
Abstract
Background
Controversial information is available with reference to the role of type or yield of cigarettes on the risk of cardiovascular disease.
Design
We considered the issue in a combined dataset of three case-control studies of acute myocardial infarction conducted in Italy between 1983 and 2003.
Methods
Cases were 1990 subjects with a first episode of non-fatal acute myocardial infarction, and controls were 2521 patients in hospital for acute diseases unrelated to smoking or other recognized risk factors for myocardial infarction. The odds ratio and the corresponding 95% confidence interval (CI) were derived by unconditional multiple logistic regression models, including terms for age, sex, and several major risk factors for myocardial infarction.
Results
As compared to never smokers, the multivariate odds ratio was 2.70 (95% CI 2.01–3.63) for smokers of low tar cigarettes (<10 mg), 3.06 (95% CI 2.53–3.70) for intermediate (10–19 mg) and 3.14 (95% CI 2.12–4.64) for high tar yield (≥ 20 mg). After further allowance for duration of smoking and number of cigarettes per day, as compared to low tar yield cigarettes, the odds ratio was 1.14 (95% CI 0.85–1.53) for intermediate, and 1.28 (95% CI 0.81–2.02) for high tar yield.
Conclusion
Our study confirms that no substantial reduction in acute myocardial infarction risk resulted from the decrease of cigarette tar yield.
Introduction
There is a strong association between tobacco smoking and risk of cardiovascular disease, including acute myocardial infarction (AMI) [1–4]. Different types of smoking products (cigarettes, cigars, pipes) increase the risk of coronary heart disease (CHD) [5–8].
Contradictory information is available on tar yield of cigarettes and the risk of CHD [9–11]. The 13th Monograph on Smoking and Tobacco Control of the US National Cancer Institute (NCI) [9] reviewed the epidemiological studies conducted before 2001 and reported that there was no consensus on CHD risk in relation to use of filtered or low tar yield cigarettes. Among the 14 reviewed studies, one based on four cohorts from the UK, including a total of more than 56000 men and 2931 deaths from CHD [12], found a significant reduction in mortality from CHD with a decrease in tar yield of 15 mg [relative risk 0.77; 95% confidence interval (CI) 0.61–0.97]. The International Studies of Infarct Survival (ISIS), a case-control study from the UK including 14000 cases of AMI and 32000 controls [1], found an odds ratio (OR) of 1.10 (95% CI 1.00–1.22) for smokers of intermediate (≥ 10 mg) as compared to low (< 10 mg) tar cigarettes; Limiting the analyses to subjects with no previous disease, the OR declined to 1.06 (95% CI 0.91–1.22).
After the publication of the NCI Monograph, at least three studies analysed the issue. A case-control study [4], the data from which are part of a study included in the present re-analysis, conducted in northern Italy between 1995 and 1999 on 507 cases of AMI, found similar increased risks for low tar (OR, 2.3; 95% CI 1.5–3.4) and high tar cigarette smokers (OR, 2.0; 95% CI 1.2–3.5), as compared to never smokers. In a cohort from Scotland, including 3464 smokers followed for 13 years, of whom 209 died for cardiovascular disease [13], the RRs were 1.48 (95% CI 0.74–2.96) for smokers of low/intermediate (10–15 mg) and 1.35 (95% CI 0.79–2.60) for intermediate/high (≥15 mg) as compared to smokers of low tar yield cigarettes (< 10 mg). Conversely, a population-based case-control study, conducted between 1995 and 1997 in the USA on 587 cases of AMI in smokers [3], showed a significant increased risk for low (6–11 mg) as compared to very low tar yield (≤ 5 mg), the multivariate OR being 2.05 (95% CI 1.30–3.23). The risk of AMI, however, did not increase for subsequent tar levels, the ORs being 2.16 for low/intermediate (11–15 mg), 2.36 for intermediate/high (16–20 mg) and 2.42 for high tar yield (≥ 20 mg).
Tar yield of cigarettes has steadily decreased in western countries over the last few decades [9, 14, 15]. The average tar yield of Italian cigarettes was around 25 mg in the 1960s, around 17 mg in the early 1980s [16], declined to about 12 mg in the late 1990s, and since 1997 the sale of cigarettes with a tar yield of 12 mg or greater is forbidden [17].
