
Abstract
This consensus paper on behalf of the Study Group on Sports Cardiology of the European Society of Cardiology follows a previous one on guidelines for sports participation in competitive and recreational athletes with supraventricular arrhythmias and pacemakers. The question of imminent life-threatening arrhythmias is especially relevant when some form of ventricular rhythm disorder is documented, or when the patient is diagnosed to have inherited a pro-arrhythmogenic disorder. Frequent ventricular premature beats or nonsustained ventricular tachycardia may be a hallmark of underlying pathology and increased risk. Their finding should prompt a thorough cardiac evaluation, including both imaging modalities and electrophysiological techniques. This should allow distinguishing idiopathic rhythm disorders from underlying disease that carries a more ominous prognosis. Recommendations on sports participation in inherited arrhythmogenic conditions and asymptomatic gene carriers are also discussed: congenital and acquired long QT syndrome, short QT syndrome, Brugada syndrome, catecholaminergic polymorphic ventricular tachycardia, arrhythmogenic right ventricular cardiomyopathy and other familial electrical disease of unknown origin. If an implantable cardioverter defibrillator is indicated, it is no substitute for the guidelines relating to the underlying pathology. Moreover, some particular recommendations for patients/athletes with an implantable cardioverter defibrillator are to be observed.
Keywords
Introduction
The major final common pathway to sports-related sudden death comprises ventricular tachyarrhythmias. The prevalence of sport-related sudden cardiac death in athletes is 2.1/100 000 athletes per year [1]. Moreover, ventricular tachyarrhythmias may result in hemodynamic impairment with the risk of syncope or presyncope, which may compromise the safety of the athlete or other participants. Many cardiovascular conditions, like hypertension, ischemic and valvular heart disease, congenital malformations and dilated cardiomyopathy, may predispose to ventricular arrhythmias and form the focus of other articles in the series on recommendations for sports eligibility in this journal. The question of imminent life-threatening arrhythmias is especially present when some form of ventricular rhythm disorder is documented, or when the patient is diagnosed to have inherited a genetic disorder (channelopathy) that may predispose to ventricular arrhythmias. These topics form the subject of the current article, together with recommendations on sports participation of patients already treated with an implantable cardioverter defibrillator (ICD).
It is important to note that there is a scarcity of large-scale or prospective data on the safety of sports participation with the aforementioned conditions. In this respect, a panel of experts proposes in this paper a consensus on what they consider appropriate participation in competitive or recreational sports activity. Clinicians dealing with athletes or patients have to consider these recommendations as guidelines for individualized medical advice, not as rigid standards or protocols. Factors that have to be taken into account when tailoring recommendations are the type of sports (degree of static or dynamic work; low, moderate to high total cardiovascular demand; progressive demand or burst activity) [2, 3], patient motivation, ambient factors (temperature, humidity) and relevance of any incapacitating situation like dizziness or (pre)syncope (e.g. during sports like diving, driving, mountaineering). It is also important to realize that often there is no clear distinction between competitive and leisure-time activities, nor between competition and training (with the latter sometimes demanding more strenuous exercise than the competition itself). Patients often ask for quantitative limits of allowed activity (e.g. based on heart rate); there are, however, no data to support such quantitative advice, except in the individual case for which exercise testing has shown reproducible arrhythmia induction beyond a certain level and never below. The physician should also discuss with the patient that systematic or progressive training cannot cure or prevent exercise-related arrhythmias, contrary to the belief of many. In general, patients should even be advised not to pursue progressive training effects in endurance programs like running or biking (even during noncompetitive activity) since these may lead to an insidious increase in work load (with an increased risk for arrhythmia triggering) or a progression of the underlying disease process [e.g. arrhythmogenic right ventricular cardiomyopathy (ARVC), see below].
The recommendations mentioned in this paper extend the more condensed recommendations towards competitive sports from the Study Group on Sports Cardiology of the European Society of Cardiology [3] and are in line with the North-American recommendations for competitive athletes [4–6]. Since this text also addresses leisure-time activity, it may also apply to professional working environments demanding more than light physical activity. This text follows a prior document on supraventricular arrhythmias and pacemakers in this journal [7].
Documented arrhythmias
Cardiovascular evaluation, performed during regular follow-up or triggered by aspecific symptoms, may reveal ventricular arrhythmias on the 12-lead electrocardiogram (ECG), exercise ECG or long-term ECG recording (Holter, event recorder). Many of these documented arrhythmias may pass unnoticed as such by the patient/athlete.
Ventricular premature beats
Ventricular premature beats (VPBs) are common in the general and athletic population alike, being present in a majority of people [8]. It is still unclear whether their prevalence is higher in trained individuals [9–11]. In the majority they are fully asymptomatic [12]. The most frequent VPB morphology has a left bundle branch pattern and inferior axis, indicating origin in the right ventricular outflow tract, which is a recognized idiopathic and benign entity [13, 14]. Although prospective studies are lacking, it is considered that VPBs do not confer adverse prognosis when no underlying heart disease is present [15]. Cardiovascular abnormalities are, however, more commonly observed in athletes with frequent and complex VPBs (>2000/24h) (30 versus 1.8%; P<0.001) [15].
