
Abstract

011 Type-D personality but not ICD indication is associated with impaired health-related quality of life 3 months post implantation
S.S. Pedersen1,2, D.A.M.J. Theuns2, A. Muskens-Heemskerk2, R.A.M. Erdman2,3, L. Jordaens2
1CoRPS-Department of Medical Psychology, Tilburg University, Tilburg, The Netherlands
2Department of Cardiology, Thoraxcentre, Erasmus Medical Centre, Rotterdam, The Netherlands
3Department of Medical Psychology and Psychotherapy, Erasmus Medical Centre, Rotterdam, The Netherlands
Objectives Indications for the implantation of an implantable cardioverter defibrillator (ICD) have expanded since the device was first introduced, with current guidelines recommending its use in both primary and secondary prevention. Although the superiority of device therapy compared to anti-arrhythmic drugs for the primary prevention of sudden cardiac death in high-risk patients is well established, little is known about the impact of ICD indication on health-related quality of life (HRQL). Indication may also interact with psychological factors, such as personality. Using a prospective design, we examined whether ICD indication and type-D personality (i.e. experiencing increased negative emotions paired with emotional non-expression) serve as modulators of HRQL at baseline and 3 months post-implantation.
Methods Consecutively implanted ICD patients (n = 154) completed the Type-D Scale (DS14) at baseline and the Short-Form Health Survey 36 (SF-36) at baseline and 3 months.
Results Of all patients, 82 (53%) received an ICD due to prophylactic reasons; the prevalence of type-D was 23%. ANOVA for repeated measures showed that indication had no influence on HRQL (p = 0.75). Further stratification by personality showed a main effect for type-D personality (p < 0.001), with type-D patients generally experiencing poorer HRQL; there was no main effect for indication (p = 0.45) nor was the interaction effect indication by type-D significant (p = 0.22). However, there was a significant improvement in HRQL over time (p = 0.001). Adjusting for clinical factors and shocks during follow-up, Type-D remained an independent predictor of impaired HRQL (p < 0.001), although there was no longer a significant change in HRQL over time (p = 0.099).
Conclusions Type-D personality but not ICD indication was associated with impaired HRQL at the time of implantation and at 3 months, with type-D exerting an effect on HRQL independent of shocks and other risk factors. In the quest for enhancing risk stratification in clinical practice, personality factors, such as type-D, should not be ignored, as both type-D and poor HRQL have been associated with increased risk of mortality in cardiac patients.
014 Low density lipoprotein subclass distribution in children with renal diseases
S. Alabakovska, D. Labudovic, K. Tosheska, M. Alabakovski, B. Todorova
Medical Faculty, Department of Medical Biochemistry, Skopje, Macedonia
Background LDL lipoproteins are heterogeneous and composed of several subclasses. Small LDL3 and LDL4 particles are more atherogenic than larger LDL1 and LDL2 subclasses, and their frequency may depend on plasma lipid and apoprotein levels. Because there is not enough literature data presenting LDL subclass distribution in childhood, the aim of this study was to examine LDL subclass profile in children with renal diseases compared with healthy children.
Methods Plasma LDL subclasses in 100 healthy and 30 children with renal diseases aged 9–;18 years were analyzed using non-denaturing polyacrilamide gradient (3–;31%) gel electrophoresis. Plasma lipid and apoprotein parameters affecting LDL size were determined as well.
Results In 89% of the healthy children bigger LDL subclasses were dominant (phenotype A), whereas 11% of the children belong to phenotype B (small LDL3, LDL4). In children with chronic renal failure on haemodialysis the frequency of phenotype B was increased (58, 5%), and the mean LDL diameter was smaller (p < 0,0005) compared with control group. In patients with renal diseases who were not on haemodialysis the frequency of phenotype B was even more increased (88%) and the mean LDL diameter was smaller (p < 0,0001) compared with control group. In all patients significant negative correlation between LDL diameter and plasma triglycerides (p < 0,0001) and Apo B concentration (p < 0,0001) was noted.
Conclusion Children with chronic renal diseases are at high risk for atherosclerosis, especially in the patient not going on haemodialysis. Determination of LDL subclasses distribution in healthy children population and in patients may help prevent and reduce the risk for atherosclerosis.
015 Cytotoxin-associated gene-A bearing strains of Helicobacter pylori and atrial fibrillation due to ischemic origin. Is there a link?
H. Badran1, M. Mahfouz2
1Menoufiya University
2Tanta University, Tanta, Egypt
Objectives Previous studies suggested an association between infection by cytotoxic CagA bearing Helicobacter pylori (Hp) strains and atherosclerosis. We hypothesized that CagA strains could increase the risk for atrial fibrillation (AF) in patients with chronic coronary heart disease (CHD) by induction of systemic inflammatory reactions. Our aims were: (1) to verify the association between CagA strains and CHD, (2) to attest the presence of Cag A strains in AF due to ischemic etiology.
Methods and subjects Serological status for Hp cagA by a semi quantitative commercial (ELISA) kit against the p120 antigen of CagA, C-reactive protein, total leucocytic count and atrial size using echocardiography were determined in 185 patients with proved CHD. Patients were assigned to CHD and AF (Group A, n = 82) or CHD with sinus rhythm (Group B, n = 103). Eighty subjects from the same geographical area free of clinical cardiovascular disease matched for age and sex were assigned to a control group.
Results 52(63%) patients were seropositive for Hp Cag A in Group A versus 40(39%) in Group B (odds ratio 3.95 with 95% confidence interval 1.94–;6.0). Only 21(26%) of the control were seropositive. A significant association between seropositivity for Hp Cag A and having previous myocardial infarction (68 versus 53%, odds ratio 2.04 with 95% CI: 1.02–;2.82, P = 0.034) was perceived. These findings remained valid in a multivariate analysis including possible confounding factors (for instance age, sex, smoking and hypertension; odds ratio 2.35 with 95% CI 2.01–;4.83). Left atrial dimension and CRP were significantly increased in Cage A seropositive compared with seronegative subgroups 4.31 ± 0.66 vs 3.1 ± 0.58 cm & 3.32 ± 0.86 vs 1.79 ± 0.72 mg/l in group A and 3.7 ± 0.62 vs 2.85 ± 0.66 cm & 2.5 ± 0.54 vs 1.62 ± 0.5 mg/l in group B respectively (P < 0.01).
Conclusions This study provides further support for the hypothesis that there is a causal relationship between chronic infection with Hp and CHD especially if AF arises. The positive association between Hp (Cag A) with elevated CRP and increased atrial size in patients having CHD and AF may reflect the inflammatory changes in the atrial structure that promotes the development or persistence of AF.
Key Words Helicobacter pylori, Cag A strain, Atrial fibrillation, Coronary artery disease.
021 Statins in calcific aortic stenosis: a meta-analysis
Arnold S. De Guzman, MD
Heart Institute, St Luke's Medical Center, Philippines
Background Calcification of the aortic valve is the third leading cause of heart disease in adults (Oudit and Chow, MD, Statin Therapy for Valvular Aortic Stenosis: Opportunities and Challenges) and the most common cause of valve replacement in developed countries. Compelling data now suggest that it is an active disease process similar to atherosclerosis. Hence, it raises the possibility that the treatment used in preventing or slowing the progression of vascular atherosclerosis may be effective in patients in patients with aortic stenosis. In limited observational studies, aortic stenosis progressed at a slower rate in patients who received statins than in those who did not. The objective of this meta-analysis is to determine the efficacy of statin treatment in preventing the progression of calcific aortic stenosis.
Methods Clinical trials were identified from Medline search, PUBMED, and Cochrane collaboration databases 1999 to 2006 using the following keywords: statins, aortic stenosis, aortic valve calcification, randomized controlled trials and MESH terms Hydroxymethylglutaryl-Coa Reductase Inhibitors, heart valve disease. A total of 7 articles were queried, 2 of which are RCTs and were subjected to data extraction, quality scale and included in the study. Independent quality assessment scale and the inclusion criteria were strictly applied. Included studies were randomized controlled trials involving a total of 294 patients with mild to moderate calcific aortic stenosis (Vmax 2.0 –; 3.9m/s). Patients with coexisting more than mild aortic regurgitation, severe mitral valve stenosis, left ventricular dysfunction (ejection fraction, < 35 percent), planned aortic valve replacement, intolerance to statins, statin therapy or a potential benefit from statin therapy (according to the treating physician) and baseline serum cholesterol of less than 150 mg per decilitre, and presence of a permanent pacemaker or cardiodefibrillator.
Main results The analysis of the rate of annual increase in peak aortic velocity (m/s/year) of the two trials showed to be homogenous (Chisquare = 0.14, df = 1, P = 0.70). The result showed that the use of statins did not significantly improve the rate of annual peak aortic velocity from the baseline as compared with the placebo with P value of 0.75 with mean duration of more than 24 months.
Conclusions Statin therapy favours trend towards benefit but did not reach statistical significance in terms of slowing the rate of change in aortic-jet velocity nor induces its regression.
Reviewer's conclusion Statin therapy is neither cost-effective nor recommended for patients with mild to moderate calcific aortic stenosis. Large, prospective, randomized controlled trial should be done using statins in the different stages of calcific aortic stenosis to determine its specific value and effectiveness.
022 Clustering of psychosocial risk factors enhances the risk of depressive symptoms 12-months post-PCI
S.S. Pedersen1,2, J. Denollet2, P.W. Serruys2, R.T. van Domburg2
1CoRPS - Department of Medical Psychology, Tilburg University, Tilburg, The Netherlands
2Department of Cardiology, Thoraxcentre, Erasmus Medical Centre, Rotterdam, The Netherlands
Objectives Psychosocial risk factors tend to cluster together within individuals, but generally a single factor approach has been adopted when studying their impact on health outcomes in patients with coronary artery disease. We examined the influence of co-occurring psychosocial risk factors (i.e. anxiety and type-D personality) on depressive symptoms at 12 months in patients treated with percutaneous coronary intervention (PCI). Type-D is defined as the tendency to experience increased negative emotions paired with their non-expression.
Methods Consecutive patients (n = 416) with stable or unstable angina, treated with PCI using the paclitaxel-eluting stent as the default stent, completed the Type-D Scale (DS14) and the Hospital Anxiety and Depression Scale anxiety subscale (HADS-A) at baseline and the depression subscale (HADS-D) at 12 months.
Results Of all patients, 27% experienced depressive symptoms at 12 months. The presence of depressive symptoms could not be attributed to the experience of a cardiac event during follow-up (p = 0.76). There was a dose-response relationship, with the prevalence of depressive symptoms being lowest in the no anxiety/no type-D group (13%), followed by anxiety only (38%) and type-D only (45%), with the highest prevalence in patients with co-occurring anxiety/type-D (64%; p < 0.001). The single risk factors type-D personality (OR: 5.82; 95% CI: 2.93–;11.56) and anxiety (OR: 4.36; 95% CI: 2.23–;8.55) and their co-occurrence (OR: 12.38; 95% CI: 6.11–;25.09) remained independent significant predictors of depressive symptoms at 12 months, adjusting for demographic and clinical baseline characteristics.
Conclusions Patients with the co-occurrence of anxiety and type-D personality, two risk factors that have independently been associated with adverse prognosis, had a considerably higher risk of depressive symptoms 12 months post-PCI compared to patients with none or one of these risk factors. Further research is warranted to examine whether the co-occurrence of psychosocial risk factors also has deleterious effects on prognosis.
036 The efficiency of therapy by atorvastatin at high dose in prevention of cardiac complications after aorta-femoral bypass operation in patients with atherosclerosis and heart failure
Shchukin Y., Vachev A., Seleznev E., Dyachkov V., Medvedeva E., Pikatova E., Surkova E.
Samara State Medical University, Samara, Russian Federation
Objective To assess the efficiency of atorvastatin in prevention of cardiac complications after The aorta-femoral bypass (AFB) operation in patients with atherosclerosis and heart failure (HF).
Methods 78 patients with atherosclerosis and HF (II-III functional class), undergoing AFB operation, were included in the study. The level of cholesterol, low-density lipoproteins (LDL), C-reactive protein (CRP), interleykin-6 (IL-6), tumor necrosis factor–;alpha (TNF-a), endotelin-1 (ET-1), soluble CD40 ligand (sCD40L), extracellular superoxiddismutaza (EC-SOD), neopterin, stable metabolites of Nitric oxide (NOx), production of radical O2 by activate leucocytes in blood were measured. The postoperative myocardial ischemia was determined by means of electrocardiography monitoring (Holter). Patients were divided into two groups: 1. 38 patients received atorvastatin (atoris, KRKA) 60 mg per day during 7–;10 days before operation; 2. 40 patients were prepared in traditional way without atorvastatin. The control group included 36 healthy people.
Results Before treatment we found increase of concentration of cholesterol, low-density lipoproteins, the signs of oxidative stress and endotelial dysfunction in both patients groups. In the first group after atorvastatin treatment we revealed significant decrease in level of neopterin, ET-1, IL-6, TNF-a, CRP, sCD40L and increase in level of NOx, EC-SOD. Furthermore, we found significant increase in the rate of postoperative myocardial infarction and ischemia in the first group in comparison with the second one.
Conclusions Preoperative atorvastatin significantly reduces adverse cardiac events after AFB operation in patients with atherosclerosis and heart failure. It may be connected with reduction of inflammation, endotelial dysfunction, vascular oxidative stress and suppression of reactions of trombocytes activation.
046 Chronic coronary heart disease. Failure of annual checkups to achieve secondary prevention targets
C. Peía Gil, E. Abu Assi, R. Vidal Pérez, F. Soto Loureiro, A. Amaro Cendón
Hospital Clínico Universitario. Santiago de Compostela. Spain
Objective To analyze the monitoring of cardiovascular risk factors in patients suffering from coronary heart disease (CHD) follow-up by primary physician and annual cardiology checkup.
Methods 361 consecutives patients suffering from CHD with more than one previous annual checkup in the cardiology office were studied. Fasting plasma glucose and lipid profiles (total cholesterol (TC), LDL cholesterol and HDL cholesterol) were measured and blood pressure, weight, height, physical activity and treatments were recorded.
Results Mean age was 67.8 ± 11, 271 (75%) males. 11% of patients were smokers. 20% were sedentary. Body mass index (BMI) was 28.5 ± 3.8 Kg/m2, 32% of patients demonstrated BMI > 30 Kg/m2 and 51% were in the overweight range (BMI 25 to 29.9 Kg/m2). In 36% systolic blood pressure was > 140 mmHg, and in 18% diastolic blood pressure was > 90 mmHg. 20% demonstrated glucose fasting levels ≥ 125 mg/dl (6.9 mmol/l) and 27% between 105–;125 mg/dl (5.8 to 6.9 mmol/l). 49% of patients demonstrated total cholesterol > 190 mg/dl. 81% of patients demonstrated LDL cholesterol ≥ 100 mgrs/dl (2.6 mmol/l) with an average of 125 ± 32 mg/dl. 22% demonstrated HDL cholesterol < 35 mg/dl (0.9 mmol/l). 77% pts were on Statin and 85% were on Aspirin.
Conclusion The combined primary care monitoring and annual specialist checkup fail in achieving secondary prevention targets, fundamentally in LDL cholesterol control in spite the high number of Statin prescriptions. Its necessary and urgent to design new more effective assistance approaches.
050 The National Program of Quality Indicators of Community Health Care (QIC) in Israel: prevention of cardiovascular risk factors
Avi Porath1,2,3
1Ben Gurion University of the Negev
2Soroka Medical Center
3Clalit Health Services
The QIC program was initiated by the four Israeli HMOs and with the support of the Israel Medical Association and sponsorship of the Israel Institute for Health Policy and Health Services Research. In March, 2004, the Ministry of Health declared this activity to be a permanent, institutionalized national program. Its main objectives are: to improve the quality of community health care in Israel by ongoing measurement of clinical performance; to provide information to the public and to policymakers about the quality of health services in Israel.
The program presents a nationwide picture of the quality of community health care in Israel for 2003–;2005. The data relate to the five areas of community health care –;primary and secondary prevention of cardiovascular risk factors, diabetes management, screening for detection of colorectal and breast cancer, treatment of asthma, and flu vaccination. In 2005 forty-six measures were reported to the public. Primary prevention of cardiovascular disease was reported in terms of screening blood cholesterol levels, measuring blood pressure and evaluating the status of the target blood cholesterol levels in the general population. As an example, approximately 70% of the adult population underwent testing for blood cholesterol levels, based on the frequency adjusted for the age of the population. In both age groups, 35–;54 and 55–;74, women underwent more tests than men. The age-adjusted target was reached in 64% of the target population.
No significant differences were found in achieving targets with respect to socio-economical status. The rate of testing for LDL cholesterol in diabetes patients reached 87% in 2005, and 48% of them reached the target LDL level below 100 mg/dl. Documentation of blood pressure was found for 50% of the younger age group and for 60% of the older age group in the target population. This figure was considered insufficient by the HMOs and management programs were introduced to improve performance. Significant improvements were noticed in all measures since the first annual report in 2004. These improvements were the result of the initiatives and specific management programs introduced by the health plans in response of the findings.
070 Relationship between visceral adiposity and postprandial hyperlipidemia
Y. Hata1, M. Takikawa2, T. Kasai3, K. Oikawa4, H. Kakuchi5
1Tokai University Hachioji Hospital
Objective To evaluate the influence of lipid loading on lipid and carbohydrate metabolism, and to examine its relationship with visceral adiposity. [Subjects] 87 patients, hospitalized to undergo a coronary angiography (67 ± 8 years of age; 63 cases of ischemic heart disease).
Methods We measured visceral adiposity using an abdominal MRI during hospitalization. On the day of discharge, we performed lipid (Oftocream) loading with the patient in a fasting state. We measured fasting blood sugar, insulin (IRI), triglycerides (TG), HDL-Cho, LDL-Cho and RLP-C before and two hours after lipid loading.
Results Both blood sugar (104.9 ± 15.8 → 108.5 ± 17.6) and IRI (8.4 ± 5.2 → 10.3 ± 5.3) increased due to lipid loading (p < 0.01). We also observed a significant increase in TG, HDL-Cho, LDL-Cho and RLP-Cho (p < 0.01). In the 53 cases with visceral adiposity of more than 100 cm2, we observed a significant correlation between the amount of visceral adiposity and the amount of change of TG and RLP-C due to lipid loading (p < 0.05).
Discussion Study findings suggest that lipid loading has an effect not only on lipid metabolism, but also on carbohydrate metabolism. In patients with visceral adiposity syndrome, we were able to observe a correlation between the amount of visceral adiposity and the amount of change of TG and RLP-C due to lipid loading.
074 Hyperlipoperoxidemia among patients with coronary atherosclerosis
G. Chapidze,
Emergency Cardiology Center, Tbilisi, Georgia
Patients with established coronary heart disease (CHD) are at high risk for developing of recurrent coronary events. The aim to take care of such patients is trying to prevent progression of coronary atherosclerosis. The importance of traditional risk factors, including dyslipidemia is well known, but they can not completely explain pathogenesis of atherosclerosis, approximately half of cardiovascular events occur in persons with low to average levels of low-density lipoprotein cholesterol, which is one of the most important risk factors for atherosclerosis. Hence the great attention has been paid to nontraditional risk factors including oxidative stress. This is a retrospective cohort study of outpatients with coronary atherosclerosis, who are under observation in the Department of Secondary Coronary Prevention of CHD of our center.
Study population consisted of 179 patients. Mean age was 55.6 ± 7.3 years, 119 were male. 90 (50.3%) patients had undergone coronary artery bypass graft operation, 33 (18.4%)-percutaneous coronary intervention and 56 (31.3%) patients had CHD without myocardial revascularization. All patients were on aspirin treatment. An important biomarker of oxidative stress — plasma lipoperoxide (LPO) was measured. Mean concentration of LPO was 2.81 ± 2.08mkmol/L which is more than 5 times upper limit of normal.
Generally, 99.4% of patients had hyperlipoperoxidemia. Hyperliopoperoxidemia was connected with an extent of coronary atherosclerosis. Mean value of LPO was 2.36 ± 1.13 mkmol/L, 2.52 ± 2.06 mkmol/L and 3.17 ± 2.21 mkmol/L for patients with one-, two- and three-vessel disease, respectively. Statistically significant difference in LPO levels was observed between patients with one- and three-vessel disease (p < 0.05). It is noteworthy that in spite of aspirin treatment patients with very high plasma LPO concentrations (> 2 mkmol/L), platelet hyperaggregation was found. In such cases mean value of this parameter was high enough –; 103 ± 7.05%. This may be interpreted as aspirin resistance in such a category of patients, which should be indeed very important in patients with CHD. Hyperlipoperoxidemia was strongly associated with platelet hyperaggregation, there was statistically significant positive correlation between LPO and platelet aggregation (r = 0.31, p = 0.01).
According to our results, hyperlipoperoxidemia is an ordinary event in patients with coronary atherosclerosis. Measurement of LPO will give useful information for cardiologists, modification of this parameter may delay progression of aggressive atherosclerotic process and thus, may prevent recurrent coronary events.
075 Lipid optimization tool database to audit LDL control rates for various guideline targets in a community cardiology group practice
1Ottawa Cardiovascular Centre, Ottawa, Canada
Objectives To validate the Lipid Optimization Tool (LOT) Database as a practice audit tool to measure current LDL control practice performance at the Ottawa Cardiovascular Centre (OCC).
Methods We have previously reported the use of the LOT to guide LDL control through a structured, nurse driven lipid management protocol in approximately 7000 patients at the OCC. For our 2006 practice audit, a database version of the LOT was developed. This database is designed to risk stratify using either Framingham or risk factor counting strategies, to calculate LDL percent reduction necessary to achieve to CCS, ATP III or user defined targets, to provide therapeutic decision support in selecting and titrating lipid lowering therapy and to track sequential control rates to specified targets. Reports including risk factors, risk modifiers, coronary heard disease (CHD) equivalents and LDL control rates are generated automatically. Parameters from 1002 sequential patients managed with the LOT by 9 OCC physicians were entered into the database.
Results Of the 1002 patients entered 69% were male and 31% female, 89% were in a high risk age category, 48% were hypertensive, 19% were diabetic and 14% were smokers. Sixty five percent (65%) of patients had coronary artery disease (CAD). LDL control rates were 92% to an LDL of 3.0 mmol/L, 84% to an LDL of 2.5 mmol/L, 61% to an LDL of 2.0 mmol/L and 47% to an LDL of 1.8 mmol/L. These results were compared to previous year's audits and published LDL control rates. OCC LDL control rates were 78% for 2004, 81% for 2005 and 84% for 2006. Comparable Vascular Protection (VP)/Guideline Oriented Approach to Lipid Lowering (GOALL) registry control rates were 51%, 22% and 20.8 to LDL's of 2.5, 2.0 and 1.8 mmol/L respectively and Canadian Lipid Study-Observational (CALIPSO) control rates of 64% to an LDL of 2.5 and 19% to an LDL of 1.8 mmol/L.
Conclusions The LOT database was used to measure performance of the LOT at the OCC. Achieved LDL control rates control rates are among the best reported in the world literature. The next steps are to validate use of the LOT Database to guide prospective lipid management at the OCC and various other clinical practice settings.
076 Troponin negative patients: outcome, management and mortality data after a 2 year follow up
Royal United Hospital Bath NHS Trust, Bath, United Kingdom.
Taunton and Somerset NHS Trust, Taunton, United Kingdom.
Introduction Troponin is an important cardiac bio-marker which helps us to identify and risk stratify patients admitted to hospital with chest pain. It helps us to adopt an early invasive strategy and institute an early aggressive treatment in high risk patients who have an elevated troponin value (> 0.03).
Objectives Our aim was to study the outcome in patients admitted to coronary care unit with cardiac sounding chest pain who were troponin negative (value < or = 0.03).
Methods 324 patients were enrolled into the study. Outcome, management and mortality data were collected after a period of 2 years. Patients were divided into 3 groups –; Outpatient Exercise Treadmill Test (ETT) group (n = 66), Inpatient ETT group (n = 80) and No ETT group (n = 178). The groups were further subdivided into patients who underwent coronary angiography and patients who did not undergo coronary angiography.
Result
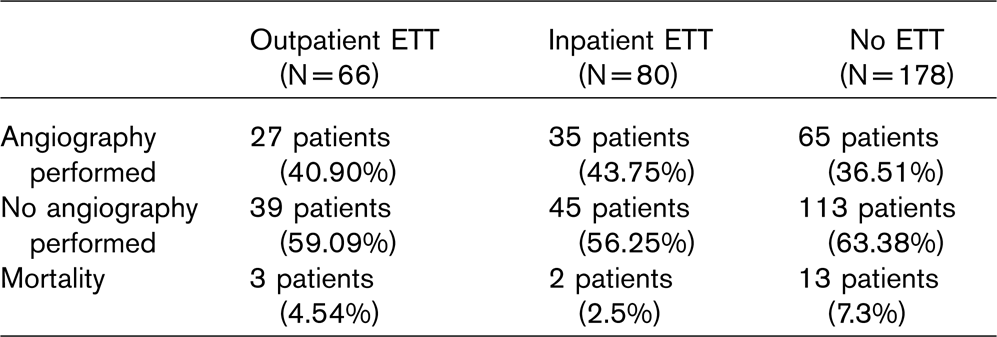
The combined total mortality rate was 5.55%. 3 patients died due to cardiac causes, 14 patients died due to non-cardiac causes, mainly carcinoma and the cause was unknown in 1 patient as he died at home. The 3 patients who died due to cardiac causes did not undergo ETT as they had known long standing cardiac problems.
Conclusions Troponin positive patients are a high risk group and troponin negative patients are a low risk group. Nevertheless, troponin negative patients should be investigated further with an outpatient ETT, inpatient ETT or coronary angiography based on clinical history/risk factors. The above data suggests that patients can be safely discharged from hospital if they are troponin negative. But it should be emphasised that cardiac risk assessment is a continuous process.
078 Prevention of the progression of coronary atherosclerosis by combination therapy with coenzyme Q10 and statins
N. Latsabidze, N. Dolidze, Z. Bakhutashvili
Emergency Cardiology Center
The goal of the present research was to assess the efficacy of combination treatment with antioxidant coenzyme Q10 (CoQ) and simvastatin as well as coenzyme Q10 without statin therapy in order to prevent further progression of coronary atherosclerosis. 73 outpatients (61 male and 12 female, mean age 58 ± 6.3 years) were divided into 2 groups: receiving coenzyme Q10 (Hasco-Lek, Poland) 90 mg daily and its combination with simvastatin (zocor, vasilip) 10 mg daily for an 8-week period. 57 patients had undergone myocardial revascularization — bypass operation and percutaneous coronary intervention.
The treatment with coenzyme Q10 demonstrated its potential independent role in positive modification of oxidative stress (measured by plasma lipoperoxide — LPO levels), antiatherogenic fraction of lipid profile (high density lipoprotein cholesterol — HDL-C), atherogenic ratio, platelet aggregation. CoQ had a beneficial effect on HDL-C. It increased by 22% (p < 0.01). This effect was more expressed in combination with statin therapy. In this group of patients antiatherogenic fraction of lipid profile increased by 28% (p < 0.001). The target levels of HDL-C were attained in 81% of cases. In both groups of patients atherogenic ratio decreased significantly as well (p < 0.01; p < 0.001). During the treatment with íoQ there was statistically significant reduction in mean plasma LPO level — it was decreased by 30%.
Similar data were observed on the background of combination therapy with CoQ and simvastatin. Among patients with very high levels of LPO (LPO ≥ 2 mkmol/L) platelet hyperaggregation was observed. Obtained results indicate antiaggregative ability of therapy with CoQ and CoQ+simvastatin in patients with high degree of oxidant stress. In conclusion, suggested approach may result in complete correction of dyslipidemia, reduce degree of oxidative stress and platelet aggregability. Consequently such a combination may be beneficial in preventing of further development of coronary atherosclerosis among all coronary heart disease patients with or without myocardial revascularization.
079 The results of secondary coronary prevention in patients undergoing myocardial revascularization
Emergency Cardiology Center, Tbilisi, Georgia
Background Patients undergoing myocardial revascularization procedures — coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) are at high risk for development of further coronary events. This fact is conditioned by ongoing atherosclerotic process, which may result in stenosis and occlusion of bypass grafts as well as of native coronary arteries. Therefore such a category of patients is considered as a top priority for preventive cardiology.
Methods 578 outpatients (482 men and 96 women, mean age — 57 ± 7.3 years) visited the Department of Secondary Coronary Prevention were enrolled in the study. 411 patients had undergone CABG operation, 162 — PCI, 3 — PCI + CABG and 2 — CABG + PCI. Mean duration of the follow-up was 874 ± 87 days. The primary end points were cardiac mortality rate and recurrent coronary events. The secondary end points were health-related quality of life according to the Nottingham Health Profile, low-density lipoprotein cholesterol levels, left ventricular ejection fraction and prescribed drugs.
Results Cardiac mortality rate after both methods of myocardial revascularization was 1.9%. Recurrent coronary events were observed in 8 and 14 cases after CABG and PCI, respectively. In 6 patients following CABG repeat angiography revealed vein graft occlusions, 2 patients had progression of atherosclerotic lesions in native coronary arteries. 8 patients undergoing PCI had restenosis and reocclusions, 6 patients — new stenosis and occlusions in native coronary arteries. No angina relapse occurred in 5 patients following CABG and PCI combination. Quality of life evaluation showed the significant improvement in 4 components — energy, pain, emotion and mobility status. There was no significant change in sleep pattern and social function deteriorated before. At the end of the follow-up target levels of low-density lipoprotein cholesterol (less than 100 mg/dl) were obtained in 78% of cases. There was statistically significant increase in left ventricular ejection fraction (from 46 ± 4% to 55 ± 6%). The first line agents after myocardial revascularization were aspirin and statins. Aspirin use was almost universal — 97% of patients received it. The use of statins was high enough — 82%. More than half of the patients received angiotensin-converting enzyme inhibitors, 41% of patients — beta-blockers. Other preparations were prescribed less frequently.
Conclusions According to our data on the background of preventive strategies and treatment the mid-term results of CABG and PCI are satisfactory. The maintenance of results of CABG and PCI by the efforts of secondary coronary prevention is not less important, if not more important, than namely myocardial revascularization.
083 Anxiety and depression symptoms in arterial hypertension and coronary heart disease patients: results of a multicenter study
National Research Center for Preventive Medicine, Moscow, Russia
We investigated the incidence of anxiety/depression symptoms in arterial hypertension (AH) and coronary heart disease patients (CHD), and the associations between anxiety/depression symptoms and cardiovascular risk factors.
Methods Anxiety and depression symptoms were assessed by means of the Hospital Anxiety and Depression Scale (HADS) in 5038 pts with AH, 3271 of whom had CHD (37,2% post-myocardial infarction) aged 55 years and more.
Results Anxiety symptoms (≥ 11 HADS anxiety subscale) were found in 33% of hypertensive pts without CHD and 38% of hypertensive pts with CHD, depressive symptoms (≥ 11 HADS depression subscale) –; in 30% and 38%, respectively. Logistic regression analysis showed a highly significant association of anxiety/depression symptoms with low level of education, low level of income, low level of physical activity, chronic life stress, endured acute stresses during a year before inclusion, blood pressure ≥ 140/90 mm Hg. Anxiety/depression symptoms were also associated with female sex, age, disability, retirement, antihypertensive treatment, non-regular antihypertensive/antianginal treatment and excessive use of medical resources (frequent visits to out-patient clinics and hospitalizations).
090 Incidence and treatment of dyslipidemia in the Czech army officers
1Central Military Hospital
2Institute of Aviation Medicine
3Institute of Chemical Technology, Prague, The Czech Republic
Introduction The negative sequelae of dyslipidemia in adults, particularly on cardiovascular morbidity and mortality, are well known as well as the positive impact on their treatment with hypolipidemic agents. During 2005, we observed the incidence of dyslipidemia in the group of army officers and treated them in accordance with EA guidelines. We assessed SCORE index based on Framingham algorithm.
Methods We carried out epidemiological, retrospective, cross-sectional study among the group of 698 officers in total. The cohort consisted of 605 males between 22–;59 yrs. mean age of 39,1 yrs. and 93 females between 23–;53 yrs. mean age of 33,9 yrs. For the purpose of our study, we used clinical criteria according to EAS. The TC upper limit was 5,2 mmol/l, for LDL-C 3,5 mmol/l, for HDL-C less than 1,0 mmol/l, and as for triglycerides, less than 1,9 mmol/l. We analysed types of dyslipidemia, incidence trends in consecutive decades and compared them with healthy individuals without metabolic disorders. Moreover, we were searching for co-morbidities like hypertension, impaired fasting glucose tolerance syndrome/diabetes mellitus, smoking/non-smoking habits, obesity. We analysed treatment strategies and medication administered.
