
Abstract
Background
Design and methods
Results
Discussion
Introduction
Approximately one out of 100 children [1] is born with congenital heart disease (CHD). The spectrum ranges from patients without or with minor impairments to very severe handicaps. In the past decades chances of survival have been prolonged by the improvement of surgical techniques [2], and by the development of sophisticated medical treatment after surgery. With improved medical success the question arises as to how well these patients are integrated into day-to-day life.
A number of studies [3] have addressed this question by examining patients’ quality of life [4, 5], but most of them covered a relatively short period of time after surgery. More recent work [6] has also considered the long-term effects of CHD [3, 7]. A few have dealt with the question of how individuals with CHD manage their lives in the long run, and one [8] (N = 47; age 3.5-17 years) was directed towards academic ability before treatment and 12 years later. In another study [3] the school achievement of patients with tetralogy of Fallot was found to be lower than expected, and employed subjects had jobs below their qualification level. A recent study from the Netherlands [9] reported that CHD patients had reached lower educational and occupational levels than the general population. In a Finnish study [10] different findings emerged, although the educational levels of individuals with CHD were comparable with the general population. Patients attained higher occupational positions than expected.
None of these studies has directly addressed the question of whether individuals with CHD have the same social mobility as the general population, i.e. whether CHD patients may attain the same or different levels of socioeconomic positions as the parental generation. Mobility analyses also take the social background of patients into account, and thus cohort effects can be avoided that may occur if different age groups are compared. In order to set social mobility as an important aspect of life chances in perspective, it has to be considered how many patients did not enter the labour market. The study to be reported below is the first to address social mobility by answering the following questions: Does the severity of CHD impede entry into the labour market? Does intergenerational upward and downward social mobility differ between individuals with operated CHD according to the severity of the initial defects? between individuals with operated CHD and a population sample of the same age?
As the results of the studies published so far are contradictory, we did not formulate hypotheses on the direction of the relationships, although we expected the severity of the disease to limit labour market participation.
Methods
The patient population consisted of males and females who underwent surgery for CHD at the University Hospital of Göttingen. At the date of interview or at examination, patients were between 14 and 45 years of age, and in order to ensure comparability with the control sample, the minimum age for being included in the following analyses was set at 17 years. Individuals with syndromes (i.e. Down syndrome, Marfan syndrome, Noonan syndrome, and Williams-Beuren syndrome), unclear diagnoses and patients whose heart disease turned out not to be congenital were excluded.
The study protocol was approved by the local ethics committee, and written informed consent was obtained from all subjects.
Data were collected by means of face-to-face interviews and by a series of medical examinations (spiroergometry, cardiological measures). The severity of the CHD was classified according to the type of surgery, which is strongly associated with the complexity of congenital heart defects at birth. With increasing complexity, curative surgery becomes unlikely, and outcomes will be more reparative or palliative and accompanied by higher degrees of residual symptomatology. The type of surgery thus rather reflects a physiological measure of initial severity associated with a congenital heart defect. According to Perloff [11] the following classification was used: curative: defects cured by surgery without or with minor postoperative residua, sequelae, or complications remaining (atrial and ventricular septal defects and arterial duct). Reparative: defects with repaired or reconstructed anatomy with obligatory postoperative residua or sequelae (all defects not assigned to the curative or palliative group). Palliative: defects with basic morphological anomalies being neither repaired nor reconstructed (Fontan circulation and transposition of the great arteries after the Mustard or Senning procedure).
The control sample was drawn from the German SocioEconomic Panel (SOEP). It is a nationwide longitudinal project designed to provide representative data for Germany in order to depict social change and stability in living conditions. The first wave was carried out in 1984, and annual follow-ups are conducted in order to catch up with recent developments and to compensate for panel attritions. Detailed accounts of the SOEP have been published elsewhere [12]. The comparisons performed in the following analyses are based on the 2002 survey.
SOEP data are available as public use files for purposes of national and international research. The minimum age for being included is 17 years, and for the sake of comparability the upper age limit was set at 45 years.
For cases and controls classifications of socio-economic positions are based on the International Standard Classification of Occupations (ISCO-88) that was transformed into a continuous social status scale as proposed by Ganzeboom and Treiman [13]. Intergenerational social mobility was determined by computing differences between parents’ and respondents’ positions. As many missing data occurred for mothers’ position, in the following analyses the fathers’ information was used as an indicator of parental socio-economic position. Positive scores indicate that a respondent has reached a higher position than his or her father (upward mobility), negative scores indicate social downward mobility. In the case of the same score for both generations, no social mobility has occurred.
