6 Global risk assessment for cardiovascular diseases in women - do we need correction of the SCORE model for the Bulgarian population?
Y Yotov1; V Sirakova1; E Shipkovenska2
1University Hospital 1st Cardiology Clinic, Varna, Bulgaria; 2Medical University Department of Public Health, Sofia, Bulgaria
The global risk assessment became an important tool in the prevention strategy of cardiovascular diseases (CVD). According to the recent guidelines, a correction of the risk equations in relation to country-specific mortality or risk profile is recommended. Bulgaria is a country among those with highest CVD mortality and morbidity.
Purpose:! To correct the SCORE formula for high risk populations in Europe for the Bulgarian female population and to apply it to a sample of healthy Bulgarian women.
Methods: The 2001 gender-specific cardiovascular mortality in Bulgaria was used as baseline hazard in the original SCORE formula for high risk populations. The country specific mortality data in five-year age periods was logarithmically transformed and then linear regression was applied on thus transformed data. The original variables coefficients in SCORE were used. A graphical version was created. The modified formula was applied to a sample of 393 women from two large cities of Bulgaria without evidence of CVD. The correlation coefficient estimation, as well as Cohen's kappa analysis was used to compare the original and modified SCORE tables and ROC curve was created.
Results: The mean age of the sample used for the validation was 57.8±7.3 years, range 40–69. The modified SCORE table showed that the Bulgarian women reach the higher risk levels approximately 2.5 years earlier than their European counterparts and the level of their global CV risk is generally higher. The median global CV risk of the sample rises from 2.0% to 2.95% after adjustment. The modified and the original formula correlate excellently with Spearman's r=0.969, p>0.0001 and AUC=0.88, 95% CI=0.85–0.94 (?>0.0001). Only in 2.3% of the participants the two ways of calculating the CV risk totally disagree.
Conclusion: The Bulgarian women have higher levels of global risk for CVD and reach them approximately 2.5 years earlier in their life than the women in other European high-risk countries. Although there is a good agreement between the corrected and the original equation, there is an obvious need for modification of the SCORE model for the Bulgarian population.
7 Cardiovascular mortality in the Netherlands is better predicted by the low-risk SCORE equation than by the high-risk SCORE equation
SJ Van Dis1; D Kromhout2; JM Geleijnse2; WMM Verschuren1
1Nat Inst for Public Health & the Environment, Bilthoven, Netherlands; 2Wageningen University Division of Human Nutrition, Wageningen, Netherlands
Background: Cardiovascular risk management in the Netherlands, is based on the estimated 10-year risk for fatal cardiovascular diseases (cvd), which is calculated using the SCORE risk equation. The SCORE risk equation was developed, using risk factor data and subsequent cvd mortality in 12 European cohorts that collected their data in the 1970s and 1980s. Subsequently, risk prediction charts were developed for low and high risk regions, with the Netherlands being considered as a high risk region.
Purpose: To validate the SCORE-risk predictions for high and low risk European regions for the Netherlands.
Methods: Data from the Dutch MORGEN-project (Monitoring Project on Risk Factors for Chronic Diseases) were used. Baseline data on risk factors for cvd were obtained from 1993–1997, for 13,500 men and women aged 37.5–62.5 years in a random sample from three Dutch municipalities. 10-Year follow-up data on cvd mortality were provided by Statistics Netherlands, using ICD-10 codes similar to the ICD-9 codes as used in SCORE.
Results: Data are presented by risk categories presented for the SCORE high risk regions.
The observed 10-year cvd mortality was half of the expected 10-year cvd mortality predicted by the SCORE high risk regions in men (observed/expected (o/e) 0.42) as well as in women (o/e 0.44). The observed 10-year cvd mortality in MORGEN showed reasonable agreement with the 10-year cvd mortality predicted by the SCORE low risk regions (o/e 0.86 in men and 0.74 in women), especially in persons with a low to moderate risk. Similar results were found for risk categories of serum cholesterol, systolic blood pressure and smoking status.
Conclusion: SCORE risk charts based on high risk regions overestimate the risk of cvd mortality in the Netherlands. This overestimation can be explained by a steady decline in cvd mortality in this country. The cvd mortality risk for a healthy Dutch cohort from the 1990s appears to be similar to the cvd mortality risk in the low risk cohorts from the 1970s and 1980s.
