
Abstract
Background
Objectives
Methods
Keywords
Introduction
Lipoprotein-associated phospholipase A2 (Lp-PLA2)is an enzyme that circulates largely bound to low-density lipoprotein [1]. Because it can hydrolyze oxidized phospholipids (which leads to the generation of pro-inflammatory products including lysophosphatidylcholine and oxidized free fatty acids), there is interest in the pro-inflammatory properties of Lp-PLA2 [1, 2]. This enzyme can, however, also hydrolyze platelet-activating factor (a factor which helps to activate platelets, monocytes, and macrophages), consistent with anti-inflammatory activity [3]. Available observational studies of the risk of cardiovascular diseases and various circulating markers of Lp-PLA2 (typically involving measurement of platelet activating factor actylehydrolase mass or activity) have reported generally positive associations (Table 1) [4–12]. These studies have, however, generally involved too few coronary heart disease (CHD) cases (and even fewer cases of other types of vascular disease) to enable a reliable assessment of associations under different circumstances (such as at different ages; in women and men; at different levels of other risk factors), or of the shape of any dose-response relationship. Moreover, most studies have related CHD risk to the baseline measurements of Lp-PLA2 (which can lead to substantial underestimation of any association due to ‘regression dilution’ [13]) and have involved different approaches to adjustment for possible confounding factors [14].
Prospective studies of lipoprotein-associated phospholipase A2 and cardiovascular diseases published by May 2006
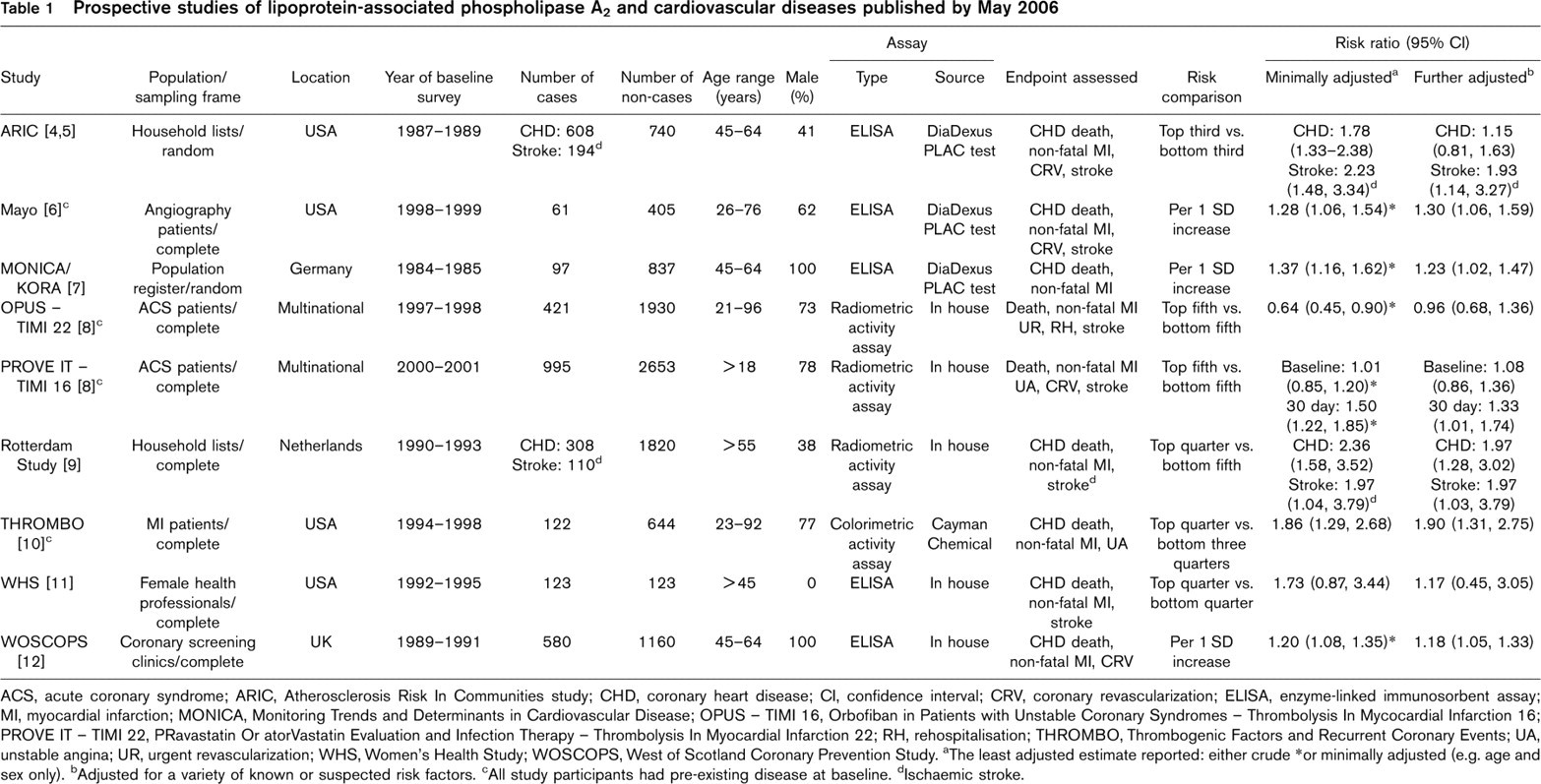
ACS, acute coronary syndrome; ARIC, Atherosclerosis Risk In Communities study; CHD, coronary heart disease; CI, confidence interval; CRV, coronary revascularization; ELISA, enzyme-linked immunosorbent assay; MI, myocardial infarction; MONICA, Monitoring Trends and Determinants in Cardiovascular Disease; OPUS – TIMI 16, Orbofiban