
Abstract

The European Heart Health Charter and the Guidelines on cardiovascular disease prevention
The European Heart Health Charter advocates the development and implementation of comprehensive health strategies, measures and policies at European, national, regional and local level that promote cardiovascular health and prevent cardiovascular disease.
These guidelines aim to assist physicians and other health professionals to fulfill their role in this endeavour, particularly with regard to achieving effective preventive measures in day-to-day clinical practice.
They reflect the consensus arising from a multi-disciplinary partnership between the major European professional bodies represented.
Why develop a preventive strategy in clinical practice?
Cardiovascular disease (CVD) is the major cause of premature death in Europe. It is an important cause of disability and contributes substantially to the escalating costs of healthcare.
The underlying atherosclerosis develops insidiously over many years and is usually advanced by the time that symptoms occur.
Death from CVD often occurs suddenly and before medical care is available, so that many therapeutic interventions are either inapplicable or palliative.
The mass occurrence of CVD relates strongly to lifestyles and to modifiable physiological and biochemical factors.
Risk factor modifications have been shown to reduce CVD mortality and morbidity, particularly in high risk patients.
What are the objectives of these guidelines?
To help health professionals to reduce the occurrence of coronary heart disease, stroke and peripheral artery disease and their complications.
To achieve this by providing practical and accessible advice with regard to the rationale for prevention, priorities, objectives, risk assessment and management through lifestyle measures and selective drug usage.
To encourage the development of national guidance on CVD prevention through the formation of multidisciplinary national guideline and implementation partnerships that are compatible with local political, social, economic and medical circumstances.
Chapter 1: Introduction
The rationale for an active approach to the prevention of atherosclerotic cardiovascular disease (CVD) is based on some key points:
CVD is the major cause of premature death in most European populations. It is also a major cause of disability and contributes substantially to the escalating costs of healthcare.
The underlying atherosclerosis develops insidiously over many years and is usually advanced and difficult to reverse by the time that symptoms occur.
Death, myocardial infarction and stroke frequently occur suddenly and before medical help is available. It follows that many therapeutic interventions are either inapplicable (if death occurs suddenly) or palliative.
The mass occurrence of CVD relates strongly to modifiable lifestyle and pathophysiological factors.
CVD is rare in countries where population risk factor levels remain low through adult life.
Risk factor modifications have been unequivocally shown to reduce mortality and morbidity, particularly in high risk patients.
These considerations have informed the new ‘European Heart Health Charter'. This charter is explained in some detail at the end of chapter 3.
By the early 1990s there was a plethora of similar yet confusingly different national and international guidelines for the prevention of CVD. In order to try to define the areas of agreement, the European Atherosclerosis Society, the European Society of Cardiology and the European Society of Hypertension agreed to collaborate, resulting in a set of recommendations for the prevention of coronary heart disease that was published in 1994 [1]. These guidelines were revised in 1998 and 2003 by the second and third Joint Task Forces [2, 3]. A strength of the guidelines is that, from the outset, it was stressed that CVD is usually the product of multiple interacting risk factors. This resulted in the production of risk charts that attempt to simplify the estimation of total or ‘global’ CVD risk, and a realization that risk management requires attention to all modifiable risk factors.
It was appreciated that the original partners needed assistance from other bodies and experts, in particular in the fields of behavioural medicine and diabetes. In addition it is acknowledged that much practical preventive advice is delivered by family doctors, nurses and through voluntary bodies such as Heart Foundations. These considerations are reflected in the expanded partnership represented in the present guidelines, and in the list of experts whose input has been sought.
The Third Joint Task Force Guidelines saw a change from coronary heart disease to cardiovascular disease prevention, to reflect the fact that atherosclerosis may affect any part of the vascular tree. A new risk chart Systematic COronary Risk Evaluation (SCORE) was developed which was based on 12 European cohort studies and allowed the estimation of 10-year risk of cardiovascular death. Separate charts were produced for high and low risk regions of Europe. More explicit clinical priorities were developed. Less emphasis was placed on the terms ‘primary’ and ‘secondary’ prevention since risk is a continuum – persons may have investigational evidence of atherosclerotic disease. A rigorous external review process was undertaken.
The Fourth Joint Task Force has taken note of feedback in several areas:
The guidelines are becoming long and unwieldy. Contributors were asked to summarize key points from the Third Joint Task Force Guidelines, but to focus on what is new. The full text of the Guidelines remains available on www.escardio.org.
More detailed guidance was sought from the the World Organization of National Colleges, Academies and academic associations of general practitioners/family physicians (WONCA) and from the ESC Working Group on Cardiovascular Nursing, since these bodies represent the professionals that are heavily engaged in the practical delivery of preventive advice in many European countries.
The SCORE risk charts may overestimate risk in countries that have experienced a decline in CVD mortality, and underestimate risk if mortality has increased. The development of national guidance has always been recommended by the Task Force and, as part of this process, recalibration of the SCORE charts to allow for time trends in both mortality and risk factor distributions is recommended. In the third Joint Guidelines the need to address the problem of a high relative but low absolute risk in younger persons was dealt with by extrapolating a young person's risk to age 60 to flag persons who will become at high absolute risk. If interpreted too literally, this approach might result in excessive use of drug treatments in young people. In the present guidelines, this approach has been replaced with a simple relative risk chart to be used in conjunction with the SCORE absolute risk chart.
A reexamination of the SCORE data sets indicated that the impact of self-reported diabetes on risk may have been underestimated. The issue of predicting total events as well as just CVD mortality also receives more attention.
A separate section on gender issues has been added.
Renal impairment may have been underestimated as a risk factor and is dealt with in more detail.
These Guidelines attempt to find areas of broad agreement among different professional bodies and scientific disciplines. With the help of the World Organization of National Colleges, Academies and academic associations of general practitioners/family physicians (WONCA), a particular effort has been made to harmonize the advice that may be given to primary care and second-line care health professionals. The production of more detailed guidelines by the partner societies is encouraged. As examples reference is made to the ESH/ESC guidelines on the management of arterial hypertension [4] and to the guidelines on diabetes, prediabetes and CVD by the ESC/EASD [5]. Implicit in this partnership process is that these will be compatible with the generic Joint Guidelines.
The development of national guidance on cardiovascular disease prevention is also specifically encouraged. The Joint Guidelines should be regarded as a framework from which national guidelines can be developed to suit local political, economic, social and medical circumstances. The production of guidelines is only one step in the process of prevention, and the development of national multidisciplinary implementation partnerships is recommended; the section on implementation addresses some of the issues involved.
It should be appreciated that the Fourth Joint Task Force Guidelines are for the use of physicians and other health professionals engaged in clinical practice. Therefore they give the highest priority to those individuals at highest CVD risk because such persons gain most by active risk factor management. But they should be complemented by national and European public health strategies aimed at whole populations in a co-ordinated and comprehensive effort to reduce the enormous burden of cardiovascular disease that afflicts European populations. In this way we hope that the guidelines will promote higher quality of care to help reduce this burden and cardiovascular diseases in Europe.
Chapter 2: The scope of the problem: past and future
Cardiovascular diseases (CVDs) are the major causes of death, hospital admissions and disability in the middle aged and elderly in Europe. By the year 2000, they were the direct cause of more than 4.35 million deaths in the whole of Europe (1.9 million in the European Union) and they accounted for 43% of all deaths in men and for 55% in women of all ages (including 40% of all deaths under age 75) [6]. It is not widely appreciated that CVDs are the main cause of death in women as well as men in all countries of Europe (Table 1) [7].
The European average rate of hospital discharges due to CVDs was 2557 per 100 000 population at around year 2002. Although 695 per 100 000 were due to CHD and 375 per 100 000 to stroke, more than half were due to other forms of heart disease of which the largest single component is usually heart failure.
All deaths from circulatory disease In Europe
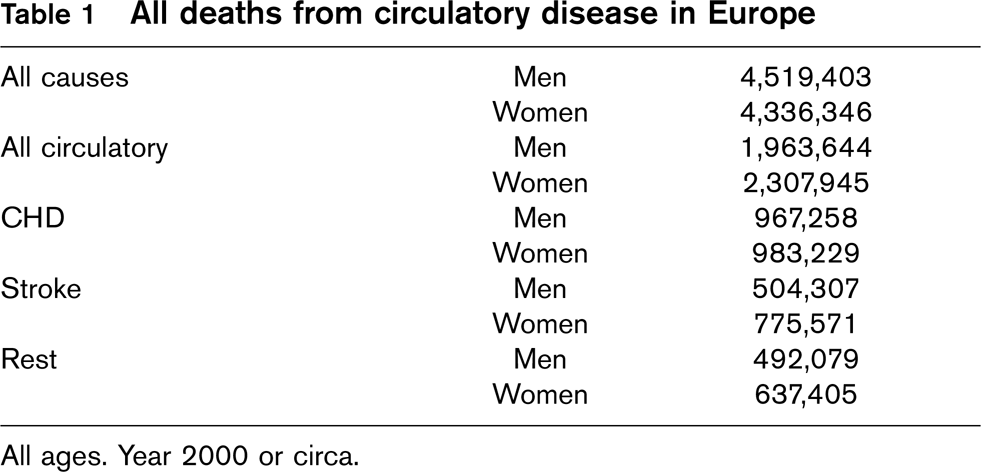
All ages. Year 2000 or circa.
In high income countries coronary heart disease (CHD) was responsible for the loss of 12.4 million disability adjusted life years (DALYs) and stroke for 9.4 million DALYs [8] whereas in the whole of Europe CVDs caused the loss of 34 million DALYs [6], that is 23% of all DALYs lost. The estimated total costs of CVDs in the EU countries were 168 757 million Euro in 2003 [9].
CVD mortality rates vary with age, gender, socioeconomic status, ethnicity and geographical region. Mortality rates increase with age and are higher in men, in people of low socio-economic status [10], in Central and Eastern Europe and in immigrants of South Asian origin [11–13]. There are marked socio-economic gradients in CHD morbidity and mortality within European countries. These differences are partially explained by socio-economic differences in conventional risk factors, such as smoking, blood pressure, blood cholesterol and blood glucose [10].
Total CVD mortality has been falling consistently, both in middle and older ages, since the 1970s in Western Europe [14]. Mortality rates have only recently started to decline in Central and Eastern Europe and they remain very high in these countries [15]. There is still nearly a 10-fold difference in CHD mortality between Eastern European countries and France among men aged 35-74 and up to six-fold difference in stroke mortality. Recent evidence strongly suggests that the recent declines in CHD mortality in certain Central European countries are related to population-wide behavioural changes in nutrition and smoking [16] similar to those which occurred earlier in other parts of Europe [17, 18]. While changes in mortality rates occurred both for CHD and stroke, the relationship of population changes in stroke with population decreases in classical risk factors is less consistent. While there is a relationship between blood pressure and stroke changes in women, it is less clear for men [19]. Blood pressure decline at population level is not attributable to an increase in the proportion of treated hypertension, indicating that despite the importance of medication to individuals, other determinants of blood pressure lowering are more powerful in whole populations [20].
The incidence of CHD [21] and of stroke [22] have also been declining in Western Europe but increasing in some countries, principally in Eastern Europe and in some Mediterranean countries [23]. The ratio of nonfatal to fatal acute myocardial infarction (AMI) events is 1 to 2 [21] and 1.5 to 5.5 for nonfatal to fatal stroke [22] between ages 35 and 64 years, although the ratios vary by country, age and sex.
Changes in CHD mortality at the end of the 20th century were mostly explained by changes in incidence rather than changes in short-term case fatality of AMI [21]. Likewise, other observational studies have shown that decreases in major risk factors like smoking, serum cholesterol and blood pressure explained more than 50% of the decline of CHD mortality [24–26]. The implications of these findings are that major emphasis is needed on the control of risk factors and of the determinants of incident CHD. A recent study on the decrease in US deaths from coronary heart disease between 1980 and 2000 attributed approximately half of the decline to reductions in major risk factors and approximately half to evidence-based medical therapies [27].
The EuroAspire surveys showed that risk factors remain poorly controlled in patients with established CHD, particularly obesity, smoking and blood pressure [28–30], especially in diabetic patients [31]. It is clear that more effective and organized national implementation strategies for guidelines are needed.
Recently published observational studies emphasize the importance of a favourable cardiovascular risk profile for young and middle-aged men and women. This effect is seen in different ethnic and socio-economic groups. It is lifestyle related, impacts on fatal and nonfatal CHD and stroke and promotes health-related quality of life in older age [32–37].
Improving survival after an acute CHD event is resulting in an increased prevalence of CHD in older people, particularly women [38]. Since diabetes is a more powerful risk factor for women than men [39], risk factor control among diabetic women becomes a special priority. As the prevalence of overweight and obesity are increasing in most countries [40], it is likely that the prevalence of type 2 diabetes with all its cardiovascular and other complications will also increase. Hence, control of the growing obesity epidemic is a priority.
The clinical manifestations of CVD may be very different. Hospital statistics reveal only the tip of the iceberg since sudden cardiac death occurring outside the hospital still represents a large proportion of all cardiovascular deaths.
2.1 Coronary morbidity
In the hospital different labels are used to classify patients presenting with chest pain, dyspnoea, syncope or other cardiac symptoms.
The widespread introduction of troponins into the diagnostic processes is likely to lead to a shift in the proportion of patients from those formerly diagnosed with unstable angina to those diagnosed with non-Q-wave myocardial infarction [41].
Stable angina is a well-recognized clinical syndrome whose natural history is well described. The incidence of new cases of stable angina pectoris diagnosed in primary care is about 2 per 100 per annum among patients aged over 45 years in Finland [42], considerably higher than the incidence of acute myocardial infarction. Intriguingly neither the incidence of diagnosed angina nor the prevalence of typical angina symptoms in the general population [43] show the marked male excess characteristic of myocardial infarction. Stable angina pectoris confers a markedly increased risk of coronary death compared to expected rates in the general population. In relative risk terms these effects are as strong in women as they are in men, based on a large series of primary care diagnosed patients in Finland [42]. The absolute risk of coronary death and nonfatal myocardial infarction among patients with angina (but without a history of heart attack) depends on case definition. In this national sample aged 45-89 years, about three quarters of all cases were treated pragmatically, without diagnostic test abnormality, among whom annual event rates were 1.28 per 100 person years in women and 2.76 in men. Among patients with an abnormal coronary angiogram or exercise ECG test the annual event rates were higher at 3.74 and 6.51, respectively. Thus patients with angina constitute a ‘high’ risk group, even among women and those without test abnormalities.
As with other manifestations of chronic ischaemic heart disease the burden on the health services in terms of diagnostic and revascularization procedures is predicted to rise in line with an increase in the proportion of elderly in European populations.
2.2 Heart failure
Pump failure of the heart is a common cause of death in the elderly although this not always reflected in mortality statistics because of the limitations of coding rules. Hospital admission rates for heart failure have been increasing in the United States [44] and in Europe [45–47]. The epidemiology of heart failure is described elsewhere [48, 49]. Hypertension, obesity and diabetes are major risk factors. Although a small proportion of clinical cases are due to valve disease (often linked with ischaemia), or to cardiomyopathy, epidemiological studies suggest that, in well developed countries, the majority of cases are due to ischaemia [50, 51].
2.3 Aortic aneurysm and dissection
Aortic aneurysm is also atherosclerotic in nature and increasing mortality trends have been shown in some European countries [52]. It is a potentially preventable cause of death, particularly when confined to the abdominal aorta. The prevalence is 5% in men aged 60 years or more and 1-2% in women. Screening for this condition has been suggested since elective surgical repair carries a 5-8% 30-day mortality in comparison with 50% mortality for ruptured aneurysm; a trial of screening conducted in the United Kingdom has shown encouraging results [53].
2.4 Peripheral arterial disease
It is known that coronary and peripheral vessels are affected by the same disease process, requiring the same treatment modalities. However, despite the high prevalence, until recently little attention has focused on the prevention and treatment of peripheral arterial disease (PAD) or ‘arteriosclerosis obliterans'. PAD occurs almost as frequently in women as in men [54]. The disease is often asymptomatic and underdiagnosed. Over half of the patients are asymptomatic and of patients with mild to moderate PAD who are symptomatic, only about one third report intermittent claudication [55]. Patients with PAD have much higher rates not only of limb amputation but also of coronary heart disease, myocardial infarction, stroke and death [56]. Despite the well known strong association with cardiovascular morbidity and mortality, patients with PAD are less likely to receive appropriate treatment for their risk factors than are those being treated for CHD. The correlation of PAD with CHD reflects the widespread nature of atherosclerosis. However, some minor differences have emerged from epidemiological studies regarding the risk factors for these diseases. Smoking appears to be more important in the aetiology of PAD than in CHD [57]. A positive family history, hypertension, diabetes, dyslipidemia including increased total and LDL-cholesterol and decreased HDL-cholesterol, increased fibrinogen and C-reactive protein, advanced age and physical inactivity seem to be common risk factors. The role of increased Lp(a) and homocysteine in PAD still remains unclear [58, 59]. The same is true for endogenous sex hormones [60, 61]. As with CHD, prevention is essential. Risk reduction can be achieved through lifestyle modification, particularly physical activity and exercise therapies, smoking cessation, use of statins, antiplatelet therapies, antithrombotic strategies, ACE inhibitors and β-blockers [54, 55, 62].
The beneficial effects of statins in these patients have been shown in large trials [63]. Statins not only lower the risk of PAD and vascular events, but they also improve the symptoms associated with PAD. There is also evidence that statins reduce surgical mortality and improve graft patency and limb salvage in PAD patients [64]. Statin therapy also improves cardiovascular outcomes of patients with PAD [65].
2.5 Stroke
In these guidelines, the emphasis is on ischaemic stroke while intracerebral haemorrhage and subarachnoid haemorrhage (SAH), which contribute 10 and 5% of strokes, respectively, are dealt with more cursorily. However, haemorrhagic strokes are often included in the term ‘stroke’ in epidemiologic studies.
The average age of patients in population-based studies of first stroke is usually 70 to 76 years, which is approximately 10 years older than patients with MI. A few studies have shown a decreasing trend in stroke incidence over the last decade, while others have found stable or increasing trends [66].
Stroke is defined as rapidly developed clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 h with no apparent cause other than a vascular origin. If symptoms last less than 24 h the attack is called a transient ischaemic attack (TIA) [67–69]. Distinction between TIA and ischaemic stroke is arbitrary. In TIAs lasting more than 1 h cerebral infarction may be found in about 20% of cases when examined by MRI. TIAs may precede clinical stroke and require the same prophylactic treatment as ischaemic stroke.
The incidence of stroke increases exponentially with age affecting about 25 per 100 000 in the age group 35-44 years and 1500 per 100 000 in age group 75-84 years per year. It is projected that even with stable age-specific incidence rates, the total number of strokes will increase in the coming decades due to increased life expectancy [66]. Therefore, measures to prevent stroke are needed.
Ischaemic stroke may be due to large vessel disease, small vessel disease, emboli from the heart or from the aortic arch, or other rarer identified causes while a large proportion still remains undetermined [70]. The pathophysiology in large vessel disease of carotid and vertebro-basilar arteries resembles the lesions in the coronary arteries, while that of the other causes of ischaemic stroke differs. Even in the case of large vessel disease the damage is more frequently caused by artery-to-artery embolism than to local vessel occlusion.
In spite of considerable pathophysiologic differences between cerebrovascular disease and ischaemic heart disease, the risk factors are largely the same for the two diseases.
Chapter 3: Prevention strategies and policy issues
The classic WHO report on Prevention of Coronary Heart Disease [71] distinguished three components for prevention: a population strategy, a high-risk strategy and a secondary prevention strategy. The three strategies were defined on the basis of a large number of observational studies and controlled trials about the multifactorial nature, the population distribution of coronary heart disease risk and the feasibility to change risk through individual and community-based interventions. The three strategies are not mutually exclusive, but are necessary and complement each other. The balance between the different strategies will depend on the absolute mean level of risk and its distribution in each specific population and the resources available [72]. However, the population strategy is the essential way to reduce the incidence and the burden of cardiovascular diseases when risk is widely distributed across society as a whole. This type of strategy is mostly achieved by establishing planned policies and community interventions. Without a well resourced national population strategy that tackles the major determinants of cardiovascular diseases, they will remain a major cause of ill health and premature death, regardless of the fact that individual lives might be saved or improved otherwise.
Consequently, the Third Task Force [3] endorsed and collaborated with the initiatives and programs of different major international organizations (i.e. WHO, European Union, International Societies) in taking steps to implement measures at the population level, such as those for tobacco control established by the WHO Framework Convention for Tobacco [73] and others. Positive actions in this field were thereafter adopted by several countries and progress has been made since then, but continuous and new actions are needed in order to maintain and reinforce control. After the publication of the Third Prevention Task Force Guidelines in 2003, further initiatives targeting other cardiovascular health determinants have been launched, like the EU initiative on obesity [74] and the WHO Global Strategy on diet, physical activity and health [75]. The Fourth Task Force aligns and fully endorses these initiatives and encourages health professionals of all countries to participate actively in the design and implementation of such national and international policies and community interventions.
3.1 Prevention in clinical practice
The ‘population strategy’ aims at shifting the distribution of risk factors towards more favourable levels through actions directed towards changing the environment and lifestyle of individuals, without the need to medically examine them, in order to reduce the incidence of disease by preventing or delaying the occurrence of acute cardiovascular events and the progression of chronic disease [76].
The high-risk primary prevention strategy deals with healthy persons with high absolute risks of future disease, and the secondary prevention strategy deals with patients with established cardiovascular organ damage or disease. The strategies aim to diminish the total cardiovascular risk of individuals belonging to the upper part of the risk distribution. The difference between the groups will be reflected in the priorities for intervention and the intensity of treatment. Since risk is a continuum, with many asymptomatic high risk people having investigative evidence of atherosclerosis, the terms ‘primary’ and ‘secondary’ prevention, while convenient, are artificial.
When dealing with prevention strategies based on individual interventions, it is necessary to bear in mind two facts. First, that to prevent one single cardiovascular event, it will be necessary to intervene upon many patients with no apparent benefit to them (prevention paradox). Second, that the number of patients needed to treat to prevent one case will vary in different populations or population subgroups (for example in women) depending on their underlying prevalences and distribution of risk factors and their incidence rate of disease. This problem is partly dealt with by using the estimation of absolute risk to trigger intervention, which helps to avoid over-treatment of low risk young women and under-treatment of high risk middle-aged men.
Coronary heart disease secondary prevention programs have proven to be effective in improving processes of care, readmissions to hospital, functional status and overall mortality, especially if they incorporate exercise programs. However, the effect sizes are quite modest and their cost effectiveness on a large scale remains uncertain [77, 78].
The term ‘screening’ refers to organized public health action targeted to examine the whole of the at risk or vulnerable population to diagnose earlier stages of disease in order to treat them under the assumption that earlier treatment will be more beneficial than treatment at later stages of disease development. It has been known for a long time that mass screening to prevent disease or its consequences has to fulfil certain conditions to be effective [79]. Screening has to be distinguished and not confused with opportunistic or systematic detection at a regular medical encounter. The term screening should not be used superficially. There is no evidence that mass screening for detection of early stages of CHD or stroke is a cost-effective way to prevent disease [80]. A different issue is screening for biological factors or for lifestyles associated with future disease. This type of screening should focus on those at high risk. But to identify those at high risk in the first instance, it is necessary to examine everyone in the population on a periodic basis, something unfeasible for any health system. Moreover, success of this type of action depends, among other things, on accurate and adequate systems of measurement, often lacking in real care settings, time for advice or treatment as appropriate, continuity of care and patients’ access to treatments, regardless of socioeconomic status. As many adults visit their GPs generally once a year, these visits can be used to identify those at high risk-in what is called opportunistic detection or case finding. This activity has implications for the doctor – patient relationship and it may imply ethical problems. In some cases, the patient will ask for risk assessment and counselling. In other cases, the doctor will identify risk factors and propose or offer further investigation and treatment. If the possibility of high cardiovascular risk is obvious, the doctor should offer counselling on lifestyle change and help but at the same time respect the patient's own values and choices. Advice should be offered but not imposed.
3.2 Policy issues
Aspects of health, economics and political action were considered in the Osaka Declaration arising from the Fourth International Heart Health Conference [81]. These may be summarized as:
Increase awareness of governments that the health agenda is not just an agenda of health departments.
Let scientists and health professionals contribute to the marketing of the heart health agenda.
Let schools for health professionals provide training in methods for community organizing, social marketing and advocacy.
Let departments of health, non-governmental organizations (NGOs) and professional organizations develop plans to make the case for heart health resources at the political level.
Let the WHO continue to strengthen the capacity for heart health promotion in all WHO regions and member states.
In recent times, in the spirit of the Osaka Declaration, the ESC has joined with the European Heart Network to engage with the European Union to promote a coordinated European approach to the prevention of cardiovascular diseases. A conference of the relevant bodies was facilitated by the Irish Ministry of Health in February 2004. This informed the conclusions of the EU Council on Employment, Social Policy, Health and Consumer Affairs in June 2004 and an EU Heart Health Conference that resulted in the Luxembourg Declaration of 29 June 2005. This declaration defined the characteristics that are associated with cardiovascular health as:
Avoidance of tobacco;
Adequate physical activity (at least 30 min/day);
Healthy food choices;
Avoiding overweight;
Blood pressure below 140/90;
Blood cholesterol below 5 mmol/l (∼ 190 mg/dl).
Importantly, factors that are essential for implementation were defined, and the need for continued European Commission, Parliament and Council activity to promote a heart healthy Europe was stressed. A European Charter on Heart Health has been prepared. The text of the Luxembourg Declaration is available by searching in http://www.google.com for ‘Luxembourg declaration heart health charter’ [82].
The European Heart Health Charter is now available through the ESC website, escardio.org. It represents the combined efforts of the European Society of Cardiology, European Union and European Heart Network in close collaboration with the World Health Organization Regional Office for Europe. The charter acknowledges that cardiovascular disease is the number one cause of death among men and women in Europe. It affirms the characteristics associated with cardiovascular health defined in the Luxembourg Declaration above. It also categorizes the major risk factors. The signatories to the charter agreed to:
Implement the policies and measures agreed upon in high level European political documents.
Advocate for and support the development and implementation of comprehensive health strategies as well as measures and policies on European, national, regional and local level that promote cardiovascular health and prevent cardiovascular disease.
Build and strengthen dedicated heart health alliances in order to achieve the strongest possible political support for policy developments and co-ordination of actions to reduce the burden from cardiovascular disease.
Further articles deal with education, health promotion, the establishment of national strategies for health promotion, and the promotion and adoption of the European Guidelines on Cardiovascular Disease Prevention. It is further agreed to prioritize research on the effectiveness of policy and prevention interventions, to assess the current status of cardiovascular health including risk factor prevalences to measure progress made at population and individual level to achieve the characteristics associated with cardiovascular health.
Fourteen major European bodies associated with cardiovascular health are signatories to the charter.
Chapter 4: How to evaluate scientific evidence
Evidence-based medicine (EBM) has been defined as the integration of individual clinical expertise with the best available clinical evidence from systematic research. It involves asking answerable questions, searching for the best evidence, critically appraising the evidence, applying the evidence to individual patient care, and evaluating the process [83]. Despite over a decade of educational effort, it is rare for clinicians to practice EBM as intended, with many considering that the major issue is finding the evidence [84].
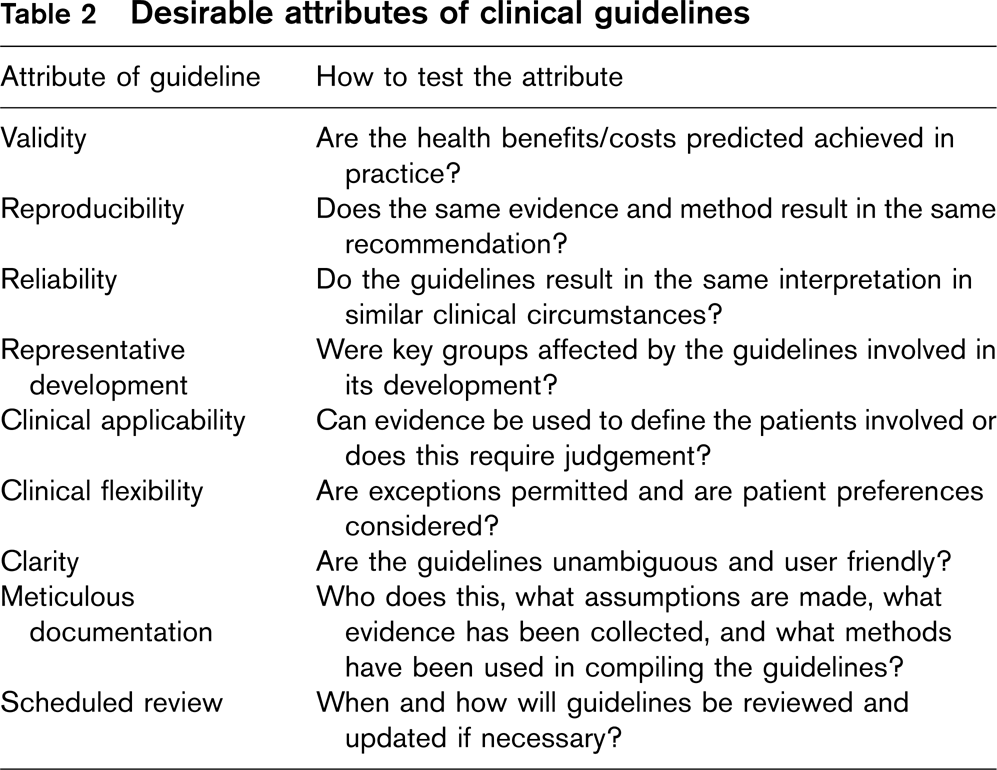
This report aims to provide guidelines under the auspices of the Fourth Joint Task Force of the European Society of Cardiology and other European Societies on Cardiovascular Disease Prevention. The Task Force wishes these guidelines to be as evidence based as possible. Good guidelines are a major mechanism for improving the delivery of healthcare and improving patient outcomes [85]. It has been shown that guidelines based on credible evidence are more likely to be adopted [86]. The desirable attributes of clinical guidelines have been discussed and are shown in Table 2 [87].
4.1 What is ‘evidence'?
The evaluation of interventions and diagnostic methods can make use of a wide range of sources of evidence: experience, retrospective case review, case reports, case series, historic and geographic comparisons, drug (and postmarketing) surveillance studies, pharmacoepidemiologic databases, cross-sectional studies, case-control studies, cohort studies, randomized controlled trials, and systematic reviews of trials and of observational studies. It is clear that different questions require different scientific methods, and that reliance on one source of evidence to the exclusion of others is likely to be misleading. This is particularly true in cardiovascular disease prevention. Lifestyle measures such as smoking cessation, exercise and healthy eating are less amenable to double blind randomized control trials than are drug treatments and too strict an adherence to the primacy of the randomized control trial may result in guidelines that promote excessive usage of drugs.
Desirable attributes of clinical guidelines
Traditionally, hierarchies of evidence have been promoted as a means of prioritizing recommendations, and these generally put systematic reviews at the top of the hierarchy and case reports at the bottom, on the grounds that the potential for bias gets progressively smaller as the hierarchy is ascended. But this approach may be misleading as the quality of the evidence ultimately depends on the question to be answered. Quality implies being fit for purpose – for example, the best evidence to identify rare hazards of treatment is not a systematic review or a randomized controlled trial. Case reports may provide the first hint that a treatment is hazardous but require confirmation in large prospective surveillance studies. Diagnostic tests are seldom evaluated in randomized controlled trials as the question is not usually ‘Does use of the test improve outcomes?', but more commonly, what is the sensitivity and specificity of this test compared with the best method.
The National Institute for Health and Clinical Excellence (NICE) in the United Kingdom and other guideline developing bodies have adopted the ‘hierarchy of evidence approach’ in grading evidence of effectiveness, resulting in grades of recommendation derived from the level of evidence. This approach is difficult to use in practice as it is easy to conflate the study design with the quality of evidence, such that a systematic review may be always viewed as ‘stronger’ evidence than a randomized trial or an observational study. Application of the hierarchy of evidence method requires explicit judgements to be made about the quality of the evidence (e.g. completeness, potential for bias, adequacy of outcomes assessed, etc.). Critically, both the benefits and the hazards of interventions need to be taken into account in producing clinical guidance. This is best done if a ‘balance sheet’ of benefits and harms is prepared that allows expert opinion, policy makers and users of services to make informed judgements in grading the strength of a recommendation.
Linking the strength of evidence underpinning a recommendation (e.g. Grade A – mandatory to implement; Grade B – implement if resources permit; Grade C-limited evidence in support) is difficult to do explicitly as the process of formulating guidance, in distinction from that of preparing synthesis of the evidence, is less well documented and more informal. Importantly, confusion arises when recommendations appear to be made on the basis of the same evidence but come to different conclusions which may reflect that different questions have been posed, additional information such as cost-effectiveness estimates have been included, or that bias has arisen in the process of conducting the review. Methods that might be used to make the process more explicit include consensus approaches or voting, but these are seldom used in practice.
4.2 The problems of evidence and guidance
In using evidence to produce guidance or recommendations for clinical or public health practice, it is important to distinguish between the quality of the evidence (is it robust, little likelihood of bias, generalizable etc.) and the strength of a recommendation underpinned by the evidence. Not all high quality evidence merits a strong recommendation.
In England and Wales, NICE currently uses a modified hierarchy of evidence approach based on the SIGN (Scottish Intercollegiate Guidelines Network) [88] grading system for intervention studies and no longer grades recommendations [89]. This change was spurred by the potential for misinterpretation of letter grades at local levels, leading to unintended problems in implementation of programmes of care. For example, in implementing a guideline, some recommendations that are crucial to the overall improvement of care may be underpinned by little or no strong evidence of benefit, and would consequently be graded as low level in terms of strength of evidence. Managers determined to implement only Grade A recommendations on grounds of resource constraints would find that the intended integrated implementation of a care pathway – for atrial fibrillation, for example – would not work properly.
A major problem in abandoning linking of grades of evidence with recommendations is that transparency is lost and it is not easy to work out what is based solely on expert opinion or lobbying by groups with special interests. Consequently, there is interest in developing a system that retains the desirable ability to maintain transparency but avoids perversity in implementation. NICE now uses a system of key recommendations which are derived from a prioritization process taking into account recommendations that: have high impact on patients’ outcomes, including mortality and morbidity; have a high impact on reducing variation; lead to a more efficient use of NHS resources; and, if implemented would mean patients reach critical points in the care pathway more quickly. To ensure that there is transparency in the link between evidence and recommendations, guidance now contains structured evidence to recommendation statements describing how judgements were made, a process that is believed to be more helpful and transparent than a letter grade.
The World Health Organization, with input from NICE and others, have established a working group attempting to develop such a system, called GRADE [90]. This system does not use letter codes but grades evidence in terms of how trustworthy it is. Briefly, the evidence is classified by the outcomes relevant to the question being answered and the evidence for specific outcomes is appraised in four domains: study design, study quality, consistency and directness. The latter attribute is defined as whether the evidence is directly applicable to the people of interest – in epidemiology this is termed ‘generalizability’ and NICE calls it ‘applicability'. Then on the basis of explicit scoring of these attributes, the evidence quality for the specific outcome is defined as ‘high’ (further research unlikely to change confidence in the estimate of effect), ‘moderate’ (further evidence is likely to have an important impact on confidence in the estimate of effect), ‘low’ (further evidence is very likely to have an important impact on confidence in the estimate of effect) and ‘very low’ (any estimate of effect is very uncertain).
In making recommendations, the GRADE system asks the question does the intervention do more harm than good? Here it is suggested that the answers to this question can be categorized as: net benefits, trade-offs, uncertain trade-offs, and no net benefits. Finally, recommendations should be presented as do it/don't do it or probably do it/probably don't do it [90]. Clearly, GRADE cannot tackle the problems of implementation discussed above. The advantage of the GRADE system is that it makes the judgement of whether the beneficial effects of an intervention outweigh its unwanted effects which is considered to provide an explicit and transparent method of prioritizing interventions for implementation. It is likely that as expertise with GRADE grows and its operational practices mature and stabilize, it will become a more widely used tool for the generation of clinical guidance [91]. Certainly at least one American College is taking it up as the means of producing its recommendations in respiratory diseases [92].
In some circumstances, these implementation problems are not an issue as a guideline development group may not have responsibility for implementation, is not intending to produce comprehensive or integrated guidance on a specific topic, or has a role only in synthesizing evidence upon which other groups will make the recommendations appropriate to local circumstances. The European task force represents a guideline group of this nature. Its role is to synthesize published evidence on each area of management of cardiovascular disease which can then be used by national groups to develop locally appropriate guidance. It is clearly important that both the quality of the evidence and the strength of a recommendation that flows from it are assessed and graded explicitly. This approach ensures that strong recommendations in the face of weak evidence are clear and the judgements made in coming to such conclusions may then be more critically appraised by implementation groups.
We have attempted to ensure that the most appropriate evidence is used to underpin recommendations. For population prevention programmes observational epidemiological findings are an important first step in considering causality. Behaviours such as smoking cessation and exercise are less amenable to randomized control trials than drug treatments. Clearly, systematic reviews (http://www.cochrane.org) of observational studies are preferable to citation of single observational studies. For example, individual studies of the relationship between homocysteine and cardiovascular disease have demonstrated variable associations [93]. Pooling data can provide greater understanding of sources of heterogeneity introduced either by study design (e.g. case-control versus cohort) or by the nature of the participants and will provide a more precise estimate of effect. However, it is important to be aware that this increased precision may be spurious if the control for confounding and other biases is weak in the index studies [94].
A further and growing concern in epidemiology is that with some associations causation has been wrongly attributed. This appears to be the case for antioxidant vitamins where observational studies suggested a reasonable protective effect, but randomized controlled trials have shown that the interventions may even be harmful [95, 96]. Similar concerns have now become apparent with hormone replacement therapy that was thought to confer benefits, but an early systematic review [97] showing adverse cardiovascular effects was ignored until recent randomized controlled trials of hormone replacement therapy confirmed this adverse effect [98].
A further concern for us is the nature of available evidence. Much of the evidence concerns drug treatments rather than lifestyle interventions or health system improvements. Since robust evidence from systematic reviews of randomized controlled trials exists for benefits of statins on cardiovascular disease outcomes [99], the use of such drugs may receive more emphasis than, for example, smoking cessation.
In examining the effects of interventions, we have given prominence to Cochrane systematic reviews where they exist, as these are conducted to a rigorous standard and are updated periodically. We have used other systematic reviews where these exist and have only cited individual trials where they make particular points of interest, or are sufficiently large to provide a clear answer to a clinical question. Where we feel the evidence is scant we have stated this.
When examining effect sizes we have not used numbers needed to treat as these have quite marked problems [100], particularly in preventive cardiology where baseline rates of cardiovascular disease vary markedly throughout Europe. Consequently, a number needed to treat would be needed for countries with low, medium and high risk. Moreover, numbers needed to treat for different age groups and for men and women would be required. Relative risk reductions of treatment are applicable to all European populations, age groups and men and women as, in general, most treatments have the same relative benefits at different levels of risk.
In this report we have attempted to follow an evidence-based approach. We have defined the following questions:
What is the evidence that specific risk factors cause cardiovascular disease?
What is the evidence that these risk factors vary in importance among those with and without established cardiovascular disease?
What is the evidence that interventions for populations lead to reductions in risk factors and cardiovascular disease outcomes?
What is the evidence that interventions for individuals lead to reductions in risk factors and cardiovascular disease outcomes?
We have systematically and critically reviewed the relevant literature to answer each question posed. Efforts have been made to implement the guidelines through the various participating societies. Previous guidelines have been evaluated by means of EUROASPIRE I and II [101]. In the future it is likely that our guidelines will be formulated using the GRADE system [90] or some variant of it.
The issues raised in this chapter raise certain difficulties with regard to the current ESC hierarchical grading system. As noted in this chapter and the preamble, the present system is likely to favour drug treatments over major lifestyle measures because the latter are less amenable to double blind randomized control trials. For this reason, after prolonged debate, the Task Force has not included tables of the grades that it prepared. However, it is anticipated that this issue will require further debate.
Chapter 5: Priorities, total risk estimation and objectives
What are the priorities for CVD prevention in clinical practice?
Patients with established atherosclerotic CVD.
Asymptomatic individuals who are at increased risk of CVD because of:
Multiple risk factors resulting in raised total CVD risk (≥ 5% 10 year risk of CVD death);
Diabetes-type 2 and type 1 with microalbuminuria;
Markedly increased single risk factors especially if associated with end organ damage.
Close relatives of subjects with premature atherosclerotic CVD or of those at particularly high risk.
What are the objectives of CVD prevention?
To assist those at low risk of CVD to maintain this state lifelong, and to help those at increased total CVD risk to reduce it.
To achieve the characteristics of people who tend to stay healthy:
No smoking;
Healthy food choices;
Physical activity: 30 min of moderate activity a day;
BMI >25 kg/m2 and avoidance of central obesity;
BP >140/90 mmHg;
Total chol >5 mmol/l (∼190 mg/dl);
LDL chol >3 mmol/l (∼115 mg/dl);
Blood glucose >6 mmo/l (∼110 mg/dl).
To achieve more rigorous risk factor control in high risk subjects, especially those with established CVD or diabetes:
Blood pressure under 130/80 mmHg if feasible;
Total cholesterol >4.5 mmol/l (∼175 mg/dl) with an option of >4 mmol/l (∼155 mg/dl) if feasible;
LDL-chol >2.5 mmol/l (∼ 100 mg/dl) with an option of >2 mmol/l (∼80 mg/dl) if feasible;
Fasting blood glucose >6 mmol/l (∼110 mg/dl) and HbA1c >6.5% if feasible.
To consider cardioprotective drug therapy in these high risk subjects especially those with established atherosclerotic CVD.
When do I assess cardiovascular risk?
If the patient asks for it.
If, during a consultation:
The person is a middle aged smoker;
There is obesity, especially abdominal;
One or more risk factors such as blood pressure, lipids or glucose is raised;
There is a family history of premature CVD or of other risk factors;
There are symptoms suggestive of CVD. If confirmed, risk factors should be assessed but use of the SCORE chart is not necessary as the person is already at high risk.
Why stress assessment of total CVD risk?
Multiple risk factors usually contribute to the atherosclerosis that causes CVD.
These risk factors interact, sometimes multiplicatively.
Thus the aim should be to reduce total risk; if a target cannot be reached with one risk factor, total risk can still be reduced by trying harder with others.
How do I assess CVD risk quickly and easily?
Those with:
∼ known CVD
∼ type 2 diabetes or type 1 diabetes with microalbuminuria,
∼ very high levels of individual risk factors are already at INCREASED CVD RISK and need management of all risk factors.
For all other people, the SCORE risk charts can be used to estimate total risk-this is critically important because many people have mildly raised levels of several risk factors that, in combination, can result in unexpectedly high levels of total CVD risk.
Assessing cardiovascular risk: what are the components?
History: Previous CVD or related diseases, family history of premature CVD, smoking, exercise and dietary habits, social and educational status.
Examination: BP, heart rate, heart and lung auscultation, foot pulses, height, weight, (Body mass index), waist circumference. Fundoscopy in severe hypertension.
Lab test: Urine for glucose and protein, microalbuminuria in diabetics. Cholesterol and if practicable, fasting lipids (LDL-and HDL-cholesterol, triglycerides) glucose, creatinine.
ECG and exercise ECG if angina suspected.
ECG and consider echocardiogram in hypertensive persons.
Premature or aggressive CVD, especially with a family history of premature CVD: consider high sensitivity CRP, Lipoprotein(a), fibrinogen, homocysteine if feasible, specialist referral.
How do I use the SCORE charts to assess total CVD risk in asymptomatic persons?
Use the low risk chart in Belgium∗, France, Greece∗, Italy, Luxembourg, Spain∗, Switzerland and Portugal; use the high risk chart in other countries of Europe. ∗Updated, recalibrated charts are now available for Belgium, Germany, Greece, The Netherlands, Poland, Spain and Sweden.
Find the cell nearest to the person's age, cholesterol and BP values, bearing in mind that risk will be higher as the person approaches the next age, cholesterol or BP category.
Check the qualifiers.
Establish the absolute 10 year risk for fatal CVD. Note that a low absolute risk in a young person may conceal a high relative risk; this may be explained to the person by using the relative risk chart. As the person ages, a high relative risk will translate into a high absolute risk. More intensive lifestyle advice will be needed in such persons.
Risk estimation using SCORE: Qualifiers
The charts should be used in the light of the clinician's knowledge and judgement, especially with regard to local conditions.
As with all risk estimation systems, risk will be overestimated in countries with a falling CVD mortality rate, and underestimated if it is rising.
At any given age, risk appears lower for women than men. This is misleading since, ultimately, more women than men die from CVD. Inspection of the charts shows that their risk is merely deferred by 10 years.
Risk may be higher than indicated in the chart in:
Sedentary or obese subjects, especially those with central obesity;
Those with a strong family history of premature CVD;
The socially deprived;
Subjects with diabetes – risk may be 5 fold higher in women with diabetes and 3 fold higher in men with diabetes compared to those without diabetes;
Those with low HDL cholesterol or high triglycerides;
Asymptomatic subjects with evidence of preclinical atherosclerosis, for example a reduced ankle-brachial index or on imaging such as carotid ultrasonography or CT scanning.
How do I manage the components of total CVD risk?
The patient and the doctor agree that a risk assessment is indicated, and the patient is informed that the result may lead to suggestions regarding lifestyle change and the possibility of lifelong medication.
There are time and resources to discuss and follow up advice and treatment.
The doctor should be aware of and respect the patients own values and choices.
Total CVD risk management: A key message
Management of the individual components of risk such as smoking, diet, exercise, blood pressure and lipids impacts on total risk.
Thus, if perfect control of a risk factor is difficult (for example, blood pressure control in the elderly), total CVD risk can still be reduced by reducing other risk factors such as smoking or blood cholesterol.
Chapter 5: Priorities, total risk estimation and objectives
5.1 Introduction
At the outset, it is stressed that these guidelines are just that, and not didactic rules. They should be interpreted in the light of the clinician's own knowledge and judgement, the patient's view, and in the light of local conditions and practicalities and as new knowledge becomes available. Indeed the development of national guidelines is strongly encouraged with objectives, priorities and implementation strategies that are adapted to suit local conditions, both medical and economic.
The PRIORITIES suggested are to assist the physician in dealing with individual people and patients. As such, they acknowledge that individuals at the highest levels of risk gain most from risk factor management. As noted elsewhere, although such individuals gain most, most deaths in a community come from those at lower levels of risk, simply because they are more numerous compared to high risk individuals who, paradoxically, develop fewer events in absolute terms – the Rose Paradox [102] (Fig. 1). Thus a strategy for individuals at high risk must be complemented by public health measures to reduce, as far as is practicable, population levels of cardiovascular risk factors and to encourage a healthy lifestyle.
The encouragement of TOTAL RISK ESTIMATION as a crucial tool to guide patient management has been a cornerstone of the Guidelines since the first (1994) edition [1]. This is because clinicians treat whole people (and not individual risk factors), whose cardiovascular risk usually reflects the combined effects of several risk factors that may interact, sometimes multiplicatively.
Although clinicians often ask for thresholds to trigger intervention, this is problematic since risk is a continuum and there is no exact point where, for example, a drug is automatically indicated. This issue is dealt with in more detail, as is the issue of how to advise younger persons at low absolute but high relative risk, and the fact that all elderly people will eventually be at high risk of death and may be over-exposed to drug treatments.
The overall OBJECTIVES of cardiovascular prevention are to reduce mortality and morbidity in those at high absolute risk and to assist those at low absolute risk to maintain this state, through healthy lifestyle. Here, the risk charts are helpful – if blood pressure is hard to fully control, for example, total risk can still be reduced by stopping smoking or perhaps reducing cholesterol levels further. Although thresholds for total cardiovascular risk included in this guideline are arbitrary, targets for individual risk factors are even more problematic in that they will always be open to debate, are not always achievable and, notably, also because they seem to promote a uni-risk factor approach to prevention.
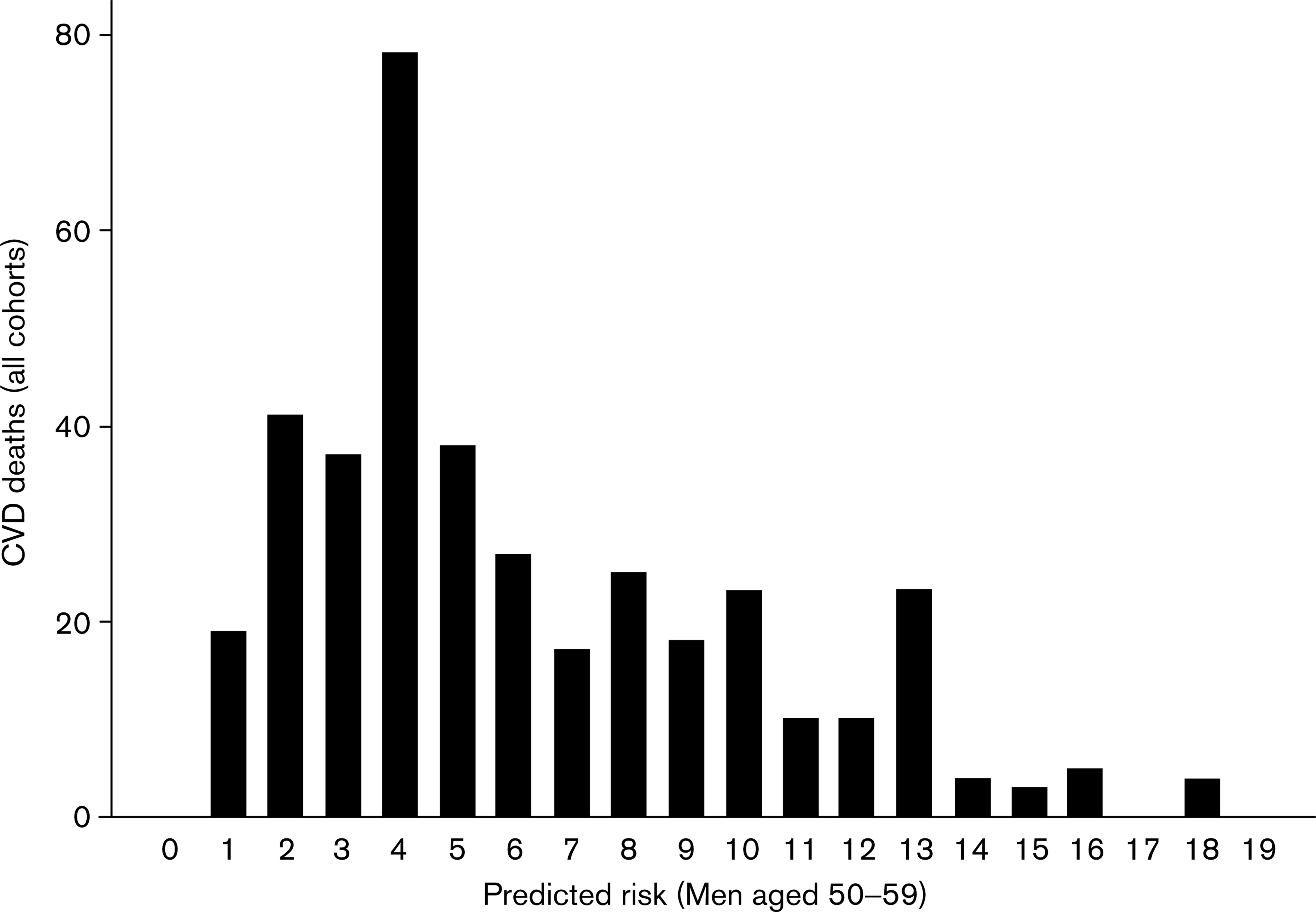
The expected number of CVD deaths at increasing levels of predicted risk (expressed in % over 10 years). Illustration of the fact that most events occur in low risk people simply because they are more numerous compared to high risk individuals who, paradoxically, develop fewer events in absolute terms.