8 Predictive accuracy of original and recalibrated Framingham risk score in the Swiss population
P Marques-Vidal1; N Rodondi2; M Bochud1; A Chiolero1; A Pecoud2; D Hayoz3; F Paccaud2; V Mooser4; G Waeber5; P Vollenweider2
1Inst. Univ. de Medecine Sociale et Preventive UPC, Lausanne, Switzerland; 2University of Lausanne Cardiovascular Prevention Clinic, Lausanne, Switzerland; 3Centre Hospitalier Universitaire Vaudois Medicine, Vascular Medicine, Lausanne, Switzerland; 4GlaxoSmithKline Medical Genetics, Philadelphia, United States of America; 5Centre Hospitalier Universitaire Vaudois Medicine, Internal Medicine, Lausanne, Switzerland
Objective: To compare the predictive accuracy of the original and recalibrated Framingham risk function on current morbidity from coronary heart disease (CHD) and mortality data from the Swiss population.
Methods: Data from the CoLaus population-based study (conducted between 2003 and 2006 on 5,773 participants aged 35–74 devoid of CHD) were used to recalibrate the Framingham risk function. The predicted number of events from each risk function were compared with those issued from local MONICA incidence rates and official mortality data from Switzerland.
Results: With the original risk function, 57.3%, 21.2%, 16.4% and 5.1% of men and 94.9%, 3.8%, 1.2% and 0.1% of women were at very low (>6%), low (6–10%), intermediate (10–20%) and high (>20%) risk, respectively. With the recalibrated risk function, the corresponding values were 84.7%, 10.3%, 4.3% and 0.6% in men and 99.5%, 0.4%, 0.0% and 0.1% in women, respectively. The number of CHD events over 10 years predicted by the original Framingham risk function was 2–3 fold higher than predicted by mortality + case fatality or by MONICA incidence rates (men: 191 vs. 92 and 51 events, respectively). The recalibrated risk function provided more reasonable estimates, albeit slightly overestimated (92 events, 5–95th percentile: 26–223 events); sensitivity analyses showed that the magnitude of the overestimation was between 0.4 and 2.2 in men, and 0.7 and 3.3 in women.
Conclusion: The recalibrated Framingham risk function provides a reasonable alternative to assess CHD risk in the Swiss population, albeit its ability to stratify risk among women is weak.
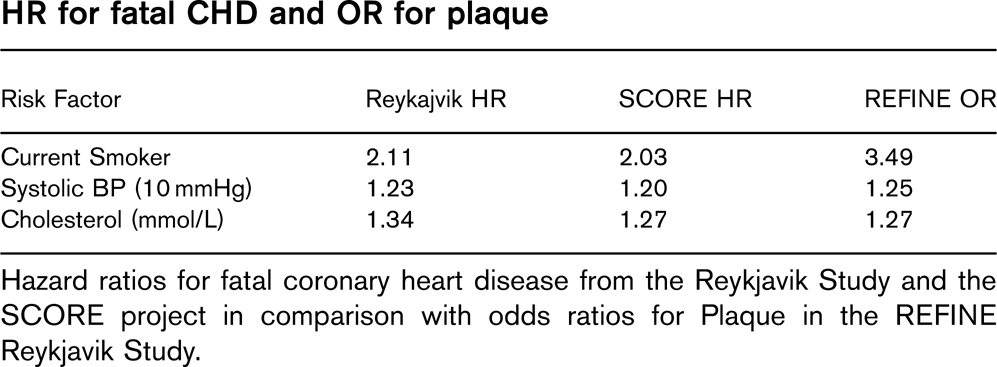
9 SCORE HDL Incorporation of high density lipoprotein cholesterol into the SCORE function
MT Cooney; T Leong; AL Dudina; CM Mc Gorrian; I Graham
Background: Systematic Coronary Risk Evaluation (SCORE) is a risk estimation system based on pooled data from 12 European cohort studies, including over 205,000 persons, representing 2.7 million person years of observation. Currently, the SCORE function estimates 10 year risk of cardiovascular disease (CVD) mortality based on gender, age, country of origin, smoking status, systolic blood pressure and either total cholesterol (TC) or TC/high density lipoprotein (HDL) cholesterol ratio. Counterintuitively, persons are classified to very similar levels of risk regardless of which lipid measure is used. We previously demonstrated the importance of HDL in the SCORE dataset. We hypothesized that a SCORE function containing HDL as separate additional variable would provide superior risk estimation.
Purpose: To create and evaluate performance of a SCORE function which contains HDL as an additional variable.
