
Abstract
Cardiovascular disease is the leading cause of death and hospitalization in both sexes in nearly all countries of Europe. The main forms of cardiovascular disease are ischaemic heart disease and stroke. The magnitude of the problem contrasts with the shortage, weak quality and comparability of data available in most European countries.
Innovations in medical, invasive and biological treatments have substantially contributed to the escalating costs of health services. It is therefore urgent to obtain reliable information on the magnitude and distribution of the disease for both adequate health planning (including preventive strategies) and clinical decision making with correct cost-benefit assessments.
A stepwise surveillance procedure based on standardized data collection, appropriate record linkage and validation methods was set up by the EUROCISS Project (EUROpean Cardiovascular Indicators Surveillance Set) to build up comparable and reliable indicators (attack rate and case fatality) for the surveillance of acute myocardial infarction/acute coronary syndrome at population level.
This manual of operations is intended for health professionals and policy makers and provides a standardized and simple model for the implementation of a population-based register. It recommends to start from a minimum data set and then follow a stepwise procedure.
Before implementing a population-based register, it is important to identify the target population under surveillance which should preferably cover a well-defined geographical and administrative area or region representative of the whole country for which population data and vital statistics (mortality and hospital discharge records at minimum) are routinely collected and easily available each year. All cases among residents should be recorded even if the case occurs outside the area. Validation of a sample of fatal and nonfatal events is mandatory. Eur J Cardiovasc Prev Rehabil 14 (Suppl 3):S3-S22 © 2007 The European Society of Cardiology
Keywords
Introduction and rationale
Burden of disease
Cardiovascular disease (CVD) is the leading cause of death and hospitalization in both sexes in nearly all countries of Europe. In the European Union (EU) (data refer to the following 25 member states: Austria, Belgium, Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, The Netherlands, Poland, Portugal, Slovakia, Slovenia, Spain, Sweden, United Kingdom) 47% of women and 39% of men die from CVD (Figs 1 and 2) [1].
CVD clinically manifests itself in middle life and older age after many years of exposure to unhealthy lifestyles (smoking habit, unhealthy diet, physical inactivity) and risk factors (total and low-density lipoprotein cholesterol, blood pressure, diabetes). Even though the clinical onset is mainly acute, CVD often evolves gradually. Contrary to common belief of a sudden death and hence of a death free of suffering, CVD causes substantial loss of quality of life, disability, and lifelong dependence on health services and medications.
For many years CVD mortality has been decreasing in the majority of western European countries and during recent years this decrease has occurred also in Eastern Europe [2]. The absolute number of patients, however, in need of using health services for CVD conditions does not decrease to the same extent because prevalence tends to increase, and this is due to an increase in survival and an increasing proportion of older people in the population. In particular, CVD is bound to become a more frequent disease of older women [3].
CVD has major economical consequences as well as human costs.
CVD alone accounts for 20% of global total disability adjusted life years (DALYs) in persons older than 30 years [4]. In terms of health, acute events may mean an increasing number of dependent, chronically ill and disabled people: this may cause increasing costs of healthcare and strain the healthcare system.
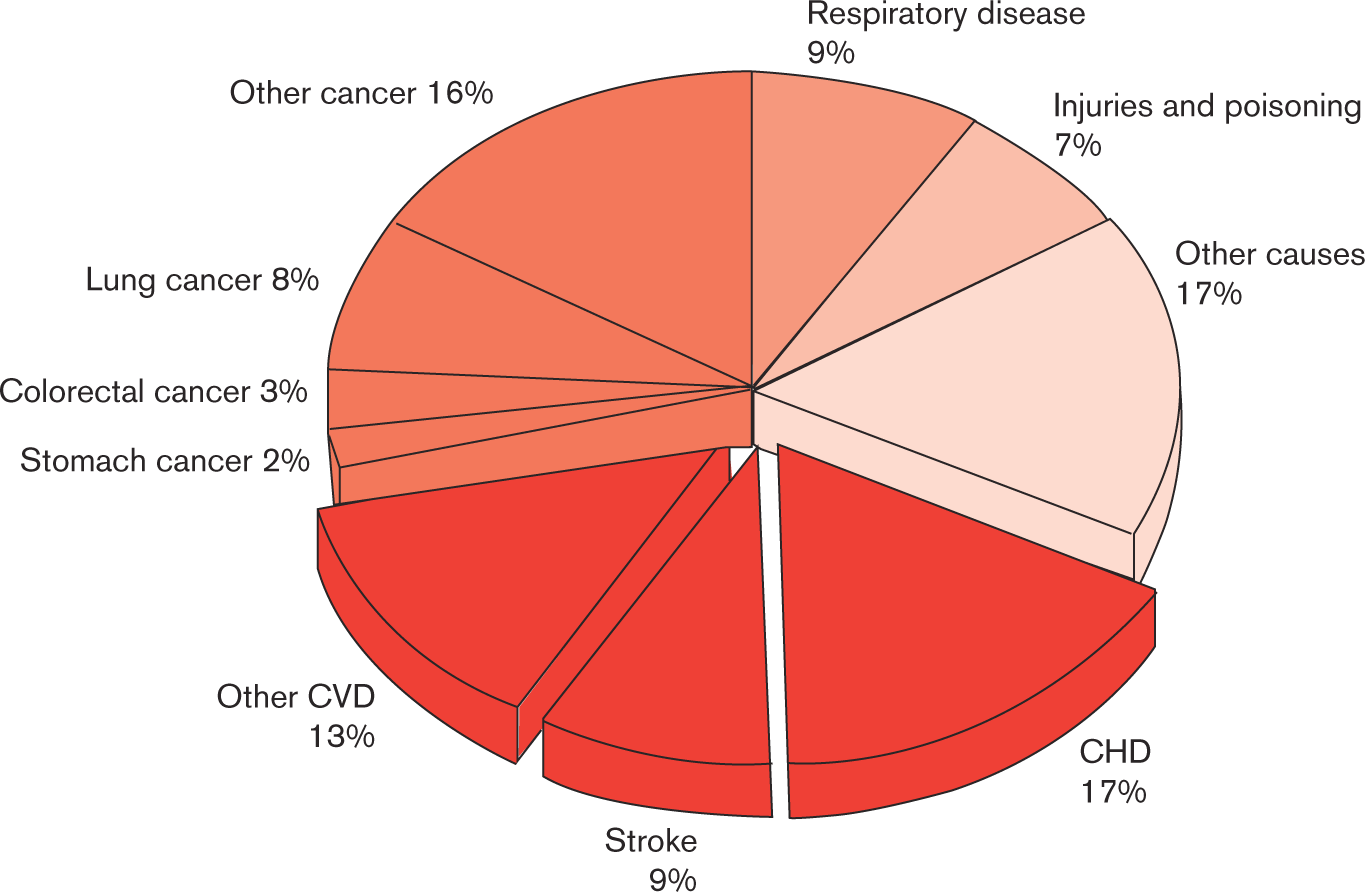
Deaths by cause, men (all ages), latest available year, European Union [1]. CHD, coronary heart disease; CVD, cardiovascular disease.
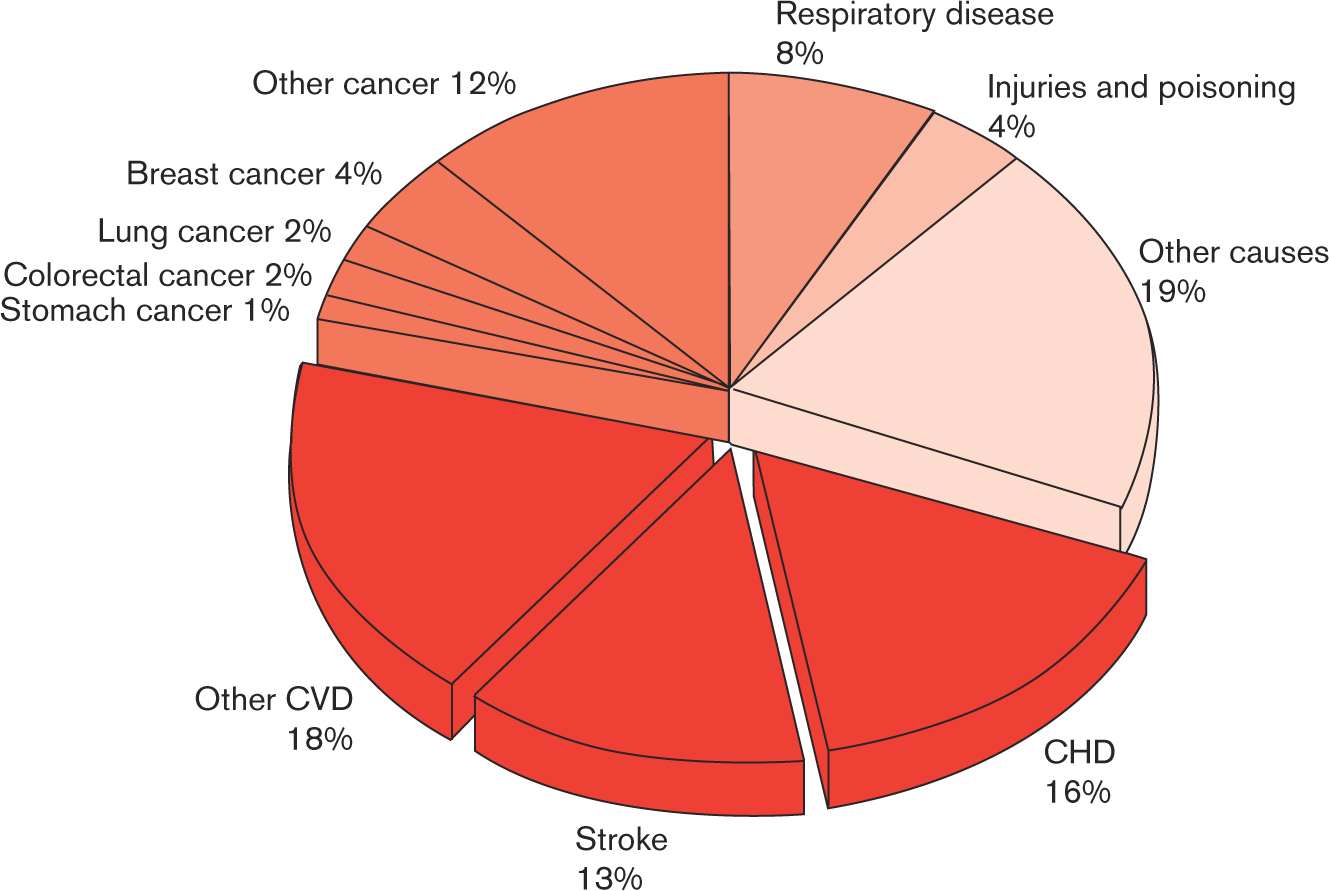
Deaths by cause, women (all ages), latest available year, European Union [1]. CHD, coronary heart disease; CVD, cardiovascular disease.
