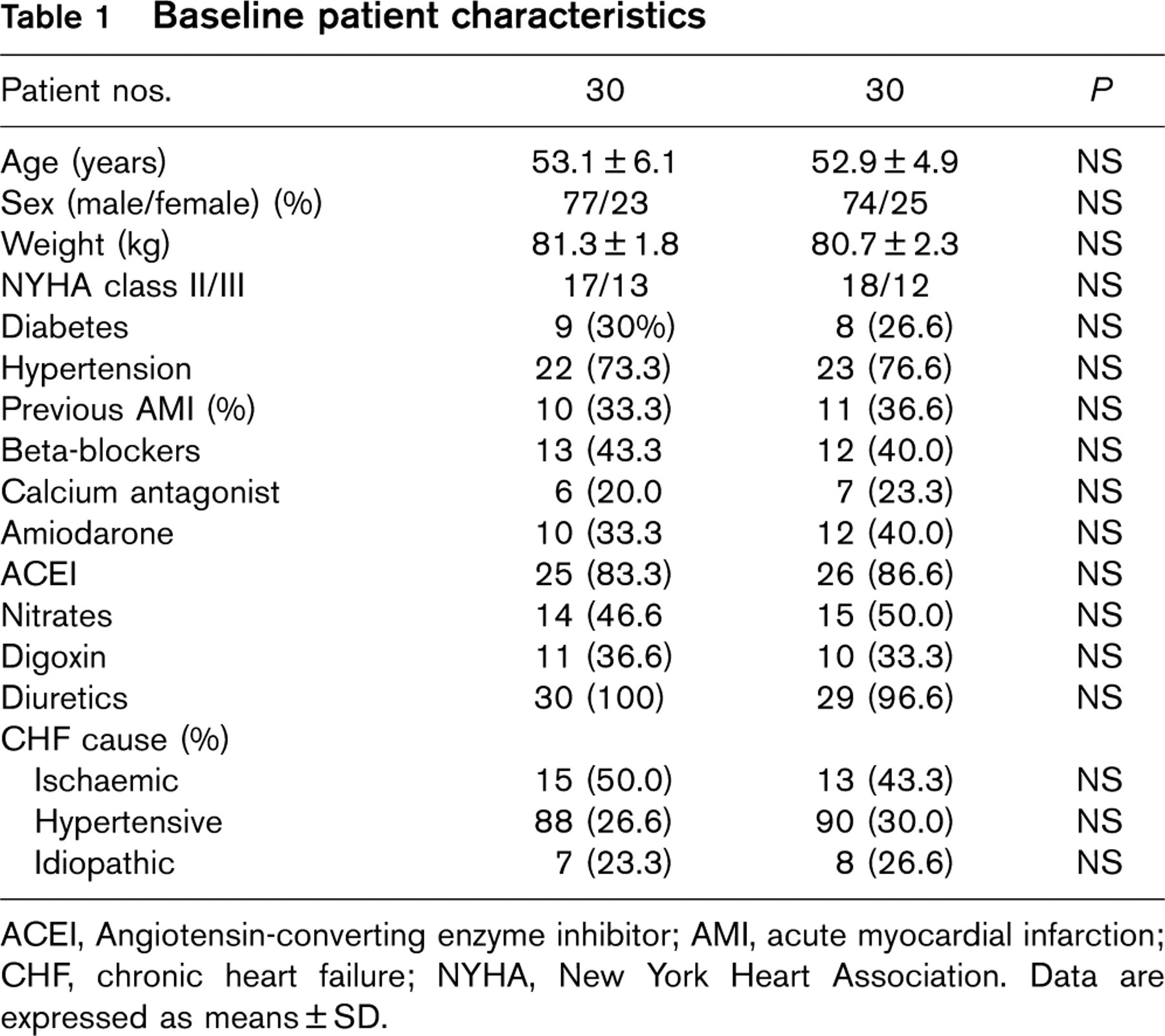
ACEI, Angiotensin-converting enzyme inhibitor; AMI, acute myocardial infarction; CHF, chronic heart failure; NYHA, New York Heart Association. Data are expressed as means ± SD.