Results 57% dyslipidemia prevalence was detected in males and 43% in females. We found out isolated hypercholesterolemia in 47%, combined one in 43% and pure hypertriglyceridemia in 10%. The dyslipidemia incidence was increasing from third to fifth decade cohort from 28% to 67%. We found a higher incidence of dyslipidemia in patiens with hypertension, overweight/obesity and subjects with IFG/DM. As for treatment strategies, 62% individuals were only on low cholesterol diet and other protective regimen measurements, 38% were additionally put on medication, particularly on statins in 75%, on fibrates in 21% and in 5% on their combinations. Taking into an account the SCORE index, those with dyslipidemia were at higher risk for fatal cardiovascular events in the near future.
Conclusion From preventive point of view, obtained data might be used for risk factors identification, officer's education, risk stratification and finally their elimination, more targeted treatment, particularly risk factors like hypertension and hypercholsterolemia are eligible, because of “the lower, the better”, in order to improve the health status and prevent from atherosclerosis-related diseases.
092 Type-D personality is a stable and independent predictor of impaired health status in patients with chronic heart failure over a 12-month period
A. Schiffer1,2, S.S. Pedersen1, J. Widdershoven2, J. Denollet1
1CoRPS-Department of Medical Psychology, Tilburg University, Tilburg, the Netherlands
2TweeSteden hospital, Tilburg, the Netherlands
Objectives Health status is an important patient-centred outcome, but impaired health status has also been associated with adverse prognosis in chronic heart failure (CHF). However, little is known about the determinants of health status in CHF. We examined whether type-D personality (joint tendency to experience negative emotions paired with their non-expression) exerts a stable effect on health status in CHF patients over a 12-month period and is an independent predictor of impaired health status at 12 months.
Methods 166 consecutive systolic CHF patients (75% men; mean age 66 ± 9) completed the Type-D Scale and the Beck Depression Inventory (depressive symptoms) at baseline, and the Minnesota Living With Heart Failure Questionnaire (disease-specific health status) and the Short-Form Health Survey (mental and physical generic health status) at baseline and 12-month follow-up.
Results There were no significant differences between type-D (23% of total sample) and non type-D patients on baseline characteristics. Although there was a general improvement in disease-specific (F(1,164) = 7.101; p = 0.008) and mental generic (F(1,164) = 3.648; p = 0.06) health status over the 12-month period, type-D patients reported significantly lower disease-specific (F(1,164) = 25.482; p < 0.001) as well as mental generic health status (F(1,164) = 45.311; p < 0.001) compared to non type-D patients (37.4 ± 21.7 versus 21.6 ± 17.1, and 45.2 ± 10.9 versus 55.8 ± 8.4, respectively). The negative impact of type-D personality on disease-specific (F(1,164) = .020; p = 0.89) and mental generic health status (F(1,164) = .164; p = 0.69) was stable, as indicated by the non-significant interaction effects for type-D × time. In multivariable linear regression analyses, type-D personality was an independent predictor of disease-specific (β = .20; t = 3.0, p = 0.003) and mental generic (β = −.25; t = −3.5, p = 0.001) health status, controlling for socio-demographic variables, LVEF, NYHA class, diuretics, spironolacton, long-acting nitrates, psychofarmaca, depressive symptoms and baseline health status. Type-D personality was not related to physical generic health status.
Conclusions Type-D personality was a stable and independent predictor of impaired disease-specific and mental generic health status over a 12-month period. Because health status is an important patient-centred outcome and related to death and hospitalisation in CHF, counselling of patients at high risk for impaired health status is indicated.
094 Co-morbid depression (hopelessness) and diabetes are associated with 3-year prognosis in PCI patients treated with the paclitaxel-eluting stent
S.S. Pedersen1,2, R.T. van Domburg2, P.W. Serruys2, Johan Denollet1
1CoRPS-Department of Medical Psychology, Tilburg University, Tilburg, The Netherlands
2Department of Cardiology, Thoraxcentre, Erasmus Medical Centre, Rotterdam, The Netherlands
Objectives Depression and diabetes both comprise risk factors for adverse prognosis in patients with coronary artery disease (CAD). However, studies have examined their separate influence on clinical outcome rather than their co-occurrence, although risk factors tend to cluster together within individuals. Hopelessness comprises a characteristic feature of depression, but correlates weakly with standard depression scales, suggesting that it deserves studying in its own right. We examined the impact of co-morbid hopelessness and diabetes on 3-year prognosis in percutaneous coronary intervention (PCI) patients.
Methods Consecutive PCI patients (n = 534) treated with the paclitaxel-eluting stent as the default strategy completed a one-item hopelessness measure at baseline. Patients were followed up for adverse clinical events (mortality and non-fatal myocardial infarction (MI)) for 3 years.
Results At 3-year follow-up, there were 38 events. The incidence of death/MI was 4% in patients with no risk factors (hopelessness nor diabetes), 8% in the diabetics, 11% in the high hopelessness patients, and 16% (p = 0.002) in patients with co-morbid hopelessness and diabetes, showing a dose-response relationship. Patients with diabetes (HR:2.40; 95%CI: 0.82–;7.01) and hopelessness only (HR:3.28; 95%CI: 1.49–;7.23) were at increased risk of adverse clinical outcome, with patients with co-morbid hopelessness and diabetes being at the highest risk (HR:4.89; 95%CI: 1.86–;12.85) compared to patients with no risk factors. Patients with co-morbid hopelessness and diabetes (HR: 4.86; 95%CI: 1.78–;13.31) remained at the highest risk for adverse prognosis at 3 years, followed by high hopelessness patients (HR:3.32; 95%CI: 1.49–;7.40) and patients with diabetes (HR:2.37; 95%CI: 0.77–;7.26), adjusting for demographic and clinical risk factors.
Conclusions Co-morbid depression (hopelessness) and diabetes were associated with the highest risk of adverse clinical outcome at 3-year follow-up. This finding testifies to the importance of identifying patients with co-morbidity, as they likely require special management in clinical practice including additional intervention, e.g. of a behavioural nature, in addition to pharmacological treatment.
108 Association between inflammatory states of respiratory tract and protective effect of influenza vaccination in patients with coronary heart disease
I. de la Puerta1, G. Piíol-Ripoll2, L.M. Alvarez1, C. Ortas1, I. Lacambra1, A. del Río1
1Cardiology Division, Zaragoza.
2Neurology Division, Zaragoza.
Objective Prior studies have suggested that infections might trigger vascular events, but the role of Influenza Vaccination (IV) as protecting factor remains unclear. The most accepted hypothesis is that infection is associated with atherogenesis and thrombotic states related to atherosclerotic plaque rupture; and avoiding influenza infection by vaccination would reduce the risk of cardiovascular events. We studied the importance of Chronic Bronchitis, as chronic inflammation state; the use of antibiotics in previous three month, as situation of acute inflammation; and the antecedent of IV as a possible protecting factor. We hypothesized that inflammation states would be more frequent and the use of IV less frequent in acute coronary syndrome (ACS) patients than in patients with established coronary atherosclerosis.
Methods Since 15th of September 2004 until 10th of January 2005, we performed standardized interviews assessing vaccination status (this year, last year, three last years and five last years), risk factors, body mass index, smoking, chronic bronchitis, use of antibiotics in previous 3 month in 150 consecutive patients with ACS and 150 controls with previous history of coronary artery disease matched for age and sex. The patients with ACS were classified at discharge in: Q wave myocardial infarction, non Q wave myocardial infarction and unstable angina.
Results Patients with ACS were less often vaccinated against influenza than controls during current influenza season (56% and 74% respectively, p < 0.05), this results occurs in all subtypes of ACS (p < 0.05). Chronic bronchitis and acute infections in the previous three months to ACS were more frequent in patients than in controls (p < 0.05).
Conclusions Chronic bronchitis and the use of antibiotics in previous three month were more frequent in ACS patients suggesting that chronic and acute inflammatory states of respiratory tract would be associated with a transient increase of the risk of vascular events.
IV was less frequent in ACS patients than in controls, insinuating that vaccination have a protective effect against atherosclerotic plaque rupture.
111 Secondary prevention of myocardial infarction in elderly patients-gap between clinical research and practice
S. Ilic1, M. Deljanin Ilic1, D. Petrović1, B. Ilic1, I. Tasic1
1Institute of Cardiology, Niska Banja, University of Nis; Serbia
Numerous randomized clinical trials have shown that early started therapy with beta-blockers, angiotensin-converting enzyme (ACE) inhibitors and aspirin may reduce morbidity and mortality rates in patients with acute myocardial infarction (MI).
Aim To determine physician prescribing patterns of beta-blockers, ACE inhibitors and aspirin in patients who experienced acute myocardial infarction.
Methods We reviewed drug therapy at discharge in 840 patients (mean age 70.8 ± 7.7 years) with acute MI from 28 hospitals to assess the frequency of prescription of beta-blocker, ACE inhibitor and aspirin therapy. We also investigated which clinical characteristics were predictive for patients receiving those life-saving therapy.
Results Aspirin was the most frequently prescribed drug in pts with acute MI (84%). Low ejection fraction, heart failure, diabetes and hypertension were not influenced significantly on decision for aspirin therapy, but aspirin was prescribed more often in pts 65 years or above (P < 0.05). Beta-blocker and ACE inhibitor therapy was given lees often in pts with acute MI (45% and 41%). Beta-blockers were prescribed more often in pts with than in those without low ejection fraction, hypertension and frequent or complex ventricular arrhythmias (P < 0.05). ACE inhibitor therapy was prescribed more frequent for patients with low ejection fraction or in pts with heart failure than in pts with preserved left ventricular function (P < 0.05), in pts with than without prior MI (P < 0.01), in pts with diabetes than in those without diabetes (P < 0.05) and in hypertensive than in normotnesive pts (P < 0.01).
Conclusion Beta-blockers, ACE inhibitors and aspirin are under-prescribed in elderly patients who experienced a myocardial infarction, illustrating the gap between clinical research and clinical practice. Those pts with the greatest expected benefit receive those drugs most often but the majority of these patients were discharged without this life-saving therapy.
113 Survey of smoking habits in a single center tertiary cardiology outpatient clinic using Fagerstrom nicotine dependence test in Ankara/Turkey
T. Sayin, D. Oguz, M. Kilickap, T. Altin
Ankara University Department of Cardiology, Ankara/Turkey
Objectives To search for the smoking habits in detail in a cohort of single center, tertiary cardiology outpatient clinic.
Methods We prospectively examined smoking habits in detail, in consecutive patients during October 2006. We noted demographic variables, medical, educational status and we also performed Fagerstrom nicotine dependence survey to active smokers (points). We arbitrarily defined patients who have not been smoking for more than 3 months as exsmokers. Patients who have just quitted smoking (less than 3 months) were not analyzed.
Results Among 289 patients, 163 were female (56,4%). Mean age was 55,6 ± 12. Seventy seven patients (26,6%) were active smokers, 72 patients (24,9%) were ex-smokers and 138 patients (47,8%) had never smoked. In this cohort sex and educational status had significant effect on smoking habits. Women were less educated and they smoked less than man (P < 0.01 for both conditions). Paradoxically, in our cohort, more educated patient group (more than 5 years to university versus no education or primary school) used to smoke (active plus ex-smokers) more frequently (p < 0.01). Among 60 patients with documented atherosclerotic vascular disease (mainly coronary artery disease), 5 (8,3%) were active, 38 (63,3%) were ex-smokers. Using Fagerstrom survey, 19 (25.6%) of active smokers were severe addicts (taken as four points or more from a maximum of 10 points). Fagerstrom score and number of package-years of exsmokers/active smokers had a good correlation (r = 0,7, p < 0.01) indicating validity of the nicotine dependence survey.
Conclusions Smoking rates is very high in Turkey. One in two patients examined in cardiology outpatient clinic settings is either active or past smoker, while one in four is an active smoker. More efforts should be undertaken to combat this silent killer.
114 Type D personality is associated with lone atrial fibrillation recurrences rate: negative affectivity predicts the increased risk
E. Hatzinikolaou-Kotsakou, G. Bobotis, T. Beleveslis, E. Reppas, G. Moschos, A. Chantas, K. Tsakiridis
Saint Lukes Hospital
Background Type D (distressed) personality-a joint tendency towards negative affectivity (NA) and social inhibition (SI) -has been observed that might affect the atrial fibrillation recurrences rate (AFRR) in patients with lone atrial fibrillation (LAF).
Hypothesis We hypothesized that both Type D personality and its individual traits (NA and SI) predict AFRR in a population with LAF.
Methods Over a follow-up period of 4.2 ± 0.6 years we recorded the incidence of atrial fibrillation recurrences in a cohort of 185 consecutive patients (mean age 48 ± 11 years), who were known with LAF. At baseline, these patients completed the Type D Personality Scale (DS-14, German Version), a validated self-describing standard questionnaire.
Results NA and SI was diagnosed in 31.8% and 34.5% of the patients respectively.
From the total cohort, 22.3% had both NA and SI and therefore were classified as having a Type D personality. In Cox regression analysis, Type D personality proved significantly and independently predictive for AFRR, with an adjusted HR of 2.19 (95% CI 1.07–;4.48, P = 0.031). When The dimensions of Type D were entered as individual variables into regression models adjusting for age, gender, and arrhythmia duration, only NA significantly predicted AFRR (HR 2.27 (95%CI 1.15–;4.78, p = 0.029), whereas SI was not associated with AFRR. (HR 1.10 95%CI 0.57–;2.28, p = 0.745).
Conclusions Our results confirm Type D personality is as a potential risk for lone atrial fibrillation recurrences rate. Importantly, however, we found that the increased risk of AFRR with type D personality is solely driven by NA (representing experience of increased negative distress), whereas SI (representing inhibition of negative emotions) is not associated with AFRR.
115 Importance of stroke prevention in atrial fibrillation elderly patients
Bozinovic S1, Cvetkovic Matic D2
1Clinical Hospital Center Dr D Misovic, University Clinic for Internal Medicine Belgrade, Serbia
2Clinical Center of Serbia, Institute for Cardiovascular Disease, Belgrade, Serbia
Objectives Among survivors of stroke, who comprise at least 0.8% of the general population, at least half are permanently disabled. Cerebrovascular disease (stroke/TIA) as a health burden, and in Europe/North America: No. 1 cause of physical disability, No. 2 cause of dementia, No. 3 cause of death. The aim of this study was to evaluate the relationship between cardiovascular diseases-CVD (congestive heart failure-CHF, atrial fibrillation-AF, coronary artery disease-CAD), which might be responsible for cardioembolic stroke, and functional ability, quality of life and developing post stroke dementia in the elderly stroke patients, and recommend preventive measures for this population.
Methods 117 consecutive post stroke patients (74 women, age 68–;94, 75.4 ± 5,8 years) were divided into two groups: Group 1, pts with CVD, n1 = 69 (58,9%) and Group 2, pts with vascular risk factors (VRF) for stroke, like hypertension and diabetes, without CVD n2 = 35 (41,1%). We have analyzed their sex, age, functional ability for performing activities of daily living, quality of life, and cognitive impairment.
Results There were no differences in sex and age between the examined groups. Bed ridden were 46/117, 59/117 had bad quality of life, 38/117 developed post stroke dementia. In Group 1 35/69 had CHF, 29/69 had AF, and 39/69 had CAD. None of the pts with AF were using warfarin before stroke, 26/29 of them were using aspirin. In Group 2 most of the patients 30/48 had both diabetes and hypertension. Group 1 pts more often had post stroke dementia (χ 2 = 7.38, p < 0.01), worse quality of life (χ 2 = 8.12, p < 0.01), and worse functional ability (χ 2 = 5,12, p < 0.05). Among all patients the worst survival had pts with AF, F = 14,88, p < 0.01.
Conclusions Post stroke elderly pts had worse prognosis and more complications if the stroke is consequence of the heart disease, especially AF. All preventive measures should be applied to prevent stroke in CVD pts. Most of all, doctors must start administering more freely anticoagulant treatment according to ESC Guidelines for pts with AF (INR 2–;3), even elderly ones, because this is the most vulnerable population, with high incidence of stroke and bad prognosis. Aspirin didn't show any protective effect in this group.
124 The effect of aspirin on C-reactive protein in hypertension
Myung-A Kim1, Sang-Hyun Kim1, Joo-Hee Zo1, Hong Sook Ko2, Chee Jeong Kim2, Wang Seong Ryu2
1Seoul National University Boramae Hospital
2Chung-Ang University Hospital
Objectives This study was designed to assess the interaction between aspirin and C-reactive protein (CRP) in controlled hypertensive patients.
Background Many studies have confirmed that C-reactive protein (CRP) is an important cardiovascular risk factor. CRP promotes atherosclerosis by inducing production of inflammatory cytokines and promoting tissue factor expression. High level of C-reactive protein (CRP), the most popular inflammatory marker, increases the risk of thrombotic cardiovascular events. Aspirin has the potential to influence CRP release, either by reducing vascular inflammation or by preventing thrombosis. It is generally accepted that aspirin lowers CRP levels without solid evidences. However the clinical significance of this potential interaction has not completely been studied.
Methods Fifty five patients with hypertension were randomly divided into two groups; Aspirin group (n = 28, 100 mg of aspirin) and control group (n = 27). Patients with a CRP level > 10 mg/L were excluded. C-reactive protein level and lipid profiles (total cholesterol, triglyceride, HDL-, and LDL-cholesterol) were measured before and 3 months after therapy.
Results Their mean age was 59.8 +/− 10.0 years old. There were no differences in baseline clinical characteristics between two groups. Low dose aspirin elevated CRP levels (from 0.93 +/− 1.30 to 1.40 +/− 1.76 mg/L, p = 0.018). There were no changes in the control group (from 1.00 +/− 0.13 to 0.92 +/− 0.70 mg/L, p = 0.59). When each group was divided into two subgroups according to median values of baseline CRP levels, CRP levels increased in subgroup with lower baseline CRP levels of the aspirin group (n = 13, from 0.28 + 0.12 to 0.57 + 0.62 mg/L, p = 0.028) and showed the trend to increase in subgroup with higher baseline CRP levels of the aspirin group (n = 15, from 1.49 + 1.57 to 2.12 + 2.10 mg/L, p = 0.13). In the control group, CRP levels increased in subgroup with lower baseline CRP levels (n = 12, from 0.26 + 0.17 to 0.63 + 0.62 mg/L, p = 0.006), however, did not change in higher baseline CRP levels (n = 15, from 1.59 + 1.50 to 1.15 + 0.73 mg/L, p = 0.35).
Conclusions Low dose aspirin failed to decrease CRP levels. The anti-inflammatory mechanism might not play a significant role in the cardioprotective effect of aspirin.
141 Does length of diabetes mellitus impact on in-hospital mortality in diabetic 2 type patients with acute myocardial infarction?
Svetlana Myung-A
Urgent Cardiology Department of City Clinical Hospital No 1, Kiev, Ukraine.
Background The number of patients with diabetes mellitus 2 type (DM) has tendency to increase around the world. The main reasons of death in patients with DM are vascular accident and first of all-acute myocardial infarction (AMI). Despite significant success in AMI treatment the mortality in diabetic patient is still twice-four times higher than that in non diabetic patients. However, how the duration of DM is linked to number of lethal outcomes of in-patient subjects with AMI is scarcely investigated.
Aim To study correlation in-hospital mortality in diabetic patients with AMI and length of diabetes
Methods 227 patients with AMI and DM (mean age 70±8,6 y) were hospitalized and examined during period from 2002 to 2005 in Department of Urgent Cardiology.
Results Among diabetic patients with AMI died 59 patients (26%), 42% was length of DM more then 10 year, 38%-length of DM 5–;10 year, less then 5 year −12% and in patient with first time found DM was 8% died patients. The general number died patients with DM length of diabetes more then 5 year was 80% and risk in hospital mortality in this patient was significant more compared with patients with length DM less then 5 year (OR 0.79, CI 0.61 to 0.84).
Conclusion In patients with AMI and DM length of diabetes associated with risk early mortality. Patients with AMI and DM length of diabetes more then 5 year relative to group with high risk mortality and this group must recommend more intensive therapy.
145 Psychosocial intervention for women coronary patients may enhance effects of pharmacotherapy and reduce mortality
Kristina Orth-Gomér
Karolinska institutet, Stockholm, Sweden
The Stockholm Female Coronary Risk Study has shown that multiple psychosocial stress may increase the risk and worsen the prognosis of coronary disease in women. Stress in family life was more important than job stress, and associated both with depression - and progress of coronary disease. Women with both types of stress had the worst prognosis.
We developed a multiple stress reduction for women coronary patients and monitored effects on coronary morbidity and mortality.
Methods Consecutive Stockholm women patients, 30 to 75 years, hospitalized for an acute coronary event (Acute Myocardial Infarction, CoronaryArtery By-pass Graft or Coronary Angioplasty), were randomized to either usual cardiological care, or usual care with psychosocial intervention.
In an educational psychosocial program, led by a behavioral therapist, the women met in groups of 6 to 8, in 20 half day sessions, over a year. Increasing their knowledge and training their skills to fight stress and care for the heart, the sessions focused on women's multiple sources of stress at work and at home, on coping strategies, on self care and adherence to clinical advice.
Results All women were followed for up to ten years and their all cause mortality assessed. Eight out of 113 women (7%) who received the intervention, died, whereas 25 out of 125 control women (20%) died (p = 0.004). In age controlled life table analyses, the odds of dying for women in the intervention group was 0.35 relative to women in the control group. Pharmacotherapy at baseline did not differ between groups, in the use of beta-blockers, ACE-inhibitors, Ca-channel blockers, anti-thrombotic or hormone replacement therapy. However, an interactive effect with use of statins was suggested. Only one out of 65 women who were on statins and received psychosocial intervention, died (1.5%), whereas 15 out of 70 women, who received none of these therapies (21%) died within ten years.
Conclusion Although mechanisms are not fully known, it is suggested that psychosocial stress can be attenuated, mortality risk reduced and pharmacologic preventative effects enchanced by psychosocial intervention in women with coronary disease.
149 Clinical practice versus prevention guidelines: the importance of heartscore risk charts
A. Pipilis, S. Kaliambakos, C. Xenodochidis, G. Tsakonas, N. Sourlas, K. Mallios
1st Cardiology Clinic, Hygeia Hospital, Athens, Greece
Objectives Cardiovascular risk charts significantly assist clinical decision making for the management of asymptomatic individuals. However, most decisions are made without referring to the risk charts. The aim of our study was to identify the degree of agreement between decisions in usual clinical practice and the proposed management by the Prevention Guidelines of the European Society of Cardiology.
Methods We presented with random order seven cases of asymptomatic individuals at varying level of total cardiovascular risk (10-year Heartscore risk ranging from 1% to 9% as a result of different combinations of age, cholesterol level, blood pressure and smoking habit) to 30 physicians, who in their daily practice deal with primary prevention consultation. These physicians were asked whether they would prescribe hypolipidemic therapy and their answers were compared with the recommended management of the ESC Guidelines using Heartscore data.
Results The mean percentage of agreement was 70%; Disagreement was either due to over- or under-estimation of total risk. In the two extreme cases (one with obviously very low and one with obviously very high risk) the agreement was 100%. However, in the other less obvious cases agreement ranged from 20–;90%. Specifically in cases where cholesterol was 200–;240 mg% the agreement was only 40% with a tendency to ignore other risk factors and make a decision based just on total and LDL cholesterol levels.
Conclusion In cases with obviously very low or very high risk usual clinical practice agrees with guidelines and the use of risk charts may not be necessary. In cases of intermediate risk there is substantial variation in clinical practice with either overestimation of risk and unnecessary drug prescription or underestimation of risk and no prescription of indicated therapy. The use of Heartscore risk charts may provide a significant assistance for a more objective practice of primary prevention.
161 Hierarchical analysis of dietary habits in relation to cardiovascular disease events, in patients with heart failure: a 12-month follow-up
G. Pounis1, D. Panagiotakos1, I. Kotroyiannis2, C. Pitsavos2, L. Papademetriou2, P. Aggelopoulos2, E. Gerodimou2, C. Stefanadis2.
1Department Of Nutrition and Dietetics, Harokopio University of Athens, Athens, Greece.
2First Cardiology Clinic, School of Medicine, University of Athens, Athens, Greece.
Background The role of dietary habits on cardiovascular disease risk is of crucial importance. In this work, we sought to investigate the relationship between dietary habits and the development of fatal or non-fatal cardiac events during a period of 12 months, in patients with heart failure.
Methods From 2005 to 2006, 106 consecutive patients (mean age 65 +/−14 y) with newly-diagnosed systolic heart failure were enrolled in the study. Consumption of various foods and beverages during the last year was assessed using a special food frequency questionnaire. Moreover, several socio-demographic, anthropometric, lifestyle, and bio-clinical factors were also measured. Every 3 months, and for a total period of 12 months after initial examination, all patients were reexamined. Main outcome of interest was death or re-hospitalization due to cardiovascular disease. Discriminant analysis using Fisher's function and lambda of Wilk's were used to hierarchically evaluate various food groups in relation to the outcome.
Results The annual death rate was 16%, while 45% of the patients were hospitalised due to a cardiovascular event. Increased legumes intake (6.4% of total variance explained), followed by reduced cheese (4.1% of total variance), and increased consumption of fish (3.9% of total variance) and cereals (1.3% of total variance) were the most significant dietary factors that discriminated patients with from those without an event. Overall, all 23 food groups or items included in the analysis were accounted for 44% of the total variance of the observed events. From the clinical factors that were taken into account, presence of diabetes (7.9% of total variance explained), followed by hypercholesterolemia (0.6% of total variance explained) and hypertension (0.3% of total variance explained) were the most important discriminating factors for an event.
Conclusion Dietary habits seem to account for a large proportion of an event in patients with chronic heart failure.
164 Effect of a dietary prevention programme on blood pressure levels in a Portuguese primary care setting
S. Contreiras and Pedro Marques-Vidal
Unidade de Nutriçäe e Metabolismo, Instituto de Medicine Molecular, Avenida Professor Egas Moniz, 1649–;028, Lisboa, Portugal
Introduction Hypertension is one of the main risk factors in cardiovascular and brain vascular disease, sensitive to change through nutritional factors.
Objective To evaluate the effect of the promotion of a healthy eating plan in the blood pressure values of hypertense patients.
Methods In the first step of this study we applied a questionnaire that included the evaluation of the clinical, psychosocial and psychosocial and physiological characteristics of the subjects. Furthermore, we evaluate the knowledge and eating habits, smoking habits and physical activity of the same subjects. In addition to these procedures an eating educational programme was implemented, after which we evaluated the blood pressure of the patients in a weekly basis and after one month we proceeded to a new evaluation of the anthropometric parameters, practice of physical activity and main eating changes.
Results In a sample of 21 hypertense subjects, all of them medicated with at least one anti-hypertension drug, most of them presented unbalance values and overweight. From the first analysis of the information and eating habbits of the subjects, several gaps became evident which are incompatible with healthy eating. Most subjects did not have any regular physical activity. After the eating education sessions we observed a significant reduction of blood pressure values in the majority of the subjects, mainly in what concerns systolic pressure. Between the first and the second evaluation the systolic values decreased from an average value of 160 to 151 mmHg (p = 0,048) and after four weeks they decreased to 147 mmHg (p = 0,001). Diastolic pressure decreased from an average value of 83 to 80 mmHg after four weeks. Regarding weight, waist perimeter and physical activity we did not find any significant differences between the first and the second evaluation. Therefore, these items were not considered with any responsibility in the reduction of the observed blood pressure values.
Conclusions From these results we can conclude that before the educational intervention only 5% of the hypertense patients were adequately balanced although all of them were medicated and 70% even multimedicated. The eating education sessions allow a significant blood pressure reduction after 4 weeks without immediate change in weight or the practice of physical activity. These results indicate the strong necessity of the implementation of healthy eating habits in hypertense patients in order to achieve an adequate control of their blood pressure without increasing medication.
169 Correlation among cardiovascular risk scores and new echographic markers of atherosclerosis
R. Campuzano1, A. García-Lledó1, J.L. Moya2, J.P. Tomas2, C. De Pablo2, J. Balaguer1
1Servicio de Cardiología. Hospital Universitario de Guadalajara, Guadalajara, Spain
2Instituto de Enfermedades del Corazón. Hospital Ramón y Cajal, Madrid, Spain
Introduction Cardiovascular risk (CVR) assesment is extremely useful in cardiovascular prevention. Several echographic markers of early atherosclerotic disease can be considered for risk stratification by reflecting functional atherosclerotic changes, such as flow mediated vascular dilation (FMD) and coronary flow reserve (CFR), or anatomic changes as intima-media thickness (IMT) does.
Objectives To explore the correlation among these echographic markers of CVR and validated risk score scales like Framingham, Regicor and Heartscore.
Methods One hundred and six subjects were studied; mean age 59.3 ± 14 years, 61 women (57.5%). CVR was calculated for each patient using Framingham score, Regicor y Heartscore. Doppler-Ultrasound was used to analyse endothelium-dependent FMD in the brachial artery, IMT in the common carotid artery and CFR in the left anterior artery.
Results The mean FMD was 4.83 ± 4.37%, mean IMT 0.84 ± 0.30 mm and mean CFR 2.93 ± 1.10. Mean CVR estimated by Framingham to 10 years was 13.24 ± 9.15, CVR calculated by Regicor was 5.67 ± 3.49 and with Heartscore de 2.25 ± 2.12. Patients with cardiovascular risk factors had significantly impaired FMD, greater IMT and lower CFR.
There was a stronger correlation among IMT, the Framingham risk score and Regicor, both with r = 0.655, p = 0.000, and weaker with Heartscore (r = 0.521, p = 0.000). Functional markers correlated only weakily to Regicor and Framingham.
Conclusions Scores in use are related with anatomical changes of atheroclerosis but not with early functional damage. Framingam and Regicor scores are the best predictors of anatomical atherosclerotic damage in our population.
172 The effect of a life style change and stress management program on the promotion of cardiovascular health in non graduate students
C. Figueroa1, L. Alcocer2, B. Ramos1, B. Dominguez1, G. Rodriguez1
1National Autonomous University of Mexico, Mexico
2General Hospital of Mexico, Mexico
Objective To promote cardiovascular health behaviors to prevent and/or modify measures of cardiovascular risk in college students using a life style behavior change and stress management program.
Method The program consisted in 3 phases: pretest, intervention, and posttest. It included the following components: Conceptualization of the cardiovascular risk; strategies for the cardiovascular risk management (modification of life style); strategies for the stress management (conceptualization of stress, symptoms and sources of stress, stress disease relation, diaphragmatic respiration, and progressive muscular relaxation)
Results Psychosocial factors were correlated in 50 psychology students aged 17 to 30 years in the National Autonomous University of Mexico. The factors studied were Life Style Questionnaire, Stress Symptoms Inventory, Stress Sources Inventory, State Trait Anger Expression Inventory, General Information (marital status, jobs, etc), medical history, baseline systolic blood pressure, body mass index (BMI), abdominal obesity, and level of physical activity. The results showed both statistical and clinical significance in these variables.
Conclusions Young adults who react to psychological stress with a large blood pressure response are at risk of developing hypertension as they approach midlife. In the last 10 years the evidence has increased that also the psychosocial factors influence in the development of a cardiovascular disease. However, the cardiovascular health area, in terms of smoke control, diet, exercise, stress management, among others relevant healthy habits, is far from optimum, suggesting the need of continue working in the cardiovascular prevention/promotion area.
173 Psychosocial stress and basal blood pressure levels, not a family history of hypertension, determine sympathetic nervous system hyperresponsivity and recovery to stress
C. Figueroa1, L. Alcocer2, B. Ramos1, B. Dominguez1, G. Rodriguez1
1National Autonomous University of Mexico, Mexico
2General Hospital of Mexico, Mexico
Objective To determine the association between cardiovascular reactivity and recovery to stress with hypertension risk factors in university students with and without a family history of hypertension.
Method 110 normotensive undergraduates students were assigned to: Group 1 (n = 52), with a positive family history of hypertension, and Group 2 (n = 58), with a negative family history of hypertension. The following were carried out and administered: a) a Clinical History to determine family history of hypertension, sex, age, height, weight, body mass index and hypertension risk factors based on JNC7; b) a Type A behavior inventory; c) a psychophysiological stress profile to determine cardiovascular reactivity and recovery.