Among CVD, ischaemic heart disease (IHD) by itself is the single most common cause of death in the EU accounting for 744000 deaths each year: around one in six men (17%) and over one in seven women (16%) die from the disease [1].
In the last decade innovations in diagnostic technologies have facilitated diagnosis at earlier phases in the course of the natural history of disease or in the presence of less severe tissue damage. The use of new biomarkers, such as the routine introduction of new myocyte damage markers (troponins), has required a rethink of the concept of myocardial necrosis and has led to a new and more exhaustive definition of acute coronary syndrome (ACS) [5–7].
Coding changes in international disease classification have also posed new challenges for the comparability of disease indicators. All these factors may produce spurious trends in disease frequency, severity, prognosis and subsequent variations in medical practice if not properly controlled with the adoption of updated and valid epidemiological methods.
The magnitude of the CVD contrasts with the usual paucity and poor quality of data available on the incidence and prevalence of CVD, except for few rigorous but limited studies carried out in certain geographical areas.
According to the Organisation for Economic Cooperation and Development (OECD), it does not appear inevitable that longer life leads to higher healthcare costs. This is one of the reasons why the health system should be largely oriented toward work on preventive actions. Epidemiological studies have shown that IHD is preventable to a large extent. Different preventive strategies can be implemented to reduce the occurrence and impact of IHD, such as the identification of individuals at high risk, and to intensify treatment in those people who have already experienced a coronary event.
At the European level, the World Health Organization (WHO), OECD and the Statistical Office of the European Communities (EUROSTAT) collect simple CVD indicators (mortality and hospital discharge rates) and process them into tables available on their web sites (www.euro.who.int/hfadb; www.oecd.org; www.europa.eu.int/comm/eurostat). These data are rarely comparable due to the different methodology in their collections and the peculiar health system of each country.
Disease register
The objectives of an acute myocardial infarction (AMI)/ACS population-based register are to (a) evaluate the frequency, distribution and prognosis of the disease providing indicators, such as attack rate, incidence rate, prevalence and case-fatality rate; (b) evaluate trends and changing patterns, outcomes and treatment effectiveness; and (c) monitor CVD prevention programmes. If survival rates are assumed to be known, prevalence can also be estimated.
Focusing on the general population, an AMI/ACS register may provide a comprehensive picture of this disease in the community, highlight problem areas and suggest where treatment facilities are most in need of improvement. This register may also provide information systems needed to plan healthcare services and to develop and test which methods are most useful as a basis for preventive actions.
A population-based register includes all cases in a defined population, whether treated at home or in hospital, in whichever season of the year or time of the day they may occur, and would also include rapidly fatal cases unable to reach the medical service.
Therefore, it is desirable that collection of information on suspected events and application of diagnostic criteria follow a standardized methodology to enable data comparison in different areas or between different countries.
To summarize, a population-based register is intended for health professionals and policy makers and provides the means to understand the characteristics, the burden and the consequences of the disease in the population through:
the monitoring of the occurrence of the disease (i.e. to assess population differences and trends in attack and incidence rates and in mortality over time);
the understanding of the differences and changes in the natural disease dynamics between sexes, age groups, social classes, ethnic groups, etc.;
the identification of vulnerable groups;
the monitoring of in-hospital and out-of-hospital case fatality;
the assessment of relations between disease incidence, case fatality and mortality;
the monitoring of the consequences of disease in the community in terms of drug prescriptions and rehabilitation;
the monitoring of the utilization of new diagnostic tools and treatments and their impact.
This is crucial to:
develop health strategies and policies;
plan health services and health expenditures;
improve appropriate allocation of resources;
evaluate the effectiveness of interventions.
A register must be validated. Validation provides the means to:
take into account bias from diagnostic practices and changes in coding systems;
trace the impact of new diagnostic tools and redefinition of events;
ensure data comparability within the register (i.e. different subpopulations, different time points, etc.);
ensure data comparability with other registers within and between countries.
Historical background
The first experience of population-based registers in the field of CVD were the WHO Myocardial Infarction Community Registers in 1967 [8]; they were implemented by a group of experts convened by the WHO Regional Office for Europe to (a) evaluate the extent of AMI in the community; (b) monitor the effect of changes in the management of AMI and different kinds of intervention; (c) provide an assessment of the validity of mortality statistics; (d) select a pool of patients who could be studied in detail and focus attention on specific problem areas. The register examined the incidence of myocardial infarction (MI) and the influence of smoking, obesity and hypertension on MI to show which people in the community were specifically at risk.
The WHO Myocardial Infarction Community Registers were followed by the WHO MONICA Project (MONItoring trends and determinants in CArdiovascular diseases) [9] which was indeed designed to answer key questions on decline in IHD mortality, in particular which part was attributable to survival improvement and coronary event decline as a consequence of risk factor reduction and improving coronary care. During 10 years of surveillance of 37 populations in 21 countries 166 000 events were registered. The mean annual decrease in official IHD mortality rates (on the basis of death certification) was −4% in men and −4% in women. By MONICA criteria, fatal coronary events mortality rates were higher but fell less (−3% and −2%). Changes in nonfatal rates were smaller (−2% and −1%). MONICA coronary event rates (fatal and nonfatal combined) fell more (−2% and −1%) than case fatality (−1% and −1%). Contribution to changing IHD mortality varied, but in populations in which mortality decreased, coronary event rates contributed two-thirds and case fatality one-third [10].
Existing registers in Europe: an overview
The data collection for the international MONICA study ended in 1994/95. Some countries continued to collect data every year, whereas others did so only periodically (usually every 5 years). Currently, the existing population-based registers in Europe adopt different data collection procedures: some registers are based on the procedures used in the MONICA study, others on administrative databases with or without record linkage, some are national and some are regional. Different age groups are covered, the degree of validation of the diagnostic information varies and in most registers is much less intensive than in the MONICA study [11].
Tables 1, 2a, 2b and 3 give a brief overview of the existing AMI/ACS registers in Europe. Table 1 shows the national registers in the northern countries, which are all based on record linkage between routine databases [hospital discharge records (HDR) and cause-of-death registers].
Tables 2a and 2b show regional population-based registers: most of them are based on disease-specific data collection comparable with the MONICA registers, whereas the others are based on different data collection methods.
Table 3 shows registers on the basis of data from healthcare institutions such as general practitioners (GPs) and hospitals. These registers do not include out-of-hospital fatal events (sudden death), therefore they are not intended to assess disease occurrence but rather to evaluate outcome and survival of patients.
Objectives
The purpose of the EUROCISS project is to provide a general guide and updated methods for the surveillance of AMI/ACS to those EU countries which lack appropriate surveillance systems and therefore wish to implement a population-based register to produce comparable and reliable indicators.
Taking into account developments in new diagnostic criteria, treatment and information technologies in recent years, this manual provides a standardized and simple model for the implementation of a population-based register. It recommends starting from a minimum data set and following a stepwise procedure based on standardized data collection, appropriate record linkage and validation methods.
This manual is intended for investigators, health professionals, policy makers and data collection staff interested in the surveillance of AMI/ACS.
Although in many countries data extracted from some sources of information (mortality and HDR) are now available thanks to the continuing process of computerization, they are rarely reliable and comparable. These data can produce reliable indicators only if properly processed and validated by independent epidemiological sources.
