
Abstract

110 Impact of sport activity on myocardial function evaluated by Doppler tissue velocity sampling
M. Deljanin Ilic1, S. Ilic1, M. Zdravkovic2, V. Ilic1
1Institute of Cardiology, Niska Banja, University of Nis, Serbia
2Clinical Center, Bezanijska Kosa, Belgrade, Serbia
The aim of the study was a quantitative assessment of the impact of sport activity on overall diastolic and regional systolic and diastolic myocardial function using pulsed wave Doppler tissue imaging (PW DTI).
Methods Forty-three male subjects were studied: 23 endurance athletes (ATE group; swimmers, runners) and 20 subjects without sport activities (C group). Overall left ventricular (LV) diastolic function was assessed by DTI velocity sampling of the mitral annulus. We measured peak annular velocity during early (VE) and late (VA) diastole and calculated their ratio VE/VA. Regional myocardial function of basal LV segments was obtained by PW DTI, and in each adequately visualized segment we calculated peak velocity of systolic (Vs), early (Ve) and late (Va) diastolic waves and their ratio Ve/Va.
Results Overall LV diastolic function was significantly higher in ATE than in C group (P < 0.0001). Regional systolic and diastolic myocardial velocities were measured in 95 basal LV segments in ATE and in 85 basal LV segments in C group. Ratio Ve/Va of basal LV segments was significantly lower in C than in ATE group (1.52 ± 0.33 vs 2.01 ± 0.37, P < 0.0001; difference 24.3%). Systolic function of basal LV segments was significantly higher in ATE than in C group (13.7 ± 2.1 vs 12.6 ± 2.2 cm/s, P < 0.005; difference 8.0%).
Conclusion Quantification of myocardial velocities by PW DTI demonstrated positive influence of sport activity on overall diastolic and regional myocardial function. This is expressed through significantly higher overall diastolic and regional systolic and diastolic myocardial function of basal LV segments in endurance-trained athletes than in subjects without sport activity.
128 Assessment of global longitudinal and peak systolic strain by echocardiographic two-dimensional strain (2D-Strain) in top level athletes and in patients with hypertrophic cardiomyopathy
T. Butz, L. Faber, F. van Buuren, C. Langer, O. Oldenburg, K.A. Treusch, D. Horstkotte, K.P. Mellwig
Department of Cardiology, Heart and Diabetes Center North Rhine-Westphalia, Ruhr University Bochum, Bad Oeynhausen, Germany
Objectives Two-dimensional strain (2D-Strain) is a novel method to assess strain from standard two-dimensional echocardiographic images. Strain imaging has been proposed as a sensitive tool to detect early systolic dysfunction in hypertrophic cardiomyopathy (HCM). Aim of our study was to characterize global and regional function abnormalities using this technique in top level athletes (German national handball league) and in patients (pts.) with pathological left ventricular hypertrophy (LVH) caused by nonobstructive HCM.
Methods We studied 20 consecutive athletes and 18 HCM-pts. by echocardiography according to ASE guidelines. Global longitudinal strain (GLS) and regional peak systolic strain (PSS) was assessed by 2D-Strain in the apical four-chamber-view using a dedicated software package (Vivid 7, GE Healthcare).
Results Mean enddiastolic thickness of septum was significantly increased in the HCM-group (20 ± 7 mm vs. 12 ± 1 mm; p < 0.01). Mean LV enddiastolic index was 26 ± 5 and 25 ± 4 cm/m2 (n.s.).
Mean GLS was −11.2 ± 5.2% in the HCM-group and −15.2 ± 3.7% in athletes (p < 0.01). Pts. with HCM demonstrated lower longitudinal PSS in the septal segments (basal: −9.9 ± 4.0% vs. −16.4 ± 4.0%, p < 0.01, mid: −11.53 ± 5.9% vs. −17.8 ± 3.8%, p < 0.01; apical: −14.5 ± 7.9% vs. −21.2 ± 4.4%; p < 0.01) and in the lateral segments (basal: −14.2 ± 5.5% vs. −15.4 ± 6.6%, n.s.; mid: −11.58 ± 5.8% vs. −13.73 ± 4.5%, n.s.; apical: −11.5 ± 6.6% vs. −17.2 ± 6%, p < 0.01).
Conclusions Two-dimensional strain is a simple and rapid method to measure GLS and PSS. This new technique might be very helpful to differentiate physiologic from pathologic LVH.
155 Electrocardiographic features of high training level athletes with bradycardia
N. Ville1, C. Zobo1, G. Kervio1, A. Gehanne1,2, F. Carré1,3
1Cardiovascular Research Group (EA3194) and Technological Innovation Center, Rennes 1 University, Rennes, France
2Cardiology Department, Pontchaillou Hospital, Rennes, France
3Functional Explorations Department, Pontchaillou Hospital, Rennes, France
Objectives High level of physical training may induce cardiac adaptations called “Athlete's heart”. Specific electrocardiographic (ECG) patterns, classically associated with autonomic nervous system (ANS) alterations are described. Bradycardia is a highly prevalent ECG characteristic in endurance trained athletes. The aim of this study was to describe the ECG features associated with pronounced bradycardia in high training level athletes.
Methods 283 male clinically healthy highly trained athletes, aged 18 to 35 years, with a pronounced resting bradycardia (heart rate, HR ≤ 50 beat/min) have been included in this prospective study. Resting 12-derivation ECG has been recorded then analysed. Studied parameters included HR, rhythm, P wave form in DII, presence of right (RBBB) or left bundle branch blocks, PR and QT interval durations and repolarisation peculiarities (classified as minor or major with a personal classification).
Results Bradycardia was always associated with a sinus rhythm. HR < 40 beat/min was observed in few subjects (7.8%). P wave was mostly normal and often bifid (67.7% and 31.9% of the athletes, respectively). PR duration was poorly correlated (r = 0.17, p < 0.01) with and not significantly influenced by the bradycardia level (4 HR ranges: ≤ 35, [35–40], [40–;45], [45–;50 beat/min]). Incomplete RBBB and repolarisation peculiarities were often observed (43.7% and 94.2% of the athletes, respectively), whatever the bradycardia level (χ2 = 4.1 and 1.7 respectively, p > 0.05). Repolarisation peculiarities classified as minor were noted in 91.0% of the athletes. They consisted in negative or diphasic T waves in V1 (76.7% of the athletes), tall and peaked V1 to V6 leads T waves (23.7%), early repolarisation syndrome (20.1%) and U wave (19.7%). Few repolarisation peculiarities classified as major were noted (7.6%). They mainly consisted in negative or diphasic T waves in V1, V2, V3 without any RBBB. None ST depression was observed.