Yet clinicians ask for guidance so an attempt to define desirable levels of individual risk factors has been made in the context of more specific objectives.
5.2 Priorities
Individuals at highest risk gain most from preventive efforts, and this guides the following priorities:
Patients with established atherosclerotic cardiovascular disease (CVD), whether of the coronary, peripheral, cerebral vessels or of the aorta, even if asymptomatic.
Asymptomatic individuals who are at high risk of symptomatic CVD because of:
Multiple risk factors resulting in a markedly raised total CVD risk.
Diabetes type 2 and diabetes type 1 with microalbuminuria.
Markedly raised levels of single risk factors especially if associated with end organ damage.
Close relatives of persons with early onset atherosclerotic CVD (typically before age 60), or at particularly high risk.
In general, a middle-aged person with a 10-year risk of CVD death of 5% or more, is regarded as at high risk. Examination of the FINRISK MONICA data (which contribute substantially to the SCORE high risk population charts) suggests that the equivalent combined fatal + nonfatal CVD risk is about 10% – more in younger men and less in women and the elderly. The Dutch guidelines on CVD risk management present an adaptation of the SCORE risk function which estimates the risk of fatal and nonfatal CVD, based on Markov modelling. This shows that with increasing risk of fatal CVD the relative increase in the risk of fatal and nonfatal CVD is smaller. At 5% risk of fatal CVD the risk of fatal and nonfatal CVD events was 10% in this model [103]. The likelihood of requiring medication in addition increases with increasing risk.
5.3 Total risk estimation
Cardiovascular risk in the context of these guidelines means the likelihood of a person developing an atherosclerotic cardiovascular event over a defined period of time.
'Total risk’ implies an estimate of risk that is made by considering the effect of the major factors age, gender, smoking, blood pressure and lipid levels. While the term has become widely used, it is acknowledged that it is not comprehensive in that the effects of other risk factors are not considered except as qualifying statements.
Impact of combinations of risk factors on risk
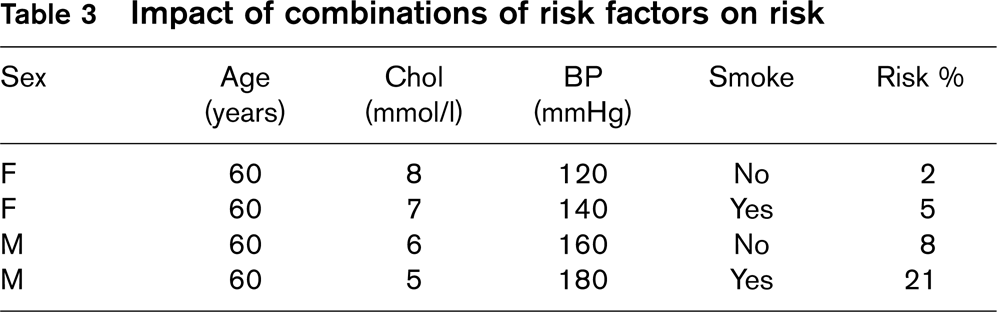
The importance of total risk estimation before management decisions are made is illustrated in Table 3 and Fig. 2. The figure illustrates that the effect of lipid levels on risk is modest in women who are at otherwise low risk, and that the risk advantage of being female is lost by the combination of smoking and mild hypertension. Table 3 shows that a person with a cholesterol of 8 mmol/l can be at 10 times LOWER risk than someone with a cholesterol of 5 mmol/l if the latter is a male hypertensive smoker. Randomized controlled drug trials of single risk factors do not give sufficient data to fully address these issues. While audits such as EuroAspire [101] suggest inadequate risk factor management in very high risk patients, it is also likely that, in the context of low risk patients who have not had a vascular event, there is the potential for substantial overuse of drugs by inappropriate extrapolation of the results of trials conducted mostly on high risk men to low risk individuals. In general, women and old and young patients have been underrepresented in the classic drug trials that have informed guidelines to date.
For these considerations to have an impact on clinical practice, it is essential for the clinician to be able to assess risk rapidly and with sufficient accuracy to allow logical management decisions.
This realization led to the development of the risk chart used in the 1994 and 1998 Guidelines [1, 2]. This chart, developed from a concept pioneered by Anderson [104] used age, sex, smoking status, blood cholesterol and SBP to estimate the 10-year risk of a first fatal or nonfatal coronary heart disease event. There were several problems with this chart. First, it was derived from American data from the Framingham study and the applicability of the chart to all European populations was uncertain. Second, the data set used was fairly small. Third, the definitions of nonfatal CHD events differed from those used in many other studies making it difficult to validate the chart. Finally, estimation of the risk of other manifestations of atherosclerosis such as stroke or aneurysm of the abdominal aorta was not possible.
The 2003 Guidelines [3] used a new system for risk estimation called SCORE (Systematic COronary Risk Estimation) [105], based on data from 12 European cohort studies and includes 205 178 patients examined at baseline between 1970 and 1988 with 2.7 million years of follow-up and 7934 cardiovascular deaths. The SCORE risk function has been externally validated using different datasets [106].
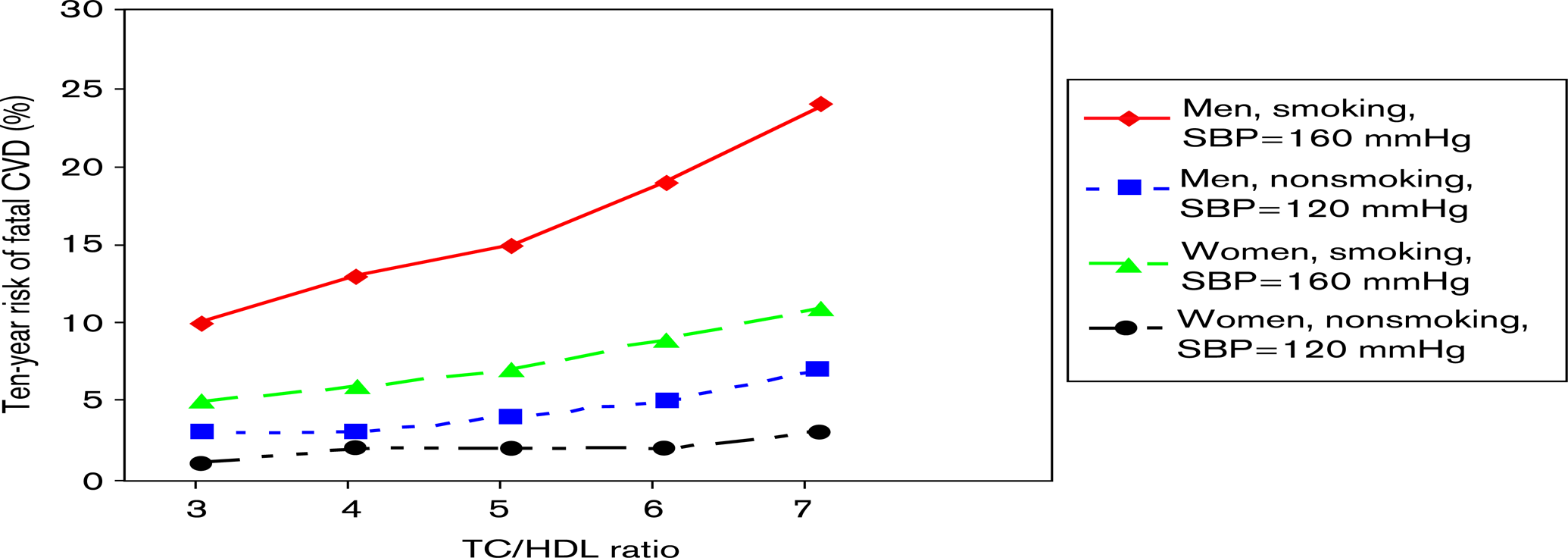
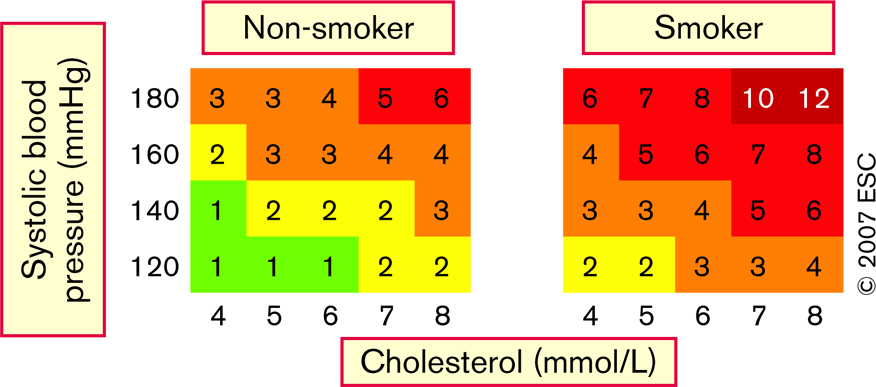
The relationship of total cholesterol/HDL-cholesterol ratio to 10-year fatal CVD events in men and women aged 60 years with and without risk factors, based on a risk function derived from the SCORE project.
Risk charts such as SCORE are intended to facilitate risk estimation in ostensibly healthy persons. Patients who have had a clinical event such as an acute coronary syndrome or stroke have already declared themselves to be at high risk of a further event and automatically qualify for intensive risk factor evaluation and management.
SCORE differs from earlier risk estimation systems in several important ways, and has been modified somewhat for the present guidelines:
The SCORE system estimates the 10-year risk of a first fatal atherosclerotic event, whether heart attack, stroke, aneurysm of the aorta or other. All ICD (International Classification of Diseases) codes that could reasonably be assumed to be atherosclerotic are included. Most other systems estimate coronary heart disease risk only.
The choice of CVD mortality rather than total (fatal + nonfatal) events was deliberate although not universally popular. Nonfatal event rates are critically dependent upon definitions and the methods used in their ascertainment. Striking changes in both diagnostic tests and therapies have occurred since the SCORE cohorts were assembled. Critically, the use of mortality allows recalibration to allow for time-trends in CVD mortality. Any risk estimation system will over-predict in countries in which mortality has fallen and underpredict in those in which it has risen. Recalibration to allow for secular changes can be undertaken if good quality, up-to-date mortality and risk factor prevalence data are available. Data quality do not permit this for nonfatal events. For these reasons, the CVD mortality charts were produced and have, indeed been recalibrated for a number of European countries. Country-specific versions of HeartScore are available for Belgium, Germany, Greece, The Netherlands, Poland, Spain and Sweden. Nevertheless it is essential to address the issue of total risk.
In the 2003 guidelines [3], a 10-year risk of CVD death of 5% or more was arbitrarily considered high risk. Yet this implies a 95% chance of not dying from CVD within 10 years, less than impressive when counselling patients. The new nomenclature in this 2007 guideline is that everyone with a 10-year risk of CV death of 5% or more has an increased risk. Naturally the risk of total fatal and nonfatal events is higher, and clinicians naturally wish for this to be quantified. The biggest contributor to the high risk SCORE charts is FINRISK, which has data on nonfatal events defined according to the MONICA project [107]. Calculating total event rates from FIN-RISK suggests that, at the level (5%) at which risk management advice is likely to be intensified, total event risk is about 10%, more (15%) in younger men and somewhat less in women and in older persons.
As noted in the introduction, clinicians often ask for thresholds to trigger certain interventions, but this is problematic since risk is a continuum and there is no threshold at which, for example, a drug is automatically indicated. A particular problem relates to young people with high levels of risk factors – a low absolute risk may conceal a very high relative risk. In the 2003 Guidelines [3] it was suggested to extrapolate risk to age 60 to stress that a high absolute risk would occur if preventive action were not taken. It was not intended that such a young person should be necessarily treated as if they were 60, but a literal interpretation of this suggestion could lead to excessive drug treatment in younger persons. This part of the text has been rephrased, and a relative risk chart added to the absolute risk charts to illustrate that, particularly in younger persons, lifestyle changes can reduce risk substantially as well as reducing the increase in risk that will occur with ageing.
Another problem relates to old people. In some age categories the vast majority, especially of men, will have estimated CV death risks exceeding the 5 to 10% level, based on age (and gender) only, even when other CV risk factor levels are relatively low. This could lead to excessive usage of drugs in the elderly. This issue is dealt with later in this section.
As before, charts are presented for both total cholesterol and cholesterol: HDL-cholesterol ratio. They look remarkably similar. However, subsequent work on the SCORE data base, as yet unpublished, has shown that HDL-cholesterol can contribute substantially to risk prediction if entered as an independent variable.
Dealing with the impact of additional risk factors such as HDL-cholesterol, body weight, family history and newer risk markers is difficult within the constraint of a paper chart. The electronic, interactive version of SCORE, HeartScore (available through escardio.org)is not so constrained. It presently replicates SCORE in electronic format but will be used to accommodate the results of new SCORE analyses, such as those relating to HDL-cholesterol as these are checked and validated. It should be stressed, however, that although many risk factors other than the few included in the available risk functions have been identified [such as C-reactive protein (CRP) and homocysteine levels] their contribution to absolute CV risk estimations of individual patients (in addition to the older risk factors) is generally modest.
The impact of self-reported diabetes has been reexamined. While there is heterogeneity between cohorts, overall, the impact of diabetes on risk appears greater than in risk estimation systems based on the Framingham cohort, with relative risks of approximately five in women and three in men (unpublished data).
Some of the advantages of using the risk charts may be summarized:
ADVANTAGES IN USING THE RISK CHART
Intuitive, easy to use tool
Takes account of the multifactorial nature of CVD
Allows flexibility in management if an ideal risk factor level cannot be achieved, total risk can still be reduced by reducing other risk factors
Allows a more objective assessment of risk over time
Establishes a common language of risk for clinicians
Shows how risk increases with age
The new relative risk chart helps to illustrate how a young person with a low absolute risk may be at a substantially high and reducible relative risk
The SCORE risk charts are shown in Figs 3–7, including a chart of relative risks. Instructions on their use and qualifiers follow.
This relative risk chart is useful in explaining to a younger person that, even if his/her absolute risk is low, it may still be 10-12 times higher than that of a person of a similar age with low risk factors.
5.3.1 How to use the risk estimation charts
The low risk charts should be recommended for use in Belgium, France, Greece, Italy, Luxembourg, Spain, Switzerland and Portugal and also in countries which have recently experienced a substantial lowering of the CV mortality rates. The high risk charts should be recommended in all other countries of Europe. Note that several countries have undertaken National recalibrations to allow for time trends in mortality and risk factor distributions. Such charts are likely to better represent current risk levels.
To estimate a person's 10-year risk of CVD death, find the table for their gender, smoking status and age. Within the table find the cell nearest to the person's blood pressure and total cholesterol or cholesterol: HDL-cholesterol ratio. Risk estimates will need to be adjusted upwards as the person approaches the next age category.
Low risk persons should be offered advice to maintain their low risk status. While no threshold is universally applicable, the intensity of advice should increase with increasing risk. In general, those with a risk of CVD death of 5% or more qualify for intensive advice, and may benefit from drug treatment. At risk levels over 10% drug treatment is more frequently required. In persons older than 60 these thresholds should be interpreted more leniently, because their age-specific risk is normally around these levels, even when other CV risk factor levels are ‘normal'. In particular, uncritical initiation of drug treatments of all elderly with risks beyond 10% threshold should be discouraged.
Relative risks may be unexpectedly high in young persons, even if absolute risk levels are low.
The charts may be used to give some indication of the effects of reducing risk factors, given that there will be a time lag before risk reduces and that the results of randomized controlled trials in general give better estimates of benefits. Those who stop smoking in general halve their risk.
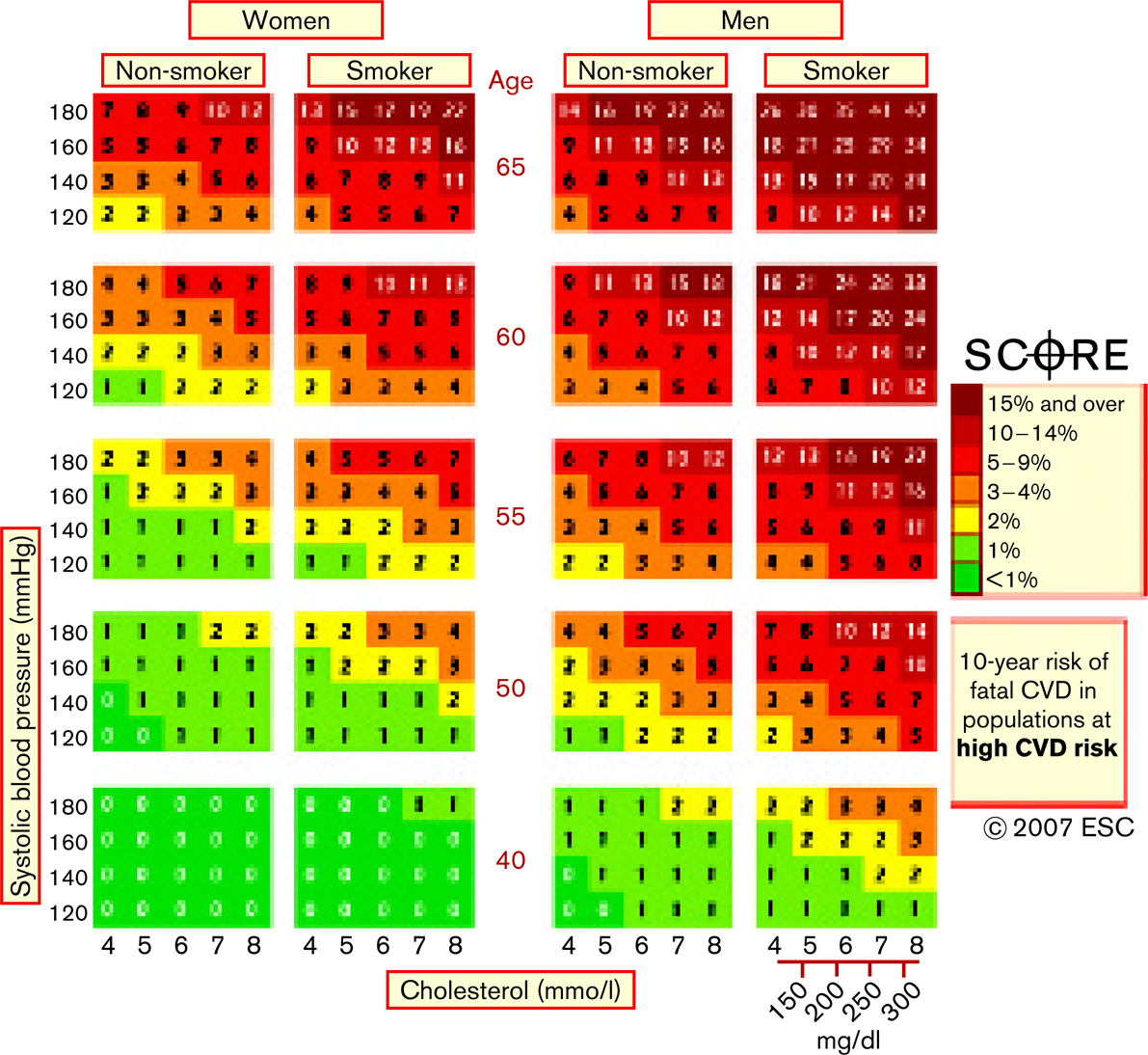
SCORE chart: 10-year risk of fatal CVD in populations at high CVD risk based on the following risk factors: age, gender, smoking, systolic blood pressure, total cholesterol.
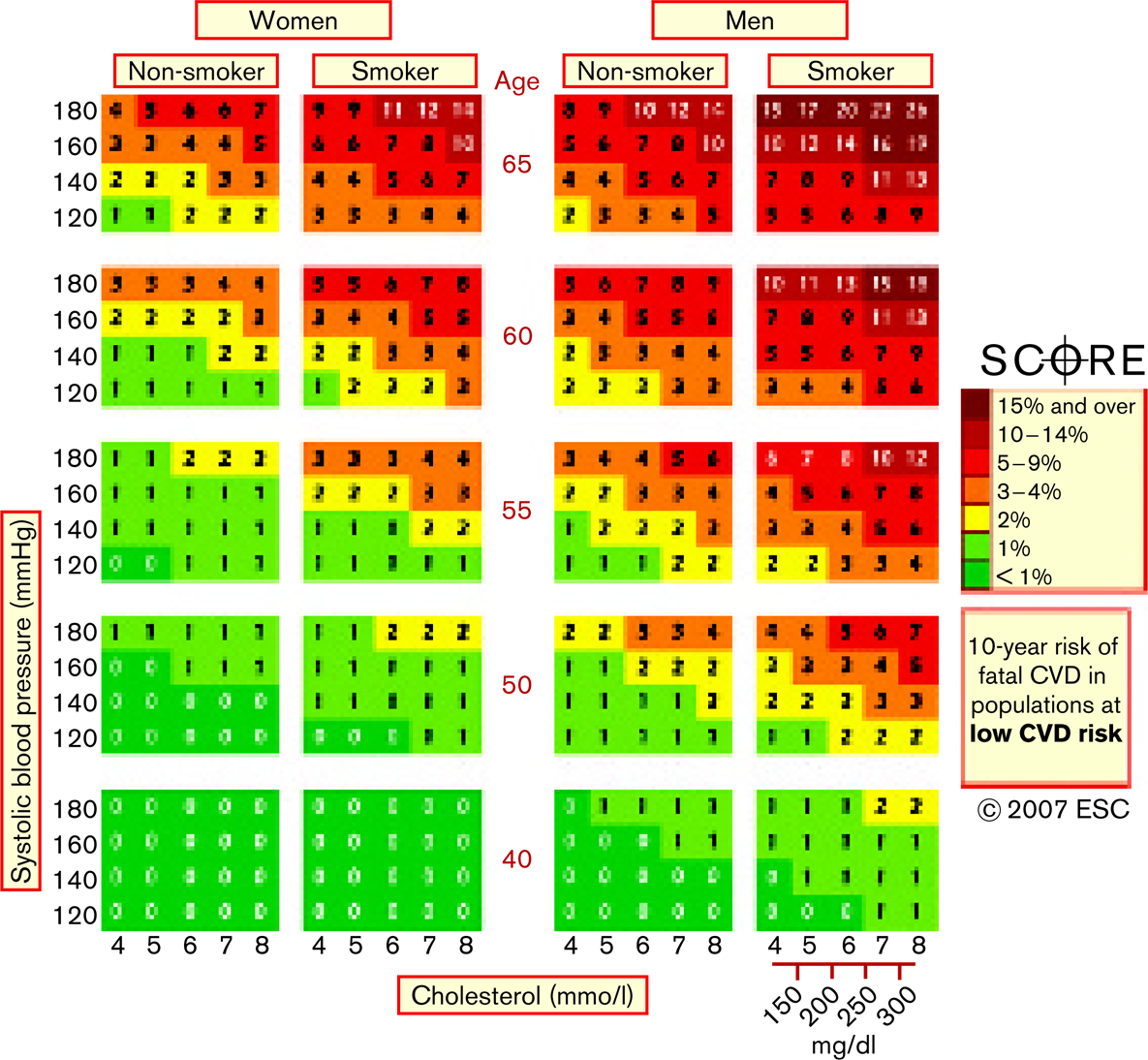
SCORE chart: 10-year risk of fatal CVD in populations at low CVD risk based on the following risk factors: age, gender, smoking, systolic blood pressure, total cholesterol.
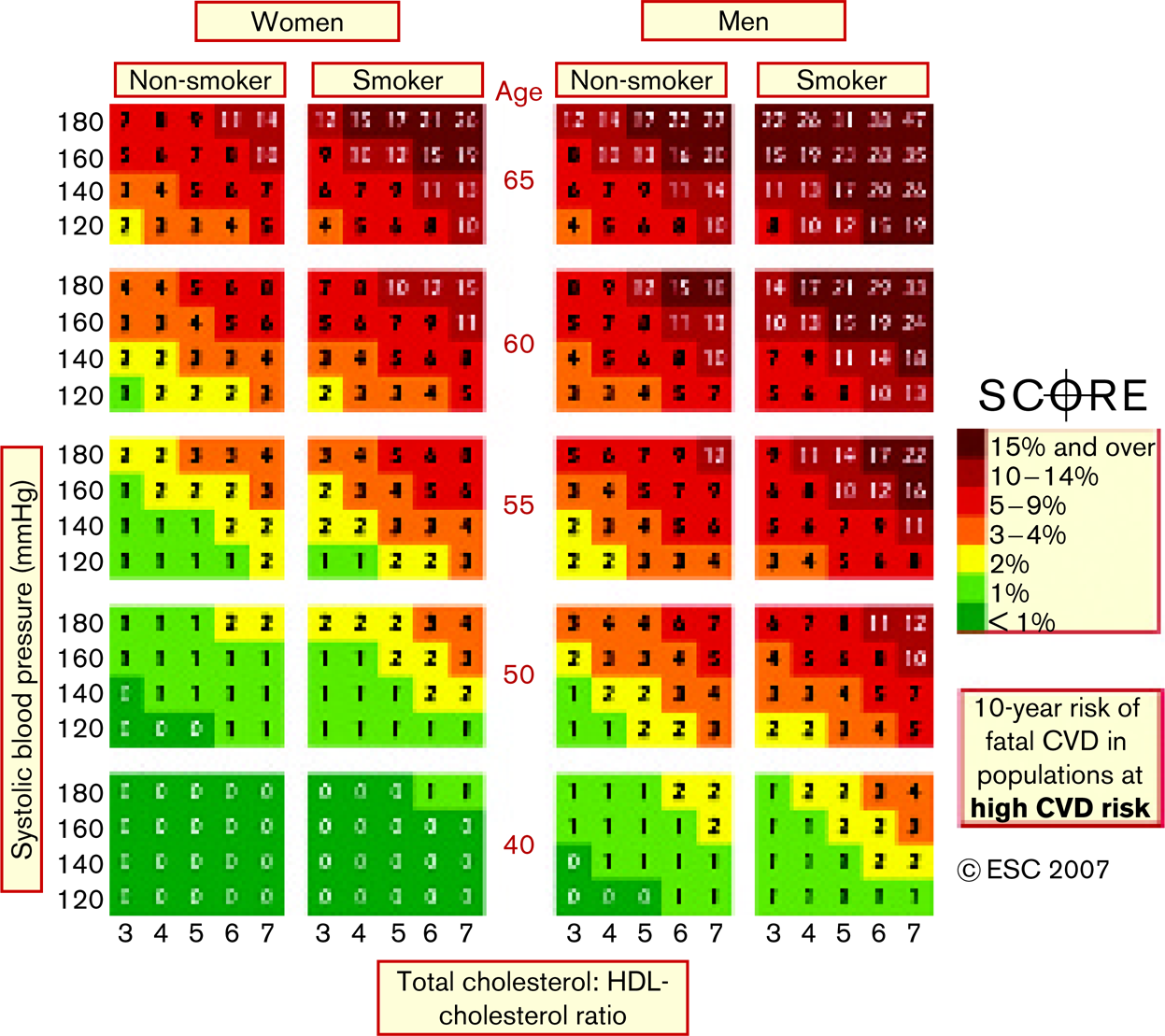
SCORE chart: 10-year risk of fatal CVD in populations at high CVD risk based on the following risk factors: age, gender, smoking, systolic blood pressure, total cholesterol/HDL-cholesterol ratio.
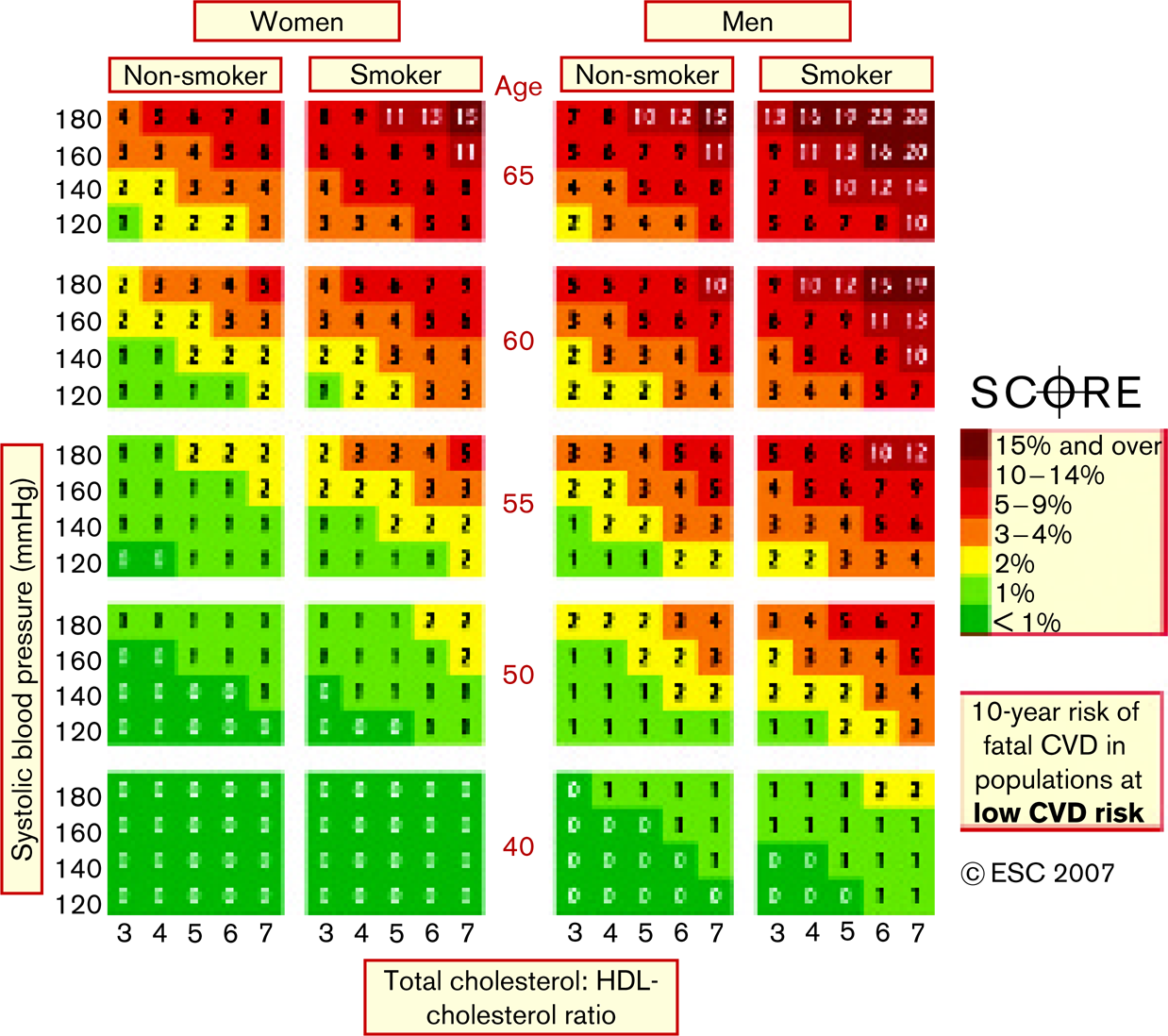
SCORE chart: 10-year risk of fatal CVD in populations at low CVD risk based on the following risk factors: age, gender, smoking, systolic blood pressure, total cholesterol/HDL-cholesterol ratio.
Relative risk chart.
The relative risk chart may be helpful in identifying and counselling such persons.
5.3.2 Qualifiers
The charts can assist in risk assessment and management but must be interpreted in the light of the clinician's knowledge and experience, especially with regard to local conditions.
Risk will be overestimated in countries with a falling CVD mortality, and underestimated in countries in which mortality is increasing.
At any given age, risk estimates are lower for women than men. This may be misleading since, eventually, at least as many women as men die of CVD. Inspection of the charts indicates that risk is merely deferred in women, with a 60-year-old woman resembling a 50-year-old man in terms of risk.
5.3.3 Risk will also be higher than indicated in the charts in
‘Sedentary individuals’ and those with ‘central obesity'; these characteristics determine many of the other aspects of risk listed below.
Socially deprived individuals;
Individuals with a strong family history of premature CVD;
Individuals with diabetes: Reanalysis of the SCORE database indicates that those with known diabetes are at greatly increased risk; five times higher in women and three times higher in men. Risk rises with increasing blood sugar before overt diabetes occurs;
Individuals with low HDL-cholesterol, increased triglycerides, fibrinogen, apoB and lipoprotein(a) levels and perhaps increased high-sensitivity CRP and homocysteine levels;
Asymptomatic individuals with preclinical evidence of atherosclerosis, for example on ultrasonography.
5.4 Objectives of CVD prevention
To assist those at low risk of CVD to maintain this state lifelong, and to help those at higher total CVD risk reducing this to reduce cardiovascular mortality and morbidity.
Desirable characteristics of the components of total risk include:
No smoking;
Healthy food choices;
Physical activity: 30 min of moderate exercise a day;
Body mass index of less than 25 kg/m2 to avoid central obesity;
Blood pressure of less than 140/90 mmHg;
Total cholesterol less than 5 mmol/l (∼ 190 mg/dl);
LDL-cholesterol less than 3 mmol/l (∼ 115 mg/dl);
Good glycaemic control in diabetic individuals.
Rigorous blood pressure and lipid control is desirable in the highest risk patients, particularly those with ‘established atherosclerotic CVD’ and ‘diabetes':
Blood pressure less than 130/80 mmHg;
Total cholesterol less than 4.5 mmol/l (∼ 175 mg/dl), with an option of less than 4 mmol/l (∼ 155 mg/dl) if feasible;
LDL-cholesterol less than 2.5 mmol/l (∼ 100 mg/dl), with an option less than 2.0 mmol/l (∼ 80 mg/dl) if feasible;
Fasting blood glucose less than 6 mmol/l (∼110 mg/dl) and HbA1c less than 6.5% if feasible.
Consideration of prophylactic drug therapy in particular groups, especially those with established atherosclerotic CVD.
5.5 Conclusions
The PRIORITIES defined in this section are for clinical use and reflect the fact that those at highest risk of a CVD event gain most from preventive measures. This approach should complement public actions to reduce community risk factor levels and promote a healthy lifestyle.
Estimation of TOTAL RISK remains a crucial part of the present guidelines. The SCORE system has been updated with an estimate of total CVD risk as well as risk of CVD death. New information on diabetes is included. Information on relative as well as absolute risk is added to facilitate the counselling of younger persons whose low absolute risk may conceal a substantial and modifiable age-related risk.
The difficulty in imposing arbitrary thresholds or targets upon a continuous variable such as risk is acknowledged. Nevertheless, specific OBJECTIVES are defined in terms of desirable levels of individual risk factors. This must be seen as an aid to clinicians in planning risk management strategies with their patients. The primacy of managing total risk rather than focusing on individual risk factors is stressed.
Priorities, risk estimation and the definition of objectives reflect an attempt to make complex issues simple and accessible. Their very simplicity makes them vulnerable to criticism. Above all they must be interpreted in the light of the physician's detailed knowledge of their patient and in the light of local guidance and conditions.
A summary of the recommendations is given in the flow chart below:
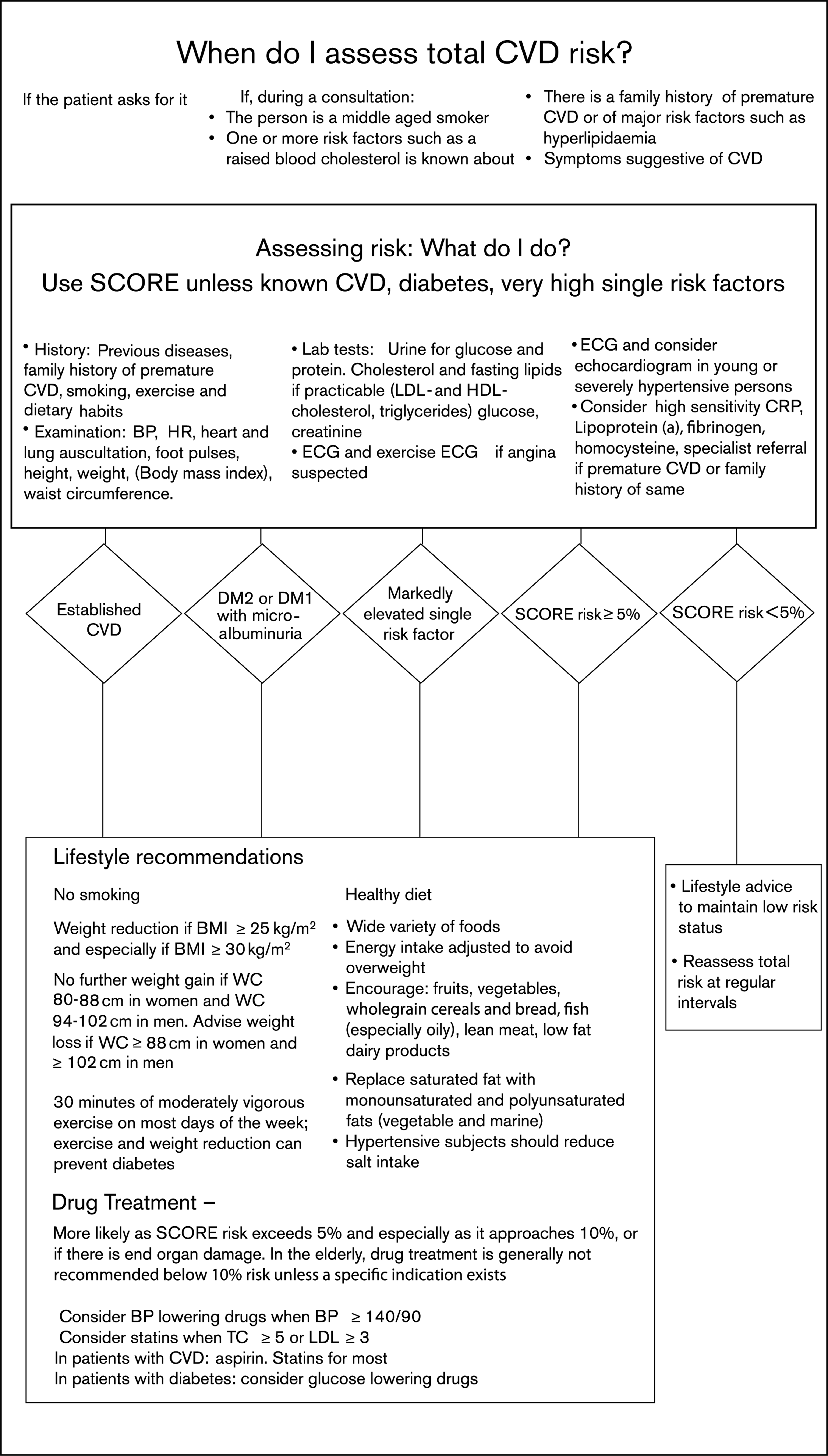
When do I assess total CVD risk?
Chapter 6: Principles of behaviour change and management of behavioural risk factors
Managing total CVD risk-TIPS TO HELP BEHAVIOUR CHANGE
Develop a sympathetic alliance with the patient.
Ensure the patient understands the relationship between lifestyle and disease.
Use this to gain commitment to lifestyle change.
Involve the patient in identifying the risk factors to change.
Explore potential barriers to change.
Help design a lifestyle change plan.
Be realistic and encouraging – ‘ANY increase in exercise is good and can be built on'.
Reinforce the patient's efforts to change.
Monitor progress through follow-up contacts.
Involve other healthcare staff wherever possible.
Managing total CVD risk-WHY DO PEOPLE FIND IT HARD TO CHANGE THEIR LIFESTYLE?
Socio-economic status: Low SES, including low educational level and low income, impedes the ability to adopt lifestyle change.
Social isolation: People living alone are more likely to have unhealthy lifestyles.
Stress: Stress at work and at home makes it more difficult for people to adopt and sustain a healthy lifestyle.
Negative emotions: Depression, anxiety and hostility impede lifestyle change.
Complex or confusing advice.
Increased physician awareness of these factors facilitates empathy, counselling and the provision of sympathetic, simple and explicit advice.
Chapter 6: Principles of behaviour change and management of behavioural risk factors
In developing a strategy for behaviour change, health planners have long debated the effects of societal change compared with changes in the individual's behaviour. Legislative control of tobacco, availability of foodstuffs and facilities for exercise, for example may have, overall, greater effects than individual counselling. Nevertheless, physicians need to be aware of communication and behaviour change techniques that will help them in the individual patient consultation.
6.1 Strategies for promoting behavioural change
Physicians and other health professionals in the primary and out-patient care setting are in a unique position to contribute significantly to the improved prevention and management of CVD. Physicians are generally perceived by the general public as the most reliable and credible source of information on health and advice. Patients usually want to receive as much information as possible from physicians, and often prefer to receive assistance from them in order to change behaviours such as smoking, nutrition and diet, and physical activity, rather than to attend special programmes elsewhere [108].
6.2 The physician/caregiver-patient interaction as a means towards behavioural change
A friendly and positive physician-patient interaction is a powerful tool to enhance patients’ coping with stress and illness and adherence to recommended lifestyle change and medication. Social support is known to exert positive influences on illness behaviour, on coping and on adherence; conversely, a nonsupportive environment can lead to a cycle of misunderstandings and destructive emotions (e.g. rage and anger), which in turn result in attention shifts, motivational problems and ignorance of the threats of chronic illness and the need to change lifestyle.
Social support provided by caregivers, including physicians, may be of primary importance to help patients maintain healthy habits and follow medical advice. Decision-making should be shared between physician/ caregiver and patient (also including the patient's spouse and family) to the largest extent possible, thus assuring patients’ and families’ active involvement in lifestyle change and medication adherence.
The physician's use of some principles of effective communication will facilitate successful treatment and prevention of CVD.
6.2.1 Recommendations for good and effective physician/caregiver-patient interactions
Spend enough time with the patient, even 2 min more can make a difference;
Listen carefully to the patient and recognize strengths and weaknesses in the patient's attitude to illness and lifestyle change;
Accept the patient's personal view of his/her disease and allow expression of worries and anxieties;
Speak to the patient in his/her own language and be supportive of every improvement in lifestyle;
Make sure that the patient has understood your advice and has the means to follow it;
Acknowledge that changing life-long habits can be difficult and that gradual change that is sustained is often more permanent;
Be prepared that your patient may need your support for a long time and that repeated efforts to encourage and maintain lifestyle change may become necessary in many patients.
In counselling their patients, physicians can build on recommendations to assess the individual's thoughts, attitudes and beliefs concerning the perceived ability to change behaviour, as well as the environmental context in which attempts to change are made, and subsequently to maintain the lifestyle change. One useful model underlying these recommendations is the ‘stages of change model’ [109, 110]. Behavioural interventions based on social cognitive theory seem to increase self-efficacy and thereby improve long-term adherence with behavioural recommendations. Previous negative, unsuccessful attempts to change behaviour, however, often result in a lower self-efficacy for future change in that behaviour, and often lead to another failure. A crucial step in changing negative experiences to positive is to set realistic goals, and goal-setting combined with self-monitoring of the chosen behaviour are the main tools to achieve a positive outcome. This in turn will increase self-efficacy for the chosen behaviour, and thereafter new goals could be set. Moving forward in small consecutive steps is one of the key points in long-term behaviour change. Ten strategies to enhance the effectiveness of counselling on behavioural change are summarized below.
6.2.2 Ten strategic recommendations to enhance the effectiveness of behavioural counselling [110]
Develop a therapeutic alliance;
Counsel all patients;
Ensure that patients understand the relationship between behaviour and health;
Help patients to assess the barriers to behaviour change;
Gain commitments from patients to behaviour change;
Involve patients in identifying and selecting the risk factors to change;
Use a combination of strategies including reinforcement of patient's own capacity for change;
Design a lifestyle modification plan;
Monitor progress through follow-up contact;
Involve other healthcare staff wherever possible.
6.3 Interventions to improve adherence
Preventive interventions can only exert their effects if patients actually adhere to them. Recent meta-analytic data show that adherence with beneficial medications is associated with improved survival. However, adherence with placebo also improves survival [111] indicating that it may reflect generally better health behaviour. Measures should therefore be taken to improve adherence and health behaviour in general. Motivational interviewing and counselling based on the individual situation of the patient and his or her readiness to adopt behaviour changes increases the likelihood of these changes taking place and shared decision making can facilitate the maintenance of measures agreed upon.
6.4 Evidence for psychosocial risk factor modification programs
A number of psychosocial intervention strategies have been demonstrated to have positive effects on risk factors (see specific chapters on nutrition, smoking, physical activity and psychosocial factors) – but the specific content and approaches taken by these interventions vary. Even if they intend to target only one behavioural risk factor, such as low social support, group-based behavioural interventions often contain elements, which affect multiple risk factors [112, 113]. For example, cardiovascular patients in a smoking cessation program may also benefit from social support or behavioural advice from their peers. Interventions adding psychosocial and psycho-educational components to standard cardiologic care can significantly improve quality of life and diminish cardiovascular risk factors. Nevertheless, data are inconclusive for effects of psychosocial interventions on disease progression and survival [114]. Such programs that achieve their proximal goals, that is reduction of behaviour-dependent risk factors, also seem to have the potential to prevent the progression of clinical CHD. There is some evidence that intervention programs should be individualized based on individual risk constellations and include gender-specific aspects [115].
6.5 Multimodal interventions
The physician/caregiver should recognize the social, emotional and cognitive problems associated with illness and lifestyle change and help to develop strategies to solve them. Continuing education curricula to increase physicians’ behavioural and psychosocial skills have been developed in some countries [116–119] and may help to increase the effectiveness of counselling and behavioural advice. It should, however, be recognized that the physician is not the only professional person involved. The expertise of psychiatry, psychology, psychosomatic medicine, nutrition and behavioural sciences in a broader sense is also needed. In particular, therapeutic and preventive interdisciplinary team work should be attempted, combining the appropriate knowledge and skills to optimize the preventive efforts.
Multimodal, behavioural interventions are especially recommended for patients with clinically manifest CVD and for individuals at very high risk. These interventions should integrate education on healthy lifestyle and medical resources, exercise training, relaxation training, and smoking cessation programmes for resistant smokers. Whenever needed, additional individual or group counselling should be performed. Such counselling can enhance coping with illness, improve adherence with prescribed medication and efforts to change behaviour, and facilitate adequate utilization of medical resources, in particular to minimize delay in seeking help in case of central chest pain or other serious symptoms. Psychosocial risk factors (stress, social isolation and negative emotions) that may act as barriers against behaviour change will also be addressed in individual or group counselling sessions, according to specific needs of the participants.
Multimodal interventions need special education of the staff. There is evidence that more extensive/longer interventions may lead to better long-term results with respect to behaviour change and somatic outcome [120]. Patients of low socio-economic status, of older age, or female gender may need tailored programmes, in order to meet their specific needs regarding information and emotional support.
6.5.1 Recommendations to add psychosocial interventions
In patients with manifest CVD or very high risk, add psychosocial and/or psychoeducational components to standard cardiological care in order to improve risk factor control and quality of life;
Individualize intervention programs to patients’ individual risk profiles, age, socioeconomic status, and gender.
Chapter 7: Smoking
Managing total CVD risk-SMOKING
All smokers should be professionally encouraged to permanently stop smoking all forms of tobacco. The five A's can help-
A-ASK: Systematically identify all smokers at every opportunity
A-ASSESS: Determine the person's degree of addiction and his/her readiness to cease smoking
A-ADVISE: Unequivocally urge all smokers to quit
A-ASSIST: Agree on a smoking cessation strategy including behavioural counselling, nicotine replacement therapy and/or pharmacological intervention
A-ARRANGE a schedule of follow-up visits
7.1 Smoking as a risk factor
There is overwhelming evidence for an adverse effect of smoking on health [121]. In long-term smokers, smoking is responsible for 50% of all avoidable deaths and one half of these are due to cardiovascular disease [122, 123]. Tobacco smoking causes heart attacks at any age, not only in the elderly; in the MONICA project more than half of all nonfatal myocardial infarctions in young people aged 35-39 years could be attributed to smoking [124]. This adverse effect of smoking is related to the amount of tobacco smoked daily and to the duration of smoking [125, 126]. The risk of future cardiovascular disease is particularly high if smoking starts before the age of 15 years [127]. Initially, smoking of tobacco was mainly taken up by men but within the past decades male and female smoking habits have become more similar in Europe. In recent prospective studies the mortality from vascular disease has been found to be proportionately higher in female smokers than in male smokers [128, 129]; this difference remains significant after adjustment for major CV risk factors. A higher risk of lung cancer in smoking women as compared to men has also been described in several studies. This could be related to differences in nicotine metabolism and smoking-related behaviours. Women metabolize nicotine faster than men, especially women taking oral contraceptives [130]. Women under oral contraceptive treatment should specifically avoid smoking as cigarettes have a synergistic effect on the risk of both ischaemic heart disease and cerebral thromboembolism [131].
There have also been some questions on the relative strength of the association between smoking and CVD within ethnic subgroups; there have been some suggestions that Asians may have less excess risk from smoking than Caucasians. However, recent findings have shown that Asians and the Caucasian Australians and New Zealanders have similar increased proportionial CV risk from smoking cigarettes and similar relative risk reduction from quitting [128].
The impact of smoking on atherosclerosis progression is also greater for patients with diabetes and hypertension [132]. Smoking is more common among those who have received little education and widening education-related inequalities in smoking cessation rates have been observed in many European countries in recent years [133].