To quantify the issue, we re-analysed data from three combined case-control studies on AMI conducted in northern Italy.
Methods
Data were derived from a combined dataset of three hospital-based case-control studies, conducted in the greater Milan area, northern Italy, on the risk of non-fatal AMI.
The first study was conducted in 1983–1992 and included 314 women with AMI and 733 female controls [18]; the second one was conducted in 1988–1989 within the Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto (GISSI)-2 study and included 916 cases and 1106 controls [11]; the third one was conducted in 1995–2003 and included 760 cases and 682 controls [19]. The present analysis includes therefore a total of 1990 cases of non-fatal AMI (1381 men and 609 women; median age 55 years, age range 18–79 years), and 2521 controls (1415 men and 1106 women; median age 53 years, age range 17–79 years) in hospital for acute diseases unrelated to smoking or other recognized risk factors for AMI. Cases admitted to the studies were patients with a first episode of non-fatal AMI with no history of other cardiovascular disease. Among controls, 35% had traumatic conditions, 19% non-traumatic orthopaedic disorders, 12% acute surgical conditions, and 34% miscellaneous other illnesses, such as ear, skin, and eye diseases. Participation was over 95% for both cases and controls.
All interviews were conducted in hospital by trained interviewers using structured questionnaires for the three studies. The three questionnaires included information on sociodemographic factors, anthropometric measures, alcohol and coffee drinking, a problem-oriented medical history and family history of AMI. Information on smoking was satisfactorily reproducible [20], and included the smoking status (never, former, or current), number of cigarettes smoked per day, and the duration of the habit. Ever smokers were subjects who had smoked at least one cigarette per day for at least 1 year and ex-smokers were defined as patients who had stopped smoking at least 1 year before the interview. A specific question considered the brand and type of cigarettes smoked by current smokers in the last 6 months before interview.
Tar yields of more than 100 types of cigarette, namely the most common Italian and international brands, were obtained from the Laboratory of the British Government Chemist [16] and from published sources by the Italian Government [17]. The cigarette brands were classified into three categories according to their tar yield: high tar (≥ 20 mg), including older, mostly unfiltered, cigarettes, intermediate tar (10–19 mg), and low tar (< 10 mg), including vented filter cigarettes.
A single file including only comparable variables codified in a uniform format was obtained from the three datasets. The multivariate OR and the corresponding 95% CIs were derived using unconditional multiple logistic regression models [21], including terms for age, sex, study, education, body mass index (BMI), alcohol and coffee consumption, serum cholesterol, history of diabetes and hypertension, and family history of AMI in first-degree relatives. When considering current smokers only, ORs were estimated after further allowance for number of cigarettes and duration of smoking.
Results
Table 1 shows the distribution of cases and controls according to study age, sex, education, BMI, alcohol drinking and family history of AMI in first-degree relatives. As compared to controls, cases were more educated, reported more frequently a first-degree relative with AMI, and had higher BMI.
Table 2 shows the distribution of cases and controls according to smoking habits. Compared to never smokers, the OR was 1.18 for former, and 2.9 for current smokers. Among current smokers the OR was 1.98 for smokers of fewer than 15 cigarettes per day, 3.08 for 15–24, and 6.10 for 25 or more cigarettes per day. The risk of AMI did not sensibly vary according to duration of smoking, the OR being 2.84 for under 30 years, 2.59 for 30–39 years, and 3.1 for 40 years or more of smoking, as compared to never smokers.