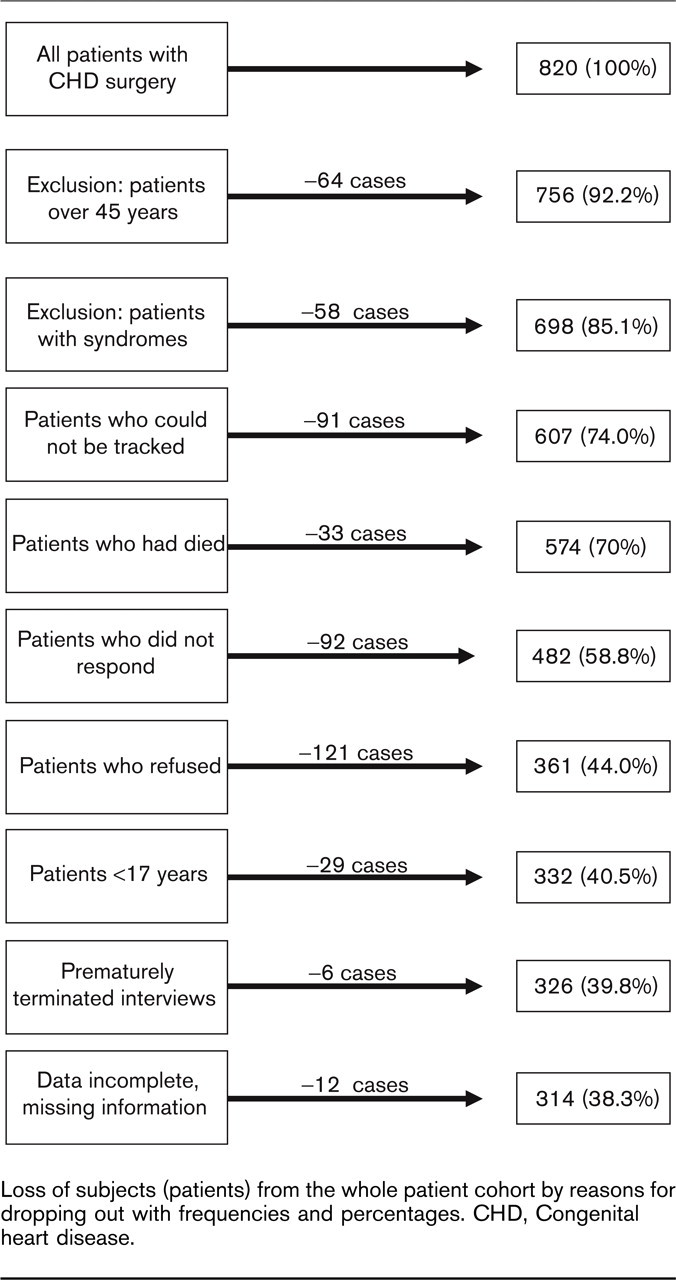
Loss of subjects (patients) from the whole patient cohort by reasons for dropping out with frequencies and percentages. CHD, Congenital heart disease.
Statistical analyses
Ordinary least squares regression was used as the appropriate procedure for estimating effects on intergenerational social mobility. The results are presented as standardized regression coefficients (β), ranging from 0 (no effect) to 1.0 (perfect relationship). All statistical calculations were performed using Stata statistical software, release 8SE (Stata Corp., College Station, Texas, USA).
Results
In 2003 a maximum of three written invitations for participation and a detailed explanation of the study were sent out. In the case of a positive response appointments were made by telephone, then respondents came to the outpatient clinic where the examinations for the study were combined with medical checkups.
Altogether, 820 patients with operated CHD were registered, but the final study population was smaller. A complete account of the loss of patients from the whole cohort can be found in Fig. 1.
Participants and non-participants did not differ with respect to the type of surgery, type of heart defect, sex, and age. In multivariate analyses it turned out that the group with palliative surgery had a somewhat higher likelihood of being represented among non-participants. The subgroup of individuals with transposition of the great arteries and single ventricle tended to be more likely to participate.