Within Europe, the impact of smoking on the absolute risk of coronary heart disease has been found to be smaller in Mediterranean populations than in Northern European populations [134]. Dietary factors probably explain this difference in the effect of smoking.
Passive smoking has now been shown to increase the risk of coronary heart disease and other smoking-related diseases [132, 135–137] and the effects of second-hand smoke on the cardiovascular system may even be greater than what was expected [138]; some of these effects appear rapidly and can precipitate acute manifestations of CVD in patients [139]. While cigarette smoking is certainly the most deleterious of the tobacco habits, other uses of tobacco, such as different forms of smokeless tobacco, are also related to health problems [140].
Although the exact mechanisms by which tobacco smoking increases the risk of atherosclerotic disease are not yet fully understood, smoking enhances both the development of atherosclerosis, the occurrence of superimposed thrombotic phenomena and leukocyte activation [141, 142]. Some of these effects may be even more important, because stopping smoking leads to a quicker reduction in the risk of subsequent coronary heart disease events in patients with established coronary heart disease than in asymptomatic individuals; in patients with established coronary heart disease the risk falls within 2-3 years to the level of those coronary heart disease patients who never smoked [126], whereas in asymptomatic individuals up to 10 years are needed to reach the risk level of those who never smoked [127, 143].
In a meta-analysis of cohort studies on the effect of smoking cessation on mortality after a myocardial infarction, all studies showed a mortality benefit of 0.54 with a combined odds ratio in those who quit (95%CI 0.46-0.62). The mortality benefit was consistent regardless of sex, duration of follow-up, study site and time period [144]. Therefore stopping smoking after a myocardial infarction is potentially the most effective of all preventive measures. Sufficient efforts should be devoted to this end.
7.1.1 Smoking and risk of CVD
Smoking of tobacco is a strong and independent risk factor for CVD in asymptomatic patients and in patients with CVD;
Passive smoking is also associated with an increase in CVD risk;
The effects of smoking on CVD interact synergistically in the presence of other CVD risk factors.
7.2 Smoking assessment
The assessment of the smoking status of people should be done at every opportunity. Smoking history should include the following questions: Is the person a current smoker? If yes, number of cigarettes or grams of tobacco (cigars, pipes) smoked daily; life-time duration of smoking; earlier attempts to stop. If the person has stopped smoking, for how many years or months has he/she stopped?
In addition, in some individuals it may be of interest to know their degree of addiction and their state of mind with regard to change. The Fagerström test for nicotine dependence can be used for the latter [145].
7.3 Prevention and management of smoking
Stopping smoking should be encouraged in all smokers. There is no age limit to profit from the benefits of smoking cessation. Some of the advantages are almost immediate, others take more time. Figure 8 outlines the World Health Organization's recommended approach to the individual patient.
The benefits of smoking cessation have been extensively reported [121, 146]. Tobacco cessation strategies should involve behavioural, pharmacological and community-oriented interventions.
At the level of the individual patient a combined behavioural and pharmacological intervention may be the most appropriate, yet the public health impact may be greater by community-oriented interventions.
Quitting smoking is a complex and difficult process, because this habit is strongly addictive both pharmacologically and psychologically. Despite this, many people who succeed in quitting manage to do this without any special programme or treatment. The chances for becoming an ex-smoker at 6 or 12 months are, however, slim, somewhere around 1-3%. These results can be improved by professional assistance.
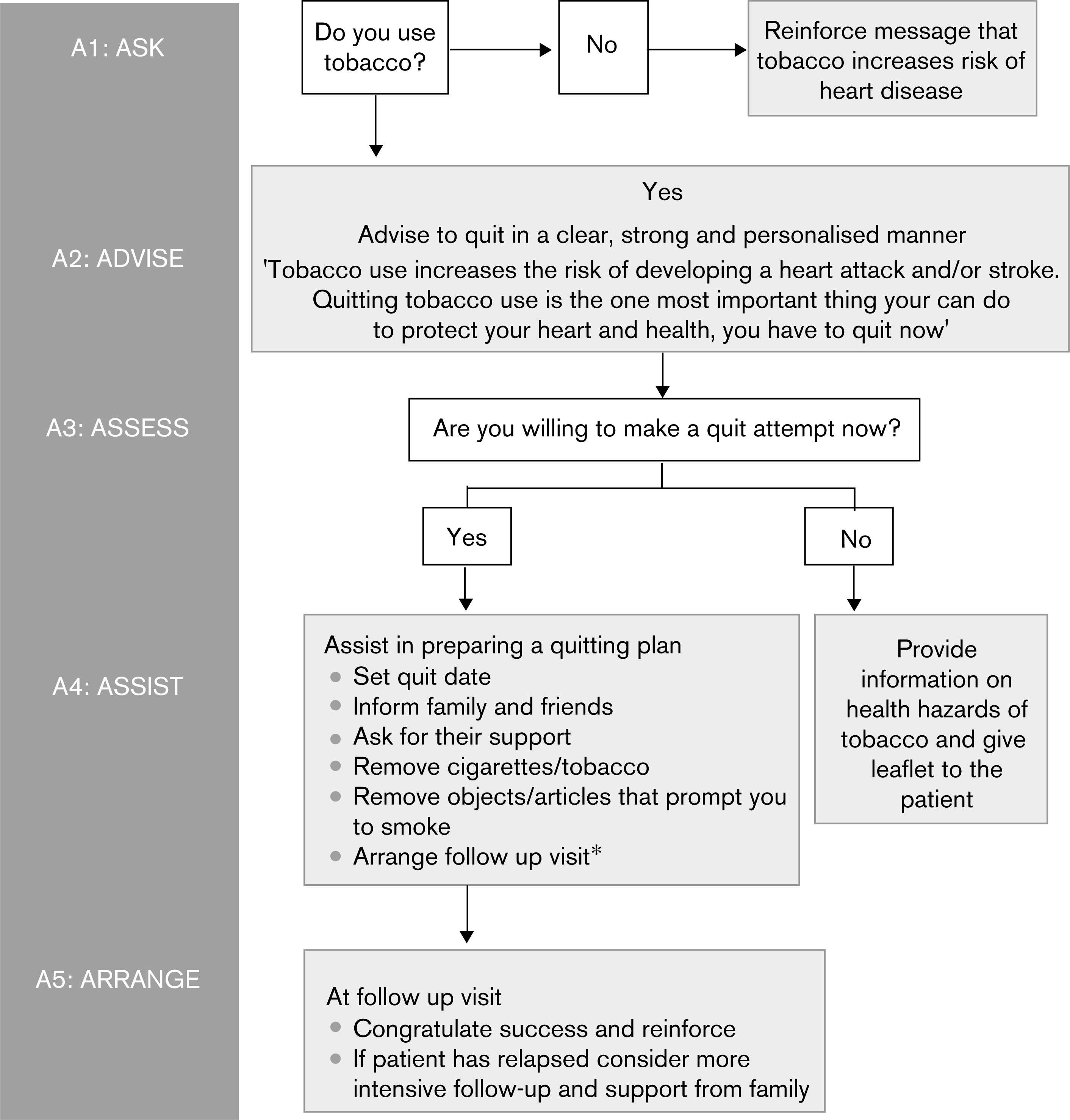
WHO Smoking Cessation Algorithm.
The physician's firm, explicit but sympathetic advice that a patient with coronary heart disease or other atherosclerotic disease should stop smoking is the most important factor in getting the smoking cessation process started. The momentum for smoking cessation is particularly strong at the time of diagnosing athero-thrombotic cardiovascular disease and in connection with an invasive treatment, such as coronary artery bypass grafting, percutaneous transluminal coronary angioplasty or vascular surgery. The physician's advice is equally important in helping healthy high-risk individuals to attempt quitting smoking. The physician's explicit advice to quit smoking completely and ascertainment that the person is willing to try to do it, or at least to start the process of contemplating such an action, are the decisive first steps. Brief reiteration of the cardiovascular and other health hazards of smoking, providing appropriate literature, and agreeing on a specific plan with a follow-up arrangement are the essential features of the brief advice version of smoking cessation in clinical practice. This may involve the assessment of the degree of addiction and their stage of change. Pooled data from 17 trials of brief advice versus no advice (or usual care) revealed a small but significant increase in the odds of quitting (odds ratio 1.74, 95% CI 1.48-2.05). This equates to an absolute difference in the cessation rate of about 2.5% [147]. Both individual and group behavioural interventions are effective in helping smokers to quit as well [148–150]. A recent randomized trial in patients with acute cardiovascular disease found that a minimum of 12 weeks of behaviour modification counselling and individualized pharmacotherapy were superior to simple counselling plus printed educational materials not only in terms of 2-year smoking cessation; patients in the intervention group also had lower rates of rehospitalization and mortality than patients receiving simple advice [151].
Readers are referred to specific recommendations describing the principles of brief advice and other interventions for smoking cessation in clinical practice [145, 152]. At hospital-based clinics and primary healthcare practices nurses are an important resource in individual counselling on smoking cessation. Physicians and nurses need to set an example for their patients by not smoking themselves. Primary pipe or cigar smokers may be at somewhat lower cardiovascular risk than cigarette smokers, mainly because many of them tend to be noninhalers. It is advisable to try to get patients with atherosclerotic disease and high-risk individuals to also stop these forms of smoking. If cigarette smokers shift to pipe or cigar smoking, they usually continue to inhale and therefore this shift should be discouraged.
Nicotine chewing gum and the transdermal nicotine patch have been widely used in helping quitters to go through the difficult initial weeks or months of smoking cessation. A Cochrane review on the effectiveness of different forms of nicotine replacement therapy (NRT) revealed that the quit rates increase approximately 1.5 to 2-fold with the use of nicotine replacement [153]. Initial success is often followed by a relapse, but cessation rates of 10% or more for 1 year or longer have been achieved following nicotine replacement therapy. The use of nicotine patches has been successfully tested in patients who have coronary heart disease without any adverse effects [145].
The effectiveness of antidepressant medication in aiding long-term smoking cessation has been reviewed [154]. From this it seems that bupropion and nortriptyline can aid smoking cessation. In one trial the combination of bupropion and nicotine patch produced slightly higher quit rates than the patch alone.
Another new pharmacological agent that may be of help in smoking cessation is varenicline, a nicotine acetylcholine receptor agonist. Among long-term smokers treatment with varenicline was associated with a smoking cessation rate of 23% at one year as compared to 15 and 10.3% in the groups treated with bupoprion and placebo respectively [155, 156]. Reports that it may be more effective than buproprion or placebo need confirmation.
Support by the spouse and family is very important in smoking cessation. Involvement of the family in the smoking cessation process and getting other smoking family members to quit smoking together with the patient is of great help. There is no consistent evidence that acupuncture, acupressure, laser therapy or electrostimulation are effective for smoking cessation [157].
In many European countries a favourable development has occurred with the creation of ‘smoke-free’ environments, including restrictions of smoking at work sites, in public transport vehicles, restaurants, etc. These changes provide an improved atmosphere for smoking cessation attempts by individuals. The steps for effecting smoking cessation recommended by the WHO are detailed in Fig. 8 [158].
Chapter 8: Nutrition, overweight and obesity
Managing total CVD risk-HEALTHY FOOD CHOICES
All individuals should be advised about food choices that are associated with a lower CVD risk. High risk persons should receive specialist dietary advice if feasible.
General recommendations should suit the local culture:
A wide variety of foods should be eaten.
Energy intake should be adjusted to avoid overweight.
Encourage: Fruits, vegetables, wholegrain cereals and bread, fish (especially oily), lean meat, low fat dairy products.
Replace saturated fats with the above foods and with monounsaturated and polyunsaturated fats from vegetable and marine sources to reduce total fat to >30% of energy, of which less than 1/3 is saturated.
Reduce salt intake if blood pressure is raised by avoiding table salt and salt in cooking, and by choosing fresh or frozen unsalted foods. Many processed and prepared foods, including bread, are high in salt.
Managing total CVD risk-BODY WEIGHT
Increasing body weight is associated with increased total and CVD mortality and morbidity, mediated in part through increases in blood pressure and blood cholesterol, reduced HDL-cholesterol and an increased likelihood of diabetes.
Weight reduction is recommended in obese people (BMI ≥ 30 kg/m2) and should be considered for those who are overweight (BMI ≥ 25 and >30 kg/m2)
Men with a waist circumference of 94-102 cm and women with a waist circumference of 80-88 cm are advised not to increase their weight. Men above 102 cm and women above 88 cm are advised to lose weight.
Restriction of total calorie intake and regular physical exercise are the cornerstones of weight control. It is likely that improvements in central fat metabolism occur with exercise even before weight reduction occurs.
Chapter 8: Nutrition, overweight and obesity
8.1 Scientific background
The role of nutrition in the aetiology and prevention of atherosclerosis and cardiovascular disease has been extensively reviewed [159]. Worldwide, there are strong, consistent and graded relationships between saturated fat intake, blood cholesterol levels and the mass occurrence of cardiovascular disease. The relationships are accepted as causal.
8.1.1 Total fat
The fat content of the diet affects other cardiovascular risk factors. In nutritional studies, a lowering in the intake of fats is usually associated with a relative or absolute increase in the intake of carbohydrates. In such circumstances, a decrease in LDL-and HDL-cholesterol levels and an increase in triglyceride concentrations is observed [160]. The lowering of HDL-cholesterol is attenuated when the patient loses weight or when the carbohydrates are derived from food with high fibre content.
Dietary intervention trials with cardiovascular end points have evaluated the effects of reducing fat [161]. Two studies of those reviewed were of relatively short duration, had a rather small sample size, reduced cholesterol levels only minimally and thus neither showed a significant benefit. In the Women's Health Initiative Dietary Modification Trial, 19 541 women were randomly assigned to an intensive behaviour modification group aimed at reducing total fat intake to 20% of calories [162]. After 6 years, mean fat intake decreased by 8.3% of energy intake as compared to the control group. Intermediate cardiovascular risk factors were only minimally affected by the intervention. The diet had nonsignificant impact on the incidence of CHD, stroke and cardiovascular disease in these postmenopausal women.
8.1.2 Fatty acid composition
Food lipids are made up of three major classes of fatty acids (FAs): saturated, monounsaturated and polyunsatu-rated FAs. This classification is based on the number of double bonds between carbon atoms. Fatty acids regulate cholesterol homeostasis and concentrations of blood lipoproteins and affect the levels of other cardiovascular risk factors, such as blood pressure, haemostasis and body weight through various mechanisms.
Saturated fatty acids in food are mainly derived from products of animal origin (meat and dairy products), oils used for cooking or ready-cooked meals from the food-processing industry (coconut and palm oils) and some cooking fats (lard, hard margarines). Reducing saturated fat intakes and replacing with complex carbohydrate, polyunsaturated fat or monounsaturated fats result in lower LDL-cholesterol serum lipids in healthy volunteers [163].
Monounsaturated FAs have a single double bond. Replacement of carbohydrates with monounsaturated FAs increases concentrations of HDL-cholesterol without changing LDL-cholesterol levels [164], and replacement of saturated fats with monounsaturated fats raises the ratio of HDL to LDL, whereas replacement with carbohydrates leave this ratio unaltered. Epidemiological prospective studies have shown that the substitution of saturated FAs by monounsaturated FAs is associated with a lower risk of coronary disease.
Trans FAs are monounsaturated or polyunsaturated FA isomers whose conformation has been modified during the digestion in ruminants or by hydrogenation during industrial processing of foods [165]. Frying food may also increase trans FA content and consumption. Trans FAs are mainly derived from meat, dairy products, margarines and ready-cooked meals from the food-processing industry. Important efforts have been made to reduce the trans FA content in margarines in Europe. Compared with oleic acid, trans FAs increase LDL-cholesterol concentrations and, to a lesser extent, they reduce plasma HDL-cholesterol concentrations [163]. Prospective epidemio-logical studies have found associations between the intake of trans FAs and cardiovascular morbidity and mortality in Northern America and in Europe [166].
Polyunsaturated FAs belong to two major groups having different chemical compositions: n-6 and n-3. Linoleic acid is the main representative of the n-6 group. It is made up of 18 carbon atoms and two double bonds. The n-6 group fatty acids mainly originate from vegetable oils. Experimental clinical studies have shown that the intake of polyunsaturated FAs reduced plasma LDL-cholesterol and, to a lesser extent, HDL-cholesterol as compared to saturated FAs [163]. In prospective epidemiological investigations, the consumption of polyunsaturated FAs instead of saturated FAs or trans FAs is inversely correlated to coronary artery disease risk [167]. A number of nutritional intervention trials have measured the possible impact of replacing saturated fats by polyunsaturated fats on cardiovascular end points (Table 4 – adapted from [161]). These interventions resulted in a significant lowering of plasma cholesterol and cardiovascular outcomes [161].
A Cochrane review on the subject in 2000 concluded that in trials longer than 2 years, the evidence suggests a small but potentially important reduction in cardiovascular disease [168]. Lifestyle advice to all those at high risk of cardiovascular disease (especially where statins are unavailable or rationed), and to lower risk population groups, should continue to include permanent reduction of dietary saturated fat and partial replacement by unsaturates.
8.1.3 n-3 Fatty acids
α-Linolenic acid (ALA) is the precursor in the n-3 group. It is made up of 18 carbon atoms and three double bonds. The main food sources are certain vegetable oils: soybean, sunflower and linen oils. ALA is an essential fatty acid. In prospective epidemiological studies, a high intake of ALA is associated with a reduction in fatal cardiovascular events [169]. Data from randomized clinical trials on the effects of ALA on CVD events are limited and of poor quality [170].
Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are two significant representatives of the n-3 group [171]. These fatty acids are mainly derived from fish oils and fats. There is much evidence suggesting that consumption of EPA and DHA are beneficial for triglycerides, blood pressure, haemostatic balance and heart rhythm [172, 173]. Prospective epidemiological population studies show lower rates of fatal coronary occurrences and sudden death among people who regularly consume fish than among nonconsumers. A recent meta-analysis of cohort studies showed an 11% reduction of CHD mortality in individuals consuming fish one to three times per month, 15% reduction in those consuming fish once a week, 23% for intake of fish two to four times a week and 38% for five or more per week [174]. Similarly, a meta-analysis indicates that the intake of fish is inversely related to risk of stroke, particularly ischaemic stroke [175]. In general, the evidence for the benefits of fish oil is stronger in secondary than primary prevention [170].
Three secondary prevention trials have assessed the effect of fish or fish oil capsules on fatal coronary events. The GISSI study [176] showed a protective effect of EPA/DHA supplementation on fatal events in patients who had suffered a previous MI [RR for total mortality 0.59 (95% CI 0.36-0.97), n = 11 323]. The DART study [177] also showed an initial mortality benefit of dietary advice to increase oily fish intake. In the DART II trial [178], 3114 men with angina were randomized to diet advice to increase oily fish intake, advice to take fish oil supplements or no advice. In contrast to the other two large trials, DART II failed to demonstrate any beneficial effect. In fact, risk of cardiac death was higher in the intervention group (RR for cardiac death 1.26 (95% CI 1.00-1.58), the risk was mainly seen in those on the fish oil supplements. Many consider this study to be flawed, because it was not a randomized controlled trial, the trial was stopped and restarted and the supplement was not pure EPA/DHA and may have contained n-6 fatty acids, which are thought to interfere with the health benefits of n-3 fatty acids.
Lipid lowering and high polyunsaturated fat intervention trials and coronary heart disease
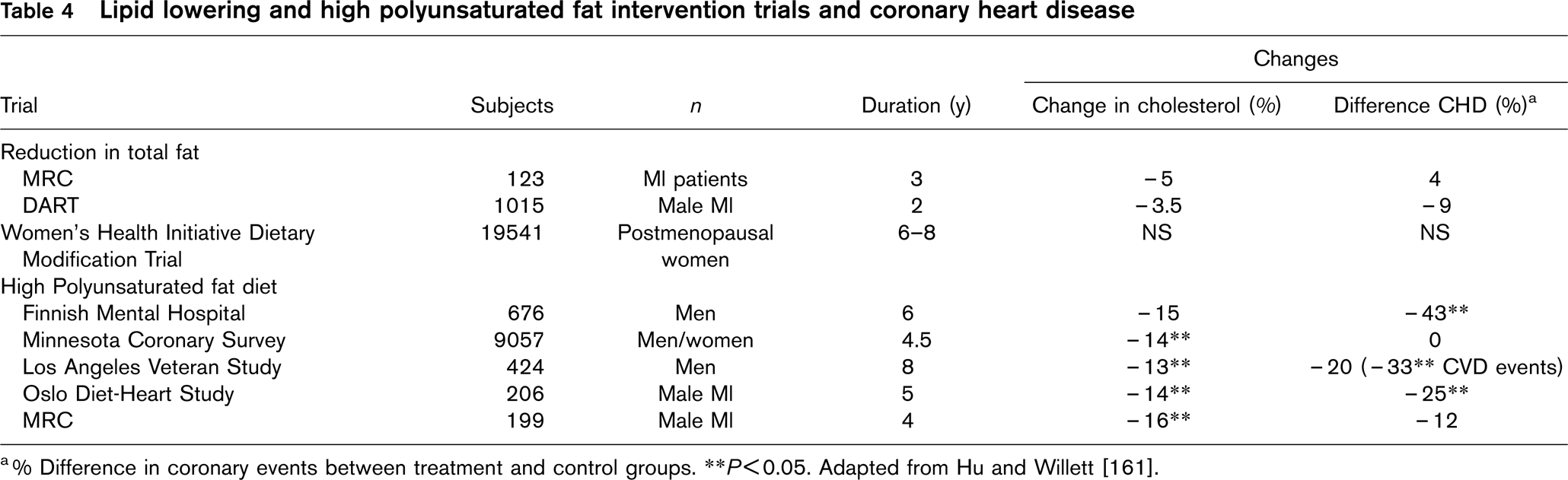
a% Difference in coronary events between treatment and control groups. ∗∗P >0.05. Adapted from Hu and Willett [161].
A recent Cochrane review [179] and meta-analysis [180], both by Hooper et al., concluded: ‘while it is unclear whether ω-3 fats alter cardiovascular end points, there is no evidence we should advise people to stop taking rich sources of ω-3 fats and further high quality trials are needed to confirm suggestions of a protective effect of n-3 fats on cardiovascular health.’ This meta-analysis was criticized mainly because the result was largely influenced by the inclusion of the DART II trial, which is considered to be flawed. On exclusion of this trial the pooled relative risk was similar to that seen previously [RR for all-cause mortality 0.87 (95% CI 0.73-1.03) with DART II, RR 0.83 (95% CI 0.75-0.91) without DART II]. The review was also criticized for considering trials with differing end points and differing patient populations together and for the inclusion of trials of plant and fish-derived n-3 fatty acids together. The above systematic review and the results of the DART II study should not be ignored. However, the many meta-analyses and RCTs showing a significant beneficial effect of ω-3 fatty acids on risk of CVD must also be considered. It is clear that further high quality RCTs are required.
Experimental, clinical and epidemiological data suggest that part of the benefit of n-3 fatty acids on fatal cardiovascular events could be due to antiarrhythmic or heart-rate regulating properties of these fatty acids [181]. In observational studies consumption of fish is associated with a lower incidence of atrial fibrillation in one [182] but not in another study [183]. A meta-analysis of randomized controlled studies with fish oil shows that fish oil reduces heart rate in humans [184]. The analyses on heart rate variability and baroreflex sensitivity has shown inconsistent results [185] andrandomizedclinicaltrials aimed at assessing the occurrence of premature ventricular complexes in patients with implantable defibrillators showed mostly no benefit from n-3 supplementation [185–188].
Recent studies have pointed out the possible harmful effects of methyl-mercury exposure on cardiovascular disease [189]. Because fishes accumulate methyl-mercury and fish consumption is a major source of mercury exposure in humans, several countries have posted fish consumption advisories to reduce exposure of sensitive subpopulation [190, 191].
8.1.4 Dietary cholesterol intake
Dietary cholesterol intake appears to have relatively little effect on serum lipids. Reduction of 100 mg dietary cholesterol per day appears to reduce total serum cholesterol by only 0.06 or 0.07 mmol/l, roughly 1% [192, 193], although this relationship may not be linear [194].
8.1.5 Dietarypattern
It is perhaps naive to expect any single nutrient to have a major effect in preventing CVD. In the past decade nutrition research has moved from the study of micro-nutrients and macronutrients cardioprotective properties to focus on evaluating food-based approaches to prevent cardiovascular diseases [195]. In observational studies, specific dietary patterns have been identified that are associated with increased or decreased incidence of cardiovascular events.
In the Nurses’ Health Study and the Health Professionals’ Follow-up Study a prudent dietary pattern characterized by higher intake of vegetables, fruits, legumes, whole grains and fish was inversely associated with the occurrence of coronary heart disease. In contrast, the Western dietary pattern, characterized by a higher intake of processed meat, red meat, butter, high fat dairy products, eggs and refined grains was associated with an increased risk [196]. The Mediterranean diet is characterized by an abundance of plant food, minimally processed foods, fresh fruit and vegetable, olive oil, dairy products, red meat and eggs consumed in moderate amounts, and a moderate consumption of wine [197]. Several observational cohort studies support the benefit of a Mediterranean diet. In the Greek participants to the European Prospective Investigation into Cancer and Nutrition, a higher degree of adherence to the Mediterranean diet was associated with a reduction in coronary heart disease [adjusted hazard ratio, 0.67 (95% CI, 0.47-0.94)] [198]. Similar results were observed in elderly European men and women [199]. These associations reflect complex behaviours that include, among many other factors, nutritional habits. As part of the GISSI Prevention trial men and woman who had had a myocardial infarction were given the advice to increase their consumption of fish, fruit, vegetables and olive oil. Adherence to diet was assessed with a diet score. Patients who adopted the diet had significantly lower event rates than those with the worst diet score [200].
8.2 Alcohol
Alcohol is not an essential nutrient. The pathophysiological consequences of its consumption depend on the conditions of use (chronic or acute), the quantities ingested, the pattern (with meals, only at weekends) as well as many individual factors (gender, age, genetic susceptibility etc.). Alcohol consumption is linked with an increase of haemorragic cerebrovascular accidents and, to a lesser extent, ischaemic stroke [201] which depends on the dose. On a population scale, the relationship between alcohol consumption and total mortality has a U or J shape. Reduced mortality related to moderate alcohol use results from reduced coronary mortality; an association that was attributed in large part to an effect on HDL-cholesterol, glucose intolerance and fibrinogen [202]. In contrast, observational studies and clinical trials have consistently demonstrated a direct, dose-dependent relationship between alcohol intake and blood pressure [203]. To date no randomized trial has proven that the voluntary intake of a moderate quantity of alcohol is beneficial in terms of cardiovascular morbidity and mortality. There is also no reliable proof showing any higher cardiovascular benefit of any drink, compared with another [204]. Furthermore, advocating the therapeutic cardioprotective use of alcohol raises serious concerns with regard to dependence and abuse with consequent toxicity.
8.3 Sodium, potassium and other electrolytes and blood pressure
There is abundant evidence from animal studies, clinical trials, epidemiological studies and meta-analyses that sodium intake increases blood pressure and therefore the risk of arterial hypertension, stroke, CHD and heart failure [205, 206]. In societies with low salt intake there is no age-related increase in blood pressure [207].
In a recent meta-analysis [208], a median reduction in urinary sodium excretion of 1.8 g/d lowered systolic and diastolic blood pressure by 2 and 1 mmHg in normoten-sive and 5 and 2.7 mmHg in hypertensive individuals.
Animal experiments, observational epidemiological studies and clinical trials support the evidence that high potassium intake is associated with reduced blood pressure. In a recent meta-regression, the average blood pressure reduction associated with a median −77 mmol/24 h increase in urinary sodium was 2.54 mmHg systolic and 1.96 mmHg diastolic [209]. The corresponding values for increased potassium intake of 44 mmol/24 h were −2.42 and −1.57 mmHg, respectively. Blood pressure response was larger in hypertensive than normotensive individuals, both for sodium and potassium. The effect of potassium on blood pressure depends on the concurrent consumption of salt. An increased intake of potassium has a greater lowering effect on a high salt intake background.
A recent Cochrane review on dietary salt reduction for the prevention of CVD [210] sounded a note of caution – intensive interventions, unsuited to primary care or population prevention programmes, resulted in minimal reductions in blood pressure during long-term trials. Further evaluations to assess effects on morbidity and mortality outcomes are needed for populations as a whole and for patients with elevated blood pressure. A low sodium diet may help to maintain a lower blood pressure after the withdrawal of antihypertensives.
8.4 Fruits and vegetables
Fruits and vegetables are significant sources of minerals, vitamins and fibres. Observational studies have shown favourable relationships between the consumption of the main antioxidant vitamins or of the plasma levels of such vitamins and cardiovascular diseases. These results have been confirmed in cohort studies which have shown negative correlations between the consumption of fruits or vegetables and the occurrence of stroke or coronary events [211]. In a meta-analysis of prospective observational studies each serving increment of fruit and vegetable intake was associated with a 4% reduction in risk of coronary events, respectively [212]. Similarly, in another meta-analysis, the consumption of each additional portion intake of fruit and vegetable per day was associated with a 5% reduction in the relative risk of stroke [213]. The results of these observational studies suggest that eating fruits and vegetables on a regular basis has beneficial effects on the cardiovascular system. However, in line with other lifestyle trials, a randomized controlled trial assessing the exact magnitude of this benefit would be difficult to conduct because of compliance and cross-over issues. This was the subject of a Cochrane review in 1999 [214].
The most important sources of potassium are fruits and vegetables. The effects of potassium on blood pressure are discussed above. The results of the DASH trials have demonstrated that the combined increase in the intake of fruit and vegetable and salt restriction was followed by greater reduction in blood pressure than the single effects of sodium restriction [205, 215–217]. Another trial used a brief negotiation method to encourage an increase the consumption of fruit and vegetables to at least five portions a day in patients aged 25-64 years without serious chronic illness. Systolic and diastolic blood pressure fell significantly by 4 and 1.5 mmHg, respectively, in the intervention group [218].
8.5 Whole grain intake
There is now evidence from large epidemiological studies which show a risk reduction of about 25-30% when whole grain consumption is at least three servings per day [196, 219–227]. There are no clinical trials to date. It is important to remember that carbohydrate intake contributes the major part of energy intake.
8.6 Vitamins supplements
8.6.1 Vitamin E: α-tocopherol
Vitamin E is a powerful antioxidant. The incorporation of vitamin E to LDLs, through food supplementation, reduces the susceptibility of LDLs to oxidation in vitro. Cohort studies have demonstrated an inverse relationship between the intake of vitamin E and cardiac morbidity and mortality. Intervention trials with vitamin supplements have not confirmed these observations [176]. Vitamin E is not indicated for CVD prevention.
8.6.2 Vitamin A: β-carotene and retinol
Vitamin A is a general term combining a set of molecules: carotenoids (pro ‘vitamin A') and retinoids. Many epidemiological observation, case/control and prospective studies have found an inverse relationship between vitamin A plasma levels, the intake of vitamin A in food and cardiac morbidity and mortality. Intervention studies of vitamin supplements have failed to confirm these results. Again, these vitamins have no proven role in CVD prevention.
8.6.3 Multivitamin supplementation
In the SI.VI.MAX study, 13 017 French adults (7876 women and 5141 men) were randomized to a combination of 120 mg of ascorbic acid, 30 mg of vitamin E, 6 mg of β-carotene, 100 μg of selenium, and 20 mg of zinc or a placebo. After 7.5 years, low-dose antioxidant supplementation had no effect on cardiovascular incidence [228].
8.6.4 Homocysteine, vitamin B12, folic acid and vitamin B6
Homocysteine is an amino acid produced by the catabolism of methionine. Homocysteine plasma concentrations are determined by genetic and nutritional factors. They are increased by dietary deficiencies in leaf vegetable vitamin, vitamin B6 (pyridoxine), vitamin B12 (cobalamin) and folate and excessive methionine intake. In a systematic analysis of case/control studies and prospective inquiries, a moderate increase in blood homocysteine is linked with a higher coronary risk [229–232]. Three recent intervention trials have tested the hypothesis that reducing homocysteine by vitamin B6 (pyridoxine), vitamin B12 (cobalamin) and folate supplementation will prevent cardiovascular events. In the VISP (Vitamin Intervention for Stroke Prevention) trial [233], 3680 patients with nondisabling cerebral infarction and plasma homocysteine levels ≥ 25th percentile for North America stroke population (≤ 10 μmol/l) were randomly assigned to a low-dose or high-dose vitamin cocktail containing pyridoxine, cobalamin and folic acid. During the follow-up mean homocysteine was 2 μmol/l lower in the high dose vitamin supplement group. After 2 years of intervention there was no evidence of any benefit of high dose vitamin supplementation on any of the end points. The NORVIT trial included 3749 men and women with myocardial infarction; [234]. Patients were randomly assigned in a two-by-two factorial design to receive folic acid and vitamin B12, vitamin B6, both or placebo (approximately 930 patients per group). During the intervention period homocysteine level was lowered by 27% among patients taking the combination of folic acid and vitamin B12. After 3.5 years of follow-up there was no evidence of any benefit of vitamin supplementation for cardiovascular end points (new nonfatal and fatal MI, stroke and sudden death). Contrary to the author's expectation, there was a trend toward an increased rate of events among patients taking the combination of folic acid, vitamin B12 and vitamin B6. In the HOPE trial [235], 5522 patients with vascular disease or diabetes were randomly assigned to receive a combination treatment of folic acid, vitamin B6 and vitamin B12 or placebo for an average of 5 years. Mean plasma homocysteine was decreased by 2.4 μmol/l in the active-treatment group. Active treatment did not significantly decrease the risk of death from cardiovascular death (death from cardiovascular causes, MI and stroke). There was, however, a marginal reduction in stroke and more patients hospitalized for unstable angina in the active treatment group. Altogether, these trials provide no evidence of clinical benefit from the use of folic acid, vitamin B12 or vitamin B6 to prevent cardiovascular events in patients with established vascular disease. It has been pointed out that some of these studies were carried out in populations exposed to mandatory folate supplementation, and that all studies to date were underpowered. A recent meta-analysis of folate trials concluded that while folic acid supplementation has not been shown to reduce risk of cardiovascular diseases or all-cause mortality among participants with a prior history of vascular disease, several ongoing trials with large sample sizes may provide a definitive answer to this important clinical and public health question [236].
8.7 Plant sterols
Plant sterols are naturally occurring constituents of plants that differ from cholesterol only in the structure of their side chain. The two most common constituents are sistosterol and campesterol and their saturated products sistostanol and campestanol, respectively. Previous findings indicate that plant sterol reduce cholesterol absorption by 30-50% [237]. This reduction is thought to result from the direct competition of plant sterols with cholesterol for incorporation into mixed micelles [238]. Because plant sterols are slightly more hydrophobic than cholesterol they are preferentially incorporated into the micelles in place of cholesterol. In order to be used in foods plant stanols need to be esterified. Consumption of 2 g/d of plant sterols has been shown to lower total and LDL-cholesterol in a variety of different populations [239]. In contrast, it has no impact on plasma triglycerides and HDL-cholesterol. In a dose-response study ranging from 0.8 to 3.2 g/d of stanol ester intake for 4 weeks, a significant decrease in LDL-cholesterol level was observed at doses 1.6 g/d or more. However, higher intakes at 3.2 g/d did not add further lowering compared to the 2.3 g/d dose. Further analyses reached the same conclusion and demonstrated an average of 10% reduction in LDL-cholesterol levels for an optimal intake of 2 g/d [240]. In general, the LDL-lowering effect of plant sterol esters is proportionately greater in individuals with high intakes of saturated fat and cholesterol than those with low intake. When associated with a high polyunsaturated fatty acid diet, LDL decreased by 19%. Few studies have analysed the efficacy of stanol esters in different dietary backgrounds. Most studies have used vehicles that were high in fat such as margarine. Recently, stanol esters were administered with low-fat yoghurt resulting in similar dose-to-dose LDL-lowering as stanol ester from margarine.
There are a number of concerns with the use of plant sterol and stanol esters. To date no randomized nutritional trial has yet proven that plant sterol or stanol esters confer a benefit in terms of cardiovascular mortality. Furthermore, plant sterol contents have been found to accumulate in atherosclerotic plaque [241]. Until long-term studies are performed to ensure safety in all individuals plant sterols should be regarded as optional, adductive therapy in adults with elevated LDL-cholesterol levels [240].
8.8 Policosanol
Policosanol, a natural mixture of aliphatic primar alcohols isolated from sugar cane, has been reported to lower total and LDL-cholesterol and increase HDL-cholesterol in healthy volunteers, in patients with hypercholesterolemia as well as hypercholesterolemic patients with type 2 diabetes [242]. The results of some studies with sugar cane policosanol even suggested similar efficacy to statins [243]. However, most of these studies were performed in a relatively small number of patients and in very few centres. There was just one study performed with rice policosanol which showed much less effect on total cholesterol and no effects on LDL-cholesterol, HDL-cholesterol and triglycerides [244].
8.9 Obesity and overweight: risk and management
8.9.1 Scientific background
As societies develop a higher standard of living, cardiovascular mortality initially increases. This is followed by a reduction in both major risk factors such as blood cholesterol and high blood pressure which, together with improvements in therapy, translate into reduced cardiovascular mortality. The exceptions to these trends are body weight and diabetes which tend to increase as other risk factors decline. Obesity is becoming a world wide epidemic in both children and adults [245]. Currently, it is estimated that, worldwide, over one billion people are overweight, and over 300 million are obese. Over one third of children are overweight or obese.
8.9.2 Body weight and risk
It is now clear that fat, and in particular intra-abdominal visceral fat, is a metabolically active endocrine organ that is capable of synthesizing and releasing into the bloodstream an important variety of peptides and nonpeptide compounds that may play a role in cardiovascular homeostasis. Excess adipose tissue is associated with increased secretion of free fatty acids, hyperinsulinaemia, insulin resistance, hypertension and dyslipidaemia [246, 247]. This impacts on CVD risk factors and hence on risk. The mechanical effects of overweight impact on noncardiovascular cause of morbidity and mortality. The health effects of increasing body weight are summarized in Table 5.
Interestingly, the effects of multivariate adjustment on the association between lipid levels and risk and between body weight and risk are different. Raised blood cholesterol and reduced HDL-cholesterol level remain independently associated with risk after adjustment for other major risk factors, whereas the association between weight and risk tends to lose significance. This should not be interpreted as indicating that body weight is not important; rather, it may be critically important because it exerts its effect on risk by its adverse effects on many risk factors.
Impact of increasing body weight on risk factors, morbidity and mortality
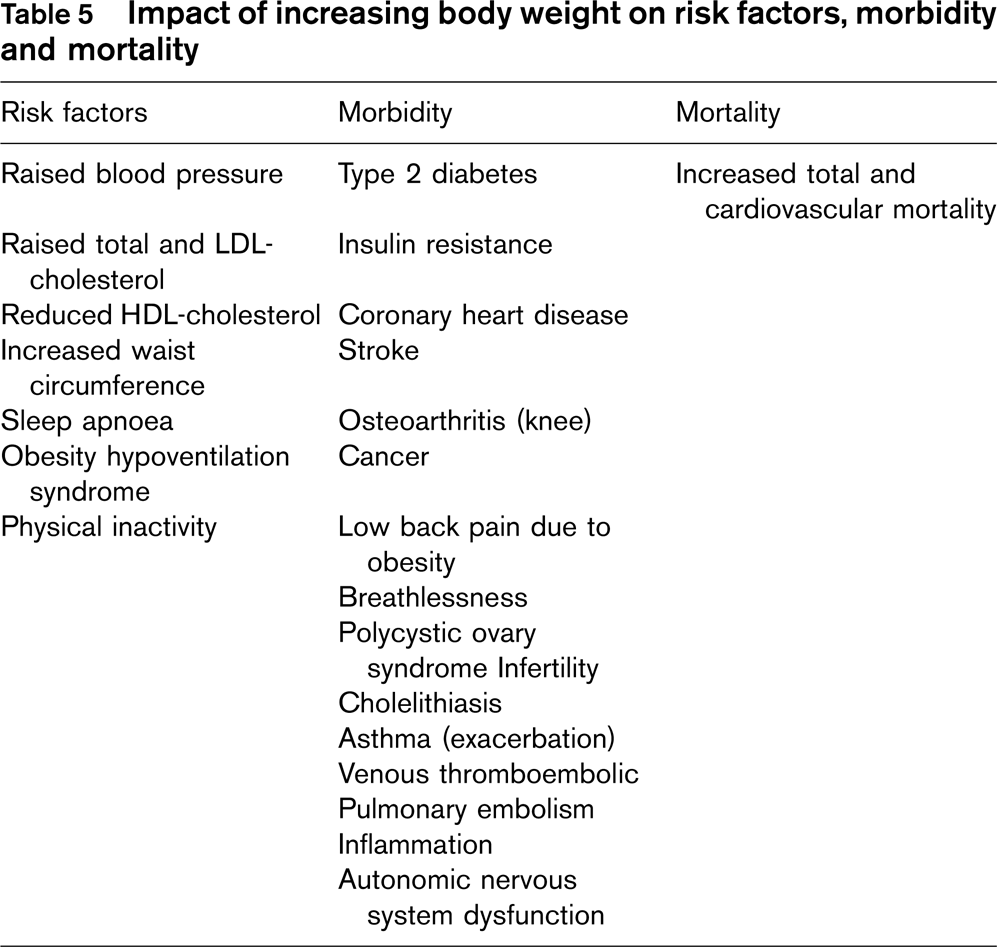
8.9.3 Which index of obesity is the best predictor of cardiovascular risk and cardiovascular risk factors – BMI, WC or WHR?
Recent studies have demonstrated that regional distribution of adipose tissue may be more important in determining cardiovascular risk than total body weight. Excess central (visceral abdominal) fat in particular has been shown to be strongly associated with metabolic and cardiovascular risk [248]. This has led to increased interest in anthropometric measures of risk. Most data are available for body mass index (BMI), waist-hip circumference ratio (WHR) and, more recently, simple waist circumference (WC). Such measures are cheap and universally available measures of risk. Waist circumference, while simple, may be more prone to measurement error than body mass index. The optimal level for measurement of WC is midway from the lower rib margin to the anterior superior iliac crest, in the standing position [249]. The evidence supporting each measure in estimating risk is now considered.
Body mass index (BMI) has been extensively used to define the groups of body weight [kg/height (m)2] using classifications suggested by the National Institutes of Health and the World Health Organization. In adults, overweight is defined by an increased BMI ranging from 25 to 29.9 and obesity by BMI ≥ 30. Increasing BMI is highly associated with cardiovascular disease.
Several cross-sectional and cohort studies have assessed whether the measurement of WC in addition to BMI improved the ability to predict the presence/development of cardiovascular risk factors associated with obesity, for example high blood pressure, markers of insulin resistance, low high density lipoprotein cholesterol and high low density lipoprotein cholesterol. In general, these have indicated that within BMI categories the finding of elevated WC indicates a greater probability of the presence of risk factors and CHD mortality [249–257]. The added predictive ability has been shown to be more marked in women [252, 254, 257] and in younger age groups [253]. In some the findings have not held in men [254, 258].
The opposite situation has also been addressed – does the addition of BMI to WC improve the prediction of presence of cardiovascular risk factors? Janssen et al. [259] concluded that when WC was measured as a categorical variable (high/normal) addition of BMI category improved prediction; however, the addition of BMI as a continuous variable to a model containing WC as a continuous variable did not improve predictive ability. Other studies have failed to confirm superiority of WC over BMI in prediction of risk factors [260] or shown improvement in predictive ability when BMI is included in models containing WC [256, 257]. The weight of evidence therefore supports the use of both BMI and WC in assessing risk of metabolic abnormalities and cardiovascular risk factors associated with obesity.
In longitudinal studies in men [261] and women [262], increased WHR was associated with increased risk of CHD mortality. In these studies neither WC nor BMI was significantly associated with CHD mortality. In men the development of diabetes was also related to the WHR even when adjusting for the effect of BMI. These findings are in contrast to the results of the Iowa women's health study [251] which showed WC to be the anthropometric measure with the strongest ischaemic heart disease mortality association. The INTERHEART case-control study compared 12461 patients with myocardial infarction to 14 637 controls and showed that both increased WC and WHR were associated with MI even after adjustment for other cardiovascular risk factors and BMI [263].
Most of the cross-sectional studies which compared WHR and WC as markers of risk factors have demonstrated superiority of WC [251, 256]. One study that examined the effect of both WC and hip circumference on the development of risk factors, showed that both measures had independent but opposite effects on the presence of risk factors [255]. Hip circumference was particularly linked to fat-free mass in men, and they suggest further investigation into the value of this measure. They also found that the relative contributions of the two variables were poorly captured in the WHR. Further confirmation of this is provided by a study which showed WC correlated better with both abdominal visceral adipose tissue as measured by computed tomography and metabolic risk factors, than WHR [264]. While it is clear that there are some discrepancies in the evidence base regarding which anthropometric measure is superior, assessment of abdominal obesity in addition to BMI is recommended.
Both the WHO report on obesity [265] and the American National Heart, Lung and Blood Institute expert panel on obesity [266] recommend the use of WC as an additional indicator of risk for metabolic risk factors, within each category of BMI. Of various definitions [265–268], the WHO cut points are the most widely accepted in Europe; two action levels are recommended. Action level 1 – WC ≥ 94 cm in men and ≥ 80 cm in women represents the threshold at which no further weight should be gained. Action level 2 – WC ≥ 102 cm in men and ≥ 88 cm in women represents the threshold at which weight reduction should be advised. The cut points have been calculated based on white people and it is apparent that different cut points for anthropometric measurements are required in different races and ethnicities [269].
In conclusion, there is no solid evidence for superiority of either variable in the prediction of risk factors. Waist circumference has the advantage of simplicity, may be a slightly better estimator of risk than BMI, but is probably more prone to measurement error.
8.9.4 Imaging and fat distribution
Several measurements have been described for assessing the anatomical distribution of fat such as computer tomography (CT), ultrasound (US) and magnetic resonance imaging (MRI). They allow changes in intra-abdominal fat to be monitored. But they are expensive and time consuming and are to be regarded as specialist research tools rather than everyday risk assessment tools at this time.
Anthropometric measurements such as WC and WHR provide a useful estimation of the proportion of abdominal or upper-body fat but they do not distinguish between accumulations of deep abdominal (visceral) fat and subcutaneous abdominal fat. CT can be considered the gold standard not only for adipose tissue evaluation but also for multicompartment body measurement [270]; the subcompartments of adipose tissue volume, visceral and subcutaneous adipose tissue, can be accurately measured with errors of 1.2 and 0.5%, respectively.
MRI provides results similar to CT without exposure to ionizing radiation, the main problem with CT multislice measurements. It demonstrates good reproducibility for total and visceral adipose tissue volumes [271].
Two studies have compared estimates of subcutaneous and visceral adipose tissue by CT and MRI. Comparison between MRI and CT in seven patients showed a high degree of agreement in measurement of total subcutaneous adipose tissue area but not visceral adipose tissue area [272]. Moreover, it has been shown [273] that MRI when compared with CT overestimates subcutaneous adipose tissue (+ 8%) and visceral adipose tissue (+22%).
Several studies demonstrated a highly significant correlation between the intraabdominal adipose tissue determined by CT and by US [274, 275]. The intraindividual and interindividual reproducibility of US measurements was very high both for intraabdominal and subcutaneous thickness [274].
Sagittal abdominal diameter (SAD) is derived either from a CT abdominal scan [264] or by using a sagittometer placed over the abdomen perpendicular to the length axis of the trunk at the iliac crest level (L4-5) when the patient is in supine position on a firm bench with the knees bent [276]. Kvist et al. [277] were first to demonstrate and other authors confirmed that the sagittal abdominal diameter correlates strongly with visceral fat volume as measured by computed tomography (CT) [278, 279]. Petersson et al. [276] investigated the association of SAD compared to conventional anthropometric measures and showed that SAD was a stronger predictor of cardiovascular risk factors, especially of insulin resistance, apoB, insulin, triglycrides and CRP, than the other anthropometric measures.
CT scanning is expensive and involves exposure to radiation. It is not as yet recommended for routine clinical risk asessment.
8.9.5 Exercise and impact on weight, fat metabolism and risk
Sedentary lifestyle and obesity are important lifestyle-related public health problems throughout the world. Physical inactivity and excess body mass are associated with a number of health-related risk factors, and are also independent risk factors for cardiovascular disease (CVD). Weight reduction is an important first step to control risk factors for coronary heart disease. Although weight loss is the major target, treatment involves a range of strategies including prevention, weight maintenance and management of obesity-related risk factors.
The primary prevention strategy is promotion of a healthy lifestyle including a low-calorie intake combined with an increased physical activity. There is sufficient evidence available from intervention studies which supports the role of physical activity and moderate to vigorous exercise in promoting weight loss [280]. Several recent reviews have shown the relationship of physical activity with CVD; individuals who exercise regularly are less likely than sedentary individuals to die from coronary heart disease and CVD. Haapenen-Niemi et al. [281] reported relative risks of 1.61 for men and 4.68 for women for CVD mortality with no weekly activity compared with the most active individuals. Physically active people have significantly lower mortality from cardiovascular, cancer and all causes compared with sedentary people.
Most studies of the relationship between physical activity and lipid profile indicate a reduction in plasma triglycerides and an increase in HDL-cholesterol [282–286].
Hu et al. showed the effect of physical activity and body mass index on CVD mortality among 47 212 middle-age Finnish men (22 528) and women (24 684). Among the inactive and obese men, compared with the reference group, the hazard ratios for CVD and total mortality were 2.09 and 1.78. Among women the hazard ratios were 2.18 and 2.10, respectively [287]. Regular physical activity and normal weight are both important indicators of a decreased risk of mortality from all causes, CVD and cancer. Physical activity had a strong independent effect on mortality.
Recent research has indicated that exercise may have beneficial effects before a training effect is apparent [288, 289] and may impact on abdominal fat metabolism before weight loss occurs [288, 289]. This information may be valuable in motivating high risk persons to initiate exercise. The Multiple Risk Factor Interventional Trial [290] data showed that men performing light and moderate intensity leisure time physical activity, as measured by the Minnesota Questionnaire [291], for 30 min or more a day, had a significant reduction in risk of fatal CHD events, as compared to men performing less physical activity [292].
8.9.6 Management
8.9.6.1 Nutritional treatment of cardiovascular diseases
Nutrition is an integral part of cardiovascular patient treatment. All patients with cardiovascular disease and individuals at high risk should be given recommendations on the food and dietary options which reduce the cardiovascular risk.
Dietetic recommendations should be defined individually, taking into account the individual's risk factors – dyslipaemia, hypertension, diabetes and obesity.