Distribution of 1990 cases with acute myocardial infarction (AMI) and 2521 controls according to selected covariates, Italy, 1983–2003
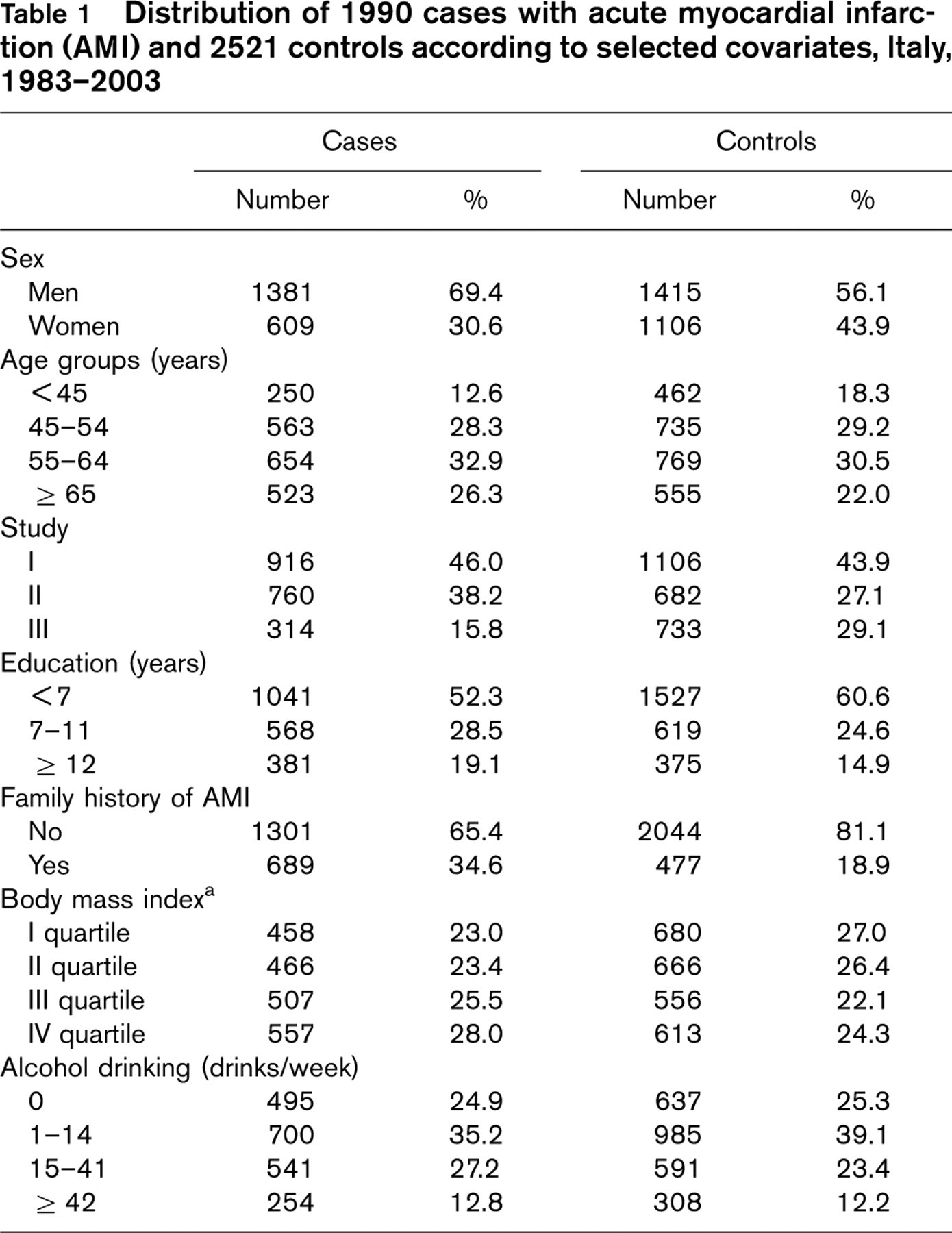
aThe sum does not add up to the total because of some missing values.
Table 3 shows the distribution of cases and controls (former smokers excluded) according to tar yield, overall and in strata of sex and age. Compared to never smokers, the OR was 2.70 (95% CI 2.01–3.63) for smokers of low tar cigarettes, 3.06 (95% CI 2.53–3.70) for intermediate and 3.14 (95% CI 2.12–4.64) for high tar yield cigarettes. No systematic pattern of risk was evident across strata of sex and age.