Results A multiple linear regression analysis showed that the extent of cardiovascular reactivity and recovery to stress was related to the following risk factors: sedentary lifestyle (B = 1.156, sig. = 0.088), elevated ingestion of fats (B = 0.846, sig. = 0.115), and those related to stress (stressful occupation: B = 1.935, sig. = 0.007; stressful personality: B = 1.163, sig. = 0.106); there was also a relationship to initial basal values both for diastolic blood pressure (B = 0.273, sig. = 0.012) and for heart rate (B = 0.392, sig. = 0.038); there was no association to the variable of a family history of hypertension (B = −0.952, sig. = 0.439). As for cardiovascular recovery, it was found to be related to initial basal values for systolic blood pressure (B = 0.314, sig. = 0.03), diastolic blood pressure (B = 0.459, sig. = 0.01), and heart rate (B = 0.498, sig. = 0.01); there was no relation to the variable of a family history of hypertension (B = 0.970, sig. = 0.240).
Conclusion The extent of cardiovascular reactivity and recovery to stress in blood pressure measurements is determined by the initial basal values for blood pressure and other cardiovascular risk factors, like psychosocial stress. The relationship between the family history of hypertension and cardiovascular reactivity and recovery was not proved.
176 From expensive technology to poor prevention
Irurita M1, Irurita J1, Martínez de Saavedra MT1, López y Juan L1, Déniz C1, Saavedra JM3, Culebras C2, Molina I1, López y Juan JA4, Belón JA1, Chirino R5, Sánchez F1
1Dr. Negrín Hospital, Las Palmas de Gran Canaria, Spain
2Insular Hospital, Las Palmas de Gran Canaria, Spain
3Sta. Catalina Hospital, Las Palmas de Gran Canaria, Spain
4Primary Care Lugo, SERGAS, Lugo, Spain
5Las Palmas de Gran Canaria University, Las Palmas de Gran Canaria, Spain
Cardiovascular mortality trends increase fast, despite powerful drugs, sophisticated invasive and costly diagnostic and therapeutic procedures, efforts outspreading updated guidelines or ambitious preventive programs.
Objectives and methods To analyze prevention targets we studied 696 patients with premature acute coronary syndrome (ACS), with an average of 6 years follow-up; 18% were females. The mean age was 45 years (43.7 in males and 49.5 in females; p < 0.001).
Results Despite their youth, our patients showed a very high prevalence of risk factors: diabetes 30%, hypertension 55%, dyslipidemia 75%, metabolic syndrome 46%, smokiers 78% and family history of premature coronary heart disease 35%. Only 19 patients lacked any classical risk factor. A total of 51% had multiple vessel disease (MVD) and 29% experienced recurrent events. Coronary angiography was performed in 92%, revascularization in 63% (89% underwent PCI and 15% CABG). Revascularization showed a significant gender bias (52% females and 67% males; p < 0.004). Patients received multiple drug combinations including anti-platelet (96%), beta-blockers (78%), ACE inhibitors or ARBs (47%), calcium channel blockers (28%) and lipid lowering (83%). Up to 30% of the smokers were unable to quit following the first ACS. Lipid lowering follow-up was deficient or C-LDL levels were over 100 mg/dl in diabetics (80%), current smokers (74%), multivessel disease (53%), PCI patients (74%) and recurrent ACS (61%). Moreover only 9% of diabetics, 8% of multivessel disease, 7% of PCI and 10% of recurrent ACS achieved TNT targets (C-LDL under 70 mg/dl). Revascularized patients had higher recurrence rates compared with only medically treated (34% vs. 21%; p < 0.003). The risk of recurrence was twofold in revascularized patients with LDL over 100 mg/dl (16% vs. 33%; p < 0.000). In current smokers multivessel disease explains 79% of recurrence (p < 0.000: OR: 1.12–;8.89).
Conclusions Our series shows that during hospitalizations and office visits, patients do not learn enough about the importance of preventative strategies and are unaware of the value of secondary prevention. Despite expensive technology or repeated interventions for acute coronary syndromes, prevention in young patients is still deficient and the gap between the guidelines and real life situations of modifiable factors, such as smoking or lipid lowering is huge. We are being blinded by technology and seem unable to complete revascularization procedures with effective prevention strategies. Poor prevention may contribute to explain why the Canary Islands remain as the Spanish community with highest coronary mortality. Educating or modifying human conduct is almost as difficult as quantifying its impact.
177 Triglyceride to HDL ratio and C-reactive protein levels as predictors of the metabolic syndrome in a primary prevention cardiology clinic
Mónica Acevedo, Veronica Krämer, Lorena Orellana, Marcelo Fernandez, Jose A. Rodriguez, Gastón Chamorro, Ramón Corbalán. Pontificia Universidad Católica de Chile, Santiago, Chile.
Background Some of the most important features of the metabolic syndrome (MetSyn) are both insulin resistance and atherogenic dyslipidemia. Triglyceride to HDL ratio has proven to be a good predictor of the presence of small and dense LDL and insulin resistance. C-reactive protein levels predict MetSyn. We sought to determine the level of prediction of TG to HDL ratio alone and with CRP in Chilean adults.
Methods Prospective study in subjects without history of CHD. In all of them, we evaluated classical risk factors. BMI, waist, fasting lipid profile, Glycemia, CRP levels, and systolic and diastolic blood pressure. ATP III definition of the MetSyn was used.
Results We studied 1892 subjects (1232 men), mean age 54 ± 13 yo; 35% had HTN, 6% were diabetics and 68% had high cholesterol levels. Eighteen percent had the MetSyn. Subjects in the highest tertile for TG to HDL ratio had a more adverse lipid profile, glycemia and systolic blood pressure, as well as higher CRP levels (table). Of subjects with CRP > 2 mg/L, 23% had the MetSyn versus 12% in those with CRP < 2 (OR = 2.08, p < .0001). Of those individuals with a TG/HDL ratio > 3.5, 46% had the SMET versus 8% in those with TG/HDL < 3.5 (OR = 9.7, p < .0001). For both, TG/HDL > 3.5 CRP > 2 mg/L, 29% had the MetSyn versus 3% of those with TG/HDL < 3.5 and CRP < 2 (OR = 12.7, p < .0001).
Conclusions This study demonstrates the usefulness of TG/HDL ratio or CRP levels as good predictors of the MetSyn. When both determinants were present, the level of prediction of the syndrome was the best.
Risk Factors by Triglyceride to HDL ratio Tertiles
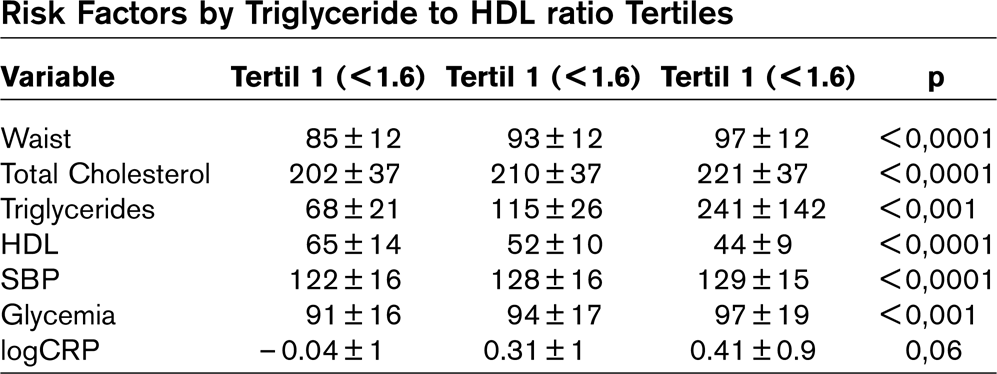
178 Comparison among subclinical atherosclerosis, C-reactive protein levels and classical risk factors in obese and non obese children in Chile
Pilar Arnaiz, Mónica Acevedo, Salesa Barja, Ximena Berríos, Beatriz Guzmán, Claudia Bambs, Myriam Ferreiro, Jacqueline Carvajal, Berta Cassis
Departaments of “Enfermedades Cardiovasculares, Pediatría y Salud Pública, Pontificia Universidad Católica de Chile, Santiago.
Background Atherosclerosis is an inflammatory and progressive disease that begins in childhood and develops on adulthood depending on the burden of risk factors. Non-invasive techniques and novel risk factors are now available to assess subclinical atherosclerosis.
Objective We sought to determine classical, C-reactive protein levels (CRP), and brachial arterial endothelial function and carotid intima-media thickness (IMT) in both non-obese and obese children.
Methods We prospectively studied 57 non-obese (BMI ≤ Pc 95) children randomly selected from 3 neighborhoods in Santiago (Chile) and 26 obese children (BMI ≥ Pc 95) coming from a pediatric nutrition clinic. We determined in all of them fasting lipids and glycemia, CRP levels, brachial artery flow-mediated dilation (FMD) and carotid IMT.
Results 50% were girls and 41% prepuberals. Comparisons between both groups are shown in the table.
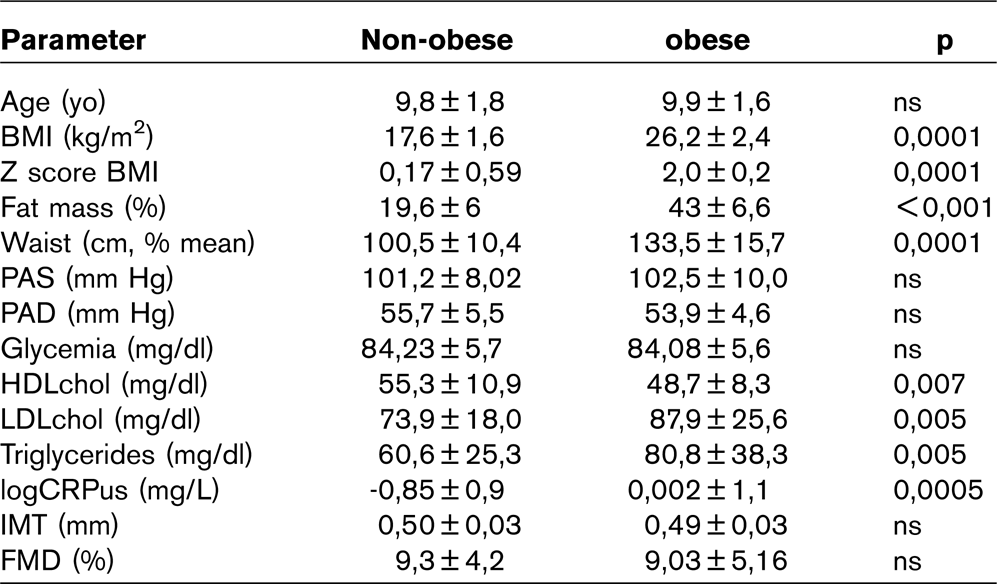
Conclusions Obese children had a significant burden of classic and novel risk factors, as well as abdominal obesity. However, no statistically significant differences were demonstrated between both groups of children regarding early atherosclerosis. This study underlines the importance of knowing at what age does early atherosclerosis begins in children, in order to intervene before the start of the disease.
179 Prevalence of metabolic syndrome in elderly patients with acute ischemic stroke
C.L. Calin1, A. Caltea1, C. Caltea1, C. Sinescu1
1Bagdasar-Arseni Emergency Hospital, Bucharest, Romania
Objective The aim of this study was to identify prevalence of metabolic syndrome (MS) in elderly patients (pts) who present an acute ischemic stroke (AIS).
Method This was a retrospective study. We analyzed 237 elderly pts (age ≥ 65 years) (group1) hospitalized in the last 4 year for acute cardiac disease complicated with AIS. They were compared with 276 elderly pts (group 2) without positive history for cardiac or cardiovascular disease - AIS was proved by CT-scan and MS was defined according with actual guidelines. The distribution based by gender was similarly in the both groups.
Results Prevalence of MS was significantly higher in group 1 vs group 2 (43.6% vs 21.2%, p < 0.001). The atherogenic profile was more alterated in group 1 than in group 2: LDL-cholesterol > 130 mg/dl: 41.3% vs 20.6%, p < 0.05; HDL-cholesterol: females < 50 mg/dl: 45.3% vs 23.8%, p < 0.05; TGL > 150 mg/dl: 40.2% vs 19.3%, p < 0.05. Pts from group 1 had a higher values of plasma uric acid (7.2 ± 2.4 mg/dl vs 5.7 ± 1.4 mg/dl). Incidence of MS in pts with AIS increased with BMI: 23.4% for normal weight; 33.4% for overweight and 56.8% for obese.
Conclusions The prevalence of MS is significantly higher in elderly pts with AIS. It is in directly relationship with atherogenic profile, obesity and the higher value of plasma uric acid.
180 Smoking habits and left ventricular thickness in untreated hypertensives
C.L. Calin1, R. Ciomag1, A. Popa1, D. Mincu1, C. Sinescu1
Bagdasar-Arseni Emergency Hospital, Bucharest, Romania
Objective Started from the already known fact that smoking is associated with the profiles of atherosclerosis, we studied how smoking affect the thickness of LV wall.
Method 256 pts with untreated arterial hypertension (UAH) divided into two groups: group 1-smokes 96 pts (68 males) and group 2-nonsmokers 160 pts (72 males). Mean age was 56 ± 9 years. Lipid profile, complete HLG and 2D echocardiography were registrated for all pts.
Results The thickness of LV walls (interventricular septum-IVS and LV posterior wall-LVP) in group 1 was significantly higher than in group 2. IVS: 11 ± 1.5 mm vs 10.6 ± 1.2 mm, p < 0.01 and LVP: 10.5 ± 1.5 mm vs 9.6 ± 1.2 mm, p < 0.05. No significant difference were observed in blood pressure (BP) between group 1 and group 2. Systolic BP was: 159 ± 16 mmHg vs 163 ± 18 mmHg; Diastolic BP was: 99 ± 8 mmHg vs 102 ± 10 mmHg. Group 2 had significantly higher HDL-cholesterol than group 1 (50 ± 13 mg/dl vs 39 ± 3 mg/dl, p < 0.05). No difference was observed for other profile lipids components. Group 1 had significantly higher haematocrit (Ht) than group 2.
Conclusions Smoking is associated with increased LVT independently of BP level in UAH.
185 Risk factors for cardiovascular diseases in field and office work employees of an onshore oil and gas company, Sindh, Pakistan
K. Zakir1, I. Javed2, Q. Riaz1
1Aga Khan University Hospital, Karachi, Pakistan
2Dow University of Health Sciences, Karachi, Pakistan
Introduction Significant over weight and obesity among oil and gas employees has been linked to unhealthy diet and lack of physical activities. Sedentary life style and unhealthy eating habits are major contributors of developing cardiovascular diseases.
Objective Purpose of this study was to assess the effect of lifestyle on the health of field workers and office workers in regard to risk factors of cardiovascular diseases at a gas producing plant in rural Sindh, Pakistan.
Method This cross sectional study was conducted from Feb-March 2005; among male field and office work employees of an-onshore oil and gas company located 450 kms north-east of Karachi in Sindh, Pakistan. Employees who had been working at the same site for more than two years were included in the study. Office employees were mostly involved in automated tasks and were physically less active. The field employees were mostly involved in moderate to heavy work, hence, were physically more active than the other group.
Results Total 150 employees (112 office workers and 38 field workers) of the company were included in the study. The mean age (± SD) of office work employees and field work employees was 39.66 ± 8.2 years and 32.51 ± 8.8 years, respectively. Univariate analysis showed that total high serum cholesterol level (> 200 mg/dl), OR 5.5 [95% CI 2.0 –; 15.1] and age > 40 yrs, OR 3.86 [1.57 –; 9.47] were the significant risk factors among office workers as compared to field workers. Multivariable analysis showed that age > 40 yrs, adjusted OR 2.80 [1.10 –; 7.14] and high cholesterol levels, 4.11 [1.45 –; 11.61] were important risk factors in our study population.
Conclusion Work place health promotion is much needed to improve health behavior amongst employees for the long term benefit of the individuals and the organizations for whom they work.
186 Smoking and prognosis of patient with ischemic heart disease
Ibatov A.D.
Moscow Medical Academy at I.M. Sechenov, Moscow, Russia
Purpose To study influence of smoking on prognosis of patients with ischemic heart disease (IHD).
Materials and methods 277 patients with IHD (192 men and 85 women) from 36 till 67 years (average age 56.9 + 0.5 years) were examined. All patients had angina pectoris of 11–;1 V functional class. The first group included 136 smoking patients (the average age has made 54.7 + 0.8). The control group was 141 not smoking patients (average age-56.8 + 0.9; p > 0.05). Patients were observed during 24.7 + 0.38 months. The follow end points were taken: myocardial infarction (fatal and nonfatal), unstable angina pectoris, surgical methods of myocardial revascularization (coronary artery bypass surgery and percutaneous transluminal coronary angioplasty). Also two combined points were analysed. First included all nonfatal cardiovascular events and second-all cardiovascular events (including death from IHD). Kaplan-Meier method was used to study influence of different factors on cardiovascular events. Statistical significant differences were determined by Cox's F-Test.
Results The groups did not differ on age, duration IHD, function class of angina pectoris, therapy. 59 events were registered: 9 cases of myocardial infarction (4 cases of fatal and 5 cases of nonfatal), 19 cases of unstable angina pectoris, 20 cases of surgical myocardial revascularization, 9 cases of death, connected with cardiovascular pathology, 6 cases of death not connected with cardiovascular pathology, 15 cases of death from all causes (total mortality). There were 44 nonfatal cardiovascular events and 59 cases of all cardiovascular events. Smoking patients had of increasing mortality, connected with cardiovascular pathology (p = 0.060) in comparison with nonsmoking patients. Smoking patients had more myocardial infarctions (p = 0.0094), cases of unstable angina pectoris (p = 0.021), cases of surgical myocardial revascularization (p = 0.0017), nonfatal cardiovascular events (p = 0.043) and all cardiovascular events (p = 0.025) versus nonsmoking patients.
Conclusions Smoking worsens the prognosis of patients with ischemic heart disease and increases number of cardiac events. This influence appears, both among the men, and among the women.
196 The effect of moxonidine on C-reactive protein and urinary excretion rate in hypertensive patients
Ilgar Alizade, Nigar Karayeva
Hospital of Ministry of Internal Affairs, Baku, Azerbaijan
Recent studies have shown relationship between C-reactive protein and urinary albumin excretion rate (UAER) in essential hypertension (EH).
The aim of our study was to estimate the effect of moxonidine on high sensitivity C-reactive protein (hs-CRP) levels in conjunction with UAER measurement in patients with EH.
Methods Fifteen newly diagnosed untreated patients with stage II essential hypertension (36men, aged 33.8 ± 7.3 years. UAER was determined in three non-consecutive 24h urine samples. Moreover, venous blood samples were drawn for estimation of lipid profile and hs-CRP, according to established techniques. Moxonidine was given alone in a daily dose 0.4–;0.8mg for 8 weeks.
Results Body mass index (BMI) was 28,8 ± 3.9 kg/m2, total cholesterol was 238 ± 54 mg/dl, triglycerides were 141 ± 75 mg/dl, low-density lipoprotein cholesterol was 161 ± 37 mg/dl and plasma levels of hs-CRP were 2.26 ± 1.8 mg/l. According to the echocardiographic examination, left ventricular mass index (LVMI) was 106.6 ± 24 g/m2. In the entire population, hs-CRP was associated with BMI (r = 0.36, p < 0.01) and UAER (r = 0.52, p < 0.001). UAER was correlated with office systolic blood pressure (BP) (r = 0.28, p < 0.05) and LVMI (r = 0.32, p < 0.05).
It was revealed that the use of moxonidine led to the lowering of systolic BP (from 158 ± 6.6 to 134.4 ± 3.0 mmHg; p < 0.05) and diastolic BP (from 103.8 ± 4.9 to 88.2 ± 6.1 mmHG; p < 0.05). Moreover, LVMI was decreased by 28%. These patients showed sifnificantly decrease of hs-CRP (from 2.28 ± 1.8 to 1.03 ± 0.1 mg/dl; p < 0.001) and UAER (from 36.8 ± 6.2 to 19.1 ± 9.0 mg/24h; p < 0.05).
Results These data suggest that moxonidine therapy showed significant reduction of hs-CRP levels and associated reduction of UAER. This beneficial effect of moxonidine ttherapy may contribute better cardiovascular risk prevention in EH.
197 The role of echocardiographic myocardial performance index and pulmonary venous flow in detection of early stages of left ventricular diastolic dysfunction in young asymptomatic patients with long-lasting diabetes mellitus type 1
Katarzyna Kurnicka, Barbara Lichodziejewska, Katarzyna Grudzka, Michala Ciurzyíski, Danuta Liszewska-Pfejfer
Department of Internal Medicine and Cardiology, Medical University of Warsaw, Poland
Objective Left ventricular (LV) diastolic dysfunction (LVDD) usually precedes systolic dysfunction and may contribute to development of symptomatic heart failure in diabetics. Myocardial performance index (MPI) reflects global LV function independent of age, heart rate, blood pressure and LV geometry. Pulmonary venous flow (PVF) complements the mitral valve flow (MVF) in the evaluation of LV diastolic function (LVDF).
Aim To assess echocardiographic parameters reflecting diastolic and global LV function and define their usefulness in detection of preclinical LVDD in young patients with diabetes mellitus type 1 (DM1).
Materials and method The study group (DM) formed 60 DM1 patients (30 M, mean: age 26.8 yrs, DM1 duration 14.4 yrs, HbA1c 9,8%) with total cholesterol < 200 mg/dl, without symptoms of cardiovascular disease. As control group (C) served 45 healthy persons (22 M, mean age 27.5 yrs). In MVF: the maximal velocity (Vmax) of early and late phase (E, A), E/A ratio, deceleration time (DT) and isovolumetric relaxation time (IRT) were measured. In PVF: Vmax of systolic and diastolic flow (S, D) and S/D ratio were evaluated. The MPI was defined as the sum of isovolumetric contraction time (ICT) and IRT divided by LV ejection time, with normal values: 0.39 ± 0.05.
Results Body mass index, heart rate, blood pressure, ejection fraction, LV mass and diameter did not differ between groups. In MVF: DT was higher (169.6 ± 17.8 vs 157.6 ± 16.7 ms; p < 0,001) and E/A was lower (1.36 ± 0,3 vs 1.50 ± 0.3; p = 0,03) in DM than in C. These results tend to show the impairment of LV diastolic function, but they remain normal for this age group. In PVF the S/D was higher (1.1 ± 0.2 vs 0.9 ± 0.2; p < 0,0001) in DM than in C. The S/D > 1, abnormal for this age group and typical for LVDD was observed in 62% of diabetics. MPI was also abnormally higher in DM than in C (0.53 ± 0.07 vs 0.37 ± 0.05; p < 0,001). No correlation between ECHO parameters and DM1 duration was found.
Conclusions 1. Abnormal MPI indicates global LV dysfunction and changes of PVF suggest impaired LV relaxation (when MVF pattern remains normal); both confirm negative influence of DM on the heart function. 2. Conventional doppler parameters are sensitive markers of early left ventricular diastolic dysfunction, helpful in screening and prevention of heart failure development in young diabetics.
198 Clinical predictors of carotid intima-media thickness
A. Timoteo1, A. Galrinho1, F. Miranda1,
1Cardiology Department, Santa Marta Hospital, Lisbon, Portugal
Introduction Carotid intima-media thickness (IMT) is a manifestation of peripheral cardio-vascular disease, associated with other localizations of atherosclerotic disease, sharing the same risk factors with other manifestations of atherosclerotic disease.
Objectives To evaluate in a population of patients submitted to invasive tests, the correlation between IMT and several demographic and laboratorial variables and median IMT according to the usual risk factors.
Methods In a population of 867 patients submitted to an invasive cardiac test, an ultrasound exam of the carotid arteries was performed, with the measurement of carotid IMT (left and right), and the highest value was the value considered for analysis. Pearson's correlation was done for carotid IMT with the following variables: age, abdominal circumference, body mass index and laboratorial variables (fasting blood glucose, serum creatinine, total cholesterol, HDL-cholesterol, LDL-cholesterol, triglycerides, glicosilated haemoglobin, blood insulin, HOMA index). We compare mean IMT in patients with and without each classical risk factor for coronary artery disease (hypertension, hyperlipidemia, smoking, diabetes and male gender).
Results Mean age of the patients was 64 ± 12 years, 25% male, 37% with hypertension, 4% smokers, 11% diabetics e 31% with hyperlipidemia. Carotid IMT only correlated with age (r = 0.24, p < 0.001) and blood creatinine (r = 0.14, p = 0.005), however with low levels of correlation. There was no correlation with the other variables analysed. Calculating mean IMT for each cardiovascular risk factor, only male gender (0.96 ± 0.39 vs. 0.87 ± 0.34 mm in female, p = 0.012) and hypertensive patients (0.96 ± 0.38 vs. 0.76 ± 0.20 mm in non-hypertensive patients, p < 0.001) had a significantly different IMT.
Conclusions Carotid IMT does not correlate with the most frequently mentioned anthropomorphic and laboratorial cardiovascular risk factors, with the exception of age and blood creatinine, however with a low level of correlation. Nonetheless, in male patients and in patients with hypertension, IMT was significantly higher.
199 Is NT-pro-BNP a predictor of one-year mortality in patients with stable angina?
A. Timoteo1, F. Miranda1,
1Cardiology Department, Santa Marta Hospital, Lisbon, Portugal
Introduction Left ventricular function is a prognostic marker in patients with stable angina. NT-pro-BNP is a marker of left ventricular function, so, theoretically, it can influence prognosis in those patients.
Objectives To evaluate in a population of patients, admitted for coronary angiography because of angina and/or positive non-invasive tests for myocardial ischemia, if NT-pro-BNP can predict one-year mortality.
Methods We analyse 754 patients admitted electively for coronary angiography due to coronary artery disease suspicion. The one-year mortality predictors (demographic, risk factors for coronary disease and NT-pro-BNP) were evaluated by univariate and multivariate logistic regression analysis.
Results Mean age was 65 ± 10 years, 65% males, 91% with hypertension, 90% with hyperlipidemia, 16% smokers and 29% diabetics. In 63% we detected significant coronary artery disease (lesions ≥ 70%). In the follow-up (one year), 20 patients died. The predictors of death in the follow-up were age (OR 1.06, 95% CI 1.0–;1.11, p = 0.04), the presence of coronary artery disease (OR 3.44, 95% CI 1.0 –; 11.83, p = 0.04) and NT-pro-BNP (OR 1,0, 95% CI 1.0–;1.0, p = 0.002). By ROC curve analysis, the best cut-off value of NT-pro-BNP to predict death was 76,8 pg/ml (AUC 0.76, 95% CI 0.66–;0.86, p < 0.001, with a sensibility of 100% and specificity of 24%). By multivariate analysis, NT-pro-BNP was the only independent predictor of death (OR 1.0, 95% CI 1.0–;1.0, p = 0.008).
Conclusions NT-pro-BNP can predict one-year mortality, independently of patient age and coronary disease. NT-pro-BNP adds prognostic information to the usual predictors.
200 Are the anthropomorphic variables predictors of short- and medium-term mortality in patients with stable angina?
A. Timoteo1, J. Feliciano1,
1Cardiology Department, Santa Marta Hospital, Lisbon, Portugal
Introduction Weight, abdominal circumference (AC) and body mass index (BMI) are risk factors for atherosclerotic disease and diabetes. Their prognostic impact in patients with stable angina is debatable.
Objectives To evaluate in a population of patients admitted electively for coronary angiography for suspicion of coronary artery disease because of angina and/or myocardial ischemia by non-invasive tests, the impact of AC, BMI and the presence of metabolic syndrome (MS) (by the NCEP-ATP III actualization), a variable strictly related with anthropomorphic parameters, for the occurrence of death at one-year follow-up.
Methods We analysed 790 consecutive patients admitted electively for coronary angiography, with a mean age of 65 ± 10 years, 66% males, 91% with hypertension, 90% with hyperlipidemia, 16% smokers, 29% diabetics and 34% with MS. Significant coronary artery disease (lesions ≥ 70%) was detected in 63% of patients. Univariate and multivariate logistic regression analysis was performed to detect one-year mortality predictors.
Results The potential predictors of death by univariate analysis were age (OR 1.06, 95% CI 1.0–;1.13, p = 0.04), BMI (OR 0.93, 95% CI 0.86–;1.01 –; in this case protective, p = 0.08) and the presence of coronary artery disease (OR 2.77, 95% CI 0.79–;9.73, p = 0.097). Neither AC (OR 0.98, 95% CI 0.94–;1.02) or MS (OR 0.81, 95% CI 0.28–;2.32) were predictors for mortality. However, after correction for age and the presence of coronary artery disease, BMI no longer predicted mortality (OR 0.95, 95% CI 0.88–;1.03, p = NS).
Conclusions Anthropomorphic variables and related variables, as MS, are not prognostic predictors in patients with stable angina, reinforcing the debate related with these variables. They shouldn't be used as a tool for prognostic evaluation of patients with stable angina.
202 Predictors for the presence of significant coronary artery disease in patients with stable angina
A. Timoteo1, R. Ramos1, J. Azeitona1, J. Feliciano1, M. Fernandes1, R. Ferreira1
1Cardiology Department, Santa Marta Hospital, Lisbon, Portugal
Introduction Anthropomorphic variable, beyond classical risk factors, have been more studied as risk factors for atherosclerotic disease and diabetes. However, its importance in coronary artery disease is still debated.
Objectives To evaluate a population of patients admitted electively for coronary angiography because of stable angina, the predictors for significant coronary artery disease.
Methods We analysed 1268 consecutive patients admitted electively for coronary angiography for suspicion of coronary artery disease based in the presence of angina and/or presence of myocardial ischemia by non-invasive tests. We detected significant coronary artery disease (lesions ≥ 70%) in 64% of patients. Univariate and multivariate logistic regression analysis was done to detect the predictors of coronary artery disease.
Results Mean age was 65 ± 10 years, 65% male. In this population, 90% had hypertension, 13% were smokers, 87% had hyperlipidemia, 30% diabetics and 25% had metabolic syndrome (MS) (by the actualized NCEP-ATP III definition). The predictors of coronary artery disease by univariate analysis were all the classical risk factors. For anthropomorphic variables (abdominal circumference, body mass index-BMI) and MS, only BMI could predict coronary disease (OR 0.97, 95% CI 0.95–;0.99 –; as a protective factor, p < 0.001). By multivariate analysis, all the classical risk factors remained as independent predictors for coronary artery disease, as well as BMI (OR 0.95, 95% CI 0.93–;0.97, p < 0.001). ROC curve analysis detected the best cut-off value for BMI to predict the presence of coronary artery disease: 40.3 Kg/m2 (AUC 0.44, 95% CI 0.41–;0.47, p < 0.001), with a sensibility of 84% and specificity of only 17%.
Conclusions BMI is the best anthropomorphic predictor for the presence of significant coronary artery disease in patients with stable angina, with a paradoxical effect. However the adequate cut-off value has higher sensibility but low specificity. This fact can contribute for the debate about the value of abdominal circumference and related variables, particularly MS, as a risk factor for coronary artery disease. BMI should be more emphasised and should be analysed when we evaluate the probability of coronary artery disease and in the selection of patients for coronary angiography.
218 Review of metabolic control and cardiovascular risk in 41 familial hypercholesterolemia patients
I. de la Puerta1, G. Piíol-Ripoll2, J. Escota1, A. Casasnovas3, A. del Río1
1Cardiology Division, Clinical University Hospital. Zaragoza.
2Neurology Division, Clinical University Hospital. Zaragoza.
3Cardiology Division, Miguel Servet Hospital. Zaragoza.
Objective Familial Hypercholesterolemia (FH) is an autosomal dominant genetic disorder due to a Low Density Lipoprotein Cholesterol (LDLc) receptor mutation. It is characterized by very high plasma LDLc levels and high risk of premature atherosclerosis, mainly coronary heart disease.
The aim of our study has been to revise the metabolic control, prescribed lipid treatment, healthy habits and future cardiovascular risk in FH patients.
Methods We performed standardized interviews to HF diagnosed patients (Lipochip genetic test) in Lipid Unit of Clinical Hospital of Zaragoza. We assessed age and sex; smoking, absence of physical activity, unhealthy diet and obesity; hypertension; Diabetes Mellitus (DM); and plasma levels of total cholesterol (TC), LDLc, High Density Lipoprotein Cholesterol (HDLc) and Triglicerides (TG). We analysed the fulfilment of the National Cholesterol Education Program objectives and the 10-years cardiovascular risk according to Civeira et. al. criteria: age > 30 years in men and > 45 years in women, smoking, LDLc > 330 mg/dl, HDLc < 40 mg/dl, Blood pressure > 140/90 mmHg, DM, Lipoprotein (a) and family history if premature coronary disease, stratifying patients in low, moderate and high risk if no factors, one factor and two or more than two factors were found respectively.