in Patients with Unstable Coronary Syndromes – Thrombolysis In Mycocardial Infarction 16; PROVE IT – TIMI 22, PRavastatin Or atorVastatin Evaluation and Infection Therapy – Thrombolysis In Myocardial Infarction 22; RH, rehospitalisation; THROMBO, Thrombogenic Factors and Recurrent Coronary Events; UA, unstable angina; UR, urgent revascularization; WHS, Women's Health Study; WOSCOPS, West of Scotland Coronary Prevention Study. aThe least adjusted estimate reported: either crude ∗or minimally adjusted (e.g. age and sex only). bAdjusted for a variety of known or suspected risk factors. cAll study participants had pre-existing disease at baseline. dIschaemic stroke.
Collaborating prospective studies of lipoprotein-associated phospholipase A2 and cardiovascular diseases known to be in progress but not reported by May 2006 (numbers of disease cases listed are only estimates)
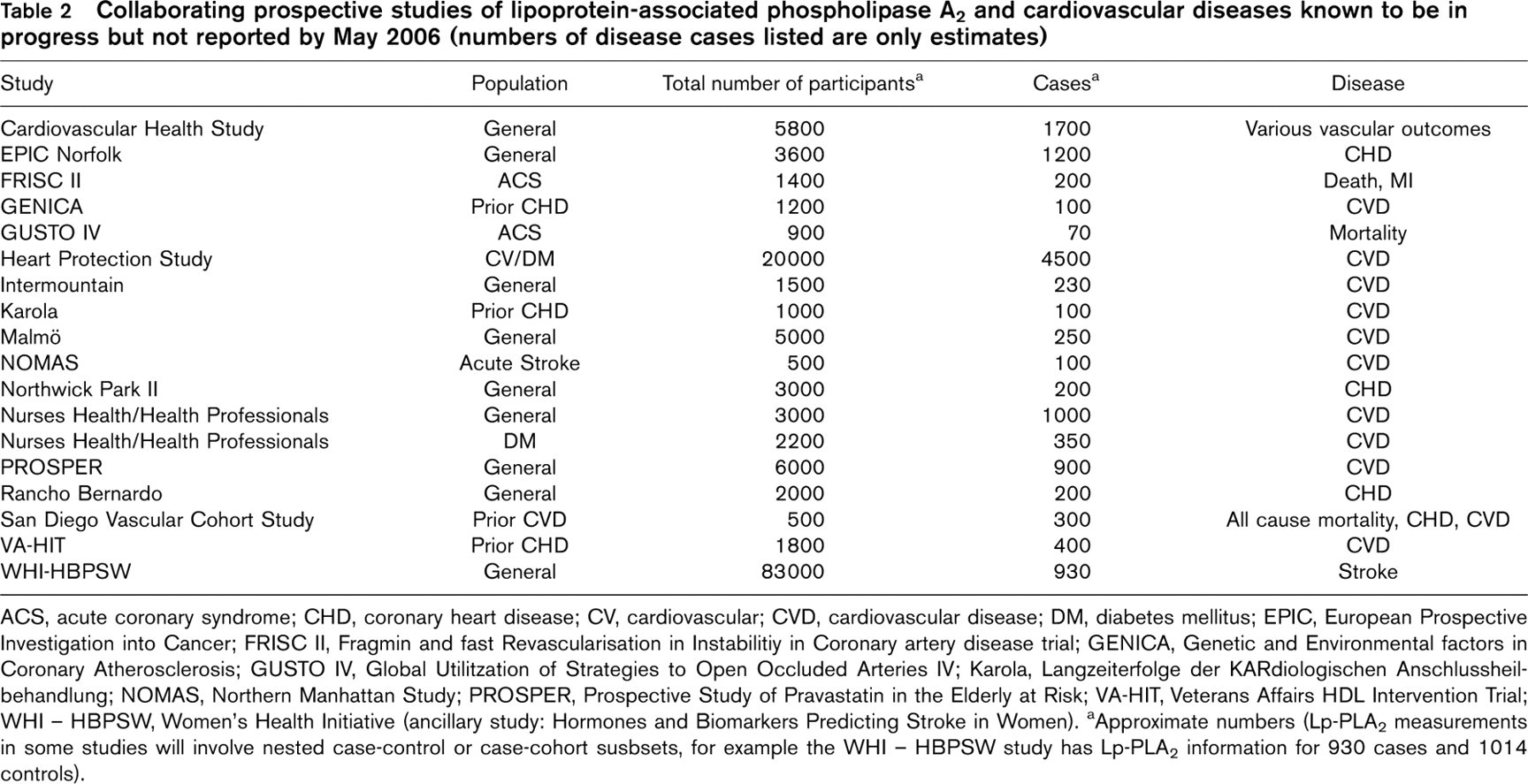
ACS, acute coronary syndrome; CHD, coronary heart disease; CV, cardiovascular; CVD, cardiovascular disease; DM, diabetes mellitus; EPIC, European Prospective Investigation into Cancer; FRISC II, Fragmin and fast Revascularisation in Instabilitiy in Coronary artery disease trial; GENICA, Genetic and Environmental factors in Coronary Atherosclerosis; GUSTO IV, Global Utilitzation of Strategies to Open Occluded Arteries IV; Karola, Langzeiterfolge der KARdiologischen Anschlussheilbehandlung; NOMAS, Northern Manhattan Study; PROSPER, Prospective Study of Pravastatin in the Elderly at Risk; VA-HIT, Veterans Affairs HDL Intervention Trial; WHI – HBPSW, Women's Health Initiative (ancillary study: Hormones and Biomarkers Predicting Stroke in Women). aApproximate numbers (Lp-PLA2 measurements in some studies will involve nested case-control or case-cohort susbsets, for example the WHI – HBPSW study has Lp-PLA2 information for 930 cases and 1014 controls).
Objectives of the Lp-PLA2 Studies Collaboration