Assessment
Routine screening in all athletes consists of medical history, both personal (dyspnea or atypical chest sensations, dizziness, sudden fatigue, syncope, particularly during exercise) and familial (abrupt syncope or sudden death), physical examination and a 12-lead ECG [16]. It is important to realize that isolated VPB may be an indicator of underlying heart disease or that more complex (nonsustained or sustained) ventricular arrhythmias may also be present in the same athlete/patient. Therefore, a more thorough evaluation to rule out underlying heart disease is required. The optimal assessment strategy is not known but routine screening should in athletes with VPB on the 12-lead ECG at least be supplemented with echocardiography, exercise testing and 24-h Holter.
Frequent ectopy on Holter, an increase in the frequency of VPB with physical activity, as well as subjective palpitations or symptoms of hemodynamic impairment (even when vague and nonspecific) should all prompt for a more extensive cardiovascular evaluation to rule out underlying structural or electrical abnormalities. This evaluation should include both imaging modalities and electrophysiological assessment, for which some points of focus are described under the following section on Ventricular tachycardia.
Recommendations
Athletes with VPBs and underlying abnormalities should not participate in competitive sports, since even activities with low cardiovascular demand may be associated with important changes in autonomic tone, which could lead to malignant ventricular arrhythmias and sudden cardiac death. Only when cardiovascular abnormalities can effectively be excluded, when there are no frequent VPBs (< 2000/24 h) and no exercise-induced increase of VPB or VBP-related symptoms (without or with treatment), all competitive and leisure-time sports activity are allowed (Table 1). A yearly follow-up for re-evaluation is advised or earlier on the occurrence of symptoms, even when aspecific. In a majority of athletes with frequent VPBs, deconditioning for 3–6 months may result in a substantial decrease in the number of VPBs, which may confirm good prognosis [17]. Whether this is also true for athletes with proven underlying cardiovascular abnormalities, remains to be confirmed. It is recommended that athletes who after deconditioning remain symptomatic or keep having a clear increase in VPB frequency by exercise (even in the absence of underlying disease) should refrain from competitive sports and only participate in light to moderate leisure-time activity. A 6-monthly follow-up is warranted to exclude progression or the development of symptoms during recreational activity.
Nonsustained or sustained ventricular tachycardia
Documentation of more complex nonsustained ventricular arrhythmias (three or more consecutive beats at ≥ 120 bpm) or sustained ventricular tachycardia (VT) (≥ 30 s or requiring earlier cardioversion due to hemodynamic compromise) requires stringent evaluation to exclude underlying cardiovascular disease and to evaluate risk. Only slow idioventricular rhythms (< 100–150 bpm) in the absence of structural heart disease are benign and can be approached as outlined for VPB above.
Assessment
Evaluation should include imaging techniques like echocardiography (to rule out dilated, hypertrophic and right ventricular cardiomyopathy (ARVC), pulmonary hypertension or valve disease), nuclear scintigraphy and coronary angiography (to rule out coronary abnormalities [18] or premature atherosclerosis) and cardiac magnetic resonance imaging (to rule out ARVC). Imaging, however, may not be able to rule out unequivocally mild right ventricular (RV) structural changes, which could however confer an ominous prognosis in some cases [19] nor underlying inherited arrhythmogenic conditions [that are described under the section titled ‘Inherited arrhythmogenic conditions (channelopathies)’].
Therefore, careful assessment of electrophysiological data is warranted. It will help to categorize the cause, anatomic origin and mechanism of the ventricular arrhythmia.
Repolarization abnormalities are very commonly observed on a 12-lead baseline ECG in a young and athletic population [20]. Their presence therefore is often nonspecific [21, 22]. Negative T-waves in the right precordial leads, however, may herald underlying ARVC [19, 23, 24] and deep negative T-waves in the left precordial leads must raise suspicion of pathologic left ventricular hypertrophy [25]. Hence, when these repolarization abnormalities are seen, a more thorough cardiovascular examination to exclude these pathological entities is warranted.
Late activation of the RV may lead to slightly wider QRS-complexes in V1 or V2, sometimes with a characteristic epsilon-wave appearance or a prolonged S-wave upstroke in V1 to V3 (≥ 55 ms) [26]. These findings may point to ARVC [23].
There should be attempts to document a 12-lead ECG of the ventricular arrhythmias: a left bundle branch morphology with negative QRS-complexes in V1, electrical transition between V2–V3 or V3–V4, a QS-complex in aVL and dominant inferiorly directed QRS-complexes is pathognomonic for origin in the RV outflow tract (RVOT) [13, 14]. It is a very common form of idiopathic VT, often described as ‘repetitive monomorphic VT’. Similar morphology but with earlier precordial transition may indicate origin in the LVOT. These arrhythmias are not usually associated with heart disease, in which case they have a benign prognosis. A rare clinical entity is VT with a right bundle branch morphology and left axis (rarely right axis). If structural or arrhythmogenic heart disease is ruled out, it is pathognomonic for origin in the left posterior (or rarely anterior) hemibundle (‘fascicular VT’, ‘Belhassen VT’) [27, 28]. It carries no adverse prognosis unless associated with (pre)syncope during exercise. Polymorphic VT or VT with alternating complexes (‘bi-directional VT’), especially when induced during exercise, carries a high risk of sudden death. This ECG manifestation may point to an inherited disorder (catecholaminergic polymorphic VT; CPVT), which is described under the section ‘Brugada syndrome’ below.