National population-based AMI/ACS registers

AMI/ACS, acute myocardial infarction/acute coronary syndrome; NBHW, National Board of Health and Welfare; NIPH, National Institute of Public Health. Source: European J of Public Health 2003,
Regional population-based AMI/ACS registers: population characteristics
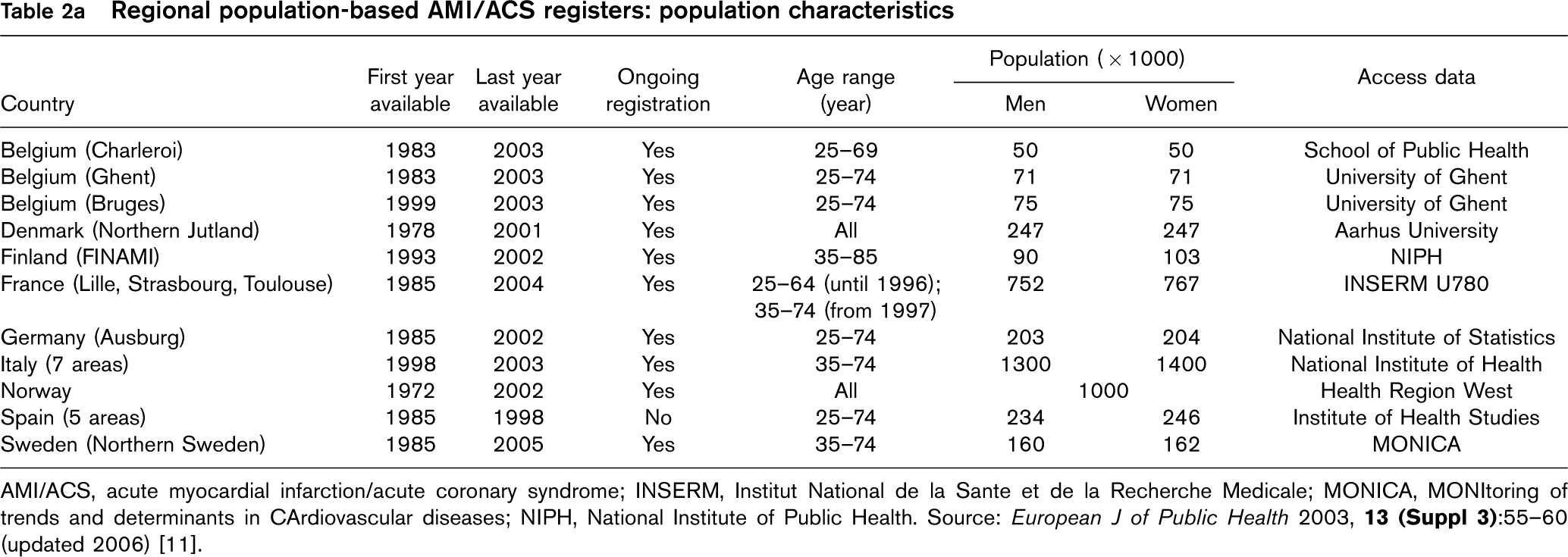
AMI/ACS, acute myocardial infarction/acute coronary syndrome; INSERM, Institut National de la Sante et de la Recherche Medicale; MONICA, MONItoring of trends and determinants in CArdiovascular diseases; NIPH, National Institute of Public Health. Source: European J of Public Health 2003,
Regional population-based AMI/ACS registers: case definition
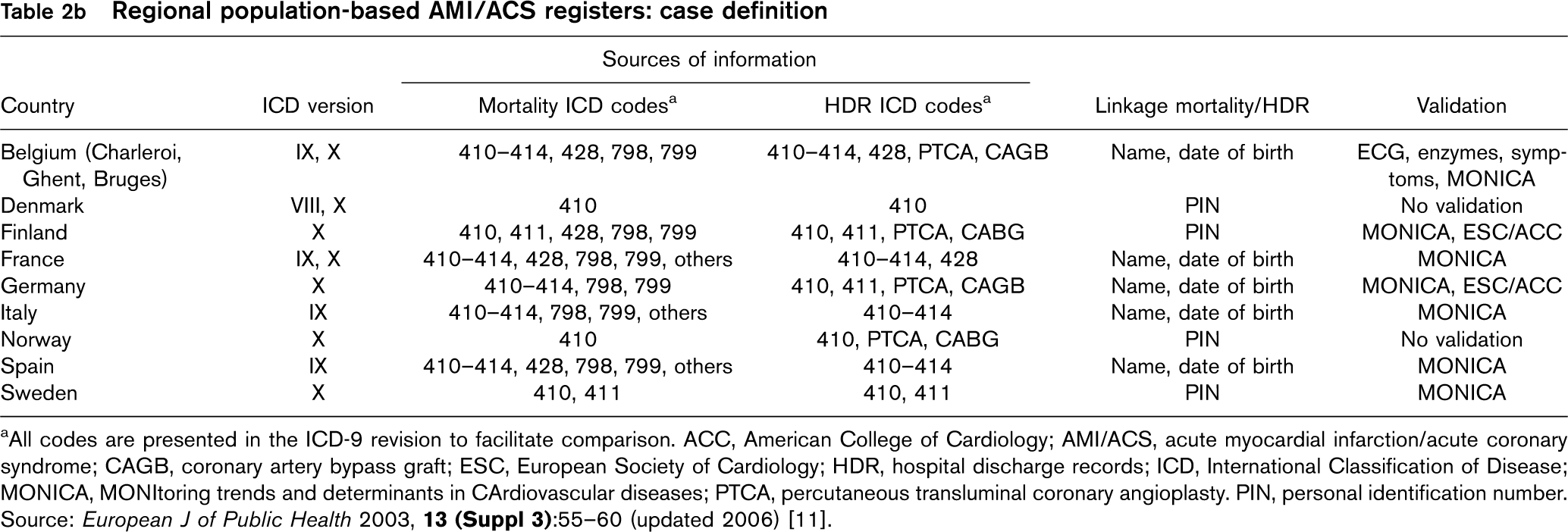
aAll codes are presented in the ICD-9 revision to facilitate comparison. ACC, American College of Cardiology; AMI/ACS, acute myocardial infarction/acute coronary syndrome; CAGB, coronary artery bypass graft; ESC, European Society of Cardiology; HDR, hospital discharge records; ICD, International Classification of Disease; MONICA, MONItoring trends and determinants in CArdiovascular diseases; PTCA, percutaneous transluminal coronary angioplasty. PIN, personal identification number. Source: European J of Public Health 2003,
This manual represents a valid tool to build the core indicators (attack rate, incidence, case fatality) recommended by the EUROCISS project research group for inclusion in the short list of health indicators set up by the European Community Health Indicators Monitoring (ECHIM) project. This project was launched in 2005 with the aim of implementing health monitoring in the EU [12].
Strategy for surveillance Surveillance methods and types of registers Surveillance is the ongoing, systematic collection, analysis, interpretation and dissemination of health information to health professionals and policy makers. Surveillance, defined as a continuous and not episodic or intermittent activity, differs from monitoring [13, 14].
Disease surveillance in a population can be done using many different data sources (Table 4).
Most countries have national databases on causes of death and discharge diagnoses for hospitalized patients. Mortality statistics have for many years been the main tool for comparing health and disease patterns among countries and today still remain the only source of information for some countries. Since the 1950s, the cause of death has been registered according to the International Classification of Disease (ICD). Different classification of disease within versions and different methods of ascertainment have led to problems in comparison between different revisions of ICD and/or similar versions among countries. In recent years, routine statistics have also included discharge diagnoses from hospitalization and visits to outpatient clinics coded according to the same international classification as the mortality data.
Some countries also have some kind of health interview survey/health examination survey (HIS/HES). These surveys are primarily used for monitoring prevalence of disease (including IHD, effort angina, old MI), prevalence of risk factors (health behaviour, social network, environmental risk factors) and of disease consequences (disability, reduced physical function, unemployment).
Institutional-based registers
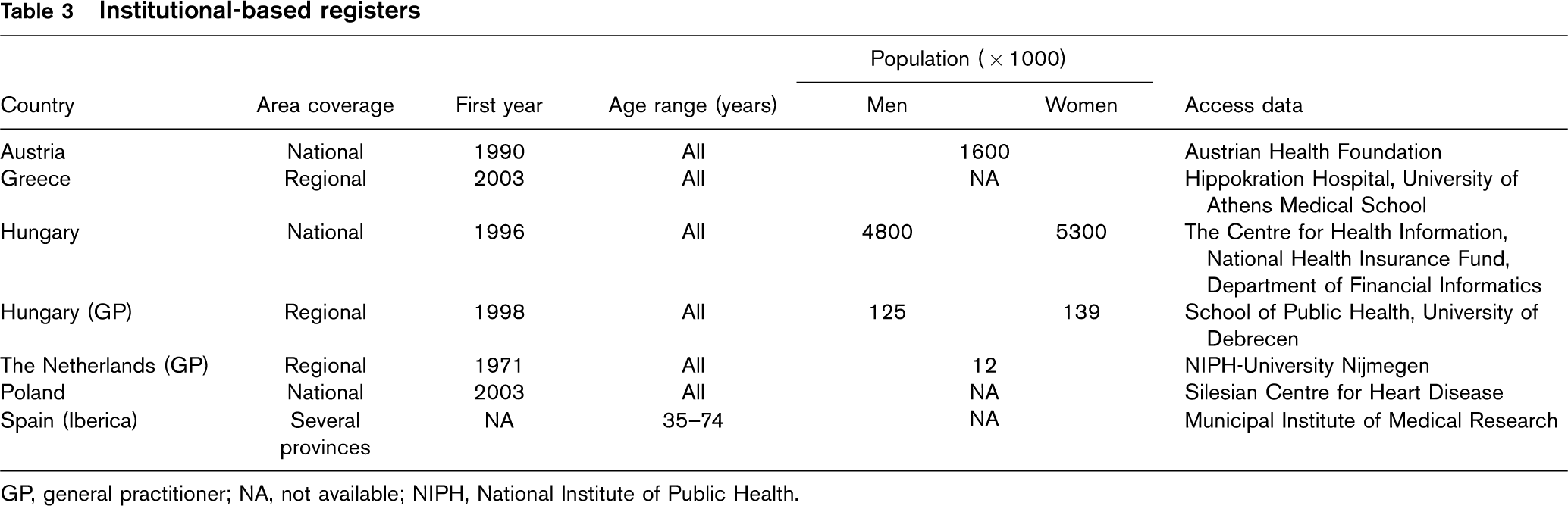
GP, general practitioner; NA, not available; NIPH, National Institute of Public Health.
Methods of surveillance of AMI/ACS
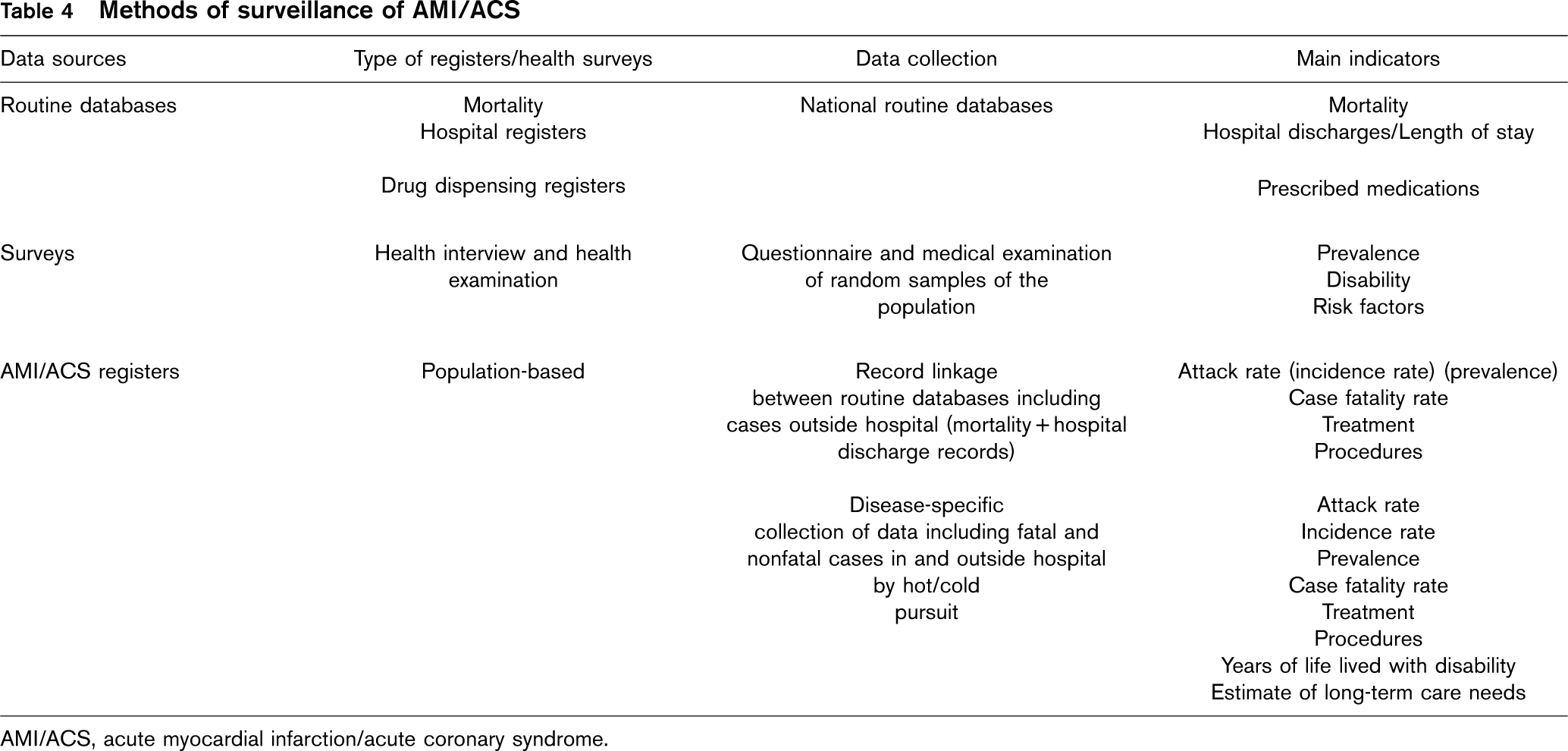
AMI/ACS, acute myocardial infarction/acute coronary syndrome.