In terms of CHD type, 83 (26.4%) were born with tetralogy of Fallot, 39 (12.4%) had a transposition of the great arteries, 19 (6.1%) had a single ventricle, 80 (25.5%) had a left-to-right shunt, 83 (26.4%) had a stenosis type, and 10 (3.2%) had miscellaneous types of CHD, thus the final patient population consisted of 314 individuals (Table 1). In 53% of patients the operation was performed before the age of 6 years, in 76% it took place before the age of 10 years, and 90% underwent CHD surgery before the age of 16 years (mean age at surgery 7.3 years; SD 7.4).
In the SOEP follow-up of 2002 the total number of subjects between 17 and 45 years was 12 016, but as a result of missing data on the biographical dataset only 4864 women and men made up the control group (Table 1). The proportion of subjects refusing to respond to the biographical questions was 0.4%. As the mean age in the patient group was lower than in controls (Mpatients 26.9 years, Mcontrols; T= 11.76; P < 0.01), age had to be introduced in all multivariate analyses.
At the first step, the patient population is considered by differentiating between those who had entered the labour market and experienced intergenerational mobility and patients who had not been economically active at the date of the interview (Table 1). Thirty-seven patients had given up their jobs prematurely for health reasons. The most salient characteristics of this group are the relatively high proportions with palliative surgery, and the patients who had given up their jobs also had the highest mean age (32.2 years; SD 7.4) compared with the economically active individuals (28.2 years; SD 7.6). For 61 subjects no information on socio-economic position was available. Their mean age was lower (22.3 years; SD 8.8) than of the patient group as a whole. Splitting them up according to employment status, 18 had a job, but their social position was not available, five were still apprentices, 27 were at school or university, one woman was a housewife, one man did his military service, seven were unemployed, and for two subjects no information on the reasons was available.
Basic characteristics of the patient sample and controls
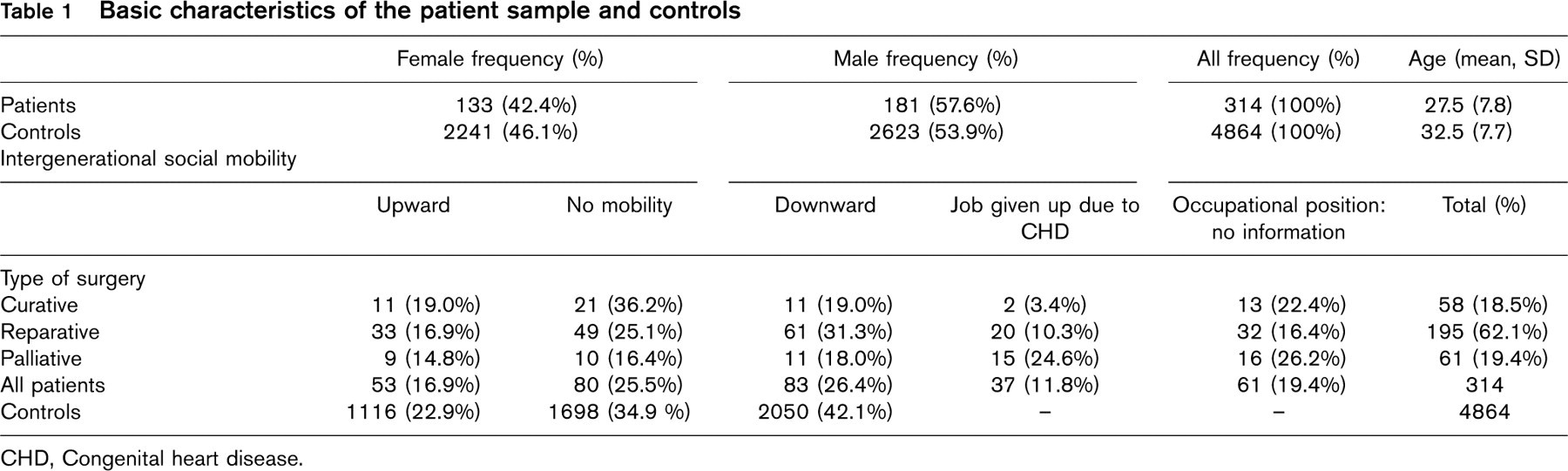
CHD, Congenital heart disease.