Conclusion Marked resting athlete's bradycardia is rarely associated with other marked ECG abnormalities. Incomplete RBBB and minor repolarisation peculiarities are mostly observed but are not influenced by bradycardia level. Moreover and surprisingly, other patterns classically linked to ANS physical training adaptations such as PR duration and major repolarisation peculiarities were not linked to bradycardia level. Thus, athlete's ECG patterns physiopathology seems multifactorial and needs further research.
275 Study on prognostic value of thyroid hormone in the progression of syndrome differentiation type of TCM in patients with congestive heart failure (CHF)∗
ZhouJie, Gao Xiao-Ling, Zhang Bao-Zhou, HuangShi-Jun, Wang Lan-Di, ShengLi, Shi Dong-Jing, Yan Xiao-Xia, Yang A-Ni, Huang Teng-Hui, Pei Yu-Qing, Chen Jin-Fan, ChengXuan
Department of Cardiology, Gansu Provincial TCM Hospital, LAN Zhou 730050, P.R. China
∗The above research work won the second price for Huangpumi TCM science and technology awarded by Gansu province, P.R. China.
Corresponding to: ZhouJie, MD Department of cardiology, Gansu Provincial TCM Hospital, LAN Zhou 730050, P.R. China Tel: (+86)013893337012 Fax: (+86) 931–;2314730. E-mail:
Congestive heart failure (CHF) is the final common pathway of different heart diseases, but there are few reports on the relationship between thyroid hormone and the syndrome types described in TCM in patients with CHF. Multivariate linear regression analysis was used in this study. 100 patients with CHF were divided into four subgroups: the Heart-Qi Deficiency Syndrome (HQDS), the Yin Deficiency Syndrome (YDS), the Blood Stasis Syndrome (BSS) and the Oedema and Blood Stasis Syndrome (OBSS). Doppler echocardiography and thyroid hormone were used to observe the 4 groups. The results showed that the level of T3 in OBSS was obviously lower than that in the control group, HQDS, YDS and BSS (P < 0.01, P < 0.01, P < 0.05, P < 0.01, respectively). The levels of LVEF, mVcf in OBSS were obviously lower than that in the control group, HQDS, YDS and BSS (P < 0.01, all); the ratio of A/E in the control group was obviously lower than that in HQDS, YDS, BSS and OBSS (P < 0.01, all); the ratio of A/E in OBSS was obviously higher than that in BSS, YDS, HQDS and the control group (P < 0.01, all). Therefore, the data suggest that among the 4 TCM Syndrome-type groups of CHF, left ventricular systolic dysfunction (LVSD) can be seen in OBSS, while left ventricular diastolic dysfunction (LVDD) become more serious gradually with the progression of HQDS→YDS→BSS→OBSS, A/E radio may be as a quantitative indices for evaluation of the Syndrome Differentiation Type of TCM in patients with congestive heart failure. and the lowering of T4 may be, no less than mVcf, the prognostic predictor that correlated with LVEF of OBSS in patients with CHF.
Keywords Congestive heart failure; Thyroid hormone; Prognostic value; Syndrome differentiation type of TCM
322 Echocardiographic assessment of left ventricular hypertrophy regression in highly trained athletes after deconditioning
L. Maskhulia, N. Chabashvili, V. Akhalkatsi, T. Chutkerashvili, T. Svanishvili
Tbilisi State Medical University, Tbilisi, Georgia
Objectives Statistic studies have shown that the sudden death of a prominent athlete in the prime of life is devastating event and a result of cardiac disease in more than 80% of cases. Several autopsy-based studies have documented the diseases responsible for sudden cardiac death (SCD) in young competitive athletes with predominance of hypertrophic cardiomyopathy (HCM)(36%), coronary anomalies, unexplained increase in cardiac mass (10%). Extreme alterations in left ventricular (LV) morphology observed in athletes unavoidably raise critical issue of the clinical significance and consequences of the hypertrophy induced by training and the likelihood of complete reversibility after deconditioning. The purpose of our study was to investigate LV regression after deconditioning and to reveal the most persistent patterns of LV remodeling.
Methods Highly trained normotensive male athletes with increased LV mass index (> 125 g/m2) were selected on the basis of echocardiographic investigation (47 footballers and 5 wrestlers, mean age 22.57 ± 0.78 years). Eccentric hypertrophy (EH) was registered in 41, concentric hypertrophy (CH) in 9, concentric remodeling (CR) in 2. None of them had a family history of HCM or SCD; all denied use of illicit drugs. Standard resting 12-lead ECGs were performed. According to the ECG athletes were divided into 2 groups: 27 athletes with ECG abnormalities (group A), and 25 athletes with minor alterations or normal ECG (group B). During 10 weeks physical activity of group A was ceased, and for group B-restricted by 50% of its volume.
Results In the group A morphologic parameters decreased in 74% and ECG changes-in 81.5%, and in the B group the same parameters significantly decreased in 84% and ECG normalized in 96%. Changes in morphologic parameters did not depend on the chosen regimen of the altered physical activity (p > 0.2). Athletes with EH complete normalization of the morphologic parameters in 83%, and the athletes with CR- in 100%. 55.6% of the athletes with CH did not show regression of the morphologic parameters, in 42.9% of them ECG alterations were unchanged.
Conclusions 10-week period of detraining was not sufficient for the regression of the CH pattern. Incomplete resolution of marked increase of LV mass index needs longitudinal follow-up over longer periods and regular preparticipation examination of the athlete during sports career.
405 DIAKTIV (Endurance training compared with strength training in therapy of type-2-diabetics)
K. Edel1, M. Koster1, I. Aufderheide1, R. Degenhardt2
1Heart and Diabetes Clinic Bad Hermannsborn, 33014 Bad Driburg, Germany
2Clinical Research Institute, Centre for Cardiovascular Diseases, 36199 Rotenburg upon Fulda, Germany
Objectives Physical activity should be basic therapy in diabetic individuals. Especially type-2-diabetics should integrate appropriate activities in their daily routine to gain better blood glucose levels. Are there any differences between endurance and strength training in relation to cardiovascular effects? Is strength training a recommendable, alternative training method for type-2-diabetics?