Some authors have suggested that in the absence of epsilon-waves on the surface-ECG, late potentials recorded on a signal-averaged ECG may be a sign of delayed (right) ventricular activation and of a proarrhythmogenic substrate [29]. Late potentials may be a subtle but definite criterion for ARVC [23].
Recommendations for participation in competitive sports and leisure-time physical activity of patients with ventricular arrhythmias, potentially arrhythmogenic conditions and implantable defibrillators
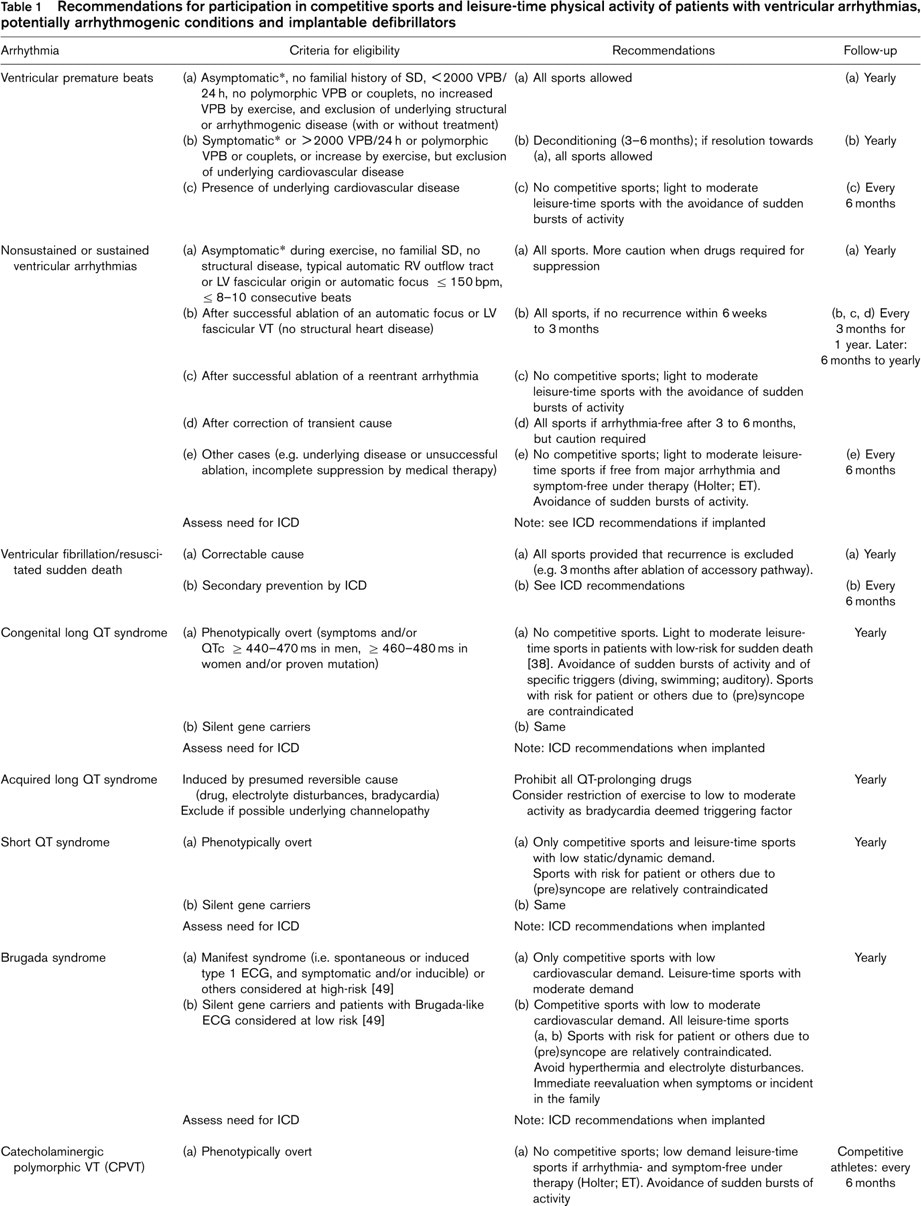
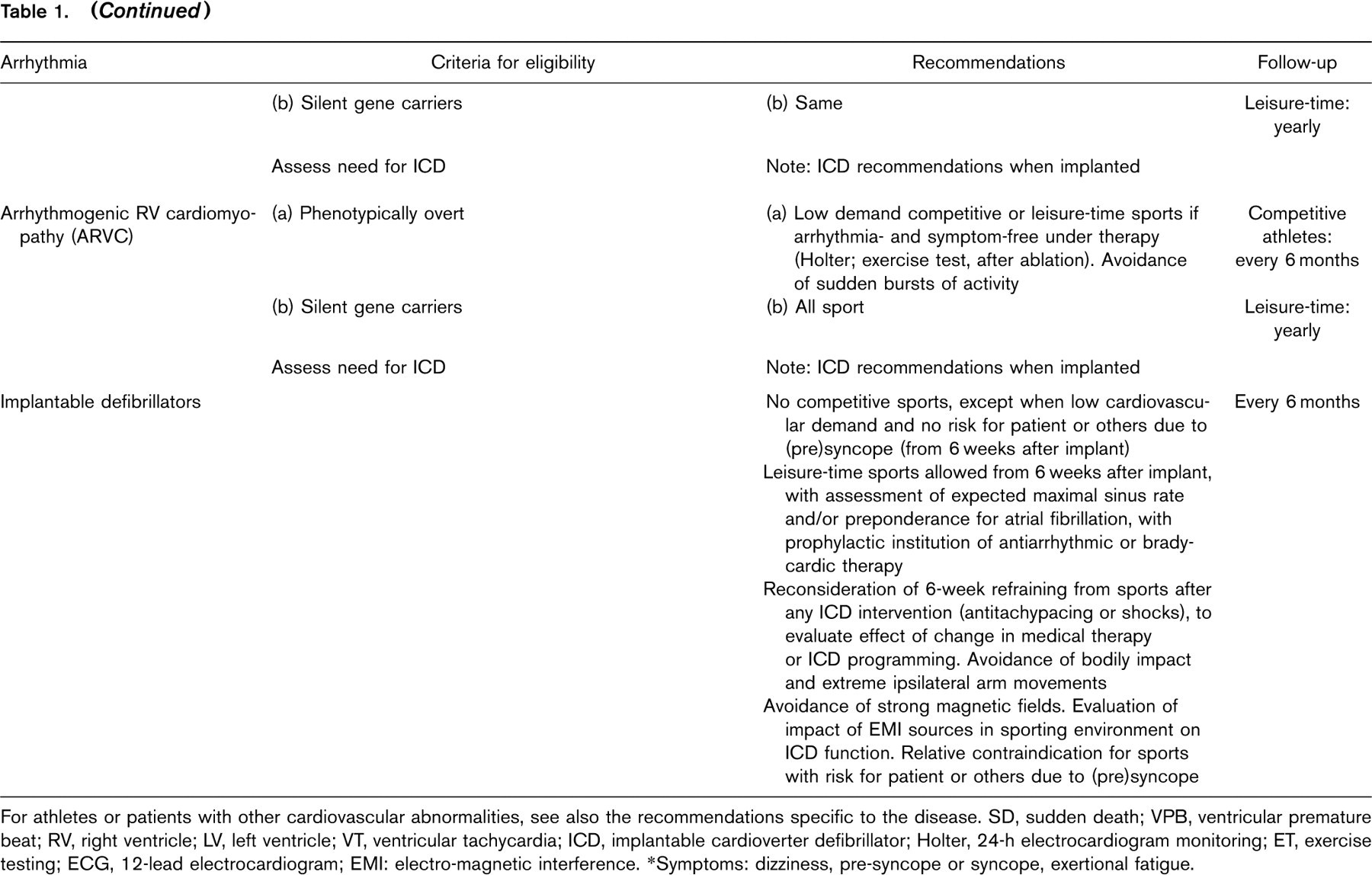
For athletes or patients with other cardiovascular abnormalities, see also the recommendations specific to the disease. SD, sudden death; VPB, ventricular premature beat; RV, right ventricle; LV, left ventricle; VT, ventricular tachycardia; ICD, implantable cardioverter defibrillator; Holter, 24-h electrocardiogram monitoring; ET, exercise testing; ECG, 12-lead electrocardiogram; EMI: electro-magnetic interference.
∗Symptoms: dizziness, pre-syncope or syncope, exertional fatigue.
Holter recordings have to be performed during periods of intense physical activity and preferably whenever the athlete is performing her or his specific sport activity. The recordings may show abundant unifocal ectopy (even with couplets, triplets or runs), which may point to automaticity as the underlying arrhythmia mechanism, as seen in typical idiopathic RVOT-VT.