Protocol
The protocol, approved by the Ethical Committee of the Buccheri La Ferla Fatebenefratelli Hospital, was a prospective, randomized, controlled study. All patients gave written informed consent. Patients were randomly assigned into two homogeneous groups. Randomization was performed using a preliminary computer algorithm prepared by an external coordinating centre; the assignment of patients was decided by an independent external team of physicians. The patients were randomly and externally assigned to the training group or control group by a central telephone system. The events were communicated by treating physicians to the randomization centre, and this centre provides elaboration of data to the end of the study. The treating physicians were blinded to the results up to the final analysis.
The exercise group (n = 30) underwent a supervised physical training programme using a bicycle ergometer for 30 min three times a week at a load corresponding to 60–70% of their Vo2 peak for 3 months. The control group (n = 30) did not change their previous physical activity. On study entry and after 3 months, in all patients NT pro-BNP levels were measured, and all performed an exercise test with gas exchange analysis and an echocardiographic study. All studies were performed by skilled operators and evaluated by two experienced observers blinded to each other's interpretation. A third observer was asked to resolve differences when agreement was not achieved. A consensus decision was obtained in all cases.
Exercise testing
Patients performed symptom-limited incremental cycle ergometer exercise testing with electrocardiography monitoring at baseline and at 3 months. Patients pedalled in the upright position on an electronically braked cycle ergometer (Lode Corival, Groningen, The Netherlands) at a constant rate of 60 rpm. The work load started at 20 watts for 3 min (warming-up) and increased by 1 watt every 5 s (ramp protocol). Blood pressure was measured by auscultation at every change in work load. The 12-lead electrocardiogram was recorded during the final 30 s of every change in work load and at the peak exercise. Heart rate was determined from the electrocardiograph recording. Symptoms were assessed by means of the 10-point Borg scale rating. Calibration of volumes and gases (oxygen and carbon dioxide) was carefully performed before each test. The ventilatory threshold was measured by the V-slope method [20]. Peak oxygen uptake was measured with commercially available metabolic carts (Sensor Medics model Vmax; Yorba Linda, California, USA) and defined as the highest Vo2 during the last 30 s of exercise.
Exercise endurance was determined by the duration of ergometer cycling at a constant workload corresponding to 85% of the peak Vo2 at the baseline. The test was started with a warming up of 4 minutes: the first 2 min were cycled at one-third and the next 2 min at two-thirds of the final workload. The warming-up period was included in the total cycling time.
Echocardiography
A complete resting two-dimensional echocardiogram and Doppler ultrasound examination (Philips Sonos 5500; Andover, Massachusetts, USA), including all standard views and subcostal imaging of the inferior vena cava, was performed at entry and before discharge. We obtained standard two-dimensional parasternal short-axis and apical two and four-chamber views during held inspiration. The analysis of wall motion was obtained by subdividing the left ventricular chamber into 16 segments according to the American Society of Echocardiography recommendations [21]. Left ventricular end-diastolic volume (EDV) and end-systolic volume (ESV) were obtained from the apical four and two-chamber views by a modified Simpson's rule, from which the ejection fraction was automatically calculated as the differences between EDV and ESV normalized to EDV. The interobserver and intraobserver coefficients of variations were 4 and 3%, respectively.