Methods In this prospective randomised cohort study 32 obese type-2-diabetics were observed (17 female, 15 male, age: 61.4 ± 9.5 years) and either assigned to endurance training (AT) or strength training (KT). The groups realized the training 45 minutes twice weekly for 6 months (Oct. 2004 to Apr. 2005). The endurance group trained at 50–;65% V02 max. by ergocycling. The strength group used 5 working stations at 60–;80% of maximum strength level. At the beginning (T1), 3 months (T2) and 6 months (T3) a symptom limited bicycle ergometer test was carried out and HbA1c, total cholesterol, HDL-chol., LDL-chol., triglycerides, strength of extremities, BMI were analysed.
Results 2-way ANOVA for repeated measurements revealed no significant differences between the treatment groups in regard of the analysed parameters. HbA1c, cholesterol, HDL-chol., LDL-chol., increased from T1 to T2 presumable in consequence to the execution of the study in the winter time. Between T2–;T3 the previous parameters decreased approximately to the initial values (T1). HR at rest, bodyweight and BMI decreased in both groups from T1–;T3 (n.s.). Maximum capability (watt/kg bodyweight) increased continuously over 6 months (AT: p = .09; KT: p = .02).
Conclusion In spite of the unfavourable life habits at winter time the DIAKTIV-study provides evidence of positive cardiovascular effects in type-2-diabetics. The differences between the treatments were marginal. Strength training is obviously an alternative method in therapy of type-2-diabetics and should be recommended as well as endurance training.
412 Effects of regular exercise training on skeletal muscle regeneration in patients with end-stage chronic heart failure
R. Hoellriegel, S. Erbs, A. Linke, V. Adams, S. Gielen, R. Hambrecht, G. Schuler
University of Leipzig –; Heart Center, Department of Internal Medicine/Cardiology, Leipzig, Germany
Patients with chronic heart failure (CHF) are limited in their exercise capacity, in particular due to peripheral alteration. Inflammatory activation in advanced stages of the disease was recently shown to contribute to a loss in capillary density and loss in muscle mass finally leading to cardiac cachexia.
Given the regenerative capacity of exercise training, it was aim of the present trial to determine, whether physical exercise training influences capillary density in the skeletal muscle and whether this was associated with a change in exercise capacity in patients with CHF.
Methods 37 patients with CHF (LVEF 24 ± 2%, NYHA class IIIb) were randomized to 12 weeks of exercise training (30 min bicycle ergometer training daily at 50–;60% of peak oxygen uptake) or sedentary lifestyle (control). At begin and after 12 weeks patients were undergoing a biopsy of the vastus lateralis muscle and a spiroergometry. Capillary density was quantified applying immunohistochemestry.
Results 3 months of exercise training results in an increase in capillary density in the skeletal muscle by 17% from 1.45 ± 0.02 to 1.70 ± 0.02 capillaries/muscle fibre (p < 0.05 vs. begin and control). The training-induced increase in capillary density was associated with an improvement in oxygen uptake by 16% from 15.3 ± 0.8 to 17.8 ± 0.8 mL/min/kg at peak exercise (p < 0.05 vs. begin and control) and by 20% from 11.9 ± 0.6 to 14.2 ± 0.7 mL/min/kg at the ventilatory treshold (p < 0.05 vs. begin and control). All of the above-mentioned parameters remained virtually unchanged in the control group.
Conclusion In patients with severe chronic heart failure regular exercise training leads to an increase in capillary density in the skeletal muscle. This training-induced skeletal muscle regeneration is associated with an augmentation in exercise capacity in pts. with CHF.
435 Aortic root dimensions in a large serie of athletes
Boraita A1, De la Rosa A2, Heras E1, Rabadán M1, Santaella O1, Canda A1, Lamiel R3, Antón P1, García T1.
1Cardiology, Physiology and Anthropometry of Sport Medicine Center. Higher Sports Council, Madrid, Spain.
2Cardiology, Universitary Hospital of La Laguna, Tenerife, Spain.
3Cardiology, Hospital Ntra Sra de América, Madrid, Spain.
Objective Morphologic and functional adaptations of the athletés heart are well known. However, there are not enough studies about the aortic root (AR) in a large serie of athletes. Our purpose is to describe whether these adaptations affect or not the AR.
Methods 3415 (2330 males and 1085 females) elite athletes without cardiovascular diseases have been studied at the Sport Medicine Center of Higher Sports Council, between 1994 and 2005. All the athletes underwent physical examination including anthropometric evaluation, maximal incremental exercise test with oxygen uptake and echocardiographic study according to the recommendations of the American Society of Echocardiography. AR dimensions were measured by M-mode and 2D echocardiography at the anulus (PV), sinuses of Valsalva (SV), sinotubular junction (US), and the proximal ascending aorta (AA). The results were analysed according to gender and age: group 1 younger than 20, group 2 between 20–;30 and group 3 older than 30 years old.
Results Results are shown by gender and age in Table 1 (mean ± SD). Two-dimensional measurements at the SV (30,6 ± 3,8 mm) were larger than M-mode AR values (28,6 ± 3,8 mm; p < 0.001). Interestingly, a positive correlation between AR and body surface area (PV: r = 0,51; SV: r = 0,51; US: r = 0,46; AA: r = 0,48; p < 0.001) and between AR and age (PV: r = 0,25; SV: r = 0,32; US: r = 0,33; AA: r = 0,34; p < 0.001) was observed.
Conclusions Age, gender and body surface area affect the aortic dimensions in athletés heart although abnormal growth of the AR have not been observed. Measures of the AR in 2D mode have to be made to avoid mistakes. Presence of AR dilatation should not be considered as an adaptation of the athlete's heart.
437 Prevalence of hypertrophic cardiomyopathy in elite athletes
S. Basavarajaiah1, L. Carby2, M. Wilson2, A. Shah1, G. Whyte2, S. Sharma1
1Kings College Hospital, Denmark Hill, London UK SE5 9RS
2CRY Centre of Sports Cardiology, Olympic Medical Institute, Northwick Park hospital, Watford Road, Harrow, Middx HA1 3UJ
Objectives The prevalence of hypertrophic cardiomyopathy (HCM) in the general population ranges from 0.16 to 0.29%. The exact prevalence of HCM in highly trained athletes is unknown and has important implications with regards to a potential future national screening programme.