Results
Middle age: 38 years old. No sex statistical differences.
We found absence of physical activity in 41% patients, current smoking in 33.3% and high percentage of healthy diet. Thirteen percent of patients were in treatment with estanols and sterols, 82.9% with statins and 24.3% with Ezetimibe.
Thirty percent of men and women had an abdominal perimeter > 102cm and > 88cm respectively. BMI index was < 25 Kg/m2 in 40.7%, between 25–;30 Kg/m2 in 51.8% and > 30 Kg/m2 in 7%.
Twenty seven percent of patients had high blood pressure and 90% of them were diagnosed in our Unit.
Only one patient was diabetic.
TC was > 200 mg/dl in 77.5% of patients, LDLc > 100 mg/dl in 97.5%, HDLc < 40 mg/dl in 15% and TG > 150 mg/dl in 17.5%.
Civeira et. al. cardiovascular objectives are not achieved by 40.5% and 38.8% of men and women respectively. Ten years cardiovascular risk was high, moderate and low in 58%, 21% and 21% of men and 11%, 50% and 39% of women respectively.
Conclusions We conclude that this group of patients, despite of being young, has an inadequate lifestyle, metabolic control and a high 10-years cardiovascular risk. We emphasise the need of Lipid Units to improve primary prevention of HF patients.
237 Adherence to a healthful life attenuates lipid parameters among a healthy Italian population
F. Sofi1, A.M. Gori1, F. Cesari1, A. Capalbo1, G. Innocenti2, C. Surrenti2, A. Casini2, R. Abbate1, G.F. Gensini1,3.
1Department of Medical and Surgical Critical Care, Thrombosis Centre, University of Florence, Italy. 2Department of Clinical Pathophysiology, Unit of Clinical Nutrition, University of Florence, Italy. 3Fondazione Don Carlo Gnocchi, Onlus IRCCS, Impruneta, Firenze. Centro Interdipartimentale di Ricerca per la Valorizzazione degli Alimenti (CeRA), Università degli Studi di Firenze.
Objectives During the last 5 years, an increasing body of evidence on the association between adherence to mediterranean diet (MD), calculated through specific diet-scores, and health status have been accumulated, but limited data regarding the association between MD score and biomarkers are available. Similarly, many reports demonstrated a significant protection versus chronic diseases for a global healthy lifestyle pattern which includes not only dietary habits but also physical activity and abstinence from smoking habit, whereas few data regarding the influence of a healthy lifestyle pattern on circulating biomarkers are present. On the frame of an epidemiologic study conducted in Florence, Italy between 2002 and 2004 we evaluated the association between 2 different scores (a score of adherence to MD and a score of adherence to a healthful life (HL) which includes abstinence from smoking and a moderate-to-high physical activity) and some circulating parameters linked to chronic diseases.
Methods Dietary habits, anthropometric and biochemical profiles were studied in 932 individuals (365 M; 567 F) with a median age of 47.5 years.
Results Subjects who reported a greater adherence to MD were found to be more frequently males, married and over 45 years. A general linear model, by dividing the study population into quartiles of scores, was performed. After adjustment for age, gender, educational status, body mass index, and total energy intake we observed no influence of adherence to MD on circulating levels of biomarkers. On the other hand, as HL score is concerned, an inverse association between circulating levels of lipid parameters, namely total cholesterol, LDL-cholesterol and triglycerides and higher score of adherence to a healthy life, was reported. In addition, a significant difference between the highest and the lowest quartile of HL score for homocysteine plasma levels was observed (p = 0.04).
Conclusions A high adherence to a healthful life, which includes not only a high adherence to MD but also to lifestyle factors (i.e. smoking habit and physical activity during the leisure time), is able to lower lipid parameters and homocysteine in a clinically healthy Italian population.
239 Fish intake and LPA 93C>T polymorphism: gene-environment interaction in modulating lipoprotein (a) concentrations
F. Sofi1, C. Fatini1, E. Sticchi1, M. Lenti1, A.M. Gori1, B. Giusti1, A. Casini2, R. Abbate1, G.F. Gensini1,3.
1Department of Medical and Surgical Critical Care; Thrombosis Centre; University of Florence, Azienda Ospedaliero-Universitaria Careggi, Florence, Italy. 2Department of Clinical Pathophysiology, Unit of Clinical Nutrition, University of Florence, Italy. 3Don Carlo Gnocchi Foundation, Onlus IRCCS, Florence, Italy.
Objective High plasma lipoprotein (a) [Lp(a)] concentrations are an independent risk factor for atherosclerotic diseases. To date, no effective intervention strategies on reducing Lp(a) concentrations have been reported. Aim of the study was to evaluate the possible modulation of 2 polymorphisms of LPA gene (LPA 93C > T and LPA 121G > A) and nutritional habits on Lp(a) concentrations.
Methods We studied 647 healthy Italian subjects (260 M; 387 F) with a median age of 48 years (range: 19–;78) enrolled in an epidemiological study conducted in Florence, Italy between 2002 and 2004.
Results A linear regression analysis showed a significant negative influence of fish intake (β = −0.174 ± 0.084; P = 0.04) on Lp(a) concentrations, after adjustment for smoking habit, C-reactive protein serum concentrations, dietary habits and LDL-cholesterol concentrations.
With regard to LPA polymorphisms, LPA 93C > T polymorphism resulted to significantly affect Lp(a) circulating concentrations in a dose-dependent manner, with lower concentrations showed by subjects carrying the T rare allele. No significant influence of LPA 121G > A polymorphism on Lp(a) concentrations was observed. Moreover, by analysing the possible interplay between LPA 93C > T and dietary fish intake, a significant interaction between these two determinants in lowering Lp(a) concentrations was observed. Lower Lp(a) concentrations were observed in subjects carrying the T allele of the LPA 93C > T polymorphism and consuming a high intake of fish with respect to those being in the highest tertile of fish consumption but homozygotes for the common allele of the polymorphism.
Conclusions In conclusion, this study reported a significant interaction of daily fish intake and LPA 93C > T polymorphism in decreasing Lp(a) concentrations.
240 Effect of fish eating on lipid, inflammatory and haemorheological variables: an intervention study
F. Sofi1, A.M. Gori1, F. Cesari1, R. Paniccia1, L. Mannini1, G. Parisi2, B.M. Poli2, R. Abbate1, G.F. Gensini1,3
1Department of Medical and Surgical Critical Care, Thrombosis Centre, University of Florence, Azienda Ospedaliero-Universitaria Careggi, Florence, Italy. 2Dipartimento di Scienze Zootecniche, University of Florence, Italy. 3Don Carlo Gnocchi Foundation, Onlus IRCCS, Impruneta, Florence.
Centro Interdipartimentale di Ricerca per la Valorizzazione degli Alimenti (CeRA), Università degli Studi di Firenze.
Objective Fish eating has long been indicated as a protective dietary factor for cardiovascular diseases. Numerous studies have demonstrated that fatty acid profile of cultured fish diet has a strong impact on the fatty acid profile of the lipid deposited in muscle. Aim of this study was to evaluate the influence of short-term dietary intake of fish on biomarkers related to the atherosclerotic process.
Methods In 9 dyslipidemic subjects (5 females; 4 males) with a mean age of 52.8 years we evaluated lipid profile (total cholesterol, HDL-cholesterol, LDL-cholesterol and triglycerides) inflammatory markers [highly-sensitive C-reactive protein (hsCRP), interleukin−6 (IL−6) and interleukin−8 (IL−8)], and haemorheological profile [whole blood viscosity (WBV), plasma viscosity, erythrocytes' filtration rate (EF)] before (T0) and after a dietary intervention with 900 g of Orbetello farmed sea bass (Dicentrarchus labrax) per week for 10 weeks (T1).
Results A general linear model for repeated measurements after adjustment for age, gender, weight change and total fats' intake was conducted. Fish intake significantly decreased triglycerides (T1: 184.3 ± 29.2 vs. T0: 140 ± 20.3 mg/dL; p = 0.04), whereas no significant changes for the other lipid variables have been observed. With regard to inflammatory pattern, dietary intervention significantly decreased all the parameters investigated, namely hsCRP, (T1: 2.6 ± 0.04 vs. T0: 2.2 ± 0.06 mg/L) IL−6 (T1: 3.1 ± 0.6 vs. T1: 1.9 ± 0.7 pg/mL) and IL−8 (T1: 17.4 ± 0.06 vs. T0: 12.6 ± 0.09 pg/mL). Furthermore, as regarding haemorheological parameters, a significant (p = 0.04) improvement in EF was reported after 10 weeks of fish dietary intake (T1: 9.0 ± 0.7 vs. 5.4 ± 1.0% for T1 and T0, respectively).
Conclusions Dietary short-term intake of fish seems to impose favourable biochemical changes in dyslipidemic subjects, with regard to lower circulating levels of markers of atherosclerosis, such as lipid parameters, inflammatory markers and haemorheological variables.
241 Coffee consumption and risk of coronary heart disease: a meta-analysis
F. Sofi1, A.A. Conti1,3, F. Cesari1, A. Capalbo1, A.M. Gori1, M.L.E. Luisi2, A. Casini3, R. Abbate1, G.F. Gensini3.
1Department of Medical and Surgical Critical Care, Thrombosis Centre, University of Florence, Italy; 2Department of Clinical Pathophysiology, Unit of Clinical Nutrition, University of Florence; 3Fondazione Don Carlo Gnocchi, Onlus IRCCS, Impruneta Florence.
Objective Coffee is among the most widely consumed beverages in the world. During the past decades, the relationship between habitual coffee drinking and coronary heart disease (CHD) has been assessed in numerous studies, with conflicting results. Aim of this study was to examine the association between habitual coffee consumption and risk of CHD.
Methods A systematic literature search of MEDLINE, EMBASE, Web of Science, and the Cochrane Database up to February 2006 was conducted using a combined text word and MeSH heading search strategy. Studies were eligible if they had reported estimated of the association with CHD for the different consumption of coffee, as reported by cups per day.
Results We identified 11 case-control studies and 9 cohort studies, including more than 5,500 cases of CHD for case-control studies and over 250,000 subjects followed for a follow-up time ranging from 2 to 21 years for cohort studies. The summary ORs for CHD of included case-control studies were statistically significant for all the categories of coffee consumption considered: 2.01 (95%CI 1.62–;2.49; p > 0.001) for the highest consumption category (> 4 cups/day), 1.55 (95%CI 1.26–;1.90; p < 0.0001) for the second highest category (2–;4 cups/day), and 1.16 (95%CI 1.06–;1.40; p = 0.01) for the third highest category (1–;2 cups/day). On the other hand, the analysis for long-term follow-up cohort studies showed no significant association between coffee intake and CHD, with ORs of 1.20 (95%CI 0.94–;1.53; p = 0.4) for the highest consumption category, 1.10 (95%CI 0.92–;1.31; p = 0.3) for the second highest category, and 0.97 (95%CI 0.82–;1.15; p = 0.7) for the third category.
Conclusions The present systematic review performed on the association between coffee intake and risk of CHD, seems to indicate that coffee consumption is not significantly associated with higher risk of CHD, despite a mild significant association within case-control studies has been observed.
242 Physical activity during leisure time and primary prevention of coronary heart disease: an updated meta-analysis of cohort studies
F. Sofi1, A. Capalbo1,2, F. Cesari F1, N. Pucci1, R. Abbate1, G.F. Gensini1,3
1Department of Medical and Surgical Critical Care; Thrombosis Centre; University of Florence, Azienda Ospedaliero-Universitaria Careggi, Florence, Italy.
2Institute of Sports Medicine, Florence, Italy.
3Don Carlo Gnocchi Foundation, Onlus IRCCS, Florence, Italy.
Objective A vast body of evidence showed a clear preventive role for physical activity on the occurrence of cardiovascular disease. We systematically assessed the relationship between physical activity during leisure time (LTPA) and primary prevention of coronary heart disease (CHD) in an updated meta–;analysis of prospective cohort studies.
Methods We searched MEDLINE, EMBASE, the Cochrane Library and bibliographies of retrieved articles. Studies were included if they reported relative risks and their corresponding 95% CIs for categories of LTPA in relation to CHD.
Results Eighteen cohort prospective studies, incorporating 363,553 subjects (16,103 CHD events) followed up for 4–;23 years, met the inclusion criteria. We grouped all the categories of LTPA reported into 3 levels of intensity: high, moderate and low or sedentary. The high level of physical activity was determined in order to obtain a level of intensity attainable by the general population. Under a random–;effect model, the overall analysis showed that individuals who reported to perform a high level LTPA had a significant protection versus CHD (relative risk 0.73 [95% CI 0.65–;0.81], p < 0.00001). A similar significant protection on the occurrence of CHD for subjects who practise a moderate level of LTPA has been also demonstrated (relative risk 0.86, [95% CI 0.81–;0.92], p < 0.0001).
Conclusion The present meta–;analysis reports a significant protection of a moderate–;to–;high level of physical activity against the occurrence of CHD. These results strengthen the recommendations of guidelines indicating the protective effect against cardiovascular disease of physical activity profiles attainable by the ordinary people.
243 Physical activity and cardiovascular risk factors in a middle-aged urban Italian population
1Department of Medical and Surgical Critical Care; Thrombosis Centre; University of Florence, Azienda Ospedaliero-Universitaria Careggi, Florence, Italy. 2Department of Clinical Pathophysiology, Unit of Clinical Nutrition, University of Florence, Italy. 3Don Carlo Gnocchi Foundation, Onlus IRCCS, Florence, Italy. 4Institute of Sports Medicine, Florence, Italy.
Objective A large number of studies demonstrated that a regular physical activity accounts for a significant protection against cardiovascular diseases (CVD). However, the mechanisms through which this protection is determined are not completely established. Aim of this study was to evaluate the possible influence of a different amount of regular physical activity during the leisure-time (LTPA) and at work (occupational physical activity: OPA) on circulating levels of several biomarkers associated with an increased risk of CVD.
Methods We studied 932 individuals (365 M; 567 F, with a mean age of 54 years) living in Florence, Italy who were enrolled in a population study conducted between 2002 and 2004.
Results Subjects were divided into 3 classes of LTPA and OPA according to the amount of physical activity performed. LTPA was inversely related to BMI, hip circumference, diastolic blood pressure, and triglycerides, as well as directly correlated with HDL-cholesterol and vitamin B6. Likewise, a higher level of physical activity at work was found to be associated with higher HDL-cholesterol levels. Moreover, a multivariate logistic regression analysis adjusted for possible confounders showed that a moderate-to-high intensity of LTPA was able to confer a significant protection against having abnormal levels of BMI, waist circumference and triglycerides, main features of the metabolic syndrome, whereas no associations with OPA were observed.
Conclusions A moderate-to-high LTPA was found to be significantly associated with a more favourable cardiovascular profile in terms of anthropometric, metabolic, lipid and vitamins' circulating levels among a middle-aged urban Italian population. In addition, a relationship between higher level of OPA and HDL-cholesterol was reported.
248 Moderate intensity exercise training improves endothelial function but not body composition or high sensitivity C-reactive protein in postmenopausal women
S.E. Barber, N.T. Lewis, L.B. Tan, K.M. Birch
University of Leeds, Leeds, United Kingdom
Objectives Endothelial dysfunction, body composition and high sensitivity C-reactive protein (hsCRP) are independent predictors for the development of cardiovascular disease (CVD), whilst hsCRP is also an index of endothelial function. Following the menopause, endothelial function deteriorates and central adiposity increases independently of changes in other CVD risk factors. Endothelial function is independently related to cardio-respiratory fitness in these women, however the influence of exercise training upon endothelial function in postmenopausal women is unclear. Thus this investigation examined the impact of a six month moderate intensity exercise programme upon endothelial function, body composition and hsCRP in sedentary postmenopausal women aged 57 ± 3.6 yrs.
Methods Participants were assigned to either an exercise (n = 18) or control (n = 10) group, groups did not differ in age or years post-menopause (P > 0.05). The exercise group undertook two 45 min supervised sessions of aerobics/cycling at an intensity progressing from 55–;75% heart rate reserve and one home-based exercise session per week for 6 months. The control group continued life as normal. Prior to and following the 6 months the following variables were assessed: VO2 peak via a Bruce treadmill test, body composition via skinfold analysis, measurement of waist and hip circumferences, BMI and body mass, hsCRP via fasting venous blood sample and endothelial function via flow mediated dilation (FMD). A two-way mixed mode ANOVA with repeated measures was used to test for interactions between time (0 v 6 months) and group (exercise/control) for each variable.
Results Table 1 displays the variables that revealed a time by group interaction.
Following the exercise intervention VO2 peak and FMD improved by 22% and 71% compared to controls. W:H ratio increased from 0 to 6 months in the control group, conversely there was no change in W:H ratio in the exercise group. hsCRP, body mass and BMI did not change following exercise (P > 0.05), whilst percent fat decreased by 2.4% (P > 0.05).
Means±SD for time and group differences
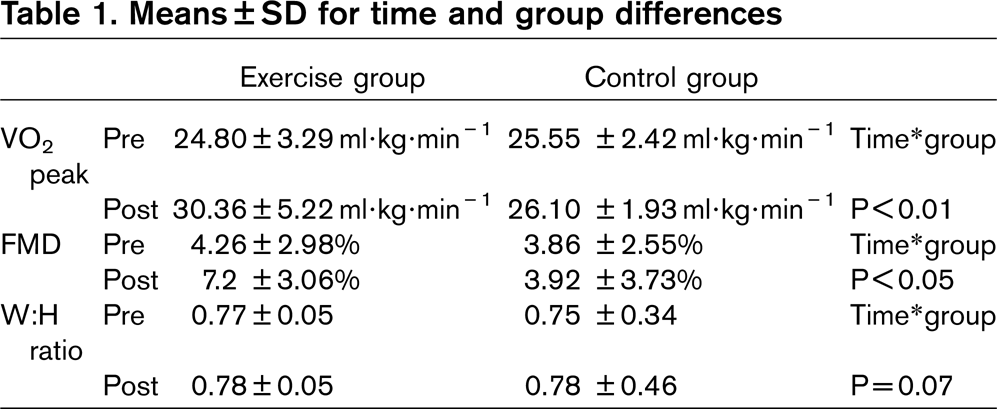
Conclusion In postmenopausal women, a moderate intensity 6 month exercise training programme can improve endothelial function and VO2 peak without any appreciable changes in body composition or hsCRP.
254 Cardiovascular risk factors and patient behavior models in Russia
A. Kontsevaya1, A. Kalinina1, M. Omeljanenko2, T. Romanenko2
1National Research Center of Preventive Medicine
2Ivanovo State Medical Academy
Objective To study behavior models of patients with cardiovascular risk factors (obesity, smoking and stress).
Methods The study involved 843 persons, aged from 20 to 60, in four Russian regions, which visit their doctor in policlinic for any reason. Survey with standard questionnaires, anthropometry, tonometry, were performed. Risk factor prevalence was estimated by standard criteria. Behavior models included patient's readiness to correct risk factor and need in specialist help.
Results The risk factors prevalence, patient's readiness to correct this risk factor and need in specialist help were calculated. The prevalence of lifetime smoking was 36,7%, 59,4% in male and 23,3% in female. Of these patients' 42,8% wanted to stop smoking (45,2% smoking male and 38,2% smoking female). The need in specialist help was in 25,2% smoking patient. Prevalence of overweight (body mass index of 25 kg/m2 and higher) was 36,3%. Of these patients' 71,4% wanted to decrease body mass (45,9% obese male and 85,7% obese female). The need in specialist help was in 48,5% obese patient. Prevalence of stress was 43,4%, 39,3% in male and 45,8% in female. Of these patients' 87,4% wanted to correct stress (55,3% male with high stress and 100% female with high stress). The need in specialist help was in 55,1% obese patient. Only 17,6% persons checked their cholesterol and knew its value, for serum glucose this parameter was 23,5%.
Conclusion Cardiovascular and cerebrovascular diseases are likely to remain significant epidemics in Russia as long as the risk factors remain widely prevalent. Interventions are clearly needed to reduce the prevalence of tobacco smoking, obesity, and stress. When planning preventive interventions one must consider patients behavior model. If patient don't want to correct risk factor, the preventive medicine provider must use serious motivation technologies, if patient are ready to lifestyle modification and need in specialist help, the strategy will be another and much easier.
260 Evaluation of cerebrovascular risk by ecocolordoppler in patients with acute coronary syndrome
F. Fini1, G. Illuminati2, G. Zampi1, F. Barillà1, V. Paravati1
1Dpt. Cuore e Grossi Vasi “A. Reale”, University of Rome “La Sapienza”, Rome, Italy.
2Dpt. Chirurgia “F. Durante” University of Rome “La Sapienza”, Rome, Italy.
Objectives Stroke is the third cause of death in western countries. Patients (pts) with acute coronary syndrome (ACS) have a high incidence of cerebrovascular ischemia risk. The purpose of this study was to evaluate the correlation between instability of atherosclerotic carotid plaque and its morpho-functional pattern showed by ecocolordoppler, in patients with ASC.
Methods The study included 77 patients, 52 men and 25 women, average of 60 ± 10 years. All patients selected, at the admition presented ACS, all underwent to ecocolordoppler of epiaortic vessels. The population was followed for 6 months to evaluate cerebrovascular events. The patients were divided into two groups: Group A, 34 pts with diabetes type 2; Group B, 43 pts without diabetes.
Results During admission 3 pts of Group A and only 1 pts of Group B have had a stroke, all these patients showed a soft plaque at the ecocolordoppler. During the follow up, exactly, in the 4th month of observation, only 1 patient of Group A had a transitory ischemia attack. This patient showed a fibrocalcific plaque associated with an carotid artery stenosis of 70%.
The table shows the results of ecocolordoppler epiaortic vessels of the patients examined.
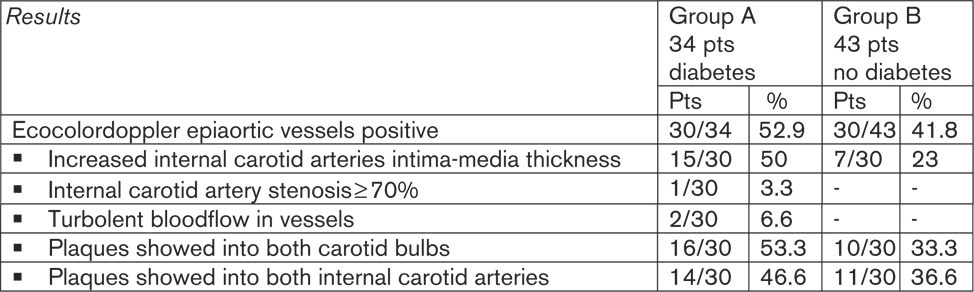
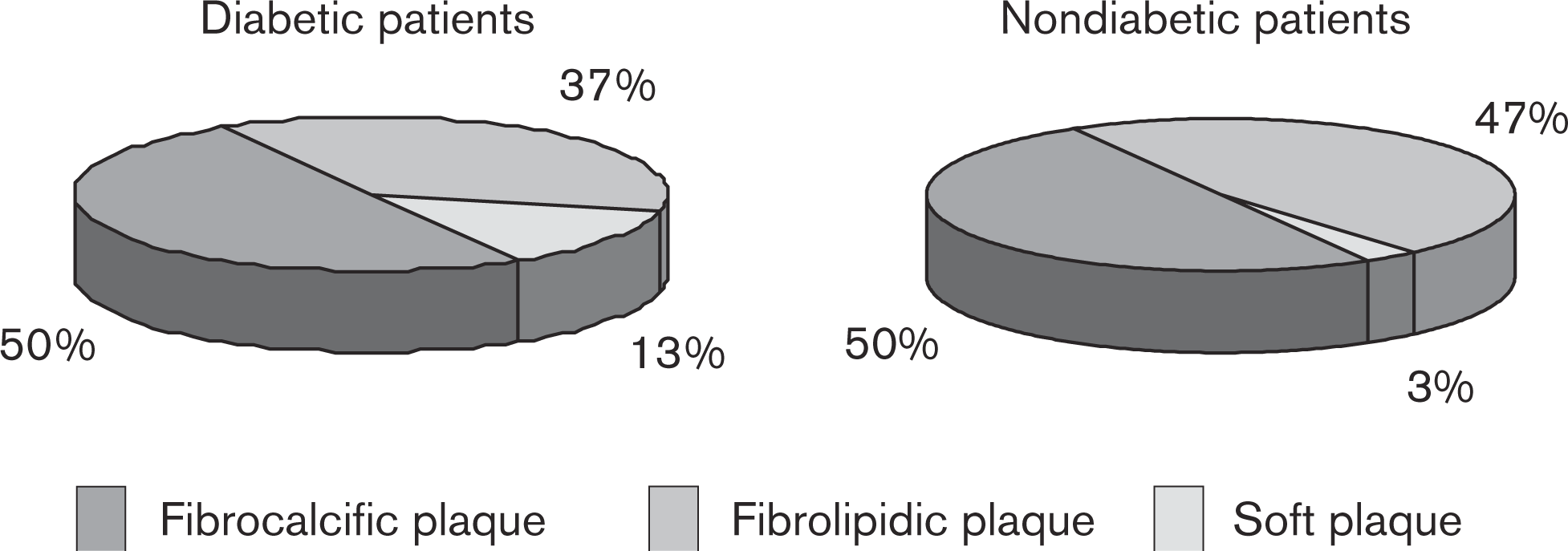
The pie-charts show the morphologic pattern of the atherosclerotic carotid plaque documented by ecocolordoppler in diabetic and non diabetic patients.
Conclusion In agreement with literature, our study shows that diabetic patients have an atherosclerotic disease more aggressive than non diabetic patients, therefore these patients have a high risk to develop cerebrovascular events. The study advises that to stratify cerebrovascular disease risk, the morphology of atherosclerotic plaque correlates with its instability better than its functional pattern.
263 The difficult transition from research to clinical practice: the CUORE project experience
S. Giampaoli1, C. Orsi1, P. Ciccarelli1, P. De Sanctis1, A. Giannelli1, P. D'Argenio2, A. Addis3, S. Panico4, F. Dima1, C. Lo Noce1
1National Centre for Epidemiology, Surveillance and Health Promotion, Institute of Health, Rome, Italy
2Ministry of Health, Rome, Italy
3National Drug Governance Agency, Rome, Italy
4Federico II University, Napoli, Italy
Objectives The CUORE project was launched in 1998 and is coordinated by the National Institute of Health with the support of the Ministry of Health and the cooperation of the National Drug Government Agency. It aims to: 1. implement a national population-based register of cardiovascular events; 2. describe risk factors distribution and high risk adult population through a health examination survey; 3. estimate cardiovascular risk of the Italian population; 4. implement the evaluation of cardiovascular risk in clinical practice.
Methods The first and the second objectives were achieved through the National Register of Coronary and Cerebrovascular Events and the Osservatorio Epidemiologico Cardiovascolare. Methods and results have already been published and made available on the CUORE Project website (www.cuore.iss.it).
The third objective was reached through the identification of the best risk equation to assess the probability of developing a major cardiovascular disease in 10 years. A free downloadable software (cuore.exe) that enables GPs to calculate the individual risk score is available on the website. The last objective includes: 1. GPs training to assess cardiovascular risk; 2. rational and continuous prescription of drugs promotion; 3. GPs training to recommend patients to adopt a healthy lifestyle. A National Prevention Plan for 2005–;2007, launched by the Ministry of Health, put cardiovascular risk assessment and cardiovascular prevention as top priorities. Within this framework, an agreement between the Ministry of Health and the Regions was signed and financial support was allocated to implement risk assessment in the general population and to support a national training programme for GPs on the use and application of cardiovascular risk. This programme foresees frontal teaching and/or distance learning, followed by the collection of risk factors which are then pooled and analyzed on a national basis.
Results To date, about 874 professionals participated to the training programme and about 4.000 professionals (GPs, cardiologists, centres for blood transfusion and for preventive medicine) have downloaded the software cuore.exe.
Conclusions The primary purpose of the CUORE Project is to emphasize the key role of prevention and to encourage GPs to focus not only on high risk individuals but increase the proportion of low-risk individuals in the general population through the promotion of healthy lifestyles.
This close cooperation among the Ministry of Health, the National Drug Governance Agency, the National Institute of Health, the Federation of Cardiologists and the College of General Practitioners is the greatest step forward a sustainable disease prevention strategy.
266 Optimizing the care for patients with an acute myocardial infarction by implementation of an all-phases integrated care program: the MISSION! project
S.S. Liem, MD, B.L. van der Hoeven, MD, H.F. Verwey, MD, D.E. Atsma, MD, E.T. vd Velde, PhD, J.W. Jukema, MD, J.J. Bax, MD, E.E. van der Wall, MD, M.J. Schalij, MD
Leiden University Medical Center, Leiden, The Netherlands
Background Acute myocardial infarction (AMI) guideline implementation programs enhance adherence on evidence-based medicine (EBM) and improve AMI care. Although, under-treatment of AMI patients is known in both acute and chronic care, most programs focus on the index hospitalization phase only. We hypothesize that an all-phases integrated AMI program can further maximize the use of EBM in daily practice.
Methods MISSION! is a guideline implementation program, which addresses the pre-hospital, in-hospital and outpatient phase, up to one year following the index event. MISSION! concentrates on early reperfusion therapy, structured medical therapy and changing risk behaviours. Using a before (n = 100, January 2003-December 2003) and after implementation cohort of AMI patients (n = 416, February 2004-January 2006), we assessed the effects of the MISSION! program by the use of performance indicators.
Results In both groups more than 90% of the patients were treated with primary PCI. MISSION! pre-hospital triage resulted in a significant reduction of median door-to-balloon time from 76 min to 49 min (p < 0.001), and 96% of the patients were treated within the recommended 90-minutes door-to-balloon time compared to 74% (p < 0.001). The MISSION! patients received more frequently beta-blocker (85% vs. 72%; p < 0.01) and ACE-inhibitor therapy (89% vs. 38%; p < 0.001) within 24 h after admission, and more patients were discharged with an ACE-inhibitor (97% vs. 64%; p < 0.001). At 1-year follow-up more MISSION! patients used clopidogrel (92% vs. 59%; p < 0.001), beta-blockers (89% vs. 82%; p < 0.001), and ACE-inhibitors (97% vs. 69%; p < 0.001). Despite a similar rate of statin use (both above 95%), more MISSION! patients achieved the target cholesterol level of < 4.5 mmol/L (78% vs. 59%; p < 0.001), and the target LDL level of < 2.5 mmol/L (70% vs. 8%; p < 0.001). At 1-year follow-up more MISSION! patients stopped smoking (62% out of 50% vs. 32% out of 53% current smokers at the time of index; p = 0.02)
Conclusion Optimal AMI care starts pre-hospital. In addition, regular monitoring and adjustment of therapy during follow-up is of major importance to further optimize care. An all-phases integrated AMI program is a strong tool to maximize the use of EBM in daily practice.
267 Cardiovascular risk in young apparently healthy descendents from Asian Indian migrants in the Netherlands: the SHIVA study
Su San Liem1, Pranobe V. Oemrawsingh2, Suzanne C. Cannegieter1, Saskia Le Cessie1, Joop Schreur2, Frits R. Rosendaal1, Martin J. Schalij1
1Leiden University Medical Center, Leiden, The Netherlands
2Medical Center Haaglanden, The Hague, The Netherlands
Objectives First and 2nd generation Asian Indian migrants in the Western world are highly susceptible for ischemic heart disease. For optimal prevention, knowledge of the cardiovascular risk profile of younger generations is crucial. We assessed the cardiovascular risk profile in asymptomatic 3rd to 7th generation Asian Indian descendants, and compared the results with Europeans.
Methods and results In a cross-sectional study, 1790 Asian Indians (45% men, age 35.9 ± 10.7 years) and 370 native Dutch hospital employees (23% men, age 40.8 ± 10.1 years) were recruited. Subjects were classified as asymptomatic if they were not known with ischemic heart disease, diabetes, hypertension or high cholesterol. Asian Indians had higher levels of total cholesterol, LDL, triglycerides, and lower HDL levels than the Dutch. Glucose intolerance was present in 7.1% vs. 0.5% men, and in 6.1% vs. 1.4% women (both p < 0.001). Asian Indian women were more frequently obese (12% vs. 5%; p < 0.001), and central obese (44% vs. 25%; p < 0.001) as compared to the Dutch women. Prevalence of most of the conventional and modifiable cardiovascular risk factors in each 10-year age group was higher in Asian Indians compared to controls, which reflected in higher Framingham risk scores. Twenty-three percent of smoking Asian Indian men aged 30–;35 years had a risk > 10%. In the age group 50–;54 years all of the smoking men had a 10-year risk > 10%, and 77% had a risk > 20%. In smoking Asian Indian women between 40 and 44 years 29% had a 10-year risk > 10%; this was all above the age of 50 years.