Exercise testing with sport-specific and special protocols may result in the induction of arrhythmias. Polymorphic ventricular tachycardia during exercise always carries a bad prognosis, since it may point to an underlying inherited electrophysiological disorder (see section titled ‘Inherited arrhythmogenic conditions (channelopathies)’) or to underlying structural disease (like ARVC or hypertrophic cardiomyopathy, which may phenotypically not be evident from imaging examinations). Repetitive monomorphic bouts of VPBs, especially with the typical LBBB-type ECG pattern as described above indicating an RVOT-origin, reveal an automatic focus as the underlying cause of arrhythmia. Often, these arrhythmias increase in frequency at the beginning of exercise, disappear at peak-exercise and re-appear during recovery.
Finally, an invasive electrophysiological study may be warranted in selected patients to evaluate the inducibility of sustained arrhythmias, to differentiate supraventricular tachycardia with aberrant conduction, and to assess the arrhythmia mechanism (automaticity or reentry). There are many theoretical data and some cohort evidence that reentry arrhythmias confer a more ominous prognosis since they occur in structurally altered myocardium with the potential for development of more life-threatening arrhythmias, whereas automatic and unifocal arrhythmias may be idiopathic and are usually benign [19]. Spontaneous VT with rates below 100–150 bpm are generally also focal in nature and carry a good prognosis in the absence of underlying heart disease.