Population-based registers ensure a more precise and valid monitoring of this disease. This register derives from a variety of currently available sources but requires a further level of processing to ensure accuracy.
A population-based register is usually formed through linkage of various sources of information (mortality data, hospital discharge and GP records) and covers a defined population (entire municipalities, regions or whole country) and a specific age group (35–74, 35–64 years or all ages).
A population-based register is the best data source for the surveillance of AMI/ACS morbidity and mortality as it considers both fatal and nonfatal events occurring in- and out-of-hospital; therefore, it provides estimates of key indicators such as attack rate and case fatality. Incidence can be assessed if information on first event is available. If survival rates are available, prevalence can be assessed as well.
Case findings and validation procedures depend on data collection methods, healthcare system, financing system [Diagnosis-Related Group (DRG)] and diagnostic criteria applied in the definition of events. The accuracy of rates produced using a population-based register is related to the completeness and quality control of data collected for numerator (death and hospital discharge registers) and denominator (census or population register). Completeness also depends on tracing patients treated outside hospital (nursing home, clinic, etc.). A valid population-based register should also collect events in the target population which occur outside the area of surveillance.
The definition of the event must take into account both the ICD codes reported in the hospital discharge diagnoses or causes of death and the duration of event. This definition is of particular importance as an AMI/ACS may occur more than once and it is therefore necessary to consider both first and recurrent events. In this context, hospital admissions and deaths occurring within 28 days (onset is day 1) are considered to reflect the same event [15] (see Definition of events).
A personal identification number (PIN) for each participant is a strong tool in linkage procedures between hospital discharge diagnoses, GP's records and death certificates; alternatively, multiple variables (e.g. name, date and place of birth, sex, residence) may be used for record linkage.
Specific acute myocardial infarction/acute coronary syndrome population-based register
The strength of this register lies in the possibility of validating each single event according to standardized diagnostic criteria and collecting disease-specific clinical and paraclinical data [16, 17]. The weakness lies in the fact that data collection is expensive and this kind of register can usually be maintained only for a limited period of time in a defined population of reasonable size. Another limitation is that local or regional registers may not be representative for the whole country.
Identification of events can be obtained by ‘hot pursuit’ or ‘cold pursuit’. Hot pursuit means identifying case admissions to hospital usually within one or two days from event onset and acquiring relevant information by visiting the ward or interviewing the patient. Information bias is minimized by the hot pursuit approach as information is collected immediately after the event. The process is very expensive. Cold pursuit implies the use of routine and delayed procedures, by means of hospital discharge and the review of medical and death records. The process is easier and less expensive than hot pursuit; the number of cases studied is typically smaller because discharge diagnoses are more precise and specific than those on admission, but there is a possibility of missing important information. Both methods are used to identify suspected events, which are subsequently validated using specific diagnostic criteria.
A specific AMI/ACS register provides the most valuable epidemiological measures for public health initiatives aimed at preventing the disease. It has been used in the WHO MONICA project, where uniform criteria for recording coronary events have been applied to 37 populations in 21 countries for a period of 10 years [10].
Population-based register on the basis of routine databases
Events are identified using mortality data and HDR. This register has existed for many years in the northern countries, where all individuals are identified by a PIN which allows record linkage between different information sources. It is economical, covers the whole country, all age groups and collects large numbers of events. The main objective of administrative databases is to produce relevant statistics to plan health services and healthcare expenditure and to give internationally comparable data on mortality, causes of death and hospital admissions. The register is not primarily planned for research purposes but is increasingly used in epidemiological research. Its strength lies in the fact that it covers the whole country and the completeness is close to 100%. The weakness lies in the fact that data are not standardized to the same degree as in the disease-specific data collection and that the clinical and paraclinical data available are limited. If used in research, the register on the basis of routine databases needs to be carefully validated. AMI/ACS registers on the basis of administrative data, such as HDR and death certificates, have been employed in Denmark, Sweden and Finland to obtain national rates of AMI/ACS incidence, mortality and case fatality [17–23].
Hospital-based register
A hospital-based register provides the number of hospitalizations but does not provide data on less severe events and out-of-hospital mortality. Hence, it cannot directly be used to estimate incidence or prevalence in a defined population.
Even so, case series from hospital-based registers present important clinical information about AMI/ACS.
A hospital-based register collects information about hospital patients through surveillance of admission and discharge records. In particular, it provides detailed information on diagnostic and therapeutic procedures and on risk factor levels prior to admission to hospital. One primary objective of this type of register is to assess length of stay, in-hospital treatments and outcomes.
Target population
A population-based AMI/ACS register may cover a whole country; where this is not feasible, the population under surveillance would typically be residents of a defined region in the country. The target population should preferably cover a well-defined geographical and administrative area or region for which population data and vital statistics are routinely collected and easily available each year. Both urban and rural areas should be monitored: differences often exist with regard to exposure to risk factors, treatment of predisposing disease and access to facilities.
It is important that all cases among those with residence in the area are recorded even if the case occurs outside the area (completeness). In the same way, all cases treated at hospitals within the area but with residence outside the area must be excluded. If this is not possible, it is important to give an estimate of the magnitude of the loss of cases and establish whether it could be changing and interfering with the validity of the observed trends in the rates over a period of years.
It is also important to consider to what extent an area is representative of the whole country (representativeness): it should be representative according to the CVD mortality rate, distribution of risk factors (socioeconomic status and health behaviour) and distribution of health services (specialized hospital, GP).
The population to be monitored should be selected to produce estimates of disease rates that are sufficiently robust from a statistical point of view, so that trends can be established and data comparability ensured. In general, it is necessary to select more than one area to have a comprehensive picture for the whole country. In such cases, a coordination between the areas is recommended to ensure comparability. The target population should be selected taking the following parameters into account.
Age
The age range covered by the MONICA project was 35- 64 years. The EUROCISS project suggests the wider age range 35–74 years or even up to 84 years of age when possible, considering that more than half of the events occur in patients above 65 years of age. The age groups recommended from the EUROCISS project to present morbidity and mortality are decennia, in particular, the age ranges 35–44, 45–54, 55–64, 65–74 years and, if possible, 75–84 years. If administrative routine data are used, all ages will automatically be included, but for patients above the age of 85 the diagnostic information tends to be less reliable.
Age-standardized rates (35–74 and 35–84) are recommended using the European Standard Population as reference.
Sex
The differences in AMI/ACS incidence and mortality between men and women are well documented in the literature. Therefore, it is important that the same high quality data collection methods are applied to both women and men.
Population size
The size of the population under surveillance is determined by the number of events. The number of events is determined by the definition of the event and the event rate in the age groups included. In most cases the population size has to be determined on the basis of mortality statistics. Notably, the mortality rate for IHD is greater than that for ACS which is greater than the mortality rate for AMI; in addition, the age-specific mortality rate for men is greater than that for women.
This means that to estimate attack rates in middle-age participants with the same degree of precision, the population should be larger for women than for men.
To estimate the size of the population under surveillance for the register, the age range 45–74 years, (excluding 35–44 years where few events occur), is taken into consideration. To be eligible to participate in an AMI/ACS population-based register, a minimum of 300 coronary events (fatal and nonfatal, men and women together) per year in the population ages 45–74 years is necessary. The minimum of 300 total events has been established to detect a decrease by 2% in attack rate per year, taking into account that the population to be under surveillance could range between approximately 1800000 (all ages) in a low incidence country like Italy and 200000 (all ages) in a high incidence country like Finland, basing the calculation on female attack rates, usually lower than male attack rates (1998–99 Register data).
If more areas are enrolled, it would be desirable that the same number of 300 total events is considered for each single area.
Patient eligibility
A patient is considered eligible for inclusion in a population-based AMI/ACS register only if he/she is resident in the area under surveillance, meets the selected age and had an AMI/ACS event within the defined time period.
Data sources
To monitor AMI/ACS in the general population, the following sources of information should be available at a minimum: mortality records with death certificates; and, HDR with clinical information.
Some events occur suddenly and patients are not able to reach the hospital and some nonfatal cases may not be referred to hospital for treatment. Therefore, additional sources are usually needed to achieve complete information on all fatal and nonfatal events: clinical pathology laboratories (autopsy register), nursing homes, clinics, emergency or ambulance services, GPs, drug dispensing registers.
Death certificate
The death certificate provides complete data on fatal events and is collected in a systematic and continuous way in all EU countries. Mortality statistics are easily accessible in all countries but are usually published in a detailed and complete form after 2–4 years.
The format of the death certificate varies from country to country but generally includes personal identification data, date and place of death (i.e. municipality, nursing home, hospital or other) and causes of death (underlying, immediate and contributing). CVD causes of death are coded according to the ICD. Problems of temporal and geographic comparisons derive from the different versions of the ICD adopted over time (seventh, eighth, ninth, tenth revisions) and from different coding practices in each country. Furthermore, diagnostic criteria for coding death certificates are not defined at international level and ICD versions are updated every 10 years by WHO. Some countries code the underlying cause of death only.
The reliability of mortality data depends on the completeness and accuracy of the vital registration system of the country as well as the registration and coding of causes of death. When the proportion of deaths coded as ‘unknown cause of death’ is higher than 5%, cause specific mortality data should be used with caution. The accuracy of the recorded causes of death depends on the autopsy rate. This rate varies largely between countries and over time. In some countries the autopsy rate has declined in recent years, which is a problem for the use of mortality statistics in disease surveillance.
Hospital discharge records
HDR give the number of hospitalizations for AMI/ACS, which are absolutely necessary to monitor CVD. Moreover, clinical information and medical care reported in hospital documents are important for validation of events. Hospital discharge data are available in most EU countries, but in some countries only as aggregated tables without detailed information on age and sex distribution and without AMI/ACS as separate diagnostic categories.