Conclusion This study confirms the persistence of a strikingly unfavourable cardiovascular risk profile in 3rd–;7th generation migrated Asian Indians. These observations support an aggressive screening and intervention strategy in this high-risk population to prevent subsequent cardiovascular events and to improve their long term prognosis. Furthermore these strategies should focus on younger age groups than currently applied in Europeans.
271 Accuracy of the hypertriglyceridemic waist measure to diagnose metabolic syndrome and insulin resistance
Hospital Dipreca. Santiago, Chile
Background The “hypertriglyceridemic waist” (HTG-W) has been considered a simpler measurement to diagnose metabolic syndrome (MS) in a clinical setting. Also, studies have shown that it is a good predictor of insulin resistance (IR) in Caucasian population, eventhough it is not recommended on the guidelines.
Objective Analyze in a Latin-American population the accuracy of the HTG-W index in predicting insulin resistance and metabolic syndrome.
Methods Cross sectional study design, done in a high risk CV prevention clinic. We evaluated patients at admission with: waist circumference (WC), body mass index, blood pressure, lipid profile, fasting plasma glucose (FPG) and insulin (FPI). We diagnosed MS based on Modified ATPIII and International Diabetes Federation (IDF) definitions. IR was measured by HOMA equation considering abnormal a value greater than 2,5. A positive HTG-W was considered a triglyceride plasma level greater than 2 mmol/L (177 mg/dl) and a WC for men greater than 90 cm (Lemieux et al. 2000) and for women greater than 80 cm. The SPSS® 13.0 program was used for the statistics analysis. Frecuencies of variables was calculated. Chi- square and Fischer exact test were applied for evaluation of nominal variables and the estimate risk was analyzed.
Results We studied 221 patients (59,8 + −10,7 years), 50,2% male 93% hypertension, 13,1% diabetes and 49,3% obese. 65 patients (29,4%) presented a positive HTG-W. The prevalence of IR in the positive HTG-W group was 71%, instead of 51,9% in the negative HTG-W group. (p: 0,012) O.R: 2,1 (CI:1,17–;4,06). The prevalence of modified ATP III metabolic syndrome in the positive HTG-W was 83% vs 44,8% in the negative HTG-W group (p < 0,001) O.R: 6,0 (CI: 2,9–;12,4) The prevalence of the IDF metabolic syndrome in the positive HTG-W was 100% vs 55,7% (p < 0.001) O.R.: 50,7 (CI: 6,8–;375).
Conclusion The HTG-W presented a good correlation with insulin resistance and an excellent correlation with MS diagnosis, considering both definitions. It appears as a simple diagnostic tool to health screening population in a primary prevention setting.
272 The triglyceride-HDL cholesterol ratio is not a marker of insulin resistance in Latin Americans
Hospital Dipreca. Santiago, Chile
Background In Caucasians a ratio of triglycerides (TG) to high-density lipoprotein cholesterol (HDL-C) greater of 3 can predict insulin resistance in individuals with a body mass index (BMI) greater of 25 kg/m2; nevertheless in other population like Afro Americans it is not a reliable marker.
Objective Our goal was to determine if TG-HDL-C ratio predicted insulin resistance (IR) and metabolic syndrome (MS) in Latin Americans with a BMI of 25 kg/m2 or more.
Methods Cross-sectional study design, done in a high risk CV prevention clinic. We evaluated 221 patients at admission with: BMI, waist circumference, blood pressure, lipid profile, fasting plasma glucose (FPG) and insulin (FPI). We diagnosed MS based on modified ATP III definition. IR was measured by HOMA equation considering abnormal a value greater than 2,5. The SPSS 13.0 program was used for the statistics analysis. Categorical data were analyzed by chi-square and Fischer exact tests. Areas under the receiver operating characteristic curve (ROC) were determined to identify variables that predicted insulin resistance and metabolic syndrome, including TG-HDL-C ratio.
Results 207 patients presented a BMI ⇒ 25 (mean: 30,6 ± 4), mean age 59 ± 10,6 years, 50,7% male, mean TG level: 160 ± 83,6 mg dl and mean HDL–;C level: 48,1 ± 11,9 mg/dl. A high prevalence of ATP III and IR was detected: 57,5% and 59,9% respectively. The mean ± SE areas under the curve for BMI, WC and TG-HDL-C ratio to detected IR were 0,71 ± 0,03 (CI: 0,64 −0,78); 0,69 ± 0,03 (CI:0,62–;0,76) and 0,6 ± 0,04 (CI: 0,52–;0,68) respectively. The mean ± SE areas under the curve of the same variables to detected MS were: 0,73 + −0,03 (0,76–;0,8) 0,71 + −0,03 (I0,64–;0,78), and 0,74 ± 0,03 (CI. 0,67–;0,80).
Conclusions In Latin American population the TG HDL ratio is not a reliable marker of insulin resistance, like in Afro American. Obviously this ratio is better as a marker of MS. WC and BMI must be considered better predictors of IR.
281 Learnings from Romanian Quit&Win 2000–;2006 smoking cessation campaigns
R. Negoescu for the Quit&Win Romania Coordination Unit, Institute of Public Health, Bucharest, Romania.
Objectives International Quit&Win contest (Q&W) - a positively, prize-oriented campaign to stimulate smoking cessation coordinated by National Public Health Institute (KTL) of Helsinki-did progress from 13 countries and 60,000 participants in 1994 to 72/600,000 in 2004. Since 2002 Q&W is separately targeting health professionals (HP); Romania was coordinating the HP subcampaign in EU accession countries. Q&W Romania (QWR) is organized since 2000 by coalitions including district Authorities of Public Health, pulmonology network and civil society organizations-nationally led by the Institute of Public Health. Since 2004 the Association for Health, Education and Family (ASEF) took the executive role over.
Methods Study inter-compares QWR 2000, 2002 and 2004 follow-ups and 2006 preliminary results. QWR 2000 enrolled 1323 smokers, all of them being addressed by mail questionnaires with the 2001 follow-up (response rate: 27%) that indicated a 26,8% continuous nonsmoking status and a 44.6% nonsmoking at the follow-up time (point abstinence). Dynamics is: QWR 2002–;1389 participants; 31.5% response rate in 2003; after 1 year 25.5% continuous and 46.1% point abstinence; QWR 2004–;1103; 21.4% response rate in 2005; after 1 year 35.2% continuous and 52,1% point abstinence. HP average recruitment over Europe since 2002 was about 10% of total participants versus about 1% beforehand; QWR 2006 –; 1031 participants.
Results and discussion QWR recruitment dynamics shows the “blowing-up then recoil” pattern also seen in other countries of the EURO region. Continuous effectiveness shows plateau at 26% then significant increase at 35%; point effectiveness tends to increase progressively. Follow-ups showed levels of performance compared to the European best (continuous abstinence peak in Germany 2000 –; about 30%; point peak in Veneto (Italy) 1998–;37.3%); however lower response rates (despite monetary incentives) weaken yet QWR performance in KTL statistics that are taking all non-respondents as smokers. Romanian campaigns feature small budgets: in 2000-about $5000; 2002–;$2700; 2004–;$2000, including sponsored monetary and in-kind prizes (e.g. $1000 as the national big one) but not manpower of public health workers (directed to many other targets) or ASEF's non-paid volunteers. Media impact parallels enrolment, the public interest for personal improvement being strongly competed by time and emotional resources spent in sociopolitical turn-moil of the Romanian transition. Nearly exclusive ASEF manpower saved QWR 2004, but both central and local coalitions got thinner. In 2006 a consistent effort to strengthen broader social interests in smoking cessation allowed to preserve the enrolment. While maintaining non-governmental organizations' role remains crucial for QWR, rebuilding broader coalition of civil society & professional milieus and acquiring public and European funding is a must in view of Romania's ratification of the FCTC and EU accession.
Conclusion Despite of psycho-social climate hostile to life-style improvement, Romanians remain sensitive to positive health campaigns like Q&W. Smoking, the 2nd (after psycho-social stress) risk factor in the tableau of morbidity/mortality by chronic diseases in Romania, should maintain its priority as a main target for public health.
282 Mirthful laughter, as adjunct therapy in diabetic care, attenuates catecholamines, inflammatory cytokines, C-reactive protein, and myocardial infarction occurrence
L.G. Tan, S.A. Tan, L.S. Berk
Oakcrest Health Research Institute, Yucaipa, CA, USA
Objectives Catecholamines, especially adrenalin, are implicated in causing arrhythmias, hypertension, and MI. Inflammatory cytokines—such as tumor necrosis factor-alpha (TNF-α), interferon-gamma (IFN-γ) and interleukin−6 (IL−6)—contribute to the acceleration of atherosclerosis. C-reactive protein (CRP) is a risk stratification inflammatory marker. Attenuation of catecholamines and inflammatory cytokines may provide cardiovascular protection. We have reported that mirthful laughter attenuates adrenalin production. However, the effects of mirthful laughter on inflammatory cytokines are unknown. We hypothesized that mirthful laughter, by diminishing catecholamines production, can attenuate inflammatory cytokines, and may provide cardiovascular protection.
Methods We divided 20 high risk diabetic patients with hypertension and hyperlipidemia into 2 matched groups and followed them for one year in our Metabolic Syndrome clinic. The experimental group was asked to view self-selected humor for 30 minutes daily as an adjunct to standard diabetes (glipizide, TZD, metformin), hypertension (ACE inhibitor or ARB) and hyperlipidemia (statin) therapies. Plasma fractionated catecholamines levels, lipid panel, TNF-α, IFN-γ, IL−6, and CRP were monitored and assayed every 2 months.
Results The patients in the laughter group had lower adrenalin and noradrenalin levels by 2 months, increased HDL cholesterol, decreased TNF-α, IFN-γ, IL−6 and CRP levels by 4 months, and a lower incidence of MI (1/10) than did the control group (3/10).
Conclusions Addition of mirthful laughter lowers adrenalin and noradrenalin levels, and then lowers inflammatory cytokines and CRP levels also. Laughter increases HDL-cholesterol. These effects may contribute to lower MI occurrence. Thus, laughter can be an effective cardiovascular preventive adjunct in diabetes mellitus and metabolic syndrome care.
286 How can different cardiovascular risk factors influence on pulse pressure?
P. Zelveian1,2, A. Potosyan1, T. Uzunyan1, Y. Sahakyan1
1Armenian Medical Association, Yerevan, Armenia
2Institute of Cardiology, Yerevan, Armenia
Objectives Pulse pressure (PP) is one of the important determinants of cardiovascular outcome with high prognostic value in adult population. The main objective of this study was to determine the impact of different cardiovascular risk factors on PP in adult population of Yerevan, Armenia.
Methods The study is a part of “Blood Pressure Screening and Survey in Yerevan adult population” study conducted in April-May 2004. A survey and blood pressure (BP) screening and anthropometric parameters were performed among 748 randomly selected adults from Yerevan. To prevent treatment exposure bias, we analyzed 629 data of subjects (222 men and 407 women) who never take antihypertensive medications. BP was measured by Korotkov's method (three times on each arm with 5 minutes intervals). Overweight was defined as body mass index (BMI) 25–;30 kg/m2 and obesity as BMI > 30 kg/m2. Friendly-designed and self-reported standard questionnaires consisted of multiple-choice and open-ended questions. Surveyed participants were asked whether they smoke, physically “active”, and amount of salt intake. Mean PP was compared between different groups of study participants. Statistical analysis was performed by T-test comparisons of means.
Results
The PP significantly grows with age and reached statistically significance in all age groups (38.4 ± 7.9 mmHg in < 45y age group, 41.5 ± 10.0 mmHg in 45–;54y age group, 48.7 ± 13.4 mmHg in 55–;64y age group, 50.5 ± 15.9 mmHg in 65–;74y age group, and 63.7 ± 25.4 mmHg in > 75 years old subjects, P < 0.0001).
PP difference between both genders was 2.31 mmHg (42.5 ± 12.0 mmHg in males and 40.2 ± 10.3 mmHg in females, P < 0.006).
The smoking status impact on PP only in heavy smokers. Only those who smoke > 10 cigarettes/day have PP statistically different from nonsmoking subjects (P = 0.014). The mean PP in nonsmoking subjects was 40.0 ± 10.1 mmHg. Those who smoke 10–;20 cigarettes/day have mean PP = 43.8 ± 10.9 mmHg, and heaviest smokers (> 20 cigarettes/day): PP = 44.4 ± 14.0 mmHg, P = 0.0014.
The mean PP in subjects with normal weight, overweight and obese was 39.2 ± 10.1 mmHg, 42.0 ± 10.9 mmHg and 46.0 ± 11.3 mmHg respectively. We found out statistically significant difference in PP between overweight subjects and those with normal weight among females (P = 0.003) and between obese and normal weight subjects in both genders P < 0.000.
We did not find any difference in PP in physically “active” (40.7 ± 10.5 mmHg) and “inactive” (42.2 ± 12.2 mmHg) subjects (P = 0.07) as well as in those who have mild, moderate and high salt intake (mean PP are 41.4 ± 11.5 mmHg, 40.6 ± 9.9 mmHg and 41.8 ± 12.9 respectively, P = 0.22).
Conclusion The data support evidence that age, smoking and BMI are prognostic determiners of PP, especially in subjects with markedly expressed risk factors (elderly, obese and heavy smokers). The physical activity and salt intake did not influenced on PP.
295 Is dypiridamole stress echocardiography appropriate for predict cardiac risk in diabetic patients with peripheral artery disease?
Elisabetta Rossi, F. Citterio∗, G. Spagnoletti∗, E. Favi∗, P. Silvestri∗, P. Violi∗, G. Ghirlanda°
Department of Cardiovascular Disease, Catholic University, Rome Italy.
∗Department of Surgical Science, Catholic University, Rome Italy
°Department of Internal Medicine, Catholic University, Rome Italy
Objectives Cardiovascular events are the main cause of death in diabetic patients with severe peripheral vascular disease (Diab-PVD). This study was designed to evaluate the value of dipyridamole stress echocardiography (DSE) in predicting cardiac events in long term follow-up in Diab-PVD.
Methods A total of 130 diabetic patients, mean age 66 ± 10 years, unable to exercise because of PVD, underwent DSE according to the fast protocol (0.84 mg/kg in less than 10 min). Sixty-eight patients had IDDM and 62 NIDDM. We considered, at the follow-up of 52 ± 25 months, the following cardiac events: fatal and non fatal myocardial infarction, new occurrence of angina, heart failure. The predictive value of CV risk factors and DSE for long term CV events were tested in univariate and multivariate analysis.
Results Risk factors included known coronary artery disease (CAD) in 43 pts (33%), hypertension in 65 pts (50%), smoke habits in 41 pts (31%), dyslipidemia in 23 pts (23%). DSE was positive in 50/130 (38%) pts, 25 of them with known CAD. Cardiac events at follow-up occurred in 48 pts (37%): 28/48 (58%) in pts with positive DSE and 20/48 (42%) in pts with negative DSE. At the logistic multivariate regression analysis, considering all risk factors, only known CAD (p < 0.003, OR 3.1, CI 1.45–;6.74) and DSE (p < 0.003, OR 2.98, CI 1.42–;6.28) were significantly related to cardiac events at follow-up. The sensitivity, specificity, positive and negative predictive value of DSE for prognostic assessment were 58%, 73%, 56%, and 75% respectively.
Conclusion This study show that positive DSE is a good predictor of cardiac events in long term follow-up among the other CV risk factors present in Diab-PVD, but it is not superior as predictor to known CAD. Better tools are required to stratify CV risk in the diabetic population and to address prevention CV strategies.
296 Economic challenge of cardiovascular disease: cost-benefit ratio of primary and secondary prevention
Marcelo Nigri, Karina Stryjer, Patricia Cruz, Rafaela Neves, Aline Kimura, Vera Bejatto
Heart Institute and Victory Consulting, São Paulo, Brazil
Introduction The need of reducing morbidity and mortality due to coronary artery disease (CAD) is one of the most important challenges of modern medicine.
Objectives To reach this, public health measures are necessary, developed in a regional way, respecting peculiarities of populations from each country, region or state. This generates the need of costbenefit analysis of prevention, evaluating at one side the expenses due to the disease and at the other the benefits gained from prevention procedures and risks factors differents of CAD.
Methods Many methods have been used in cost-benefit analysis, from economic evaluation of intervention in CAD to the benefit due to the patients' returning to work, going through technics of analysis that involve the knowledge of annual cost of that specific treatment for each patient. Moreover, we also need to understanding about the models differents of atherosclerosis of world: 1) Classic model (USA and North of Europe)- Hypertension, dyslipidemia and tobacco. 2) Oxidative Stress (Easten Europe)- alimentation, alcoholism and smoking and 3) Insulin resistance (South of America and Mediterranean countries) –; Metabolic syndrome –; Diabetes type 2, hypertension, dyslipidemia and obesity.
Results The studies show some differences when interventions upon risk factors are analyzed: the cost per year of life gained of saved, for example, in lipid reduction, secondary prevention is favorable, while primary prevention is very expensive, being justified when other risk factors are present. Other type is patient choice himself treatment based of cost per quality adjusted year of life, for example, hypertension treatment and physical exercise are always favorable and better results of treatment. Tobacco cessation, although difficult to analyze, is also beneficial.
Conclusion Economic challenge is baseaded in health development and grow better of life quality of our patients. We must cust benefit can be favorate reaching the correct risk stratification of patient and restricting medication or diagnoses intervention when necessary.
305 Cardiovascular risk factors and mortality. Long-term follow-up (up to one year) in a preventive program carried out by occupational medicine
M. Nigri, K. Stryjer, P. Cruz, R. Neves, A. Kimura, V. Bejatto
Heart Institute and Victory Consulting
Objective The decrease in mortality due to cardiovascular diseases (CVD) has been achieved in the United States/ Europe and the same decrease has been happening in developing countries, thanks to favorable changes in lifestyle and risk factors. Despite such consideration, the volume of information available on the distribution and behavior of that type of disease and its risk factors in Brazil is still little.
Methods The assessment of changes in total cholesterol (TC), levels of blood pressure (BP), body mass index (BMI) and smoking was carried out, besides the occurrence of fatal (F) and nonfatal (NF) cardiovascular events, under dietary and behavioral intervention and long-term follow-up (up to one year) in a closed group, consisting of 322 emplooyes of companies of both sexes, with average age of 42.1 ± 7.1 years old. Actuarial curves were obtained to analyze the F and NF cardiovascular events.
Results The TC mean showed significant reduction due to dietary guidance. The smoking habit decreased significantly with behavioral changes. The mean of the BPs decreased significantly with a better detection and hygienic measures, and the adhesion by definite hypertensive people to the treatment showed na index of 56.6%. On the other hand, the BMI showed an expressive and gradual increase. The probability for the individuals to remain free of any cardiovascular event was of 98.1%, whereas for the fatal events, it was 99.2%.
Conclusion Those results prove that initiatives directed towards the prevention must be priorities, aiming at modifying the morbimortatility rates of CVD.
309 Diet quality and nutrition knowledge of subjects with diagnosed CVD in Polish population
A. Waskiewicz1, W. Piotrowski1, E. Sygnowska1, G. Broda2
1National Institute of Cardiology, Warsaw, Poland
2On behalf of WOBASZ investigators
Background Dietary treatment plays an important role in prevention of cardiovascular diseases (CVD).
Objectives To characterize the diet quality and nutrition knowledge of subjects with diagnosed CVD at population level in Poland.
Methods Within the frame of the National Multicenter Health Survey (WOBASZ), a representative sample of whole Polish population aged 20–;74 (3509 men and 3907 women) was screened in years 2003–;2005. A subsample of 803 persons (M−430, W−373) with a clinical history of myocardial infarction and/or coronary artery disease and/or heart failure and/or stroke and/or arrhythmia and/or PCI and/or coronary bypass surgery was analysed. Nutrients intake, supplements use and knowledge on non-pharmacological methods of CVD prevention were performed according to study protocol.
Results It was found, that the average diet of the adult Polish citizens with established CVD was not balanced concerning the intake of nutrients. The average daily food ration was characterized by high atherogenicity (fat M−36% energy/W−34% energy), saturated fatty acids (13,3%/12,6% respectively) and insufficient calcium (499 mg/433 mg) and magnesium (262 mg/206 mg) as well as vitamin B1 (1,3 mg/0,9 mg), B2 (1,5 mg/1,2 mg), B6 (1,9 mg/1,4 mg) and folic acid (259 ug/215 ug) intake. The dietary cholesterol (288 mg/206 mg), vitamins A (1071 ug/1041 ug), C (68 mg/78 mg) and E (10 mg/8 mg) were consumed in the recommended doses.
The use of vitamin/mineral supplements was reported by 7,5% men and 10,2% women. Proportion of patients with dietary knowledge about: weight reduction (M−33%/W−35%), salt reduction (23%/21% respectively), reducing fat intake (37%/36%), regular consumption of fruits and vegetables (23%/23%) was very low.
Conclusions The diet quality of subjects with diagnosed CVD did not meet RDA (dietary recommended allowances) for secondary CVD prevention. The average food ration was characterized by high fat intake and insufficient minerals (calcium, magnesium) and vitamins (group B and folic acid) intake. The dietary knowledge was very poor. Dietary advice should be incorporated into the medical treatment given to all patients with CVD.
316 Cardiorespiratory fitness, traditional and emergent risk factors in a Chilean primary prevention cardiology unit
M. Acevedo1, V. Kramer1, L. Orellana1, G. Chamorro1, M. Fernández1, P. Arnaíz1, C. Navarrete1, F. Marques1, M. Bustamente1.
1Department of Cardiovascular Diseases, Pontificia Universidad Católica de Chile, Santiago, Chile
Cardiorespiratory fitness is associated with a favorable response in most modifiable risk factors (RF). Scarce data, however, are available about its impact on emergent risk factors. In Chile, sedentary lifestyle is highly prevalent, reaching more than 80% in subjects between 45–;64 in the last national survey 2003.
Objectives To determine the impact of cardiorespiratory fitness on traditional and emergent RF in subjects seen in a primary prevention Cardiology Unit.
Methods 1973 subjects (1271 men), without history of CHD or CVD, were prospectively studied (mean age = 56 ± 13 yo). We made a survey about CV risk factors and determined body mass index, waist circumference, systolic and diastolic blood pressure, fasting lipids, glycemia, ultrasensitive C-reactive protein (CRPus) and fibrinogen. Cardiorespiratory fitness was determined with a maximal treadmill exercise testing. Fitness was divided in tertiles of maximal metabolic equivalents (METs).
Results 44% of the subjects were overweight/obese, 22% smokers, 5% diabetics, 31% hypertensives and 63% dyslipidemics. 75% of the subjects had a sedentary lifestyle defined by < 3 times per week of aerobic exercise. Men and women in the lowest fitness tertile (METS < 10) presented with significant higher: BMI (p = < 0.0001), systolic and diastolic BP (p = < 0.0001), total cholesterol (p < 0.01), glycemia (p = < 0.0001). HDL was lower in men (p < 0.01) and women in the lowest fitness tertile (p = 0.02). CRP (p = < 0.0001) and fibrinogen (p = < 0.0001) were higher in individuals in the lowest fitness level compared to those in the highest.
Conclusions Our findings show that a better level of fitness associates not only with improved level of traditional RF, but also with an improvement in emergent RF. This findings point out the importance of public health policies in order to promote physical activity in the community.
337 The Importance of carotid ultrasound in the risk stratification of patients with atherosclerotic cardiovascular disease in clinical practice
F. Mitu1, M. Mitu2, M. Turiceanu1, T.A. Caliap2, C.G. Leatu2
1University of Medicine, Iasi, Romania
2Rehabilitation Hospital, Iasi, Romania
The stratification of cardiovascular risk is important both in primary and secondary prevention. In the clinical evaluation, besides the well-known risk factors, the European Guide of Cardiovascular Prevention recommends the identification of additional markers of risk, one of them being the detection of atherosclerotic alterations by carotid ultrasound examination.
Objectives of the study were: assessment of carotid ultrasound alterations at patients with known cardiovascular disease; their relation with the other risk factors, the clinical status and echocardiography.
Methods The study included 144 patients, aged 41–;80 (84 males, 60 women) with cardiovascular disease (stable angina, myocardial infarction, peripheral arterial disease, arterial hypertension). Risk factors as smoking, hypercholesterolemia, diabetes mellitus, obesity have been determined, followed by a clinical assessment and echocardiographic examination. The ultrasound examination of the extra cranial carotid arteries included measurement of IMT of the common carotid arteries, the identification of atherosclerotic plaques and the presence of stenoses. The plaques were considered if the IMT was more than 1.3 mm.
Results Patients with IMT > 0.8 are older (61.5 ± 8.2 vs. 56.1 ± 8.2 years, p = 0.001); the prevalence of arterial hypertension is greater (63.8% vs. 21.6%, p = 0.05), and at an IMT of more than 1.1 mm all were hypertensive; the association with peripheral arterial disease is significant at the IMT = 0.8 mm (23.6% vs. 4.8%, p = 0.01). The relationship with echocardiographic markers of left ventricular hypertrophy is present at an IMT of 0.8 mm and is evident at IMT ≥ 1 mm (interventricular septum 13.2 ± 3 vs. 12 ± 2.3, p = 0.05; left ventricular wall 14 ± 5.4 vs. 12 ± 1.7, p = 0.01; left ventricular mass 323 ± 94 vs. 282 ± 68, p = 0.03), and also the relation with the degree of diastolic dysfunction expressed by E/A ratio (0.71 ± 0.24 vs. 0.99 ± 0.39, p = 0.001). The presence of atherosclerotic plaques is correlated with gender (45.1% at male vs. 24.3%, p = 0.01) and older age (61.7 ± 8.6 vs. 56.2 ± 8.5 years, p = 0.001). The IMT and carotid plaques are not significant correlated either with risk factors as smoking, hypercholesterolemia, diabetes mellitus or clinical conditions as myocardial infarction and angina.
Conclusions IMT greater than 0.8 mm is a marker of increased cardiovascular risk, associated with age, presence of peripheral arterial disease, arterial hypertension, left ventricular hypertrophy and diastolic dysfunction. IMT seems to be a more reliable index of cardiovascular risk than carotid plaques. Measurement of IMT is easy to be done in clinical practice, and is recommended for more accurate risk stratification at patients with atherosclerotic cardiovascular disease.
338 Obesity-cardiovascular risk factor in adolescents-prevalence and relationship with other cardiovascular risk factors-results from a survey in a high school from Oradea, Romania
Vatca, L1, Zdrenghea, D2
1University of Oradea, Romania
2Department of Cardiology, Rehabilitation Hospital, University of Medicine, Cluj-Napoca, Romania
Objectives This study has the aim of describing the prevalence of overweight and obesity among adolescents and also particular aspects of cardiovascular risk factors, especially hypertension, dyslipidemia and smoking in adolescents who are above normal weight comparing to normoponderals.
Methods The study sample included 721 students 390 (54,1%) girls and 331 (45,9%) boys aged between 15–;19 years from a high school in Oradea, Romania. For all of them were measured: weight, height, blood pressure and cholesterol blood level. They also were invited to answer a questionnaire consisting of questions about lifestyle: smoking, physical activity, nutrition and also about family history for cardiovascular disease. In overweight and obese adolescents we determined blood levels for: HDL-cholesterol, LDL-cholesterol, triglycerides, fasting glucose. Same samples were determined for 80 normoponderals subjects.
Results In our group, prevalence for overweight was 8% with no difference between boys and girls (9,5% versus 9%). Obesity's prevalence was 4,9%;there was a significant difference between genders 7,4% in boys and 4,1% in girls (p < 0,001). Comparing to normoponderals in overweight and obese there were significant differences in blood level for triglycerides (122,2 ± 13,7 mg/dl versus 88,0 ± 9,4 mg/dl p < 0,01), LDL-cholesterol (118,2 ± 13,3 mg/dl versus 76,8 ± 8,7 mg/dl p < 0,01) and HDL-cholesterol (44,7 ± 6,2 mg/dl versus 33,3 ± 4,7 mg/dl p < 0,05). There were no differences for fasting glucose and total cholesterol. Hypertension's prevalence is double among obese and overweight adolescents comparing to normoponderals (19,4% versus 8,8%). Smoking practice is 1,3 more frequent in adolescents above normal weight comparing with those with normal weight. Among obese and overweight adolescents, in girls smoking is 4,2 more frequent than in boys-probably because they practice this for loosing gain.
Conclusions
Overweight and obesity have a high prevalence in adolescents.
From very beginning in life, in adolescence and probably in childhood, overweight and obesity is associated with accelerated atherosclerosis proved by an altered lipidic profile.
Hypertension and smoking are frequent in adolescents with weight above normal range.
Because of tracking phenomenon for cardiovascular risk factors and because the atherosclerosis starts early on life are necessary efforts to prevent obesity and its comorbidities as early as we can.
349 Prognostic value of glycaemia at admission in acute coronary syndrome patients
Monteiro S, Monteiro P, Costa S, Gonçalves F, Gonçalves L, Freitas M, Providencia L
Cardiology department, Coimbra University Hospital, Coimbra, Portugal
Introduction High glycaemia at hospital admission in acute myocardial infarction (AMI) patients is common and associated with an increased risk of in-hospital and post-discharge death, both in subjects with and without diabetes.
Aim To evaluate, in an acute coronary syndrome (ACS) population, the relationship between glycaemia at hospital admission and in-hospital mortality.
Population and methods Retrospective analysis of a database containing 711 consecutive patients admitted to a single coronary care unit for acute coronary syndrome between May 2004 and May 2006. Our population was divided in four groups according to the quartiles of glycaemia at admission (Q1 < 5.77, Q2 5.77–;7.0, Q3 7.0–;9.22, Q4 ≥ 9.22 mmol/L).
Results There were no significant differences with regard to gender, risk factors, lipid profile, TIMI risk score at admission, reperfusion strategies and medication prescribed (except for the use of beta-blockers, lower in patients with higher glycaemia at admission). Higher glycaemia at admission was strongly correlated with higher age, body mass index, creatine kinase (CK), creatinine, C-reactive protein levels and lower left ventricular ejection fraction. In-hospital mortality in the four groups was 1.2%, 3.2%, 3.9%, and 9.4%, respectively (p < 0.001). After multivariate regression analysis (Figure 1), higher age, CK and C-reactive protein levels were independent predictors of in-hospital mortality.
Conclusion These data suggest that glycaemia at admission is an independent predictor of in-hospital mortality, in a mixed ACS population. Its routine determination may contribute to a better risk stratification in this population.
352 Risk of atherosclerosis in general Czech population is very high-preventive examinations
M. Tomeckova1, H. Grünfeldova2, J. Peleska1, P. Hanus2, P. Martinkova1
1Centre of Biomedical Informatics, Institute of Computer Science, Academy of Sciences of the CR, Prague, Czech Republic
2Centre of Biomedical Informatics, Municipal Hospital, Èáslav, Czech Republic
Objectives Cardiovascular atherosclerotic diseases (AD) are the leading course of the morbidity in developed countries till now. In most cases, the prevention is cheaper than the treatment. The prevention of AD is in the first instance concerned with the healthy life-style.
Methods In our outpatients' cardiologic department we proposed a preventive examination regarding the risk of the development of AD to the resident population in the region. The group of nonrandomly selected people consists of 980 people (428 = 43.7% men, mean age 48.01 years, and 552 = 56.3% women, mean age 49.35 years).
Results The prevalence of risk factors (RF) in this population is very high: it is 19.62% smokers and 11.71% ex-smokers. 49.64% men and 31.54% women have BMI > 25, and 24.82% men and 25.6% women were obese –; BMI > 30. Only 53.1% people have a moderate or average physical activity, 48.3% men and 43.4% women are without any leisure physical activity. With overweigh and obesity some other RF are connected: higher systolic and diastolic blood pressure, higher values of lipids, uric acid and blood sugar –; all these parameters with significant results against the people non-overweight (p < 0.0001). A fasting blood sugar > 6.0 mmol/l was detected in the 41 subjects without history of diabetes mellitus (5.6%), 257 subjects (32.8%) without history of hyperlipidemia had total cholesterol > 5.2 mmol/l.