N-terminal pro-brain natriuretic peptide
Blood samples were taken through an intravenous cannula placed at least 30 min before sampling, with the patients resting quietly semirecumbent. Samples in chilled ethylenediammine tetraacetic acid vacutainers were centrifuged within 20 min at 4°C, and NT pro-BNP immunoassay (Roche Diagnostics, Branchburg, New Jersey, USA) was determined on an Elecsys 2010. The analytical range of the NT pro-BNP assay extends from 5 to 35 000 pg/ml. The interassay coefficient of variation was 6.1% for 28.8 pg/ml, 8.4% for 586 pg/ml, and 10.2% for 1180 pg/ml. The laboratory technician who measured NT pro-BNP was at a different site and was blinded to the characteristics of the patients and the results of the echocardiograms and exercise tests.
Quality of life
Quality of life was assessed at baseline and after 3 months in both groups using the Minnesota Living with Heart Failure Questionnaire [22]. This instrument is a patient self-assessment measure and consists of 21 items focused on patient perceptions concerning the effects of congestive heart failure on their physical, psychological, and socioeconomic lives. Some studies have shown this questionnaire to be responsive to changes in quality of life in patients with chronic heart failure [13, 23].
Statistical analysis
Results are expressed as the mean ± SD. The statistical analysis was performed by the two-tailed t-test to identify differences between the groups and analysis of variance (ANOVA) for repeated measures with Bonferroni correction for intragroup data. Nominal data were analysed by the chi-squared test or Fischer's test. Differences were considered significant at a P value less than 0.05. All analyses were performed using SPSS version 11.5 software (SPSS Inc., Chicago, Illinois, USA).
Results
Baseline characteristic
Sixty patients were randomly assigned (30 in the exercise group and 30 in the control group). There were no differences between the exercise training and control groups with respect to age, resting ejection fraction, NYHA class, cause of heart failure, or duration of heart failure. There were no differences in types and doses of medications, blood chemistry, and previous cardiac events (Table 1).
Exercise endurance
There was no significant baseline difference for exercise endurance between exercise (15.8 min; ±2.3 SD) and control (15.3 min; ±2.5 SD) groups. There was a significant increase in exercise endurance compared with baseline at 3 months for the exercise group (29.9 min; ±2.1 SD; P < 0.0001). No significant differences were found in control group at 3 months (16.4 min; ± 2.7 SD; P = 0.10; Table 2).
Incremental exercise test performance
There was no significant baseline difference for peak oxygen uptake and Vo2 at the anaerobic threshold between the exercise and control groups. After 3 months, the peak oxygen uptake and Vo2 at the anaerobic threshold of the exercise group increased significantly compared with baseline (P < 0.0001) and with the control group (P < 0.0001). No significant difference was found in the control group at 3 months (P = NS). The NYHA functional class decreased from 2.6 (± 0.1 SD) to 1.6 (± 0.1 SD) after 3 months' training (P = 0.025). No change was observed in this variable in the control group (Table 2). All the enrolled patients completed the study.
N-terminal pro-brain natriuretic peptide
There was no significant baseline difference for NT pro-BNP levels between exercise (3376 pg/ml; ± 3133 SD) and control (3285 pg/ml; ± 3012 SD) groups. NT pro-BNP levels decreased significantly in the exercise group compared with baseline at 3 months (1434 pg/ml; ± 1673 SD; P < 0.0001). No significant difference was found in the control group at 3 months (2985 pg/ml; ± 3241 SD; P = 0.72; Table 2).
Echocardiography
There were no significant baseline differences between groups for ejection fraction, EDV or ESV. No significant changes in left ventricular diameter were observed after 3 months in either group. The ejection fraction was also unchanged (Table 3).
Quality of life
There was no significant baseline difference in the Minnesota Living with Heart Failure scores for trained (31.2; ± 2.2 SD) and untrained (30.6; ± 2.5 SD) patients. After 3 months, there was a greater improvement in the Minnesota Living with Heart Failure questionnaire response in the exercise group compared with baseline at 3 months (35.5; ± 1.9 SD; P = 0.0001) No significant difference was found in the control group at 3 months (31.2; ± 2.6 SD; P = 0.36).