Table 4 considers current smokers only, and gives the ORs according to tar yield without and with allowance for number of cigarettes per day and duration of smoking. As compared to low tar yield (< 10 mg) cigarettes, the ORs were 1.12 (95% CI 0.84–1.49) for intermediate tar (10–19 mg), and 1.25 (95% CI 0.80–1.96) for high tar yield (≥ 20 mg). Corresponding estimates after further adjustment for number of cigarettes per day and duration of smoking were 1.14 (95% CI 0.85–1.53) and 1.28 (95% CI 0.81–2.02) for intermediate and high tar, respectively. No significant trend in risk was evident.
Distribution of 1990 cases with acute myocardial infarction and 2521 controls and corresponding odds ratios (OR) a with 95% confidence intervals (CI) according to number of cigarettes smoked and duration of smoking, Italy, 1983–2003
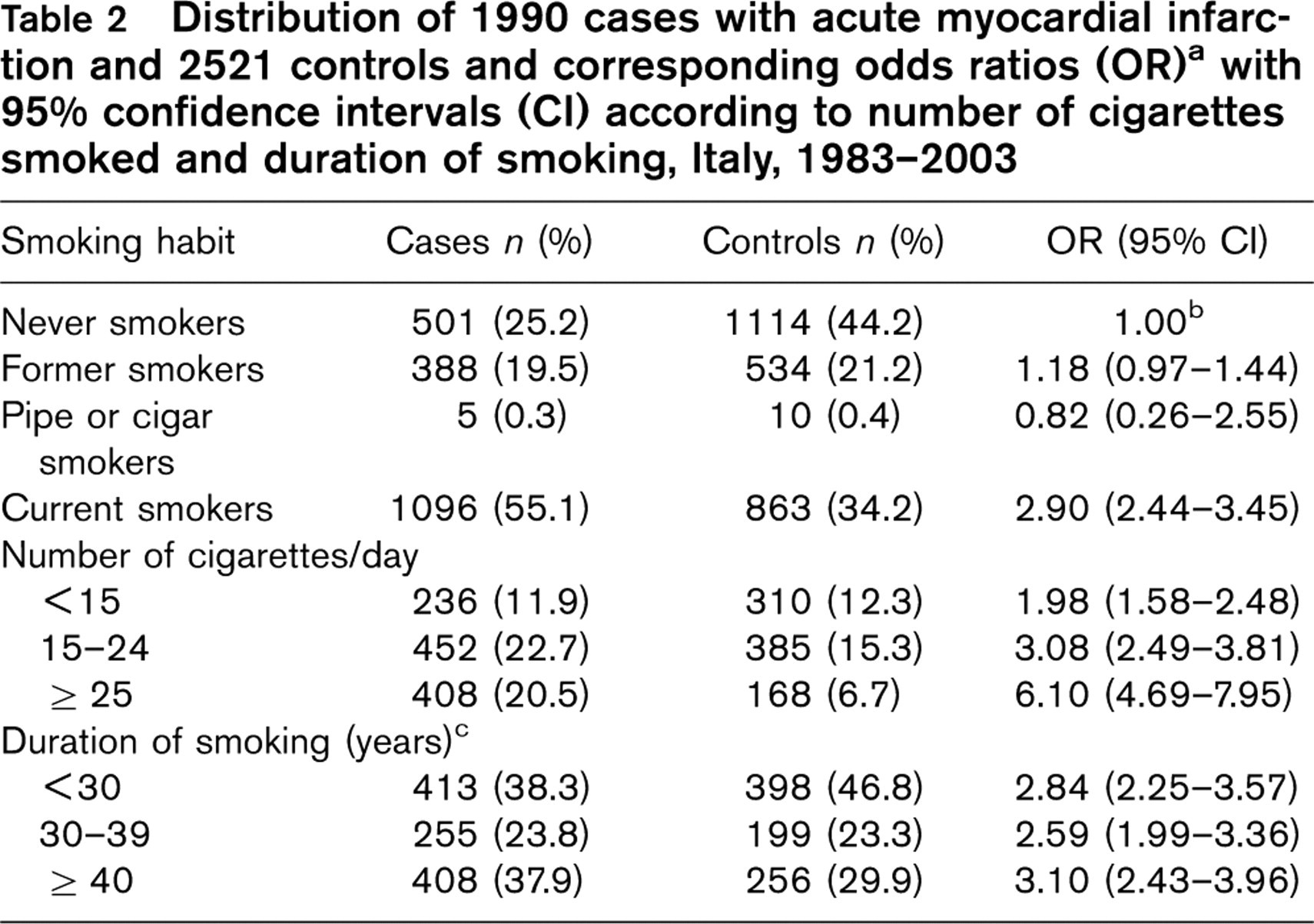
aEstimated by unconditional logistic regression models after allowance for age, sex, study, education, body mass index, alcohol and coffee consumption, cholesterol concentration, family history of acute myocardial infarction, history of diabetes and hypertension.