Conclusions Neither worldwide nor in the Czech Republic the situation in the prevention of AD is satisfactory. We confirmed a very unfavourable atherosclerotic risk profile in the healthy middle-aged Czech population. In accordance with a great epidemiological study, women are more interested in the preventive examination and in the preventive arrangements.
The paper was partly supported by the project 1M06014 of the Ministry of Education, CR.
354 Evaluation of development and progression markers of chronic heart failure in patients with acute coronary syndrome
Koziolova N.A., Polyanskaya E.A.
Perm State Medical Academy, Perm, Russia
Objective Research of CHD risk factors in patients with acute coronary syndrome and detection of their correlation connected with the development and progression of chronic heart failure.
Methods Clinical single-stage cohort study was conducted. 60 patients with acute coronary syndrome (unstable angina) without myocardial infarction in medical history were examined. Among them there were 32 men (53%) and 28 women (47%) aged from 43 to 75. The following risk factors, concomitant diseases and complications were registered in patients: smoking, heredity of cardiovascular disease, hypertension, stroke in medical history, clinically significant peripheral arterial disease, diabetes mellitus 2 type, nephropathy, chronic renal insufficiency, clinical symptoms of chronic heart failure in medical history. Waist, weight, height, body weight index were determined. Lipid spectrum including apolipoproteins ApoA1, ApoB100, lipoprotein (a), and inflammation indices (C-reactive protein, fibrinogen) were evaluated in patients. In patients evidence of chronic heart failure were determined depending on presence of systolic dysfunction (ejection fraction is less than or equals to 45%) according to echocardiography conducted within 3 days from the beginning of development of acute coronary syndrome. Depending on the presence of systolic dysfunction patients were divided into two groups.
Results The first group of patients with ejection fraction that is less than or equals to 45% was formed of 19 persons (31.7%), the second group was formed of 41 persons (68.3%). Clinic signs of chronic heart failure in medical history, diabetes mellitus 2 type and stroke in medical history were marked reliably more often in patients of the first group (p < 0.05). Body weight index of patients in the first group was reliably higher than in the second group and made up 27.91 +/−2.76 and 24.48 +/−4.78 kg/m2 respectively (p = 0.05). Levels of total cholesterol, triglycerides, ApoB100 apolipoprotein, lipoprotein (a) in the first group of patients reliably did not differ from the similar indices in the second group. Reliable differences between the groups were detected according to the level of high-density lipoprotein: in the first group this figure made up 0.83 +/−0.14 mmole/l, in the second group −0.95 +/−0.20 mmole/l (p = 0.023); according to the level of ApoA1 apolipoproteins: in the first group this figure made up 122.32 +/−19.76 mg/dl, in the second group −111.02 +/−18.05 mg/dl (p = 0.032). No reliable differences between the groups were found according to the levels of fibrinogen and C-reactive protein.
Summary In patients with acute coronary syndrome (unstable angina) chronic heart failure that manifests itself by systolic dysfunction was registered in 31.7% of cases. Chronic heart failure and stroke in medical history, diabetes mellitus 2 type, body weight index more than 27 kg/m2 were marked reliably more often in patients with acute coronary syndrome in combination with systolic dysfunction. Compared with the patients with normal systolic function of the left ventricle the level of high-density lipoprotein was reliably lower and the level of ApoA1 apolipoproteins was reliably higher in patients with systolic dysfunction in combination with acute coronary syndrome.
358 Is it possible to improve the cardiovascular risk profile in patients with cardiovascular diseases and type 2 diabetes by a complex intervention?
B. Petrlova, H. Rosolova, I. Sipova, P. Sifalda, J. Simon
University Hospital, Pilsen, Czech Republic
Objectives Patients with type 2 diabetes (DM 2) and concomitant cardiovascular disease (CVD) are considered to have the highest risk for new atherothrombotic CV events among the whole population. Aim of the study was to asses the efficacy of Complex Intervention Programme (CIP) and an addition of fenofibrate to the already constituted drug treatment in diabetics with evidence of CVD.
Method Patients followed by their GPs, cardiologists and diabetologists in the Pilsen city area were included. All data i.e. personal history, anthropometric and laboratory parameters and current medication were extracted from the patients' medical reports. The CIP consists of educational interview of lifestyle (especially diet recommendation, smoking intervention and regular weekly physical exercise offer) and start hypolipidemic therapy by micronised fenofibrate 267 mg daily added to the current therapy.
Results We recruited 420 patients with DM 2; about 227 (54%) had evidence of concomitant CVD (105 males, mean age 70 ± 8 y., and 122 females, mean age 71 ± 9 y.). Only about 40% included patients received statins. No changes in antihypertensive and statin therapy were realized during the investigational period. After 6 months of CIP the risk profile and risk factors control of diabetic patients with CVD improved. Recommended fasting plasma lipid levels, i.e. total cholesterol < 4.5 mmol/L, LDL-chol < 2.5 mmol/L, TG < 1.7 mmol/L and HDL-chol > 1.0 in men and 1.3 mmol/L in women, were achieved before CIP only in 14% males and 17% females, after CIP in 60% of the both sexes. Blood pressure control (i.e. BP below 130/80 mmHg also improved from 6% to 18% in males and from 9% to 20% in females, although any change of antihypertensive therapy was realized.
Conclusion The results provide the evidence that the special care in high risk patients is fruitful; improvement in treatment compliance is also suggested. The number of DM 2 patients using statins in secondary care was poor, nevertheless, fenofibrate hypolipidemic treatment was much more successful in hypolipidemic intervention than suspected.
Supported by the Research Grant IGA Ministry of Health CZ 8279–;3 (2005–;2007).
360 On issues of prevention and fighting smoking in Georgia
N. Burkadze1, N. Beritashvili1, M. Perashvili1
1Preventive Cardiology Department of Academician M. Tsinamdzgvrishvili S/R Institute of Cardiology, Tbilisi, Georgia
Objectives To research the prevalence of smoking in Georgian population and evaluate effectiveness of anti-smoking measures
Method The research considered representative groups of adults and youth (12–;18 years) of both sex in Georgia (14 768 people total). The method used was personal interviews and questionnaires in adults and anonymous questionnaires with youth. In addition, there were conducted all know anti-smoking activities with identified smoker groups on permanent, stage-by-stage basis.
Results In 1990s 75% of cities' male population were smokers, in respective village population 59%. With female group this figure varied from 8–;12%, and with youth it was 14%. In 1990–;98 the number of smokers reduced to 40–;38% due to the decrease of social-economic conditions in the country. In recent years the number has increased again in males up to 63% in females 47% due to the stable social-economic situation. Furthermore the difference in figures between the city and village population disappeared and the smokers' age became younger. If several years ago boys started smoking in the age of 15, now both girls and boys start smoking at the age of 12. In city schools 55% of boys and 35% of girls aged 14–;18 smoke. The results of 15-year dynamic observation and active intervention with observed population showed positive dynamics in decrease of frequency and intensity of smoking.
Conclusion Many years of observation showed that anti-smoking campaigns should be complex and integrated. Only verbal consultations and using visual aids have not proven to be effective in fighting this habit; it also needed intervention with pharmacotherapy. In schools it is necessary to have social workers/teachers that would be responsible for the introduction of healthy lifestyles principles with special emphasis on smoking. Real fight with smoking can only begin when this issue is seriously considered on governmental level.
362 Emergency hospitalizations and SCORE indexes at hypertensives with metabolic syndrome
M. Orynchak, E. Neiko, V. Neiko, N. Artemenko, O. Chovganyuk, O. Kocherzhat
Ivano-Frankivsk State Medical University, Ivano-Frankivsk, Ukraine
Objectives Hypertensives with metabolic syndrome are usually at high risk of cardiovascular disease (CVD). The purpose of the study was to investigate the relationship between the frequency of emergency hospitalizations and levels of Systematic Coronary Risk Evaluation (SCORE) indexes at hypertensives with metabolic syndrome.
Methods The study included 105 subjects, aged 43–;68 years, with 3 or more signs of the metabolic syndrome by ATPIII criteria (2001). The control group consisted of 10 healthy people. Indexes of 10 year risk of fatal CVD by SCORE (2003) for high risk regions of Europe by gender and age, systolic blood pressure (BP), total cholesterol, smoking status and the ambulatory BP monitoring, body mass indexes (BMI), serum triglycerides and plasma glucose levels were measured.
Results During one year of observation 23 patients (21.90%) had symptoms of cardiovascular events, requiring hospitalization and intensive medical therapy. Among them 7 patients (30.43%) had BMI levels in the range of overweight and were equal to 27.00 ± 1.90 kg/m2 (group I). 16 patients (69.57%) had BMI in the range of obese grads I–;II and were equal to 35.0 ± 4.0 kg/m2 (group II). The mean BP and glucose levels did not differ between the groups. Serum total cholesterol and triglycerides levels were higher than 4.5 mmol/l and 1.7 mmol/l in 5 (55.56%) cases of group I and 10 (62.50%) cases of group II respectively. The indexes of SCORE were equal to 0–;4% (low risk) in group I and > 5% (high risk) in group II. SCORE indexes decreased in all patients after 2 weeks of drugs treatment but remained higher than 5% in 8 cases (50.00%) in group II.
Conclusions Emergency hospitalisations are more frequent among hypertensives with obesity and dyslipidemia and index of SCORE is higher than > 5%. Antihypertensive treatment promotes a decrease of SCORE levels.
369 The ten most preferred drugs in the prevention and treatment of cardiovascular diseases
B. Georgiev, N. Gotcheva, M. Hazan, I. Ivanov
National Heart Hospital, Sofia, Bulgaria
Very often physicians prescribe drugs, chosen on the basis of their own clinical experience. The drugs, chosen by them, are not always the ones that have been shown to improve morbidity and mortality outcomes in large trials.
Objective Of the study was to establish which cardiovascular drugs Bulgarian physicians most commonly prefer.
Methods Over a period of one year, using an anonymous questionnaire, we assessed which were the 10 cardiovascular drugs, most commonly preferred by Bulgarian GPs and specialists. The study included 626 GPs, looking after a total number of 144 459 cardiac patients, 90 outpatient cardiologists, and 135 hospital specialists. A classification was made, based on a score system analysis.
Results GPs gave first place to a generic Enalapril (2817 points), followed by short-acting Metoprolol (1988 points) and Indapamide (1748 points). The top ten also included 2 other generic Enalapril and cheaper antihypertensive and generic antiischemic products. The group of outpatient specialists gave first place to Indapamide (242 points), followed by short-acting Metoprolol (205 points). Their top ten included the original Carvedilol (152 points), Perindopril (137 points), and Metoprolol succinate (107 points). Hospital specialist preferred most the short-acting Metoprolol. The top ten included 2 generic forms of Enalapril, 2 original beta-blockers, and Perindopril.
Conclusions Bulgarian GPs choose to prescribe generic drugs with lower prices. Outpatient specialists use generic, as well as original drugs, but they also take into consideration the evidence of their efficacy. Hospital specialists prefer drugs with proven cardioprotective efficacy. Still underpreferred are long-acting beta-blockers and the newer ACE inhibitors with conclusive evidence from large clinical trials. Unfortunately, the lists of the preferences of all 3 groups of physicians do not include statins, as well as aspirin. The explanation could be that hypertension is the most common disease and, respectively, the most commonly prescribed drugs are hypertensive agents.
384 EUROACTION: the effectiveness of a 1-year preventive cardiology programme in general practice to achieve the lifestyle goals in cardiovascular disease prevention
J. Jones1,4, A. Mead1, C. Jennings1, A. Holden1, K. Kotseva1, S. Connolly1, D. De Bacquer2, G. De Backer2, T. Collier3, D. Wood1, on behalf of the EUROACTION Study Group
1Department of Cardiovascular Medicine, Imperial College, London, UK
2Department of Public Health, University of Ghent, Belgium
3Department of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK
4School of Health Sciences and Social Care, Brunel University, London, UK
Objectives EUROACTION is a cluster randomised controlled trial of a preventive cardiology nurse-led programme in general practice. The programme aims to manage patients and their partners to the European lifestyle, risk factor and therapeutic targets.
Methods In six European countries one pair of matched practices was randomised to receive the EuroAction programme or usual care. High risk individuals (I. HEARTSCORE risk ≥ 5% over 10 years, II treated hypertension/dyslipidaemia and III diabetes) over the age of 50 were identified. Intervention patients and partners were invited to attend a nurse-led 1-year comprehensive risk factor and lifestyle management programme. All patients and partners were reviewed at 1 year in intervention (INT) and usual care (UC). Lifestyle measurement tools included breath carbon monoxide, a food habit questionnaire and 7-day physical activity recall.
Results 67% of all patients identified attended the final assessment (1019/1257 INT, 1005/1752 UC). The majority of eligible partners (225/356 INT, 363/542 UC) also attended. Using random effects meta-analysis (REML estimation) differences in proportions achieving goal were compared.
Proportions of patients and partners achieving smoking, dietary and physical activity goals at 1-year
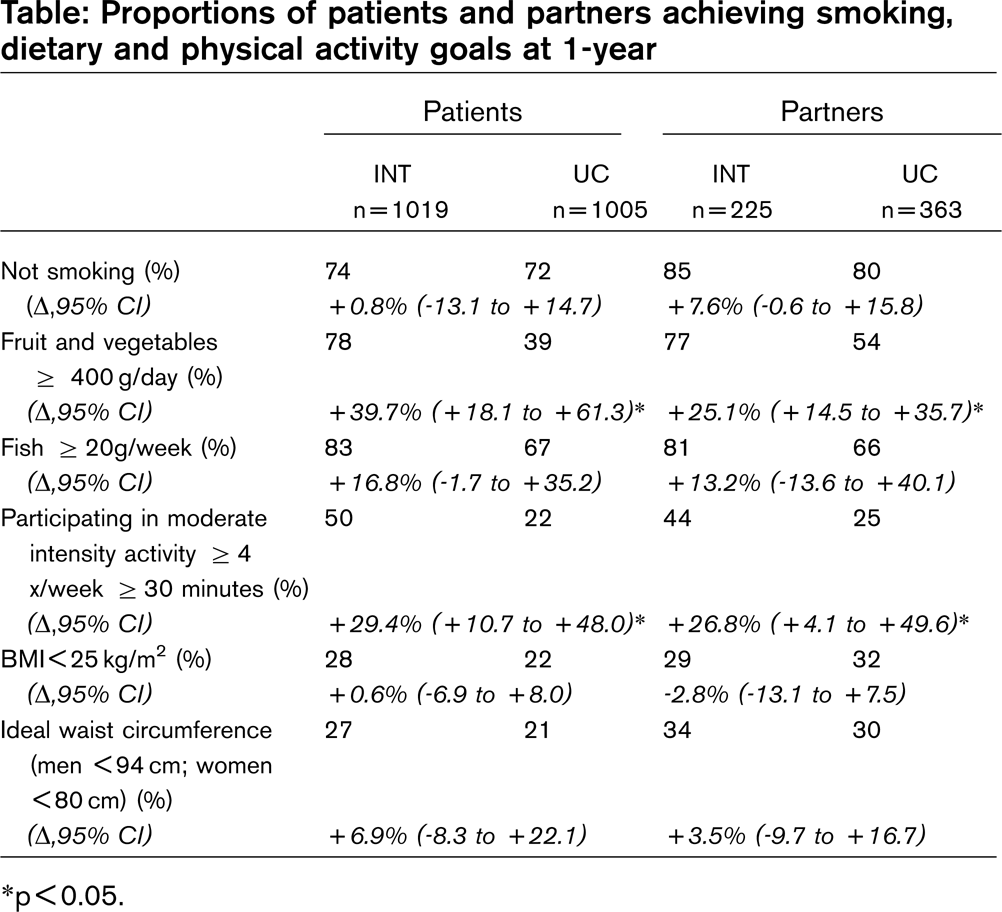
∗p < 0.05.
In those patients with a BMI ≥ 25 kg/m2 and waist circumference above target at the initial assessment the intervention achieved greater reductions in weight [−0.56 kg/m2 (−0.86 to −0.25)] and waist circumference [−1.76 cm (−3.04 to −0.49)] than usual care.
Conclusions EUROACTION has demonstrated that it is possible to improve on usual care. This preventive cardiology programme helped more high risk patients and their partners achieve healthier lifestyle changes, especially for diet and physical activity, together with reductions in weight and central adiposity, thereby reducing the risk of cardiovascular disease in everyday clinical practice.
393 EUROACTION: achieving lifestyle behaviour targets in a 16 week multidisciplinary cardiovascular prevention and rehabilitation hospital programme. One year results
A. Mead1, J. Jones14, K. Kotseva1, S. Connolly1, C. Jennings1, A. Holden1, D. De Bacquer2, G. De Backer2, T. Collier3, D. Wood1 on behalf of the EuroAction Study Group
1Department of Cardiovascular Medicine, Imperial College, London, UK
2Department of Public Health, University of Ghent, Belgium
3Department of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK
4School of Health Sciences and Social Care, Brunel University, London, UK
Objectives EUROACTION is a European Society of Cardiology cluster randomised controlled trial of a nurse-led multi-disciplinary preventive cardiology programme which aims to manage coronary patients and their families to the European lifestyle, risk factor and therapeutic targets.
Methods In each of six European countries, one pair of matched hospitals was randomised to intervention (INT) or monitored for usual care (UC). All new coronary patients and their partners were invited to attend a 16 week comprehensive risk factor and lifestyle management programme. Measurement tools included breath carbon monoxide, a food habit questionnaire, 24hr dietary recall, 7-day physical activity recall. All patients and partners were reviewed at 1 year.
Results 946 (60% of those eligible) patients and 401 (61% of those eligible) partners in INT 994 (66% of those eligible) patients and 335 (64% of those eligible) partners in UC attended the final assessment. Using random effects meta-analysis (REML estimation) differences in proportions achieving goal were compared.
Proportions of patients and partners achieving smoking, diet and physical activity goals at 1 year
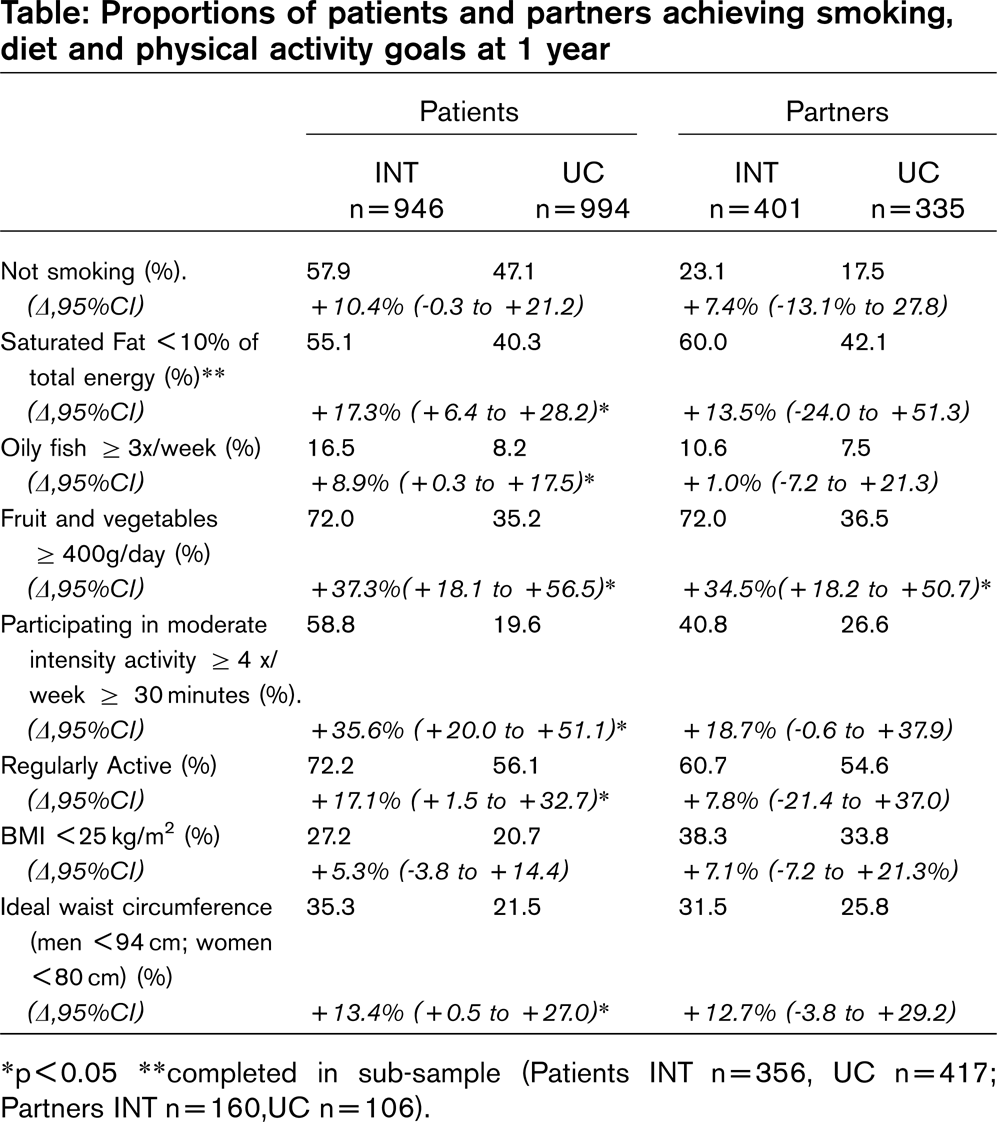
∗p < 0.05 ∗∗completed in sub-sample (Patients INT n=356, UC n=417; Partners INT n=160,UC n=106).
Conclusions EUROACTION has demonstrated that it is possible to improve on usual care. This preventive cardiology programme helped more coronary patients and their partners achieve healthier lifestyle changes, especially for diet and physical activity, together with reductions in weight and central adiposity, thereby reducing the risk of cardiovascular disease in everyday clinical practice.
403 EuroAction: achieving blood pressure, lipid and glucose targets in a 16 week multidisciplinary cardiovascular prevention and rehabilitation hospital programme - one year results
K. Kotseva1, S. Connolly1, C. Jennings1, A. Mead1, J. Jones1,4, A. Holden1, D. De Bacquer2, G. De Backer2, T. Collier3, D. Wood1 on behalf of the EUROACTION Study Group
1Department of Cardiovascular Medicine, Imperial College, London, UK
2Department of Public Health, University of Ghent, Belgium
3Department of Statistics, London School of Hygiene, London, UK
4School of Health Sciences and Social Care, Brunel University, London, UK
Objectives EUROACTION is a cluster randomised controlled trial of a nurse-led multi-disciplinary preventive cardiology programme which aims to manage coronary patients and their families to the European lifestyle, risk factor and therapeutic targets for cardiovascular disease prevention.
Methods In each of 6 European countries, a pair of comparable general hospitals was randomised to receive the EUROACTION intervention programme or to be monitored for usual care. Consecutive coronary patients were proactively identified by the study nurse and invited with their partners to attend the 16 week EUROACTION programme with a repeat assessment at one year.
Results 60% (946/1589) of all eligible patients and 61% (401/661) of all eligible partners in Intervention (INT) hospitals and 66% (994/1499) of all eligible patients and 64% (335/522) of all eligible partners in usual care (UC) hospitals attended the final assessment. Using random effects meta-analysis (REML estimation) differences in proportions achieving goal were compared.
Proportions of patients achieving the European blood pressure, cholesterol, glucose and therapeutic targets for cardiovascular disease prevention
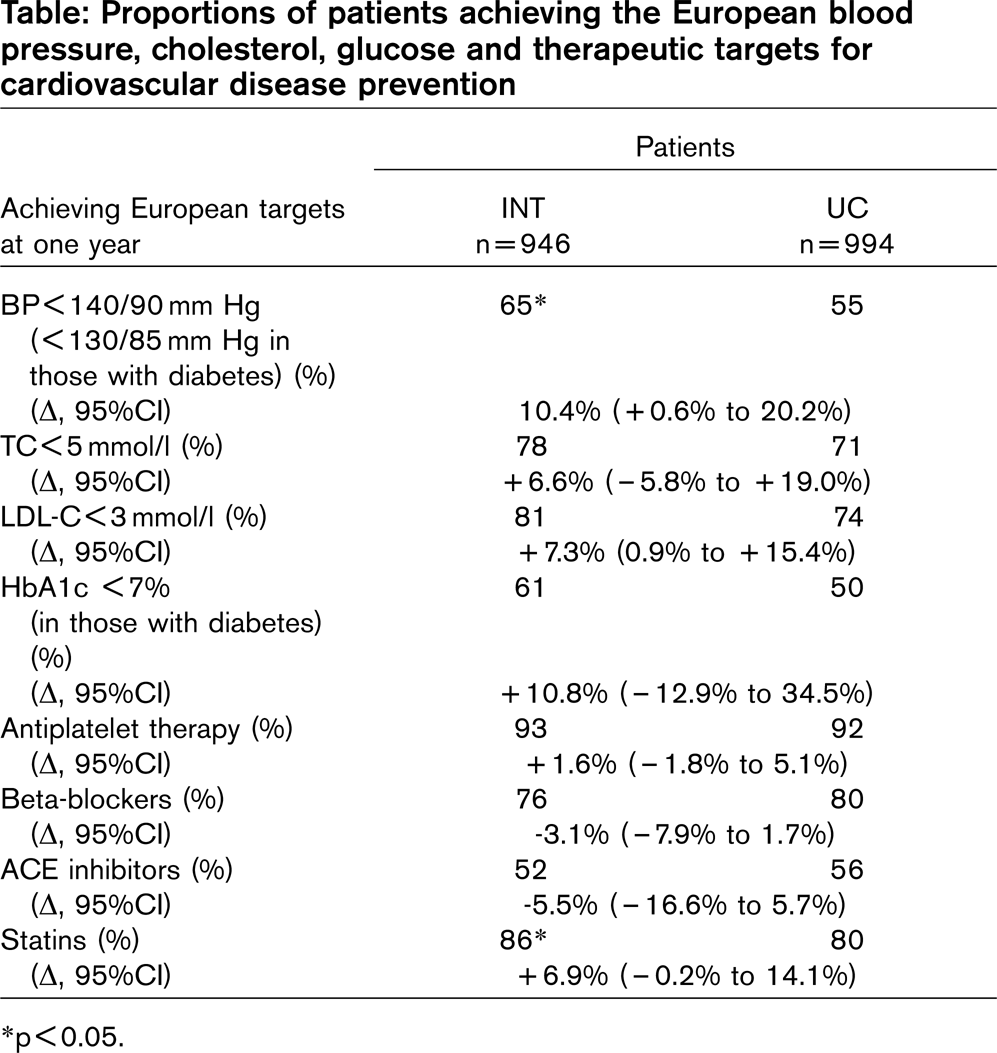
∗p < 0.05.
Similar trends were seen for risk factor management, and in particular blood pressure control, in partners. However, proportion of partners using cardio-protective drug therapies was much lower than in patients.
Conclusions The EUROACTION programme helped coronary patients and their families to achieve better blood pressure, lipid and glucose control although significant for blood pressure only. There was a significant increase in the use of statins. EUROACTION achieved its overall aim in raising standards of preventive cardiology care for coronary patients and their partners in everyday clinical practice which will reduce their risk of further cardiovascular disease.
404 A west of Ireland community model of heart disease prevention
I. Gibson1, K. Daly2, J. Crowley2, P. Nash2
1Croi, The West of Ireland Cardiology Foundation
2Consultant Cardiologist, University College Hospital, Galway, Ireland
Background In 2004 as part of it “Action against Heart Disease” strategy, Croi the West of Ireland Cardiology Foundation in partnership with the Cardiology Department of University College Hospital, Galway, established a nurseled primary prevention programme called “Heart Smart, Your Heart is your Life”. The programme, which was introduced on a pilot basis, aimed through lifestyle and behaviour modifications, to reduce the risk factor profile of individuals living in the West of Ireland.
Objective To examine the effectiveness of “Heart Smart” using measures of risk factor modification and behaviour change.
Methods The programme involved:
Opportunistic targeting of high-risk individuals i.e. males/females over 40 with 1 or more risk factors for heart disease, through a variety of community based settings, e.g. Community Groups, Agricultural Mart Co-operatives, Workplaces etc.
Assessing the non-modifiable and modifiable risk factors for heart disease using a standardised approach (Cholesterol, Glucose, B.P, BMI as well as lifestyle risk factors).
Recording the results on a Personal Record Card and explaining/discussing results with the individual.
Providing lifestyle advice using techniques of motivational interviewing, reinforced by the “Croi Healthy Heart Kit”.
Encouraging individuals to agree on lifestyle changes that could be realistically achieved and to set objectives for change.
Referring individuals with elevated risk factors to General Practice, in accordance with a protocol that is based on the European Guidelines for CVD Prevention (2003).
Follow up of individuals 6 months later at the original location/site of assessment.
Results The results of this study proved to be very positive. A total of 333 people were invited to attend for a follow up visit with a response rate of 212 (62.7%).
Over 50% of people who were referred to the G.P. attended as advised.
A total of 34.4% of people reached the recommended target levels for cholesterol, with 23% of people reaching the recommended target levels for blood pressure.
Over 70% of people self reported improvements to diet and 40% self reported improvements to exercise.
Conclusion This model of primary prevention is uniquely innovative in that it represents a swing away from the more traditional methods of health service delivery to that of a more novel approach. Motivating & empowering individuals, is essential for positive behaviour change. It is envisaged that by adopting a collaborative approach and working with the Health Service Executive, West the true value of primary prevention will be realised.
414 Impact of a heart failure outpatient program on clinical status, quality of life and self-care adherence
L. De La Rosa, J. Delgado,
Servicio de Cardiología, Hospital Central de Maracay, Venezuela
A program of frequent visits, increment of pharmacological treatment and education on self-care was applied in heart failure (HF) patients and the results were assessed by different instruments in a group of them.
Objectives To asses changes in readmissions, quality of life (QOL) and self-care behaviour after the program.
Patients and Methods In twenty-seven patients (57 ± 13 years old, 74% males) with advanced HF of different aetiologies (60% ischemic and hypertensive), 70% in NYHA Class III–;IV, three different interventions were applied: 1) treatment according to HF guidelines 2) frequent visits and 3) instruction on self-care conduct. Changes were assessed by: a) number of hospitalisation in previous year compared with readmissions during the program. b) changes in response to a validated questionnaire, EuroQOL (QOL European Scale) referring to 5 dimensions of health and with a visual analogue scale (rather like a thermometer) rating patients appreciation of well-being. c) individuals and relatives instruction on self-care conduct assessed using the European Heart Failure Self-Care Behaviour Scale (1999, Jaarsma et al).
Results Media permanence in the program was 8 month. Readmissions decreased by 80%. Seventy percent was in Class I at the end of the period. According to the QOL scale, 81% better health status was present, and, in self-health perception, the initial value was 30 and the final value was 79. In self-care a 22% of improvement was present, especially in initial Class IV patients.
Conclusions Improvement was evident after exposure to the program, and the use of the two instruments permitted an objective assessment of the benefit obtained, that is, prevention of progress of symptoms and severity of HF.
422 Effectiveness of a preventive strategy performance based on telephone structured surveys in a labor population with high cardiovascular risk. Two years follow-up
∗A. García García; E. Calvo Bonacho;
Introduction and aim Routine medical checkups in workers represent an opportunity for the early screening of cardiovascular risk factors. IBERMUTUAMUR Cardiovascular Investigation Plan, started in May 2004, aims to detect, stratify and prevent cardiovascular risk in workers affiliated to a single Mutua (benefit society complementary to the Public Health Service). The present study was aimed at investigating the effectiveness of telephone surveys in our high cardiovascular risk labor population at modifying cardiovascular risk factors.
Subjects and methods 5.634 workers from the group of individuals with two consecutive checkups (at the beginning and one year later) A structured questionnaire, physical exam, and standard serum biochemical parameters were obtained in all cases, excluding those with previous cardiovascular disease, hypertension, dislipemia and diabetes. Subjects were distributed in two groups: Group A (n = 3.661), intervention group, in which three telephone surveys were performed (1st, 4th, 8th months), evaluating patient's degree of awareness about cardiovascular risk recomendations and the extent of modifying life style. Group B (n = 1.973) did not have telephone survey. Cardiovascular risk was stratified as low, moderate or high following the cardiovascular SCORE for low-risk European countries. Individuals with a relative risk higher than 4 were also considered as high-risk.