The difficulty of drawing a line, however, between ‘idiopathic’ and ‘no underlying structural heart disease’ is exemplified by the fact that a more careful morphological evaluation of non-athletic patients with RVOT revealed, in rare cases, minor structural abnormalities indicative for ARVC [30]. This overlap is even more prominent in athletes who often have cardiac structural adaptations and electrophysiological changes (e.g. repolarization variants) [21, 22] as part of the athlete's heart secondary to training and competition. This overlap is also illustrated by the observation that some athletes with manifest signs of structural abnormalities may, however, present with clearly automatic foci (and even without inducible reentrant arrhythmias during electrophysiological study) [19].
Recommendations
Nonsustained or sustained ventricular arrhythmias disqualify for competitive sports except for the particular case when there is absence of any familial antecedents of sudden death, no indication of any underlying structural pathology, a typical presentation of idiopathic RVOT ectopy or fascicular VT (or another idiopathic form of automatic and slow VT ≤ 150 bpm) with nonsustained bouts of tachycardia (eight to ten or fewer beats), and no symptoms of hemodynamic compromise during exercise. When such patients require drug treatment for suppression, more caution should be used since the extreme conditions of competition can never fully be reproduced during noninvasive or invasive testing. Also in rare cases with a manifest transient cause (like myocarditis or electrolyte disturbances) and after complete resolution is confirmed (including absence of any inducible arrhythmias during exercise or electrophysiological study), resumption of competitive sports can only be considered after a 3–6-month period. It should be noted in this regard that there are indications that these patients may remain at higher risk for sudden death, even after resolution of the transient cause (especially when it is ischemic in origin) [31]. Prospective studies should be awaited to confirm this, but caution and close follow-up of these athletic patients is advisable in case they want to resume competitive sports.
In some athletes implantation of an automatic implantable defibrillator may be warranted, especially when electrophysiological testing has shown inducibility of life-threatening ventricular arrhythmias in the presence of underlying structural heart disease. Recommendations for such patients are spelled out below. Competitive sports are not allowed except those with a low cardiovascular demand (like golf, billiards or bowling) [2, 3]. Therefore, the ICD is no substitute for prohibition from performing competitive or high-intensity leisure-time sports.
Idiopathic ventricular arrhythmias (as from RVOT-origin or fascicular VT) and some other automatic VTs are amenable to radiofrequency catheter ablation, with a reasonable ablation success. The procedures, however, carry a small risk of perforation, thrombo-embolic complications or aortic valve damage, which should be discussed with the athlete. Noninducibility during electrophysiological testing may preclude ablation, although newer mapping techniques may be able to localize the ablation target in some of these patients [32–34]. After successful ablation and absence of any recurrent symptoms during a 6-week to 3-month period, resumption of competitive or leisure-time athletic activity can be permitted in patients without underlying structural disease. Close early follow-up is warranted, however, (every 3 months for the first year, and immediately after recurrence of symptoms) and also later (at least yearly), since some may have underlying slowly progressive cardiac disease which will only manifest itself over time. There are no data to indicate that resumption of athletic activity after successful ablation of reentrant ventricular arrhythmias is safe, since the underlying substrate likely is still present. It seems to be advisable that only light-to-moderate recreational sports [2, 3] are allowed (with close follow-up as mentioned above) but competitive sports are prohibited.
In all other patients with documented ventricular arrhythmias, only light-to-moderate leisure-time activity can be allowed, provided that there is proven arrhythmic control with installed therapy, both based on exercise-ECG and long-term ECG recordings (preferably during these sports activities) and that the patients have no symptoms of hemodynamic compromise. Supervised activity as in rehabilitation programs may provide added assurance for these patients [35]. Burst physical activity and sports in extreme circumstances (like skiing in unusual circumstances or high altitude) should be avoided given the unpredictable autonomic or electrolyte changes they may provoke.
Ventricular fibrillation/resuscitated sudden death
Unless a clearly identifiable reversible condition can be defined and treated (like atrial fibrillation with rapid conduction over an accessory pathway which is subsequently ablated), many of these athletes will require implantation of an ICD. Recommendations for such patients are spelled out below. In others without definitive guarantee that the resolved transient cause will never recur, competitive sports are contraindicated in any case, given the concern that these patients may remain at higher risk for sudden death, as outlined above [31].
Inherited arrhythmogenic conditions (channel-opathies)
A number of familial arrhythmogenic conditions have been characterized over recent decades and in the near future this number will grow. They have in common that they are associated with life-threatening arrhythmias in young adults, even during recreational sports activities and at rest or during night-time [5, 36, 37]. They are mainly due to mutations in transmembrane ion channels or proteins involved in intracellular calcium handling.
Congenital long QT syndrome
Congenital long QT syndrome (LQTS; i.e. a prolonged corrected QTc interval according to Bazett's formula) is due to mutations in channels involved in the maintenance of the cardiac action potential plateau and repolarization. It generally is defined by a QTc of 440 ms or longer in men and 460 ms or longer in women, but some have suggested values up to and above 470 ms in male and 480 ms in female athletes to account for the longer QTc values in athletes [6]. Scoring systems have been proposed that illustrate the difficulty of defining an optimal cut-off QTc value by taking other ECG and clinical factors into consideration for diagnosis [38, 39]. QT-prolongation predisposes to Torsade de Pointes polymorphic VT and ventricular fibrillation.