bReference category.
cThe sum does not add up to the total because of some missing values.
Discussion
Our study, considering data from three large Italian datasets, confirms that no significant reduction in AMI risk resulted from the decrease of cigarette tar yield [10], in agreement with several [4, 9, 11, 13], but not all [3, 12] studies.
Among the limitations of the study there is the lack of information on the very low yield cigarettes (i.e., tar ≤ 5 mg). However the real yield of very low tar cigarettes in vivo remains undefined, however, but is known to be much higher than in machine testing conditions [9].
The use of hospital controls to analyse smoking-related risks remains open to discussion. The prevalence of smoking in the comparison group, however, was comparable to that of the 1995 Italian National Multipurpose Survey [22]. Furthermore, cases and controls came from the same geographic area, the participation was almost complete, and we excluded from the control group any patients admitted to hospital for chronic conditions, particularly those associated with smoking or alcohol drinking, or diseases related to other known risk factors for AMI. Any possible residual selection bias, is unlikely to affect risk estimates for different levels of tar yield. The similar interview setting provides further reassurance against potential information bias, and information on cigarette smoking was satisfactorily reproducible [20]. Moreover, the main findings were consistent in the three studies. When limiting analyses to current smokers only, we had the possibility to control for intensity and duration of smoking [9]. Tar yield, in fact, may be associated with the number of cigarettes smoked, since smokers who switch from higher tar yield cigarettes to lower ones may compensate for reduced nicotine by smoking more cigarettes, taking larger puffs, inhaling more sharply, puffing more frequently, leaving a shorter butt, and blocking the filter holes to increase nicotine intake [9, 12, 17].
Distribution of 1597 cases with acute myocardial infarction and 1977 controls (former smokers excluded) and corresponding odds ratios (OR) a with 95% confidence intervals (CI) according to tar yield of cigarettes smoked in the last 6 months, in strata of sex and age, Italy, 1983–2003
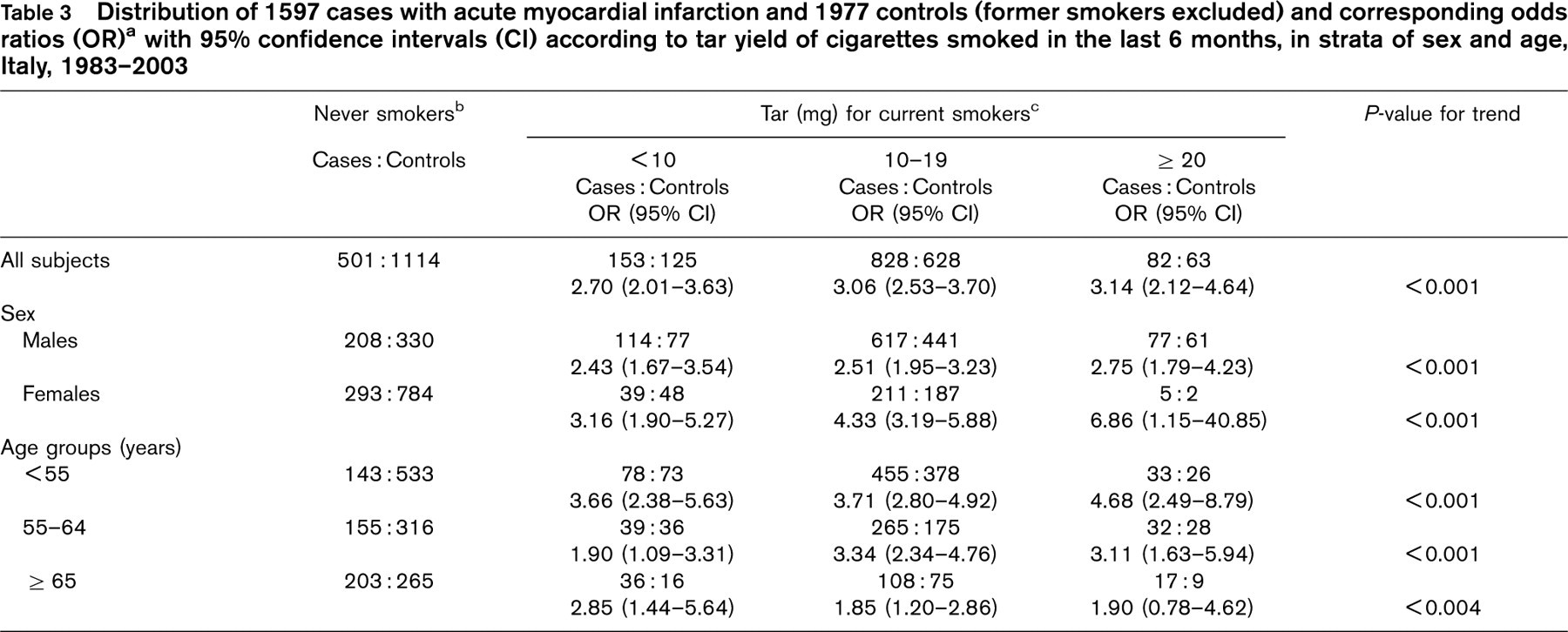
aEstimated by unconditional logistic regression models after allowance for age, sex, study, education, body mass index, alcohol and coffee consumption, cholesterol concentration, family history of acute myocardial infarction, history of diabetes and hypertension.
bReference category.