By appropriate combination of data from individual participants from all relevant observational studies in a systematic meta-analysis, with correction for regression dilution, the Lp-PLA2 Studies Collaboration aims to characterize more reliably than has previously been possible the age and sex-specific relevance of Lp-PLA2 to CHD. This protocol prospectively defines the main objectives, and study identification, data collection and statistical methods to be used.
The primary objectives of the collaboration are to assess the age and sex-specific associations of Lp-PLA2 with CHD making appropriate allowances for regression dilution bias; to determine to what extent associations of Lp-PLA2 and CHD are independent of possible confounding factors; and to enable detailed exploration of potential sources of heterogeneity among studies, involving study-level characteristics (such as assay methods, features of study design, geographical location) and personal characteristics (such as age, sex, and levels of several established risk factors). Secondary objectives include initiation of investigations of Lp-PLA2 circulating markers with stroke and with other vascular conditions, and of Lp-PLA2 genotypes with cardiovascular disease outcomes [15–24]. It is anticipated that the present collaboration will serve as a framework for evidence emerging from studies on Lp-PLA2 and cardiovascular outcomes, not only for studies which are already published, but also for those known to be in progress and those yet to be identified (Tables 1 and 2).
Identification of relevant studies and collection of data
Selection criteria and identification of studies
Eligible prospective studies are those that have recorded baseline circulating Lp-PLA2 measurements in participants and subsequent cardiovascular disease outcomes. Studies listed in Tables 1 and 2 were identified through computer-assisted literature searches of databases, scanning of reference lists, hand-searching of relevant journals, and correspondence with authors of relevant reports. The list of eligible studies will continue to be updated until at least 2007.