Seven subtypes have been described depending on the protein involved: pore-forming or regulatory subunits of sarcolemmal ion channels [40, 41]. Congenital long QT syndrome should be distinguished from acquired forms, due to circumstances which can be reversed and prevented (see below). In case of a borderline long QTc interval and a negative personal plus familial history, arrhythmias should further be excluded by exercise testing and long-term ECG recording. Infusion of low doses of epinephrine may reveal a paradoxical increase of the QT interval, which is strongly indicative of LQT1 syndrome [42]. Modern mutational analysis can reveal mutations in 70% of the index patients by analysis of the five main genes involved. It remains, however, time-intensive and expensive, and therefore is generally reserved to research-oriented large referral centers. The availability of commercial test kits may change this in the future. It is important to realize, however, that in 30% of cases, no definitive diagnosis can be made by genotyping, stressing the importance of careful phenotypic evaluation.
Recommendations
Sympathetic stimulation is well-known to be proarrhythmogenic in patients with a congenital form. Therefore, competitive sports are not allowed in patients with definitive or strongly suspected LQTS. Even activities with low cardiovascular demand may be associated with important changes in autonomic tone, which could lead to malignant ventricular arrhythmias and sudden cardiac death. Such low-intensity sports could only be allowed in proven SCN5A mutation carriers, since they are mainly at risk for malignant arrhythmias at rest. No firm data exist concerning the exercise-related risk of silent mutation carriers: family members without overt phenotype but with a proven mutation. Given the fact that sudden death has been described in such carriers [38], it seems advisable for them to also refrain from competitive sports, especially when there is a family history of sudden death or a manifestly prolonged QTc interval [38]. Beta-blockers remain the mainstay therapy, but are no substitute for recommendations regarding sports participation.
Recommendations regarding leisure-time activity should weigh the benefits of physical activity (including psychological well-being and self-assurance) against the risks of sports participation. Considerations should include the risk for syncope or cardiac arrest due to LQTS [38]; increased risk if presyncope occurs during sports, activities like diving or driving, free weight-lifting, climbing and others are relatively contraindicated [2, 3]; avoidance of sports with a high cardiovascular demand or high adrenergic tone [2, 3]; and avoidance of potential triggering conditions.
This last advice may be more specific when the underlying genotype is known: LQT1 patients (KCNQ1 mutations) are susceptible for arrhythmia-development after sudden exposure to cold water (swimming, diving), while sudden unexpected auditory stimuli may trigger polymorphic VT in patients with the LQT2 subtype (i.e. HERG/KCNE2 mutations). In those without known underlying genotype, all restrictions should be considered.
In athletes who have experienced a previous out-of-hospital cardiac arrest or a LQTS-related syncopal episode, only exercise with low static and dynamic demand is allowed, regardless of QTc or underlying genotype.
For high-risk patients, the implantable cardioverter-defibrillator (ICD) offers an effective therapeutic option to reduce mortality. If implanted, specific recommendations apply (see below).
Acquired long QT syndrome
Acquired LQTS is more common than the congenital LQTS. The most frequent cause is use of QT-prolonging drugs, which block the delayed rectifier IKr current. Once a patient had drug-induced Torsade de Pointes, he or she is prone to develop further episodes of Torsade de Pointes when exposed to any other QT-prolonging drug [43]. There are several reports of gene mutations/polymorphisms in cardiac ion channels in drug-induced Torsade de Pointes, which indicate that they are in fact a latent form of congenital LQTS [44]. Other causes of acquired LQTS are organic cardiac diseases, profound bradycardia (due to sinus node disease or atrioventricular block) and noncardiac causes (like electrolyte disorders, dietary deficiencies, anorexia nervosa, hypothyroidism, metabolic abnormalities and diabetes mellitus). Athletes are prone to metabolic disturbances (electrolyte changes, fluid depletion) and conduction defects (physiologic at rest).
Recommendations
Once acquired LQTS is established all QT-prolonging drugs are prohibited and triggering factors should be avoided. This may include restriction of activity to low to moderate dynamic–static sports, and those in which there is additional risk in case of syncope. In recurrent Torsade de Pointes, implantation of an ICD should be considered.
Short-QT syndrome
Recently, a new familial repolarization abnormality has been identified due to increased potassium conductance related to mutations in at least three possible potassium channels [45, 46]. The resulting short-QT interval (defined as a QTc < 300–325 ms) may predispose to atrial fibrillation and malignant ventricular arrhythmias. Data are still limited, but adrenergic stress has been linked with the development of life-threatening arrhythmias [47].
Recommendations
Competitive sports are not allowed except for those with low static or dynamic demand [2, 3]. Until more clinical data become available, restraint should be used to even allow moderate leisure-time activity, certainly avoiding sudden bursts of activity. As with the long-QT syndrome, short-lasting arrhythmic episodes may result in (pre)-syncope: therefore, sports activity in which dizziness leads to increased risk of the patient or others are relatively contraindicated. In many affected individuals, an ICD will be recommended until more specific therapy may become available.