Within the family setting, the role of the person in charge of buying and cooking food is clearly important.
8.9.6.2 General recommendations
Eating food from each major food group will ensure the appropriate supply of nutrients, minerals and vitamins.
The intake of fish, fruit and vegetables, cereals and whole grain products, skimmed dairy products, low salt and lean meat is encouraged.
Energy intake should be adjusted to maintain ideal weight.
Eating oily fish and ω-3 FAs may be associated with a reduction in risk of fatal cardiovascular accidents.
Replacement of saturated and trans FAs with monounsaturated or polyunsaturated fats of vegetable origins decreases LDL-cholesterol.
Eating fruit and vegetables and restricting salt is associated with lower blood pressure.
8.9.7 Specific recommendations
8.9.7.1 LDL-cholesterol
A reduction in plasma LDL-cholesterol is obtained by
Lowering the intake of saturated FAs and trans FAs and, to a lesser extent, by reducing the intake of cholesterol in food. Saturated and trans FA should be substituted for polyunsaturated fat of vegetal origin.
Saturated fats are found in a wide variety of foods, including meat and dairy products, meat pies, sausages, cheese, butter and lard, pastry, cakes, biscuits, cream, coconut oil, palm oil and in a large number of processed foods.
Trans FAs are found in animal-based foods. Dairy and beef fat typically contains around 3-6% TFAs (% of total fatty acids). The TFA content of bakery products (rusks, crackers, biscuits, etc …) as well as some breakfast cereals with added fat, French fries, soup powders and some sweet, snack products and hard margarine may vary considerably (from below 1% up to 30%). Soft margarines contain only trace TFAs. Consumers are invited to check saturated and trans FA content on food labels.
Soluble fibres and phytosterols may help to reduce the plasma concentrations of LDL-cholesterol.
8.9.7.2 HDL-cholesterol
An increase in the concentration of plasma HDL-cholesterol is obtained by:
Increasing exercise in sedentary individuals, weight loss in obese individuals and controlling glycaemia in diabetic individuals.
Eating refined sugars is associated with a reduction in HDL-cholesterol concentrations among certain susceptible individuals. These sugars should be replaced with complex sugars.
Olive oil may help to increase HDL-cholesterol levels. An increase in monounsaturated FA may be recommended in patients with the metabolic syndrome.
The moderate use of alcohol may increase HDL-cholesterol. While not a positive recommendation, it is not contraindicated in individuals with a low HDL-cholesterol concentration.
8.9.7.3 Triglycerides
Lowering triglycerides is obtained by:
Increasing exercise in sedentary patients, weight loss for obese patients and controlling glycaemia for diabetic patients.
The intake of refined sugars and alcohol should be controlled as it is associated with increases in plasma triglycerides, among certain susceptible patients.
The intake of ω-3 FAs present in oily fish and some vegetable oils can contribute to a decrease in plasma triglyceride concentrations.
8.9.7.4 Arterial blood pressure
Lowering blood pressure is obtained by:
Weight loss for overweight/obese patients, controlling the intake of salt and alcohol and increasing the intake of potassium.
To reduce salt intake, consumers should choose fresh or frozen foods low in salt and limit the amount of salt added to food. Because the vast majority of ingested salt comes from processed foods, any meaningful strategy to reduce salt intake must involve food manufacturers. Consumers are invited to check food labels for salt content.
Fruit and vegetables should be preferred as a source of potassium rather than supplements.
8.10 Management of obesity and overweight
Intentional weight loss in obese patients can improve or prevent many of the obesity-related risk factors for CHD. It is important for cardiovascular healthcare professionals to understand the clinical effect of weight loss and be able to implement appropriate weight-management strategies in obese patients [293]. The beneficial effects of weight reduction on the cardiovascular system are listed in Table 6 [245]. Reduction in blood pressure occurs before attainment of desirable body weight. In a recent meta-analysis blood pressure reduction were −1.05 mmHg systolic and −0.92 mmHg diastolic/kg of weight loss [294]. A Cochrane review concluded that weight reducing diets in overweight hypertensive persons can affect modest weight loss in the range of 3-9% of body weight and are probably associated with modest blood pressure decreases of roughly 3 mmHg systolic and diastolic. Weight reducing diets may decrease dosage requirements of persons taking antihypertensive medications [295].
8.11 Diet and behavioural interventions
Many different diets and behavioural interventions have been proposed for the treatment of obesity. The control of overweight is dependent upon achieving the appropriate balance between energy intake and expenditure. The dietary approaches vary in their total energy content, macronutrient composition (protein, carbohydrates and lipids), energy density and glycaemic index [293]. The low fat diet is considered the standard approach to weight reduction and has a more favourable effect on LDL-cholesterol. Total fat intake should be kept between 25 and 35% of energy. Reduction in saturated fats is the preferred target due to its effects on the lipoprotein profile. Saturated and trans FA intake should be less than 7% [162].
Effects of weight reduction on the cardiovascular system
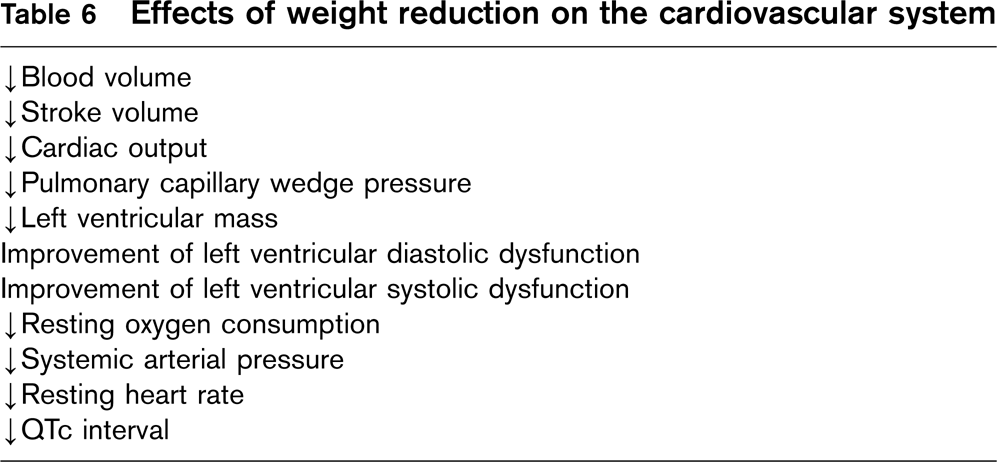
The low-carbohydrate diet has become popular and in the short-term decreases body weight greatly and also has a good effect on plasma triglycerides and HDL-cholesterol [296]. However, the long-term safety is still under investigation. Alcohol is a major source of calories and reduction may be an important part of weight control.
Behaviour modification inducing long-term lifestyle change leading to a gradual weight loss is the basis of all obesity treatment. The behaviour change process is facilitated by the use of goal-setting, self-monitoring and problem-solving techniques [297]. Studies using this approach often achieve a weight loss of 8-10% of the initial body weight at 6 months follow-up [298]. One key feature of such a programme is to discuss with the patient, in an empathic manner, both short-term and long-term goals. Furthermore, the goals should be realistic, measurable, concrete and engaging. Another key feature is self-monitoring, where the patient keeps a detailed record of his behaviours such as food intake and physical activity. Using goal-setting and self-monitoring together, individuals may easily experience satisfaction by looking at their recordings and find out that their goals have been attained. This will boost the self-efficacy for the behaviour in question. A randomized trial examining the combined effects of lifestyle modification and pharmacologic treatment (using sibutramine), showed that the combination gave a significantly larger weight loss than sibutramine alone at 1 year follow-up [299], indicating that medication may complement but should not replace efforts to achieve healthier behaviour.
According to a recent Cochrane review, behavioural and cognitive-behavioural therapy help with losing additional weight when added to diet and exercise programs [300]. Behavioural interventions have also been shown to help maintain weight loss [301].
8.12 Drug treatment of overweight
In general, the contribution of drug treatments is modest and, in the past, some products have had serious side effects.
Orlistat inhibits intestinal lipases to prevent the hydrolysis and uptake of fat. Weight loss is usually modest and gastro-intestinal disturbance may occur. It should be used with full and balanced diet.
Sibutramine enhances a feeling of satiety after food by an effect of its metabolites which inhibit noradrenaline and serotonin uptake. Both contraindications and side effects are appreciable.
Rimonabant is an endocannabinoid receptor inhibitor that appears capable of inducing a modest but sustained weight loss in combination with a calorie controlled diet. It may improve glucose tolerance, beneficially affect lipid metabolism and is associated with a modest reduction in blood pressure. Possible adverse effects on depression are being monitored. It remains to be seen if its promising effects on weight and other risk factors will translate into hard evidence of reduced cardiovascular events.
8.13 Practice points
Overweight people are at increased risk of diabetes, hypertension, and dyslipidaemia and of many causes of general and cardiovascular illness and death.
Overweight with consequent adverse effects on cardiovascular risk such as diabetes is increasing in all developing and developed countries.
Intra-abdominal fat is metabolically active and more strongly associated with risk than total body weight.
The most widely accepted measures of overweight are body mass index (BMI) and waist circumference (WC). WC may be a slightly better estimator of CVD risk but may be more prone to measurement error.
WC of 80 cm in women and 94 cm in men represents the level at which no further weight should be gained and WC of 88 cm in women and 102 cm in men represents the level at which weight reduction should be advised.
Effective weight reduction, especially when combined with exercise, reduces cardiovascular risk factor levels.
It is not yet certain that weight reduction alone reduces mortality.
It is not known whether drug treatment of overweight has the same, less or more impact on cardiovascular risk as lifestyle change.
Chapter 9: Physical activity
Managing total CVD risk-PHYSICAL ACTIVITY
Stress that the positive health benefits occur with almost any increase in activity; small amounts of exercise have an additive effect; exercise opportunities exist in the workplace, for example by using stairs instead of the lift.
Try to find leisure activities that are positively enjoyable.
30 minutes of moderately vigorous exercise on most days of the week will reduce risk and increase fitness.
Exercising with family or friends tends to improve motivation.
Added benefits include a sense of well being, weight reduction and better self esteem.
Continued physician encouragement and support may help in the long-term.
Health benefits occur with almost any increase in physical activity at any age; this is an important and powerful message to help people to start to become more active.
Chapter 9: Physical activity
9.1 Scientific background
9.1.1 Physical inactivity as a risk factor
Physical inactivity is a growing public health problem. This will have a major impact on the prevalence of atherothrombotic cardiovascular diseases in the coming decades as a lack of physical activity is apparent in the young generation in several European countries.
Physical fitness has both a direct protective effect on the development of vascular lesions and an indirect effect through influencing other risk factors: lowering plasma LDL-cholesterol and triglycerides, increasing plasma HDL-cholesterol and insulin sensitivity, reducing body fat and lowering blood pressure. A lack of physical fitness will have a reverse effect.
Thus, the promotion of regular physical activity at school, at the place of work, during leisure time and after old-age retirement is an important target for preventive cardiology as it may effectively improve the future course of CVD in Europe.
9.1.2 Physical activity in children and adolescents
Atherosclerosis begins in childhood: the first stage, an often reversible fatty streak, is seen in most children. The more harmful later stage, the atheromatous plaque, does not appear until after puberty in boys and much later in girls. Thus, positive modification of traditional risk factors, such as hypertension, dyslipidemia and smoking are important in the early stages of the process [302]. Regular physical activity at a young age protects against the early onset of atherosclerosis.
Studies have shown that physical activity in children is declining, with children today expending approximately 600 kcal/day less than their counterparts 50 years ago [303]. Outdoor games such as football and skipping have been replaced by long hours in front of a computer, often combined with the intake of unhealthy amounts of fast-food. Consequently, the prevalence of obesity is increasing at an alarming rate, and type 2 diabetes mellitus previously not seen in children is now diagnosed at a younger age [304, 305].
Physical education in school may form the starting point for an active lifestyle later in life. Yet, in few countries do children have access to the recommended daily dose of physical activity. School gymnastics and sports have been given lower priority in many countries in recent years. More than half of the adolescents become physically inactive after leaving school.
9.1.3 Physical activity in adults without clinical signs of CVD
Over the past decades the physical demands at the place of work have decreased significantly. Only a minority of labourers will experience some degree of breathlessness in their daily work. Even in domestic work and during leisure time there is a trend to a lower energy demand.
Prospective epidemiological studies have shown that a sedentary lifestyle is associated with a doubling of the risk of premature death and with an increased risk of cardiovascular disease [306–317]. In both healthy men and individuals diagnosed with CVD exercise capacity is a more powerful predictor of mortality than other established risk factors for cardiovascular disease [318]. Both fitness and physical activity are predictors of mortality, although exercise capacity has a stronger predictive value. Increasing activity to expend a further 1000 kcal/week, which is approximately similar to 1 metabolic equivalent (METs) increase in fitness, may result in a mortality benefit of 20% in men [319]. Avoiding a sedentary lifestyle during adulthood may even substantially extend the total life expectancy and the cardiovascular disease-free life expectancy for women and men (1.3-3.5 years) [320].
It has recently been shown that physical activity among women is associated with CVD risk in a dose-response fashion, where even a slight increase of activity for sedentary women will provide benefits [321]. In women increased adiposity and reduced physical activity are strong and independent predictors of mortality: the combination of excess weight (BMI ≥ 25) and physical inactivity (>3.5 h of activity per week) could account for 59% of premature cardiovacular mortality [322].
A high level of habitual physical activity helps to prevent overweight, improves dyslipidemia and lowers blood pressure levels. Even moderate physical activity can have a beneficial effect on mortality as well as on the risk of nonfatal coronary heart disease events [307, 308, 312].
Maintaining regular physical fitness may also have a direct protective effect against CVD independent of other risk factors. Restitution of endothelial dysfunction has been proposed as an explanatory mechanism [323]. The blunting effect of exercise on oxidative stress may lead to the assumption that exercise training should be considered as an effective antioxidant and antiatherogenic therapy [324].
Regular exercise has been demonstrated to protect against the risks of strenuous exertion precipitating myocardial infarction: for the untrained individual sudden heavy work will increase the risk of an acute cardiac event considerably; a well-trained person will develop an adaptation to work stress, which will be protective against an acute cardiac event [325, 326].
9.1.4 Physical activityin adults with clinical signs of CVD
Once CVD has been diagnosed patients tend to restrict their physical activity in fear of further deterioration of their heart condition or in order to prevent exercise induced attacks of chest pain. The protective attitude of the family may contribute to a sedentary lifestyle.
In Europe a minority of patients with CVD are routinely referred for comprehensive cardiac rehabilitation including exercise training programmes. Yet, meta-analyses of randomized trials of cardiac rehabilitation in patients surviving an acute myocardial infarction have shown that participation may lead to a 20-25% reduction in overall mortality [327, 328]. In the latest meta-analysis, including 8940 patients, the pooled effect estimate for total mortality for the exercise only intervention showed a reduced all-cause mortality (odds ratio [OR] = 0.80; 95% CI: 0.68-0.93) and cardiac mortality (OR = 0.74; 95% CI: 0.61-0.96) [329].
In earlier studies it has been shown that exercise training contributes to an increase in cardiorespiratory fitness with a lower heart rate and blood pressure at comparable workloads. It improves peripheral adaptation, HDL/LDL-cholesterol balance and enhances the threshold for angina pectoris. Beneficial effects on fibrinolysis, carbohydrate metabolism, blood viscosity, weight reduction, mental health and the resumption of work have been reported.
Recent studies have brought new insights: leisure time physical activity may affect the natural history of the atherosclerotic lesions through an effect on endothelial dysfunction [330]. Exercise training affects the production of free radicals, protecting trained patients from the workload-induced oxidative stress [331]. It improves insulin sensitivity and metabolism and it reduces plasma homocysteine levels [332, 333]. Physical activity may aid in the reduction of the metabolically active intra-abdominal fat even before weight loss is evident. A physically active lifestyle may modify the sympathovagal balance towards a parasympathetic dominance resulting in protection against malignant arrhythmias and less myocardial wall stress. Heart rate variability (HRV) reflects this balance, which may be disturbed in patients with CVD. Exercise training, supervised or at home may restore this imbalance [334, 335].
Physical inactivity is common in patients with congestive heart failure. Over the past decade several studies have shown the benefit of improving physical fitness in patients with mild to moderate CHF [336]. Evidence suggests that the rate of congestive heart failure progression, morbidity and mortality can be attenuated via exercise training [337]. The role of physical inactivity in patients suffering from other common cardiac conditions such as atrial fibrillation and valvular disease is less well established.
9.1.5 Physical activity in the elderly
Approximately one quarter of the population above 65 years suffer from CVD. This age group accounts for two thirds of all acute myocardial infarctions and half of all coronary interventions. Within the next 50 years it is expected that the number of individuals 65 years and older will double in the Western society.
Several physiological changes that occur in the elderly may lead to physical inactivity. They include a decrease in maximum heart rate, stroke volume, cardiac output and down-grading of β-adrenergic receptors, leading to a lower aerobic work capacity. Peripheral changes contribute: a decrease in muscular strength and co-ordination, peripheral O2-uptake, mineral skeletal content and lung function. Comorbid conditions, for example, arthrosis, hypertension and diabetes mellitus, may further deteriorate physical capacity. With increasing age, larger parts of the activities of daily life demand a workload on submaximum or maximum level.
Regular physical activity will counteract or effectively slow down the age-related changes, thereby improving physical functioning and extending disease-free survival. Thus, preventive cardiology will have to play a major role in the elderly, promoting a healthy lifestyle with special focus on daily physical activity.
9.2 Estimating physical activity
For an assessment of physical activity three different methods may be used: (i) criterion methods, for example, doubly labeled water, indirect calorimetry or direct observation, (ii) objective methods, for example, activity monitors (pedometers, accelerometers) or heart rate monitors, (iii) subjective methods such as questionnaires or activity diaries [338]. For physical fitness and exercise capacity maximal incremental exercise testing is used.
9.2.1 Assessment in children and adolescents
The assessment of physical fitness in the general population of young people remains the responsibility of school health facilities and primary care physicians. Accurate assessment is necessary to identify current levels of activity and to demonstrate the effectiveness of programmes provided to increase physical activity. Recently, devices such as heart rate monitors, pedometers and accelerometers have become increasingly popular as measurement tools, although they may not be able to register all physical activity. These tools yield relatively high correlations using oxygen consumption or direct observation as criterion measures (r = 0.62-0.93 and 0.80-0.97, respectively) [339]. Surveys and recall instruments must be used cautiously in a paediatric population that has difficulty recalling such information. Further investigation is needed to improve accuracy of the available methods.
In high-risk individuals, for example children with hereditary dyslipidemia or with a high CVD burden in the family and children suffering from diabetes mellitus, a formal assessment using standard exercise testing may be used in order to provide a starting point for lifestyle counselling.
9.2.2 Assessment in adults without CVD
In the prevention of CVD in clinical practice the assessment of physical activity and fitness should be combined with a total risk assessment according to the SCORE/HeartScore method.
In low-risk individuals (>5% CVD mortality within 10 years and without previous CVD, diabetes mellitus or markedly elevated single risk factors), a brief interview concerning the person's physical activity at work and leisure gives the basis for assessing his or her general level of fitness and the need to give advice for an increase in physical exercise. There are several self-reported recall questionnaires available. Even diaries for noting daily physical activity may be useful.
In high-risk persons (≥ 5% CVD 10-year mortality risk at present age or extrapolated to the age of 60, diabetes mellitus or markedly elevated blood pressure and/or blood lipid levels) this may be completed with an exercise test using a bicycle ergometer or treadmill for diagnostic purposes and in order to obtain an objective estimate of the exercise capacity of the individual. Guidelines for exercise testing in healthy individuals and in patients with symptoms suggestive of CVD have been issued by the European Society of Cardiology Working Group on Exercise Physiology, Physiopathology and Electrocardiography [340] and more recently by the American Heart Association [341].
9.2.3 Assessment in adults with CVD
The medical and social history of CVD patients usually needs supplementary objective assessment using exercise testing procedures in order to detect myocardial ischaemia, to stratify for risk of a further major ischaemic event, to select for coronary arteriography and to assess the impact of revascularization or the response to antianginal medication.
Recently, guidelines for exercise testing in patients with congestive heart failure have been issued by a study group from the ESC Working Groups on Heart Failure and on Cardiac Rehabilitation & Exercise Physiology [342].
9.2.4 Assessment in the elderly
As in the younger age groups the patient interview remains the basis for assessing physical activity. In the elderly the specific problems of deteriorating physical capacity, especially regarding the activities of daily living and the need of social support, should be addressed.
Exercise testing on a bicycle ergometer or treadmill may be needed in persons with symptoms of CVD. Less resource demanding methods as the 6-min Walk Test or the Shuttle Walk Test may also provide valuable information on the physical capacity of the elderly. Recommendations for physical activity are summarized in Table 7.
9.3 Management of physical activity
Practice point: All individuals should be professionally encouraged and supported to increase their physical activity to the level associated with the lowest risk of CVD. Although the goal is at least half an hour of physical activity on most days of the week, almost any increase in activity is associated with a variety of health benefits – a very encouraging message!
Recommendations for physical activities
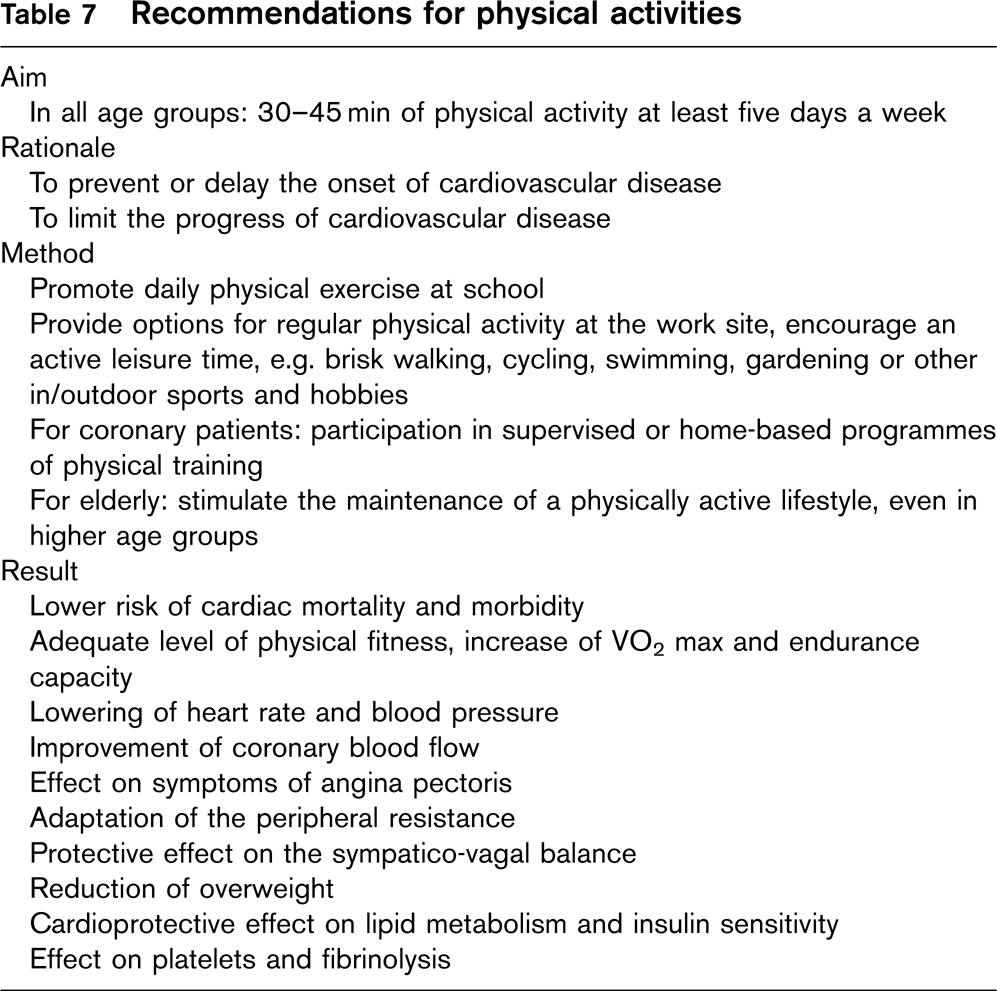
Healthy people should be recommended to choose enjoyable activities which fit into their daily routine, preferably for 30-45 min, 4-5 times weekly at a 60-75% of the age-adapted maximum heart rate. For patients with established CVD and for those with a high CVD 10-year mortality risk, advice must be based on a comprehensive clinical judgement, including the results of an exercise test.
In addition to improving aerobic fitness, physical activities that facilitate endurance, strength, balance and flexibility should be encouraged.
9.3.1 How to improve physical activity in children and adolescents
One of the main aims of preventive cardiology is to lessen the burden of CVD throughout Europe, thus creating a strong argument for physical fitness in young age. Physical activity in young age is a major predictor of maintained fitness throughout life.
In the general young population the promotion of physical fitness is the shared responsibility of parents, school staff, healthcare providers, politicians and society as a whole, which should be translated into tangible action. Each child in Europe should have access to periods of physical activity each day, be it in school or during leisure time. Physical education should be upgraded in the curriculum of the schools. Special efforts should be made to ensure that adolescents maintain a physically active lifestyle, using the available resources in society such as sport clubs, gymnasia, swimming pools and the like.
In predisposed individuals the simple and effective measures for prevention include regular physical exercise, maintenance of ideal body weight, avoidance of smoking, eating a balanced diet and early periodic monitoring of blood pressure, lipids and blood sugar. The family doctor may play a supportive role in the advice and follow-up of the young patient at high risk for future CVD.
As well as promoting physical activity, research needs to be intensified, especially in finding instruments for measuring physical fitness and activity and in validating programmes dedicated to improve physical activity in the younger age groups.
9.3.2 How to promote physical activity in adults without CVD
Interventions promoting physical activity among the general public are more likely to be effective if they involve activities which can fit into an individual's daily routine than if they require attendance at exercise facilities [343]. The physician can help by discussing activities that the person may positively enjoy. The choice of lifestyle, including maintained physical fitness, remains the sole responsibility of the individual person. This choice may be supported by family and friends, her or his work environment, access to attractive and affordable leisure time activities and by health promoting campaigns. The employer will benefit from physically fit workers as this will diminish the loss of labour due to sick leave. Thus, it should be recommended to support regular physical exercise within the resources of the work place, as is being provided in several European countries. The ultimate goal should be at least half an hour of physical activity on most days of the week.
A most encouraging recent trend is the observation that almost any increase in activity is associated with measurable health benefits, even before a training effect is manifest, and before any change in weight is evident. Thus, simple and practicable changes such as using the stairs at work or choosing public transportation instead of taking the car can be useful. This information can have a powerful motivating effect. For a training effect, professional advice about the intensity, duration and frequency of exercise may be helpful. Using goal-setting and self-regulation techniques, a study of sedentary older individuals with a high risk for CVD found significantly increased physical fitness at 12 months follow-up compared to a structured exercise program [288]. Additional studies have supported this finding [344, 289, 345]. Current public health recommendations for physical activity include 30 min of moderate intensity activity on most days of the week which will provide a broad range of benefits, especially for a sedentary population. A weekly energy expenditure of at least 1000 kcal (4200 kJ) will be needed.
The intensity may be defined in terms of target heart rate during peak exercise, 60-75% of the average maximum heart rate being the preferred target heart rate. Alternatively, as not all persons are used to monitoring heart rates, the Borg scale of perceived exertion may be applied, using the level of ‘moderate exertion’ as a guide level. This level is easily achieved by exercises involving the large muscle groups, such as brisk walking or jogging, cycling, swimming, aerobic dancing, tennis, golf or crosscountry skiing.
The recommended level of energy expenditure may be insufficient to prevent unhealthful weight gain in some people and should therefore in some cases be increased up to 60 min daily and combined with caloric restrictions.
The duration of physical activity should preferably be 30-45 min, including a 5-10 min warm-up phase, an aerobic phase of 20-30 min and a 5-10 min cool-down phase at its end. The activity can be performed in shorter bouts but they should last at least 10 min. Should the physician in prescribing physical activity wish to choose between moderate or vigorous intensity aerobic exercises, yet keeping the total energy expenditure constant, greater cardioprotective benefits may be obtained from the more vigorous activities [346].
Recently, the ESC Study Group of Sports Cardiology has issued recommendations for participation in leisure-time physical activity and competitive sports for persons at different risk levels for CVD and for patients with ischaemic heart disease [347]. In summary, for persons at low risk according to the SCORE algorithm no restrictions are recommended when participating in leisure-time physical activity or competitive sports. For healthy persons at high risk but with a normal exercise test the same advice applies provided adequate risk management (lifestyle counselling and drug treatment if needed) is given by the physician.
9.4 The use of exercise training in adults with CVD
Recommendations for patients with clinically established CVD have to be based on a comprehensive clinical judgement including the results of exercise testing. Patients with unstable angina pectoris should be attended to with conventional noninvasive or invasive methods before they may be included in physical training. Patients with stable angina pectoris often obtain marked subjective benefit from gradually increased and regular exercise, but their antianginal and other medical treatment should be optimal before starting such a programme. The intensity and duration should initially be set low and increased step-wise according to the limits imposed by exercise-induced symptoms. Here, the result of pretraining exercise testing will be valuable.
Patients recovering from an acute myocardial infarction or other ischaemic event and, similarly, patients following angioplasty or recovering from coronary artery bypass grafting should be recommended to start a suitable, increasing physical activity programme. Many patients will benefit from an organized rehabilitation programme provided by a multidisciplinary team. Such a programme may be available on an ambulatory basis or as an in-patient facility in specialized centres, as is the tradition in some central European countries. The rehabilitation programmes, in addition to supervised physical exercise, give a good opportunity for a comprehensive evaluation of the patient's risk factor status and for further advice and measures aimed at risk reduction.
If patients prefer to undertake their physical training programme at home, they will need clear prescriptions, encouragement and regular follow-up by their physician. Written material, audiocasettes, videos or CD-ROM disks are useful supplements to verbal advice. Devices such as heart rate monitors or pedometers maybe helpful in the follow-up of a home-based programme for physical training.
Detailed recommendations on exercise prescription and rehabilitation for cardiac patients, as well as on counselling for recreational and vocational activities have been published by the European Society of Cardiology Working Group on Rehabilitation [348], the ESC Study Group of Sports Cardiology [347], the American Association of Cardiovascular & Pulmonary Rehabilitation [349] and other experts in this field [350–352].
For patients with mild to moderate heart failure guidelines are available, issued by the ESC Working Groups on Heart Failure and on Cardiac Rehabilitation & Exercise Physiology [342]. Different forms of aerobic training have shown beneficial effects on exercise capacity, the need for rehospitalization and on quality of life, but there are as yet no data on mortality. Although there is no consensus on the optimal training regimen in CHF both dynamic interval training with moderate intensity and resistance training may be advantageous.
9.5 Promoting physical fitness in the elderly
General public health measures regarding the promotion of physical fitness apply to the elderly population as they do to younger generations. With the growing number of senior citizens these measures will have a major impact on healthcare resources. In several European countries gymnastic classes for elderly are being organized. Sports clubs, patient organizations and other commercial and noncommercial institutions provide a growing diversity of physical exercise facilities. Yet, further initiatives are recommended, especially for the large group of sedentary elderly women.
When counselling elderly persons the family doctor is recommended to assess activity regularly and advise to maintain daily physical activity on a moderate to submaximum level. The physician should be aware of the risk/benefit ratio when prescribing exercise. Low-intensity and longer duration exercise should be preferred over high intensity, short duration. Brisk walking at a pace at which a conversation still can be held (walk and talk model) is a good example of advise for the healthy elderly and carries a low risk/benefit ratio. The key-elements of activity programmes for the elderly are: a combination of endurance, strength, balance and flexibility training. Principles of behavioural change including social support, self-efficacy and positive reinforcement should be applied and programmes should start off at low intensity but gradually increase to moderate levels [353].
Older patients with signs of CVD will benefit from comprehensive rehabilitation programmes: exercise training is safe and improves strength, aerobic fitness, endurance and physical function. It will improve conventional risk factors, mental state and quality of life [354]. There are no gender differences in the outcome of training for elderly CVD patients. Resistance training may be an attractive alternative; it can be used in home-training, if transport is a limiting factor for participation in ambulatory group training.
However, as in the healthy population of all ages and among patients with established CVD the ultimate goal of all physical training programmes should be the acceptance and maintenance of a lifestyle in which efforts of regular physical exercise are rewarded by the cardiovascular as well as other benefits of general physical fitness.
Cognitive behavioural counselling enhances the effect of exercise recommendations. Physicians should therefore use techniques to increase motivation and self-efficacy. Group-based cognitive-behavioural interventions should be offered if simple recommendations fail.
9.6 Heart rate
9.6.1 Scientific background
The association between elevated resting heart rate and reduced life expectancy has been demonstrated in animals as well as in humans. Levine showed the semi-logarithmic inverse relationship between heart rate and life expectancy in mammalian species; smaller animals with faster heart rates have a shorter life expectancy than larger mammals with slower heart rates [355]. Within mammalian species the average number of heart beats in a lifetime has been shown to be constant within one order of magnitude. Reduction of heart rate in cholesterol-fed monkeys, both through sinoatrial node ablation and pharmacological treatment, has been shown to reduce the progression of atherosclerosis [356, 357]. In this section, the evidence linking heart rate and cardiovascular disease in humans is reviewed and treatment recommendations presented.
9.6.2 Epidemiological studies
Many longitudinal studies have shown the association between elevated heart rate and increased risk of total and cardiovascular mortality in the general population [358–368]. The risk associated with increasing resting heart rate is both graded and strong. The association between elevated heart rate and cardiovascular incidence and mortality in women is weaker. In the majority of studies the effect on total mortality remained but the association with cardiovascular mortality was not statistically significant after adjustment for other cardiovascular risk factors [360, 364, 365]. Conversely, in men the association has been robust, with the majority of studies showing an independent association with cardiovascular mortality even after adjustment for conventional cardiovascular risk factors including systolic blood pressure [360–365]. Level of physical activity is a possible confounder of the relationship so it is important to note that physical activity or surrogate markers of this [362] have been included in the multivariate analyses in many of the studies [360, 361, 365].
Estimates of the relative risk associated with elevated heart rate range from 1.2 per increase of one standard deviation (approximately 10-12 bpm) [359, 366] to estimates of between 1.95 and 2.5 when comparing groups less than 70 bpm and greater than 70 bpm [361, 362] and 3.2 when comparing greater than 90 bpm to less than 60 bpm [363]. The relationship between sudden death and elevated heart rate has been even stronger, with relative risk of 5.2 comparing less than 60 bpm to greater than 90 bpm demonstrated in men in one large study [363]. These relationships have held in both hypertensives and nonhypertensives [360, 363, 369] and also in those with coronary artery disease [370]. Studies investigating the effect in the elderly have yielded varying results [360, 366, 371, 372].
9.6.3 Benefits of heart rate reduction
Heart rate can be reduced by physical training, avoidance of excessive use of stimulants such as caffeine or by means of drugs such as β-adrenergic blockers or If channel blockers. Beta blocking drugs have many effects other than on heart rate whereas the effect of If channel blockers is highly selective.
The benefits of exercise are accepted. Both β-blockers and If channel blockers are effective therapy for angina pectoris [373]. With regard to mortality, the only clear randomized control trial evidence for a benefit from pharmacological heart rate reduction is in coronary heart disease and congestive cardiac failure [374, 375]. The contribution of reduced heart rate to the beneficial effect of β-blockade in these patients has been investigated; some but possibly not all of the benefit of β-blockers in these patients is due to heart rate lowering [376, 377]. These results cannot be applied to healthy people. There are no trial data to indicate whether pharmacological heart rate reduction might be benefical in, for example, healthy high risk individuals.
9.6.4 Is the relationship between heart rate and CVD causal?
The epidemiological studies discussed above indicate that the association between elevated heart rate and CVD is ‘strong’ and ‘graded’ with an appropriate ‘temporal sequence'. The results are highly ‘consistent’ in men, but less so in women and the elderly. The association is ‘biologically plausible’ and although the mechanism is not certain, mechanistic theories include the anti-ischaemic and antiarrhythmic benefits of a low heart rate and the atherogenic haemodynamic effects of an elevated heart rate. There is ‘agreement across the disciplines’ including animal studies and epidemiological studies, however, as discussed, there is no trial showing benefit of treatment in the general population. Although elevated heart rate is ‘treatable’ the criteria of ‘benefit resulting from treatment’ is incompletely fulfilled, at least in the general population.
9.6.5 Heart rate in risk estimation systems
At present, resting heart rate is not included as a variable in risk estimation systems [105]. Given the clear demonstration of the relationship between elevated heart rate and development of cardiovascular disease it is probable that its inclusion would improve risk estimation. This is currently under investigation by the SCORE group [23] and if successful will provide improvement in total risk estimation through the addition of a measure which is quickly and easily obtained.
9.6.5.1 Recommendations
Given the lack of randomized controlled trials investigating whether heart rate reduction in the healthy population is beneficial in terms of primary prevention of cardiovascular disease, it would not be reasonable to recommend pharmacological reduction of heart rate in asymptomatic people with elevated resting heart rate at this time. However, prevention of elevated resting heart rate through lifestyle measures such as regular physical activity, and avoidance of psychological stressors and excess intake of caffeine can certainly be advocated, especially as many of these have been shown to be beneficial for primary prevention of CVD in their own right.
Both β-blockade and If channel blockade with ivabradine can be recommended for the symptomatic relief of angina. Beta-blockers are recommended in patients who have had a myocardial infarction and, in carefully titrated doses, in heart failure. While If channel blockade may be an attractive choice in those intolerant of β-blockade, its effects on prognosis, and therefore its independent therapeutic role, remain to be defined.
Chapter 10: Blood pressure
10.1 Blood pressure as a risk factor for CVD
Elevated blood pressure has been identified as a risk factor for coronary heart disease (CHD), heart failure, stroke, peripheral arterial disease and renal failure in both men and women in a number of epidemiological studies [378–381]. Observational evidence is also available that blood pressure levels correlate negatively with cognitive function and that hypertension is associated with an increased incidence of dementia [382]. A large compilation of observational data [381] confirms that both systolic and diastolic BP show a continuous graded independent relationship with the risk of stroke and coronary events. Data involving one million individuals have indicated that death from both CHD and stroke increases progressively and linearly from BP levels as low as 115 mmHg systolic and 75 mmHg diastolic upward [383]. Increased risks are present in all age groups ranging from 40 to 89 years old. For every 20 mmHg systolic or 10 mmHg diastolic increase in BP, there is a doubling of mortality from both CHD and stroke [383].
In addition, longitudinal data obtained from the Framingham Heart Study indicated that BP values in the 130139/85-89 mmHg range are associated with more than a two-fold increase in relative risk from CVD compared with those with BP levels below 120/80 mmHg [384].
The apparently simple direct relationship between increasing systolic and diastolic BP and CV risk is confounded by the fact that systolic BP rises throughout the adult age in the vast majority of populations whereas diastolic BP peaks at about age 60 in men and 70 in women, and falls gradually thereafter [385].
This observation helps to explain why a wide pulse pressure (systolic BP-diastolic BP) has been shown in some observational studies to be a better predictor of adverse CV outcomes than either systolic or diastolic BP individually [386] and to identify patients with systolic hypertension who are at particularly high risk [387]. However, in the largest meta-analysis of observational data in one million patients in 61 studies (70% of which have been conducted in Europe) [383], both systolic and diastolic BP were independently predictive of stroke and CHD mortality and more so than pulse pressure. This meta-analysis also confirmed the increasing contribution of pulse pressure after age 55.
It has also been shown that, compared to normotensive individuals, those with an elevated blood pressure are more likely to have other risk factors for CVD such as diabetes, insulin resistance and dyslipidaemia [379, 388–390] and various types and degrees of target organ damage. Because risk factors may interact positively with each other, the overall cardiovascular risk of hypertensive patients may be high even if blood pressure is only moderately raised [104, 384].
Blood pressure can be reduced either by lifestyle interventions or by drugs. Lifestyle measures should be instituted in all patients including individuals with high-normal BP and patients who require drug treatment. The purpose is to lower BP and to control other risk factors, thereby potentially reducing the occurrence of BP-related clinical conditions. In nonhypertensive individuals, including those with high-normal BP, dietary changes that lower BP have the potential to prevent hypertension and, more broadly, to reduce BP and thereby lower the risk of BP-related clinical complications. However, lifestyle measures have not been shown to prevent CV complications in hypertensive patients, and should never delay the initiation of drug treatment unnecessarily, especially in patients at higher levels of risk, or detract from adherence to drug treatment. On the other hand, even an apparently small reduction in BP, if applied to an entire population, could have an enormous beneficial impact [102]. A substantial body of evidence strongly supports the concept that multiple nutritional factors affect BP [206]. Well-established dietary modifications that lower BP are reduced salt intake, weight loss, and moderation of alcohol consumption among those who drink. Over the past decade, increased potassium intake and dietary patterns based on the DASH diet (a diet rich in fruit, vegetables, and low-fat dairy products, with a reduced content of dietary cholesterol as well as saturated and total fat) [216] have emerged as effective strategies that also lower BP. The effects of sodium reduction on BP tend to be greater in blacks, middle-aged, and older persons and in individuals with hypertension, diabetes, or chronic kidney disease. These groups tend to have a less responsive renin-angiotensin-aldosterone system [391]. The recommended adequate sodium intake has been recently reduced from 2.4 to 1.5 g/day (65 mmol/day) [392], corresponding to 3.8 g/day sodium chloride.
A substantial and largely consistent body of evidence from observational studies and clinical trials documents that body weight is directly associated with BP. In one meta-analysis, mean systolic and diastolic BP reductions associated with an average weight loss of 5.1 kg were 4.4 and 3.6 mmHg, respectively [294]. In a subgroup analysis, BP reductions were similar for nonhypertensive and hypertensive individuals but were greater in those who lost more weight. Within-trial dose-response analyses [393, 394] and prospective observational studies [395] also document that greater weight loss leads to a greater BP reduction. Modest weight loss with or without sodium reduction can prevent hypertension in overweight individuals with high-normal BP [396], and can facilitate medication step-down and drug withdrawal [397, 398].
Several predominantly small clinical trials and meta-analyses of these trials [399–401] have documented that high-dose ω-3 polyunsaturated fatty acid (commonly called fish oil) supplements can lower BP in hypertensive individuals with BP reductions occurring at relatively high doses (≥ 3 g/day). In hypertensive individuals, average systolic and diastolic BP reductions were 4.0 and 2.5 mmHg, respectively [401].
Overall, data are insufficient to recommend an increased intake of fibre alone [402], supplemental calcium or magnesium [403, 404] as means to lower BP. Additional research is warranted before specific recommendations can be made about the amount and type of carbohydrate [405, 406] to affect BP.
Epidemiological studies suggest an inverse relationship between habitual physical activity and BP. Higher levels of physical activity and greater fitness are associated with a reduced incidence of hypertension [407]. A meta-analysis of controlled interventional trials concluded that adequate dynamic physical training contributes usefully to blood pressure control. In normotensive individuals, the training-induced decrease in BP averaged 2.6/1.8 mmHg, and in hypertensive individuals, 7.4/5.8 mmHg [408, 409]. The BP-lowering effects of exercise are most pronounced in hypertensive individuals engaging in endurance exercise with BP decreasing approximately 5-7 mmHg after an isolated exercise session (acute) or following exercise training (chronic). Moreover, BP is reduced for up to 22 h after an endurance exercise bout, with the greatest decreases among those with the highest baseline BP. In a recent meta-analysis of randomized controlled trials, resistance training at moderate intensity was found to decrease BP by 3.5/3.2 mmHg [410]. For hypertensive individuals, an exercise program that is primarily aerobic-based with adjunctive resistance training is recommended [407]. The evidence is limited regarding frequency, intensity, and time recommendations; the antihypertensive effect appears to occur at relatively low duration and intensity.
Systolic BP during bicycle exercise (no systematic studies using a treadmill are available) has been proposed as a more sensitive indicator of CV risk and risk of developing hypertension [411]. A rise in exercise systolic BP to >200 mmHg during the first 6 min of bicycle exercise predicts a doubling of CVD incidence in middle-aged men [412]. If the exercise-induced rise in cardiac output is impaired in hypertensive individuals, exercise BP no longer carries an independent prognostic power [413].
Smoking causes an acute increase in BP, heart rate, and circulating catecholamines persisting for more than 15 min after smoking one cigarette. Paradoxically, several epidemiological studies have found that BP levels among cigarette smokers were the same as or lower than those of nonsmokers [414, 415]. A few studies using ABPM (ambulatory blood pressure monitoring) have shown that both untreated hypertensive and normotensive smokers present higher daytime BP than nonsmokers [416–419]. Although any independent chronic effect of smoking on BP is small [420] and smoking cessation does not lower BP [421], total cardiovascular risk is greatly increased by smoking [422]. Patients should be strongly counselled to quit smoking to reduce overall CV risk.
Combinations of two or more lifestyle modifications can achieve better results [215].
It should be emphasized that the size of all lifestyle intervention trials has been too small and their duration too short to provide evidence of the effect of lifestyle changes on cardiovascular morbidity and mortality. Furthermore, adherence to lifestyle changes out of the context of controlled trials has been shown to be poor, particularly with regard to weight loss whose maintenance represents a universal problem in the long-term [423]. However, the TOHP study [396] has shown that even when body weight is regained, blood pressure may remain lower than in the control group. This finding suggests that some degree of weight loss, even if not sustained beyond 6 months, confers benefit [394]. Also, in responsive and compliant individuals, lifestyle changes may (i) decrease the number and doses of antihypertensive drugs necessary to control blood pressure, (ii) make it unnecessary to restart medication after effective drug treatment has been stopped, and (iii) reduce the overall cardiovascular risk profile. This makes this approach mandatory under all circumstances.
Large-scale randomized controlled trials performed mostly in Caucasian populations have conclusively demonstrated that, in hypertensive individuals a blood pressure reduction by antihypertensive drugs substantially reduces cardiovascular morbidity and mortality [424–428]. It should be noted that most of the hypertension trials involved patients over 55 years of age with overt vascular disease and that there is an alarming absence of data in younger (>55 years old) individuals [429].
The trials have also provided evidence that the benefit:
Occurs in both men and women [430];
Extends at least to individuals up to 80 years of age [424, 426, 431, 432, 433]; and
Includes all major conditions for which hypertension is a risk factor, for example, stroke, coronary heart disease, congestive heart failure, progressive renal damage and insufficiency and, possibly, also cognitive dysfunction and dementia [434–438]. However, the evidence of the favourable effect of antihypertensive treatment on cognitive dysfunction and dementia is not so strong. The vascular dementia project performed as part of the Syst-Eur trial showed that antihypertensive treatment in elderly people with isolated systolic hypertension was associated with a lower incidence of dementia [438]. Other trials were either negative [437, 439] or difficult to interpret [440, 441].
Evidence from placebo-controlled and comparative trials also makes it clear that cardiovascular protection can be obtained by treatments based on a variety of antihypertensive drug classes, that is, diuretics, β-blockers, ACE inhibitors, calcium antagonists and angiotensin II antagonists. This presumably means that the protection is due, to a substantial degree, to blood pressure lowering per se [4].
The benefit of β-blockers compared with that of other antihypertensive agents has recently been questioned on the basis of the results of two large randomized trials, the LIFE study [442] and the ASCOT study [443], both of which showed superiority of an angiotensin receptor antagonist and a calcium antagonist, respectively, over therapy initiated by a β-blocker as far as stroke (LIFE) or stroke and mortality (ASCOT) were concerned. These two large trials have strongly influenced a recent meta-analysis [444], which concluded that β-blocker-initiated therapy is inferior to others in stroke prevention, but not in prevention of myocardial infarction and reduction in mortality. On the basis of a similar meta-analysis, NICE in the United Kingdom has advised to use β-blockers only as fourth-line antihypertensive agents [429]. These conclusions must be considered with critical caution. Both the LIFE and the ASCOT studies were characterized by a design that led to early use of combination therapy, so that the vast majority of the patients randomized to a β-blocker-based therapy actually received a β-blocker-thiazide combination. A recent meta-analysis shows that, when compared to placebo, β-blocker-based therapy did indeed reduce stroke significantly [445]. Part of the β-blocker-thiazide combination reported in ASCOT may be due to a smaller reduction of blood pressure [443], particularly of central blood pressure [446] that occurred in this trial with this therapeutic regimen.
β-Blocker-thiazide combinations have nevertheless been consistently associated with metabolic disturbance and new-onset diabetes and may have specific contraindications in patients prone to diabetes. In any case, the above meta-analyses of β-blocker-initiated trials [444, 445] well illustrate the difficulties inherent in many recent trials in which combination therapy hinders the attribution of either benefits or harms to individual compounds.
Following a myocardial infarction, BP elevation is associated with an increased risk of reinfarction and death [447–449]. No randomized controlled trial evidence is available on the effect of BP lowering per se under these circumstances. However, use of β-blockers, ACE inhibitors and nondihydropyridine calcium antagonists immediately after an acute myocardial infarction has resulted in a secondary cardioprotective effect together with a modest BP reduction [450–452]. This has been seen both in individuals with elevated and normal BP. Furthermore, antihypertensive treatment by several drug classes has been found to prevent cardiovascular disease in normotensive and hypertensive patients with a more distant history of myocardial infarction [453]. Finally, recent trials have demonstrated that clinically stable normotensive and hypertensive patients with a history of cerebrovascular disease show a marked decrease in their otherwise elevated incidence of stroke recurrence if blood pressure is reduced by ACE inhibitors in combination with diuretics [454], with a concomitant decrease in the incidence of myocardial infarction. This suggests use of antihypertensive drugs for secondary coronary and cerebrovascular prevention, even when blood pressure is not elevated. Treatment should be given according to guidelines for primary prevention but BP should be lowered slowly and carefully because tissue necrosis, atherosclerotic plaques and cardiac hypertrophy may make coronary and cerebral blood pressure flow auto-regulation less effective in preserving organ perfusion when perfusion pressure is reduced [455, 456]. In addition, the HOPE study [457] suggested that treatment of high risk people with an ACE inhibitor may have benefits beyond blood pressure control.