HDR include personal data, admission date, type of hospitalization (urgent, ordinary or transfer to other structure) and discharge diagnoses. Hospital discharge diagnoses are coded by ICD codes (currently ICD-9 or ICD-10). For some countries, only a limited number of diagnoses are coded.
Problems in the assessment of a specific coronary event may arise when an acute event is followed by a period of rehabilitation or transfer to other wards and the event could be counted more than once.
Discharge diagnoses are not validated on a routine basis and validation studies are necessary to check the diagnostic quality. The validity of a hospital discharge diagnosis may vary on the basis of patient characteristics, geographical region and type of hospital or clinic.
Hospital admission policies vary over time and place; the registration of the most severe cases dying shortly after the arrival to the hospital differs between hospitals, depending on the administrative procedures connected to hospital admissions. HDR may also include patients not resident in the area under surveillance.
The adoption of new diagnostic techniques, such as troponin, may cause major changes in event rates estimated from hospital discharge data.
A further problem may derive from the use of DRGs. In some countries, hospital reimbursement is based on the DRG tariff system, which is built on equal-resources criteria and aggregates events in major diagnostic categories (MDC).
Countries using the DRG system are Denmark, Finland, France, Germany, Italy, Norway, Portugal, Spain and Sweden. To assess the occurrence of AMI/ACS, HDR from all hospital departments should be used. If this is not possible, then at minimum, the following departments must be taken into consideration:
cardiology;
heart surgery;
intensive care (an intensive care unit, including any type of acute medical unit);
medical (a general medical ward, including a geriatric unit);
rehabilitation (a specialized rehabilitation unit);
other (other units, e.g. outliers or patients on surgical wards).
Autopsy register
Not all countries perform autopsy on suspected or sudden deaths on a routine basis. Autopsy is performed on violent deaths or on deaths occurring in hospital when clinical diagnosis is undetermined. The first type is performed by a forensic medicine specialist, the second by a pathologist of the hospital where death occurred. Data from autopsy register refer therefore to a low percentage of deaths but provide a more valid diagnosis to complement the information reported on the death certificate.
Nursing home and clinic
Nursing home and clinic mainly provide data on cases among elderly patients who sometimes get care from these institutions without being admitted to hospital. Therefore, information on events occurring in the nursing home can be critical, especially if the register covers elderly patient up to 84 years of age.
In some countries rehabilitation after an acute event is provided by the rehabilitation clinic which may give information on patients who have received the acute care outside the region.
Emergency and ambulance services
Data provided by emergency and ambulance services are useful to integrate information for register implementation as patients dying from sudden death or experiencing fatal AMI/ACS are not always able to reach the hospital. These services are able to provide data otherwise not obtainable, such as electrocardiogram (ECG) during the acute phase of the event, blood pressure measurement, level of consciousness and muscular deficit at the time of event occurrence in paucisymptomatic patients recurring to emergency services. The need of very urgent medical treatment often makes information partial but the integration of these data with those from other sources of information contributes to the implementation of the register and event validation.
General practitioner register
A GP register gives information on those events which do not reach the hospital and for those patients who are hospitalized outside the area of usual residence. This register may also provide an adequate coverage for prevalence of old MI. This network operates in a few countries (e.g. The Netherlands and UK).
GP networks may be affected by selection bias as usually only volunteer GPs participate in studies. For this reason data from GP networks requires validation.
Drug dispensing register
In some member countries, patients may receive comprehensive drug reimbursement under their national sanitary system, and so drug prescriptions can serve as a proxy for disease. Prescribing guidelines for CVD indicate prescription of antihypertensives, low-dose aspirin, antiplatelets, anti-diabetics and statins. The administration of thrombolytic therapy can also be used as a proxy for disease.
Methods
Definition of events
The disease under surveillance is AMI (ICD-9 410; ICD-10 I21, I22) and the broader diagnostic group is ACS (ICD-9 410–411; ICD-10 I20.0, I21, I22). AMI is defined as myocardial cell death due to prolonged ischaemia [5, 24].
Criteria for acute myocardial infarction/acute coronary syndrome events
The diagnosis of AMI/ACS events is based on symptoms, ECG changes, elevation of biomarkers, and in fatal cases, autopsy findings. Since the early 1980s, the MONICA definition has been used for standardized diagnostic classification of suspected cases of AMI and IHD death (Table 5) [9]. The situation changed with the adoption of more sensitive and specific biomarkers of myocardial injury, first creatine-kinase MB mass (CK-MBm) and then the introduction of cardiac troponins (troponin T and troponin I). In the year 2000, the Joint European Society of Cardiology (ESC) and the American College of Cardiology (ACC) [5] created a new consensus document redefining AMI (Table 6).
In 2003, new case definitions were published as an American Heart Association (AHA) statement (Table 7) [6].
A more recent classification is proposed by the British Cardiac Society (BCS, Table 8) [7].
Identification of events
Fatal events include ICD-9 codes 410–414 (ICD-10: I20-I25) as the underlying cause of death as these codes include the majority of definite and possible events. Nonfatal events include ICD-9 codes 410–411 (ICD-10: I20.0, I21, I22) as primary or secondary hospital discharge diagnosis (Table 9).
Onset and survival
AMI/ACS events are defined as first ever, recurrent, nonfatal and fatal.
First ever AMI/ACS event: refers to people who have never had an AMI/ACS event before.
Recurrent AMI/ACS event: for a new episode of symptoms to be counted as a new or recurrent AMI/ACS event, general AMI/ACS criteria must be met and either:
- onset is day one (1);
- a new AMI/ACS occurring after 28 days is a new event.
Criteria for definition of acute myocardial infarction, MONICA Project

For further information, http://www.ktl.fi/publications/monica/manual
Criteria for definition of acute, evolving or recent myocardial infarction, ESC/ACC criteria

CK-MB, creatine-kinase; ECG, electrocardiogram; ESC/ACC, European Society of Cardiology/American College of Cardiology; MI, myocardial infarction. Source: The Joint European Society of Cardiology/American College of Cardiology Committee (2000).
Case definition for AMI/ACS in epidemiology and clinical research studies, AHA criteria
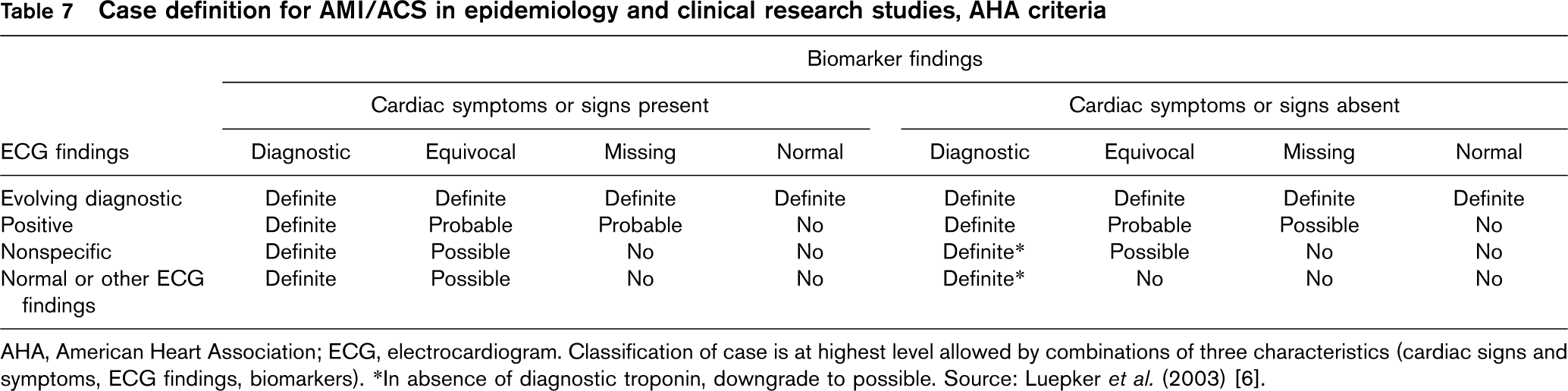
AHA, American Heart Association; ECG, electrocardiogram. Classification of case is at highest level allowed by combinations of three characteristics (cardiac signs and symptoms, ECG findings, biomarkers). ∗In absence of diagnostic troponin, downgrade to possible. Source: Luepker et al. (2003) [6].
Spectrum of acute coronary syndrome, British Cardiac Society
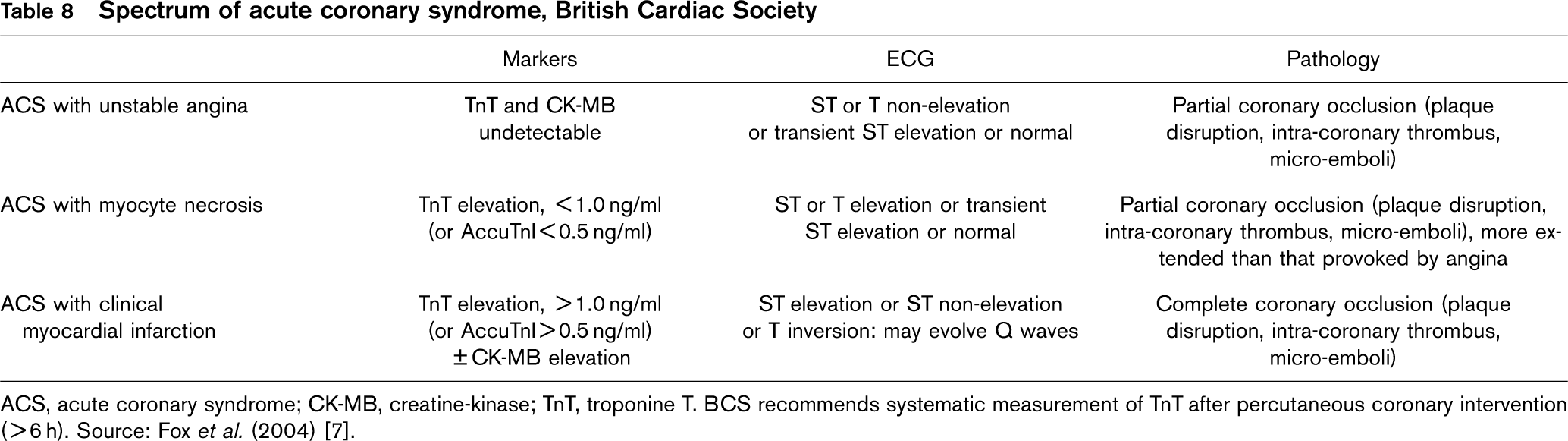
ACS, acute coronary syndrome; CK-MB, creatine-kinase; TnT, troponine T. BCS recommends systematic measurement of TnT after percutaneous coronary intervention (>6 h). Source: Fox et al. (2004) [7].