Comparisons of intergenerational mobility for patients
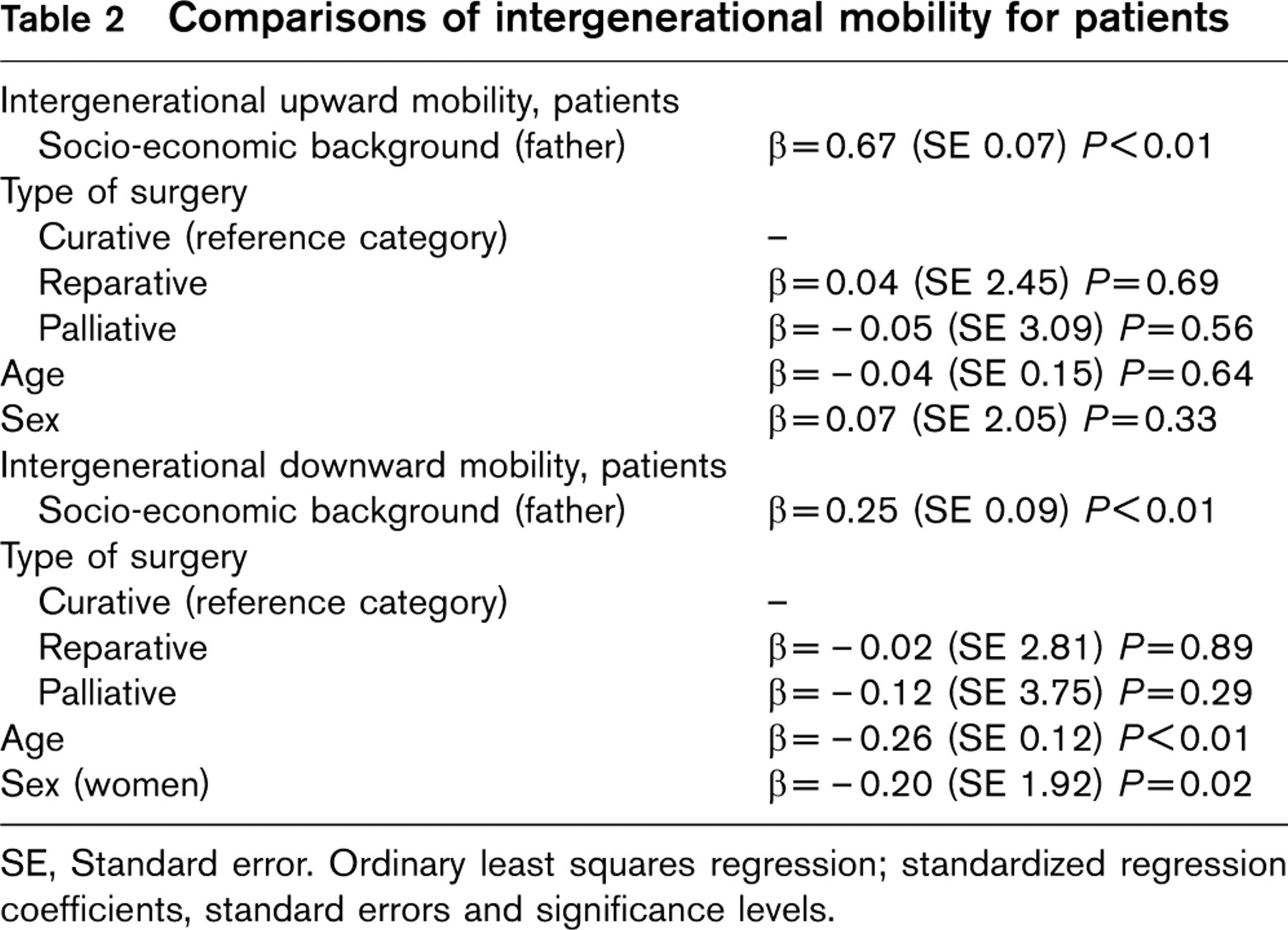
SE, Standard error. Ordinary least squares regression; standardized regression coefficients, standard errors and significance levels.
At the second step, intergenerational social mobility in the patient group was considered (Table 2). For upward social mobility parental socio-economic background turned out to have the strongest effect (β = 0.67) In this case disease severity was unimportant, and the same held for age and sex.
For downward mobility the social background had only a moderate effect (β = 0.25), and there was a significant sex effect, i.e. downward mobility in women is less likely to occur than in men. In order to exclude selection effects, the analyses of this step were repeated by including the patients who had given up their job for health reasons. Their last occupation was used for classifying them. It turned out that for this case the effects of the familial background were slightly higher, but the substantial results as reported in Table 2 remained unchanged.