Long-term observational data [458] provide evidence that, in hypertensive patients in whom treatment effectively controls BP, coronary, cerebrovascular and overall CV morbidity remains higher than that of normotensive controls. This may be accounted for by factors such as irreversible organ damage at the time treatment is started pointing to the need for earlier identification and correction of blood pressure elevation. Research efforts, however, currently also focus on the possibility that greater cardiovascular protection may be achieved by (i) antihypertensive drugs with direct organ protective properties that might complement the protection due to the blood pressure reduction [453], (ii) multiple drug treatments that more comprehensively address the overall cardiovascular risk profile, and (iii) more aggressive blood pressure reductions below 140/90 mmHg. To date, trial evidence that for a given BP reduction some antihypertensive agents are more protective than others is limited to the greater nephroprotective effects of drugs primarily acting on the renin-angiotensin system (ACE inhibitors and angiotensin II antagonists) [459–461] because, with few exceptions [442, 462], comparisons between drugs have not shown differences in primary cardiovascular end points and no substantial advantage of one class over another had emerged from their meta-analysis [463, 464]. Similar results were obtained in a recent meta-analysis performed by the same collaborative group in patients with and without diabetes showing a comparable reduction of total major CV events [465]. Another meta-analysis comparing the effects of ACE inhibitors and angiotensin II antagonists with other antihypertensive drugs yielded a relative risk of 0.71 for doubling of creatinine (95% CI of 0.49-1.04) and a small benefit on end-stage renal disease (relative risk, 0.87; 0.75-0.99). In patients with diabetes, additional renoprotective action of the substances beyond lowering blood pressure remains unproven [466].
Several large-scale studies have shown statins to be very effective in primary and secondary prevention and also in patients with hypertension and antihypertensive treatment [63, 467]. Two trials – ALLHAT [468] and ASCOT [469] – have evaluated the benefits associated with the use of statins, specifically in patients with hypertension. ALLHATcompared the effect of 40 mg/day pravastatin with usual care in over 10 000 patients, 14% of whom had established vascular disease. The differential effect of pravastatin on total and LDL-cholesterol (11 and 17%, respectively) was smaller than expected due to extensive statin use in the usual care group and was associated with a modest, nonsignificant 9% reduction in fatal CHD and nonfatal myocardial infarction, and a 9% reduction in fatal and nonfatal stroke. There was no impact on all-cause mortality, which was the primary end point of the trial. By contrast, the results of ASCOT, which also included over 10 000 hypertensive patients, showed a 36% reduction in the primary end point of total CHD and nonfatal myocardial infarction, and a 27% reduction in fatal and nonfatal stroke associated with the use of atorvastatin 10 mg/day compared with placebo in patients with total cholesterol less than 6.5 mmol/l [469]. Based on ASCOT data, well controlled high risk hypertensive individuals may receive a modest additional benefit from the use of a statin.
Evidence has been obtained, on the other hand, that in hypertensive patients in whom treatment provides an adequate blood pressure control, the addition of acetylsalicylic acid (ASA) at a low daily dose (75 mg) further decreases (−35%) the incidence of myocardial infarction [470], the benefit being particularly evident in males [471] and in the subgroup with renal damage [472]. However, an increase in rates of nonfatal major bleeds was also shown and therefore, ASA should not be recommended in hypertension with low total CV risk and poor BP control.
There is also evidence that in patients with type 2 diabetes mellitus or with diabetic nephropathy, aiming at blood pressure values well below the traditional ones is associated with a lower incidence of cardiovascular and renal events, respectively [473–475]. The latter is the case particularly in the presence of marked proteinuria. Furthermore, in diabetic and nephropathic [476, 477] patients on-treatment blood pressure values less than 130/80 mmHg or lower (>125/75 mmHg in patients with proteinuria >1 g/24 h) should be achieved using all available drugs with evidence of antihypertensive efficacy and safety [478, 479].
10.2 Blood pressure measurements
The large physiological variations in blood pressure [480] mean that, to diagnose hypertension, blood pressure should be measured in each individual several times on several separate occasions. If systolic and/or diastolic blood pressure is only slightly elevated, repeated measurements should be made over a period of several months to achieve an acceptable definition of the individual's ‘usual’ blood pressure and to decide about initiating drug treatment. If systolic and/or diastolic blood pressure is more markedly elevated, repeated blood pressure measurements are required within a shorter period of time (weeks or days) in order to make treatment decisions. This is also the case if the blood pressure elevation is accompanied by evidence of endorgan damage, associated clinical conditions, and/or by the concomitance of other cardiovascular risk factors that markedly increase overall cardiovascular risk. Repeated blood pressure measurements on several occasions are necessary to identify the relatively large number of persons in whom blood pressure elevation disappears following the first few visits. These individuals may need blood pressure measurements more frequently than the general population but drug treatment does not appear to be necessary because their cardiovascular risk is probably low [481].
10.2.1 Office or clinic BP measurement
In general, the diagnosis of hypertension should be confirmed during at least two to three visits, with a minimum of two BP readings taken per visit. Blood pressure measurement is carried out in the sitting position from the right or the left arm, after the patient has rested for 5 min. At the initial visit, blood pressure values from both arms should be obtained to detect patients in whom atherosclerotic plaques in subclavian or more central arteries may be responsible for substantial between-arm discrepancies. Under this circumstance the arm with the higher values should be selected. In elderly hypertensive individuals and in diabetic patients, it is also important to measure blood pressure in the standing position to detect possible orthostatic hypotension.
The use of a conventional sphygmomanometer with an appropriate bladder size has been considered the gold standard for clinical measurement of blood pressure. The reading of diastolic blood pressure should be taken at the disappearance of the sound (phase V) and blood pressure levels should be read to the nearest 2 mmHg. At least two measurements have to be made on each visit. Because medical use of mercury has been banned in some European countries, performance of nonmercury blood pressure measuring devices is becoming increasingly important. These devices should be properly tested and validated according to standardized protocols [482], as mentioned in the guidelines on blood pressure measurements of the European Society of Hypertension [483]. Currently available devices measuring blood pressure in the fingers or on the wrist should be avoided because of possible inaccuracy [484].
Blood pressure measurements during exercise or laboratory stressors have been proposed as more sensitive indicators of blood pressure elevation and increased cardiovascular risk, but their clinical superiority over conventional blood pressure has never been conclusively proved and their use cannot be routinely recommended.
10.2.2 Ambulatory BP monitoring
ABPM provides information about BP during daily activities and sleep. Blood pressure has a reproducible circadian profile with higher values while awake and mentally and physically active, with much lower values during rest and sleep, and early morning increases for 3 or more hours during the transition from sleep to wakeful-ness. Several devices (mostly oscillometric) are available. However, only devices validated by international standardized protocols should be used. Automatic and semiautomatic BP monitoring does not induce an alarm reaction to a BP rise and thus does not overestimate daytime BP values [485]. Ambulatory BP monitoring is usually several mmHg lower than office BP. In population studies, office values of 140/90 mmHg correspond approximately to 24-h average values of 125-130/80 mmHg. Mean daytime (130-135/80 mmHg) and nighttime (120/70 mmHg) values are several times mmHg higher and lower, respectively, than the 24-h mean and are markedly influenced by activities during day or night. These values may be regarded as approximate threshold values for diagnosing hypertension by ABPM. Clinical decisions may be based on 24-h, daytime or nighttime values but, preferably, on 24-h mean. Virtually all national and international guidelines for the diagnosis and treatment of hypertension at least mention 24-h ABPM, noting its superiority over the office BP in diagnosing hypertension. Several studies in hypertensive individuals have documented that 24-h ABPM was a better predictor of CV events than office BP [486–491]. There are only three studies in the general population showing the superiority of ABPM over office BP in predicting CV mortality [492–495].
Long-term follow-up of the PAMELA population sample provided evidence that office, home and ambulatory BP values are predictive of the risk of cardiovascular and all-cause deaths, with superiority of systolic over diastolic BP and of nighttime over daytime values. It may be desirable to include 24-h ABPM into the diagnostic algorithm of all national and international guidelines for hypertension management [496–498].
10.2.3 Home BP measurement
Self-measurement of BP at home cannot provide extensive information on 24-h BP values provided by ABPM. However, it can provide values on different days in a setting close to daily life conditions. When averaged over a period of a few days, these values have been shown to share some of the advantages of ABPM, that is, to have no white-coat effect and to be more reproducible and predictive of the presence and progression of organ damage than office values [499, 500]. Home BP measurements for suitable periods (e.g. a few weeks) before and during treatment can therefore be recommended also because this relatively simple and inexpensive procedure may improve patient's adherence to treatment regimens [501]. Home monitoring devices should be checked for accuracy every 1-2 years.
One factor that has delayed a wider use of home or self-monitoring in clinical practice has been the lack of prognostic data. Two prospective studies [502–505] have found that home BP predicts morbid events better than conventional clinical measurements. Home BP readings within the range 130-135/85 mmHg correspond approximately to 140/90 mmHg measured in the office or clinic.
10.3 Isolated office or white-coat hypertension
In some patients, office BP is persistently elevated while daytime or 24-h BP falls to within the normal range. This condition is widely known as ‘white-coat hypertension’ [506], although the more descriptive and less mechanistic term ‘isolated office (or clinic) hypertension’ is preferable because the office-ambulatory BP difference does not correlate with the office BP elevation induced by the alerting response to the doctor or the nurse, that is, the true ‘white-coat effect’ [507]. Regardless of the terminology, evidence is now available that isolated office hypertension is not infrequent (about 15% in the general population) [508] and that it may account for a noticeable fraction of individuals in whom hypertension is diagnosed [494, 497, 509]. There is also evidence that, in individuals with isolated office hypertension, CV risk is less than in individuals with both office and ambulatory BP elevations [508]. Sustained hypertension may develop in some patients with white-coat hypertension, and the risk of stroke may increase [510]. Several, although not all studies, however, have reported this condition to be associated with a prevalence of organ damage and metabolic abnormalities greater than that of normal individuals, which suggests that it may not be an entirely innocent phenomenon [497]. This was also confirmed more recently by the PAMELA study showing an increase in both CV and all-cause mortality in white-coat hypertensive individuals [511].
Physicians should diagnose isolated office hypertension whenever office BP is ≥ 140/90 mmHg at several visits while 24-h and day ambulatory BP are less than 125-130/80 and 130-135/85 mmHg, respectively. Diagnosis can also be based on home BP values (average of several days’ readings >135/85 mmHg). Identification should be followed by the search for metabolic risk factors and target organ damage (TOD). Drug treatment should be instituted when there is evidence of organ damage or a high CV risk profile. Lifestyle changes and a close follow-up should, however, be implemented in all patients with isolated office hypertension in whom the doctor elects not to start pharmacological treatment.
10.4 Masked hypertension or isolated ambulatory hypertension or ‘reversed white-coat’ condition
Normal BP in the office and elevated blood pressures elsewhere (e.g. at work or at home) is called masked hypertension or isolated ambulatory hypertension [495, 497, 505, 512]. These individuals have been shown to display a greater than normal prevalence of TOD [497, 513] and may have a greater CV risk than truly normotensive individuals [495, 505, 511]. Alcohol, tobacco, and caffeine consumption and physical inactivity outside the office/clinic may contribute to this phenomenon. The prevalence of masked hypertension in treated hypertensive individuals is about 10% [514] and is somewhat greater in the general population [515]; in the PAMELA study 1 in seven to eight normotensive patients had it [497]. The clinic BP of patients with masked hypertension may underestimate the risk of CV events. A study of patients with treated hypertension showed about one third of those seen in a hypertension clinic had masked hypertension over a 5-year follow-up period, and their relative risk of CV events was 2.28 as compared with patients whose BP was adequately controlled according to the criteria for both clinic BP and ambulatory BP [516]. Other studies have shown masked hypertension in patients with untreated hypertension and often in those with undiagnosed hypertension, it is associated with an increased rate of TOD [513] and adverse prognosis [517]. Masked hypertension may be suspected on the basis of high BP readings taken at home, and one study has shown that masked hypertension diagnosed solely on the basis of home recordings is associated with increased mortality [505].
In patients with an acute myocardial infarction who have been treated for hypertension before their infarction, blood pressure may remain at much lower levels, or even return to normotensive values, for months or years without continuing antihypertensive treatment [518]. This observation preceded the widespread use of β-blocking drugs after myocardial infarction. In such instances, the blood pressure level has to be measured properly to detect whether and when hypertensive values are regained and effective antihypertensive treatment should be restarted without delay.
10.5 Control of arterial hypertension
Guidelines on the management of hypertension vary slightly in their definitions of hypertension and its subdivision into further blood pressure categories [519, 520]. As stated in the 1996 World Health Organization Expert Committee report on hypertension control [521], all definitions of hypertension are by necessity arbitrary because the risk of cardiovascular disease increases continuously with rising blood pressure. In epidemiologic studies, there is a continuous relationship with cardiovascular risk down to systolic and diastolic levels of 115-110 and 75-70 mmHg, respectively [381, 383]. The dividing line between ‘normotensive’ and ‘hypertensive’ individuals can only be determined operationally by intervention trials demonstrating at which blood pressure levels treatment is beneficial.
Definition and classification of blood pressure levels
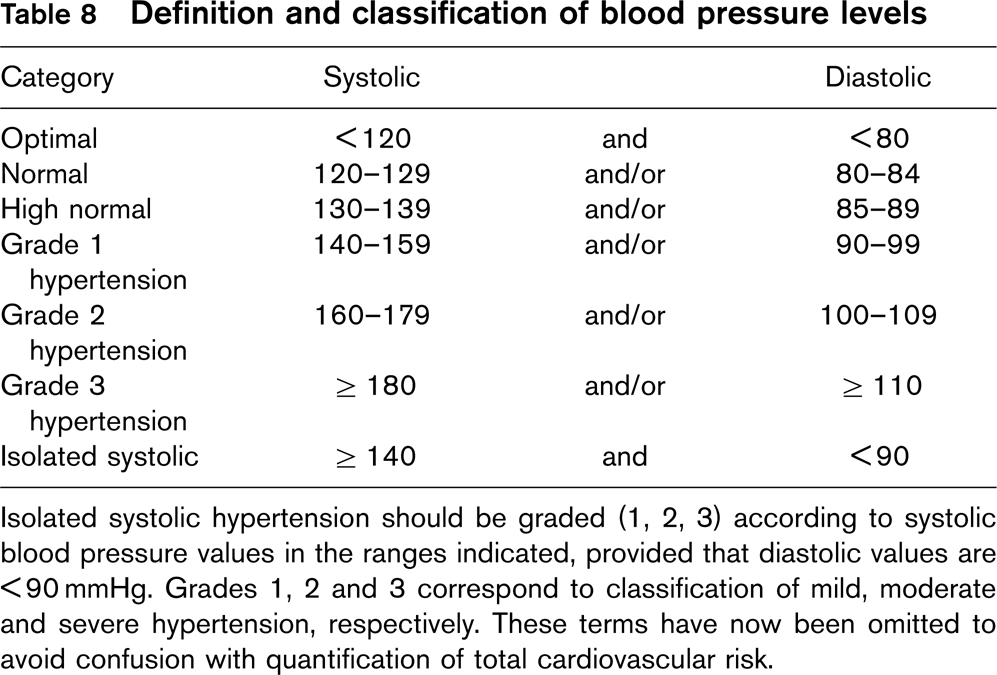
Isolated systolic hypertension should be graded (1, 2, 3) according to systolic blood pressure values in the ranges indicated, provided that diastolic values are >90 mmHg. Grades 1, 2 and 3 correspond to classification of mild, moderate and severe hypertension, respectively. These terms have now been omitted to avoid confusion with quantification of total cardiovascular risk.
The classification of hypertension used in the 2003 and 2007 ESH-ESC guidelines has been retained [4, 520] (Table 8). Isolated systolic hypertension should be graded to the same systolic blood pressure values indicated for systolic-diastolic hypertension. However, the association with a low diastolic blood pressure (e.g. 60-70 mmHg) should be regarded as an additional risk.
The decision to start pharmacological treatment, however, depends not only on the blood pressure level but also on total cardiovascular risk, which calls for a proper history, physical examination and laboratory examination to identify (i) the presence of clinically established cardiovascular or renal disease, (ii) the coexistence of other cardiovascular risk factors, and (iii) the presence of subclinical cardiovascular disease or end-organ damage. The presence of clinically established cardiovascular or renal disease (myocardial infarction, angina pectoris, heart failure, coronary revascularization, transient is-chaemic attacks, stroke, renal insufficiency or overt proteinuria, peripheral arterial disease, advanced retinopathy, etc.) dramatically increases the risk of subsequent cardiovascular events regardless of the blood pressure level. This is also the case for the association of hypertension and other cardiovascular risk factors such as diabetes (Table 9).
Owing to the importance of target organ damage as an intermediate stage in the continuum of vascular disease and as a determinant of overall cardiovascular risk, signs of organ involvement should be looked for carefully.
Factors influencing prognosis in hypertension
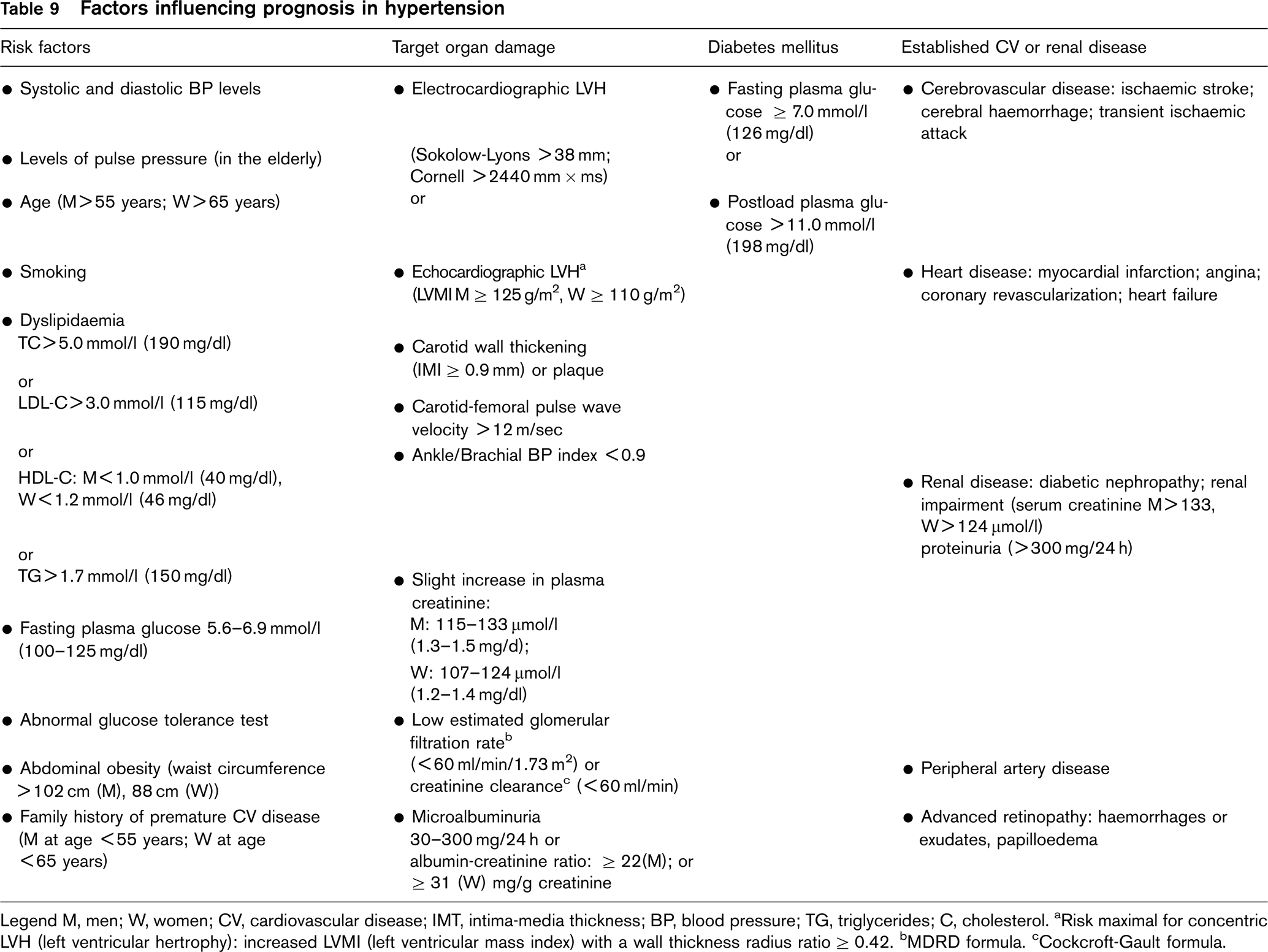
Legend M, men; W, women; CV, cardiovascular disease; IMT, intima-media thickness; BP, blood pressure; TG, triglycerides; C, cholesterol. aRisk maximal for concentric LVH (left ventricular hertrophy): increased LVMI (left ventricular mass index) with a wall thickness radius ratio ≥ 0.42. bMDRD formula. cCockcroft-Gault formula.
Electrocardiography should be part of routine assessment of hypertensive patients. Its sensitivity in detecting left ventricular hypertrophy is low, but hypertrophy detected by the Sokolow-Lyons index (SV1 + RV5-6 >38 mm) or by the Cornell voltage QRS duration product (> 2440 mm × ms) is an independent predictor of cardiovascular events [522]. Use of ECG hypertrophy as a marker of cardiac damage as well as a tool documenting LVH regression, which may also be associated with a reduced incidence of new-onset atrial fibrillation appears to be valuable, at least in patients aged more than 55 years [523].
Echocardiography is more sensitive than electrocardiography in diagnosing left ventricular hypertrophy [524] and predicting cardiovascular risk [525], and may help in more precise stratification of the overall risk and in directing therapy [390].
Carotid ultrasound with measurement of intima-media thickness (IMT) or the presence of plaques has been shown to predict both stroke and myocardial infarction [526–530]. The relationship between carotid IMT and cardiovascular events is a continuous one but for the common carotid arteries an IMT >0.9 mm can be taken as a conservative estimate of existing alterations. Ultrasound scans limited to the common carotid arteries (an infrequent site of atherosclerosis) are likely to detect vascular hypertrophy only, whereas assessment of atherosclerosis also requires scanning of bifurcations and/or internal carotids where plaques are more frequent. Presence of a plaque can be identified by an IMT >1.3 or 1.5 mm or by a focal increase in thickness by 0.5 mm or by 50% of the surrounding IMT value [531, 532]. There is evidence that, in untreated hypertensive individuals without target organ damage at routine examinations, these alterations are common and, thus, carotid ultrasound may often detect vascular damage and make risk stratification more precise [390].
Evidence of arterial damage may also be suggested by an ankle-brachial blood pressure index less than 0.9, using a continuous wave Doppler unit and a blood pressure manometer. A low ankle-brachial index indicates advanced atherosclerosis [533, 534], whereas carotid IMT measurements are able to detect earlier changes [530]. Nevertheless, a reduced ankle-brachial index predicts further development of angina, myocardial infarction, congestive heart failure, need for coronary bypass surgery, stroke, carotid and peripheral artery surgery [535–539] and, in patients with multivessel coronary disease, it confers an additional risk [540].
A large body of evidence has been collected over the past 10 years on large artery stiffening and the wave reflection phenomenon, which have been identified as the most important pathophysiological determinants of isolated systolic hypertension and pulse pressure increases [541]. Measurement of carotid-femoral pulse wave velocity provides a comprehensive noninvasive assessment of arterial stiffness, which is simple and accurate enough to be considered for diagnostic purposes [542]. This measure has been shown to have an independent predictive value for all-cause and cardiovascular morbidity, coronary events and strokes in patients with uncomplicated essential hypertension [543–545]. Although the relationship between aortic stiffness and events is continuous, a threshold more than 12 m/s has been suggested as a conservative estimate of significant alterations of aortic function in middle-aged hypertensive individuals. Though a wider clinical use of pulse wave velocity measurement may add further precision to assessment of arterial damage, availability of the technique is largely limited to research centres.
The diagnosis of hypertension-induced renal damage is based on the finding of a reduced renal function and/or the detection of elevated urinary excretion of albumin. Renal insufficiency is now classified according to the estimated glomerular filtration rate calculated using the MDRD formula that requires age, gender, race and serum creatinine [546]. Values of estimated glomerular filtration rate below 60 ml/min/1.73 m2 indicate chronic renal disease stage 3, while values below 30 and 15 ml/min/1.73 m2 indicate chronic renal disease stages 4 and 5, respectively [547]. Another option is the Cockcroft-Gault formula estimating creatinine clearance and based on age, gender, body weight, and serum creatinine. This formula is valid in the range greater than 60 ml/min, but it overestimates creatinine clearance in chronic kidney disease stages 3-5 [548]. Both formulas help to detect mildly impaired renal function, particularly if serum creatinine values are still within the normal range [549].
While an elevated serum creatinine concentration or a low estimated glomerular filtration rate (or creatinine clearance) points to a reduced rate of glomerular filtration, an increased rate of urinary albumin or protein excretion points to a derangement in the glomerular filtration barrier. Microalbuminuria (urinary albumin excretion from 30 to 300 mg/24 h) has been shown to predict the development of overt diabetic nephropathy in both type 1 and type 2 diabetic individuals [550], while the presence of overt proteinuria (> 300 mg/24 h) generally indicates established renal parenchymatous damage [551]. In both diabetic and nondiabetic hypertensive patients, microalbuminuria, even below the currently used threshold values [552], has been shown to predict cardiovascular events [553–561], and a continuous relationship between cardiovascular, as well as noncardiovascular, mortality and urinary protein/creatinine ratios ≥ 3.9 mg/g in men and 7.5 mg/g in women has been reported in several studies [560]. Microalbuminuria can be measured from spot urine samples (24-h or nighttime urine samples are discouraged due to the inaccuracy of urinary sample collection) by indexing the urinary albumin concentration to the urinary creatinine concentration [547]. Classic dipstick tests detect albuminuria above 300 mg/g creatinine and the ‘microalbuminuric’ dipstick test above 30 mg/g creatinine. A sensitive dipstick for the lower range of low grade albuminuria is not yet available.
In conclusion, the finding of an impaired renal function in a hypertensive patient is frequent and constitutes a very potent predictor of future cardiovascular events and death even in treated patients [472, 554, 562–565]. Therefore, it is recommended that glomerular filtration rate is estimated, and the presence of urinary protein (by dipstick) sought in all hypertensive patients. In dipstick-negative patients, low grade albuminuria should also be searched for in spot urine using one of the validated commercial methods.
The coexistence of other cardiovascular risk factors (smoking, increased plasma cholesterol, family history of premature cardiovascular disease) also greatly adds to the risk associated with a mild blood pressure elevation (see SCORE risk chart) [105].
ESC guidelines (2007) [4] suggest the following tests to be performed routinely in hypertensive patients: fasting plasma glucose, serum total cholesterol, serum HDL-cholesterol, fasting serum triglycerides, serum potassium, serum uric acid, serum creatinine, estimated creatinine clearance (Cockcroft-Gault formula) or estimated glomerular filtration rate (MDRD formula), haemoglobin and haematocrit, urinalysis (complemented by micro-albuminuria dipstick test and sediment examination), and electrocardiogram, whereas echocardiography, carotid ultrasound, ankle-brachial index, fundoscopy and measurement of pulse wave velocity are listed as tests to be considered. If fasting plasma glucose is more than 5.6 mmol/l (∼ 100 mg/dl), a glucose tolerance test is recommended. Blood pressure measurement at home or 24 h ambulatory blood pressure monitoring are also part of recommended tests.
10.5.1 Who to treat?
The decision to start antihypertensive treatment depends on systolic and diastolic blood pressure, as classified in Table 8, and on total cardiovascular risk as estimated from the SCORE charts (Figs 3–6). However, in hypertensive patients, prognosis is also affected by the presence or absence of target organ damage, diabetes mellitus, and established CV or renal disease (Table 9). All patients in whom repeated blood pressure measurements show grade 2 or 3 hypertension (i.e. systolic values ≥ 160 or diastolic values ≥ 90 mmHg) are candidates for antihypertensive treatment because a large number of placebo-controlled trials have conclusively demonstrated that, in patients with these blood pressure values, blood pressure reduction lowers cardiovascular morbidity and mortality [434, 464, 566, 567]. The benefit may be modest in those at low CVD risk. Benefits of drug treatment should be weighed against side effects, cost, use of medical resources and turning healthy people into ‘patients'.
Evidence for the benefit from treating grade 1 hypertensive individuals is admittedly scanter, as specific trials have not addressed this issue. However, the recent finding of the FEVER study on the protective effect of lowering systolic blood pressure to less than 140 rather than more than 140 mmHg even in hypertensive patients at moderate risk [568] lends support to the recommendation to consider antihypertensive interventions when systolic blood pressure is ≥ 140 mmHg.
In all grade 1 to 3 hypertensive individuals, lifestyle counselling should be provided after hypertension is diagnosed, while promptness in the initiation of pharmacological therapy depends on the level of total cardiovascular risk. In the high risk hypertensive individuals enrolled into the VALUE study, the treatment arm with blood pressure control achieved later showed a trend towards more cardiovascular events [569]. Therefore, in hypertensive patients with established CV or renal disease, TOD or diabetes, the acceptable time delay to assess the results of lifestyle changes is shorter than indicated in the previous guidelines [520]. Drug treatment should be initiated promptly in grade 3 hypertension, as well as in grade 1 and 2 hypertensive individuals with high or very high total cardiovascular risk (i.e. in hypertensive patients with established CV or renal disease, target organ damage or diabetes). In grade 1 or 2 hypertensive individuals with moderate total cardiovascular risk, drug treatment may be delayed for several weeks and, in grade 1 hypertensive individuals without any other risk factor, for several months. However, even in these patients, lack of blood pressure control after a suitable period of lifestyle measures should lead to instituting drug treatment in addition to lifestyle measures. Recommendations for blood pressure management are summarized in Table 10.
When initial blood pressure is within the high normal range (130-139/85-89 mmHg), the decision on drug intervention depends heavily on total cardiovascular risk.
Management of total CVD risk – blood pressure
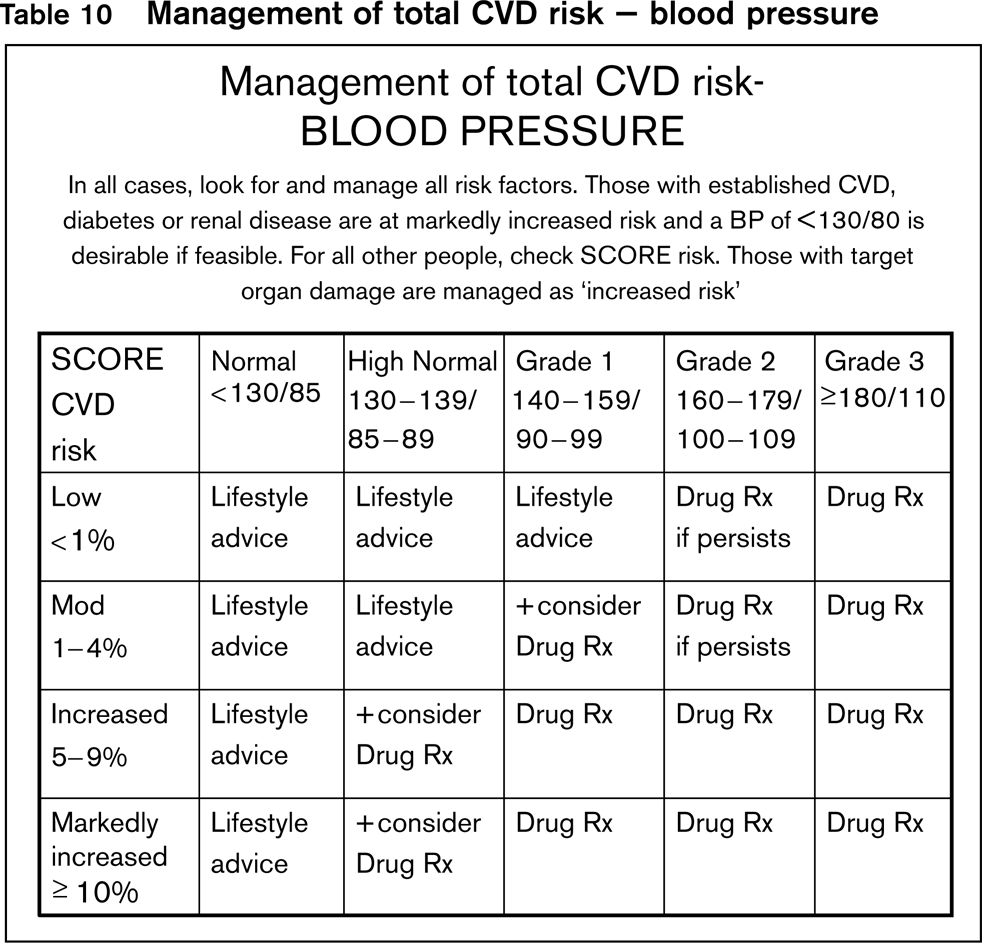
In case of diabetes or a history of cerebrovascular or coronary disease, recent randomized trials [12, 570–573] have shown that antihypertensive treatment is associated with a reduction in cardiovascular fatal and nonfatal events although no benefit of blood pressure lowering was reported in two other trials in coronary patients. A reduction of cardiovascular events was only seen when initial blood pressure was within the hypertensive range [574, 575]. Evidence is also available that, in diabetic patients with increased protein excretion, reductions in blood pressure to very low values (>125/75 mmHg) are associated with reductions in urinary albumin excretion or proteinuria as well as with a reduced rate of progression to more severe proteinuric states. This is also the case when initial blood pressure values show a borderline or zero elevation, and drugs with a direct antiproteinuric effect such as blockers of the renin-angiotensin system are used [466, 573, 576–578]. This justifies the recommendation to start antihypertensive drug administration (together with intense lifestyle changes) even in patients with blood pressure in the high normal (and sometimes normal) range, with associated cardiovascular disease or diabetes.
Whether a similar therapeutic approach (i.e. intense lifestyle changes combined with antihypertensive drug treatment) may also benefit individuals with high normal blood pressure who are at high total risk is uncertain. It should be emphasized that prospective observational studies have demonstrated that individuals with high normal blood pressure have a higher incidence of cardiovascular disease compared to individuals with normal or optimal blood pressure [381, 383, 384]. Furthermore, the risk of developing hypertension is higher in individuals with high normal than in those with normal or optimal blood pressure, with an additional increase in risk when, as often occurs, concurrent multiple risk factors and the metabolic syndrome are present [579–581]. Lifestyle measures and close blood pressure monitoring should be the recommendation for individuals with normal blood pressure who are at low or moderate risk.
10.5.2 How to treat?
Lifestyle. Several lifestyle interventions are known to have a blood pressure-lowering effect. Treatment based on these interventions alone may be sufficient for patients with mildly elevated blood pressure and, as emphasized before, it should always be advised for patients receiving antihypertensive drugs, because the dosage of antihypertensives needed for good blood pressure control can be reduced by lifestyle measures. As long-term adherence to lifestyle changes may be poor, frequent reinforcement of these recommendations in connection with blood pressure measurements is needed.
Lifestyle interventions include: weight reduction in overweight individuals; reduction in the use of sodium chloride to less than 3.8 g/day (sodium intake less than 1.5 g/day, i.e. 65 mmol/day) [582]; restriction of alcohol consumption to no more than 10-30 g/day ethanol in men (1-3 standard measures of spirits, 1-3 glasses of wine, or 1-3 bottles of beer) and to no more than 10-20 g/day ethanol in women (1-2 of these drinks/day); and regular physical activity in sedentary individuals.
Since tobacco smoking has a particularly adverse effect on the cardiovascular risk of hypertensive patients, intensive effort should be made to help hypertensive smokers to stop smoking. Where necessary, nicotine replacement [583] or bupropione therapy should be considered since they appear to facilitate smoking cessation [584]. Varenicline is a novel selective nicotinic acetylcholine receptor partial agonist developed specifically for smoking cessation, with documented short-term and long-term efficacy versus placebo [585]. Because the acute blood pressure effect of smoking may raise daytime blood pressure [419], this may also directly favour blood pressure control, at least in heavy smokers.
As the blood pressure lowering effect of increased potassium has been well documented in the DASH diet (rich in fruit, vegetables, and low-fat dairy products with a reduced content of dietary cholesterol as well as saturated and total fat), hypertensive individuals should be generally advised to eat more fruits and vegetables (4-5 servings per day, i.e. 300 g) [586] and to reduce intake of saturated fat and cholesterol.
Hypertension is often associated with plasma lipid abnormalities. Even in the absence of marked dyslipidaemia, hypertensive patients should be encouraged to change their diet in terms of fat content and composition.
10.5.3 Oral contraceptives
Oral contraceptives result in a mild elevation of blood pressure in most women and induce overt hypertension in about 5% [587, 588]. The risk of cardiovascular complications is mostly in women over 35 years of age and in those who smoke [589]. Hypertension induced by oral contraception is usually mild and blood pressure returns to normal within 6 months of withdrawal. Oral contraceptive use may also result, albeit rarely, in accelerated hypertension [590] and biopsy-proven renal damage in the absence of primary renal disease [587, 591]. Oestrogens are commonly believed to be the main factor responsible for the blood pressure effect, but the mechanisms are as yet unknown [587]. Although oestrogens have been reported to improve endothelial function [592], their administration may also stimulate the hepatic synthesis of angiotensinogen [593]. Furthermore, arterial distensibility fluctuates during the menstrual cycle in relation to changes in estrogen concentration [594], and use of oral contraceptives has been reported to be associated with an increased albuminuria [595].
Preparations with an oestrogen content of 30 μg and progestogen of 1 mg or less are regarded to be relatively safe. However, a cross-sectional survey of a stratified random sample of English women showed that, although most combined oral contraceptives used in England in 1994 contained low-dose oestrogen, there were slightly but significantly higher blood pressure values (2.3/ 1.6 mmHg) among oral contraceptive users [588]. In a large prospective cohort study in American nurses, a doubling in the adjusted relative risk for hypertension was documented in current users of low-dose oral contraceptives [589].
Several case-control studies performed in the late 1960s supported an association between use of oral contraceptives and stroke [596–598]. Despite recent data [599] questioning the clinical relevance of this association when low-dose oral contraceptives are used, a recent systematic review of combined oral contraceptive use in hypertensive women does show a higher risk for stroke and acute myocardial infarction in contraceptive users than in nonusers [600]. Thrombotic stroke has also been reported to be more frequent with use of oral contraceptives associated with a two-to six-fold increase in the relative risk of venous thromboembolic disease [601].
The progestogen-only pill is a contraceptive option for women shown to have high blood pressure, either induced by use of combined oral contraceptives or due to other causes. So far, no significant association between hypertension and use of progestogen-only pills has been found over 2-4 years of follow-up [602], but this matter has not been addressed by randomized studies because family planning is largely a matter of personal choice, which makes random allocation to interventional and control arms difficult and ethically questionable.
10.5.4 Hormone replacement therapy
In Western societies, women show a steeper increase in systolic blood pressure after the menopause, but whether this is due to the effect of age or the menopause is debated because studies exploring this issue have obtained diverging results, that is, an association of the menopause with higher blood pressure values [603–609] but, also, no significant blood pressure differences [610–614]. The most recent cross-sectional study in 18 326 women [603] indicates that the menopause has some blood pressure-raising effect, but this is small (about 3/3 mmHg) and largely masked by the pressor effect of aging.
Women after the menopause are at an increased risk of cardiovascular disease; this initiated the assessment of the cardiovascular impact of hormone replacement therapy. A number of observational studies have shown that women taking hormone replacement therapy had better cardiovascular risk profiles [615] and a reduced prevalence of coronary disease [616–618] and stroke [619–622] compared to those not taking hormone replacement therapy. Furthermore, a smaller increase in systolic blood pressure over time was reported in postmenopausal women taking hormonal replacement therapy compared to controls [623]. However, rather than confirming a cardiovascular benefit, recent large intervention trials have shown an increased risk of cancer and cardiovascular disease with hormonal replacement therapy [624, 625]. A recent Cochrane systematic review indicates that the only significant benefit of this therapy was a decreased incidence of bone fractures and colon cancer, accompanied, however, by a significantly increased risk of coronary events, stroke, thromboembolism, breast cancer, gallbladder disease and, in women over 65 years of age, dementia [626]. Therefore, at the present time, hormone replacement therapy is not recommended for cardioprotection in postmenopausal women [627].
10.5.5 Antihypertensive drugs
The large number of randomized trials of antihyperten-sive therapy, both those comparing active treatment versus placebo, and those comparing treatment regimens based on different compounds, confirm that (i) the main benefits of antihypertensive treatment are due to lowering of blood pressure per se, and are largely independent of the drugs employed, and (ii) thiazide diuretics (chlorthalidone and indapamide), β-blockers, calcium antagonists, ACE inhibitors and angiotensin receptor antagonists can adequately lower blood pressure, and significantly reduce cardiovascular morbidity and mortality. These drugs are thus all suitable for initiation and maintenance of antihypertensive treatment, either as monotherapy or in combination.
Two recent large-scale trials [442, 443] and a meta-analysis [444] have concluded that β-blockers may have a reduced ability to protect against stroke, though being equally effective in reducing coronary events and mortality. Moreover, administration of β-blockers has been proven beneficial in patients with angina, heart failure and a recent myocardial infarction [628–630]. Thus β-blockers should still be considered a valid option for initial and subsequent antihypertensive treatment strategies. However, as they induce weight gain [631], have adverse effects on lipid metabolism [443], and increase (compared to other drugs) the incidence of new-onset diabetes [632] they should not be preferred in hypertensive individuals with multiple metabolic risk factors including the metabolic syndrome and its major components (i.e. abdominal obesity, impaired fasting glucose, and impaired glucose tolerance), or conditions increasing the risk of new-onset diabetes [633, 634]. This applies also to thiazide diuretics, which have dyslipidaemic and diabetogenic effects, particularly when used at high doses [632]. Thiazides have often been administered together with β-blockers in trials showing a relative excess of new diabetes, thus making a distinction between the contributions of the two agents difficult to dissociate. However, this may not apply to vasodilating β-blockers such as carvedilol and nebivolol shown to have less or no dysmetabolic action, as well as a reduced incidence of new-onset diabetes compared to conventional β-blockers [635, 636].
Trials assessing intermediate end points suggest other differences between various antihypertensive agents or compounds: ACE inhibitors and angiotensin receptor antagonists have been reported to be particularly effective in reducing left ventricular hypertrophy [637], including the fibrotic component [638, 639]; they are also quite effective in reducing microalbuminuria and protei-nuria [573, 640–642], and in preserving renal function and delaying end-stage renal disease [459, 460, 473, 642]; calcium antagonists, besides being effective on left ventricular hypertrophy, appear particularly beneficial in slowing down progression of carotid hypertrophy and atherosclerosis [531, 532, 643]. Evidence concerning the benefits of other classes of antihypertensive agents is much more limited. Alpha1-blockers, centrally acting agents [α2-adrenoreceptor agonists and imidazoline receptor agonists] and antialdosterone drugs have been shown to effectively lower blood pressure [644]. However, there are no data documenting the ability of these drugs to reduce cardiovascular morbidity and mortality in hypertension as the only trial testing an α1-blocker (the doxazosine arm of the ALLHAT trial) was stopped prematurely before crucial evidence could be obtained [645]. All these agents, however, have been frequently used as added drugs in trials documenting cardiovascular protection and can thus be used for combination treatment.
Aliskiren, a new drug inhibiting the effect of renin and prorenin on their specific receptors [646], has been shown to effectively lower blood pressure in hypertension, both alone and in combination with a thiazide diuretic [647–649] and, also, to have an antiproteinuric effect [650]. It has been suggested that renin inhibitors may have effects independent of the renin-angiotensin system and be a prognostic factor independent of angiotensin II production [651]. Conclusive evidence that this is the case as well as data on the cardiovascular protective effects of renin inhibition is not yet available.
Identification of the first class of drugs to be used in the management of hypertension has always been a matter of debate. However, there is now conclusive evidence from trials that combination treatment is needed to control blood pressure in the majority of patients [652]. Thus, if two or more drugs are likely to be required it is of marginal relevance which one is used in monotherapy for the first few weeks or months. However, drug classes (and even compounds within a given class) differ in type and frequency of adverse effects they may induce. Furthermore, drugs may have various effects on risk factors, target organ damage and hypertension-related events. When selecting an antihypertensive drug, the following should be taken into account: (i) the previous favourable or unfavourable experience of the individual patient with a given class of antihypertensive drugs (both in relation to blood pressure lowering and adverse events); (ii) the effect of drugs on cardiovascular risk factors in relation to the cardiovascular risk profile of the individual patient; (iii) the presence of target organ damage, associated clinical conditions, renal disease or diabetes, which may be treated more effectively by some drugs than by others; (iv) the presence of other coexisting disorders that may either favour or limit the use of particular classes of antihypertensive drugs; (v) the possibility of interactions with drugs used for other conditions present in the patient and (vi) the cost of drugs, either to the individual patient or to the healthcare provider. Cost considerations, however, should never predominate over efficacy, tolerability, and safety of the individual patient. Physicians should prefer drugs that have a long-lasting effect and a documented ability to effectively lower blood pressure over 24 h with once-a-day administration. Simplification of treatment improves adherence to therapy [653], while effective 24-h blood pressure control is prognostically important in addition to office blood pressure control [491]. Long-acting drugs also minimize blood pressure variability and this may offer protection against progression of organ damage and risk of cardiovascular events [654–656].
10.5.6 Desirable blood pressure
The primary goal of treatment of the hypertensive patient is to achieve the maximum reduction in the long-term total risk of cardiovascular morbidity and mortality. This requires treatment of all the reversible risk factors identified, including smoking, dyslipidaemia, or diabetes, and the appropriate management of associated clinical conditions, as well as treatment of the elevated blood pressure per se.
The existence of a J-shaped curve relating outcomes to achieved blood pressure has so far been suspected as a result of post hoc analyses only [456, 657–660] and for quite low diastolic pressures. That the inflection of the curve may only occur at blood pressure levels much lower than those aimed at in even intense antihypertensive therapy is supported by a large number of randomized studies in postmyocardial infarction or chronic heart failure patients, in whom benefits of β-blockers or ACE inhibitors administration occurred despite some further reduction of blood pressure already in a quite low range [628, 629].
It should be mentioned that, despite extensive use of multidrug treatment, the average systolic blood pressure achieved in most trials remained above 140 mmHg [661], and even in trials succeeding to achieve average blood pressure values less than 140 mmHg, the rate of control was only 60-70% of recruited patients.
Achieving the target blood pressure may be difficult, particularly when initial blood pressure is higher and in the elderly, since aging makes the elevation in systolic blood pressure strictly dependent on increased aortic fibrosis and stiffness. Trial evidence also shows that, for the same or even greater use of combination treatment, the systolic blood pressure achieved usually remains somewhat higher in diabetic than in nondiabetic patients [565, 573, 662].
In all patients, however, the blood pressure reduction should be obtained gradually. This is particularly important in elderly patients, in those with isolated systolic hypertension, in patients with severe atherosclerotic disease, and in diabetic patients. In all these patients, an excessive orthostatic blood pressure fall should be avoided and the optimal blood pressure value, which can be achieved, should be established by monitoring patients’ symptoms, vital organ function, and well-being.
10.6 Blood pressure target in the general hypertensive population
The 2003 ESH-ESC Guidelines [520], while recommending to lower blood pressure below 140/90 mmHg in all hypertensive individuals, admitted that this was only a prudent recommendation, since trial evidence of the benefit of achieving this goal was limited to patients with diabetes or preexisting cardiovascular disease, and to a post hoc analysis of the HOT trial data [470], indicating the lowest event incidence to be at blood pressures of about 138/83 mmHg. In addition to the evidence reviewed in the 2003 guidelines [520], further indirect evidence supporting a blood pressure goal less than 140 mmHg has been provided by post hoc analyses of the VALUE and INVEST trials. In the VALUE study [663], hypertensive patients whose blood pressure was ‘controlled’ by treatment (>140/90 mmHg) had a significantly lower incidence of stroke, myocardial infarction, and heart failure as well as cardiovascular morbidity and mortality than those remaining ‘uncontrolled', independent of the antihypertensive regimens to which they were allocated. Lower rates of nonfatal and fatal cardiovascular events have also been reported in ‘controlled’ versus ‘uncontrolled’ hypertensive patients of the INVEST study [664]. All this is consistent with what has been reported in studies in hypertensive patients followed in the setting of clinical practice, with those achieving blood pressure values less than 140/90 mmHg showing cardiovascular morbidity and mortality rates much lower than those treated but uncontrolled [665].
On the basis of current evidence it can be recommended that in those who qualify for drug treatment, blood pressure be lowered at least to below 140/90 mmHg in all hypertensive patients and that lower values be pursued, if tolerated, in higher risk persons.
10.7 Blood pressure targets in diabetic patients
In order to maximize cardiovascular protection in diabetic patients, it has been recommended that antihypertensive treatment should be more intense and a goal blood pressure of less than 130/80 mmHg has been proposed. There is very solid evidence of a beneficial effect (reduction in macrovascular and microvascular complications) of a greater versus a smaller blood pressure reduction in type 2 diabetic patients as demonstrated by the HOT and UKPDS trials [470, 666] and confirmed by the ABCD studies [576, 667]. A recent meta-analysis of available trials in diabetic patients has calculated a reduced incidence of cardiovascular events (particularly stroke) with more versus less intense treatment, for a between-group difference in systolic and diastolic blood pressure averaging 6.0 and 4.6 mmHg, respectively [465]. Nevertheless, evidence of the benefit of the strict goal of less than 130/80 mmHg is more limited. Several randomized trials have shown the benefit of reducing diastolic blood pressure to values very close to or even below 80 mmHg [470, 573, 576, 667], but very few data are available on the beneficial effect of systolic blood pressure targets less than 130 mmHg. However, (i) in the ABCD studies [576, 667] in diabetic hypertensive or normotensive patients, achieved systolic blood pressure values of 132 and 128 mmHg, respectively, were associated with lower incidence of outcomes (total mortality and stroke, respectively) than in the groups with slightly less rigorous blood pressure control (systolic blood pressure of 138 and 137 mmHg, respectively) and (ii) a prospective observational study within the UKPDS programme has found a significant relationship between follow-up systolic blood pressure and incidence of macrovascular and microvascular complications in diabetic patients, with a continuous increment in complications for values more than 120 mmHg [668]. Episodes of postural hypertension should be avoided, particularly in diabetic patients.