ICD codes of interests for definitions of events
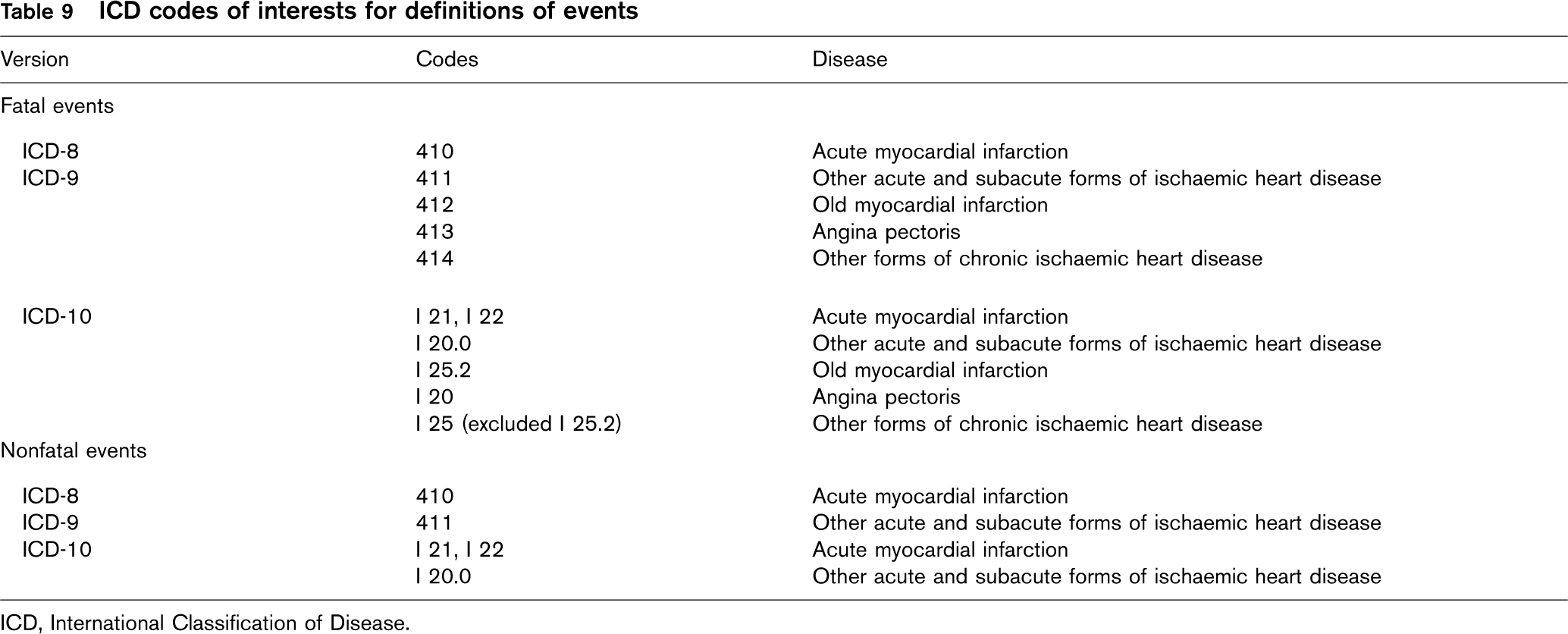
ICD, International Classification of Disease.
If a patient experiences further acute symptoms suggestive of AMI/ACS within 28 days (as stated above) of the onset of a first episode, this second episode is not counted as a new AMI/ACS event. Equally, if a patient experiences further acute symptoms suggestive of AMI/ACS after 28 days (as stated above) of the onset of a first episode, this second episode is counted as a new event.
Nonfatal AMI/ACS event: refers to cases who survived at least 28 days from the onset of the AMI/ACS symptoms.
Fatal AMI/ACS event: refers to cases who died within 28 days of AMI/ACS symptoms onset. It should be noted that each event is registered separately.
Indicators
Attack rate
Attack rate is calculated identifying the events by using primary or secondary hospital discharge diagnoses or underlying cause of death for out-of-hospital deaths. Almost 32% of the patients die before they reach the hospital, and therefore a hospital discharge register alone is not sufficient [25].
Incidence rate
This indicator can be estimated only if information on first event is available.
In northern countries an event is defined as ‘first’ if there is no discharge with AMI as primary or secondary diagnosis in-hospital discharge records of the past 7 years.
Case fatality
Case fatality is the proportion of events that are fatal by the 28th day.
The EUROCISS project recommends 1-day and 28-day case fatality. All in-and out-of-hospital fatal and nonfatal events are to be considered as denominator.
Data collection methods
The different types of registers described in ‘Surveillance methods and types of registers’ use different data collection methods. Registers with disease-specific data collection can be divided into population-based registers using record linkage of administrative databases (mortality and HDR) and disease-specific registers using hot and cold pursuit for the identification of events.
Population-based register on the basis of routine administrative data
In recent years, the development of computerized record linkage has made it possible to overcome obstacles in linking existing administrative databases. Record linkage methods can be summarized into three broad categories: manual, deterministic and probabilistic.
Manual matching is the oldest, most time-consuming and most costly method. In general, it is not a feasible option when large databases are involved.
Deterministic linkage matches records from two data sets (or two records from different locations in a single data set) using a unique variable (e.g. PIN or hospital chart number) or by full agreement of a set of common variables (e.g. name, sex, birth date).
Probabilistic linkage [26] is used to identify and link records from one data set to corresponding records in another data set (or two records from different locations in a single data set) on the basis of a calculated statistical probability for a set of relevant variables (e.g. name, sex, date of birth). This type of linkage links records with a specified high probability of a match. The method requires detailed prior knowledge about various measures of the relative importance of specific identifier values in both files that are to be linked.
The main limitations of record linkage are the difficulties in:
obtaining administrative files for research purposes: mortality data files are usually available at the National Institute of Statistics, whereas hospital discharge data are available at the Ministry of Health. These kinds of data are anonymous and therefore do not allow record linkage. Nominal files of both mortality and hospital discharge are available at the regional level or at the sanitary units;
combining data: missing events are mainly explained by errors in PIN or in name and they lead to unsuccessful record linkage;
defining and obtaining minimal data set (for mortality: PIN; family and first name; date and place of birth; sex; residence; date and place of death; underlying and secondary causes of death. For hospital discharge diagnosis the same variables should be considered together with admission date and hospital discharge diagnoses);
obtaining necessary funds for processing large administrative files.
The national AMI registers in the northern countries use record linkage between HDR and causes-of-death registers as the basis for the register. The linkage as such is easy because of the PIN attached to every citizen in the country.
The linkage, however, has to be followed by many specific definitions on how to handle primary and secondary diagnoses, underlying and contributory causes of death, transfer between hospitals with differences in the diagnoses between the admitting hospital and the hospital where the patient is transferred, how to define date of attack, first time events, reinfarctions, etc.
Practical suggestions on how to handle these problems have come from the work carried out in northern countries [23, 27, 28].
Specific acute myocardial infarction/acute coronary syndrome population-based register
Hot pursuit [15] This method of detecting events involves identifying patients with acute illness in hospital and interviewing them directly while they are under care. The problem with this method is that the data collection technique is very difficult to standardize (e.g. descriptions of symptoms may vary with the observer). Periods of staff shortages or holidays may lead to loss of cases that cannot be recovered and a large team is needed to search the wards for cases. Some information, however, may be more complete than that obtainable from case notes.
Notification of events should be instituted on a routine basis checking admission registers on the wards.
Although the extreme forms of hot pursuit involve getting the information from the patient who is acutely ill, an alternative is to use the hot pursuit method to identify the patients of interest and to mark their notes or list them for review later. An efficient and reliable routine is needed for picking up the case notes at an identifiable point in their processing.
A benefit of the hot pursuit method is that information on the diagnosis is collected soon after admission. This has its limitations, however, as initial diagnosis can sometimes be superseded by subsequent tests and other more detailed investigation.
Residents hospitalized outside the area will always have to be registered by cold pursuit, weeks or months later.
Cold pursuit [15] Use of discharge diagnoses rather than hospital admissions is a more simple system of identifying events for the study. Its advantage is that it can be done months or years after the event but it is limited because the information in the case notes may not be complete and the notes themselves may not be accessible.
Once the event has been identified, if validation is required, medical notes should be obtained to extract the necessary information from them.
When a register is launched for the first time, a plan for future evaluation of trends is recommended. This can be achieved by continuous surveillance as part of a broader health information system or annual register compiled at 5–10-year intervals. The minimum recommended period of observation is one complete calendar year because of possible seasonal variation.
Combined approach A mix of hot and cold pursuit ensures the most complete identification of coronary events. Some of the patients must have been identified as soon as possible after symptoms onset with the possibility of direct examination, whereas the remaining events are based on routine data.
It is difficult to check up on a hot pursuit system several months later, but discharge lists can be used as a backup method to ensure that the hot pursuit method had detected all the diagnosed cases. Residents hospitalized outside the area and other late-detected cases mean that a proportion of events will always have to be registered by cold pursuit, weeks or months later.
Quality control
Quality control of registers is extremely important for valid monitoring and comparison between regions and countries. The quality of the register depends on:
completeness of cases and completeness of information;
internal validity;
external validity (representativeness).
Completeness of cases and completeness of information
Completeness of cases means that all AMI/ACS cases in the target population have been included; that is both cases taking place within the region and cases taking place outside the region. The register also has to cover hospitalized cases whenever they occur during day/night or winter/summer as well as cases occurring outside hospital (e.g. sudden death among patients who never reach the hospital).
Completeness of information means that all relevant information has been registered (e.g. place of treatment, date of admission, date of discharge, PIN, sex, hospital discharge diagnostic codes, intervention/procedure codes, department/ward, date of birth).
The most important source of systematic bias in estimating incidence is related to the coverage of event registration. The registration system must attempt to identify all possible cases of the disease that have come to the attention of the existing medical and medicolegal sources. The completeness of event identification and the completeness and availability of information, obtainable for event recording and diagnosis, depend on the existing standard of medical care: if the medical care system misses or misdiagnoses cases, the register cannot remedy the omission.
When the event is defined (codes and duration), it may be easy to identify duplicate coding and to take out information for quality control purposes. Duplicate codes may include events transferred from one ward to another, for example for an acute percutaneous coronary intervention (PCI). In some cases the duration of the admission is very short (>2 days) either because of transferral or because of diagnosis misclassification. These cases may also be picked up for validation.