Results Both groups improved their cardiovascular risk profile at the second check-up, being better in Group A that in Group B: ∗SCORE (Group A, 45,4%, Group B 36,29%, P = 0,0001), and ∗gave up smoking (Group A, 26,28%, Group B 20,53%, P = 0,0001). Significative mean value differences between both Groups (differences between 2nd and 1st check-ups) (A/B) stratified by sex, age and professional groups. Men: ∗Systolic blood pressure (SBP) (−10,61/−7,85, P = 0,0002), ∗Diastolic blood pressure (DBP) (−4,86/−3,1, P = 0,0002), ∗LDL-Chol > 125 mg/dl, (−24,92/−22,26, P = 0,03). < 45 years: ∗SBP (−14,55/−11,12, P = 0,01), ∗wheight (−0,15/0,79, P = 0,003). > 45 years: ∗SBP (−9,37/−6,89, P = 0,0037), ∗DBP (−4,58/−2,64, P = 0,0001), ∗Tchol (−21,55/−17,79, P = 0,009). Blue Collar: ∗SBP (−10,66/−7,60, P = 0,0002), ∗DBP (−4,76/−2,86, P = 0,0001).
Conclusions Telephone structured surveys, as a base of cardiovascular primary prevention, is an effective tool to prevent cardiovascular diseases. Changes towards healthful habits of life entail a significant reduction of the cardiovascular risk. Routine medical check-ups carried out in workers affiliated to a Mutua, constitute a privileged and efficient frame in primary cardiovascular prevention at assessing young and “healthy” people with low sanitary service use and low prevention applied programs.
427 Does physical activity prevent pre-eclampsia? The HUNT study and the medical birth registry of Norway
E.V. Tyldum1,2, P.R. Romundstad1, S. Slørdahl1
1Faculty of Medicine, Norwegian University of Science and Technology, Trondheim, Norway
2Central Norway Regional Health Authority, Stjørdal, Norway
Objective The objective of this study was to assess whether women engaged in pre-pregnancy physical exercise have reduced risk of developing pre-eclampsia. The rationale for our study is that important hallmarks of pre-eclampsia, like endothelial dysfunction, disturbances of the lipid profile, and increased risk of cardiovascular disease, are all factors which individually have been shown to be reduced by physical exercise.
Methods A prospective cohort study was designed based on data on physical activity from the HUNT−1 Study performed in the county of Nord-Trøndelag, Norway, from 1984–;1986 with a participation rate of 88% (n = 74,599). The Medical Birth Registry of Norway provided information on the first birth after the time of participation in the health study. Women with singleton live births were included. Pregnancy at the time of participation in the baseline health study was set as exclusion criterion. This rendered a population of 3,656 women for our study, of whom 167 (4.5%) suffered from pre-eclampsia. Logistic regression was used to estimate odds ratios with 95%-confidence intervals. The odds ratios were adjusted for maternal age, parity, smoking, body mass index and the time span from HUNT−1 to childbirth.
Results Relative to women who never exercised, the women who exercised less than once a week had an odds ratio of developing pre-eclampsia of 2.1 (0.9–;4.9), whereas the women who exercised once a week or more had an odds ratio of 1.8 (0.8–;4.2). With regard to intensity, the odds ratio of the women who exercised with low intensity was 1.9 (0.7–;4.9), with moderate intensity 2.4 (0.9–;6.0) and with high intensity 2.0 (0.6–;7.1), all relative to those who never exercise.
Conclusion Women engaged in physical exercise prior to pregnancy did not have reduced risk of developing pre-eclampsia.
431 Improving predictive accuracy of the Framingham coronary risk score by including psychosocial risk factors
V Timmaraju, F Dunstan, J Gallacher
Cardiff University, Cardiff, UK
The Caerphilly Study is a prospective cohort study investigating risk factors for cardiovascular disease and related outcomes. Nearly 3000 men, aged 45 to 59 years, were recruited during 1979–;1983 from the town of Caerphilly and surrounding villages in South Wales. Cardiovascular risk factors, including blood pressure, cholesterol, body mass index, smoking, alcohol consumption and psychological risk factors such as anxiety, depression, anger and attitude towards coronary related behaviours were measured. Outcomes of ischaemic heart disease and stroke have been recorded since recruitment. The outcome variable used in this analysis is Myocardial Infarction (MI).
Initially the Framingham risk equations were used to predict the number of events after 10 years and it was found that they over-predicted the number of events. Similar risk equations were developed from the data in this cohort and compared with the Framingham risk equations. ROC (Receiver Operating Characteristic) curves were derived for both the Framingham and Caerphilly risk equations and it was found that there was no significant difference between the two equations (p = 0.44, Area Under the Curve (AUC) for Caerphilly and Framingham equations were 0.693 and 0.688 respectively); the problem with the Framingham equation is one of calibration in that it overstates the risk.
Several psycho-social factors, recorded in the Caerphilly study, were found to be significantly associated with the risk of an MI, including anger, leisure activity and attitudes towards coronary related behaviours. When these were added to the new Caerphilly model the prediction of MIs improved significantly. Comparing the ROC curves from the Framingham and new Caerphilly risk models showed a significant advantage of the new Caerphilly risk equation over the Framingham risk equation in predicting MI (p = 0.02, AUC for the new Caerphilly equation was 0.723). Testing a risk model on the data from which it was derived introduces bias and the results of cross-validation exercises to reduce this bias will be presented.
433 Hospital variation in use of secondary preventive medicine after discharge for first acute myocardial infarction during 1995–;2004
S. Rasmussen1, J.N. Rasmussen1, S.Z. Abildstrom1,2, G.H. Gislason2, T.K. Schramm3, F. Folke3, L. Køber4, C. Torp-Pedersen2, M. Madsen1
1National Institute of Public Health, Copenhagen, Denmark
2Department of Cardiology, Gentofte University Hospital, Copenhagen, Denmark
3Department of Cardiology, Bispebjerg University Hospital, Copenhagen, Denmark,
4Department of Cardiology, Copenhagen University Hospital, Copenhagen, Denmark
Objectives Several studies have reported substantial hospital variation in use of secondary preventive medicine after discharge for acute myocardial infarction (AMI). We examined nation-wide temporal trends in hospital use of secondary preventive medicine after discharge for first AMI in Denmark over a 10-year period.
Methods Observational study using national administrative databases including 60 339 patients who survived 90 days after discharge for a first AMI at 73 acute-care hospitals during 1995–;2004. Outcome measures were at least one prescription claim for angiotensin-converting enzyme (ACE) inhibitors, beta-blockers or statins within 90 days of discharge. We used random effect logistic regression to examine the hospital variation in use of medicine and the relationship with hospital factors (county, volume and type) adjusted for age, gender, period, income, co-morbidity, prior and concomitant pharmaceutical therapy.
Results In 1995 the odds ratios (OR) between hospitals in the highest and lowest deciles were 8.5 (95% CI: 5.5–;12.2) for beta-blockers, 6.2 (4.1–;8.8) for statins and 3.0 (2.3–;3.7) for ACE inhibitors. By 2004, the hospital variation had decreased for beta-blockers (3.2; 2.3–;4.0) and statins (4.2; 3.0–;5.5) but had increased for ACE inhibitors (3.8; 2.7–;4.9) (See Figure). All the changes over time were statistically significant (p < 0.001). Hospital type was related to use of statins, in that patients admitted to invasive centres had a greater chance of using statins than those admitted to local hospitals (OR, 1.64; 1.13–;2.38). No significant difference was found between regional and local hospitals (OR, 1.19; 0.96–;1.43). Hospital type explained 9% of the variation in use of statins in 1995, but this was reduced to almost 0% by 2004. Hospital volume was not related to use of secondary preventive medicine. Hospital county explained 32% of the variation in use of beta-blockers in 2004 and 27% in 1995, 29% of the variation in use of statins and 19% in 1995, 39% of the variation in use of ACE inhibitors in 2004 and 3% in 1995.
Conclusions Hospital use of secondary preventive medicine after discharge for AMI varied substantially. Hospital variation in use of beta-blockers and statins reduced with time whereas variation in ACE inhibitors increased. This may be attributed to more uniform guidelines for the use of beta-blockers and statins and lesser agreement of use of ACE inhibitors. Geographical characteristics of the hospitals were a more important predictor for use of secondary prevention than hospital volume and type.
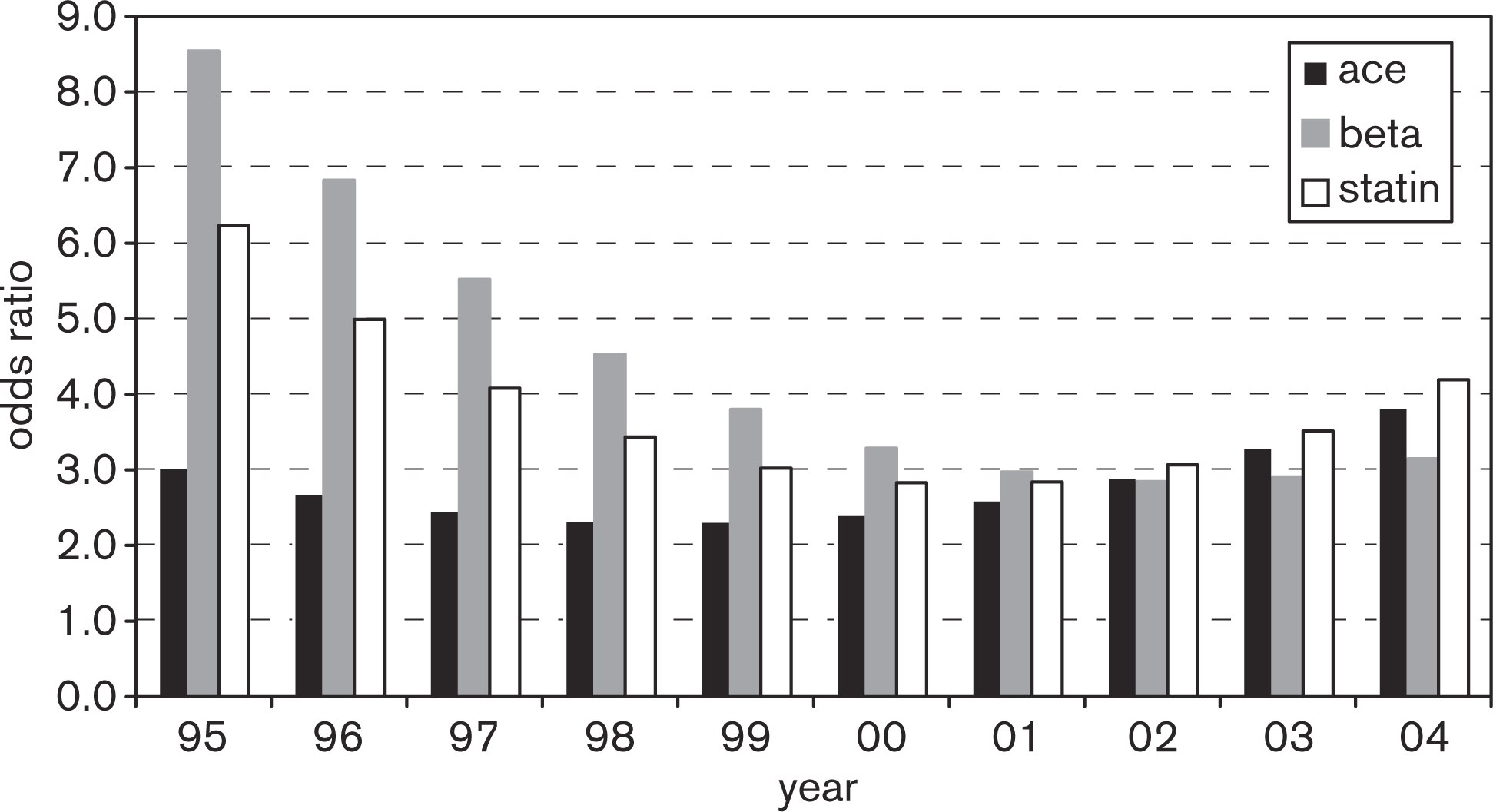
Odds ratios between lowest and highest deciles of 73 hospitals for 60 339 patients, who survived 90 days after discharge following first AMI, in use of beta-blockers (beta), statins and angiotensin-converting enzyme (ACE) inhibitors, during 1995–;2004.
447 Risk factors of cardiovascular diseases in students
S. Boldueva,
St Petersburg State Mechnikov Medical Academy, St Petersburg, Russia
Objectives The question of primary prevention has become relevant in our days when cardiovascular morbidity is very high. The aim of our research was to detect risk factors of Ischemic Heart Disease (IHD) in young people.
Methods 466 students of the Mechnikov Medical Academy (aged 19–;22 years) were asked to fill in a questionnaire. The questionnaire included questions concerning risk factors of cardiovascular diseases (CVD).
Results 382 (81.6%) students had hereditary risk for: arterial hypertension along –; 139 students (29.70%), IHD along−10 (2.14%), arterial hypertension and IHD in combination−38 (8.12%). 95 students (20,29%) were smokers. 122 students experienced episodes of high blood pressure at least once in their life, 75 individuals (61.5%) of them had hereditary risk for arterial hypertension. 191 students (41.0%) are physically active and go in sports. 119 students (25.5%) were found to have 3 risk factors, 93 (78%) of them had hereditary risk for arterial hypertension and IHD. 130 (27.9%) had 2 risk factors and 134 (28.8%) –; one risk factor. Only 85 (17.7%) students didn't have any risk factors.
Conclusions prevention of CVD should be started in younger age, especially in those who have hereditary or more than two any risk factors.
458 Association between self-reported perception of general health and cardiovascular risk, and lifestyle factors in a population of Swedish adults
Pernille Langkilde1, Lauren Lissner2, Georgios Lappas3, Leyla Nunez2, Annika Rosengren1
1Department of Medicine, Sahlgrenska University Hospital/östra, Göteborg, Sweden
2Department of Community Medicine (Primary Health Care) Sahlgrenska Academy at Göteborg University, Sweden
3Cardiovascular Institute, Sahlgrenska Academy at Göteborg University, Sweden
Objective Theory on life-style intervention suggests that patients' awareness and understanding of their own health are predictors for successful outcome of changes in lifestyle. This purpose of this study is to assess the association between self-reported perception of general health and cardiovascular risk, and life style factors in a population of Swedish adults.
Method Data is based on the INTERGENE-study, a population-based research programme assessing the INTERplay between GENEtic susceptibility, environmental factors, lifestyle, gender and psychosocial background for the risk of chronic diseases, as well as trends in cardiovascular disease and risk factors in western Sweden including Gothenburg. The Cohort Study collected data from April 2001 to the end of 2004 from 3610 individuals aged 25–;75 years.
The perception of general health was self-reported using a four-point scale from “Poor” to “Very Good”. For this analysis we reduced the responses to “Poor health” and “Good health”. Cardiovascular risk factors include overweight, high waist-to-hip ratio, hypertension, dyslipidaemia, diabetes, and glycaemia. Lifestyle factors include stress, low physical activity, smoking, and high alcohol consumption. Analyses were stratified by sex, and by age (less than 45, and 45 years, or more).
Results In the four age and gender-specific groups subjects who reported poor health were more likely to be overweight or obese, with high WHR, to report low physical activity, to be smokers, and to have high levels of stress, whereas high alcohol consumption was not related to poor health. In women and older men, self-perceived poor health was associated with hypertension, and with high triglycerides. High LDL was not related to self-perceived poor health.
Conclusion In the study population smoking, low physical activity, stress and obesity, particularly abdominal obesity, were associated with a perception of poor general health.
459 In-Hospital and long-term outcome after carotid artery stenting (CAS) with embolic protection devices in elderly patients
A. Rizza1, G. Trianni1, C. Palmieri1, L. Sulcaj1, A. Al-Jabri1, M. Ravani1, M. Vaghetti1, S. Berti1
1Institute of Clinical Physiology-CNR, “G. Pasquinucci” Hospital, Massa, Italy
Objectives Our objective was to evaluate the outcome of elderly patients during and after treatment with CAS with embolic protection device.
Methods Eligible for inclusion in this study were considered patients older than 75 years with significant carotid stenosis who underwent CAS with embolic protection device in our hospital. A total of 70 patients with a mean age of 79 ± 4 years were included. Of the total study population 24 patients were women, 19 patients had diabetes mellitus, 63 patients had arterial hypertension, 59 patients had hypercholesterolemia. Bilateral carotid-artery disease was present in 43% of the patients; 17% of patients had suffered prior ischemic events. Of the whole population, 53 patients had a history of coronary artery disease (of these 70% of patients had undergone prior coronary revascularization), 18 patients suffered from peripheral artery disease and 1 patient had renal artery stenosis. Study patients underwent implantation of the following types of carotid stents: Acculink (66 patients), Precise (3 patients) and Wallstent (1 patient). The embolic protection devices used were: Accunet (54 patients), Percusurge (5 patients), Mo. Ma (8 patients) and PAES (3 patients). All patients were treated postprocedurally with aspirin and either ticlopidine or clopidogrel for at least one month; afterwards all patients were asked to continue aspirin indefinitely. Patients were followed-up during a mean period 25 ± 13 months by means of office visits.
Results With the exception of 1(1.4%) patient who developed stroke during the stenting procedure, all other patients had an uneventful in-hospital period with a mean hospitalization time 3 ± 1 days. At the end of long-term follow-up 1 (1.4%) patient had a transient ischemic attack and 3 (4.2%) patients developed restenosis. No cases of death of myocardial infarction were observed during this period.
Conclusions CAS with embolic protection devices is associated with favourable in-hospital and long-term outcome in elderly patients with significant stenosis of carotid arteries.
465 EUROACTION: The achievement of blood pressure, lipid and glucose targets in a cardiovascular prevention programme in general practice - one year results
S.B. Connolly1, K. Kotseva1, C. Jennings1, A. Mead1, J. Jones1, A. Holden1, D. De Bacquer2, G. De Backer2, T. Collier3, D. Wood1, on behalf of the EUROACTION Study Group
1Department of Cardiovascular Medicine, Imperial College, London, UK
2Department of Public Health, University of Ghent, Belgium
3Department of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK
4School of Health Sciences and Social Care, Brunel University, London, UK
Objectives EUROACTION is a cluster randomised controlled trial of a preventive cardiology nurse-led programme in general practice. The programme aims to manage high risk patients and their partners to the European lifestyle, risk factor and therapeutic targets.
Methods In six European countries one pair of matched practices was randomised to receive the EuroAction programme or to be monitored for usual care. High risk individuals over the age of 50 were identified in the three following groups: I. HEARTSCORE risk ≥ 5% over 10 years; II. Treated hypertension/dyslipidaemia; III. Diabetes mellitus. Patients and partners in the intervention arm of the study were invited to attend a nurse-led 1-year comprehensive risk factor and lifestyle management programme. All patients and partners were reviewed at 1 year in intervention (INT) and usual care (UC).
Results 67% of all patients identified attended the final assessment (1019/1257 INT, 1005/1752 UC). The majority of eligible partners (225/356 INT, 363/542 UC) also attended. Using random effects meta-analysis (REML estimation) differences in proportions achieving goal were compared.
Proportions of patients and their partners achieving the European blood pressure, cholesterol, glucose and therapeutic targets for cardiovascular disease prevention
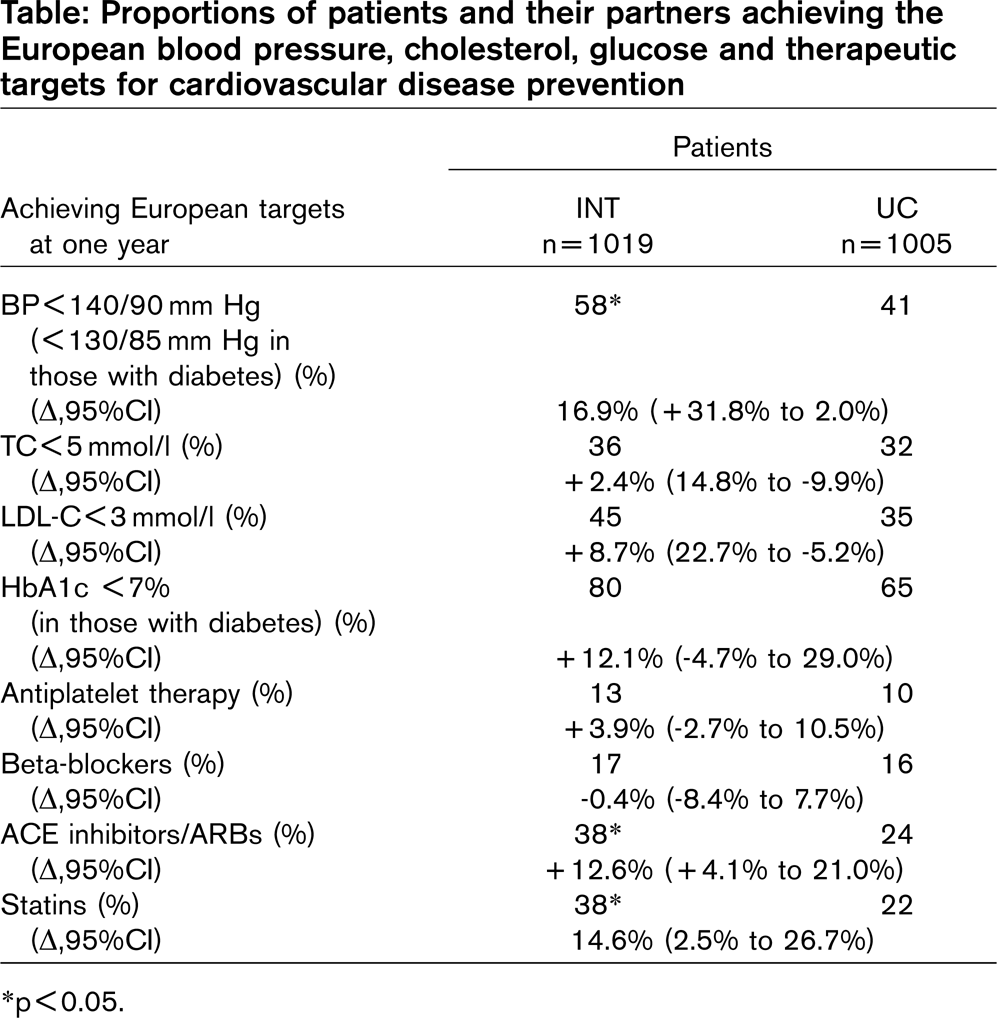
∗p < 0.05.
More partners in INT also achieved these targets although this was significant for blood pressure only. Furthermore, the proportion of partners using cardioprotective medication was much lower than in patients.
Conclusions The EUROACTION programme helped high risk individuals and their families to achieve significantly better blood pressure control. There was also a significant improvement in lipid control in patients and a trend towards improved glucose control. Furthermore, there was a significant increase in the use of statins and ACE inhibitors/ARBs. EUROACTION achieved its overall aim in raising standards of preventive cardiology care for high risk individuals and their partners in everyday clinical practice.
471 Women with high normal blood pressure have a higher incidence of hypertension development than men
G. Pannarale1, R. Licitra1, V. Basso1, D. Mutone1, A. Pergolini1, A. Madeo1, F. Rabbia2, E. Testa2, M.C. Acconcia1.
1Unit of Preventive Cardiology, Sapienza University, Rome, Italy
2Hypertension Center, Division of Internal Medicine, S. Vito Hospital, University of Turin, Turin, Italy
Objectives To evaluate in a prospective study predictors and incidence of established hypertension development in subjects in the age range of 30–;65 years with high normal blood pressure (HNBP).
Methods 90 non-diabetic subjects (47 M, 43 F, age 48 ± 10 years) with HNBP (office BP 133/83 ± 4/5 mmHg) screened for cardiovascular risk factors. All the subjects had a normal ECG and no signs of cardiovascular disease and were followed-up to 84 ± 57 months. Cox proportional hazards stepwise regression analysis was performed in order to evaluate the role of some covariates in hypertension development (age, gender, weight, BMI, total cholesterol, cigarette smoking, office SBP and DBP). The Kaplan-Meier method was used to estimate hypertension free survival and survival differences between genders were analyzed by the Mantel-Cox test.
Results Multivariate analysis showed that only female gender affect hypertension development at follow-up (HR = 1.66, IC95% 0.98–;2.83), while considered cardiovascular risk factors did not influence hypertension-free survival. In comparison with males, female subjects with HNBP were older (51 ± 10 vs. 46 ± 10 years, p = 0.02) and had a lower BMI (25 ± 3 vs. 26 ± 3 kg/m2, p = 0.04). The Kaplan-Meier survival curves showed a higher incidence of hypertension development in women with HNBP (Fig. 1).
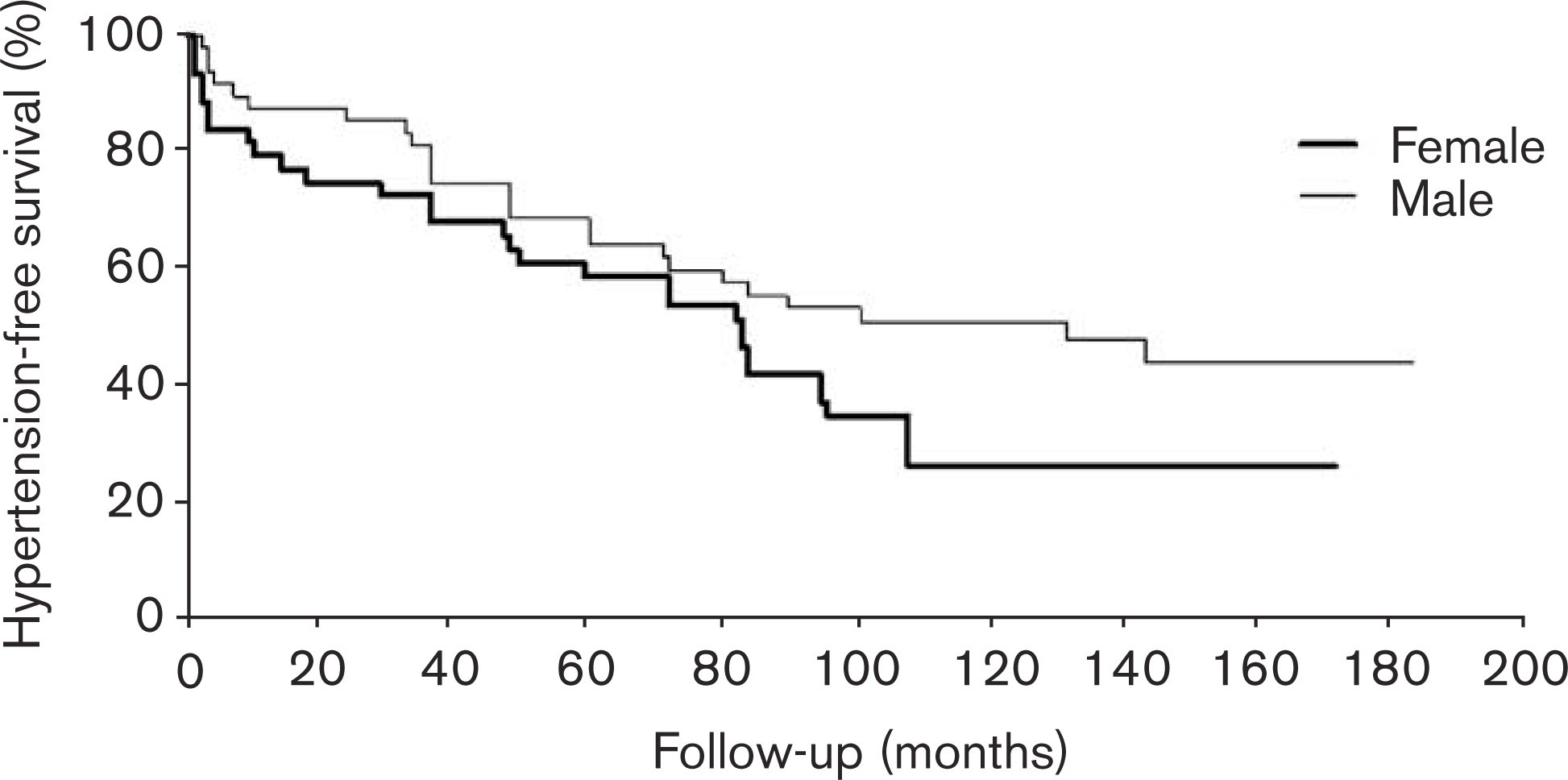
Conclusions Our data, despite of the limited population sample, confirm that subjects with HNBP (or prehypertension) have a high risk of developing established hypertension independently from other cardiovascular risk factors and this risk is about 1.7 fold higher in female gender at a follow-up of 4 years.
479 Ineffective secondary cardiovascular prevention in patients with previous coronary artery disease history presenting with acute myocardial infarction
D. Mytas1, P. Stougiannos1, I. Kyriazis2, E. Zervas2, K. Kontos3, S. Makrygiannis3, M. Zairis3, S. Foussas3, V. Pyrgakis1
1Cardiology Department, General Hospital, Corinthos, Greece
2Internal Medicine Department, General Hospital, Corinthos, Greece
3Cardiology Department, Tzanio General Hospital, Piraeus, Greece
Objectives We aimed to study the metabolic profile and the prevalence of cardiovascular risk factors in patients presenting with an acute myocardial infarction (AMI). Furthermore we evaluated the secondary cardiovascular prevention effectiveness in patients with previous history of coronary artery disease (CAD).
Methods We study 336 consecutive patients, mean age 64 +/−12years, 237 male, who were admitted to our cardiology department due to an AMI. Two hundred twenty seven suffered a ST Elevation MI (STEMI) and 109 a Non ST Elevation MI (NSTEMI). We received a detailed medical history registering baseline characteristics including major cardiovascular risk factors and the presence of metabolic syndrome according to ATP-III criteria. Furthermore, we determined lipid profile in the first 12 h from patient's admission.
Results Two hundred eighteen patients had dyslipidaimia history (64.9%), while diabetes was detected in 84 (25%) and hypertension in 154 (45.8%) of them. Besides, 182 were current smokers (54.2%) and MS was present in 163 of them (48.5%) The admission lipid profile revealed that 272 patients (81%) had uncontrolled dyslipidemia (UD) according to NCEP−2004 criteria. Evaluating the group of 90 patients (26.8%) with previous CAD history we revealed that only 11.1% presented with well controlled lipidemic profile [32 of them (35.5%) were receiving statins but 26 (81.25%) had UD]. Furthermore, only 42% followed psychical activity recommendations, 14 (15.5%) were obese (BMI > 30 Kg/m2BSA) and 54 (60%) overweight (BMI:25–;30 Kg/m2BSA) while MS was present in 54 (60%) of them. Finally, 33 previous CAD patients (36.7%) continuing to be smokers ignoring medical instructions.
Conclusions The prevalence of all major cardiovascular risk factors including metabolic syndrome is substantial among patients presenting with AMI. Furthermore, they reveal a highly distorted metabolic profile. Interestingly, this observation also applies to patients aware of their high-risk condition, such as patients with previous history of CAD.
492 Cardiovascular diseases in turkey: a proposal for re-arrangement of primary health care
M. Turkay∗
∗Akdeniz University Faculty of Medicine, Specialist in Public Health
Cardiovascular Diseases (CVD) are the first among causes of death in Turkey. CVD prevalence is 6.7% among adults over 20 years (7.3% in females, 6.7% in males). The prevalence in coronary heart disease (CHD), hypertension, rheumatic heart disease (RHD), and the others are 3.8, 2.2, 0.5 and 0.3 percent respectively. Number of adults with RHD and CHD is about 150.000 and 1.6 million respectively.
Approximately 130.000 deaths are seen every year. Number of CHD and related deaths increase nearly 5% annually. Although Turkey has a young population, the prevalence of CHD and related deaths are very high compared to other European countries which have older populations.
Problems of healthcare services on CHD in Turkey: The first problem is in the diagnosis. CHD is diagnosed improperly or sometimes delayed, so the cases are faced for the first time in a fatal situation like myocardial infarction. Another problem is insufficient use of primary care for CVD. However, prevention of CHD is impossible with cardiologists working in the secondary care. Under these conditions, Turkey will face serious problems related to CHD and its risk factors in the future. In order to cope with these problems organization of health services should be reorganized gathering local, regional, and national data. The aim of this report is to offer a proposal for re-organization of CHD services in PC. Utilization of the health services is a good opportunity to determine patients with high-risk and to diagnose current CHD.
However, such an approach will not work in large populations. There are some inequalities in utilization, distribution and quality of PC services. It is already known that primary, secondary and primordial prevention should be community based. Furthermore, laborers, students and immigrants should be considered in the re-arrangements of these services. The proposal is placing health units in factories, schools and small sized enterprises and these units should be in connection with PC centers via IT technology. A PC center should be available per every 5,000–;10,000 people. Additionally, health units and health care centers should be equipped with adequate number of health staff, necessary instruments and mobile teams (including physicians and public health nurses) for prevention and follow-up.