At the final step, patients and the population sample were compared with respect to social mobility (Table 3). Concerning upward mobility, the social background as measured by fathers’ socio-economic position turned out to have a strong effect on respondents’ mobility. Group membership (patients or controls) had only a negligible effect, the same held for sex, thus there was no need for separate analyses for women and men.
Separate analyses for patients and controls confirmed these results, but in patients the regression effect of the social background was smaller, although statistically significant. Again social mobility was not affected by group membership, and there was only a negligible sex effect. After dividing by group membership, the results remained largely unchanged, but in the patient group an age effect emerged.
Discussion
Social mobility in patients and controls
We started with the question as to whether individuals after CHD surgery can expect the same prospects of intergenerational social mobility as the general population. These analyses had been performed in order to examine to what extent medicine is successful in setting preconditions for leading a normal life. We have shown that, once having entered the labour market, the former patients did not differ from the general population with respect to their social mobility, and the regression analyses have shown that the severity of the heart defect did not matter. As known from the general population, mobility is strongly dependent on respondents’ social background. This holds particularly for upward mobility, in which the effect had been more pronounced in patients than in controls, and this may be explained by patients’ parents being more considerate and more concerned for their offspring.
Comparisons of intergenerational mobility for patients and controls
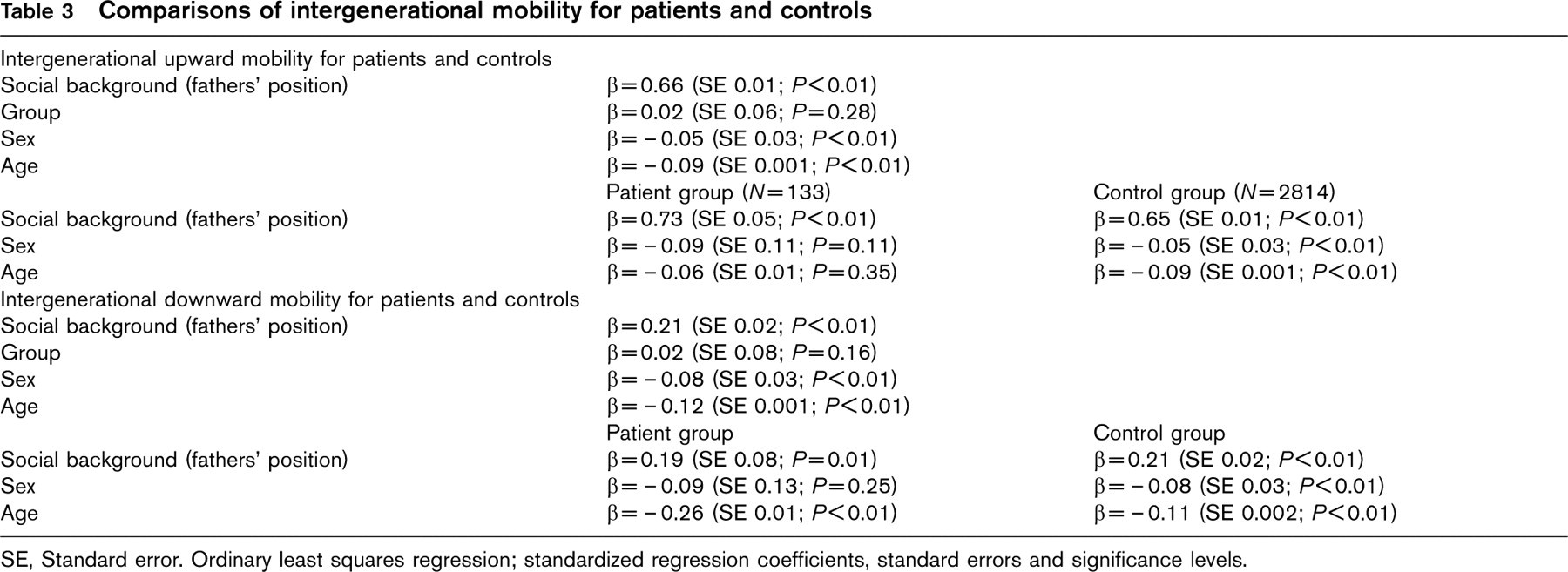
SE, Standard error. Ordinary least squares regression; standardized regression coefficients, standard errors and significance levels.