Brugada syndrome
The Brugada syndrome is defined by characteristic J-point and ST-segment elevations in the right precordial leads. Three different types of repolarization abnormalities have been described, of which only the most prominent form (type 1) is diagnostic [48]. In others, provocation by class-1 antiarrhythmic drugs may unmask a diagnostic type 1 ECG. Also a febrile state, electrolyte disturbances and autonomic changes may increase the ECG manifestation and even trigger ventricular arrhythmias [49]. Differentiating right precordial early repolarization (which may be present in about 4% of athletes) from Brugada syndrome can be difficult, but downsloping of the ST-segment and a slightly prolonged QRS-duration (i.e. > 100 ms) are indicators for the Brugada ECG [50]. In about 20% of patients, the origin of the syndrome can be linked to a mutation in the SCN5A protein, which is the α-subunit of the cardiac sodium channel. Although also in those without positive genotyping cellular sodium current abnormalities are suspected, no molecular cause has been defined. The sodium current defect explains why some of these patients and families have mixed phenotypic expressions ranging from repolarization abnormalities to isolated cardiac conduction defects. Although sudden death typically occurs at rest [51], the conduction defects explain why some may develop ventricular arrhythmias during exercise [52]. Moreover, increased vagal tone as a consequence of chronic athletic conditioning may also enhance the propensity to die at rest, and hyperthermia during exercise can be a trigger during strenuous activity [50].
Recommendations
Patients with a Brugada syndrome (i.e. with a distinctive spontaneous or induced type 1 ECG, symptoms of cardiac arrest or syncope, or inducibility at electrophysiological study) most often will receive an ICD and should be restricted from all competitive sports except those with low cardiovascular demand [2, 3]. Also in others, primary or secondary ICD implantation may be proposed based on a combination of personal or familial history of sudden death or unexplained syncope, the presence of a spontaneous type 1 ECG, male sex, or inducible ventricular arrhythmias during electrophysiological study [49]. In these, the recommendations for ICD recipients apply (see below).
When in patients with a Brugada-like ECG the risk for malignant ventricular arrhythmias and sudden death is judged to be low based on such a combined evaluation [49], all noncompetitive sports activity can be allowed. Patients should, however, be convinced that re-evaluation is urgently needed in case of symptoms of hemodynamic impairment (even when aspecific). It is also advisable that family data are centralized in referral genetic centers, so that any familial event can be communicated to all patients/physicians concerned and appropriate adjustments to recommendations can easily be disseminated to all family members at risk. Finally, it is unclear at present which recommendations should be made for phenotypically negative family members that have been identified as carriers (by class-1 antiarrhythmic drug provocation or genotyping). It seems prudent to restrict them too from competitive sports but to allow all leisure-time activities with close follow-up.
Catecholaminergic polymorphic ventricular tachycardia
Mutations in the ryanodine receptor (RyR2; the calcium release channel of the sarcoplasmic reticulum), calsequestrin (CASQ2; another protein involved in intracellular calcium handling) or the structural protein ankyrin-B (also referred to as LQT4-syndrome) have been defined as the underlying molecular mechanism of arrhythmias typically provoked by exercise or stress [53]. The ECG in baseline is undiagnostic, but exercise ECG shows multifocal VPB or VT with alternating QRS-axis, dubbed as ‘bi-directional VT’. They may degenerate into polymorphic VT or ventricular fibrillation. This inherited form of adrenergically-dependent arrhythmias is highly lethal, typically before age 20–30 years. This clinical entity may comprise 5–10% of patients with familial arrhythmias but without QTc prolongation or Brugada-type ECG abnormalities [54].
Recommendations
Competitive and even moderate leisure-time sports are formally contraindicated. Beta-blockers form the therapy of first choice but are not always effective and pose an extra risk when intake is forgotten. Therefore, in many patients an ICD will be advised. When electrocardiographic (stress test) follow-up under treatment shows absence of recurrence, low to moderate leisure-time sports can be performed, with immediate re-evaluation if symptoms recur. In the presence of an ICD, the ICD-related recommendations apply.
Arrhythmogenic right ventricular cardiomyopathy
There is a heterogeneous assortment of conditions that have in common that structural right ventricular fibrofatty replacement of the myocardium leads to arrhythmias, especially during adrenergic stress and exercise. As a group they are called ARVC. A diagnostic framework has been described for diagnosis of the syndrome, based on major and minor criteria including electrocardiographic, arrhythmic, noninvasive imaging, histopathologic, and genetic factors [23]. Different causes have been described, from mutations to inflammatory conditions [55, 56]. Also intense endurance athletic activity has recently been suggested as a factor that may contribute to ARVC development, given the higher relative work-load for the RV during these activities [19]. In some families, mutations in the ryanodine-receptor gene have been detected, indicating that there may be overlap forms between ARVC and catecholaminergic VT [57].
Recommendations
Given its predisposition to ventricular arrhythmias and the recognition of ARVC as a cause for sports-related sudden death [58–60] its diagnosis precludes participation in any competitive sports, with a possible exception for sports with a low static and dynamic demand [2, 16]. The same may apply to asymptomatic gene carriers in families in which a mutation has been detected. Leisure-time activities with a moderate to high cardiovascular demand are also contraindicated [2, 3], but activities with low demand are allowed when electrocardiographic evaluation under treatment has shown absence of arrhythmias and when there are no exercise-related symptoms. The need for ICD should be evaluated based on clinical presentation, electrophysiological findings and family history, with accordant recommendations when implanted.