Baseline covariates and characteristics to be studied
Data have been sought from investigators on Lp-PLA2 values recorded at the baseline survey and at any subsequent surveys during follow-up to allow for study-specific correction for regression dilution [13]. To investigate the relevance of possible confounding factors and effect modifiers, data have been sought (where available) from baseline on ethnicity; total cholesterol; high and low-density lipoprotein cholesterol; triglycerides; apolipoproteins A1 and B; systolic and diastolic blood pressure; acute phase reactants (e.g., C-reactive protein, fibrinogen, albumin, white cell count); haemostatic factors (e.g., von Willebrand factor, fibrin D-dimer); metabolic factors (eg, fasting glucose and insulin); history of coronary heart disease, stroke and diabetes; weight and height; waist and hip circumference; smoking; alcohol consumption; use of cardiovascular medications (including those allocated in randomized trials) and exogenous hormones; physical activity; and socio-economic status (Fig. 1). In addition, data from all subsequent examinations have been sought on Lp-PLA2 values, serum lipids, blood pressure, and other recorded biochemical factors. Collection of data on age at baseline and at the disease event (or at last follow-up) and sex will enable age and sex-specific analyses. Collection of information on the different assay methods and standards used in Lp-PLA2 measurement [25] and on features of study design (e.g., case-control versus prospective cohort studies) will enable exploration of any heterogeneity among study results. Categorical variables, such as alcohol consumption, physical activity and smoking, will be re-coded to maximize comparability among studies.
Outcomes to be studied
For each individual, data have been sought on any of the following outcomes and on their dates of occurrence: non-fatal myocardial infarction (MI); non-fatal stroke; cause-specific mortality (or at least fatal CHD and fatal stroke); and other cardiovascular outcomes. Precise details of the diagnostic criteria used for the definition of cases have been sought from each study (as have data on the completeness of follow-up in the prospective studies). Analyses will be based on events classified according to the International Classification of Diseases (or, where this is not available, on available study-specific classification systems).
Data transfer and checking
Data can be transferred from the individual studies to the coordinating centre using any machine-readable medium and in any format convenient to the collaborators. Risk factor and outcome data will be accepted in whatever format they were originally coded and stored by the study investigators. The data obtained from each participating study will be checked for consistency by the secretariat and any queries then referred back, in confidence, to the study collaborators. The data will then be converted to a standard format for incorporation into a central database to be used for collaborative analyses. The content of the data will be unchanged by this process, and computer-generated detailed summary tabulations based on the converted data will be returned to each collaborator for review and confirmation.
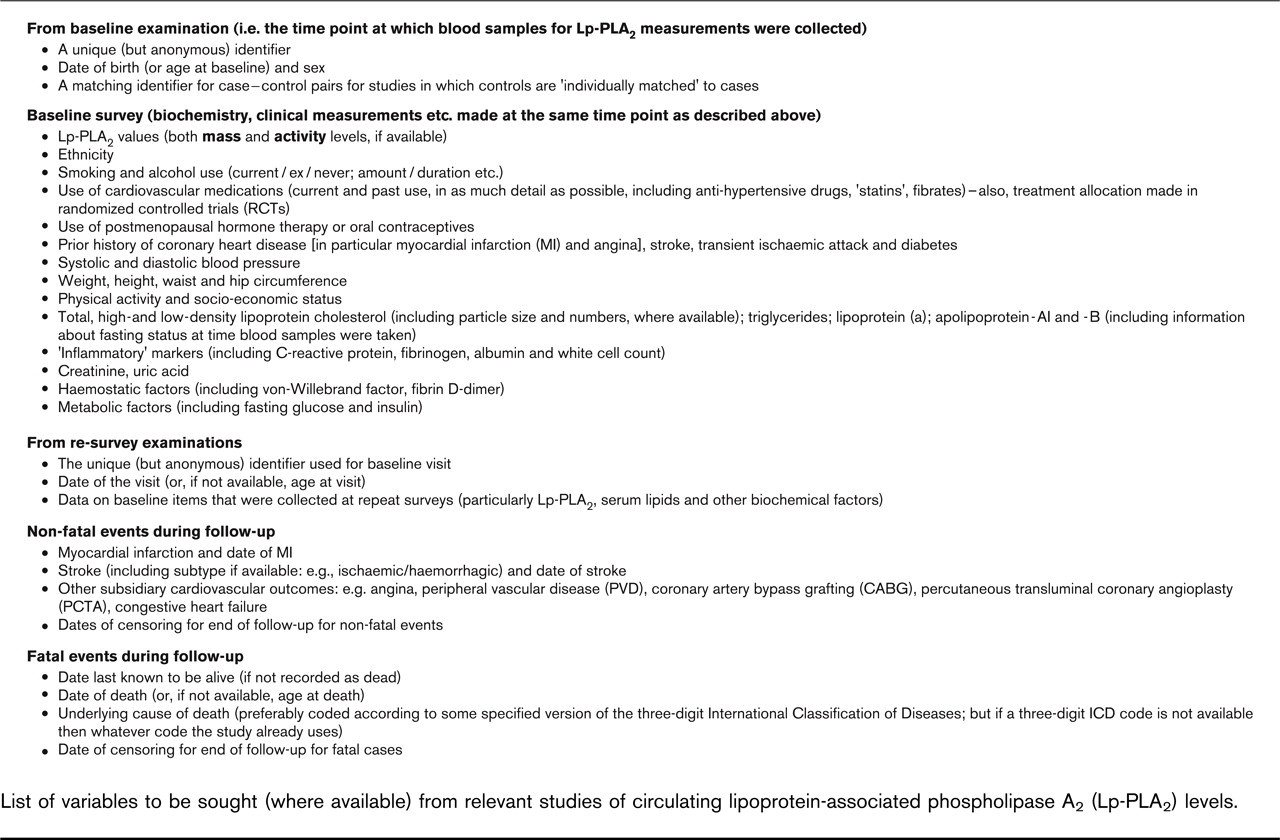
List of variables to be sought (where available) from relevant studies of circulating lipoprotein-associated phospholipase A2 (Lp-PLA2) levels.
Confidentiality of data provided
The data provided from each study will remain entirely the property of the principal investigators of that study, and will be held in confidence by the coordinating centre. Anonymous data on individual participants in each of the studies will be stored securely on the computer database at the coordinating centre.