Adverse events during exercise training
No significant cardiovascular events occurred during the training sessions. Six patients had sporadic supraventricular and ventricular premature contractions during exercise and recovery. No patient had angina during the training periods. Compliance with exercise training, defined as the percentage of sessions attended, averaged 93% (range 81–100%). No drop out was observed during the study period.
In addition, we also followed the patients who refused consent to participate in the study, and they showed similar results to the control group (data not shown).
Discussion
The results of this study demonstrate that moderate exercise training improves functional capacity and neurohormonal modulation in patients with stable chronic heart failure. This beneficial effect translated into a favourable outcome (improvement in NYHA functional class, alleviation of symptoms, and improvement in quality of life). These benefits appear to be primarily related to changes in peripheral haemodynamics and skeletal muscle by reversing a ‘deconditioning’ process, common in sedentary heart failure patients. Leg blood flow has been shown to increase at maximal exercise, whereas during submaximal exercise significant decreases in blood lactate concentrations and vascular resistance occur in trained patients [8, 24, 25]. Patients with heart failure exhibit a blunted vasodilator capacity in the skeletal muscles during exercise, which contributes to increased total peripheral resistance and peripheral hypoperfusion, with a subnormal blood flow response to exercise. Two primary reasons for this reduction in nutritive blood flow are a decreased release of endothelium-derived relaxing factor (nitric oxide vasodilator system) from arterioles supplying the metabolic active muscles, and an exaggerated increase in vasoconstrictive neurohormones such as endothelin, norepinephrine, renin, angiotensin II, and vasopressin (vasoconstrictor system). It has recently been shown that exercise therapy exerts its primary effects on the endothelial function of peripheral resistance vessels, contributing to the reduction in peripheral resistance at rest and at peak exercise [26]. Peripheral vascular resistance may also be reduced by attenuating sympathetic overactivity and by increasing vagal tone, as noted in a multicenter study, the European Heart Failure Training Group [1]. Endothelin and norepinephrine are closely correlated with exercise capacity in patients with chronic heart failure [27, 28]. However, the use of these markers is difficult, impractical, and associated with long-lasting assays [29]. Even if a superiority of NT pro-BNP has not been shown, for this reason NT pro-BNP seems to be the most simple, reliable, readily available laboratory marker of cardiac dysfunction at present. Several studies have recently demonstrated that there is a good correlation between BNP and exercise capacity [14–18]. In our study, we found that patients performing training had an improvement in exercise capacity and a significant reduction in NT pro-BNP levels after 3 months of exercise training. The present results are in agreement with most of the earlier studies demonstrating the beneficial effects of physical training in patients with chronic heart failure. Coats et al. [9] observed a mean increase of 18% in the peak oxygen uptake after 6 weeks of exercise training at 60–80% of peak heart rate. Compared with the earlier studies, however, our data have the advantage of having a well-matched separate control group. We think that this is important in studies investigating exercise capacity, because the training effect of repeated exercise tests may exaggerate the effect of the intervention. This fact is emphasized by our results showing that the exercise endurance also tended to improve in the control group. It has been shown that in patients with chronic heart failure, the change in peak Vo2 correlates with the intensity of training (hours per week) as in healthy individuals [8]. Therefore, the training programme should be intensive enough to be beneficial but not too strenuous to preserve the motivation of the patients to continue. We chose a training programme of moderate intensity, 60–70% of peak Vo2 for 30 min three times a week commonly regarded as the minimum to improve functional capacity in healthy individuals. This probably explains the fact that no significant cardiovascular event occurred during the training session, and compliance with exercise training, defined as the percentage of sessions attended, averaged 93% (range 81–100%). Peak Vo2 is a valid parameter to measure the effect of physical training in patients with chronic heart failure, and has also been found to correlate with prognosis [2, 10, 13]. However, peak Vo2 does not correlate as well with changes in the quality of life score as submaximal exercise capacity [30]. Our study showed that the increase in exercise endurance at the submaximal workload (89% of improvement in trained patients after 3 months) was far more pronounced than the increase in peak exercise oxygen uptake (22% of improvement in trained patients after 3 months). The improved capacity to exercise at submaximal levels contributes to the general wellbeing of the patients in their daily activities. This is reflected in the present study by the improvement of the NYHA functional class and of the quality of life in the training group. In addition, we observed a significant reduction in NT pro-BNP plasma levels in the training group, whereas the control group did not show any difference. This finding is probably related to an improvement in cardiac function or a reduction in wall stress. We hypothesized that this result is determined by the effects of the training on peripheral compliance, and it could be the explanation of the improvement in quality of life. There were no significant differences observed in cardiac function between the exercise and control groups at 3 months. These findings are also consistent with other studies, which found that training does not adversely affect cardiac function [2, 13].