Methods Between 1996 and 2006, 3200 asymptomatic and normotensive elite athletes (75% males) aged between 14–;35 years (mean: 20.5 ± 5.80) and a mean body surface area of 1.86 ± 0.16 m2 (range1.36–;2.29) participating in 14 sporting disciplines underwent 12-lead ECG and 2D-echocardiography. No athlete had a family history of HCM or sudden cardiac death. Cardiac dimensions and function were measured using conventional methods.
Results Of the 3200 athletes, 33 (1.0%) had maximal left ventricular wall thickness (LVWTd) > 12 mm (mean: 13.60 ± 0.89, range: 13–;16). All 33 athletes were males. The mean left ventricular internal cavity dimension and left atrial diameter in the 33 athletes were 58.5 ± 5.14 mm and 32 ± 4.8 mm respectively. Indices of diastolic function were normal. Only 3 athletes (0.09%) had a non-dilated LV cavity and bizarre ECG changes that could have been consistent with the diagnosis of HCM. Their echocardiographic measurements are tabulated below:
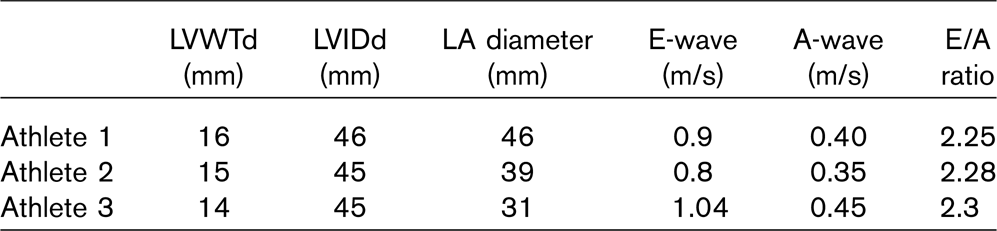
Only one of the 3 athletes could be persuaded to detrain for 3 months, which resulted in regression of left ventricular hypertrophy and normalisation of ECG changes that were seen before. The other 2 athletes did not have any other phenotypic features of HCM on exercise stress testing with gas exchange or 48-hour Holter monitoring.
Conclusion Although 1% of elite male athletes develop left ventricular hypertrophy > 12 mm and in the range compatible with the diagnosis of morphologically mild HCM, most (91%) have a dilated LV cavity indicating physiological LVH. In this study only 3 athletes had echocardiographic findings consistent with HCM but further investigations in all three failed to support the diagnosis. These results indicate that the prevalence of HCM in highly trained athletes is extremely rare. The augmentation of stroke volume required to generate large cardiac output during exercise probably selects out most individuals with HCM. Our findings question the validity of previous data, which propose that HCM is the commonest cause of exercise related death in young athletes.
438 Prevalence and significance of an isolated long QTc interval on a 12-lead ECG in elite athletes
S. Basavarajaiah1, M. Wilson2, L. Carby2, A. Shah1, G. Whyte2, S. Sharma1
1Kings College Hospital, Denmark Hill, London UK SE5 9RS
2CRY Centre of Sports Cardiology, Olympic Medical Institute, Northwick Park hospital, Watford road, Harrow, Middx HA1 3UJ
Objectives Congenital Long QT syndromes (LQTS) are relatively rare but a recognised cause of sudden cardiac death (SCD) in young athletes. Many individuals with congenital LQTS are asymptomatic and SCD may be the first presentation. The prevalence and significance of an isolated Long QTc (LQTc) interval on the 12-lead ECG in asymptomatic athletes has never been reported. Its identification represents a dilemma, since the diagnosis of congenital LQTS calls for permanent disqualification from competitive sports.
Methods Between 2002 and 2006, 1800 elite asymptomatic athletes aged between 14–;35 years (mean 20.26 ± 5.40) underwent 12-lead ECG as a part of pre-participation screening programme. Nine hundred and seventy five (69.64%) were male and 425 (30.4%) were female athletes. The QT interval was measured using callipers and corrected for the heart rate using Bazett's formula (QTc). Athletes with LQTc (> 440 ms in males and > 460 ms in females) were investigated further with 24-holter monitor and an exercise stress test. All athletes with a LQTc were offered genetic testing and their first-degree relatives were offered a 12-lead ECG.
Results Out of 1800 athletes, 7 (0.4%) (6 males and 1 female) athletes had LQTc interval. The QTc interval ranged from 460–;580 msec. Three males and one female athlete had QTc interval > 500 ms. None had a family history of syncope or SCD. Subsequent Holter monitoring did not reveal polymorphic ventricular tachycardia, but exercise stress testing demonstrated paradoxical prolongation of the QTc during the recovery phase in 3 (43%) of these athletes. All 3 of these athletes had a QTc > 500 msec and 2 had first degrees relatives with a LQTc on ECG. One among the 3 athletes was tested gene positive for LQT1. None of the other athletes had family members with prolonged QTc interval and the genetic results on these athletes for known LQT mutations have proved negative so far.
Conclusions The prevalence of an isolated LQT on the ECG in asymptomatic athletes is 0.4%. More than one third of our athletes with a LQT had other phenotypic manifestations of the disorder and their QTc interval > 500 msec was highly suggestive of LQTS. Our results indicate that the finding of an isolated LQTc is rare in athletes and warrants detailed investigations for congenital LQTS. Presence of LQTc on a 12-lead ECG in athletes is not a part of athletic heart syndrome.
442 Left ventricular remodelling in highly trained black athletes of African/Afro-Caribbean origin
S. Basavarajaiah1, L. Carby1, M. Wilson2, A. Shah1, G. Whyte2, S. Sharma1
1Kings College hospital, Denmark Hill, London UK SE5 9RS
2CRY Centre of Sports Cardiology, Olympic Medical Institute, Northwick Park hospital, Watford road, Harrow, Middx HA1 3UJ
Objectives Upper limits for physiologic left ventricular (LV) remodelling for the purposes of differentiation from cardiomyopathies are well established in Caucasian athletes. However, there are few data regarding physiologic LV remodelling in black athletes in whom deaths from hypertrophic cardiomyopathy (HCM) are more prevalent. This study compared ethnic differences in LV remodelling between Caucasian and black athletes.