Cases not admitted to general hospitals are a problem when the registration system is based only on hospital records. Another source of potential loss of identification is private practice: private physicians and hospitals may be less cooperative than those in the public system. In private hospitals the staff may be more sensitive to criticism and anxious to show how they register medical documents.
The identification of fatal events is in some ways less difficult than that of nonfatal events. Whereas survivors may be lost in the totality of inhabitants of the surveillance area, death is unequivocal. Registration of causes of death, however, may be incorrect and needs to be validated and collection of information of deaths occurring outside the area of residence has to be ensured. It is to be expected that some events occur outside hospital. If the proportion of fatal events coded as hospitalized is very high it may indicate incomplete registration of out-of-hospital AMI/ACS deaths.
Identification of potential events may be based on many different data sources. This may involve a considerable amount of record linkage, which is facilitated if the PIN is adopted.
Another problem relates to medical records whose quality may be variable: younger patients may have had no other illness episodes and the records may be restricted to the relevant coronary event. In older patients, the identification of the event is more complicated due to the existence of comorbidities.
Internal validity
The most important question regarding validity concerns the diagnostic information. The diagnostic criteria for the event definition are valid if they measure the AMI/ACS they claim to measure. Validation evaluates the sensitivity, specificity and predictive value of the registered diagnosis compared with a golden standard. To validate coronary events, the MONICA diagnostic criteria [9], the new criteria of the joint ESC/ACC committee [5], the AHA criteria [6] or the BCS criteria [7] may be applied as the golden standard.
Nowadays, the MONICA diagnostic criteria (see Table 2b) are the most widely used for the validation of events from population-based registers. The introduction of the new ESC/ACC criteria, on the basis of biomarker findings (troponin, CK-MB), does not cover early and other fatal cases, and nonfatal cases in which tests are partial, delayed, missing or curtailed [29]. The change in diagnostic criteria for AMI and the introduction of the new concept of ACS does not facilitate comparison and interpretation of trends. A comparison between MONICA diagnostic criteria and the different new criteria [30] has been made and published; it concludes that the AHA definition, when applied using troponins, identifies a sizeable new group of MI patients at high risk of a recurrent event among persons with suspected ACS.
Validation studies of routine statistics have been carried out over the years with heterogeneous results that were due to differences in methodology, or that reflected true differences in the validity of the routinely collected data between countries [17, 22, 27, 28]. Some studies have been carried out comparing community registers with national statistics and data from the MONICA project [23, 31]. These findings stress the importance of validating routine mortality and hospital statistics against the national register to determine whether and how they can be used to reflect true attack rates and mortality. Consistency of coding with the diagnosis and consistency of coding/comparability of the information for different areas of the country and over time represent other issues for validation.
If it is not possible to validate all the events included in the disease register or in the mortality routine statistics, the objective for validation should be to evaluate a sample of events. The sample should be distributed across a full year to ensure that potential seasonal or other time-related variations of diagnostic patterns are traced.
External validity
It is not essential that the whole country is covered by a surveillance system, but it is essential that the registration of events is complete with regard to events occurring in the target population. It is important to know how representative the register is for the whole country according to the IHD mortality rate, the distribution of risk factors (socioeconomic status and health behaviour) and the distribution of health service (specialized hospital, GP).
For the population chosen there must be good demographic data subject to at least annual revision; inaccuracy may become apparent years after the period being studied because of the results of a decennial national census.
A careful description of the population characteristics may help to describe how representative the target population is for the whole country.
Methods to evaluate diagnostic quality
Register validation can include examination of each single case or validation on the basis of random samples for diagnostic information, name, age and residence.
Validation has to be carried out by an epidemiological team not involved in the treatment of patients. For local registers with a limited number of cases it may be possible to validate each single event, but registers covering wider areas, for practical reasons, can only validate data on the basis of random samples of suspected cases recorded during a selected period or during some days each month. One selection method consists of choosing some days each month and recording all events, extracted either from hospital discharge or mortality records, which occur in those days. In this way seasonal variation can be traced.
To produce validated indicators, a conditio sine qua non is to allow access to personal relevant medical records and routine raw data of health statistics. In some cases it is possible to validate a register by linking the routine register to an independent data source, for example a high quality register for a small area within the region.
Validation of diagnosis in fatal events
A register of AMI/ACS is meant to produce frequency indicators of the acute forms of coronary events and of coronary death. These correspond to ICD-10 codes I 20–25 in the underlying cause of death. IHD, however, is often associated to other comorbidities, which might produce occasional miscoding of IHD in national mortality registers, in spite of the ICD coding rules. The percentage of such misclassification varies by country, age and sex. It is necessary to ensure that no true cases are hidden under other diagnoses (false negatives) and hence missed in AMI/ACS registration. In the validation process it is therefore necessary to review and validate the diagnosis in at least a sample of cases for the following diseases, against the standard chosen, in particular when they are followed by IHD as secondary cause of death: sudden death, heart failure, pulmonary thromboembolism, acute pulmonary oedema, aortic aneurisms, arrythmias, diabetes, hypertension.
Some countries only code the underlying cause of death, whereas others code all four causes of death. Those who rely on underlying cause of death only should perform validation at least twice in every 10-year period and for a full year or on a sufficiently sized sample for a full year. Depending on the percentage of false negative diagnoses for IHD death found in the first validation, decisions should be taken about the intensity and duration of the validation exercise for fatal cases throughout the registration period. A false negative rate above 10–15% should in principle be an indication to perform diagnostic validation of death certificates on a continuous basis rather than on a periodic or a sample basis.
Validation of diagnosis in nonfatal events
Registration of nonfatal events is based on both primary and secondary hospital discharge diagnoses. In those countries which register the primary diagnosis only, particular attention should be given to this type of validation. Manual coding of the secondary diagnosis may be necessary during the validation to ensure comparability with other countries and completeness of registration.
In addition, there are elective treatment procedures that might hide ACS.
Many AMI cases are treated during the acute phase with PCI and some of these cases may be identified by the ICD-9CM codes for the interventions: code 36.1 for coronary artery bypass graft and codes 36.01, 36.02, 36.05, 36.06 (stent) for percutaneous transluminal coronary angioplasty. Revascularization procedures alone are not sufficient to define the acute event.
Ethical issues
The Helsinki Declaration requires that biomedical research with human participants must conform to generally accepted scientific principles.
The ‘Recommendation n. R (97)5 of the committee of ministers to EU member states on the protection of medical data’ [32] gives guidelines on how medical data can be registered, stored and used in a way that ensures the rights and the fundamental freedoms of the individual and in particular the right to privacy (adopted by the Committee of Ministers on 13 February 1997 at the 584th meeting of the Ministers’ Deputies).
In the following the most important recommendations are presented.
‘Medical data should be collected and processed only by healthcare professionals, or by individuals or bodies working on behalf of healthcare professionals. Individuals or bodies working on behalf of healthcare professionals who collect and process medical data should be subject to the same rules of confidentiality incumbent on healthcare professionals, or to comparable rules of confidentiality.’
Therefore, it is essential that a cardiologist or physician (or study nurse) with proven experience in the field of CVD is involved in the coordination of the AMI/ACS register.
‘Medical data shall be collected and processed fairly and lawfully and only for specified purposes.’
‘Medical data may be collected and processed:
if provided for by law for:
public health reasons; or
subject to Principle 4.8 (processing of genetic data for the purpose of a judicial procedure or a criminal investigation should be the subject of a specific law offering appropriate safeguards), the prevention of a real danger or the suppression of a specific criminal offence; or
another important public interest; or
if permitted by law:
for preventive medical purposes or for diagnostic or for therapeutic purposes with regard to the data subject or a relative in the genetic line; or
to safeguard the vital interests of the data subject or of a third person; or
for the fulfilment of specific contractual obligations; or
to establish, exercise or defend a legal claim; or
if the data subject or his/her legal representative or an authority or any person or body provided for by law has given his/her consent for one or more purposes, and in so far as domestic law does not provide otherwise.’
Whenever possible, medical data used for scientific research purposes should be anonymous. Professional and scientific organisations as well as public authorities should promote the development of techniques and procedures securing anonymity. However, if such anonymisation, would make a scientific research project impossible, and the project is to be carried out for legitimate purposes, it could be carried out with personal data on condition that:
the data subject has given his/her informed consent for one or more research purposes; or
when the data subject is a legally incapacitated person incapable of free decision, and domestic law does not permit the data subject to act on his/her own behalf, his/her legal representative or an authority, or any person or body provided for by law, has given his/her consent in the framework of a research project related to the medical condition or illness of the data subject; or
disclosure of data for the purpose of a defined scientific research project concerning an important public interest has been authorized by the body or bodies designated by domestic law, but only if:
the data subject has not expressly opposed disclosure; and
despite reasonable efforts, it would be impracticable to contact the data subject to seek his consent; and
the interests of the research project justify the authorisation; or
the scientific research is provided for by law and constitutes a necessary measure for public health reasons.’
Record linkage between mortality and HDR is possible in countries which have adopted a PIN on a national level. Other nominal data (such as name, sex, date and place of birth) are usually available at a regional level. Record linkage is important to identify the event by matching admissions and discharges or admissions and deaths, thus avoiding double counting, which may occur when, for example, the same patient transferred to another ward (e.g. from cardiology to cardiovascular surgery and then to rehabilitation) is registered in the HDR more than once.
Moreover, the identification of the patient is essential for the event validation when it is necessary to collect and examine the history and clinical documentation and to assess case fatality at different intervals (28 days, 6 months, 1 year). Before starting any study, it is recommended to seek approval from the local ethics committee.
Economic consideration
Overall IHD is estimated to cost the EU economy over €45 billion a year. Of the total cost of IHD, 51% is due to direct healthcare costs, 34% to productivity loses and 15% to the informal care of people with IHD [1]. Cost considerations are essential before implementing a population-based register.
Without a valid surveillance system, it is not possible to plan and evaluate health services for populations, implement interventions for prevention and identify ‘vulnerable’ subgroups in terms of burden of disease such as the elderly, the young, the poor, the unemployed. Surveillance and evaluation mean a systematic way of learning from experience and using it to improve current activities and promote better planning by careful selection of alternatives for future actions and allocation of resources. The economic benefit of a good surveillance system clearly exceeds the cost of the registers.
A population-based register may be costly and to produce meaningful data it needs to be in operation for at least one year, but preferably for some years or continuously. The importance of a valid and efficient AMI/ACS register, however, justifies the high implementation costs and the consequent need to find adequate financing.