Exercise capacity, anaerobic threshold, and New York Heart Association functional class at baseline and after 3 months
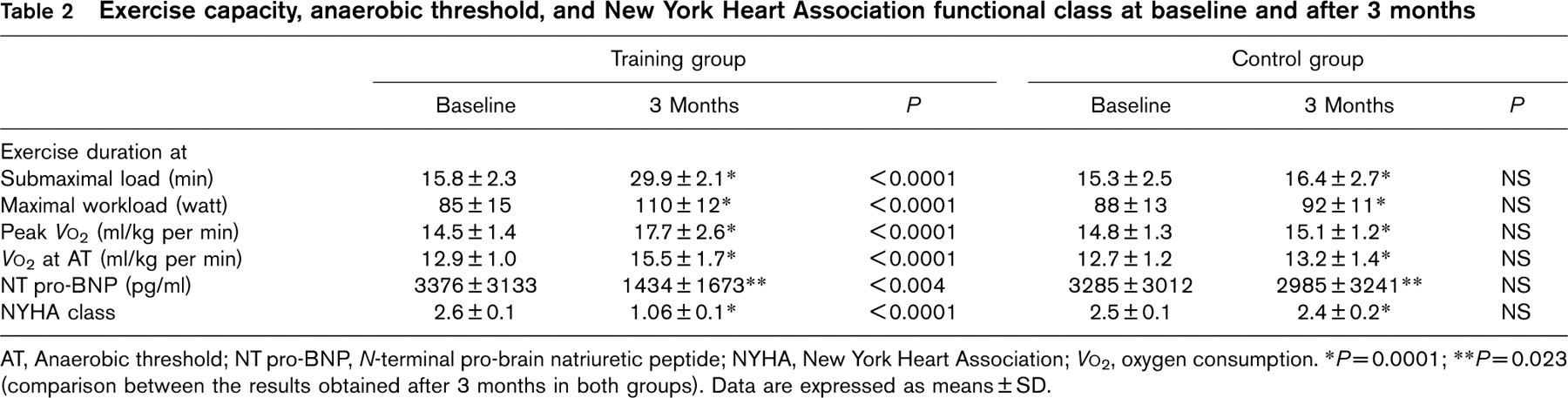
AT, Anaerobic threshold; NT pro-BNP, N-terminal pro-brain natriuretic peptide; NYHA, New York Heart Association; Vo2, oxygen consumption.
∗P=0.0001;
∗∗P=0.023 (comparison between the results obtained after 3 months in both groups).
Data are expressed as means ± SD.
Echocardiographic results at baseline and after 3 months

Conclusion
There is increasing evidence that physical training improves exercise capacity, reduces symptoms, and improves quality of life, in patients with stable mild or moderate chronic heart failure. Furthermore, training has been shown to affect some parameters favourably, such as peak Vo2 [9, 26] and plasma BNP levels [17, 18], known to be independent prognostic factors in chronic heart failure. Therefore, physical training may also favourably affect the course of chronic heart failure, but a definitive effect on prognosis remains to be proved in future large studies.