Statistical analyses
Principal analyses
The main analyses will involve regression models stratified by study and sex (and, in randomized trials, by treatment allocation). Studies provided as prospective cohort studies will be analysed using Cox's proportional hazards model [26]. The principal outcome will be a combination of CHD death or first MI, with subsidiary investigation of other vascular outcomes such as stroke, congestive heart failure and recurrent non-fatal MI (consideration of such specific associations should enable an assessment of the overall impact of Lp-PLA2 on cardiovascular disease). Separate assessments will be made of associations between Lp-PLA2 markers and relevant outcomes in individuals with and without evidence of baseline cardiovascular disease (with attempts, where possible, to stratify analyses by extent and type of baseline cardiovascular disease: for example, those with stable CHD versus unstable CHD at the time of blood collection). Apparent heterogeneity between the results of different studies will be explored partly by fitting formal interaction terms in the regression models, and partly by grouping studies by various characteristics (such as by assay method, by sample size or by study design features) and then comparing the subtotals. The effect of adjustment for established risk factors (such as smoking and serum lipid concentrations) and other characteristics will be investigated. Analyses will be presented separately by sex and by age group (where the data are sufficient to sustain such subdivisions), and any effect modification by age, sex, duration of follow-up and established risk factors (in particular, low-density lipoprotein cholesterol concentrations) will be investigated by formal tests of interaction. Exploratory analyses will be conducted that restrict attention to cases who had outcomes several years after the baseline survey (for prospective cohort studies) and to participants without evidence of vascular disease at baseline (both of which should minimize any influence of pre-existing disease). As different studies have used different Lp-PLA2 assay methods (based on either mass or activity levels) and different assay technologies (with later studies using subsequent ‘generations’ of kits), this collaboration provides an opportunity to determine to what extent data from studies with such different characteristics can be pooled; previous collaborative meta-analyses have involved similar considerations [26].
Regression models will be used in two ways to describe any dose-response relationships. The first will involve the estimation of regression coefficients per unit increase in exposure (i.e., the risk ratio per nanomole per minute per millilitre in ‘usual’ plasma Lp-PLA2 activity or per nanogram per millilitre in ‘usual’ Lp-PLA2 mass levels). But such estimates will merely describe the steepness of the straight lines that best fit the data when risk is plotted on a logarithmic scale. A fuller description of the shape of the relationships will be obtained by plotting the risk ratios in groups defined by increasing baseline levels of Lp-PLA2 against the mean ‘usual’ levels of Lp-PLA2 (see below) [27]. Confidence intervals for each risk factor level will be estimated using ‘floating’ variances, which do not alter the estimates of the risk ratios but reduce the variance attributed to those that are not exactly unity (and should also greatly reduce the unwanted covariances between them) [28].