Methods: SCORE HDL was derived using Cox proportional hazards model, with age as time variable. Survival probabilities and beta coefficients for the variables included were combined to give the 10 year risk of CVD mortality using the original SCORE methodology. For comparison, a separate function without HDL was derived using the same methods and study population; SCORE C. The two functions were compared using observed to predicted ratios, sensitivity, specificity, net reclassification indices and area under receiver operated curve (AUROC) analysis.
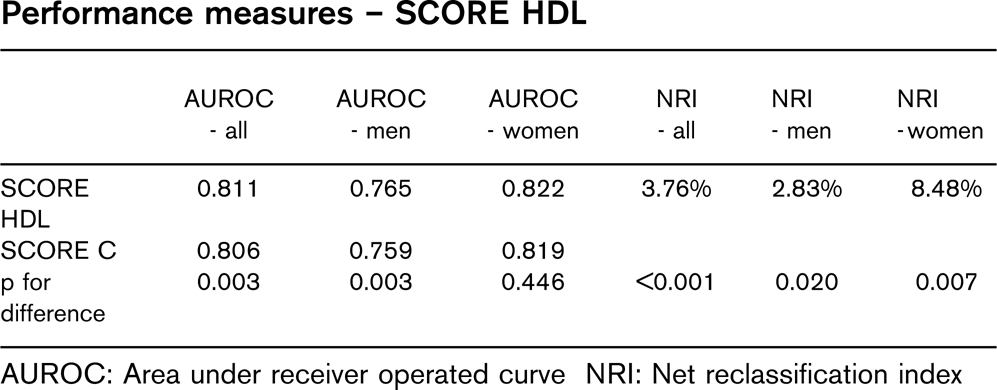
Results: SCORE charts at different HDL levels and an interactive SCORE HDL calculator were created. The table shows performance measures for the two functions.
Conclusion: Inclusion of HDL provided a small but significant improvement in risk estimation based on AUROC. However, inclusion of HDL resulted in a significant proportion of the population, especially women, being correctly reclassified to a different risk category, which is highly clinically relevant. Future work will focus on identifying particular subgroups for whom inclusion of HDL is particularly important.
Performance measures – SCORE HDL
AUROC - all
AUROC - men
AUROC - women
NRI - all
NRI - men
NRI - women
SCORE
0.811
0.765
0.822
3.76%
2.83%
8.48%
HDL
SCORE C
0.806
0.759
0.819
p for difference
0.003
0.003
0.446