The register on the basis of record linkage between administrative databases is the most cost-effective, but this register depends on the data quality of the HDR and the cause-of-death register and also on the possibility of a valid record linkage. In addition, methods need further evaluation and implementation. Notably, if the hospital discharge and mortality registers are available for record linkage, the costs for the linkage and dissemination of results are low. The main costs for using this methodology for assessment of incidence in a defined population concern the need to perform regular validation of the diagnostic information. It may be recommended to include basic epidemiologic research in the costs, which may include analysis of risk factors by linkage to health interview surveys and of treatment effect by linking the register to other data sources (e.g. data on drugs and on invasive procedures). Sometimes access to data produces separate costs.
The register based on disease-specific data collection is more expensive especially if hot pursuit is used. Besides the cost mentioned above, this type of register also needs funding for the detailed prospective data collection and for validation of diagnostic information. The data collection includes identification of patients, reading medical records, making inquiries to additional data sources, and filing and validation of the data. This means that a team of epidemiologists, nurses, medical doctors and informatics dedicated to this work full time is absolutely necessary. It should be recognized that this type of register usually collects information that permits analyses of research questions beyond the monitoring of AMI/ACS incidence, mortality and case fatality. This may concern the role of risk factors for disease occurrence or the role of treatment for survival in patients.
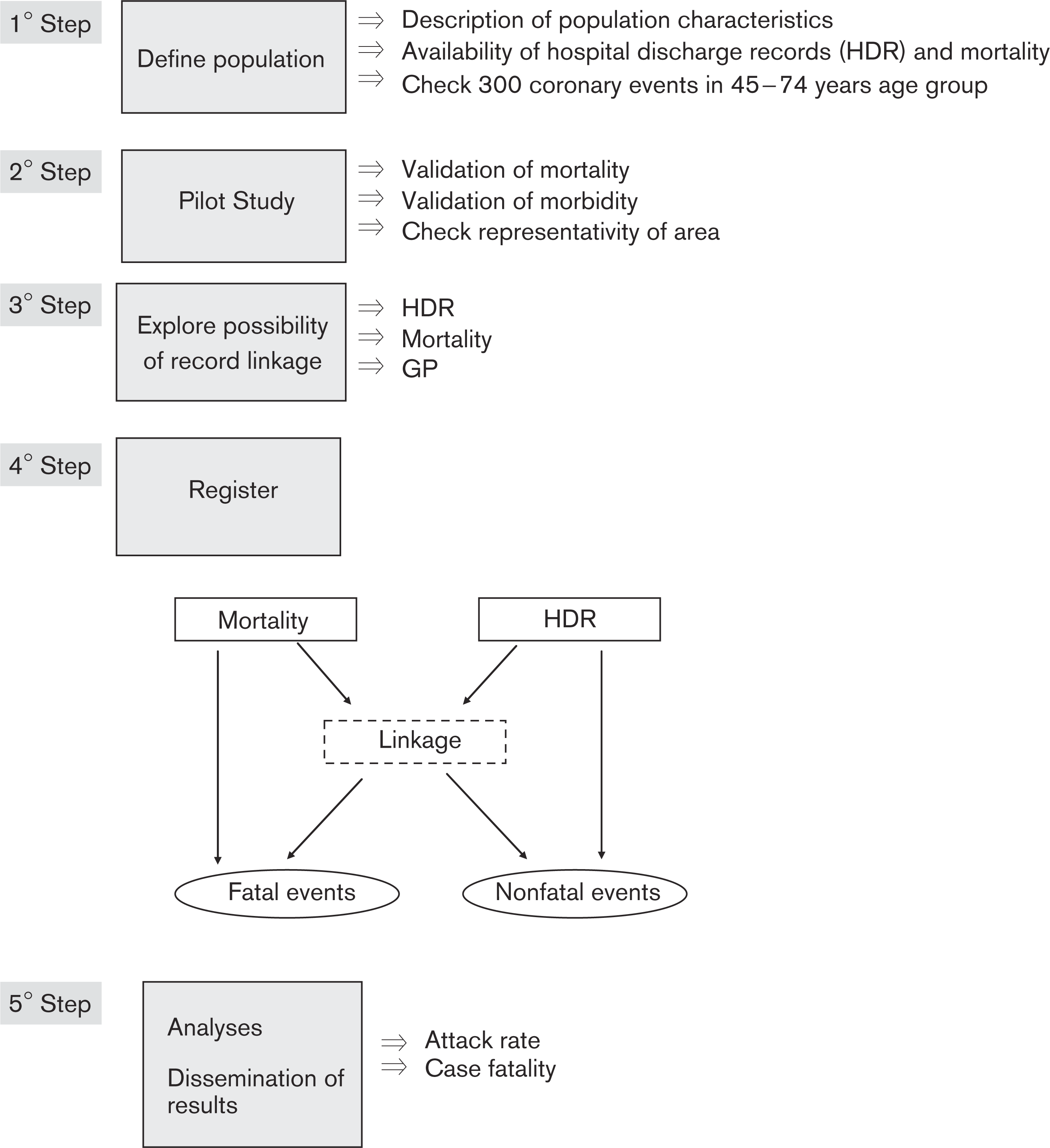
Description of the stepwise procedure for implementing an AMI/ACS population-based register.
Implementation: a stepwise procedure
This section describes the procedures required to implement an AMI/ACS population-based register taking into account the recommendations reported in this manual of operations.
The flow chart summarizes these procedures (Fig. 3).
Step 1. Define target population and routine data
Select a geographical administrative area with a population big enough to provide stable estimates. This means that a stable population in a representative area of the country with 300 fatal and nonfatal coronary events/year in the age range 45–74 years should be chosen.
Characterize population from a demographic point of view through a detailed description of the characteristics of the population under surveillance, in particular: demographic characteristics (age and sex distribution); socio-cultural characteristics (educational level, occupation, social group, unemployment rate, migration, immigrants with or without citizenship); characteristics of the healthcare system (specialized hospital, GP, rehabilitation clinic); macro and micro areas (urban and rural). Disease frequency is often different in macro areas of the country; a description of difference in mortality and risk factors allows to select those areas to be included in the surveillance system. Within the population-based surveillance study, the phenomenon of immigration plays an important role, therefore immigrants coming from European and extra-European countries resident in the study area must be enrolled. Geographical or administrative borders of the surveillance areas must be clearly defined.
Analyse existing hospital discharge and mortality data. Events in nonresidents occurring in the study area or admitted to hospital in the study area do not qualify. Events of residents occurring out of the area do qualify. Efforts must be made to find them or to estimate the potential loss and whether or not this could be changing and interfering with the validity of the observed trends in rates over a period of years.
Identify problems with these data: coverage, ICD version, identification of events, procedures, unit of analysis (number of events or discharges and/or number of patients), PIN, coherence with previous studies, etc. Data files are usually available at the regional level in detailed forms.
When a register is launched for the first time, a plan for future follow-up to measure trends is recommended. This can be achieved by a continuous surveillance as part of a broader health information system or by annual registeration repeated at 5–10 years intervals.
Step 2. Perform a pilot study and validate routine data
Before starting an AMI/ACS population-based register or a large-scale use of linked administrative data, a pilot study on available hospital discharge and mortality data in a small area is recommended to study the feasibility and to estimate internal validity.
Validation studies on available data include:
estimation of coverage: comparison of different routine data sets (electronic or manual), number of patients treated in and out-of-area, hospital/mortality ratios, age and sex ratios, principal vs. secondary and/or procedure diagnoses;
validation of discharge diagnoses according to a standard method (including revision and abstraction of medical records) in a random sample or in all cases;
validation of mortality causes according to a standard method in a random sample or in all cases;
analysis of demography and representativeness of the area in comparison with the region or country;
selection of age range of interest (35–74 or 35–84 years).
Step 3. Carry out record linkage of administrative data
In the northern countries, where every citizen has a PIN included in national registers of hospital discharges and deaths, record linkage for the identification of AMI/ACS events is efficient and reliable. For countries that have not adopted the PIN it may be much more difficult to perform this step. Files have to be organized in the same format and include the same variables (family name, name, date of birth, residence and place of birth).
It is recommended to:
explore the feasibility of record linkage within hospital records-probabilistic or deterministic approach or using either the PIN (within the same hospital, among hospitals of the area, among hospitals at regional or national level). When hospital records are collected at regional or national level, it is possible to collect events that occur out of hospital;
explore the feasibility of record linkage between hospital records and mortality register (probabilistic or deterministic approach or using the PIN);
explore the feasibility of linkage with other sources of information (e.g. GP, drug dispensing register). Not all GPs are organized in networks, with computerized documentation of patient history; when they are, the definition of events rarely uses the same diagnostic criteria.
Step 4. Set up an acute myocardial infarction/acute coronary syndrome population-based register After performing steps 2 and 3 it is possible to set up an AMI/ACS population-based register following (A) record linkage between administrative registers or (B) disease-specific data collection.
A. Register based on record linkage between routine administrative data:
when the linkage procedure between hospital discharge and mortality records is feasible, it is important to define the event, the duration, how to handle transfer between hospitals with difference in the diagnoses between the admitting hospital and the hospital where the patient is transferred, how to define first time events, recurrent events, fatal and nonfatal events, etc. (see Definition of events). A linkage system and a control for duplicate records should be set up;
validation of diagnostic information is recommended in a random sample of sufficient size of the identified events, with the estimation of sensitivity and specificity and positive predictive value of the defined events;
population data by age and sex of the area under surveillance are needed to estimate incidence, recurrence, attack rate, case fatality and mortality rates;
periodic validations should be performed.
B. Register on the basis of disease-specific data collection:
set up a pilot population-based register with proven standardized protocol for AMI/ACS and evaluate pilot study results (coverage, completeness of information and diagnostic validity);
on the basis of the results of the pilot study, set up, if feasible, a full scale register and decide whether to use hot or cold pursuit;
then, if feasible, design the full-scale register (target population, data collection methods and validation procedures).
To set up a full scale register:
select one or more populations representative for the region or the country;
for each selected population set up a population-based register with approved standardized protocol for AMI/ACS;
write a detailed protocol for the data collection including validation procedures;
evaluate the coverage, representativeness and completeness of information;
if relevant, use the results from the register to validate administrative data.
Step 5. Disseminate results
Set up a strategy for analysis of data and for the dissemination of results to decision-makers, politicians and the broader population.
Publish yearly on a web site indicators of attack rate, incidence, case fatality according to sex and age-standardized with the European population as reference (35–74 and 35–84 years).
Use data for research. This is very important to ensure the high quality of the register over time. A high quality register can be the basis for good research.
Footnotes
Acknowledgements
This project has received financial support from the European Commission, Directorate General for Health and Consumer Protection-Grant Agreement No. 2003118, and from the CUORE Project of the Italian Ministry of Health.