Adjustment for regression dilution
Analyses will be adjusted for the effects of regression dilution bias using previously described methods [13]. For analyses describing the steepness of the straight-line association between risk on a logarithmic scale and Lp-PLA2 values, an adjustment factor can be estimated from the relationship between baseline and follow-up Lp-PLA2 levels. For analyses describing the shape of the risk relationship, the adjustment will be performed by plotting risk ratios for groups subdivided by increasing baseline Lp-PLA2 values against the means of the repeat measurements made during follow-up in those groups. These provide an unbiased estimate of the ‘usual’ Lp-PLA2 during follow-up. Wherever possible, re-measurements from within each contributing study will be used, but where these data are not available correction factors will be estimated from available data in comparable studies. Previous reports have shown that, although the magnitude of the regression dilution bias for cholesterol and blood pressure did not depend strongly on age, sex or ethnicity, it did depend strongly on the duration of follow-up [13]. This will be investigated for Lp-PLA2 and, if appropriate, adjustments for regression dilution will depend on the average interval between Lp-PLA2 measurement and the event of interest. If possible, similar estimates will be used to adjust for within-person fluctuations of possible confounding factors.
Selected published studies of polymorphisms in the lipoprotein-associated phospholipase A2 gene (PLA2G7) and cardiovascular diseasesa
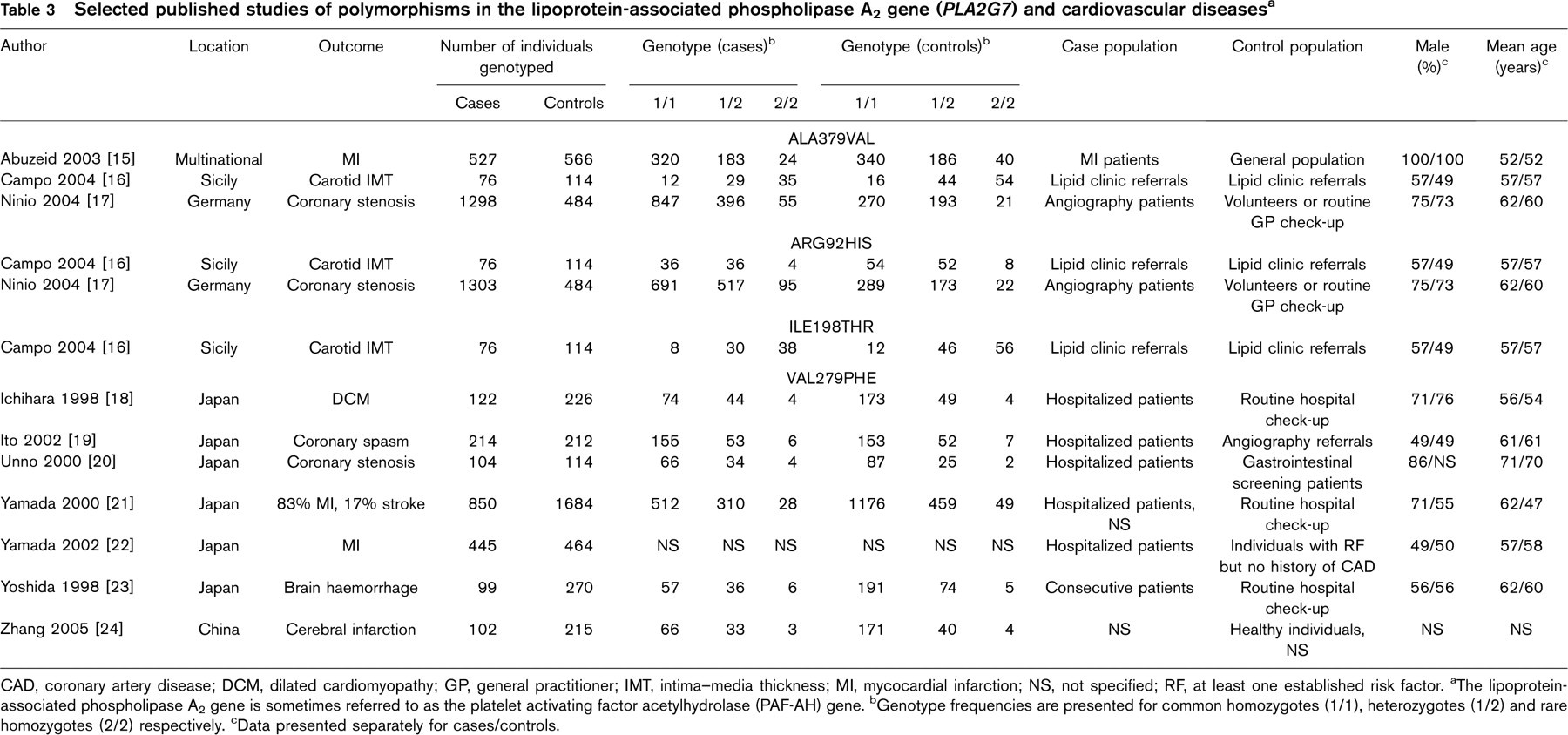
CAD, coronary artery disease; DCM, dilated cardiomyopathy; GP, general practitioner; IMT, intima-media thickness; MI, mycocardial infarction; NS, not specified; RF, at least one established risk factor. aThe lipoprotein-associated phospholipase A2 gene is sometimes referred to as the platelet activating factor acetylhydrolase (PAF-AH) gene. bGenotype frequencies are presented for common homozygotes (1/1), heterozygotes (1/2) and rare homozygotes (2/2) respectively. cData presented separately for cases/controls.
Genetic studies
Literature-based meta-analyses of genetic association studies (such as those listed in Table 3) [15–24], supplemented by tabular data from investigators, will be conducted to help quantify associations more reliably between relevant Lp-PLA2 gene variants, circulating Lp-PLA2 levels and disease risk. The results of such analyses will help to determine if pooling of individual data on these genetic factors will be prioritized in the present collaboration.
Study management and co-ordination