cThe sum does not add up to the total because of some missing values.
Distribution of 1096 current smokers with acute myocardial infarction (AMI) and 863 controls and corresponding odds ratios (OR) with 95% confidence intervals (CI) according to tar yield of cigarettes smoked in the last 6 months, Italy, 1983–2003

aEstimated by unconditional logistic regression models after allowance for age, sex, study, education, body mass index, alcohol and coffee consumption, cholesterol concentration, family history of acute myocardial infarction, history of diabetes and hypertension.
bAdjusted as above plus duration of smoking and number of cigarettes/day.
cThe sum does not add up to the total because of some missing values.
dReference category.
Since the risk of AMI is strongly influenced by recent smoking habit [23], we chose to consider the cigarette brand smoked during the last 6 months. This also probably reduced bias, since information on the distant past is often imprecise and influenced by current or more recent habits [24].
In conclusion, our findings confirm that low-tar cigarettes should not be considered a means of reducing AMI risk for smokers who cannot quit [10]. Given the favourable effects for other tobacco-related diseases, including lung and upper aero-digestive tract cancers [9, 13, 17], legislations to reduce tar levels have been adopted, but public health indications regarding tobacco control should be aimed unequivocally at promoting smoking cessation. The lack of association between tar yield of cigarettes and AMI risk has important public health implications, since tobacco companies misinformed smokers into believing that light, mild, ultra or low-tar cigarettes were safer than regular brands [9]. A recent study [25] showed how adolescents had the perception of being significantly less likely to get smoking-related diseases, including cardiovascular ones, when smoking light cigarettes, compared with regular cigarettes, for the rest of their lives. Use of light cigarettes has also been associated with lower smoking cessation [26], raising the concern that smokers may use light cigarettes as an alternative to quitting.
Footnotes
Acknowledgements
The authors thank Drs A Lualdi (Istituto di Cardiologia, Università degli Studi di Milano, Centro Cardiologico Monzino, IRCCS, Milan, Italy), A. Mafrici (Cardiology Dept. Niguarda Ca' Granda Hospital, Milan, Italy) and O. Parodi (CNR Clinical Physiology Institute, Milan, Italy) for their helpful contribution to the clinical conduction of the study, and Mrs I. Garimoldi for editorial assistance. The study was partially supported by the Italian League Against Cancer. Conflict of interest: none.