Methods Between 2005 and 2006, 140 asymptomatic and normotensive black male athletes (mean age: 20.5 ± 5.80; range 14–;35 years and a mean body surface area: 1.94 ± 0.16 m2; range1.36–;2.29) underwent 12-lead ECG and 2-D echocardiography. The results were compared to those of 100 sedentary black males and 170 highly trained white male athletes (WA) matched for age, size, sport and training programs. None of them had a family history of cardiomyopathy. Left ventricular dimension and function were measured in accordance with American Society of Echocardiography guidelines.
Results The LV dimensions of black athletes (BA) compared with black controls (BC) and WA are tabulated below:

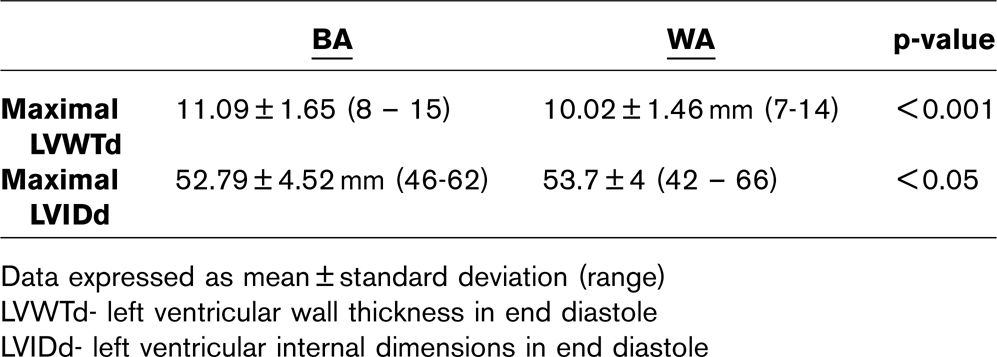
Data expressed as mean ± standard deviation (range)
LVWTd- left ventricular wall thickness in end diastole
LVIDd- left ventricular internal dimensions in end diastole
Both BA and WA had a greater LV dimensions than BC. The BA had greater LVWT than WA amounting to a 9.6% difference. In absolute terms, 24 (20%) BA had a LVWT > 12 mm compared with 9 (4.5%) WA.
However, WA had greater LVID than BA amounting to a difference of just under 2%. In absolute terms there was no difference in LVID between WA & BA as 4 in each group had LVID exceeding 60 mm. All BA with a LVWT > 12 mm had an enlarged left ventricular cavity size [55.64 ± 4.64 mm (52–;62)] and normal indices of diastolic function on Doppler studies (E wave, A wave, E/A ratio) indicating physiologic left ventricular hypertrophy rather than HCM.
Conclusion The magnitude of LVH in BA is slightly greater than in WA, however, more BA have absolute LVWT values in the region compatible with HCM. The physiological upper limits of LVWT and LVID for black athletes from our study is 15 mm and 62 mm respectively.
450 Exercise and opium usage
F. Fallahi1, Y. Shafaee2, N. Fallah3
1Medical Research Center, Shahed University
2Iran University
3Biostatistical Department, Shahed University
Background Opium usage may increase risk of cardiac events and arrhythmia. Indeed opium smoking is usually accompanying cigarette smoking that itself is suggested as the main cause of respiratory and cardiovascular disease and cancer. Also it is the most widespread factor of death in the world which is preventive. Several methods has been suggested to opium smoking cessation and one of them is exercise
Methods & Materials This study is planed in a “historical cohort” survey to obtain the role of exercise to decrease the use of opium smoking. For this mean, 200 men in two groups, 100 athletes and 100 non-athletes were examined by closed questionnaire.
Results This study showed that prevalence of opium smoking in athletes group is considerably lower than non-athletes group (2% against 11%, p = 0.009, CI 95%).
Conclusion Exercise and physical activity may have an important role in reduction of opium usage, it seems to promote exercise program especially in teenagers can decrease significantly the usage of opium and cigarette in society.
472 Master marathon runners have a reduced Framingham risk score but the extent of coronary atherosclerosis is underestimated
Stefan Möhlenkamp1, Nils Lehmann2, Gert Kerkhoff3, Martina Bröcker-Preuss4, Thomas Budde3, Karl-Heinz Jöckel2, Klaus Mann4, Raimund Erbel1
1West German Heart Center Essen, Dept. of Cardiology, University Clinic Essen
2Institute of Medical Informatics, Biometry, and Epidemiology
3Clinic of Internal Medicine and Cardiology, Alfried Krupp Hospital Essen
4Institute of Clinical Chemistry and Laboratory Medicine, University Clinic Essen
Background Coronary atherosclerosis is the main cause of exercise-associated death in athletes > 35 years. Routine screening of athletes for cardiovascular disease is, however, currently not recommended. In this study we measure the prevalence and extent of cardiovascular risk factors (RF) and of coronary artery calcium (CAC) in advanced-age marathon runners in comparison to matched controls from an unselected general population.
Methods Male marathon runners (n = 108, inclusion criteria: age > 50 yrs, at least 5 marathon races (42,195 km) during the previous 5 years, no known heart disease, no diabetes) were invited to participate. Standard RF were measured to calculate the Framingham risk score (FRS). CAC (Agatston score) was measured using electron beam CT. Marathon runners were matched 4:1 by age (n = 424) and 2:1 by age and RF (n = 216) with asymptomatic presumably healthy males from the Heinz Nixdorf Recall Study (HNRS), an ongoing prospective population-based trial on the predictive value of established RF and novel imaging modalities.
Results Marathon runners (57 ± 7 years) had completed 20 marathons and exercised regularly since 9 yrs (5x/week, 55 km/week) (median values). Conventional RF were improved in marathon runners in comparison to age-matched controls (BMI: −14%, systolic blood pressure: −10%, LDL-cholesterol: −18%, HDL-cholesterol: + 42%, (mean±SD (reduction vs. HNRS-cohort), p < 0.01 each), resulting in a significant reduction of FRS (7.0 ± 3.6 (−49%), p < 0.001)). Yet, marathon runners had a similar CAC burden in comparison to age-matched controls (Q1/median/Q3 = 0/36/217 versus 3/40/159, p = 1.0). In comparison to age- and RF-matched controls, i.e. FRS: 7.7 ± 3.4, a CAC score > 100, indicating increased cardiovascular risk, was more frequent in marathon runners (36.2%) as compared to age- and RF-matched controls (22.2%, p < 0.003).