There is more similarity than dissimilarity between patients and controls, and this result is different from an earlier study [9] in which patients were reported to having reached lower positions than the general population. However, that study is not directly comparable with ours because social mobility had not been considered. Our findings are rather in line with a Finnish study [10], in which CHD patients did better than the average population, a conclusion that is complemented by an unemployment rate of 2.2% in our patient group, a level that is lower than in controls from the SOEP (5.2%).
The finding that 37 patients gave up their job prematurely gives a hint that social mobility processes may also occur beyond the age limit set in our study. Their age mean was higher than in the remaining study population, and there is evidence that in CHD patients the risks of cardiac insufficiency may increase with age [14]. In a recent Norwegian study [15] it was shown that deteriorating health conditions beyond the age of 45 years, with increasing sickness absences and the need for more medical treatment may lead to mobility differences between healthy and less healthy individuals. We do not have information about the number of patients whose health puts them at increased risks of dropping out of employment in the future. Predicting this figure on the basis of our data is difficult and is likely to be inaccurate. Analyses of our cardiological data have shown that there is a relationship between heart failure as the primary cause of deteriorating physical condition and age, but it is not linear, and the risk of heart failure differs by the type of heart defect [14].
It has to be emphasized that our findings reflect the formal aspect of social mobility, and cannot give information on whether patients could take up the careers they had wished to. Their heart defect may have psychological effects because it had been shown that CHD patients differed from the general population in terms of depression, anxiety [16], and increased feelings of physical vulnerability [17], although the data on psychological effects are inconsistent.
Individuals inside and outside the labour market
The 61 patients for whom no information on occupational position was available do not contradict the conclusions concerning social mobility. Besides unemployed individuals, this group also contains apprentices and students who had not been classified for socio-economic position. Only the two subjects whose data on socio-economic status were unavailable may not have entered the labour market because of their bad health. Taken together, these findings may encourage patients to lead a life as close as possible to the life of individuals without a heart defect.
Beyond these positive findings, a dividing line exists within the patient group. It refers to individuals who had been excluded before the study began, especially those with syndromes that are associated with deficits ranging from mild cognitive impairments to severe mental retardations. Most of them will hardly be able to lead an independent life, instead they may need continuous care.
Another group, mostly patients who received palliative operations, will not be able to enter the labour market because of severe physical impairment. They are part of the group who did not participate in the study; their number may be small, but is difficult to quantify without having knowledge of the severity of their residual symptoms.
Alternative systems for classifying patients
Patients were classified by type of surgery [11], a system summarizing different heart defects according to the medical success that can be achieved by surgical treatment. It is highly associated with probable health impairments after discharge and is thus independent of patients’ judgement. The type of surgery was given priority over other cardiological classifications that are based on subjective reports of impairments [18], such as the Ability Index [19] or NYHA, a classification proposed by the New York Heart Association [20]. The latter also depict present states of mind or perceptions that may be confounded by individual success irrespective of the degree of physical impairment. Such measures are inappropriate for studies in which independent and dependent measures are assessed concurrently.
Limitations
The study patients had been recruited from one hospital only. Although it has a large catchment area, the practice of care differs from other sites, because patients with CHD were treated in the Department of Paediatric Cardiology also after having reached adulthood. Usually patients over 18 years are referred to adult cardiological departments, but we do not know whether the treatment in both schemes is different with respect to long-term therapeutic success.
There is reason to assume that patients with more severe residual symptomatology did not participate in the study, thus we may overestimate the number of economically active individuals. As this was a cross-sectional study, we could not take subjective factors like self-confidence or sense of control into account. These may change over the years and determine the decision to take up work. Although their numbers are small and may refer to the less severe cases of CHD only, we cannot examine the effects of surgery at a later age on the decision to take up work and on social mobility.
Another source of bias may arise out of differential response behaviour. Patients who are living in bad conditions, who have been downwardly mobile or depressed, and those rating their health as bad may have refrained from participating in the study. There is indeed evidence that such factors are associated with a decrease in response rates [21, 22], also low socio-economic position may have similar effects. This may lead to erroneous conclusions on the health of target populations, thus CHD patients as a group may appear more successful and healthy than they are. As this affects patients and control groups, it will have only minor effects on the results of our mobility analyses.
Finally, paediatric cardiac surgery has made progress over the past decades, and patients with the same underlying defect will have different prospects depending on when the operation took place. The related time-dependent effects can hardly be depicted in our study, and we had to confine our analyses to the whole group of patients.
Conclusion
A considerable proportion of patients after surgery for CHD could not or did not enter the labour market, but those who did experienced social mobility rates that are comparable with the general population.