Secondary prevention prevents early deaths only in risky individuals. But more cost effective is intervention before risks occur (primordial prevention) since it prevents deaths in overall population. This intervention cannot be achieved unless community based services are provided.
494 Gender differences in the management of risk factors in patients with cardiovascular disease
C. Brotons, N. Soriano, I. Moral, M. Martinez, on behalf of PREseAP investigators
EAP Sardenya. Primary Care Research Unit, Barcelona, Spain
Objectives To assess gender differences in the management and control of risk factors and in the quality of life in patients already diagnosed of cardiovascular disease visited in primary care.
Methods Patients diagnosed of ischemic heart disease (IHD), stroke and peripheral artery disease (PAD) were identified from 42 primary health care centres from all over Spain, from January to May 2005 as part of a ongoing randomised cluster control trial funded by the Spanish Ministry of Health (Fondo de investigación SanitariaI, Instituto de Salud Carlos II), to assess the efficacy of a comprehensive secondary prevention programme in primary care.
Results 1224 patients were identified, 54%, 41% and 5% of women were previosly diagnosed of IHD, stroke and PAD, respectively; while 62%, 31% and 7% of men were previously diagnosed of IHD, stroke and PAD, respectively. 70% were males with a mean age of 65, and 30% were females with a mean age of 69 (p = 0.043). 57,5% and 35% of women were married and widow, compared to 86% and 6% of men (p < 0.001). 89% of women had less than high school education compared to 73% of men. (p < 0.001). 7% of women were smokers compared to 21% of men (p < 0.001). Regarding comorbidity, 4% of women and 9% of men were previously diagnosed of COPD (p = 0.001), and 12% of women and 7% of men were previosuly diagnosed of a psyquiatric disorder (p = 0,003). 50% of women reached target levels on blood pressure (SBP < 140 mmHg and DBP < 90 mmHg) compared to 59% of men (p = 0.002). 25% of women reached target levels on lipids (total cholesterol < 175 mg/dl and LDL cholesterol < 100 mg/dl) compared to 36% of men (p < 0.001). All dimensions of the SF−36 quality of life questionnaire showed worse values for women than for men. Anti-platelet drugs were prescribed in 88% of men and in 83% of women (p = 0.016). No differences were found in antihypertensive or lipid lowering medication.
Conclusions Cardiovascuilar risk factors are poorly controlled in women than in men despite the fact that both groups were equally treated with antihypertensive or lipid lowering drugs. Potential reasons for these findings are that women are treated less agressive than men in order to achieve target levels recommended by European Guidelines. Socioeconomic status and education level might also explained those differences.
501 Long term quality of life follow-up on heart failure patients after therapeutic education
D Curnier1, S Mazon2, L Perez1,2, A Pathak1,2, JM Fauvel2, M Galinier1,2, J Roncalli1,2
1INSERM U858, Toulouse, France.
2Fédération des Services de Cardiologie, Centre Hospitalier Universitaire de Rangueil, Toulouse, France.
Objectives Therapeutic education is an important part in the management of heart failure. Primary health parameters like mortality and morbidity are the most pertinent measure to evaluate intervention but Quality of Life (QoL) was also study after short term therapeutic education. The aim of this study was to evaluate long term benefits of therapeutic education on QoL.
Methods Fifty three heart failure patients underwent 2 therapeutic education sessions at the entry and at 1 month. They were prospectively follow at 1, 3, 6 and 12 months with Minnesota living with heart failure QoL questionnaire (MLWHF), NYHA stage and left ventricular ejection fraction (LVEF). Population was 70% men with a mean age of 60.8 ± 14.6 years old, sex ratio: 16 women vs. 37 men, mean LVEF = 29.6 ± 9.4%; 53% were ischemic. All the patients were on optimal treatment and ACE inhibitor (100%) at the entry on the study. Statistical analysis was made with a 2 ways analysis of variance on repeated measures or on ranks if data distribution did not follow normal law.
Results At one year, MLWHF global score (30.5 ± 21.5 vs. 37.5 ± 24.1; p = 0.045), MLWHF physical component score (12.5 ± 10.0 vs. 16.3 ± 12.0; p = 0.029), NYHA stage (2.0 [1.5–;2.5] vs. 2.25 [2.0–;3.0]; p = 0.027) and LVEF (35% [27.0–;39.0] vs. 30% [22.5–;36.5]; p ≥ 0.001) improved. MLWHF emotional component improved but not significantly (6.8 ± 5.5 vs. 7.3 ± 6.0; p = 0.375). A group effect was present depending on age: MLWHF global (p = 0.0062), physical score (p = 0.0181) and NYHA stage (p = 0.0003). Levels of QoL were higher in women but with the same improvement during the follow-up.
Conclusion Short term therapeutic education improved long term QoL, NYHA stages and LVEF. QoL improvements were less important on older patients and women.
508 Working together for smoking prevention among Romanian teenagers
L. M. Lotrean1, C. Radu-Loghin2, D. Georgescu3
1Iuliu Hatieganu University of Medicine and Pharmay, Cluj Napoca, Romania
2Organization AER PUR, Romania
3National Agency against Drugs, Bucharest, Romania
In Romania the prevalence of smoking among young people is increasing, while the age of smoking upset is decreasing. This indicates the necessity of implementing innovative smoking prevention programs among Romanian adolescents.
The objective of this paper is to present the implementation, content, structure and process evaluation of two smoking prevention programs implemented among Romanian teenagers in the years 2005 and 2006: Smoke Free Class Competition and I do not smoke. Both programs were the result of a partnership between several national and international organizations coming from non governmental sector, as well as from governmental and academic environment.
The goal of Smoke Free Class Competition was smoking prevention among 11–;15 years old school students by involving them in a 4-month competition; at the end of the competition the classes who remain smoke free during this period and performed several antismoking activities could win by draw different attractive prizes. Smoke Free Class Competition was implemented in different European countries since 1997; in Romania it was implemented in the year 2005 among 355 secondary school classes and in the year 2006 among 999 classes from several towns of Romania.
I do not smoke is a smoking prevention program for 13–;15 years old teenagers which consists of five weekly sessions of forty–;five minute each where are discussed several issues regarding smoking: health consequences of active and passive smoking, social influence/pressure, the power of tobacco advertisement, tobacco refusal skills. Structure and content of each lesson can be summarized as follows: (a.) introduction of the theme in a class on video (b.) activities in small groups, peer-led (c.) return to one group and continuation of the lesson on video (d.) activities in small groups, peer-led (e.)(sometimes) home activities. The video is containing interviews with teenagers and real life scenes in order to help young people to identify bad influences, which could appear and to get cigarette refusal skills. The program was developed in 2006 in one big town of Romania and involved 30 secondary school classes.
This paper presents the strengths and weaknesses of the programs and makes recomandations for future smoking prevention activities in order to develop a national strategy regarding smoking prevention among Romanian young people.
529 Prediction of cardiovascular mortality with SCORE-Germany –; A comparison of two German study populations
HW Hense1, E Koesters1, J Wellmann1, H Voelzke2, H Loewel3, U Keil1
1Institute of Epidemiology and Social Medicine, University Muenster, 2Institute of Epidemiology and Social Medicine, University Greifswald, 3Institute of Epidemiology, GSF Research Center Neuherberg, Germany
Objectives SCORE was developed by the ESC to predict 10-year cardiovascular (CVD) mortality in the primary prevention setting. We adapted it to the current risk factor and mortality situation in Germany, creating SCORE-Germany. We investigated the prevalence of risk levels in two concurrent population-based studies in Germany and compared it with expected death rates derived from official mortality statistics.
Methods Participants from cross-section study of representative samples from the regions of Pomerania (SHIP 1997–;2001; net participation 68.8%) and Augsburg/Bavaria region (KORA 1999–;2001; 66.8%). We included men and women, aged 40 –; 64 years of age and free of any signs of cardiovascular disease. Examinations in both studies were highly standardized. We measured blood pressure (oscillometric, mean of 2 recordings), total and HDL cholesterol, and current smoking status. SCORE-Germany risk was calculated for each individual and averaged within 5-year age groups. Official cardiovascular mortality figures for the same age groups were obtained from state vital statistic records.
Results In more than 80% of women in KORA and SHIP, the SCORE-Germany risk of CVD death was below 2% per 10 years. In men, there were over 25% with a SCORE-Germany risk of > 5% per 10 years. In each age-sex group, the SCORE-Germany risk was higher in SHIP than in KORA. This is in agreement with substantially higher official CVD death rates in men and women from the Pomerania region. In most age groups, the prediction by SCORE-Germany was lower than the expected cumulative 10-year CVD death rate derived from the official mortality statistics.
Conclusion In summary, SCORE-Germany reflects well the CVD risk differences between men and women and different age groups within as well as between the two study populations. Higher expected mortality rates based on official statistic data are plausible as these include also cases with prevalent CVD. In general, risk levels are low in both study populations in women and clearly more prevalent in men. We conclude that SCORE-Germany produced consistent and plausible results in two independently sampled study groups from different parts of Germany.
534 Glycosylated hemoglobin levels in type 2 diabetics: relation with early-stage atherosclerosis
J. Silva1, M. Costa1, A. Antunes1, A. Coelho2, P. Mota1, A. Leitão-Marques1
1Department of Cardiology, Centro Hospitalar de Coimbra, Portugal
2Department of Internal Medicie, Centro Hospitalar de Coimbra, Portugal
Introduction and objectives Cardiovascular disease and the development of coronary artery atherosclerosis play a central role in increasing mortality in diabetic patients. The aim of this prospective study was the evaluation of the presence of subclinical atherosclerosis (measured as carotid stenosis and intima-media thickness) and its relationship with glycosylated hemoglobin (HBA1c), in an asymptomatic diabetic population.
Material and methods A prospective study was attained in a group of type−2 diabetic patients, excluding those with diagnosed coronary artery disease, recent cerebrovascular event or previous surgery of the carotid arteries. Blood pressure measurement, body mass index, lipid profile and serum HBA1c levels were assessed. Carotid intima-media thickness (IMT) was measured using doppler ultrasound of the carotid arteries.
Results Thirty-eight stable, non-symptomatic diabetic patients (17 male and 21 female, mean age 59,13 ± 9,94 years) were included and divided in two groups: group A comprehended those who had abnormal findings in carotid doppler (augmented IMT or presence of stenosis) and group B contained diabetics without any alterations. Fourty-five per cent of the patients had augmented IMT (> 1 mm) or stenosis of the carotid arteries, none of them with hemodynamic significance (< 50%); IMT was more pronounced on the left carotid bulb (0,93 ± 0,2 mm, p < 0,002), with carotid plaques also more prevalent in this area. No statistically significant differences were found between the two groups regarding sex (53% vs 57% females, p = 0,18), age (61 ± 9,9 vs 57,6 ± 10 years, p = 0,3), duration of the disease (13,3 ± 8,3 vs 16,2 ± 9,1 years, p = 0,3), body mass index (30,3 ± 3,3 vs 29,5 ± 3,2, p = 0,5) or presence of other cardiovascular risk factors. However, there was a statistically significant correlation between atherosclerosis, HBA1c values (8,65% vs 7,45%, p < 0,05) and previous medication with a statin (41,2% vs 57%, p < 0,05).
Conclusion A poorly controlled diabetes, assessed by HBA1c levels, is associated with a higher risk of atherosclerosis in these patients. Carotid doppler, as a non-invasive tool for monitoring the development of early-stage vascular changes, can be useful in these high risk population, and assist on planning the best therapeutic approach.
535 Daily energy consumption and parameters of the metabolic syndrome in middle-aged women. Does intensity matter?
Schmidt-Trucksäss A1, M. Sandrock2, K. Winkler3, L. Klatt5, E. Bitzer4, H.-H. Dickhuth2, M. Halle1, K. Böttcher5
1Preventative and Rehabilitative Sports Medicine, Technical University Munich, Germany
2Preventative and Rehabilitative Sports Medicine, Freiburg University Hospital, Germany
3Clinical Chemistry, Freiburg University Hospital, Germany
4ISEG, Hannover, Germany
5Kaufmännische Krankenkasse, Hannover, Germany
Objectives The parameters of the Metabolic Syndrome (MTS) are widespread and still increasing worldwide. Physical inactivity is thought to be the common soil for the parameters of the MTS. However, it is not clear, whether energy consumption by physical activity should have a certain intensity in order to obtain a significant effect on the parameters of the MTS.
Methods Assessment of waist circumference, blood pressure, triglycerides, high density cholesterol (HDL-C), HBA1c by standard methods and physical activity by the Freiburg physical activity questionnaire in 2704 women at the age between 40 and 55 years. Sports activity was defined as all activities in different sport disciplines with higher intensity, all other activities were categorized as non-sports activity with lower intensity. Both were calculated in kcal per day according to the Compendium of Physical Activities of Ainsworth. Women participating in sports and non-sports activities were subdivided into high (> 300 kcal per day) and low amount (< 300 kcal per day) activity group, respectively. Differences between groups were tested by ANOVA, independence of effect on parameters by linear regression analysis.
Results 2570 out of 2704 completed the questionnaire and the assessment of all other parameters. 24.1% consumed > 300 kcal per day by sports activities and 46.3% by non-sports activities, respectively. Sports and non-sports activities contributed independently to systolic and diastolic blood pressure, HDL-C and waist circumference as dependent variables (p < 0.05 - p < 0.01) but not to HBA1c and triglycerides. The differences between low and high amount consumers of daily energy in sports and non-sports activities were similar in systolic and diastolic blood pressure, HDL-C and waist circumference, respectively. Women with a high amount of both, sports and non-sports activities, nearly doubled the effect compared to high amount of either sports or non-sports activities.
Conclusions In a clientele of middle-aged women a high amount of either higher or lower intensity physical activity seems to have a comparable absolute effect on systolic and diastolic blood pressure, HDL-C and waist circumference, respectively. For the control of these parameters of the MTS not intensity but the amount of calorie consumption may be more important. These results may have an impact on the prescription of daily physical activity in primary prevention of the MTS and associated diseases.
537 Indo Asians exhibit a more pronounced white cell response following percutaneous coronary intervention
Iqbal Toor1, Rumi Jaumdally2
1The Heart Hospital
2University Hospital Coventry and Warwickshire
Background Percutaneous coronary intervention (PCI) seem to be linked with higher restenosis rates in Indo-Asians (IA) than their White European (WE) counterparts. White cell response (WCC) forms an integral part of the vascular reaction to injury and subsequent smooth muscle proliferation. We hypothesized that IA would exhibit a higher WCC response than WE following PCI.
Methods Retrospective registry analysis of all patients undergoing consecutive PCI during a period of 2 years was undertaken. Pre- and post-procedural white cell count were analysed in 564 White European and 210 Indo-Asian patients undergoing elective or urgent PCI. The two ethnic groups were compared with respect to the change in total white cell and differential white cell count following PCI.
Results Indo-Asians had a higher prevalence of diabetes (40% vs. 17%; p < 0.0001) and were more likely to require an urgent procedure (74% vs. 58%; p < 0.0001). The proportion of patients with single vessel disease was similar between the two groups (Indo-Asian: 79% vs. White European 78%; p = 0.92). There was no significant ethnic difference in baseline total white cell (Indo-Asian: 8.1 IQR [6.7 –; 9.4] vs. White European: 7.9 IQR [6.5 –; 9.4]; p = 0.24) or neutrophil count (Indo-Asian: 4.78 IQR [3.87 –; 5.90] vs. White European: 4.95 IQR [3.96 –; 6.13]; p = 0.39). Following PCI the increase in total white cell (0.6 IQR [−0.5 –; 1.8] vs. 0.8 IQR [−0.13 –; 2.0]; p = 0.01) and neutrophil (0.8 IQR [−0.19 –; 1.65] vs. 1.09 IQR [0.19 –; 2.01]; p = 0.006) count was significantly greater within Indo-Asian patients. In subgroup analysis of patients undergoing an elective procedure the increase in neutrophil count was greater in the Indo-Asian group (1.38 ± 0.24 vs. 0.78 ± 0.10; p = 0.012).
Conclusion Following PCI, an increase in total white cell and neutrophil count was observed in both ethnic groups. These were significantly more pronounced in IA including the elective cases undergoing PCI. Our study suggested that Indo-Asian ethnicity might be associated with a pro-inflammatory phenotype in response to angioplasty.
550 Building a knowledge network for rheumatic fever in Brazil - the methodological proposal of the PREFERE program
R.E. Müller1,2, A.L. Schilke1,2,3, A.E.A. Silva4,5, M.C.C. Kuschnir1,6, M.S. Santos1, M.J. Lucas1,2, R.M.A. Xavier1,2.
1National Institute of Cardiology, Rio de Janeiro, Brazil
2PREFERE Program, Rio de Janeiro, Brazil
3Municipal Foundation of Education, Niterói, Brazil
4Getúlio Vargas Filho Municipal Hospital, Niterói, Brazil
5State Cardiology Institute Aloísio de Castro, Rio de Janeiro, Brazil
6State University of Rio de Janeiro, Rio de Janeiro, Brazil
Introduction Rheumatic fever (RF) is a serious disease and the most common cause of acquired heart disease among children and young adults worldwide. In Brazil RF remains a major problem. Nevertheless, RF is caused by a simple sore throat and the prevention of this illness is based on the correct treatment of streptococcal tonsillitis (ST). The early recognition and adequate treatment of streptococcus tonsillitis increases the possibility of preventing RF. The school, seen as a daily reference to the child, is the right place to disseminate information about this disease and its prevention. It is also a special place to discuss about the great difficulties that this illness imposes.
Objectives The main objective of the PREFERE Program (Rheumatic Fever Prevention Program) is to build an information/formation/action network about tonsillitis and RF from school in order to disseminate and socialize knowledge about this illness and its prevention.
Methods The strategy is based on training key teachers who become responsible for spreading information about RF and its prevention within the schools. These teachers elaborate and perform also pedagogic projects regarding ST and RF and act as interlocutors between the school and the community and between the school and the regional primary health care team. These professionals also refer suspected cases of RF and tonsillitis for diagnosis.
Results In a Pilot Study in 6 month period in Niterói, Rio de Janeiro, 33 key teachers were trained and started working in 30 primary schools, conveying information about tonsillitis and RF to 850 schoolteachers and to 16.600 pupils. The pupils designed various materials as the result of pedagogic projects among the schools. This allowed the school community to comprehend the problems of RF patients and enabled them also to disseminate information about the disease.
Conclusions Health education currently should not be based only upon giving information about the diseases and its consequences, as it is not sufficient to promote behavior changes leading to a healthier life-style. The pedagogic approach proposed by PREFERE enables the school community (children, teachers, and others professionals) to form concepts, to elaborate strategies, to consider situations and to make decisions that potentially produce changes in attitude of children and their relatives regarding prevention of Rheumatic Fever.
552 Pre-procedural Neutrophil to lymphocyte ratio predicts long-term adverse events following percutaneous coronary intervention
Iqbal Toor1, Rumi Jaumdally2
1The Heart Hospital
2University Hospital Coventry and Warwickshire
Background Neutrophil to lymphocyte ratio (N/L) ratio represents white cell response and has been linked with an exaggerated inflammatory response. We sought to examine preprocedural N/L ratio and adverse outcome in patients undergoing percutaneous coronary intervention (PCI).
Methods A total of 908 patients undergoing elective or urgent PCI with preprocedural white cell count were divided into quartiles using their N/L ratio (1st quartile 1.47 ± 0.28; 2nd quartile 2.14 ± 0.19; 3rd quartile: 2.95 ± 0.29; 4th quartile 5.14 ± 1.74). Patients were followed up for the occurrence of death (including fatal stroke and myocardial infarction (MI) and/or non-fatal MI.
Results Demographic and procedural data are summarized in Table 1. Over the follow-up period of a median of 25.6 months, 61 deaths and 25 non-fatal MI occurred. Patients in the 4th quartile (odds ratio [OR] = 3.3, 95% confidence interval [CI] 1.63 –; 6.73; p = 0.001) had an increased long-term risk of adverse events compared to the 1st quartile. Multivariate analysis found N/L ratio in the 4th quartile to be an independent predictor of long-term mortality or non-fatal MI (OR = 3.24, 95% CI 1.47 −7.12; p = 0.004). In multivariate analysis, N/L ratio in the 4th quartile remained significant only in urgent cases.
Conclusion N/L ratio in the fourth quartile was an independent predictor of long-term adverse outcome following PCI. This association was also confirmed within the subgroup presenting for PCI acutely, which suggests it is a widely useful inexpensive marker of long-term risk stratification.
Clinical and procedural baseline characteristic by quartiles of N/L ratio
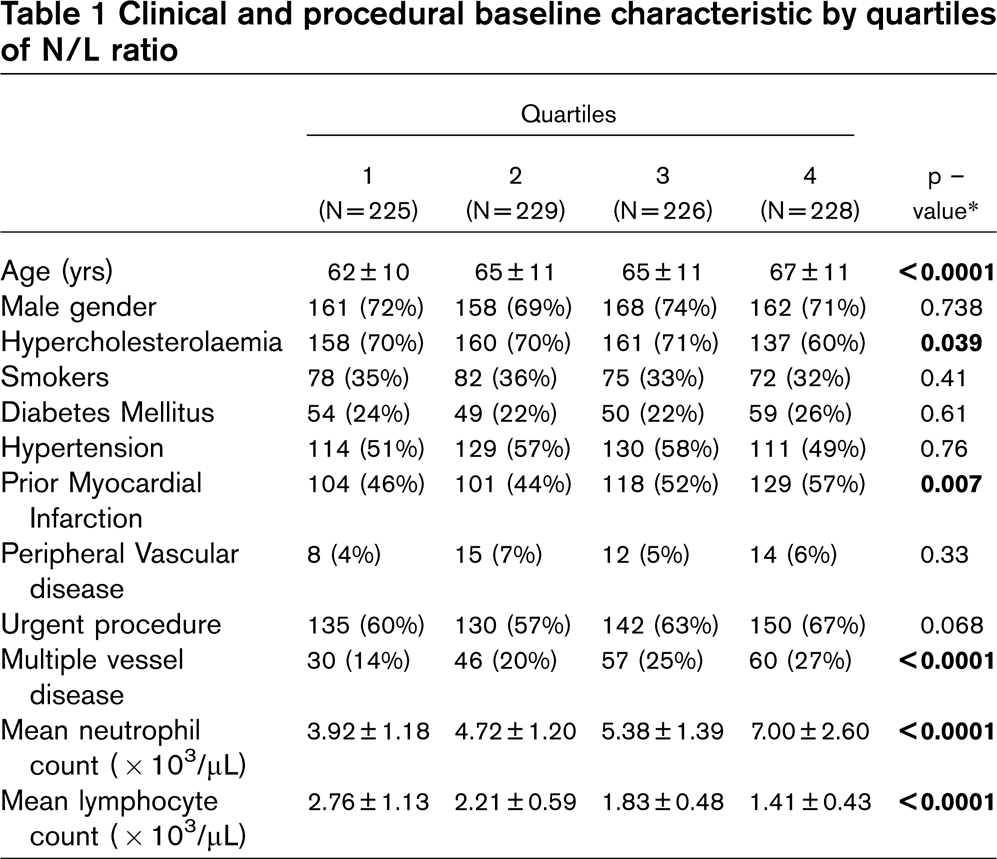
577 Exercise stress testing in asymptomatic diabetics to assess and prevent risk of coronary artery disease-CARE experience
Dr. Nitin A. Yadav, Neelam N. Yadav, G. Ravindra, Prasad Rao
Department of Cardiology, CARE Hospitals, Anantapur, India.
The risk of coronary atherosclerosis is significantly increased in diabetic patients as compared to non-diabetics. The purpose of this study was to evaluate asymptomatic diabetics with a normal electrocardiogram, for inducible ischemia and silent coronary artery disease, with exercise stress testing.
Hundred patients of diabetes mellitus, who had no cardiac symptoms and a normal electrocardiogram, were studied at our hospital over a 1-year period. Treadmill Test was done on Standard Exercise Testing System(Nasan Medicals);using Bruce protocol. Duration of diabetes mellitus ranged from 2 months to 30 years. Age range was from 25 to 60 years. 20 age-matched controls were also studied. Patients with coexisting hypertension and anemia were excluded.
28% of patients had a positive test for inducible ischemia. 3% patients had chronotropic incompetence., i.e. they failed to achieve 85% of age-predicted maximal heart rate. A positive test was more commonly noted in poorly controlled diabetics (75%) than in those with strict control. Exercise tolerance was less in diabetics than control subjects. In patients with autonomic dysfunction and sensory neuropathy(7%), abnormal exercise-induced heart rate and blood pressure responses were commonly noted, possibly due to increased anginal threshold.
In conclusion, exercise stress testing is a dependable screening test for early detection of clinically silent coronary artery disease in asymptomatic diabetics.
578 Risk factors associated to primary hypertension in Brazilian adolescents
M.C.C. Kuschnir1,2, G.A. Silva2, R.E. Müller1, R.M.A. Xavier1.
1National Institute of Cardiology, Rio de Janeiro, Brazil
2State University of Rio de Janeiro, Rio de Janeiro, Brazil
Background Primary hypertension is a prevalent chronic condition in adolescence. Berenson et al brought up the association between risk factors and early atherosclerotic illness in the Bogalusa Study. Recently, obesity in children has increased significantly in Brazil, and it can cause/worsen: hypertension, dyslipidemia, type 2 diabetes, metabolic syndrome and obstructive sleep apnea.
Objectives this study sought to investigate the risk factors associated with primary hypertension in adolescents in Rio de Janeiro, Brazil.
Methods an outpatient based case-control study was conducted with adolescents between 12 and 20 years, who were followed in Núcleo de Estudos da Saúde do Adolescente da Universidade Estadual do Rio de Janeiro, a specialized university service for adolescents in Rio de Janeiro. The nutritional status was evaluated by body mass index (BMI). Moreover the weight, height and abdominal circumference, birth weight, history of familiar hypertension and sexual maturity rating were obtained. The analysis was elaborated through unconditional logistic regression.
Results 91 cases and 182 controls participated in the study. Statistical analysis demonstrated a strong association between total adiposity and regional fat distribution and hypertension. However, after adjustmet, only total adiposity –; measured though BMI –; was shown to be associated with hypertension. Stature has shown to be associated in a positive way with hypertension in girls. Our study did not show an association between puberal development and weight at birth and hypertension in adolescence. Family history –; especially when both parents presented hypertension-was found to have a strong association with hypertension, both to boys (OR = 13,32; 95% CI: 2,25 –; 78,94), and girls (OR = 11,35; 95% CI: 1,42 –; 90,21).
Conclusion The results of our study reinforce the need for public policies directed to the prevention of overweight and obesity in adolescents and for a special monitoring of children of parents with hypertension.
585 Blood pressure control in hypertensive patients
J. Bellwon1, E. Siewaszewicz2, K. Chlebus1, A. Rynkiewicz1
1Medical University of Gdansk, Gdansk, Poland
2Pfizer Polska, Warszawa, Poland
Objective To reduce the burden of cardiovascular diseases we need quantitative information on the burden of cardiovascular diseases and the control of modifiable risk factors. The aim of the study was to evaluate control of blood pressure in hypertensiv patients.
Methods A clinic-based survey of 16684 hypertensiv patients who visited 1232 primary care physicians (GP) and 528 cardiologists. They were patients diagnosed and treated for hypertension but without other CVD events. Serum cholesterol and blood pressure were measured. Data on smoking habits were obtained. The total fatal cardiovascular risk was calculated according to ESC SCORE equations for high risk regions of Europe.
Results Mean age was 58 ± 10 years (8014 women aged 59 ± 10 years and 8670 men aged 58 ± 10 years). We divided patients into three age groups: group A- < 45 years (n = 1618), group B 45–;65 years (n = 11262) and group C ≥ 65 years (n = 3804). There were more men in group A (p < 0,01) and women in group C (p < 0,01).
Adequate blood pressure control (< 140/90 mmHg) was achieved in 9,1% subjects, significantly more in youngest group, respectively in groups A, B and C 18,2%, 8,0% and 8,6%, p < 0,001. In men adequate blood pressure control was achieved in 8,5% subjects, significantly more in youngest group, respectively in groups A, B and C 15,1%, 7,9% and 7,1%, p < 0,001. In women adequate blood pressure control was achieved in 9,7% subjects, significantly more in youngest group, respectively in groups A, B and C 22,4%, 8,0% and 10,0%, p < 0,001. Adequate blood pressure control was achieved significantly more often in women than men (p < 0,01) in groups A (p < 0,0005) and C (p < 0,002).
GP achieved adequate blood pressure control in 8,9% subjects, significantly more in youngest group, respectively in groups A, B and C 18,1%, 7,8% and 8,3%, p < 0,001. Cardiologists achieved adequate blood pressure control in 10,8% subjects, significantly more in youngest group, respectively in groups A, B and C 19,6%, 9,7% and 11,0%, p < 0,001. Adequate blood pressure control was achieved borderline significantly more often by cardiologists than GP (p < 0,05), only in group B (p < 0,05).
Mean risk SCORE was 8 ± 7%; 11 ± 8% in men and 5 ± 4% in women-p < 0,001; in group A 2,7 ± 4,1%; in B 7,2 ± 6,4% and in C 12,3 ± 8,5%-p < 0,001. The prevalence of high risk (≥ 5%) was 59%; 74% in men and 44% in women-p < 0,001; in group A 15,2%; in B 36,6% and in C 86, 8%-p < 0,001.
Conclusion There is a very unsatisfactory blood pressure control among hypertensive patients in our country. Better blood pressure control is achieved in patients < 45 years and women. Cardiologists achieve only slightly better control of blood pressure than GP in hypertensive patients. The CV mortality risk is very high in hypertensive patients.
592 IHD risk factor intervention project addressing the inequalities in cardiac health care
Bolderson L, Griffiths J, McNamara A, Durston N
Merthyr Tydfil Local Health Board/National Public Health Service
Commenced January 2002 –; first phase findings.
Aims The IHD Project focuses on Standard Two, Key Action 6,8 and 9 of the CHD NSF.
To develop regular screening services within GP practices for those patients with Coronary Heart Disease (CHD) and those at high risk of developing CHD
To reduce and modify lifestyle factors that predispose to CHD.
Methods An initial baseline assessment provided the guidance required to develop this service. Audit tools were developed to monitor patient risk factors and the documentation of data within the GP practice, as most GP practices were not fully computerised at this time. Assessment of practice nurse educational needs was also carried out.
Results The project period was from January 2002 until December 2004, the objectives achieved during that period are:
CHD registers are developed in all 13 GP practices.
All patients identified on the registers were provided with a comprehensive review of their condition, including risk factors and medication.
Developed guidelines and protocols for use by all practice staff.
Educational sessions developed for practice nurses.
The publication of a practice CHD ‘toolkit’, which all thirteen practices received.
Conclusion Evaluation has highlighted the association between reduction of risk factors and regular screening. Patient and clinicians knowledge has improved regarding management and treatment of Coronary Heart Disease. The overall aims and objectives were achieved above the expectations of the Nurse Team.
593 IHD risk factor intervention project Preventing Cardiovascular Disease in Small workplaces
Bolderson L, Griffiths J, McNamara A, Durston N
Merthyr Tydfil Local Health Board/National Public Health Service
Pilot December 2004. Main Project March 2005.
Aim To provide a designated screening service for those of the population who are at risk of developing Coronary Heart Disease but at present have no history of chronic disease such as diabetes or hypertension.
Methods
The Ischaemic Heart Disease (IHD) Nurse Team provided a comprehensive screening programme which evaluated the individual's risk of developing Cardiovascular Disease over a ten year period. The IHD Nurse Team would work in collaboration with the National Public Health Service (NPHS) Project to deliver screening and healthy lifestyle days to Small Workplaces across the Borough.
Results
The data evaluation proved by implementing ‘opportunistic’ screening you can detect very serious and adverse lifestyle factors.
The screening project has been delivered in 14 of the workplaces, and piloted in the Local Health Board.
198 clients accessed the service over a 12 month period.
Out of the 14 workplaces initiated within the second phase 38 people were referred for further medical advice or intervention.
Conclusion Evaluation has highlighted the association between reduction of risk factors and regular screening. Patient and clinicians knowledge has improved regarding management and treatment of Coronary Heart Disease. The overall aims and objectives were achieved above the expectations of the Nurse Team. The evidence from client evaluation has proved there is a need for a designated occupational health service for this client group, as various other conditions were addressed during the screening sessions.