10.8 Blood pressure targets in high or very high risk patients
Data favouring lower blood pressure targets in patients whose high risk condition is due to factors other than diabetes are of variable strength. The most clear evidence concerns patients with previous stroke or transient ischaemic attack. In the PROGRESS study [570], patients with a history of cerebrovascular disease in whom treatment reduced blood pressure from 147/86 to 138/82 mmHg showed a 28% reduction in stroke recurrence and a 26% reduction in the incidence of major cardiovascular events compared with placebo, in which the blood pressure reduction was negligible. There were substantial cardiovascular benefits also in normotensive patients in whom on-treatment values were reduced to 127/75 mmHg. Furthermore, in a recent post hoc analysis of the PROGRESS data, a progressive reduction in the incidence of stroke recurrence (particularly haemorrhagic stroke) has been reported until systolic blood pressure values of about 120 mmHg [669]. Lower levels of evidence are available for other high risk groups. In a post hoc subgroup analysis of the HOT study [670], greater reductions in diastolic and systolic blood pressure (82 versus 85 mmHg and 142-145 versus 145148 mmHg) were associated with a greater benefit in patients with a high or very high total cardiovascular risk (50% of the HOT population), but not in patients at a lower level of risk. In placebo-controlled trials in myocardial infarction survivors, administration of β–blockers or ACE inhibitors [629, 671] reduced the incidence of recurrent myocardial infarction and death even when blood pressure was normal.
Most placebo-controlled trials in patients with angina or coronary heart disease [571, 572, 574] have provided evidence of a reduced incidence of cardiovascular events by bringing blood pressure targets to rather low levels (EUROPA: 128/78 rather than 133/80 mmHg; ACTION hypertensives: 137/77 rather than 144/81 mmHg; CAMELOT: 124/76 rather than 130/77 mmHg) although, in another trial in anginal patients, similar blood pressure targets (129/74 mmHg rather than 132/76 mmHg) have provided no further benefit [575].
Therefore, similar targets should be adopted in individuals with a history of cerebrovascular disease and can at least be considered in patients with coronary disease.
There are no sufficient cardiovascular outcome data upon which to recommend a lower target blood pressure in patients with nondiabetic renal disease, but sufficient, though not conclusive evidence suggests that values lower than 130/80 mmHg may help in preserving renal function, especially in the presence of proteinuria.
10.8.1 Duration of treatment
Generally, antihypertensive therapy should be maintained indefinitely. Cessation of therapy in patients who had been correctly diagnosed as hypertensives is, in most instances, followed sooner or later by the return of blood pressure to pretreatment levels [672]. Nevertheless, after prolonged good blood pressure control, it may be possible to attempt a careful progressive reduction in the dosage, or number of drugs used, particularly in patients strictly following lifestyle recommendations. However, attempts to step down treatment should be accompanied by careful, continued monitoring of blood pressure, particularly in high-risk patients and in patients with target organ damage. Careful consideration should be given to the fact that, in general clinical practice, hypertension is not well treated and that the number of patients in whom blood pressure is reduced to below 140/90 mmHg is a minority of the hypertensive population [672]. Increasing adherence to antihypertensive treatment and achieving a wide blood pressure control in the population thus represents a major goal for clinical practice in the future.
Chapter 11: Plasma lipids
11.1 Lipids and lipoproteins as risk factors
In blood plasma, lipids such as cholesterol and triglycer-ides are bound to various proteins (apoproteins) to form lipoproteins. The degree to which lipoproteins cause atherosclerosis depends on their type, size and concentrations in plasma. HDL do not cause atherosclerosis but on the contrary, they have antiatherogenic properties. In contrast, LDL, particularly small dense LDL, IDL (intermediate density lipoproteins), and small species of VLDL (very low density lipoproteins) are atherogenic, particularly if they are chemically modified, for example by oxidation. Chylomicrons and large VLDL are not atherogenic but high concentrations of these triglyceride-rich lipoproteins can cause pancreatitis.
11.2 Total cholesterol and LDL-cholesterol
Most of cholesterol in blood plasma is normally carried in LDL and, over a wide range of cholesterol concentrations, there is a strong and graded positive association between total as well as LDL-cholesterol and the risk of cardiovascular disease [673]. This association applies to individuals without cardiovascular disease as well as to patients with established disease. It applies to women as well as men, although the general level of risk is lower in women until the menopause, and it applies to old as well as younger people [674, 675].
This association is considerably modified by other risk factors such as age, sex, smoking, blood pressure, diabetes, and low HDL measured as HDL-cholesterol [676]. However, coronary artery disease is rare in populations with total cholesterol less than 3-4 mmol/l (∼ 115-155 mg/dl), even in the presence of other risk factors. Conversely, coronary artery disease is inevitable in untreated patients with the severest forms of familial hypercholesterolaemia, even in the absence of other risk factors. In patients with the fairly common heterozygous form of familial hypercholesterolaemia, LDL-cholesterol can be quite elevated, 7-12 mmol/l (∼270-465 mg/dl), and LDL-cholesterol is extremely elevated in the rare homozygous form, 12-20 mmol/l (465-775 mg/dl).
The results of epidemiological studies, as well as trials with angiographic or clinical end points, confirm that the reduction of LDL, measured as LDL-cholesterol, must be of prime concern in both primary and secondary prevention of atherosclerotic disease.
11.3 Triglycerides
Hypertriglyceridaemia is also associated with risk of atherosclerotic disease, but the association is not as strong as it is for hypercholesterolaemia.
Although the risk of cardiovascular disease does increase with hypertriglyceridaemia [677], the risk is associated more strongly with moderate than with very severe hypertriglyceridaemia, probably because the former is often due to accumulation in plasma of triglycericeride-rich atherogenic IDL and small VLDL, whereas the latter can be due to nonatherogenic large VLDL and chylomi-crons [678]. Triglycerides levels vary on the basis of the length of fasting (no. of hours) and particular conditions (last heavy meal, alcohol consumption, smoking etc.) before blood sampling.
The association of hypertriglyceridemia to atherosclerosis can be explained by direct atherogenic effects of IDL and small VLDL on the vessel wall, by the fact that high concentrations of triglycerides are also commonly attended by low concentrations of HDL, by the relationship of hypertriglyceridaemia and thrombogenesis as well as by the fact that hypertriglyceridemia can be associated with a large number of physiological and environmental phenomena that promote the development of early-onset cardiovascular disease. They include type 2 diabetes, hypertension, hyperinsulinemia/insulin resistance, abdominal obesity, low physical activity and low consumption of fruits and vegetables.
A triglycerides value more than 1.7 mmol/l (∼ 150 mg/dl) is considered a marker of increased risk, but concentrations less than 1.7 mmol/l are not considered a goal of therapy.
11.4 HDL
Low concentrations of HDL, measured as HDL-choles-terol, are clearly associated, not only with early development of atherosclerosis, but also with poor outcome in those who already have cardiovascular disease [679, 680]. The association is not invariable, since it is not apparent in societies in which the risk of atherosclerotic cardiovascular disease is low [681]. Therefore, it has to be stressed that smoking, sedentary lifestyle, obesity and type 2 diabetes cause lower HDL-cholesterol.
The combination of moderately elevated triglycerides and low concentrations of HDL-cholesterol is very common in patients with type 2 diabetes, abdominal obesity, insulin resistance and physical inactivity having a high risk for an early-onset atherosclerotic disease. It is part of a pattern of deranged plasma lipoproteins characterized by a triad of increased concentrations of IDL and VLDL, the presence of small dense LDL, and low concentrations of HDL. It may even rival hyperch-olesterolaemia, due to high concentrations of LDL, as a cause of atherosclerosis. However, a practical limitation is that one component of this triad, atherogenic small dense LDL, cannot be measured in routine clinical practice but low HDL cholesterol and moderate hypertriglyceridemia suffice to indicate the need for preventive treatment of these patients.
HDLs are antiatherogenic [682] and it has been suggested that HDLs exert this effect through anti-inflammatory, antithrombotic and antiapoptotic mechanisms. They also inhibit expression of adhesion molecules thus inhibiting the adhesion of monocytes to endothelial cells, an early step in the atherosclerotic process. They stimulate the efflux of cholesterol from foam cells, they stimulate prostacyclin synthesis and inhibit the synthesis of platelet-activating factor in endothelial cells which all contributes to their protective role. The participation of HDL in the transportation of cholesterol to the liver from other organs and tissues containing a surplus of cholesterol (termed reverse cholesterol transport) is yet another mechanism by which HDL could protect the artery wall.
HDL-cholesterol is not considered a goal of therapy in the present document. Instead, HDL-cholesterol less than 1 mmol/l (∼40 mg/dl) in men and less than 1.2 mmol/l (∼ 45 mg/dl) in women is considered a marker of increased risk that should suggest to the physician that attention to lifestyle and management of high LDL-cholesterol, high blood pressure, smoking and obesity is necessary.
11.5 Other lipoproteins and lipoprotein components
11.5.1 Lp(a)
Lp(a) is pronounced ‘LP little a'. It is a low density lipoprotein to which is attached an additional protein called apolipoprotein(a). It has no known physiological role, and high concentrations of Lp(a) (arbitrarily >30 mg/dl) are largely resistant to modification. They identify persons at increased risk of atherosclerotic diseases [683].
11.5.2 Apolipoprotein B
Apolipoprotein B (apoB) is the major protein component of LDL, IDL, VLDL and, in truncated form, chylomicrons. Since chylomicrons normally are not present in plasma in the fasting state, almost all apoB is in atherogenic lipoproteins. Concentrations of apoB are therefore a direct measure of the concentration of atherogenic lipoproteins in plasma. The measurement is a useful indicator of risk of atherosclerosis, particularly in patients with hypertriglyceridemia [684] and in people with normal concentrations of LDL-cholesterol [685]. Values greater than 150 mg/dl are clearly associated with increased risk. However, since measurement of apoB is not generally available to all physicians in Europe, it is not included in the present recommendations for assessing cardiovascular risk.
11.5.3 Apolipoprotein A1
Apolipoprotein A1 is the major apoprotein of HDL. Low concentrations of apolipoprotein A1 are, like low HDL cholesterol, associated with higher risk of cardiovascular disease [684]. As for apoB, since measurements of apolipoprotein A1 are not generally available to all physicians, it is not included in the present recommendations for assessing cardiovascular risk.
11.5.4 Apolipoprotein B/A1 ratio
It is beyond doubt that the apoB/apoA1 ratio is one of the strongest risk markers. This was emphasized in the INTERHEART study [685]. However, it is still not established whether this variable should be used as a treatment goal. These measurements are today available in many European countries and might be recommended as a very useful additional tool for risk estimation but since they are not available to all physicians, they are not part of the general recommendations of the present document. It has to be stressed that they are much more accurate than available direct measurements of LDL. Opinion is divided as to whether the ApoB/ApoA1 ratio is [686] or is not [687] superior to total cholesterol/HDL-cholesterol ratio in terms of risk estimation.
11.6 Calculated lipoprotein variables
11.6.1 LDL
LDL can be measured directly, but it is usually calculated by the Friedewald formula [688]:
In mmol/l: LDL-cholesterol = total cholesterol-HDL-cholesterol (0.45 × triglycerides);
In mg/dl: LDL-cholesterol = total cholesterol-HDL-cholesterol (0.2 × triglycerides).
The calculation is valid only when concentrations of triglycerides are less than approximately 4.5 mmol/l (∼400 mg/dl). That is because the ratio of triglyceride-to-cholesterol in triglyceride-carrying lipoproteins (VLDL and chylomicrons) progressively increases as hypertrigly-ceridaemia becomes more severe. The fact that the calculation depends upon three laborarory measures means that three coefficients of variation are involved with potential for error. Direct measurement techniques are therefore increasing in popularity.
11.6.2 Non-HDL-cholesterol
In the fasting state, non-HDL-cholesterol is the cholesterol in LDL, IDL and VLDL. Calculated by simply subtracting HDL-cholesterol from total cholesterol, non-HDL-cholesterol, unlike LDL-cholesterol, does not require triglycerides to be less than 4.5 mmol/l (∼400 mg/dl). Therefore, it is an even better measure than calculated LDL-cholesterol, particularly for patients with high triglycerides. It is, like apoB, a measure of concentrations of atherogenic lipoproteins in plasma [689] but it is more readily available than measurements of apoB and A1. In view of the lack of RCT evidence no goal for non-HDL-cholesterol can be established at this time.
11.6.3 Total cholesterol/HDL-cholesterol
The ratio of either total cholesterol or LDL-cholesterol to HDL-cholesterol has a long history in cardiovascular risk assessment. Total rather than LDL-cholesterol is preferable in the numerator, because, as is apparent from the Friedewald formula, a mistake made in the measurement of HDL-cholesterol will affect the calculation of LDL-cholesterol and compound the mistake in the assessment of risk (an erroneously high HDL cholesterol reduces the amount of cholesterol calculated to be present in LDL and vice versa). A total cholesterol/HDL-cholesterol ratio more than 5 indicates increased risk and is particularly useful in the middle part of the cholesterol distribution (5-6.5 mmol/l, ∼ 190-250 mg/dl). In the SCORE charts [105] the total cholesterol and HDL-cholesterol charts look remarkably similar. Additonal unpublished analyses suggest that improved prediction may indeed be possible if total and HDL-cholesterol are entered separately into the risk estimation model.
11.6.4 Lipoproteins and cardiovascular disease risk
Plasma cholesterol does not always differentiate well between individuals destined and not destined to develop coronary artery disease [676]. That observation, of course, is one of the reasons for the multifactorial approach to risk estimation recommended in this document. At population level, however, concentrations of plasma total cholesterol are powerful predictors of coronary artery disease. A 10% increase in plasma total cholesterol is associated with an increase in the incidence of coronary artery disease of 27% [690] which is a good indicator of the magnitude of the public health problem associated with hyperlipidaemia. On the other hand, a 10% reduction in plasma total cholesterol is followed by a 25% reduction in incidence of coronary artery disease after 5 years, and a reduction of LDL-cholesterol of 1 mmol/l (∼ 40 mg/dl) is accompanied by a 23% reduction in CHD, 19% reduction in stroke and 21% reduction in CVD [99].
These conclusions are based upon the results of a meta-analysis of 14 large clinical trials of cholesterol-lowering with statins, which were published from 1994 to 2003. In all, they randomized more than 90 000 men and women, with and without coronary artery disease, to treatment with placebo or a statin drug [63, 467–469, 691–696, 697–700]. They showed that lowering total and/or LDL-cholesterol with a statin reduced the risk of coronary artery disease events. The exception was the ALLHAT-LLT study with pravastatin, in which the reduction in CHD events was not statistically significant. The authors explained their discrepant results by the exceptionally modest difference in cholesterol between the active and control groups of that study (9.6%) compared to that obtained in the earlier trials, including three earlier trials with pravastatin. Thus, clinical benefit does not occur if cholesterol is not adequately reduced.
The earlier trials have left unanswered several questions concerning subgroups, particularly diabetic patients. Several recent trials such as Heart Protection Study (HPS) and CARDS [696, 701] have shown the benefits of statins in preventing cardiovascular events and mortality in diabetic patients. It has to be stressed that the lifelong coronary heart disease risk in diabetic patients may be as high as in nondiabetic individuals with prior cardiovascular disease (see chapter 12). This indicates the need for early preventive efforts, even in type 2 diabetic patients with moderate risk. Not all the trials have consistently shown significant benefits of statins in diabetic patients [468, 469, 694, 695]. However, a meta-analysis [99] showed the same 21% decrease in CVD in diabetic and nondiabetic patients for each 1 mmol/l decrease in LDL-cholesterol.
The main conclusions of the lipid-lowering trials is that it is possible to inhibit progression of coronary atherosclerosis and to reduce the risk of myocardial infarction. In several trials the resulting decrease in coronary death rates translated into a reduction of overall death rates. Moreover, the trials have consistently shown that treatment with statins reduces the need for coronary artery by-pass grafting and various forms of coronary angioplasty. The Heart Protection Study extended this evidence of benefit to carotid endarterectomy and other peripheral artery revascularizations as well [63]. Recent data suggest that using statin treatment it is also possible to achieve regression of atherosclerosis as measured by intravascular ultrasound (IVUS) [702].
Despite early observational studies indicating that plasma cholesterol is not associated to overall rates of stroke [703], and that lowering cholesterol does not lower the risk of stroke [704], several of the large statin trials reported significant reductions in stroke rates in patients with or at high risk of getting coronary artery disease [467, 691, 694] due to a reduction in the rates of ischaemic stroke [705]. There was no indication in the data from the statin trials that this therapy increases the risk of haemorrhagic stroke, a concern that had been raised earlier by observational data [706], except in the SPARCL trial, which showed an increase in the risk of haemorrhagic stroke with statin therapy [707].
Most of the large statin trials included some women and patients over 65 years, although the numbers are usually small and analysed retrospectively. No differences in the effects of lipid lowering between men and women and between younger and older age groups were detected [708], although the benefits in healthy, asymptomatic women are not proven. There are benefits of lipid lowering in women with known cardiovascular disease, in reducing CHD events, CHD mortality, nonfatal myocardial infarction, and revascularization, although not on total mortality. Benefits in women and in the elderly are also strongly supported by the Heart Protection Study [63] and the PROSPER trial [695] and a recent meta-analysis [99]. However, a recent systematic review was much more cautious in its findings – ‘For women without cardiovascular disease, lipid lowering does not affect total or CHD mortality. Lipid lowering may reduce CHD events, but current evidence is insufficient to determine this conclusively. For women with known cardiovascular disease, treatment of hyperlipidaemia is effective in reducing CHD events, CHD mortality, nonfatal myocardial infarction, and revascularization, but it does not affect total mortality’ [709].
An important result of meta-analyses of the literature is that the benefits of cholesterol-lowering therapy depend on initial levels of risk: the higher the risk, the greater the benefit [710]. That concept has been central to the earlier versions of the Joint European Recommendations [1–3], and it is supported by the results of the statin trials. Since the relative reductions in risk as a consequence of lipid lowering were approximately the same in patients at higher and lower risk, the absolute reductions in risk were highest in patients at the highest baseline risk.
High-risk patients included, in particular, patients with established coronary artery disease [467, 694]. It has to be stressed, however, that the patients with cerebrovascular disease and peripheral vascular disease merit the same degree of attention to treatment of plasma lipids as patients with coronary artery disease. The results of several statin trials suggest that the absolute rate reduction in risk as a result of statin therapy are particularly marked in patients with diabetes [63]. As reviewed in chapter 12, epidemiological studies have shown that the risk of CVD is not uniformly increased in patients with type 2 diabetes, but is influenced by a number of factors, particularly duration of disease, age and sex. This does not question that fact that most of them are high-risk patients in whom lipid lowering therapy is beneficial and necessary, particularly if they have some other risk factors or have microalbu-minuria.
The large statin trials as well as several meta-analyses dispelled convincingly early concerns that lipid lowering might cause noncardiovascular mortality to increase due to cancers, suicides, depression, etc. [706]. The epidemiological evidence supports the interpretation that cancers and depression cause plasma cholesterol to fall rather than the other way around [710] and the rates of cancer and suicide seem to be unaffected by statin therapy [63, 711].
11.7 Management of dyslipidaemia
11.7.1 Exclusion of secondary dyslipidaemia
Hyperlipidaemias secondary to other conditions must be excluded before starting treatment, especially with drugs, since often the treatment of underlying disease improves hyperlipidaemia and no other antilipaemic therapy is necessary. This is particularly true for hypothyroidism. Secondary hyperlipidaemias could be also caused by abuse of alcohol, diabetes, Cushing's syndrome, diseases of the liver and kidneys, obesity and several drugs (e.g. corticosteroids, isotretionoin and etretinate, cyclosporin). Patients who could have genetic dyslipidemias such as familial hypercholesterolemia should, if possible, be referred to specialist evaluation, which might include molecular genetic diagnosis.
11.7.2 Diet
All patients with atherosclerotic disease, and persons at high risk of developing atherosclerotic disease, should follow the dietary recommendations given in this document (chapter 8). Some patients with severe hypertriglyceridaemia (> 9 mmol/l) require a diet that is severely restricted in long-chain fatty acids from vegetable as well as animal sources and all patients with hypertriglycer-idaemia should reduce alcohol intake. The purpose of this diet is to prevent pancreatitis. It differs substantially from the general dietary recommendations, and most patients will need the assistance of a well-trained dietician.
11.7.3 Physical exercise
Patients with clinically established CVD as well as persons at high risk should follow the recommendations given in chapter 9 of this document. The major effect of physical exercise, apart from a decrease in triglycerides, is an increase in HDL-cholesterol.
11.7.4 Drugs
In most European countries, the current armamentarium of lipid-lowering drugs includes inhibitors of HMG CoA reductase (statins), fibrates, bile acid sequestrants (anion exchange resins), nicotinic acid and selective cholesterol absorption inhibitors such as ezetimibe. All of these drug classes, with the exception of cholesterol absorption inhibitors, have been shown in trials to reduce myocardial infarction and coronary death.
The most convincing evidence from clinical end point trials as well as from angiographic and intravascular ultrasound (IVUS) trials demonstrating inhibition of the progression and/or regression of atherosclerosis has been obtained with the most potent of the lipid-lowering drugs – the statins. Statins are therefore first line drugs for lowering LDL-cholesterol. There are differences among statins in terms of their LDL-lowering efficacy. Among all lipid-lowering drugs, only the most potent statins in the highest doses have been shown to halt progression or induce regression of coronary atherosclerosis as found in two IVUS studies [572, 702]. Pleiotropic effects (such as inhibition of LDL oxidation, anti-inflammatory, and antithrombotic) have been suggested based on various experimental systems; it has been claimed that these mechanisms are important for statin efficacy. However, the major mechanism of their antiatherogenic properties is attributable to their lipid-lowering effect. This is confirmed in studies with more potent statins [572, 712] or higher doses of the same statin [713] in head-to-head comparison trials, as evidenced by reduced atheroma [572] or less risk of major cardiovascular events [712, 713] with more aggressive treatment. Lipid-lowering efficacy as the main determinant of the statin effects is also supported by a recent large meta-analysis of 14 statin trials [99] showing that the reduction of major vascular events was proportional to the absolute reduction of LDL levels. No significant differences suggesting different pleiotropic effects among statins were found in another recent analysis comparing studies with atorvastatin, simvastatin and pravastatin [714]. A tendency towards lower event rates with more potent statins, however, was observed in this analysis. It should be noted that no direct head-to-head comparisons between statins and other lipid-lowering drugs have been performed in appropriate trials. Pleiotropic effects unique to statins as a class therefore cannot be excluded, although a recent meta-regression analysis comparing 10 statin trials with 8 trials using other treatments (diet, bile acid sequestrants or surgery) found no additional effect for statins beyond that of LDL-lowering [715]. Unfortunately, head-to-head comparisons on clinical end points of different statins and different dosages of the same statin are scarce.
All the large trials have confirmed the good safety of statins [99] and these drugs are easy to use. The most serious side-effects are myopathy and, very rarely, rhabdomyolysis. Because statins are prescribed on a long-term basis possible interactions with other drugs deserve particular attention, as many patients will receive pharmacological therapy for concomitant conditions during the course of statin treatment [716] (Table 11).
Fibrates lower triglycerides and increase HDL quite effectively but they lower total and LDL-cholesterol much less than the statins. They are also easy to use. Since the evidence from clinical trials to support the wide-spread use of fibrates was not as good as that supporting statins, they were considered useful only for treatment of dyslipidemic patients with low HDL, high triglycerides, and other characteristics of the insulin resistance syndrome and type 2 diabetes. In FIELD, a large randomized controlled trial with high-risk diabetic patients, fenofibrate reduced only nonfatal myocardial infarctions and revascularization, but no beneficial effect on risk of fatal coronary events was observed [717]. Considering the much more convincing evidence for the efficacy of statins in diabetic patients [696, 701], fibrate monotherapy cannot be recommended as first-line treatment in this high-risk group, but may be considered in those with persistently low HDL levels. They may also be considered in those with severely elevated triglycerides, primarily to prevent complications such as pancreatitis.
Selected drugs that may increase risk of myopathy and rhabdomyolysis when used concomitantly with statin CYP3A4 inhibitors/substrates
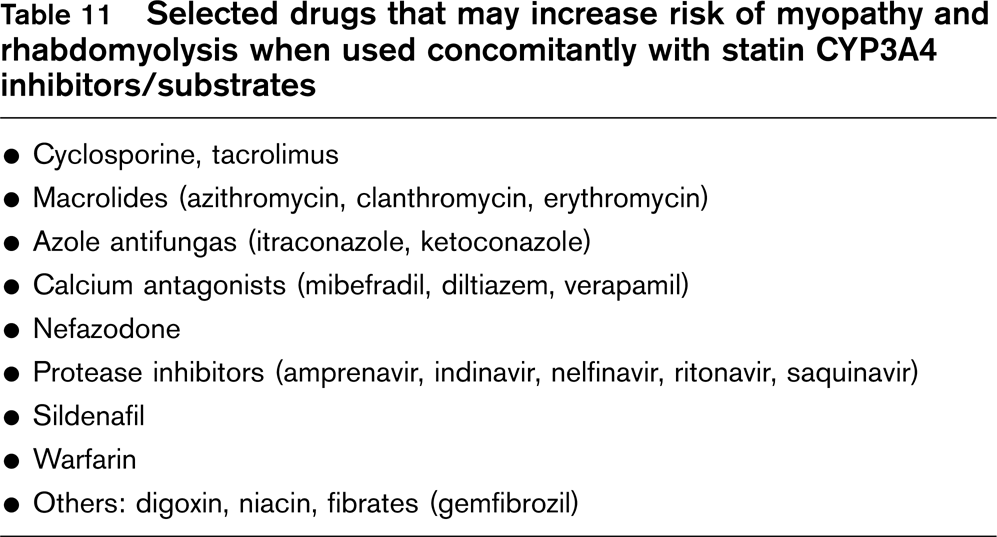
Anion-exchange resins and niacin (nicotinic acid) are also effective lipid-lowering agents. They can be difficult to use, however, and annoying side effects such as constipation and flushing, respectively, today usually limit the use of these drugs to lipid specialists. However, data suggest that nicotinic acid is more effective in increasing HDL-cholesterol than fibrates [718] and the long-term follow-up results of the coronary drug project indicated a reduction in total mortality with nicotinic acid [719].
An inhibitor of cholesterol absorption from the small intestine (ezetimibe) has become available in most European countries. In monotherapy ezetimibe has mild LDL-lowering effects and can be considered in patients with active liver disease, when statin, fibrate and nicotinic acid are contraindicated and in patients having adverse effects on statins. The main role of ezetimibe, however, is in combination therapy with statins in patients not reaching targets with statin monotherapy [720–722]. Such combination therapy has shown good LDL-lowering efficacy. No trials with clinical end points, however, have been reported.
11.8 Therapy of raised triglycerides
Some patients with raised blood triglyceride levels show a marked response to alcohol or weight reduction which form the first line of management
Bile acid sequestrants (anion-exchange resins) tend to increase triglycerides, and they should only be used when triglycerides are less than 2 mmol/l (∼ 180 mg/dl) or if given in conjunction with triglyceride-lowering agents. Statins are usually used for patients with triglycerides up to 5 mmol/l (∼ 450 mg/dl). When triglycerides are between 5 and 10 mmol/l (∼ 450-900 mg/dl), either fibrates or statins may be used as first choice drugs, and niacin is a good drug in selected patients. Fish oils are also triglyceride-lowering agents and might be useful as a third-line therapy for patients with hypertriglyceridaemia resistant to or intolerant of fibrates or niacin or in combination with other triglyceride lowering drugs. When triglycerides exceed 10 mmol/l (∼900 mg/dl), drugs are generally not useful, but fibrates may still be tried in order to prevent pancreatitis. If ineffective, triglycerides must be reduced by restriction of alcohol, treatment of diabetes with insulin, withdrawal of estrogen therapy, etc. In the rare patients with severe primary hypertriglycer-idaemia, it is necessary to restrict absolutely the intake of alcohol and severely restrict long-chain fat of both animal and vegetable origin.
11.9 Drug combinations: effects and side-effects
Lipid-lowering drugs can be used in combination and in some patients this is necessary to achieve the treatment goals both in familial hypercholesterolaemia and in combined hyperlipidaemia. In familial hypercholestero-laemia, for example, the combination of a bile-acid sequestrant and a statin is very useful, although a combination of a statin with cholesterol absorption inhibitor ezetimibe appears a more potent and better tolerated option [720–722]. A statin and niacin can be used in some patients. Statins can also be combined with fibrates, but this combination has been associated with higher incidence of myopathy, even fatal rhabdomyolysis, and patients must be carefully selected and carefully instructed about warning symptoms (myalgia). However, these adverse effects are very rare and should not be the cause to deny the combined treatment to patients who really need it. The combination of fibrate with ezetimibe may be an option in selected patients with mixed hyperlipidaemia. Although efficacy and safety of such treatment was good in one study [723], other studies and long-term data are awaited.
11.10 Lipid-lowering therapy in acute coronary syndrome
The MIRACL trial in patients with acute coronary syndromes showed that treatment with a statin, initiated within 4 days, can reduce the recurrence of myocardial ischaemia during the following 4 months [724]. The same has been shown in the PROVE-IT trial [725], although the A-to-Z trial did not show any significant benefit over the first 4 months [726]. Therefore statins should be initiated while patients are in hospital with an acute coronary event. Another strong reason to initiate statin therapy while patients are in hospital is the fact that adherence rates to statins have been shown to be much higher if patients are discharged with a prescription. Plasma lipids should be reevaluated both at 4-6 weeks and 3 months after acute event and/or initiation of the lipid-lowering therapy to evaluate whether target levels have been achieved and to screen for liver dysfunction. The second control at 3 months is important for patients after myocardial infarction, since decrease of plasma lipids due to acute phase reaction may last for such periods of time. The early drug treatment should nevertheless be combined with effective lifestyle changes and particularly dietary intervention after the hospital discharge. The strategy to ensure that goal concentrations are reached must obviously depend on the organization of medical care in each European country.
11.11 LDL apheresis
Rare patients with severe hypercholesterolaemia, especially homozygous familial hypercholesterolaemia, require specialist evaluation of the need for LDL apheresis. By this demanding and expensive but effective technique, LDL is removed from plasma during extracorporeal circulation weekly or every other week. LDL apheresis has to be combined with treatment with statins.
11.12 Goals of therapy
Physiological concentrations of LDL-cholesterol are probably around 1-2 mmol/l (∼ 40-80 mg/dl), but whether clinical benefit results from reducing LDL-cholesterol to such low levels has been the subject of some controversy. Several studies such as 4S [467] and LIPID trials [694] indicated that there is no lower threshold for benefits of total and LDL-cholesterol level reduction. The results of the Heart Protection Study [63] demonstrated the same degree of benefit, given in relative terms, of lowering LDL-cholesterol from 3 to 2 mmol/l as from 4 to 3 mmol/l, suggesting again that, at least down to about 2 mmol/l, there is no clear threshold value for benefit. This conclusion is also supported by the result of the ASCOT-LLA trial, which demonstrated clinical benefit from reducing LDL-cholesterol by about 1.2 mmol/l from a baseline level of only 3.4 mmol/l [469]. It is also consistent with observational epidemiology [725]. In patients with cardiovascular disease, the Treat to New Targets (TNT) study showed that an extra benefit could be obtained by larger reductions of LDL-cholesterol without increasing the risk of serious adverse events [713]. The IDEAL study had similar findings with a composite end point that included stroke [727].
In 1998 and 2003, the Joint European Societies recommended that reduction of total cholesterol below 5 mmol/l (∼ 190 mg/dl) and LDL-cholesterol below 3 mmol/l (∼ 115 mg/dl) could be goals of therapy consistent with the evidence available at that time [2, 3]. However, for patients with established cardiovascular disease and patients with diabetes the treatment goals were lower: total cholesterol less than 4.5 mmol/l (∼ 175 mg/dl) and LDL-cholesterol less than 2.5 (∼ 100 mg/dl).
The results of clinical trials since then raise the question of whether the goals for total cholesterol and LDL-cholesterol be lowered further. It is still not clear what the ideal LDL-cholesterol value is, but there is evidence of benefit down to 2 mmol/l and even lower in all patients with established atherosclerotic disease. In several studies benefit was seen with more intensive therapy reaching even lower levels (1.6-1.8 mmol/l) and in one noncontrolled study (ASTEROID) mean LDL of 1.55 mmol/l was associated with regression of atheroma [702]. Therefore an optional target for high risk patients of less than 2.0 mmol/l has been defined if feasible clinically and in terms of local financial resources.
Asymptomatic people at high risk of developing CVD, whose untreated values of total and LDL-cholesterol are already close to 5 (∼ 190 mg/dl) and 3 mmol/l (∼ 115 mg/dl), respectively, will definitely benefit from further reduction of total cholesterol to less than 4.5 mmol/l (∼ 175 mg/dl) and from further reduction of LDL-cholesterol to less than 2.5 mmol/l (∼ 100 mg/dl) with lipid-lowering treatment.
However, these goals cannot be reached with the same ease by all patients. Patients with concentrations of plasma lipids that are only slightly abnormal can reach these goals of therapy fairly easily with diet and moderate doses of drugs. When these goals have not been reached in asymptomatic people at high risk they will still benefit to the extent that cholesterol has been lowered.
11.12.1 Should statins be given to all persons with CVD?
Relative risk reductions seem to be constant at all lipid levels, but absolute risk reductions are small in those with low lipid levels, with little evidence of a reduction in total mortality. The universal use of statins may be unrealistic in some economies.
A minority of patients have familial hypercholesterolemia or other severe, genetically determined disturbances of lipid metabolism. Even with dual or triple drug regimens, reducing LDL-cholesterol below 2 mmol/l (∼ 80 mg/dl) can sometimes be difficult, and the physician must prepare the patient for that situation.
The current recommendations are that triglycerides greater than 1.7 mmol/l (∼ 150 mg/dl) and HDL-cholesterol less than 1 mmol/l (∼ 40 mg/dl) in men and less than 1.2 mmol/l (∼ 45 mg/dl) in women continue to be regarded as markers of increased risk. However, triglycerides and HDL-cholesterol continue not to be regarded as goals of therapy. The main reason for this recommendation is that, in contrast to the evidence underpinning reduction of LDL-cholesterol, there is still not enough evidence from clinical trials defining to which levels triglycerides should be reduced, or HDL-cholesterol should be increased, to reduce risk of cardiovascular disease. Apart from being powerful indicators of risk, measurements of triglycerides and HDL-cholesterol should also be used to guide the choice of drug therapy as can non-HDL-cholesterol, for example use of a drug with beneficial activity on these measures should be considered in patients where HDL-cholesterol and triglycerides are abnormal. The recommendations are summarized in Table 12.
11.13 Lipids and stroke risk
Cholesterol has a different history as a risk factor for cerebrovascular disease than for CHD. Only few early epidemiological studies have found increasing risk of stroke with high total cholesterol [728], and early meta-analyses have not found any significant association between stroke and total cholesterol levels [703]. However, this was due to the fact that in these studies ischaemic stroke was considered together with haemorrhagic stroke. When ischaemic stroke alone was analysed, a clear correlation with total and LDL-cholesterol levels was found indicating that high cholesterol is a risk factor for ischaemic stroke, but not for haemorrhagic stroke [729]. Conversely, an increased risk of haemorrhagic stroke has been documented in patients with extremely low cholesterol levels. Increased level of triglycerides was also significantly associated with nonhaemorrhagic strokes [730], as was decreased HDL-cholesterol [731]. Almost all big multicentre randomized controlled trials with statins have shown a significant reduction in cerebrovas-cular events including nonhaemorrhagic strokes in patients treated with statins. This was true for studies with simvastatin [63, 467], atorvastatin [469] and several trials with pravastatin [692, 694]. However, in one trial with pravastatin in elderly, despite a significant reduction in transient ischaemic attacks (TIAs), no significant reduction in strokes could be proven [695]. Many stroke patients have CHD and/or diabetes and they will clearly benefit from statins [63]. Intensive cholesterol lowering with 80 mg atorvastatin/day in a randomized, placebo-controlled trial of patients with unstable angina or non-Q-wave myocardial infarction reduced after only 16 weeks the overall stroke rate by half without increasing the risk of haemorrhagic stroke [732]. A recently published trial evaluated the effects of 80 mg atorvastatin/day in patients with ischaemic cerebrovascular disease. A significant risk reduction for recurrent cerebrovascular events has been shown but patients receiving atorvastatin had some more haemorrhagic strokes [733]. Similar beneficial effects of fibrates on risk reduction could not be proven neither for overall nor for nonhaemorrhagic stroke [734].
Chapter 12: Diabetes and metabolic syndrome
Treatment targets in patients with type 2 diabetes
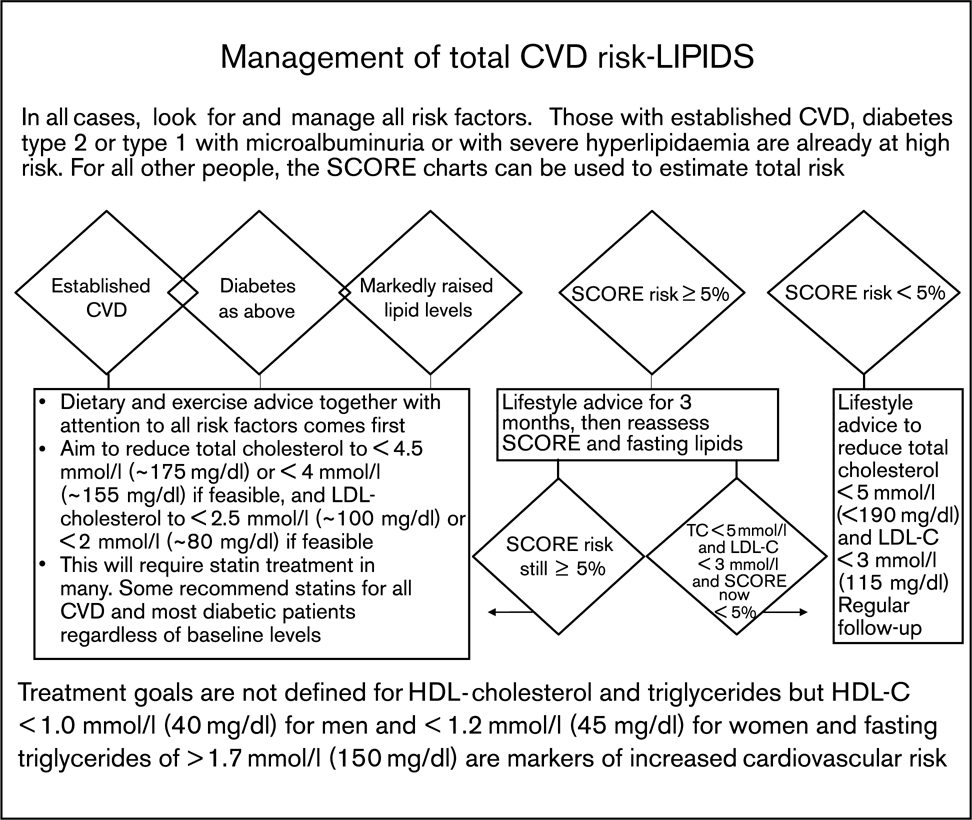
The metabolic syndrome
The term ‘metabolic syndrome’ refers to the combination of several factors that tend to cluster together-central obesity, hypertension, low HDL cholesterol, raised triglycerides and raised blood sugar-to increase risk of diabetes and CVD.
This implies that, if one component is identified, a systematic search for the others is indicated, together with an active approach to managing all of these risk factors.
Physical activity and weight control can radically reduce the risk of developing diabetes in those with the metabolic syndrome.
Chapter 12: Diabetes and metabolic syndrome
12.1 Hyperglycaemia, diabetes and CVD risk
Epidemiological studies demonstrate a linear association between increasing glucose levels and the risk of developing CVD continuing all the way down to the normal range. This has been demonstrated both using the 2-h value following an oral glucose tolerance test [735] and using the integrated measure of glycated haemoglobin HbA1c [736–741]. In the nondiabetic range, nonfasting plasma glucose values are more predictive than fasting values in relation to CVD, but these studies have compared fasting plasma glucose values with the 2-h value following an oral glucose tolerance test. The clinically more relevant comparison would be between fasting and postprandial glucose, but this study has not been performed.
Individuals can be classified into different categories (Table 13) based on fasting plasma glucose and 2-h plasma glucose measurement following a 75 g oral glucose tolerance test [742, 743].
Classification based on plasma glucose levels

aThe American Diabetes Association use ≥ 5.6 mmol/l (≥ 100 mg/dl) as the lower cut-point for IFG. This lower cut-point was not adopted in Europe, and is not recommended by WHO [743].
Normal Glucose Tolerance (NGT)
Impaired glucose regulation including
Impaired Fasting Glycaemia (IFG) and
Impaired Glucose Tolerance (IGT)
Diabetes (DM)
12.2 Hyperglycaemia and CVD risk
Epidemiological studies have shown that hyperglycaemia is associated with an increased risk of developing CHD as well as other atherosclerotic diseases [736–740]. This is true for diabetes as well as for individuals with impaired glucose tolerance (IGT) – the intermediate stage between normal and diabetic postload glucose levels. In diabetic individuals the relative risk of CVD is in the order of 2-4, while in individuals with IGT the relative risk is 1.5 compared to individuals with normal glucose tolerance [744]. Isolated IFG (fasting plasma glucose in the IFG range and normal 2 h plasma glucose) is not associated with an increased risk of CVD.
'Diabetes’ is classified into two major groups (type 1 and type 2) and a number of smaller specific entities classified on the basis of specific genetic markers, syndromes or secondary diabetes induced by other diseases, chemicals or drugs [742].
Type 1 diabetes is characterized by loss of β-cell function and endogenous insulin production to a level where the individual would die from ketoacidosis if not treated with insulin. The incidence is highest in children and young adults, but type 1 diabetes can develop at any age.
Type 2 diabetes is a condition characterized by a combination of insulin resistance and β-cell failure. With increasing duration, insulin may be necessary in up to 50% of the patients to obtain acceptable metabolic control [745]. The incidence and prevalence increases by age, but the condition is heavily associated with obesity and lack of physical activity, and for this reason the incidence is not only increasing world wide [746], but the age at diabetes onset is also decreasing, and type 2 diabetes can be seen even in teenagers. An important underlying mechanism leading to type 2 diabetes is insulin resistance, which again is associated with a long list of cardiovascular risk factors including hypertension, dyslipidaemia, endothelial dysfunction and microalbuminuria [747]. This clustering of risk factors partly explains the increased risk of CVD associated with diabetes and glucose intolerance. However, many studies have reported an association independent of traditional and nontraditional risk factors.
12.3 Risk of CVD, CHD and stroke in diabetes
The association between these macrovascular complications differs markedly between type 1 and type 2 diabetes. In type 1 diabetic patients there is a two to three-fold increase in the risk of developing CVD, CHD and stroke. This increased risk is almost entirely confined to the patients developing diabetic renal disease [748].
In type 2 diabetes, all patients are at increased CVD risk, even in the absence of diabetic nephropathy. Finnish data published in 1998 suggested that the risk of developing a myocardial infarction in patients with type 2 diabetes is of the same order as for patients without diabetes who have already suffered their first MI [749]. This had immense effect on treatment guidelines, where diabetes was labeled as a ‘CVD-equivalent’ when it came to risk assessment. Since then, however, many studies based on different study cohorts have addressed this issue and it has become clear that this is an oversimplification and that the impact of type 2 diabetes on CVD risk is influenced by a number of factors, including the duration of diabetes, age and sex [290, 750–760]. The effect of gender on the diabetes-related CVD is of major importance in the interpretation of study results. Because the relative impact of type 2 diabetes on the CVD risk is much stronger in women than in men, the concept of diabetes as CVD-equivalent has proved to be true in women in studies analysing data separately for both sexes [751, 754, 756–760]. In men the outcomes of studies have been less consistent, but in some study cohorts type 2 diabetes has been CVD-equivalent also in men, particularly in older age groups [756, 758–760].
Although a substantial proportion of the excess risk of atherosclerotic disease in both type 1 and type 2 diabetes is caused by the diabetic state itself and related factors, from the point of prevention of atherosclerotic disease it is important to emphasize that the conventional, modifiable major cardiovascular risk factors, elevated blood pressure, elevated LDL-cholesterol, and smoking show in both type 1 [761], and type 2 diabetic patients [762] similar relationships with the risk of CVD as in nondiabetic patients. Because diabetes itself increases the absolute risk of cardiovascular disease, the additional impact of conventional risk factors leads to a more dramatic increase in absolute risk than in nondiabetic patients and thus the modification of these risk factors offers a great potential for prevention. Consequently, individualized global risk assessment and individualized prevention strategies are even more important in individuals with diabetes than in nondiabetic patients.
12.4 The evidence for the current recommendations on prevention of CVD in diabetes
With the exception of glucose management, prevention of CVD follows the same general principles as for people without diabetes. A multifactorial approach to treatment and achieving low BP and low LDL are particularly important, thus many of the treatment targets are tougher for patients with diabetes.
12.4.1 Glucose
The UK Prospective Diabetes Study (UKPDS) [763, 764] evaluated the effect of improved metabolic control on the risk of developing coronary heart disease or any other atherosclerotic disease. The study demonstrated a 16% borderline significant (P = 0.052) risk reduction for myocardial infarction associated with the 0.9% reduction in HbA1c obtained in the study. In obese patients treated with metformin a significant effect was seen (P >0.01). As the study used several different treatment modalities, and many patients changed treatment during the trial [745], the authors have also estimated the overall risk reduction associated with a 1% decrease of HbA1c independent of treatment modality. On the basis of their observational epidemiological analyses UKPDS investigators concluded that a significant 14% reduction in the risk of CVD would occur per reduction in HbA1c by 1% [763]. The risk reduction for microvascular complications (retinopathy and nephropathy) was markedly larger [765], as also demonstrated in the Kumamoto study [766].
12.4.2 Blood pressure
Hypertension is markedly more common in patients with type 2 diabetes than in the general population [767].
The effect of blood pressure reduction on the risk of developing cardiovascular disease has predominantly been studied in studies including diabetic as well as nondiabetic patients, so most of the existing evidence is based on subgroup analysis from these combined trials.
The UKPDS study randomized patients with hypertension to intensive or less intensive antihypertensive therapy [666]. In this substudy, there was a marked and significant 44% risk reduction for stroke and a nonsignificant 21% risk reduction of myocardial infarction associated with a 10 mmHg reduction in systolic BP and 5 mmHg reduction in diastolic blood pressure.
Subgroup analyses restricted to the diabetic patients in the SHEP study, Syst-Eur and the HDFP study [768–770] consistently show a 30-70% risk reduction in cardiovascular morbidity and mortality, treatment effects were generally bigger than those found in the nondiabetic groups. The Hypertension Optimal Study (HOT) comparing different diastolic blood pressure goals showed the benefit from more aggressive treatment of blood pressure (goal: diastolic BP of 80 mmHg). This resulted in a reduction in cardiovascular events in diabetic individuals compared to nondiabetic individuals [470].
12.4.3 Dyslipidaemia
The Heart Protection Study (HPS) [63] has demonstrated that statin treatment produced in both diabetic and nondiabetic patients a significant 30% risk reduction in CHD and stroke. This study, a randomized controlled trial included almost 6000 type 2 diabetic patients, and almost 4000 of them did not have prior myocardial infarction or angina pectoris. Thereby this study is larger than all previous studies on diabetic patients combined, and in contrast to the previous studies, the study included all ranges of serum cholesterol down to 3.5 mmol/l (∼ 135 mg/dl). The relative treatment effect was independent of baseline cholesterol (although the absolute risk and thus also treatment effect increased with increasing cholesterol). The mean decrease in total cholesterol was 1.1 mmol/l in diabetic patients and 1.2 mmol/l in nondiabetic patients. CARDS, a specifically designed randomized controlled trial to examine the effect of statin treatment in type 2 diabetic patients without clinically manifest CVD, also showed convincingly that LDL-cholesterol lowering with statins reduces the risk of CHD and stroke events [696]. A recent subgroup analysis of 1501 diabetic patients included in the TNT study, which compared intensive statin therapy (atorvastatin 80 mg) to standard statin therapy (atorvastatin 10 mg), showed a reduction in primary events (hazard ratio 0.75 P = 0.026), cerebrovascular events (hazard ratio 0.69 P = 0.037) and all cardiovascular events (hazard ratio 0.85 P = 0.044) in those in the intensive statin therapy group [771].
12.4.4 Antithrombotic therapy
Both type 1 and type 2 diabetes are associated with increased tendency to thrombotic phenomena. When the Anti-Platelet Trialists’ Collaboration demonstrated in their meta-analyses the beneficial effect of the use of aspirin in patients with clinically established CHD, cerebrovascular disease and other forms of atherosclerotic disease [772], they also analysed data from about 4500 diabetic patients included in the trials and concluded that treatment with antiplatelet drugs (mainly aspirin) resulted in a 25% reduction in the risk of cardiovascular events and that the effect would be similar in diabetic and nondiabetic patients. The Antithrombotic Trialists’ Collaboration have, however, now extended their meta-analyses to cover a larger number of trials and diabetic patients and have arrived to a much more modest benefit from antiplatelet therapy in diabetic patients – only a 7% reduction in the risk of cardiovascular events as compared to the overall reduction of 22% in the trials [773]. Importantly, the Early Treatment Retinopathy Study demonstrated that in diabetic patients aspirin therapy did not increase the risk of vitreous or retinal haemorrhage [774]. A new trial examining the role of aspirin in the prevention of cardiovascular events in diabetic patients is in progress in the United Kingdom.
12.4.5 Multifactorial intervention
The typical type 2 diabetic patient suffers from many components of the metabolic syndrome, each of whom should be treated in accordance with existing guidelines. Despite this, very few have been targeted at all risk factors as a ‘treatment package'. The UKPDS [666] included intervention against glucose and hypertension, and demonstrated an effect of both, but was underpowered to be able to evaluate the effect of the combined intervention. The STENO-type 2 study including 160 high-risk patients with type 2 diabetes and microalbuminuria, randomized the patients into standard treatment as provided in general practice or intensive, polypharmaco-logical treatment including insulin, statins, ACE inhibitors, other antihypertensive agents, aspirin, and lifestyle intervention (smoking, physical activity and diet) provided in a specialized diabetes care unit. The benefit of the multifactorial management strategy was demonstrated with a significant difference in incidence of microvascular complications after 4 years [775] and a significant 53% risk reduction in macrovascular complications after 8 years [776]. Thus in high risk patients polypharmacological multitargeted intervention is needed to obtain the maximal risk reduction. It should be underlined that in particular the lifestyle oriented part of this study failed to reach set targets. Thus it may be speculated that an even more effective treatment would have increased the benefit. The ADDITION study is including screen-detected type 2 diabetic patients; this study will tell whether a similar intensive treatment regimen is necessary in the majority of patients with shorter duration of diabetes without signs of late diabetes [777].
12.5 Metabolic syndrome
The name ‘metabolic syndrome’ has been given to a clustering of several cardiovascular risk factors (obesity and its central distribution, elevated plasma glucose, elevated plasma triglycerides, low HDL cholesterol and raised blood pressure). The pathogenesis of the metabolic syndrome is complex and incompletely understood, but insulin resistance and accumulation of intra-abdominal fat tissue are considered to be important underlying factors. There is still an ongoing debate regarding whether this clustering of risk factors really represents an entity in its own right and whether it predicts the risk of cardiovascular disease more strongly than its individual components. The metabolic syndrome has, however, become a subject of great interest because of its association with the risk of development of type 2 diabetes and atherosclerotic CVD.