Conclusion Regular marathon running in males > 50 years reduces the Framingham risk score by 50%. Despite this favourable risk profile, the extent of subclinical atherosclerosis was significantly higher as compared to age- and RF-matched controls from the general population. The unexpectedly high coronary atherosclerotic burden may in part account for some of the exercise-related cardiovascular events in master marathon runners.
500 Assessment of cardiac autonomic nervous system function following exercise training and detraining in hemodialysis patients
E. Kouidi1, M. Petraki1, G. Koukouvou1, J. Kalevrosoglou2, E. Konstantinidou1, D. Grekas2, A. Deligiannis1
1Lab. of Sports Medicine, Aristotle University of Thessaloniki, Thessaloniki, Greece
2A' Internal Medicine Clinic-Renal Unit, Aristotle University of Thessaloniki, Thessaloniki, Greece
Cardiac autonomic nervous system (ANS) dysfunction is common in hemodialysis (HD) patients. It is reported that exercise training can effectively modify the autonomic imbalance. However, the effects of detraining on the sympathovagal interaction have not been studied yet. Thus, the aim of this study was to assess the effects of exercise training and detraining on cardiac autonomic outflow in HD patients. Fifteen HD patients free of any other systemic disease (group A-aged 56.3 ± 9.1 years) were studied at entry and after 6 months of training with stationary bicycles during their HD sessions (3/weekly), as well as following 4 months of detraining. Moreover, ten sex- and age-matched HD patients (group B) remained untrained and were used as controls. The dialysis prescription and the level of anemia were constant during the study. At entry and after training and detraining cardiac ANS was evaluated by time- and frequency-domain heart rate variability (HRV) calculation from ambulatory 24-hour Holter monitoring. The following parameters of HRV were measured: standard deviation of NN intervals (SDNN), the mean square successive differences (rMSSD), percent of NN intervals differing > 50 ms from the preceding NN (pNN50), low (LF) and high (HF) frequency components of the autoregressive power spectrum of the NN intervals and their ratio (LF/HF). The effects of training and detraining on aerobic capacity (VO2peak) were evaluated by cardiopulmonary exercise testing. Baseline measurements of the two groups were similar. Results of group A are shown in the table:
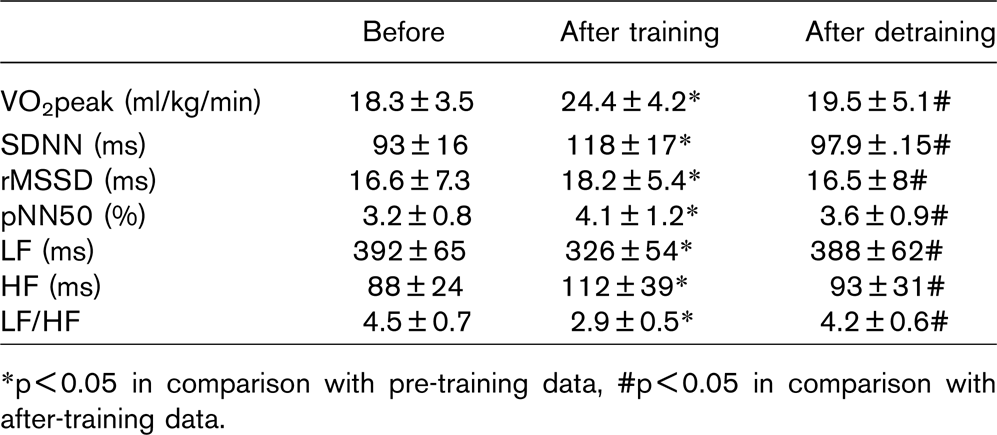
∗p<0.05 in comparison with pre-training data, #p<0.05 in comparison with after-training data.
In group B none of the above variables altered significantly over time. It is concluded that after only few months of detraining, significant reductions in the exercise training adaptations on both cardiac ANS activity and work capacity are demonstrable. Therefore, an active lifestyle is recommended for HD patients.
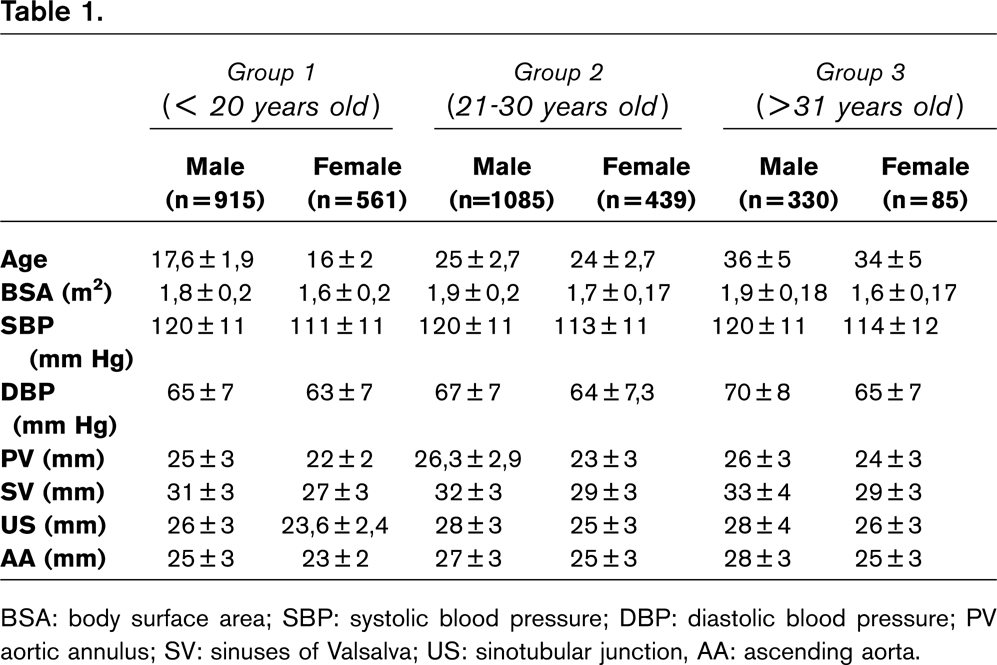
BSA: body surface area; SBP: systolic blood pressure; DBP: diastolic blood pressure; PV aortic annulus; SV: sinuses of Valsalva; US: sinotubular junction, AA: ascending aorta.