A steering group, comprising principal investigators of studies contributing individual data to the collaboration (with regular updates of the group's membership to encompass emerging studies), will meet at least once a year. Steering group members will provide input to an operations group (described below) and have opportunities to comment on draft analyses and texts prior to submission of manuscripts for publication, and will be authors of any reports including their data. Investigators will retain the right to withdraw their data from some or all of the meta-analyses at all times. An operations group – comprising representatives of the contributing principal investigators, coordinating centre, study funders, and other agreed members – will meet face-to-face about twice a year, with regular interim teleconferences. This group will provide oversight for the collaboration, particularly by establishing research priorities, setting and monitoring project milestones, and supervising the work of publications committees. An independent academic coordinating centre (jointly based in the Department of Public Health and Primary Care, University of Cambridge, and the Clinical Trial Service Unit and Epidemiological Studies Unit, University of Oxford) will be responsible for the collection, harmonization, maintenance and pooling of datasets provided by principal investigators, and for helping to lead analyses and interpretation of results. The coordinating centre will provide regular reports to the steering group and to the operations group. Only the coordinating centre will have direct access to the combined dataset.
Publication policy
This protocol has been circulated to collaborating investigators prior to submission for publication for comments and agreement, and, as described above, this procedure will be followed for all other manuscripts from this collaboration. As with this report, all subsequent reports from the collaboration will be published in the name of the Lp-PLA2 Studies Collaboration. The initial submission for publication of the main results is scheduled for 2007 and will be confined to analyses concerning the stated objectives. The timing of subsequent publications will be discussed with collaborating investigators to allow them time to publish their own analyses before any collaborative report emerges.
Conclusion
The Lp-PLA2 Studies Collaboration is a consortium of investigators of prospective studies of Lp-PLA2 and cardiovascular disease. By combining individual participant data from such studies, the proposed meta-analysis should help to determine more reliably than previously possible the strength of any independent association, the shape of any dose-response relationship with risk, the magnitude of associations in different circumstances (such as age-specific and sex-specific associations), and sources of heterogeneity between studies. Furthermore, data from repeated measurements of Lp-PLA2 and related factors taken some years apart will allow appropriate correction for regression dilution, leading to associations of disease risk with long-term ‘usual’ Lp-PLA2 levels after appropriate adjustment for potential confounding factors. The collaboration will include data from several studies involving a total of approximately 15 000 patients with major cardiovascular disease outcomes.