Several international or national expert groups have during the last years formulated definitions for the metabolic syndrome. The first of them, given by the WHO consultation report in 1999 [778] was primarily intended for research purposes (Table 14). Various modifications of this definition have been widely used in epidemiological research, usually substituting fasting plasma insulin above the highest quartile for insulin resistance (as assessed by hyperinsulinaemic euglycaemic clamp glucose uptake below lowest quartile) and omitting microalbuminuria, as proposed by the European Group for the Study of Insulin Resistance (EGIR) [779]. The definition given by the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) in 2001 [689] was created for clinical use and has become widely adopted. A revised version of the NCEP-ATP III definition was recommended in 2004 by the American Heart Association (AHA) and the National Heart, Lung, and Blood Institute (NHLBI) [780] (Table 15). The newest definition was launched in 2005 by the expert group of the International Diabetes Federation [781] (Table 16). The major components included in these definitions of the metabolic syndrome are more or less similar but there are differences in the emphasis between them and in the diagnostic threshold values given for individual components. The WHO definition includes impaired glucose regulation and/or insulin resistance as a prerequisite. The NCEP-ATP III definition does not have any prerequisite and aims at detection of increased CVD risk. The IDF definition has the presence of central obesity as its starting point.
The WHO definition of the metabolic syndrome

Original and revised NCEP-ATP III definitions of the metabolic syndrome
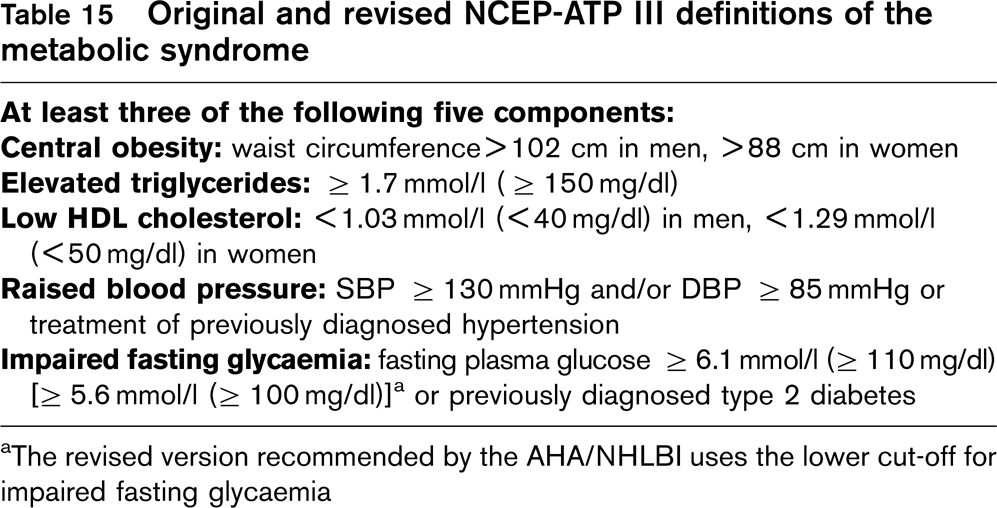
aThe revised version recommended by the AHA/NHLBI uses the lower cut-off for impaired fasting glycaemia
The International Diabetes Federation definition of the metabolic syndrome
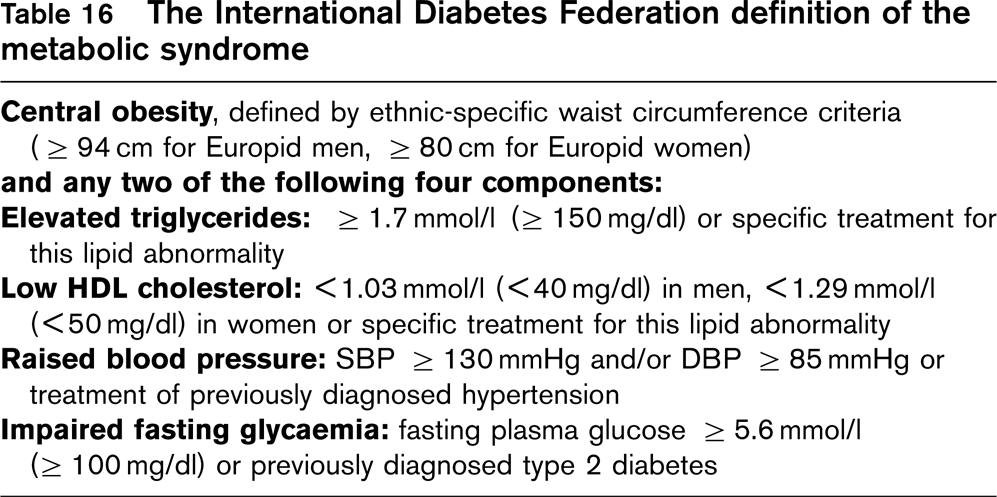
In the revised NCEP-ATP III definition, recommended by the AHA/NHLBI, the cut-off for impaired fasting glycaemia was lowered to ≥ 5.6 mmol/l (≥ 100 mg/dl) following recommendations given by the ADA. If fasting plasma glucose is ≥ 5.6 mmol/l (≥ 100 mg/dl), oral glucose tolerance testing is strongly recommended, but is not necessary to define the presence of the syndrome.
The majority of patients with type 2 diabetes have the risk factor characteristics of the metabolic syndrome and the presence of this risk factor clustering has an adverse effect on their prognosis. The diagnosis of the metabolic syndrome is, however, of greatest importance in nondiabetic patients as an indicator of an increased risk of developing type 2 diabetes and CVD.
In the DECODE Study population, pooling data from nine European population based cohorts of men and women aged 30-89 years, the overall prevalence of the metabolic syndrome was in nondiabetic men with a modified WHO definition 25%, with the original NCEP-ATP III definition 23%, with the revised NCEP-ATP III definition 30% and with the IDF definition 34%. In nondiabetic women the overall prevalence of the metabolic syndrome with these definitions was 18, 21, 26 and 32%, respectively [782]. As can be expected because of differences between the definitions of the metabolic syndrome, their concordance in the identification of subjects with the syndrome is not good. Of all patients fulfilling the criteria for any one of these definitions, only about one third fulfilled the criteria for all the definitions.
Some information is available from prospective cohort studies on the predictive value of different definitions of the metabolic syndrome with regard to the development of type 2 diabetes. A 4-year follow-up study of Finnish middle-aged men showed that men with the metabolic syndrome either with the WHO definition or the NCEP-ATP III definition were at high risk of developing diabetes; the odds ratios were from 5.0 to 8.8, depending on the cut-offs used for the measures of central obesity [783]. In a systematic review and meta-analysis of studies on the relationship of the metabolic syndrome with the original NCEP-ATP III definition to the development of type 2 diabetes the combined relative risk was 2.99 [784].
The relationship of the metabolic syndrome with the risk of CVD has been assessed in many prospective cohort studies, using mainly some modification of the WHO definition or the original NCEP-ATP III definition. A systematic review and meta-analysis of such studies showed that for studies that used the most exact WHO definition the combined estimate of relative risk for CVD was 1.93 and 2.60 for CHD [784]. For studies using the original NCEP-ATP III definition the combined estimate of relative risk was 1.65 for CVD. In the DECODE Study population, combining data from nine European cohorts with a maximum follow-up of 7 to 16 years, the hazard ratios of different definitions of the metabolic syndrome for CVD mortality, adjusting for age, serum cholesterol and smoking, were as follows in men: with the modified WHO definition 2.09, with the original NCEP-ATP III definition 1.74, with the revised NCEP-ATP III definition 1.72, and with the IDF definition 1.51. In women the hazard ratios were somewhat lower: 1.60, 1.39, 1.09, and 1.53, respectively. Some other studies using either the original NCEP-ATP III definition or the modified WHO definition have, however, shown similar or even higher hazard ratios for CVD in women with the metabolic syndrome as compared with men with the syndrome [322, 785–787].
An important issue is whether identification of patients with the metabolic syndrome will bring important additional information about CVD risk over and above that obtained from general multifactorial CVD assessment tools, such as the Framingham or SCORE risk equations based on European cohort study data. This question was addressed in a study based on the follow-up data of the nondiabetic men aged 50-69 years in the DECODE Study population [788]. Of these men 51% had an estimated 10-year risk of CVD death under 5%, using the SCORE risk equation, and 22% of them had the metabolic syndrome with the NCEP-ATP III definition. In these low risk men, the hazard ratio for fatal CVD was 2.71 for men with the syndrome compared to men without the syndrome. A large waist circumference (> 102 cm) carried a hazard ratio of 2.24 in low risk men. In men with a 10-year risk of CVD death ≥ 5%, the presence of the metabolic syndrome did not add substantially to the risk predicted by the SCORE equation. These findings indicate that the diagnosis of the metabolic syndrome may identify patients with increased risk of CVD among those who would become classified as low-risk individuals using conventional tools for CVD risk assessment. A large waist circumference appears to be a useful warning sign and should stimulate assessment of other components of the metabolic syndrome.
12.6 Management of risk in clinical practice
12.6.1 Prevention of diabetes
The optimal way to prevent the increased risk of CVD associated with diabetes would be through prevention of the disease in itself. Studies from China, Finland, USA, Canada and India have consistently shown that prevention or at least retardation of the onset of type 2 diabetes is possible through lifestyle intervention [789–792] but none of these studies were designed and powered to look at the impact on the incidence of CVD. Population-based intervention studies have apparently been successful in preventing CVD, but none of these studies compared the incidence of type 2 diabetes in the intervention and control group [793, 794].
12.6.2 Glucose
There is convincing evidence from randomized controlled clinical trials that good metabolic control prevents microvascular complications in both type 1 and type 2 diabetic patients [666, 764, 765, 795]. The evidence with respect to prevention of macrovascular complications is less convincing, although the UKPDS study strongly indicates that this may be the case.
In patients with type 1 diabetes without nephropathy strict glucose control helps maintain normal plasma lipid levels. Diabetic nephropathy, however, is accompanied by multiple plasma lipid abnormalities which are not fully normalized by good glucose control. In general, plasma lipid abnormalities associated with type 2 diabetes, particularly elevated triglycerides and low HDL cholesterol, are only partially corrected by good glycaemic control. Thus there are good reasons to aim for as good glucose control as can practically be achieved both in patients with type 1 and type 2 diabetes. This may be beneficial for the prevention of CVD manifestations, but this has so far not been studied in a well designed prospective clinical trial. In type 1 diabetes glucose control requires appropriate insulin therapy and concomitant professional dietary therapy. In type 2 diabetes professional dietary advice, reduction of overweight and increased physical activity should be the first treatments aiming at good glucose control. The impact of an effective lifestyle adjustment may be as effective as the prescription of an oral glucose-lowering agent as shown in the UKPDS study [796]. As type 2 diabetes is characterized by progressive loss of β-cell function, treatment with oral hypoglycaemic drugs (sulphonylurea or biguanide or their combination) or insulin has to be added to the treatment regimen. In overweight and obese patients metformin has proved to be the optimal treatment associated with minimal weight gain in combination with the lowest risk of late diabetic complications [765], but apart from this, no specific oral hypoglycaemic agent has proved to be superior in relation to outcome. In patients with very strict metabolic control hypoglycaemia becomes an important issue, and here very short acting sulfonylurea compounds would be preferential [797]. Insulin treatment (alone or in combination with oral hypoglycaemic agents) may be necessary in as many as 50% of the patients [745], and it is essential that barriers to insulin treatment are identified and overcome.
Thiazolidinedione drugs (glitazones) are widely used in the treatment of type 2 diabetes. They act primarily by increasing insulin sensitivity in peripheral tissues. There are currently two agents of this class available: rosiglita-zone and pioglitazone. Both are effective in lowering blood glucose either as mono or as combination therapy, but a very recent meta-analysis questions the safety profile of rosiglitazone with respect to the risk of developing CVD [798]. This question about the safety of rosiglitazione is currently unsettled [799].
Self-monitoring of blood glucose is essential in the treatment of type 1 diabetes to improve the safety and quality of treatment, and is a vital safeguard against serious hypoglycaemia. Self-monitoring may improve therapeutic efficacy and safety and should also be recommended for patients with type 2 diabetes.
There is a broad consensus between different guidelines on the glycaemic targets in type 1 diabetes [5, 800, 801]. Insulin treatment, built upon appropriate nutrition, and tailored on the basis of self-monitoring, which aims at DCCT-aligned HbA1c targets, below 6.5%, has been recommended in patients who are at particularly high risk of CVD – those with clinically established CVD, microalbuminuria or nephropathy, history of early onset CVD and those with risk characteristics of the metabolic syndrome or other CVD risk factors. Age should also be taken into consideration in decisions on targets, because the risk of CVD begins to increase after the age of 35 years. Applying a lower target should be accompanied by increasing caution regarding the avoidance of hypogly-caemic episodes.
In type 2 diabetes, different organizations have recommended HbA1c below 7.0 or 6.5% (Table 17) [800, 802, 803]. There is, however, an increasing consensus that the ideal HbA1c target for the prevention of CVD is below 6.5%. In applying low targets to patients who receive treatment with insulin or drugs stimulating insulin secretion (sulphonylureas, or rapid-acting insulin secretion-stimulating drugs, nateglinide or repaglinide) special attention should be paid to the avoidance of hypoglycaemic episodes with guidance obtained from glucose self-monitoring.
12.6.3 Blood pressure
Targets for blood pressure are generally more ambitious in patients with diabetes. This is first of all due to the fact that very strict control of blood pressure is the most important single factor preventing development of diabetic nephropathy and end stage renal failure [459–461, 573, 804]. Furthermore, subgroup analyses of the diabetic patients in trials focused on prevention of CVD in patients with hypertension have demonstrated more beneficial treatment effects in the diabetic group in the nondiabetic group, and suggests that stricter treatment targets are indicated [470, 768, 805]. The HOPE study showed that in patients with initial blood pressure of 130/79 mmHg a further, small reduction of BP (3/1 mmHg) was associated with a further reduction in cardiovascular risk [573]. The optimal BP levels to be achieved cannot be precisely defined, but values below 130/80 may be desirable in diabetic patients. In diabetic patients with diabetic nephropathy and proteinuria >lg/24h, values as low as 125/75 mmHg or lower are recommended if achievable without unacceptable side effects.
The type of antihypertensive medication also seems to be important. Angiotensin converting enzyme (ACE) inhibitors and angiotensin II receptor inhibitors have proven to be particularly effective in preventing progression from microalbuminuria to overt nephropathy in type 1 as well as in type 2 diabetic patients [459–461, 573, 804]. Thus in these groups of patients, ACE inhibitors and angiotensin II receptor blockers would be preferred as initial therapy; however, most patients will require a combination of two or more drugs [666]. Combination therapy including both an ACE inhibitor and an angiotensin II receptor antagonist has been shown to have additional beneficial effect, over and above the effect of each on progression of diabetic renal disease, and consequently this ‘dual blockade’ principle may be beneficial also in preventing CVD.
Glucose control assessment levels in patients with type 2 diabetes as recommended by different organizations
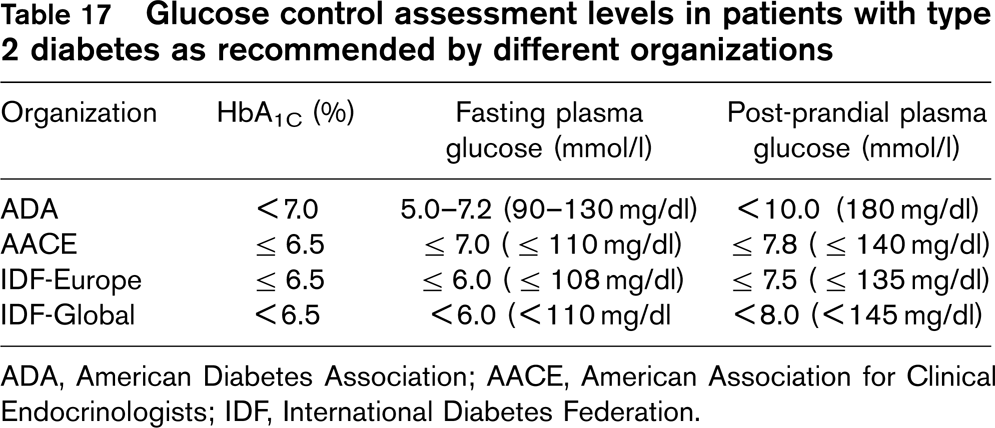
ADA, American Diabetes Association; AACE, American Association for Clinical Endocrinologists; IDF, International Diabetes Federation.
In diabetic patients with hypertension and established coronary heart disease, particularly those who have survived a myocardial infarction and in those with angina pectoris, the use of β-blockers is indicated.
12.6.4 Lipid-lowering therapy
With the Heart Protection Study [63] it became evident that treatment with a statin was effective in reducing the risk of CVD in everyone with a total cholesterol above 3.5 mmol/l (∼ 135 mg/dl). This was true also for the group of diabetic patients, but the number of patients with type 1 diabetes was too small to allow for further subgroup analysis in this group of patients. The next question then is the treatment target. The Heart Protection Study does not provide clarification here. The 2004 recommendations of the Cholesterol Education Program Adult Treatment Panel III (ATP-III) [689] state that diabetes should be considered to be a CHD risk equivalent, which means that individuals with diabetes would have a similar risk of future CHD events as patients with clinically established CHD. This was based on epidemiological data, but as discussed above, later studies have shown that this does not apply uniformly to all patients with type 2 diabetes. Therefore, in ATP-III recommendations, and similarly in the recommendations of the American Diabetes Association, the LDL-cholesterol goals and LDL-cholesterol levels for the initiation were defined to be for diabetic patients similar to those for patients with CHD or other atherosclerotic disease: LDL-cholesterol goal less than 2.6 mmol/l (∼ 100 mg/dL), and LDL-cholesterol level for the initiation of therapeutic lifestyle changes was defined to be ≥ 2.6 mmol/l (∼ 100 mg/dL).
In the absence of studies clearly defining treatment targets and in the presence of the excess risk in patients with diabetes, the treatment target in patients with diabetes should be: LDL-cholesterol less than 2.5 mmol/l (∼ 100 mg/dl) and total cholesterol less than 4.5 mmol/l (∼ 175 mg/dl) irrespective of the presence or absence of CHD or other atherosclerotic disease. But considering findings from some recent studies, particularly CARDS even lower targets [LDL-cholesterol >2.0 mmol/l (>80 mg/dl), total cholesterol >4.0 mmol/l (175 mg/dl)] may be applied, if feasible.
In type 1 diabetic patients with good glycaemic control and without nephropathy plasma lipid levels do not differ much from those in nondiabetic people. However, when nephropathy even its mildest form ensues, plasma triglyceride levels tend to increase and HDL levels which are often somewhat increased in type 1 diabetes tend to decrease. In people with type 2 diabetes LDL-cholesterol levels are similar to those in nondiabetic patients and the most common form of dyslipidaemia in type 2 diabetes is characterized by elevated triglycerides and low-HDL-cholesterol.
Although fibrates theoretically would seem to be the most suitable drug for the dyslipidaemia of type 2 diabetes, the trial experience of their use in the management of dyslipidaemia in diabetic patients has been limited. The recent FIELD-trial testing the efficacy of fenofibrate in Australia and Finland failed to show any significant beneficial effect on the primary end point [734]. Consequently, based on trial experience on efficacy and safety of statins, these are currently recommended as the first choice for lipid-lowering drugs for people with type 1 and type 2 diabetes.
The debate around the aggressive approach for lipid management in diabetic people recommended by Americans still continues in Europe and not all national or other expert groups are ready to underwrite the American recommendations. The main argument for a more individualistic approach is based on the observation that according to epidemiological observations the variation in the multifactorial risk of diabetic individuals is wide, although its distribution is shifted to a higher level than in nondiabetic individuals. The influence of age and gender and the presence or absence of diabetic complications on the benefits of lipid-lowering treatment need to be addressed in more detail on the basis of data from already completed trials and the results of trials which are still going on.
12.6.5 Antiplatelet therapy
As indicated above, recent results reported by the Antithrombotic Trialists’ Collaboration [773] have cast some doubts about the efficacy of antiplatelet therapy in the prevention of CVD events in diabetic patients. The use of aspirin or some other antiplatelet drug, if aspirin is contraindicated, may still be considered in the preventive management in diabetic patients who already have clinically established cardiovascular disease.
12.7 Precursors of diabetes
Impaired glucose tolerance (IGT) and impaired fasting glycaemia (IFG) are both conditions associated with an increased risk of developing type 2 diabetes, and IGT is associated with a deterioration of the cardiovascular risk profile [806] and increased risk of death from all causes as well as from CVD, CHD and stroke [735]. In patients with IGT, several studies have demonstrated that progression to diabetes can be prevented or delayed by lifestyle intervention, and thus these patients should be identified where possible and provided with necessary support.
Increasing levels of metabolic risk factors are seen across the spectrum of nondiabetic glucose values [807], and hyperinsulinaemia is associated with all the components of the metabolic syndrome. Individuals with the metabolic syndrome are at high risk of developing cardiovascular disease, and in these individuals a total risk assessment based on the existing risk engines should be performed to assess risk, and to identify the most important risk factors available for intervention.
12.8 Prevention in patients with the metabolic syndrome
The diagnosis of the metabolic syndrome is of greatest importance in nondiabetic patients as an indicator of an increased risk of developing type 2 diabetes and CVD. It is, however, important to emphasize that interest in the metabolic syndrome should not displace the use of conventional CVD risk assessment tools, such as SCORE and other similar risk scoring tools, from their primary place in the identification of individuals who are at high CVD risk. In fact, the components of the metabolic syndrome, with the exception of the measures of central obesity, triglycerides, IFG and IGT, are included among the risk factor measurements used in conventional risk assessment systems. Adding waist circumference measurement to this set will give possibilities to detect the presence of the metabolic syndrome and help identify people who actually are at high risk of CVD, although they do not get particularly high risk scores in conventional CVD risk assessment. The original and revised NCEP-ATP III definitions and the IDF definition of the metabolic syndrome are suitable for clinical use, but it is important to realise that because of a lowered threshold for IFG in the revised NCEP-ATP III and IDF definitions and a lowered threshold for central obesity in the IDF definition, these definitions will pick up a larger proportion of people and will have a lower positive predictive value than the original NCEP-ATP III definition.
Since lifestyles have a strong influence on all the components of the metabolic syndrome, the main emphasis in the management of the risk in people with this syndrome should be in professionally supervised lifestyle change, particularly directed to the reduction of overweight and increased physical activity. Although the dyslipidaemia of the metabolic syndrome is characterized by elevated triglycerides and/or low HDL cholesterol, lipid management should, however, be steered with LDL-cholesterol goals in mind. Subgroup analyses of large statin trials have shown that coronary heart disease patients with and without the metabolic syndrome get from statin treatment a similar substantial relative reduction of CVD events, but the absolute benefit may be even greater in those with the syndrome, because they are at higher absolute risk [808, 809].
Chapter 13: Psychosocial factors
There is increasing scientific evidence that psychosocial factors contribute independently to the risk of coronary heart disease (CHD), even after statistical control for the effects of standard risk factors [810, 811]. In addition to increasing the risk of a first event and worsening the prognosis in CHD, these factors may act as barriers to treatment adherence and efforts to improve lifestyle, as well as to promote health and well-being in patients and populations. Low socio-economic status, lack of social support and social isolation, stress at work and in family life, and negative emotions including depression and hostility, have been shown to influence both the risk of developing CHD and the worsening of clinical course and prognosis in patients with CHD. Several behavioural and psychophysiological mediators and moderators of these effects have been identified [3, 810], which have already been discussed in the previous guidelines [3].
Evidence is also accumulating of therapeutic and preventive intervention methods that counteract psycho-social stress and promote healthy behaviours and lifestyle [114, 812, 813]. These interventions are likely to have beneficial effects on physiological risk factors [812, 814] and distress. In two meta-analyses and some more recent RCTs they have also shown their potential to prevent the progression of clinical CHD [812–814], especially in white men [815] and in patients who achieved their proximal behavioural goals [813, 816]. However, other studies and one meta-analysis [114] found no such effect. Therefore, the characteristics of successful intervention programs and the question of which intervention should best be delivered to which patient at what time in the disease process still remains to be determined.
13.1 Low socio-economic status
Men and women with low socio-economic status (SES), defined as low education, holding a low status job or living in a poor residential area, have an increased all-cause as well as CHD mortality risk, which is only in part mediated by traditional risk factors [811]. Low SES persons are also more likely to experience low control at work, social isolation and lack of social support, poor capacity to cope with stressors, hopelessness and depressed mood. These mediators can be modified and preventive efforts should be directed towards those of low SES, because they are in greater need. In turn, leaving low SES unrecognized when applying standardized risk charts may underestimate CVD risk in socially disadvantaged persons [817], lead to insufficient preventive efforts and further increase CVD burden in this disadvantaged group.
13.2 Social isolation and low social support
Social support has beneficial effects on lifestyle and health behaviour. People who are isolated or disconnected from others are at increased risk of dying prematurely from ischaemic heart disease [818–820]. Similarly lack of social support leads to decreased survival and poorer prognosis among people with clinical manifestations of CVD [821].
13.3 Psychosocial stress at work and outside work
Stress at work, characterized by combinations of high demand with low control or high effort with low reward, predicts CHD risk [822]. Although these effects are seen in both women and men [823, 824], work stress appears to be more relevant for cardiovascular end points in men than in women [825].
Prolonged exposure to work at irregular hours, including work at night, increases CHD risk, with a higher risk as the number of years in shift work increases [826–828]. A direct and causal effect of shift work on CHD is suggested in women [829] and in men [830].
Conflicts, crises and long-term stressful conditions in family life have also been shown to increase CHD risk, especially in women [825, 831].
13.4 Hostility
Hostility has been identified as a risk factor for CVD [832–836] and for virtually any physical illness, although effect sizes appear to be small [837].
13.5 Depression
Clinical depression, depressive symptoms and other negative emotions have been shown to predict incident CHD [838, 839], and worsen its prognosis [840, 841], independently of standard risk factors. For example, clinical depression is associated with at least doubled risk for major cardiac events. Further evidence suggests that the prevalence of depressive symptoms is higher in women compared to men. Increased risk is mediated by a variety of behavioural and psychophysiological mechanisms. Part of it may also be due to adverse effects mainly of tricyclic antidepressants [842, 843].
In patients with manifest coronary disease, depression has well-documented effects on cardiac symptoms, overall quality of life and illness behaviour (including increased healthcare utilization, low adherence with behaviour change recommendations or cardiac medications, and low rates of work resumption) [844]. Perceived social support seems to counteract the adverse effect of depression [845], whereas lack of support was found to reinforce the effects [846]. Prognostic risk is highest in persons with a combination of chronic negative affectivity and social inhibition [847, 848].
13.6 Clustering of psychosocial risk factors and biobehavioural mechanisms
CVD's multifactorial aetiology and the multiplicative effect of coronary risk factors mean that in attempting to reduce risk we must deal with the whole person and not with isolated risk factors. This principle is no less true when it comes to psychosocial risk factors and the biobehavioural mechanisms which mediate effects on pathogenesis and prognosis. It is now evident that psychosocial risk factors do not occur in isolation from one another, but tend to cluster in the same individuals and groups. For example, both women and men of lower SES are more likely to be depressed, hostile, socially isolated, and to engage in risky health behaviours [849–851]. In addition to risky health behaviours like smoking, high alcohol consumption, and unhealthy nutrition, persons with psychosocial risk factors such as depression are also more likely to express biological characteristics that are involved in promoting cardiovascular disease. Alterations have been found in autonomic function (including reduced heart rate variability), in the hypothalamic pituitary axis (HPA) and other endocrine markers, which affect haemostatic and inflammatory processes, endothelial function, and myocardial perfusion [810].
The tendency of psychosocial risk factors and biobeha-vioural mechanisms to cluster in the same individuals and groups has important implications for strategies to modify risk and improve quality of life.
As persons with high levels of negative affect are more likely to smoke, partly due to an antidepressant-like effect of cigarette smoke [852] attempts to help them quit smoking might be more successful if they include elements designed to reduce hostility and depression. Similarly, attempts to reduce the CVD risk in the socially disadvantaged, might be more effective by incorporating training in skills that will reduce negative feelings and increase access to positive, supportive social ties as well as self-efficacy [853]. In other words, behavioural interventions that reduce levels of psychosocial risk factors are likely to have broad benefits in terms of enabling people to be more successful in modifying unhealthy lifestyles and reducing biological consequences of stress – for example altered haemostatic and inflammatory functions – that are directly involved in pathogenesis.
13.6.1 Interventions to reduce depression and distress
Three recent randomized controlled trials have targeted depression. Coronary patients with clinically significant depression can safely and effectively be treated with psychotherapy [854] or selective serotonin reuptake inhibitors (SSRIs) [855, 856]. The marked improvement in quality of life achieved by these treatments justifies their routine use in depressed patients with coronary artery disease. Although a definite beneficial effect on cardiac end points has not been documented, a recent multicentre clinical trial to decrease depressive feelings and improve social support, found beneficial cardiovascular effects in white men [815]. Results from non-randomized studies indicate that also SSRIs may have the potential to improve CVD prognosis in patients with [857] and without [858] previously documented CVD.
There are several other approaches to psychosocial intervention, which have proved to be useful. Thus it has been shown, in hostile CHD patients [859, 860] that a group based hostility-control intervention may lead, not only to decreases in behaviourally assessed hostility levels, but also decreased depression, resting heart rate and cardiovascular reactivity to mental stress, as well as increased social support and satisfaction with life. Likewise, in group based, psychosocial interventions, an element of increased social support is often the natural consequence. For example, work-reorganizations aimed at improving autonomy and increasing control at work may result in improved social support and reduction in physiological stress responses [861]. Work stress reduction in managers and supervisors may have beneficial health effects on the target individuals but also improve perceived social support in their subordinates [862]. Such effects are likely to contribute to decreased risk and improved prognosis in CHD through their stress reducing components.
Specific behavioural group treatments for women with CHD may be useful for reducing distress and exhaustion [863], although a beneficial effect of prognosis of reducing exhaustion has not been shown so far [864]. In contrast, stress management programs have repeatedly been shown to improve not only subjective well-being but also risk factor levels and CVD outcomes [812, 814].
13.7 Management of psychosocial risk factors
13.7.1 Recommendations for the management of psychosocial risk factors in clinical practice
Assess psychosocial risk factors, for example depression and hostility, low SES, social isolation, and chronic life stress by clinical interview or standardized questionnaires.
Discuss relevance with patient in respect to quality of life and medical outcome.
Prescribe multimodal, behavioural intervention, integrating individual or group counselling for psychosocial risk factors and coping with stress and illness.
Refer to a specialist in case of clinically significant emotional distress.
Recognizing the psychosocial risk associated with depression, hostility, low socio-economic status (SES), lack of social support or chronic psychosocial stress in patients and persons with risk factors may be crucial as a means to reduce risk. Standardized measurements for depression, hostility, SES, social support or psychosocial stress are available in many languages and countries [865].
Alternatively, a preliminary assessment of psychosocial factors can be made within the physicians’ clinical interview, as detailed below.
13.7.2 Core questions for the assessment of psychosocial risk factors in clinical practice
Depression: Do you feel down, depressed and hopeless? Have you lost interest and pleasure in life?
Social isolation: Are you living alone? Do you lack a close confidant? Do you lack any person to help you in case of illness?
Work and family stress: Do you have enough control over how to meet the demands at work? Is your reward appropriate for your effort? Do you have serious problems with your spouse?
Hostility: Do you frequently feel angry over little things? If someone annoys you, do you regularly let your partner know? Do you often feel annoyed about habits other people have?
Low SES: Do you have no more than mandatory education? Are you a manual worker?
For patients with low SES, lack of social support or chronic psychosocial stress, interventions need to focus on these areas in order to improve both their quality of life and medical outcome. If available, patients should be recommended to join a multimodal, behavioural intervention that includes stress management and social reintegration. Whenever possible these interventions should occur on a group basis to enhance social interaction and improve social support. Depression and other negative effects tend to persist or even increase as cardiac disease progresses. While awaiting conclusive results that treating depression will alter CVD prognosis, a prudent approach at present is to offer patients with clinically significant depression treatment with psychotherapy and antidepressant medication, according to established guidelines. Those not accepting treatment should be closely followed and treatment offered again if depression persists for more than 4-6 weeks.
Chapter 14: Inflammation markers and haemostatic factors
Risk factors may be classed into several hierarchical categories as follows: classical, established, emerging, putative and also as risk markers. The highest level of classification achieved thus far by the heterogeneous group of factors discussed in this chapter is ‘emerging’ but many are under active investigation in clinical and epidemiological studies. These factors are associated with many different biological systems such as those regulating platelets, coagulation, fibrinolysis, endothelial function and the inflammatory response. These interact in ways which remain incompletely understood, but in which scientific interest and achievement is considerable. In addition to their potential utility in long-term risk prediction of cardiovascular diseases, close associations between inflammatory markers and obesity and diabetes have been demonstrated, which strengthens the case for their scientific investigation.
There is strong evidence from pathological [866, 867] and epidemiological studies [868–871] that the circulating markers of activated inflammation and haemostasis are closely associated with the development of fatal and nonfatal myocardial infarction. A large case-series, based in a national primary care database, showed that first myocardial infarction and stroke were each more common following recent respiratory or urinary tract infections, the risk being greatest within the first three days after diagnosis (relative risks 5.0 and 3.2 respectively) and falling during the following weeks [872]. A recent report from Europe, as part of the World Health Organization's MONICA study, showed that population levels of certain haemostatic factors differed between participating centres and countries, and showed significant associations with the incidence of coronary heart disease in the centres [873].
Prospective epidemiological studies have also linked inflammatory markers with the development of type 2 diabetes mellitus [874] and interleukin-6, a pro-inflammatory cytokine, with congestive heart failure [875]. Some studies have demonstrated that risk prediction for coronary heart disease, [876, 877] and for both coronary heart disease and stroke [878] can be improved by the addition of these newer risk factors to risk models which include all established risk factors. A recent report in the United States proposed that C-reactive protein (CRP) should be as an ‘option’ in current guidelines [879] but this proposal has been questioned both in the United States [880, 881] and in Europe [882, 883].
Incorporation of CRP and other emerging risk factors into routine practice for prediction of cardiovascular risk may be premature, therefore, and criteria for the rigorous evaluation of such factors have been proposed [884]. These criteria include: applicability to all relevant clinical cardiovascular events; ability to predict in short, intermediate and long-term follow-up; standardized measurements; examination of variability; the degree of correlation with established risk factors; and improvement in overall prediction, among other criteria. A number of meta-analyses of observational epidemiological studies have been conducted for example, for CRP [885] and for fibrinogen [886]. Such meta-analyses will provide evidence of possible utility of emerging risk factors in future clinical practice; but current investigation of determinants of inflammatory markers, which include physical activity [887], dietary factors, [888] alcohol [889] and weight loss [890] as protective factors, and infections such as periodontitis as a potentially treatable risk factor, [891] encourage the detailed examination of this group of markers in future research.
Another important point regarding these meta-analyses of CRP, fibrinogen and possibly other biomarkers is that they are often seriously confounded by other unmeasured variables and subject to reverse causality; for example, preclinical disease may increase CRP. Consequently, even large scale meta-analyses, like those cited above, may fall into the trap of promoting the idea that the evidence of a causal link is strong. An alternative approach, using Mendelian randomization, has been carried out by several groups, demonstrating that predicted associations between CRP genotypes that code for higher levels of circulating CRP are not associated with CVD or risk factors [892–894]. A large meta-analysis of 7 haemostatic genes showed that variance of Factor V gene and the prothrombin gene may be moderately associated with risk of coronary disease [895].
Chapter 15: Genetic factors
Why screen close relatives?
Close relatives of patients with premature CVD and persons who belong to families with inherited dyslipidaemias such as familial hypercholesterolaemia are at increased risk of developing CVD and should be examined for all cardiovascular risk factors.
Chapter 15: Genetic factors
Genetic information may be divided into three categories: information on family history, information on phenotypes, and information on genotypes. All three types of information may be useful to identify patients who are at high inherited risk of developing CHD, and who may therefore warrant earlier or more aggressive therapeutic intervention to reduce modifiable risk factors (e.g. plasma cholesterol or blood pressure). Information on phenotypes and genotypes in combination may be particularly useful in guiding the particular therapeutic approach of choice.
15.1 Family history
The importance of a family history of CHD as a coronary risk factor has been established by a number of studies, and is included as a risk factor in some risk prediction algorithms such as PROCAM [896]. The size of the risk associated with a family history of early CHD (usually defined as evidence of CVD or CHD in a first degree male relative >55 years and female relative >65 years) is in the range 1.5-1.7, and is independent of classical CHD risk factors including blood lipids, blood pressure, body mass index etc. [897, 898]. Although some studies find that risk is higher if found in a female relative, not all studies report this [899]. Based on this, a detailed family history of CHD, or other atherosclerotic disease should be part of the assessment of all patients with CHD and in the identification of high-risk individuals.
The risk of CHD increases (i) when an individual is closely related to a family member who has developed CHD. A history of CHD in a first degree relative (parents, brother or sister, or son or daughter) is more important than a similar history in a second degree relative (grandparent, aunt, uncle) or in a third degree relative (cousin); (ii) as the percentage of family members with CHD increases; and (iii) the younger the age at which family members develop CHD. For example, one study has found that, among women with a low Framingham risk score, carotid thickening was greater in those with a family history of CHD [900].
15.1.1 Recommendation
Risk factor screening should therefore be carried out in the first degree relatives of any patient developing coronary disease before 55 years in men and 65 years in women. A family history of premature CHD should also be taken into account in assessing the risk of developing the disease in a healthy individual, including the taking of detailed history and drawing of a pedigree. Lifestyle advice and, where appropriate, therapeutic management of risk factors should be offered to members of families where coronary disease is highly prevalent.
15.2 Phenotypes
We now know that the pathophysiology of CHD is characterized by a combination of acute events, such as plaque rupture, thrombosis and vasoconstriction, acting on a substrate of chronic processes, such as dyslipidaemia, hypertension, endothelial dysfunction, diabetes, cardiac and vascular hypertrophy and atherosclerosis. The study of the genetic determinants of all of these ‘phenotypes’ is therefore likely to be clinically relevant, and each will have their own genetic and environmental determinants.
For many of these phenotypes (measurable traits) there is good evidence for a relatively strong genetic contribution to the determination of levels, which is usually estimated by ‘heritability'. For apoproteins and lipid traits heritability varies between 40-60%, [901] meaning that genetic factors are determining around half of the between-individual differences and environmental factors the remainder. While there is less evidence for the heritability of exciting emerging risk factors such as intercellular adhesion molecule (ICAM), interleukin 6 (IL6), phospholipase A2 (PLA2) etc., the data available also suggests moderate to high heritability [902, 903]. For one established risk factor, plasma Lp(a), heritability is reported to be >90%, [904] and interestingly, variability at the locus coding for the apo(a) gene itself accounts almost all of the variance of plasma Lp(a) in normal populations [905]. Since meta-analyses show that levels of Lp(a) in the top tertile are associated with a 1.6-fold greater risk of CHD, [683] an effect which is of similar magnitude as smoking, the (a) gene would appear to be a major genetic factor for CHD.
15.3 Genotypes
A gene may predispose to CHD if it occurs in functionally different forms. With the publication of the entire human genome sequence, showing that there are 25 000 different genes, and the development of the Human Genetic Diversity database, the tools are now available to explore the impact of these variations on human disease. Functional polymorphisms are relatively common and may have neutral, beneficial or detrimental consequences if they affect regulatory or coding regions of genes. Genetic polymorphisms are defined as sequence variants that occur at a frequency greater than 1%. These include single nucleotide polymorphisms (SNPs) as well as insertion/deletion and copy number variants which have recently been reported to be much more common than previously appreciated [906]. SNPs have been used with increasing momentum to study the genetic determinants of complex diseases such as CHD, in case-control analyses and association and linkage disequilibrium studies with intermediate traits. The important issue is whether and under what circumstances such genetic information will be useful for diagnosis and patient management.
In general, the levels of CHD risk traits are influenced by both environmental and genetic factors with, in most individuals, gene variants of small or modest impact being involved. Thus an individual with, for example, high plasma cholesterol may have inherited several ‘raising’ alleles acting in combination, or they may have few such alleles but eat a cholesterol-raising diet, but most likely they have a combination of both influences. Thus, the identification of the complete list of the genetic variants that an individual has inherited should be of diagnostic or prognostic value, but how this genotype interacts with the environment of the individual will also need to be taken into account. This concept of Gene-Environment interaction is key to being able to use genetic information for accurate risk estimation [907]. In practice it means that a particular genotype will predispose to elevated CHD trait levels and thus CHD risk only in a certain environment (for example in smokers or hypertensive individuals, or those with diabetes). Understanding such interactions is likely to be of major research importance in future years, since these interactions shed light on pathophysiological processes.
A large number of ‘candidate’ genes have already been investigated in relation to CHD traits and to risk of CHD itself, and a comprehensive list is beyond the scope of this report. One of the problems in the field is that many initially exciting findings of large risk associated with a particular SNP have failed to be confirmed in later studies, [908] or at least the later reported effects are much smaller than originally found (the so-called ‘winners curse'). To overcome this meta-analyses have been used to obtain a statistically robust estimate of these effects, and several variants in genes involved in lipid metabolism [e.g. apolipoprotein E (apoE), apolipo-protein B (apoB), lipoprotein lipase (LPL), cholesterol ester transport proteins (CETP)], coagulation [plasminogen activator inhibitor 1 (PAI1), glycoprotein IIbIIIa (GIIbIIIa), factor V (FV)] and different aspects of endothelial function [endothelial nitric oxide synthase (eNOS), methylenetetrahydrofolate reductase (MTHFR), angiotensin converting enzyme (ACE)] [909] appear to be associated with statistically significant although rather modest effects on risk. For example, for the common ApoE protein variants (E2, E3 and E4), there is a strong and consistent impact on plasma lipid levels (E2 lowering and E4 raising), which translates into a modest E2 lower and E4 higher impact on CHD risk such that this genotype may explain 5-8% of the attributable risk of CHD in the population [910].
The ACE polymorphism has probably been the most extensively studied polymorphism so far, in relation to preclinical phenotypes and cardiovascular end points. One important feature of this polymorphism is that it appears to be a response modulator to a wide range of inducing factors. For example, it has been reported to modify the hypertrophic response of the heart to physical training, [911] the restenotic process after stent angioplasty, [912] the evolution of cardiac function after myocardial infarction [913] and the survival of patients with congestive heart failure, [914] and with the development of diabetic nephropathy and retinopathy [915] and with the risk of CHD in smokers [916]. Other candidate gene polymorphisms may also have the characteristic of being response modifiers to a number of stimuli.
CETP and alcohol dehydrogenase genotypes modify the relationship between alcohol consumption and plasma HDL-cholesterol [917, 918] and an amino acid variant that causes enzyme instability in the MTHFR protein affects the relationship between folate intake and plasma homocysteine [230]. These interactions also need to be more widely replicated in larger studies but if confirmed they offer potential prospects for CHD prevention through the identification of responders to deleterious factors or beneficial ones (drugs for example) by genotyping appropriate candidate genes.
15.4 DNA-based tests for risk prediction
Currently available CHD risk prediction algorithms [896, 919] have a very low prediction rate, (for example 11% in a 10 year follow up of UK healthy men [920]. The addition of genetic markers to the current panel of classical risk factors is an area of potential promise for clinical application [907]. Although, individually, the impact of any one genotype on risk is modest, when such risk-genotypes are common their combination may have a strong predictive power. Modeling has suggested [921] that only around 20 genes are usually needed to explain 50% of the burden of a disease in the population if the predisposing genotypes are common (> 25%), even if the individual risk ratios are relatively small (i.e. increasing risk by only 20-50%). Thus the combination of 10-20 meta-analyses confirmed SNPs may have good clinical utility, as has been suggested recently [922]. Recently a combination of SNPs in three meta-analyses proven genes has been reported to be of utility in identifying individuals at risk of type 2 diabetes, [923] confirming the potential of such an approach.
15.4.1 Recommendation
In individuals in the general population, DNA-based tests do not, at the present time, add significantly to diagnostic utility or patient management, over-and-above the use of measures of established CHD risk factors [924]. In the longer term, understanding disease aetiology in terms of genetic determinants may be useful in identifying high-risk individuals and adapting therapeutic management to the individual's genetic make-up.
15.5 Pharmocogenetics
Much has been written about the potential of pharmacogenetic testing to inform therapy based on an individual's genetic makeup, and to decide the most effective choice of available drugs, or to avoid dangerous side effects. Currently, there is little hard data for either in the field of cardiovascular disease. The usual approach has been opportunistic use of drug trials in unrelated patients, and to look for differences in response or outcome by ‘candidate gene’ genotype, for example genes coding for drug metabolizing enzymes (activators and metabolizers), and enzymes and receptors involved in lipid metabolism, adrenergic response, etc. As with all association studies, initially promising results have often failed the test of replication in larger studies, and the relationship between the CETP Taq-I variant and response to statins has now been disproved [925]. The strongest data to date is the report [926] of a poorer cholesterol-lowering response to Pravastatin in the 7% of patients carrying a certain haplotype of the HMG CoA reductase gene (14% fall versus 19%), but if this is overcome simply by a higher dose, it is of little clinical relevance. Currently, the best example of avoiding side effects is determining genotype at the CYP2C9 locus with respect to warfarin treatment, since carriers for functional variants (> 20% of the population) require lower doses for optimal anticoagulation, and homozygotes, although rare, may well experience serious bleeding if given a usual dose [927]. The full potential of this field will only be realised with much further work.
15.6 Severe familial dyslipidaemias and CHD
There are many extremely rare inherited conditions where plasma lipids are abnormal and CHD risk is altered. Here we focus on only the three most common of these.
15.7 Familial hypercholesterolaemia (FH)
FH has an estimated prevalence of 1/500, [928] but may be much higher in some populations which recently increased in size (e.g. French Canadians, Afrikaners and Lebanese), as a consequence of the so-called founder effect. It is characterized by hypercholesterolaemia due to elevated plasma LDL levels, xanthomas, premature CHD and a family history of one or more of these. Angina, heart attacks or death typically occur in men between 30 and 50 years, and in women between 50 and 70 years, [929] and those who smoke, are hypertensive or have other risk factors are at particularly high risk. Several slightly different methods or scoring systems have been developed for the clinical diagnosis of definite, possible or suspected FH patients, [930–932] each have strengths and weaknesses, and have different sensitivity and specificity compared to the ‘gold standard’ of the presence of a detectable disease-causing DNA change [933]. It is likely that a combination of clinical, biochemical and DNA methods will give the highest clinical utility.
FH is present in 5-10% of individuals who develop CHD under the age of 55 years [929]. Thus the early identification of FH individuals will allow changes in lifestyle, including dietary intervention and smoking cessation advice as well as for drug treatment, and these measures, particularly statin treatment, will lead to a longer healthier life [934]. Statin therapy is warranted even in young FH individuals who currently have no evidence of CHD because of their high lifetime risk. Cost-benefit modeling has demonstrated the effectiveness of cascade testing in the relatives of FH patients, [935, 936] and an active program in The Netherlands has been particularly successful in identifying FH relatives in this way [930]. Similar programs are underway in several countries in Europe [937–940].
FH is an autosomal dominant inherited disorder and is usually caused by a mutation in the low-density lipoprotein receptor gene (LDLR). To date over 700 different mutations have been identified world-wide (see http://www.ucl.ac.uk/fh) although the spectrum within a single country is much smaller [940, 941]. Screening for deletions and rearrangements of the LDLR gene using a technique called multiplex ligation-dependent probe amplification (MLPA) [942] has become available, and it is known that up to 5% of FH patients may have such a deletion [943].
It is now known that mutations in at least two other genes can also cause similar symptoms and in approximately 3% of FH patients in the United Kingdom, North Europe and the USA a defect has been detected in the apolipoprotein B-100 gene (apoB), the ligand for the LDL-receptor. This disorder has been designated familial defective apolipoprotein B-100 (FDB) [944]. FDB appears to be somewhat milder in its expression that LDLR but hypercholesterolaemia occurs in childhood, and early CHD is frequent. Recently, defects in a third gene causing monogenic hypercholesterolaemia have been identified [945]. The gene called protein conver-tase subtilisin/kexin type 9 (PCSK9), codes for an enzyme that has also been called ‘neural apoptosis regulated convertase 1’ (NARC-1) which has recently been proposed to be involved in degrading the LDL-receptor protein in the lysosome of the cell and preventing it recycling [946]. Gain of function mutations in the PCSK9 gene could therefore cause increased degradation of LDL-receptors, reduced numbers of receptors on the surface of the cell and monogenic hypercholesterolaemia. An alternative mechanism for the hypercholesterolaemic effect has also been proposed, whereby the gain of function causes increased secretion of apoB-containing lipoproteins from the liver, with this being supported by in vivo turnover studies in patients carrying PCSK9 missense mutations [947] and by in vitro studies in transiently transfected rat liver cells [948]. One mutation in this gene, p.D374Y, has been reported in several independent families [945, 948–951] and appears to be associated with particularly high levels of untreated LDL-cholesterol levels and severe and early CHD, and poor response to statins. Finally, a recessive form of hypercholesterolaemia has been reported, caused by defects in a chaperone protein [952]. The frequency of this is unknown but it appears to be rare.
Since cholesterol levels in FH and non-FH subjects overlap, molecular genetic testing can be useful in the correct diagnosis of relatives in such families [953, 954].
Using currently available routine clinical genetic diagnostic techniques [931, 941], it is possible to demonstrate a mutation in the LDLR, PCSK9 or APOB gene in many of these patients, but this is usually only available in a research setting. Such specialist services are available in several European countries [937–941], but each country should have its own programme for genetic testing for FH because the spectrum of mutations varies between countries. Current data strongly suggests that DNA testing for FH complements cholesterol measurement in cascade screening to identify affected individuals unambiguously [955, 956]. However, an LDLR mutation is not found in all patients with a clinical diagnosis of FH, with reported detection rates being in the range of 60-90% depending to some extent on the molecular techniques employed, and the patients selection criteria. Detection rate is highest in those with a diagnosis of definite FH and lowest in those with only suspected FH [933, 941].