503 Cardiac adaptation and structural and functional peculiarities of the athletes' cardiovascular system
O. Orlovs1,2, I. Pontaga2, A. Konrads2, V. Larins2
1Latvian Olympic Team
2Latvian Academy of Sport Education
Background Regular intensive exercise training is associated with structural and functional changes of the myocardium, cardiac chambers cavities volume and cardiac systolic and diastolic functions.
Objective The objective of the study was estimated of routine echocardiography and veloergometer test in elite winter biathlon athletes and young basketball players.
Methods We examined 20 elite winter biathlon athletes (males, aged 21, 3 ± 4, 5) and 15 National U –; 18 team basketball players (males, aged 17, 3 ± 0, 8) by echocardiography according to the ASE guidelines. Veloergometer test and ventilation function and gas analyzing we were estimated by our method from 0, 5 W/kg to 2 W/kg in the end of test. It was aerobic fitness and end heart rate was 120–;140 beats per minute. Lactate was assessed by express methods.
Results The mean left ventricular end diastolic size was 53, 90 ± 3, 00 mm in biathlon athletes and 55, 45 ± 0, 34 mm in basketball players. End diastolic thickness of the posterior wall was 11, 03 ± 1, 11 mm in biathlon athletes, and 10, 14 ± 1, 03 mm in basketball players. The mean left ventricular end diastolic volume was 141, 3 ± 13, 5 cm3 in biathlon athletes, and 172, 4 ± 32, 0 cm3 in basketball players. No structural heart disease was found and systolic and diastolic functions were normal in all athletes. Peak oxygen consumption was 56 ± 6 ml/min/kg. But basketball players had body mass 88, 9 ± 12, 4 kg and height 195, 7 ± 7, 0 cm (BSA > 2, 10 ± 0, 12 m2).
Conclusion The largest heart stroke volume was observed in athletes trained in winter biathlon many years. The basketball players had largest cardiac end diastolic volume, but their stroke volume was smaller in comparison with biathlon athletes. Basketball players had highest heart rate values than biathlon athletes during the same intensity exercise. The heart rate increase with growth of the power of exercise in basketball players was faster than in biathlon athletes. The data confirm the better cardiovascular system adaptation of athletes trained in biathlon to endurance exercise than of young basketball players.
543 Prevalence of atrial fibrillation in former –; and still active long term endurance cross-country skiers. A 28–;30 years follow-up study
Jostein Grimsmo MD PhDstud°, Irene Grundvold MD1, Harald Arnesen MD PhD1, Sverre Mæhlum MD PhD2, Håkon Lie, MD PhD3
Ullevål University Hospital/ University in Oslo
°Department of Cardiac Rehabilitation, Feiringklinikken (The Feiring Clinic), Feiring, Norway
1Department of Cardiology, Ullevål University Hospital, Oslo, Norway
2Norwegian Institute of Sports Medicine (NIMI Ringerike), Hønefoss, Norway
3In Private Practice, Røa, Oslo
Objectives The prevalence of atrial fibrillation is approximately 0,4% in the general population and increases with age to probably more than 10% at ages over 75–;80 years. Atrial fibrillation in athletes may be more common than in the general population at the same age. This question is still unresolved.
We studied a group of endurance cross-country skiers after 28–;30 years in a follow-up study. The aim of the study was to find the prevalence of atrial fibrillation in this population.
Methods and results The population was previously studied in 1976 and consisted of 122 long-time active, highly trained cross-country skiers belonging to three preselected age groups (group I 26–;33 years, group II 43–;50 years, group III 58–;64 years). All now living men were invited to participate in our 28–;30 years follow-up study. Out of the initial 122 men 36 (29,5%) had died, with 1/35 in group I, 7/48 in group II and 28/39 in group III. Of the 86 still living 78 responded (90,7%). The tests included a resting ECG, maximal treadmill test with VO2 max and exercise ECG (not group III), echocardiography and two questionnares. 13 (16,7%) had developed paroxysmal or permanent atrial fibrillation with 6/27 (18,2%) in group 1, 5/32 (13,5%) in group II and 2/6 (25%) in group III. 11 (14,1%) seems to have developed atrial fibrillation with the first appearance at the average age of 57,8 years (38 –; 72), without known structural heart disease at the time of appearance. 2 out of 6 with paroxysmal atrial fibrillation had only had 1 and 3 episodes respectively. 2 (87 and 80 years old) developed permanent atrial fibrillation in 2004 and 2005 after many years with coronary heart disease.
Conclusion Atrial fibrillation is quite common in this population. The findings support the assumption that long term endurance exercise at this level may predispose to atrial fibrillation.
559 Correlation of electrocardiographic and echocardiographic presentation with cardio-pulmonary capacity in professional soccer players
Renata Glowczynska, Sebastian Szmit, Anna Budaj, Janusz Kochanowski, Krzysztof J. Filipiak, Grzegorz Opolski
Medical University of Warsaw, 1st Department of Cardiology
Aim Assessment of athlete's heart on echocardiography (ECHO) in relation to cardio-pulmonary capacity in Cardio-Pulmonary Exercise Test (CPET) and features in electrocardiography (ECG) in professional soccer players.
Materials 17 professional Polish soccer players underwent ECHO (Philips iE33), CPET (ZAN 680) and ECG.
Results Correlations between ECHO presentation and CPET parameters or signs of LV hypertrophy in ECG were estimated in univariate analysis of linear regression as well in Mann-Whitney's U test.
Players with left ventricle diastolic diameter (LVDD) over 52 mm had significantly elevated levels of oxygen consumption at anaerobic threshold (VO2AT, p = 0.0017), ventilatory equivalent for oxygen at anaerobic threshold (VE/VO2@AT, p = 0.002), maximal energy exercise (p = 0.02) and greater sum of R wave voltage in lead V1 and S wave voltage in lead V5 (p = 0.018).
LV systolic diameter (LVSD) over 35 mm was consisted with higher VE/VO2@AT (p = 0.03) and maximal carbon dioxide production (VCO2 max, p = 0.038).