Familial electrical disease of unknown origin
In some families an inherited pattern of clinical events (unexplained abrupt (pre)syncope, sudden death, documented arrhythmias) can be present but without demonstrable structural heart disease nor electrocardiographic indications for any of the above-mentioned conditions. Genotyping may over time lead to the discovery of mutations in other ion channels or regulatory proteins. One recently recognized phenotypic pattern is that of prominent U-waves, which may be the origin of VPB and malignant ventricular arrhythmias. Recently, the electrocardiographic characteristics of mutations in KCNJ2, coding the inwardly rectifying background IK1 current have been recognized in this respect; although considered before as a form of long QT syndrome (LQT7), there have been suggestions to categorize this entity as a different disease (Andersen–Tawil syndrome, ATS1) given its prominent U-waves and noncardiac symptoms [61]. It is likely that the future will reveal more familial genetically determined arrhythmogenic disorders, of which some can create particular vulnerability during exercise.
Recommendations
Recommendations for these familial electrical diseases are similar to those for the channelopathies described above. Moreover, in the absence of specific therapy, the need for ICD implantation should be evaluated in each family.
Implantable cardioverter defibrillator
As mentioned throughout the previous chapters, secondary or primary prevention by implantation of an ICD will often be considered in patients with documented ventricular arrhythmias or channelopathies. Advanced screening techniques and molecular diagnosis in family members is contributing to a rapid increase of this population. The recommendations concerning the underlying pathological conditions have been outlined above and generally include the advice to abstain from competitive sports. Although very effective to prevent sudden death, ICD implantation should not be regarded as a substitute for such a recommendation [62]. The efficacy of the ICD to interrupt malignant ventricular arrhythmias during intense exercise is unknown and from theoretical considerations probably suboptimal (given the associated metabolic, autonomic and potentially ischemic conditions). Specific data on the benefits and risks of ICD in physically active patients are lacking, explaining a large variability in current recommendations made by physicians to their patients [63].
Recommendations
An ICD disqualifies an athlete for competitive sports, except those with a low cardiovascular demand (like golf, billiards or bowling) [2, 3]. On the other hand, physicians and patients alike may feel more assured to continue leisure-time physical activities with low to moderate dynamic or static demand if an ICD is on board, which may contribute to physical and psychological well-being [35]. In patients with arrhythmias that are particularly sensitive to triggering by exercise, these recommendations should be made with caution.
Leisure-time sports resumption is allowed from 6 weeks after implant, preferably after a control stress test. When appropriate or inappropriate ICD interventions occur (antitachypacing or shocks), a 6-week period refraining from sports should be reconsidered to evaluate the effect of changes in medical therapy or ICD programming.
Some particular recommendations need to be made:
Sports participation with bodily contact is contra-indicated given the risk for trauma to the subcutaneously implanted device and its connection with the lead system.
Given the fact that there is a latency between arrhythmia onset and ICD intervention to terminate it (which may be antitachycardia pacing or shocks), sports activities during which dizziness or (pre)syncope would expose the patient or others to additional risks are relatively contraindicated.
Extreme ipsilateral arm-movements (like during volleyball, basketball, tennis, racket sports, handball, swimming, gymnastics, ballet) may increase the risk for lead dislocation or lead fracture (due to crush between clavicle and first rib), and therefore should be avoided, certainly during the first 6 weeks after implant.
Electromagnetic interference with ICD function is extremely rare. The patient should, however, be instructed about this potentiality if encountering any sports-related exposure to electromagnetic fields, and ICD follow-up should explicitly exclude inappropriate detection. Strong magnetic fields could temporarily (or in certain models permanently) inhibit tachyarrhythmia therapy, although no specific sports-related circumstances in which this has occurred have been described.
Exercise in young people may result in sinus tachycardia which exceeds the detection threshold for ICD intervention, leading to inappropriate therapy delivery. Inappropriate shocks are painful and may result in psychological problems like anxiety and unrest, which even may amount to aversion for the ICD protection. They also can trigger real life-threatening ventricular arrhythmias. It is therefore extremely important to tailor ICD settings and recommended exercise levels to the anticipated heart rate during sports activity for any individual patient. Prior exercise and long-term ECG recordings will be important for this assessment. When inappropriate device triggering due to sinus tachycardia is anticipated, clear instructions to the patient concerning activity limitation and/or institution of bradycardic therapy (with β-blockers if possible) are mandatory.
Many structural or arrhythmogenic conditions may also increase the risk for atrial arrhythmias (most commonly atrial fibrillation) with possible rapid atrioventricular conduction during exercise, again with the risk for inappropriate therapy delivery and thus the need for prophylactic antiarrhythmic or bradycardic drug therapy.
The implantation of a dual chamber ICD may be considered with the expectation that atrial electrogram information may increase the specificity of ventricular arrhythmia detection. Recent studies, however, have indicated that there is no significant difference in the incidence of inappropriate ICD therapy with DDD versus VVI-devices [64, 65]. Dual chamber differentiation becomes also irrelevant during high heart rates, as commonly seen for ICD indication in these patients who rarely present with slow VT. Moreover, given the fact that many of these patients will be young, there is a potential risk for increased long-term lead complications when more leads are implanted. Therefore, restraint needs to be advocated concerning the implantation of a more complex ICD system, and its indication should be weighed in every patient.