Although patients with no identified mutation may have a monogenic cause of the disorder in a yet-to-be discovered gene, it is also possible that some may have polygenic hypercholesterolaemia and have been misclassified using current clinical diagnostic criteria. These individuals would be expected to have a milder degree of hyper-lipidaemia, possibly not present from birth but only developing in later life, and would therefore be predicted to have a lower risk of CHD. In support of this, the CHD mortality risk in possible FH patients has been reported to be lower than in definite FH [957].
Current data supports the implementation of cascade testing for FH as being feasible and cost-effective but national implementation is limited to a small number of countries [956]. Funding and the infrastructure to support it may be the major stumbling blocks in implementing this in many countries. Concerns about the ethics of carrying out cascade testing, [958] and the potential psychological damage of cascade testing appear to have been largely dealt with [956].
15.7.1 Recommendation
Because of their high CHD risk, patients with FH should be aggressively treated with statins at a young age, preferably in an experienced lipid clinic setting. Lifestyle advice should be offered and supported. Cascade testing to identify affected relatives should be undertaken. For optimal diagnostic and management results, both phenotypic and genotypic diagnosis may be considered.
15.8 Familial combined hyperlipidaemia (FCH)
This is the most common of the severe hyperlipidaemias, with a prevalence of perhaps 1/100 [959]. The genetic inheritance pattern is not as clear-cut as seen for FH, and a FCH is likely to be more polygenic/multifactorial than FH, but the identification of the gene(s) involved in a particular patient is likely to be of clinical utility, whether the disorder is caused by a ‘major gene’ or the interplay of several. Recently a major gene determining the FCH phenotype has been found in Finnish families, identified as the gene for Upstream Regulatory Factor 1 (USF1) – a major controller of lipid and glucose homeostasis [960]. In the liver, USF1 regulates the glucose-responsive expression of fatty acid synthase (FAS), a key enzyme in lipogenesis. USF1 also functions in adipose tissue and the pancreas, two organs heavily involved in metabolic homeostasis. Despite no specific mutation within USF1 being identified in FCH patients, a common haplotype composed of several SNPs is associated with risk of developing FCH [961]. To what extent these findings can be extrapolated to other populations is currently unclear [962]. Modifying genes, especially influencing the high triglyceride trait, include APOC3 and APOA5, [962] the latter representing a downstream target of USF1 and implying a USF1-dependent pathway in the molecular pathogenesis of dyslipidaemias.
15.8.1 Recommendation
Because of their high CHD risk, patients with FCH should be treated with lipid-lowering therapy and lifestyle advice. There is currently little experience to support the clinical utility of cascade testing to identify affected relatives but this is likely to be beneficial.
15.9 Familial HDL deficiency Syndromes
Since the inverse and independent association between HDL-cholesterol and the risk of fatal and nonfatal CHD events has been established by clinical and epidemiological studies, low HDL cholesterol, most frequently defined as an HDL-cholesterol level less than 35 mg/dl (∼ 0.9 mmol/l), has become part of the multiparametric algorithms used for cardiovascular risk estimation [896, 919]. Familial defects that cause particularly low HDL levels, although rare, are therefore clinically important. Patients with HDL-cholesterol levels below the 5th percentile within a given population can be assumed to have Monogenic High Density Lipoprotein (HDL) deficiency [963]. These include defects in the genes of apolipoprotein A-I (apoA-I), adenosine tripho-sphate binding cassette transporter A1 (ABCA1) or lecithin:cholesterol acyltransferase (LCAT). Definitive diagnosis requires specialized biochemical tests and the demonstration of a functionally-relevant mutation in the appropriate candidate genes [963].
15.9.1 Recommendation
Once secondary causes have been ruled out, patients with a virtual absence of HDL must undergo careful physical examination for the clinical hallmarks of certain HDL deficiency syndromes. Family studies should be initiated, to demonstrate the vertical transmission of the low HDL cholesterol phenotype. Since currently there is no routinely-used drug available to increase HDL-cholesterol levels in patients with familial low HDL cholesterol, prevention of CVD in these patients should have the aim of the avoidance and treatment of additional risk factors.
15.10 Coagulation disorders
Although familial monogenic disorders have been identified they are mostly extremely rare. However, more common mutations in the genes for clotting factor V (R506Q designated factor V Leiden) and for prothrombin (G20210A) have been identified, each with a carrier frequency of 2-3%, In a recent meta-analysis the perallele relative risks (RR) for coronary disease of factor V 1691A and of prothrombin 20210A were 1.17 (95% CI 1.08-1.28) and 1.31 (1.12-1.52), respectively [895].
Chapter 16: New imaging methods to detect asymptomatic individuals at high risk for cardiovascular events
Unfortunately, sudden cardiac death is for many individuals the first manifestation of cardiovascular disease. In others a large myocardial infarction or a severe stroke may result in serious disability for the rest of their life. Therefore, one could think of a CVD detection programme as having the following objective: to identify those apparently healthy individuals who have asymptomatic arterial disease in order to slow the progression of atherosclerotic disease, to induce regression and in particular to reduce the risk of clinical manifestations.
The medical technology to detect atherosclerotic arterial disease is already available. However, during the last years an increasing number of modalities have been developed and, in some, their role in population screening has not yet been clearly evaluated.
Different criteria should be met, including:
The noninvasive technique for detecting arterial disease is valid, precise, easy and acceptable.
The relationship between arterial disease detected noninvasively and the development of symptomatic CVD has been quantified.
There is a defined screening strategy and a defined intervention and follow-up policy.
Screening and intervention result in reduction of CVD events.
Screening has no adverse effects. (It should be noted that some of the imaging modalities may use pharmaceutical agents.)
For coronary artery disease, the consequences of coronary atherosclerosis can be objectively assessed noninvasively, using a variety of techniques such as bicycle or treadmill exercise ECG testing, stress echocardiography or radionuclide scintigraphy. These techniques are routinely used in diagnostic work-up programmes in the clinic; they have rarely been used in the population as screening tools. More recently, new techniques have become available to detect coronary lesions.
These new tests are based on the principle that atherosclerosis is a systemic disease of the arterial tree, with preferential involvement of the aorta and its large branches, coronary arteries, cerebral arteries, and lower-extremity arteries. Pathology studies have documented that levels of traditional risk factors are associated with the extent and severity of atherosclerosis. However, at every level of risk factor exposure, there is substantial variation in the amount of atherosclerosis. This variation in disease is probably due to genetic susceptibility combinations of different risk factors and interactions between genetic and environmental factors. Thus, measurements of subclinical disease, representing the current effect of risk exposures, may be useful for improving CHD risk prediction. Noninvasive tests such as carotid artery duplex scanning, electron beam computed tomography (EB-CT), multislice computed tomography (MS-CT), ankle/brachial blood pressure ratios, and magnetic resonance imaging (MRI) techniques offer the potential for directly or indirectly measuring and monitoring atherosclerosis in asymptomatic persons.
16.1 Early detection of CVD in asymptomatic patients with MRI
MRI has been evaluated as a means of assessing the presence or absence of coronary artery stenosis. The value of this technique in detecting coronary artery stenosis is still in question [964–968]. Although the coronary arteries can be visualized in certain patients with the use of MRI, the sensitivity, specificity and robustness of this technique is not high enough to perform screening for coronary stenoses in asymptomatic people.
A potentially more useful approach for risk stratification is to perform in vivo imaging of the arterial wall using MRI. In vitro, MRI is able to differentiate between the plaque components of carotid, aortic, and coronary artery specimens obtained at autopsy [969–971]. Moreover, it has become possible to noninvasively depict coronary plaques by MRI [972–976]. Using optimized 3D imaging sequences to improve contrast between lumen and vessel wall, a spatial resolution of 0.66 × 0.66 × 2 mm3 can be obtained [974]. Regression of the lipid component of atherosclerotic plaques induced in animal models can now be demonstrated by serial in vivo MR examinations [977]. The current fast technical improvement has led to three-dimensional black blood vessel wall imaging which permits in vivo distinction between ‘normal’ and diseased vessel walls [978, 979]. Carotid, aortic and even coronary plaque assessment with MRI may soon lead to its use as a screening tool for quantifying subclinical disease, predicting future cardiovascular events and evaluating therapeutic interventions. For the present moment MRI is a promising research tool, but its use is limited to only a small number of research laboratories at this time. Thus, MRI is not yet appropriate for use in identifying patients at high risk for CAD. The Prevention Conference V participants [980] have recommended that more studies of MRI in CHD risk prediction should be encouraged. Additional technical development in this area is expected and should be of considerable value in the application of this emerging technology.
16.2 Quantitative assessment of coronary calcifications for the detection of asymptomatic high risk individuals
Coronary calcifications represent atherosclerosis of coronary arteries. Normally, they occur exclusively as atherosclerotic lesions within the intima layer and are not found in healthy coronary vessel walls [981–984]. On the other hand, atherosclerotic diseased coronary arteries do not necessarily always show calcifications. The extent of coronary calcifications correlates with the extent of the total coronary plaque burden [981, 982, 985]. It should be noted that coronary calcification is neither an indicator for stability nor instability of an atherosclerotic plaque [986–992]. The inflammatory component has been emphasized for patients with acute coronary syndrome, [993] underlining the concept of evaluation of the total coronary plaque burden by quantification of coronary calcium burden [988, 994].
The visualization of coronary calcium by means of fluoroscopy is not sensitive enough to detect clinically relevant information at early stages [995]. Recent developments in technology of the classic CT resulted in multislice CT-devices [996]. With the use of MS-CT it is possible to obtain a clear definition of the coronary vessels in most patients. However, the highest value of this technique seems to be its negative predictive value, reaching close to 98% in some studies. This very high negative predictive value of the technique leads to the consideration of using MS-CT for screening in certain subsets of high risk population. Still we need prospective studies to clearly determine which population may benefit most from this technology. In addition to that, coronary calcium score may be also reconsidered since the current technology provides more detailed information than was available in past years. If coronary calcium scanning is applied inappropriately, the proof of coronary calcium may lead to an unnecessary increase of diagnostic cardiac catheterizations or even coronary interventions in asymptomatic persons. Therefore, even in the presence of coronary calcium with its prognostic implications, the decision for coronary angiography remains unchanged and depends on the presence of angina pectoris and/or objective myocardial ischaemia [997–1012].
The Agatston score is the most widely used method of quantifying calcium on EBCT scan. Although today the prognostic impact of the Agatston score has been proven and accepted, one has to ask the key question whether the Agatston score is independent of the classical risk factors, meaning that the Agatston score provides additional clinically relevant information [994, 1013–1016]. Some publications supply an answer to this question: the Agatston score is an independent risk factor regarding the extent of coronary artery disease [1013, 1017–1022] and regarding prognostic impact; [997, 1001, 1021, 1023] for example, two men of the same age and identical classical risk profile may show an eightfold different risk of a coronary event [1023]. Aside from one study in older, high-risk patients, [1000] all studies showed that the prognostic value of coronary calcium offers information beyond the conventional risk factors [990, 1001, 1002, 1024]. The Rotterdam calcification study showed that the upper percentile range reflects a 12-fold increased risk of myocardial infarction – independent of the classical risk factors – even in elderly people [1025]. The calcium score also adds important prognostic information to the measurement of C-reactive protein [1026]. Furthermore, the extent of coronary calcium seems to reflect genetic components [1027]. Even psychosocial factors seem to play a role in the presence and extent of coronary calcification [1028, 1029].
16.2.1 Clinical indications
Although calcium scanning is widely applied today, it should not be uncritically used as a screening method. There is a need for prospective studies that will show the clear benefit on individual subgroups in which MS-CT scan is useful. Prospective studies proving the value of coronary scanning and unequivocally resulting in a class I indication with evidence class A for some indications, however, do no exist. With today's knowledge, these studies may be even considered unethical. According to American College of Cardiology/American Heart Association (AAC/AHA) guidelines, coronary calcium scanning can be performed in selected asymptomatic individuals, if a comparison with classic risk factors leads to expected additional analysis information for therapeutic strategies [1030]. Coronary calcium scanning is thus especially suited for patients at medium risk [1016, 1024, 1030–1034]. The US Society of Atherosclerosis Imaging recommends coronary calcium scanning as the initial diagnostic test in individuals 65 years old with symptoms atypical for angina and unknown CAD [1035]. If coronary calcium is not present, the decisions regarding necessity and extent of primary prevention are made based on the analysis of the classical risk factors.
16.3 Carotid ultrasound
Population based studies have shown a correlation between the severity of atherosclerosis in one arterial territory and involvement of other arteries [526]. The detection of atherosclerotic lesions in legs or carotid arteries is more accessible for noninvasive examinations than coronary or intra-cerebral arteries. Therefore, early detection of arterial disease in apparently healthy individuals has also focused on the peripheral arterial territory and on the carotid arteries.
Sonography of superficial arteries is a relatively inexpensive means of noninvasively visualizing the lumen and walls of arteries which are involved in the ubiquitous process of atherosclerosis. Risk assessment using carotid ultrasound focuses on measurement of the intima-media thickness (IMT) and plaque characteristics.
16.3.1 Intima-media thickness (IMT)
IMT is an integrated measurement of the involvement of both the intima and the media in the atherosclerotic process. Current ultrasound instrumentation with transducers ≥ 8 MHz is capable of identifying the borders between the vessel lumen and the intima as well as between the media and the adventitia. The two arterial interfaces are measured in both carotid arteries on the distal straight 1 cm of common carotid arteries, the carotid bifurcations, and the proximal 1 cm of the internal carotid arteries. The carotid intima-media thickness is determined as the average of 12 measurements (both sides 6 measurements each from the near and far wall of each of the three segments). B-mode ultrasound is a valid and reliable technique for measuring IMT [1036]. Reproducibility of measurements is best for the carotid arteries of normal persons.
Although there is a graded increase of cardiovascular risk with increasing IMT, a value >1.3 mm for IMT is considered abnormal. Persons without known cardiovascular disease with increased IMT are at increased risk for cardiac events and stroke [778]. Although the relative risk for events is slightly lower after statistical correction for the presence of traditional risk factors, the risk remains elevated at higher IMT [526, 778].
When IMT is used to predict the incidence of subsequent stroke, the risk is graded but nonlinear with hazards increasing more rapidly at lower IMTs than at higher IMTs [90]. Therefore, precision of measurements is of greatest importance in the sub millimetre range which poses high requirements on instruments and physicians. The risk of cardiac events over 4-7 years of follow-up in patients free of clinical coronary artery disease at baseline is also nonlinearly related to IMT [1037]. In the ARIC-study [1038] the hazard rate ratio comparing mean IMT of ≥ 1 mm to >1 mm was 5.07 for women (95% CI 3.08-8.36) and 1.85 for men (95% CI 1.28-2.69). The strength of the association was reduced by including major CHD risk factors, but remained elevated at higher IMT. The low hazard rate ratio in men indicates that the predictive power of IMT measurements is limited. However, it may be useful not to use IMT measurements to make decisions about normal and abnormal but include them in a risk assessment model.
16.3.2 Plaque characteristics
Recently, plaque characteristics as assessed by carotid ultrasound were found to be predictive of subsequent cerebral ischaemic events [1038]. Patients with echo lucent stenotic plaques had a much higher risk of stroke and cerebrovascular events than patients with other plaque types. On B-mode ultrasound assessments, lipids, thrombi, and haemorrhage all will appear as echolucent structures. As haemorrhage seldom occupies >2% of total plaque size, lipids and thrombi which are plaque components known to be associated with unstable coronary disease most likely are the major components of dangerous plaques in carotid system.
Thus, ultrasound imaging of the carotids is a noninvasive means of assessing subclinical atherosclerosis. The extent of carotid IMT is an independent predictor of cerebral and coronary events but seems to be more predictive in women than in men. Consequently, carotid ultrasound can add information beyond assessment of traditional risk factors which may help to make decisions about the necessity to institute medical treatment for primary prevention. One limitation of using carotid ultrasound for global risk assessment is the absence of reliable data relating IMT numbers to 10 year event rates. Therefore, it is currently not clear how IMT measurements can be formally incorporated into existing risk algorithms used in asymptomatic persons.
16.4 Ankle-brachial index (ABI)
16.4.1 Technical background
The measurement of the ankle-brachial blood pressure index (ABI) is an easy-to-perform, inexpensive and reproducible noninvasive test to detect asymptomatic atherosclerotic disease. Technical requirements are a regular blood pressure cuff and a doppler ultrasound device to measure the SBPs in left and right brachial arteries as well as both posterior tibial and dorsalis pedis arteries [980].
16.4.2 ABI as a measurement of peripheral artery disease (PAD)
An ABI less than 0.9 reflects ≥ 50% stenosis between the aorta and the distal leg arteries. Because of its high sensitivity and specificity (> 90% respectively), an ABI >0.90 is considered a reliable sign of peripheral arterial disease [536, 1039, 1040]. Its high specificity is partially explained by the fact that the ABI may paradoxically be elevated with age-dependent increased arterial stiffness, including arterial calcification. Therefore, an ABI >1.5 may be difficult to interpret [1014]. ABI reflecting significant PAD adds additional value to medical history, because 50 to 89% of patients with an ABI less than 0.9 do not have typical claudication [536, 1041, 1042]. The history of claudication alone ‘dramatically underestimates’ the presence of large vessel PAD [535].
16.4.3 ABI as a prognostic tool
The presence of PAD is strongly related to a high incidence of coronary events and stroke [536]. Therefore, ABI also strongly relates to further development of angina, myocardial infarction, congestive heart failure, coronary artery bypass graft surgery, stroke or carotid surgery [535–538, 1043, 1044]. Even in patients with known multivessel coronary disease, a reduced ABI confers additional risk [540]. In asymptomatic individuals over 55 years of age, an ABI less than 0.9 may be found in 12 to 27% [536, 1045]. Even in an elderly population (71-93 years), a low ABI further identifies a higher risk CHD subgroup [1046].
16.5 Ophthalmoscopy for atherosclerosis screening
Recently it has been shown that the extent of retinal arteries atherosclerosis correlates with the extent of the total coronary plaque burden. Atherosclerosis of retinal arteries also strongly correlates with plasma total cholesterol, LDL-cholesterol, triglycerides and apoprotein B levels. Since ophthalmoscopy is a noninvasive technique, easy to perform and has no adverse effects it might be used to detect asymptomatic nonhypertonic individuals at high risk for cardiovascular events [1047, 1048].
Chapter 17: Gender issues: cardiovascular disease in women
The Task Force considered the production of a separate document on cardiovascular disease in women but concluded that a section on gender aspects would be more relevant.
Cardiovascular diseases in women have been the subject of a statement arising from a policy conference of the European Society of Cardiology [627] and this section draws heavily from this document.
It is not widely appreciated that, ultimately, more women than men die from CVD [1049, 1050]; in 2004, CVDs accounted for 55% of deaths in women in Europe, in contrast to 43% of deaths in men. While CHD is slightly commoner as a cause of death in women (23 vs. 21%), stroke is markedly more common – 15 vs. 11%. Chronic CHD is also becoming commoner in older women [38]. In contrast, breast cancer accounts for 3% of all deaths in women. This is not appreciated by most women [1051], which is a barrier to effective prevention.
The SCORE charts seem to suggest that risk is lower in women than in men. This is misleading; risk is merely deferred by 10 years. Thus a 55 year old woman is identical in terms of risk to a 45 year old man. The decline in CVD mortality in recent years has been greater in men than in women and CVD incidence has actually increased in women because of an increase in myocardial infarction in older women [21].
Risk management advice, particularly with regard to drug therapy, is hampered by a defective evidence base; women are frequently underrepresented in therapeutic trials, and there may be gender differences in therapeutic response [1052].
Risk factor distributions show some gender differences. Systolic hypertension becomes more frequent in older women [1053]. Tobacco consumption has fallen more in men than in women and the use of oral contraceptives increases the risk associated with smoking [1054]. Total cholesterol levels peak at around 60 years of age in women, about 10 years later than in men [1055]. Diabetes carries a considerably greater risk of fatal CVD in women [1056]; a recent reexamination of the SCORE data set suggests that self-reported diabetes increases the 10-year risk of fatal CVD by nearly five times in women and three times in men. Obesity is more prevalent in middle-aged and elderly women and the metabolic syndrome is more common in women with CHD than in men.
The principles of total risk evaluation apply to both sexes. As noted above, risk levels in women tend to resemble those of a man who is 10 years younger. The low absolute risks in younger women may conceal very large relative risks and be falsely reassuring; the relative risk chart, Fig. 7, chapter 5 may help in this regard. On the other hand, extrapolating the results of lipid-lowering trials to young or middle-aged women without other risks may lead to substantial over-use of cholesterol lowering drugs. This is illustrated in Table 3 and Fig. 2 in chapter 5. Apart from the risk factors in the SCORE charts, overweight and diabetes should be particularly taken into account.
Despite the promise of observational epidemiology, hormone replacement therapy has not been associated with a reduction in cardiovascular risk [624, 625, 1057–1059]. The small increase in risk of heart disease and breast cancer may relate to progestin more than oestrogen [625, 1058]. A pattern of early harm and later benefit has emerged, perhaps as thrombotic effects are replaced by metabolic ones [1049]. In general, short-term HRT for symptomatic relief is not contraindicated but HRT is not currently advised for preventive purposes.
In general, women are disadvantaged at all stages of the evolution of CVD – risk is less often evaluated, chest pain is less likely to have a typical ‘male’ pattern [1049] (it has been suggested that the term ‘atypical chest pain’ may reflect the difficulty that male physicians have in listening to and understanding women), diagnostic tests are less likely to be performed and harder to interpret. In-hospital mortality for acute coronary syndromes is higher in women [1060]. Therapy may be delayed and mortality associated with interventions such as coronary artery bypass grafting has traditionally been reported to be higher, although this may no longer be the case [1061].
Management implications:
European and national public health policy needs to address the problem of inadequate recognition of the size of the problem of CVD in women and to reflect this through publicity and education of both the public and the medical profession.
Clinicians likewise need vigilance in understanding the need to think risk and CVD in dealing with female patients.
The principles of total risk estimation and management are the same for both sexes, with particular emphasis on the evaluation of smoking, weight, the use of oral contraceptives and glucose tolerance in women.
The fact that a low absolute risk may conceal a high relative risk which, if managed effectively, need not translate into a high absolute risk in later life. In this situation, detailed help with lifestyle change is in general more important than drug treatment.
Chapter 18: Renal impairment as a risk factor in cardiovascular disease
Renal impairment and cardiovascular risk
Risk of CVD rises progressively from microalbuminuria with preserved GFR to end stage renal disease, when it is 20-30x that of general population.
Applies to apparently healthy people and to those with hypertension, CVD and heart failure.
Associated with high blood pressure, hyperlipidaemia, metabolic syndrome, uric acid, homocysteine, anaemia.
Particularly vigorous risk factor control needed.
Chapter 18: Renal impairment as a risk factor in cardiovascular disease
The presence of alterations of renal function is associated with an increased risk of future development of cardiovascular (CV) events and death. The enhanced risk is already present when microalbuminuria is detected in the presence of a totally preserved glomerular filtration rate (GFR). From then until the development of end-stage renal disease (ESRD), CV risk rises continuously to attain a maximum level 20 to 30 times above that of the general population [1062]. Four stages have been defined before the development of ESRD (stage 5) in the evolution of Chronic Kidney Disease (CKD) as defined in the Kidney Disease Outcomes Quality Initiative (K-DOQI) [1063]. They are based on the level of estimated glomerular filtration rate (eGFR), obtained using the MDRD formula [1064] or of estimated creatinine clearance using the Cockroft-Gault formula [548] and on the presence of albuminuria either micro (30-300 mg/24 h of creatinine) or macro (> 300 mg/24 h). There is a continuous relationship between CV risk and eGFR; values less than 60 ml/min/1.73 m2 (stage 3) are considered to be associated with a significant increase in CV risk. The presence of albuminuria is more frequent with diminished values of eGFR and the presence of both findings simultaneously is accompanied by an additive effect on CV risk.
The relevance of CKD for the prediction of CV disease has been demonstrated in the general [1065] and hypertensive populations [472], as well as in patients with established cardiac disease, in particular coronary artery disease, [1066] post-MI patients, [1067] and heart failure [1068]. The level of renal function has also been shown to be a good predictor of outcome after coronary interventions [1069] and cardiac catheterization [1070].
The development of CKD is associated with the presence of classical CV risk factors in particular age, arterial hypertension, and hyperlipidaemia [1071] and recently it has been shown to be associated to the presence of metabolic syndrome [1072]. Longitudinal data have shown in hypertensive patients that the progressive decay of eGFR from normal or mildly diminished levels to values below 60 ml/min/m2 is accompanied by a significant increase in CV events and death during that evolution [1073]. CKD and CV disease can then develop in parallel being the consequence of the activity of similar risk factors [1074] and both contribute independently to increase the risk prediction [1075]. Once CKD has progressed and eGFR are below the figure of 60 ml/min/m2, other factors specifically dependent on the level of renal insufficiency appear and contribute to enhance the level of CV risk. These are the presence of changes in calcium/phosphate homeostasis and the ultimate development of secondary hyperparathyroidism [1076] and anaemia due to a diminished renal production of erythropoietin [1077].
In patients presenting with heart failure, it has been shown that renal function is independently associated with heightened risk for death, CV death and hospitalization from heart failure in patients with both preserved and reduced left ventricular ejection fraction (LVEF) [1068]. Interestingly, in heart failure the finding of a diminished level of eGFR could be not the consequence of established renal disease but a direct reflection of an impaired haemodynamic status related to the severity of the underlying cardiac disease causing a functional derangement in renal function [1078]. Data from the CHARM study have shown that eGFR and cardiac function had effects that were independent in terms of predicting the primary end point of the study [1068].
The factors explaining the increased risk of CV events and death in the presence of any manifestation of CKD are the presence of advanced atherosclerosis and, very frequently, hypertensive vascular disease. This fact contributes to explaining the frequent association of renal insufficiency and established CV disease and explains the need for an early integral CV intervention in an attempt to control all the different CV risk factors usually present in these patients [1079]. It also must be stressed that patients with renal insufficiency are less likely to be prescribed efficacious therapies in particular when situations like heart failure or established coronary artery disease are present [1080]. The prescription of the adequate medications is accompanied by better survival rates across the full spectrum of renal function [1080].
Chapter 19: Cardioprotective drug therapy
When to prescribe cardioprotective drugs in addition to those used to treat blood pressure, lipids and diabetes?
Aspirin for virtually all with established CVD, and in persons at >10% SCORE risk once blood pressure has been controlled.
Beta-blockers after myocardial infarction and, in carefully titrated doses, in those with heart failure.
ACE inhibitors in those with left ventricular dysfunction and in diabetic subjects with hypertension or nephropathy.
Anticoagulants in those at increased risk of thromboembolic events, particularly atrial fibrillation.
Chapter 19: Cardioprotective drug therapy
In addition to drugs to control symptoms, manage blood pressure, lipids and glucose levels to goal, the use of prophylactic drugs shown in clinical trials to reduce CVD morbidity and mortality must be considered. While some of these drugs are appropriate for all individuals at high total risk, whether from established CVD or at high risk of developing CVD, others are specifically indicated for selected patients.
19.1 Antiplatelet therapies
19.1.1 Patients with atherosclerotic disease
Aspirin or other platelet modifying drugs are recommended in all patients at high risk of occlusive arterial disease unless there are specific contraindications. The Antithrombotic Trialists’ Collaboration meta-analysis provides convincing evidence that platelet modifying drugs result in a significant reduction in all-causes mortality, vascular mortality, nonfatal reinfarction of the myocardium and nonfatal stroke in patients with unstable angina, acute myocardial infarction, stroke, transient ischaemic attacks or other clinical evidence of vascular disease [773]. Aspirin reduces the risk of myocardial infarction by approximately 30% in men as shown in meta-analysis of five primary-prevention trials but has no significant effect on the risk of stroke. In contrast, in the Women's Health Study, which compared 100 mg of aspirin every day to placebo in 40 000 healthy women, aspirin reduced the risk of stroke by 17%, but there was no significant reduction in the risk of myocardial infarction. The reasons for this apparent gender discrepancy are still unclear [1081]. In the trials which used aspirin the most widely tested doses varied between 75-325 mg/day. There was no evidence of any greater clinical benefit for any doses in between this range. Side effects from aspirin are lowest in those using lower dosages. Hence, the available evidence supports daily doses of aspirin in the range of 75-150 mg for the long-term prevention of serious vascular events in high risk patients. Although there is no clinical trial evidence of treatment beyond a few years, it would be both prudent and safe to continue aspirin therapy for life.
Clopidogrel has been shown to reduce the composite outcome of CV death, myocardial infarction and stroke during the year following the hospitalization when given together with aspirin (CURE Trial) [1082]. The same applies to patients with STEMI (COMMIT-trial; CLARITY-trial). With regard to chronic stable atherosclerotic disease, Clopidogrel at 75 mg/day has also been evaluated in two large trials (CAPRIE and CHARISMA) against and together with aspirin [1083]. In the CAPRIE trial comparing clopidogrel 75 mg with aspirin 325 mg per day the overall result shows that clopidogrel was slightly more effective than aspirin in preventing the primary end point of CV death, myocardial infarction and stroke (RRR 8.7%; P = 0.04). Based on a subgroup analysis, the two drugs are equally effective at preventing major vascular complications in patients with recent myocardial infarction or ischaemic stroke, while clopidogrel was more effective than aspirin among patients enrolled because of symptomatic peripheral arterial disease. In the CHARISMA trial clopidogrel plus low-dose aspirin was evaluated in 15 603 patients with either clinically evident cardiovascular disease or multiple risk factors. Patients received clopidogrel (75 mg per day) plus low-dose aspirin (75 to 162 mg per day) or placebo plus low-dose aspirin. The primary composite end point of myocardial infarction, stroke, or death from cardiovascular causes was 6.8% with clopidogrel plus aspirin and 7.3% with placebo plus aspirin (relative risk, 0.93; 95% CI, 0.83 to 1.05; P = 0.22). In those with clinically evident atherothrom-bosis, the rate was 6.9% with clopidogrel and 7.9% with placebo (relative risk, 0.88; 95% CI, 0.77 to 0.998; P = 0.046). The primary end point among patients with multiple risk factors was 6.6% with clopidogrel and 5.5% with placebo (relative risk, 1.2; 95% CI, 0.91 to 1.59; P = 0.20) and the rate of death from cardiovascular causes also was higher with clopidogrel (3.9% vs. 2.2%, P = 0.01). The rate of severe bleeding was 1.7% with clopidogrel and 1.3% with placebo (relative risk, 1.25; 95% CI, 0.97 to 1.61%; P =0.09); however the rate of modest bleeding (i.e. demanding blood transfusions) was significantly higher in the dual-inhibition group as compared to aspirin alone. So overall clopidogrel plus aspirin was not significantly more effective than aspirin alone in reducing the rate of myocardial infarction, stroke, or death from cardiovascular causes, and severe bleeding complications were more common with combination antiplatelet therapy.
Taken together, clopidogrel together with aspirin is indicated in all patients suffering from an acute coronary event (unstable angina (UAP), NSTEMI, STEMI) for a period of 9-12 months. In chronic atherosclerotic disease, clopidogrel should only be considered as an alternative to aspirin in the case of aspirin allergy.
19.1.2 In patients with diabetes mellitus
The Antithrombotic Trialists’ Collaboration extended meta-analysis [773] has indicated more modest benefits from aspirin in diabetic persons than might have been anticipated. At present its use is recommended only in those with established CVD.
19.1.3 Asymptomatic high risk individuals
In asymptomatic individuals with no evidence of cardiovascular disease a meta-analysis has shown that aspirin reduced the risk of the combined end point of nonfatal myocardial infarction and fatal CHD, but increased the risk of haemorrhagic strokes and major gastrointestinal bleeding. The net benefit of aspirin increases with increasing cardiovascular risk and therefore estimating total risk of CVD is an absolute prerequisite to initiating antiplatelet therapy [1084]. If the total CVD risk is >10% over 10 years then prophylactic aspirin is appropriate as long as the blood pressure has been controlled as closely as possible to the goal of less than 140/90 mmHg. In lower risk individuals in the population a small absolute vascular benefit by aspirin may be offset by the slightly greater absolute risk of bleeding complications. When aspirin cannot be tolerated alternative antiplatelet therapy such as clopidogrel should be considered.
Therefore aspirin (75 mg daily) can be considered in all patients with CVD, and those at high risk of developing CVD (SCORE >10% over 10 years) once the blood pressure has been controlled.
19.2 Beta-blockers
In a meta-analysis of β-blockers following myocardial infarction, there was evidence of a significant reduction in all-cause mortality, cardiovascular death and in particular sudden cardiac death, as well as nonfatal reinfarction [629]. The benefits of β-blockade are greatest in older patients (more than 60 years) and in patients at increased risk of reinfarction and death (e.g. patients with left ventricular (LV) dysfunction or arrhythmias or both). Apart from the indication in postinfarction, β-blockers have also comprehensive evidence from multiple large-scale trials to reduce all-cause mortality in patients with heart failure due to any cause, including coronary heart disease (US-Carvedilol; COMET; CIBIS, MERIT-HF trials) [1085–1088].
Taken together, β-blockers are indicated, providing there are no contraindications, (i) in the treatment of heart failure, (ii) as prophylaxis following myocardial infarction, including patients with diabetes; (iii) to relieve symptoms of myocardial ischaemia; and (iv) to lower blood pressure to the goal of less than 140/90 mmHg, except in diabetic patients where alternative classes of antihypertensive drugs can be considered before β-blockers.
19.3 ACE inhibitors
19.3.1 Cardiovascular disease
Several clinical trials have shown that ACE inhibitors in patients with symptoms or signs of heart failure, or left ventricular dysfunction, due to any cause including CHD will significantly reduce the risk of death, recurrent myocardial infarction and progression to persistent heart failure (CONSENSUS, SAVE, AIRE trials) [1089–1091]. Short-term studies of ACE inhibitors in the acute phase of myocardial infarction have also shown the risk of death can be reduced within the first day of treatment (TRACE trial etc.) [1092]. More recently ACE inhibition has been shown in one single clinical trial (EUROPA) of patients with stable angina pectoris without apparent heart failure to reduce the risk of myocardial infarction and cardiovascular mortality [1093]. In another single trial of patients with vascular disease (HOPE) without left ventricular dysfunction ACE inhibition reduced the risk of myocardial infarction and cardiovascular mortality [457]. In the PROGRESS study of people with a previous history of cerebrovascular disease, blood pressure lowering using an ACE inhibitor/diuretic regimen produced significant reductions in the risk of recurrent stroke and cardiovascular events [570]. However, in the PEACE trial of stable coronary disease and preserved left ventricular function there was no additional benefit from an ACE inhibitor [575].
Taken together, ACE inhibitors are indicated in all patients, unless there are contraindications, for the following reasons: (i) treatment of left ventricular dysfunction with or without overt heart failure; and (ii) to reduce blood pressure to goal less than 140/ 90 mmHg.
19.3.2 Patients with diabetes mellitus
ACE inhibition has been shown in the HOPE trial of high risk people (aged 55 years or older with evidence of diabetes plus one other cardiovascular risk factor without left ventricular dysfunction or uncontrolled hypertension) to reduce the risk of myocardial infarction and cardiovascular mortality [573].
Hence ACE inhibitors are indicated in patients with diabetes mellitus, unless there are contraindications, for the following reasons: (i) to reduce blood pressure to goal less than 130/80 mmHg, and (ii) type 1 and (possibly) type 2 diabetic nephropathy.
19.3.3 Asymptomatic high risk individuals
ACE inhibitors are indicated in asymptomatic high risk patients, unless there are contraindications, for the reason of reducing blood pressure to goal less than 140/90 mmHg.
19.4 Angiotensin-receptor blockers (ARBs)
Generally speaking ARBs are indicated in all patients who have an indication for ACE inhibitor therapy, but cannot tolerate ACE-inibitors, for example, due to side effects. In addition ARBs in combination with ACE inhibitors can reduce morbidity (i.e. rate of rehospitalization) in patients suffering from congestive heart failure (VAL-HEFT, CHARM trials) [1094, 1095].
19.5 Calcium channel blockers (CCBs)
This drug class has been shown to reduce cardiovascular outcomes in people with arterial hypertension.
In post-MI patients with contraindications to β-blockers and no evidence of heart failure, verapamil may be considered based on the results of a single large clinical trial (DAVIT-trials) [1096].
Hence, calcium channel blockers are indicated for the reason of reducing blood pressure to target less than 140/90 mmHg or less than 130/80 mmHg (diabetes).
Indications for antithrombotic therapy in patients with atrial fibrillation
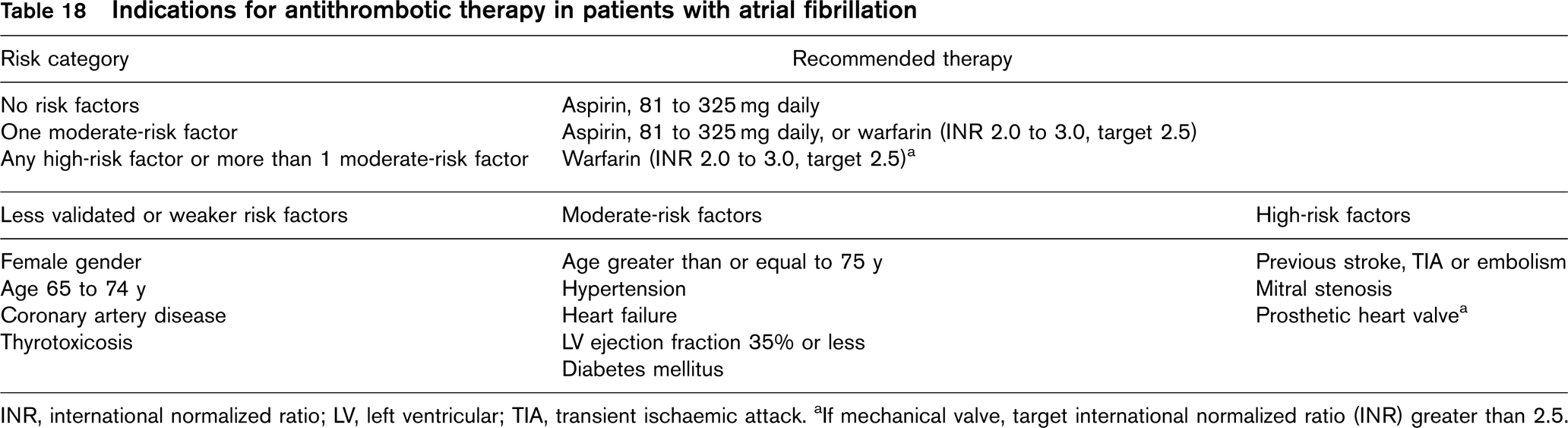
INR, international normalized ratio; LV, left ventricular; TIA, transient ischaemic attack. aIf mechanical valve, target international normalized ratio (INR) greater than 2.5.
19.6 Diuretics
Diuretics are indicated for the following reason: to reduce blood pressure to target less than 140/90 mmHg. Thiazide diuretics are not recommended as first-line antihypertensive agents in diabetic patients or those at high risk of developing type 2 diabetes.
19.7 Anticoagulation
Systemic anticoagulation with coumarins is generally not indicated prophylactically in patients with coronary artery disease. However, anticoagulation can be considered in selected patients following myocardial infarction at increased risk of thrombo-embolic events including patients with large anterior myocardial infarction, left ventricular aneurysm or thrombus, paroxysmal tachyarrhythmias and chronic heart failure, particularly in combination with aspirin (WARIS-II trial) [1097]. In patients with paroxysmal or permanent atrial fibrillation, systemic anticoagulation is indicated as shown in Table 18 [1098].
In patients with coronary heart disease, or other cardiac disease, systemic anticoagulation is indicated for the following reasons:
History of thrombo-embolic events.
Left ventricular thrombus.
Chapter 20: Implementation strategies
What would make the practice of CVD prevention easier?
Simple, clear, credible guidelines.
Sufficient time.
Positively helpful government policies (defined prevention strategy with resources, incentives including remuneration for prevention as well as treatment).
Educational policies that facilitate patient adherence to advice.
20.1 Defining the problem
Several studies have been made to evaluate the effect of different implementation strategies of guidelines on clinical practice.
EUROASPIRE I (1995/96) [1099] and II (2000/01) [101] surveys, both showed a high prevalence of unhealthy lifestyles, modifiable risk factors and inadequate use of drug therapies to achieve blood pressure and lipid goals in patients with established CHD, with wide variations in medical practice between countries. The comparison of EUROASPIRE I and II surveys showed adverse lifestyle trends, especially the substantial increase in obesity in every country, and smoking among younger patients. Half of patients continued smoking after a coronary event. There was no change between surveys in the proportion of patients who reached their blood pressure goal of less than 140/90 mmHg and one in two patients with established CHD are still not reaching this goal, despite the real improvement in the proportion of patients who reach the total cholesterol target (Tables 19 and 20).
Although implementation of guidelines improved over time, subgroups are still not receiving appropriate therapy, especially patients with stable angina and the elderly who are under treated. Many surveys have shown similar results; some also showing great variance between countries [1100–1102].
There is considerable potential through Europe in coronary patients and their families to raise the standard of preventive cardiology through more lifestyle intervention, control of other risk factors and optimal use of prophylactic drug therapies in order to reduce the risk of recurrent disease and death. Similar results have been shown for stroke.
Main findings in EUROASPIRE I and II: risk factors
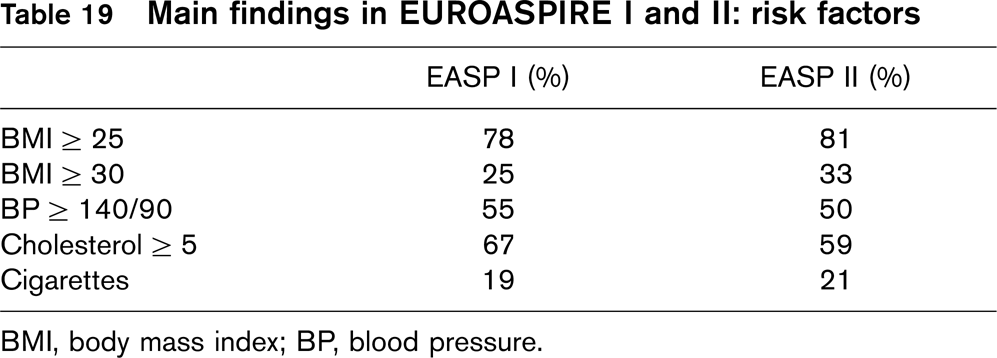
BMI, body mass index; BP, blood pressure.
Main findings in EUROASPIRE I and II: drug use
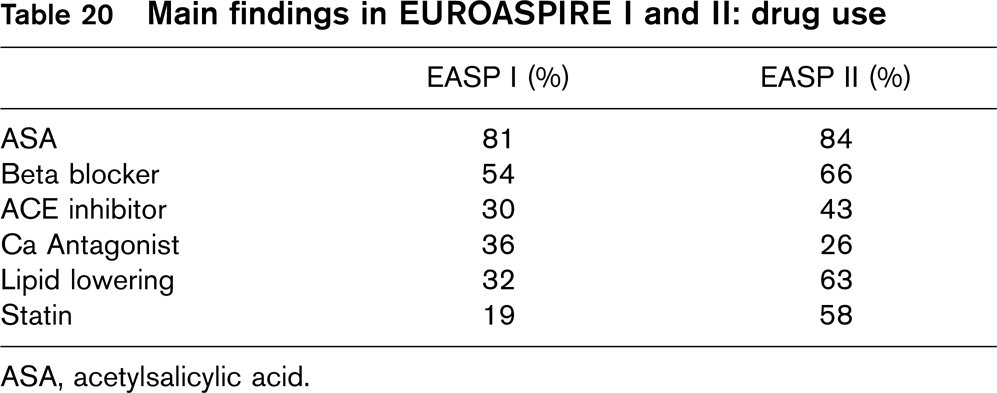
ASA, acetylsalicylic acid.
Traditional approaches to improve uptake of research findings have focused on better availability and presentation of evidence by identifying, synthesizing, and disseminating evidence to doctors in practical accessible formats – e.g. reviews in clinical journals, clinical guidelines, better access to electronic sources of information, continuing medical education (CME) courses, and conferences. Although this strategy may be all that is needed to ensure the uptake of some simple changes, most innovations require further efforts. Most clinicians can barely keep pace with the rapid advances in healthcare knowledge. Shaneyfelt calculated that general internists would need to read 20 articles a day all year round to maintain present knowledge [1103]. Although the availability of systematic reviews and guidelines reduces the need for doctors to read original studies, they still find it difficult to keep up with such syntheses. Even if doctors are aware of the evidence and are willing to change, to alter well established patterns of care is difficult, especially if the clinical environment is not conducive to change.
20.2 Barriers to the implementation of guidelines
It is essential that clinical guidelines are in concordance with priorities in the health system and with ethical values most clinicians can agree upon. If not, this may be an important reason why many clinicians do not follow guidelines [1104].
The implementation of these guidelines should be based on national surveys to adjust them to the stratification of risk factors and premature CVD death in the individual country and bring them in accordance with priorities set by the health authorities and the professional bodies. The workload put on the health system should be affordable and should not imply that resources should be allocated to prevention strategies when the outcome for the population is better by alternative use.
Given agreement that the implementation of prevention is a priority, the next step in the implementation of these guidelines is the involvement of the clinicians, in primary and secondary care.
Analyses of the barriers to changing practice, such as a review of 76 doctors, have shown that obstacles to change in practice can arise at different stages in the healthcare organization, or the wider environment. Most theories on implementation of evidence in healthcare emphasize the importance of developing a good understanding of such obstacles to develop an effective intervention (Table 21).
20.3 Doctor-patient relationship
The preventive interventions must be based on a patient-centered approach, where the doctor pays full attention to appraise and meet the patient's concerns, beliefs and values, and respects the patient's choice even if it is not in concordance with the doctor's first proposal. The changing of lifestyle or taking medication often means for the rest of the patient's life, so the decision must be owned by the patient. Therefore, treatment goals should be set in collaboration with the patient, taking into account the values and priorities of the patient. If the treatment goals are unaffordable, it may lead to frustration and clinical neglect, both by the doctor and the patient. The doctor should explore the patient's important values, beliefs and expectations regarding the prevention measures to be taken.
20.3.1 Physician-related methods to improve implementation
It has been argued that the application of guidelines in a setting of rigorous control gives the best chances to improve clinical practice. However, most front-line clinicians work in settings where such control is not practical, and mostly not wanted. The very character of this specific task – primary and secondary prevention – is not suitable for this strategy.
Barriers to implementation of guidelines
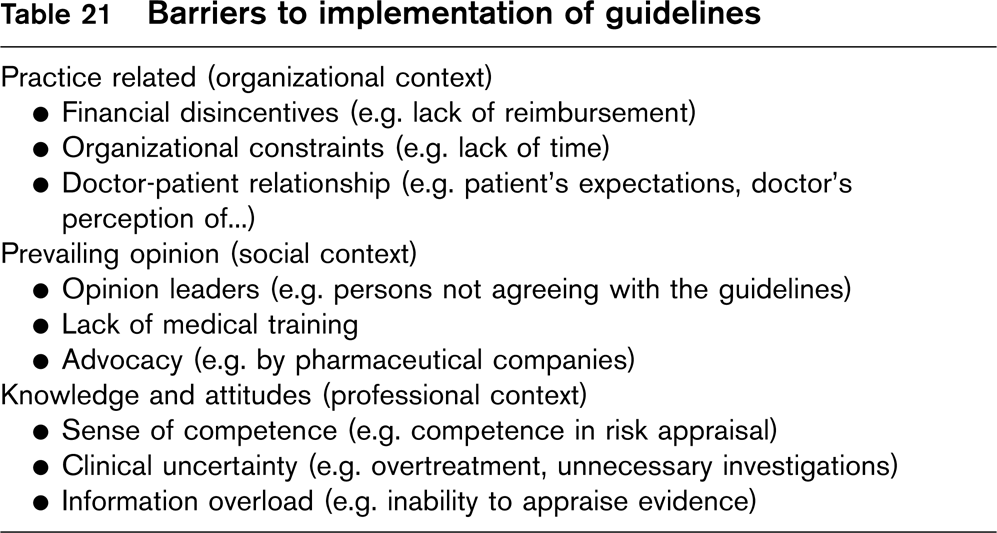
Audit and feedback, where practitioners are given data on their performance is another tool that has been used to improve practice. It seems logical that practitioners will change their practice when they get feedback indicating that their present practice is inconsistent with that of their peers or with evidence based guidelines. A recent meta-analysis from the Cochrane collaboration shows that the effect of audit and feedback, if any, is modest [1105].
The decision to start preventive measures and follow them up is more value-related than treatment of established disease, so the values and attitudes of the doctors and the patients are more important. In addition, most clinical decisions are taken more intuitively, on the basis of recognition patterns or other internal mental shortcuts (heuristics) of the individual doctor. How this affects the application of guidelines is not known, and more research is needed.
20.4 Important arenas for training
There is a need for training of doctors in patient-centered preventive care, with emphasis on:
patient-centered methods in the consultation process
the motivation to change – how to support and strengthen the patient's decision for healthy habits
how to evaluate multifactorial risk and use risk charts
how to communicate risk and the effects of interventions
how to discuss treatment goals and follow up.
20.5 Implementation strategies
On the European (international) level:
Publication of the guidelines in relevant journals.
Presentation at International conferences arranged by the participating societies.
Involvement in policy at European Union level through, for example, the Luxembourg Declaration and the development of the European Heart Health Charter.
On the national level:
If not already existing, the implementation demands a leading expert group of national organizations representing similar groups as the European Task Force. The group should have acceptance and support from national health authorities.
Adjustment and application of national standards, in accordance with the European Guidelines.
Further implementation should be organized by the National Colleges in accordance with the local needs, see below.
The implementation strategies should consist of a package of different measures, working in combination:
A public health approach, with emphasis on smoking cessation, healthier food and better access to physical activity in all ages should be implemented – to support and complement the individual-oriented high risk strategy of doctor-initiated prevention.
A public information campaign of the Joint CVD Prevention Guidelines with 2 main topics:
Information of the concept of multiple risk assessment and treatment and the intervention thresholds.
What people can do to reduce the risk. The message should encourage people with high risk to realise their risk and go to see a doctor, but should reassure people with low risk that they can stay healthy without the doctor's help.
An information and education program aimed at practicing doctors (GPs, internists, other). It should consist of a selection of the effective strategies mentioned above:
Lectures and CME activities with interactive participation.
Audit and feedback, preferably combined with outreach visits by trained colleagues.
Dissemination of electronic versions, applicable for handheld equipment.
Dissemination of simple, one sheet versions of risk algorithms and treatment recommendations.