Players with interventricular septum (IVS) thicker than 10 mm had higher levels of peak oxygen uptake (VO2peak, p = 0.015), VO2AT (p = 0.003), VCO2 max (p = 0.004), maximal exercise energy (p = 0.006) and rate of oxygen uptake normalized for body weight, age and sex (VO2% N, p = 0.01).
Players with posterior wall (PW) greater than 9 mm had significantly elevated VO2AT (p = 0.035) and VCO2max (p = 0.046). LV mass exceeding 189 g was related to higher VO2AT (p = 0.036), VCO2max (p = 0.02) and lower R wave voltage in lead aVL (p = 0.04). What is more, greater LV mass was correlated with maximal exercise energy (r = 0.579, p = 0.01), VO2peak (r = 0.54, p = 0.02), VO2%N (r = 0.525, p = 0.03) and VCO2max (r = 0.519, p = 0.03). Players with LV mass index greater than 97.4 g/m2 had higher VCO2max (p = 0.004), maximal exercise energy (p = 0.03) and lower R wave voltage in lead aVL (p = 0.001).
Conclusions Greater LV diameters were correlated with metabolic exercise parameters and ventilation equivalents of VO2 and VCO2. LV diameter and LV mass were consisted with parameters of oxygen consumption on CPET. Echocardiographic and electrocardiographic features dependent on aerobic capacity estimated in CPET.
574 Correlation of cardio-pulmonary capacity in Cardio-Pulmonary Exercise Test (CPET) with electrocardiographic (ECG) and echocardiographic (ECHO) presentation and laboratory findings in professional soccer players
S. Szmit, R. Glowczynska, A. Budaj, J. Kochanowski, K. Filipiak, G. Opolski
Medical University of Warsaw, Warsaw, Poland
Materials 17 polish soccer players of champion-team of polish league underwent ECG, ECHO (Philips iE33) and CPET (ZAN 680).
Results In univariate analysis of linear regression LV mass was correlated with peak oxygen uptake (VO2peak, r = 0.54, p = 0.02), oxygen consumption at anaerobic threshold (VO2AT, r = 0.46, p = 0.06), rate of oxygen uptake normalized for body weight, age and sex (VO2%N, r = 0.525, p = 0.03), rate of VO2AT normalized for body weight, age and sex (VO2AT%N, r = 0.459, p = 0.06).
In Mann-Whitney U test players with VO2peak > 66.4 ml/kg/min and VO2%N > 153.5% had significantly greater LV mass (p = 0.046). Players with VO2AT > 34.75 ml/kg/min and VO2AT%N > 80.5% had significantly greater sum of R wave voltage in lead V1 and S wave voltage in lead V5 (p = 0.028) and LV mass index (p = 0.017).
Players with ventilatory equivalent for oxygen at anaerobic threshold (VE/VO2@AT) > 23.6 had significantly greater LV mass (p = 0.046). Players with maximal CO2 production (VCO2 max) > 5.4 l/min had significantly lower R wave voltage in lead aVL (p = 0.005).
Players with max energy exercise > 1469 kcal had significantly lower R voltage in aVL (p = 0.03).
Moreover, players with VO2AT > 34.75 ml/kg/min had significantly higher level of lactate dehydrogenase (LDH, p = 0.019). Ventilatory equivalent for max CO2 production (VE/VCO2 max) > 29 was related to elevated level of serum creatine phosphokinase (CK, p = 0.0038). Players with maximal energy exercise > 1469 kcal had significantly lower CK-MB level (p = 0.01). Resting energy expenditure (REE) was correlated with hemoglobin (r = 0.515, p = 0.029). Maximal energy exercise was related adversely with CK-MB level (r = −0.57, p = 0.035), as well as VCO2 max with CK-MB level (r = −0.52, p = 0.05).
Conclusions
The soccer players with better aerobic capacity had greater sum of R wave voltage in lead V1 and S wave voltage in lead V5 and lower R wave voltage in lead aVL in ECG.
LV mass was correlated with all parameters of oxygen consumption on CPET.
Metabolic exercise parameters and ventilation equivalents for VO2 and VCO2 were consisted with LV mass and selected laboratory findings in soccer players.
594 BIA method, more sensitive in body composition evaluation than traditional methods, BMI and SKF thickness?
M. Dabetic, S. Mazic, J. Suzic, S. Ostojic, S. Zivanic, N. Dikic.
Sport Medicine Association of Serbia, Belgrade, Serbia
Objectives In this pilot study we compared 3 methods for evaluating body composition: body mass index (BMI), skinfold (SKF) thickness and bioelectrical impedance analysis (BIA) in elite basketball players. The aim was to show that BMI cut-off points are not superior parameters in estimating health risk associated with obesity in athletes and to show that BIA method is reliable method for evaluating body composition.
Methods Thirty-six elite basketball players aged 18–;32 were tested in pre-participation period. Body fat percentage (BF %) was estimated by BIA method using segmental body composition analyser Tanita BC−418 and SKF thickness method using calliper. BMI > 25 kg/m2 and BMI ≥ 30 kg/m2 were used as criteria for overweight and obesity respectively. Body fat percentage > 22% was the criteria for obesity in this age group. After anthropometric measurement ergospirometric testing was performed (Cosmed Quark b2).
Results Mean age of the athletes was 23.7 ± 3.4 years (height 201.5 ± 7.6 cm, weight 99.6 ± 10.3 kg). Mean years of training were 12.1 ± 4.2 (hours of training per week 22.0 ± 7.6 h). Mean VO2max was 53.4 ± 4.9 ml/kg/min. Their BMI, BF% measured by BIA method and SKF thickness were: 24.7 ± 1.9 kg/m2, 12.1 ± 3.2%, 10.9 ± 3.3%, respectively. Eighteen participants (50%) had BMI > 25 (max value of 28.3 kg/m2). Mean BF% in that group was 12.9 ± 2.9% measured by SKF method, and 13.9 ± 2.2% measured by BIA method. BIA method statistically significant correlated with SKF (r = 0.77; P < 0.0001).
Conclusions Preliminary results have shown that BMI is less sensitive method for evaluating body composition in athletes. From another side, BIA method could be useful tool for assessing body composition of athletes. It is equally reliable as SKF method, takes less time, does not need skilled personal and reduces human mistake. We believe that BIA method could be used routinely in everyday clinical practice and preventive medicine.
Key words BMI, BIA, SKF, overweight