>0.001
0.020
0.007
AUROC: Area under receiver operated curve NRI: Net reclassification index
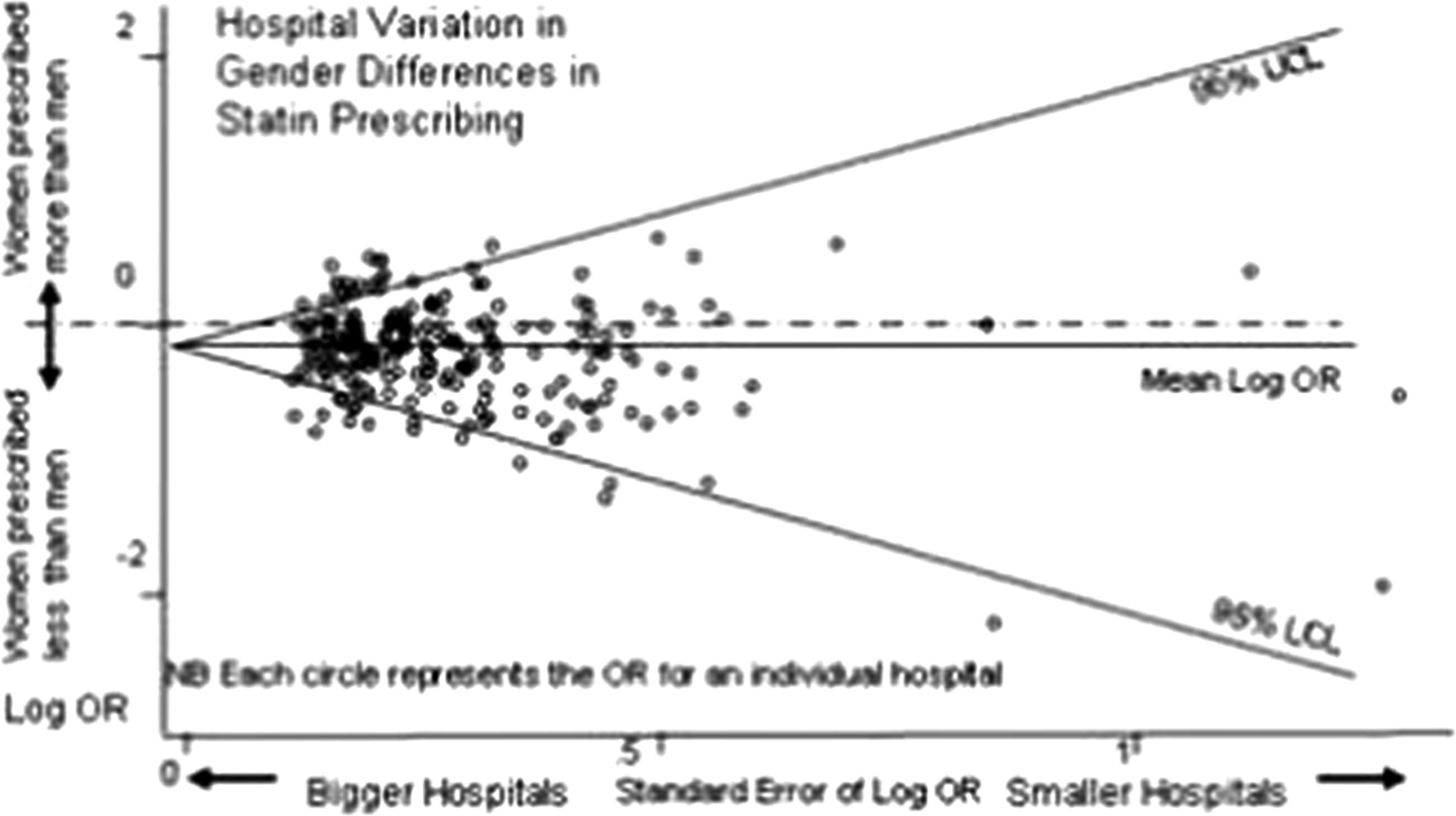
10 The prognostic significance of renal function and haemoglobin in 10,000 women and 11,000 men with incident stable angina
AD Shah; R Chen; H Hemingway
University College London Clinical Epidemiology Group, London, United Kingdom
Background: Previous studies of the prognostic impact of renal function and haemoglobin in stable angina are limited by small size (with too few women to assess gender differences) and focus on late stage disease only.
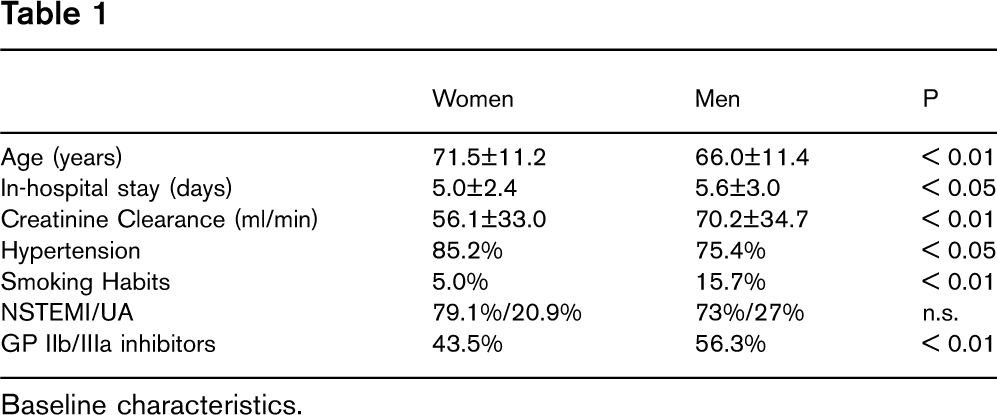
Purpose: To investigate gender differences in the prognostic significance of haemoglobin (Hb) and glomerular filtration rate (eGFR; estimated using the Cockcroft-Gault formula) in a large cohort of patients with incident stable angina pectoris.
Methods: 31,157 patients (45% women) with a new diagnosis of stable angina and no previous acute coronary syndrome were identified from 415 practices in the UK General Practice Research Database. Hb values were available in 79% of patients and creatinine off ACE inhibitors in 73%. The endpoint was non-fatal myocardial infarction or death from any cause, assessed at median 3.1 years follow up. Hazard ratios were adjusted for age, (eGFR), (Hb), smoking, diabetes, blood pressure, family history and total cholesterol.
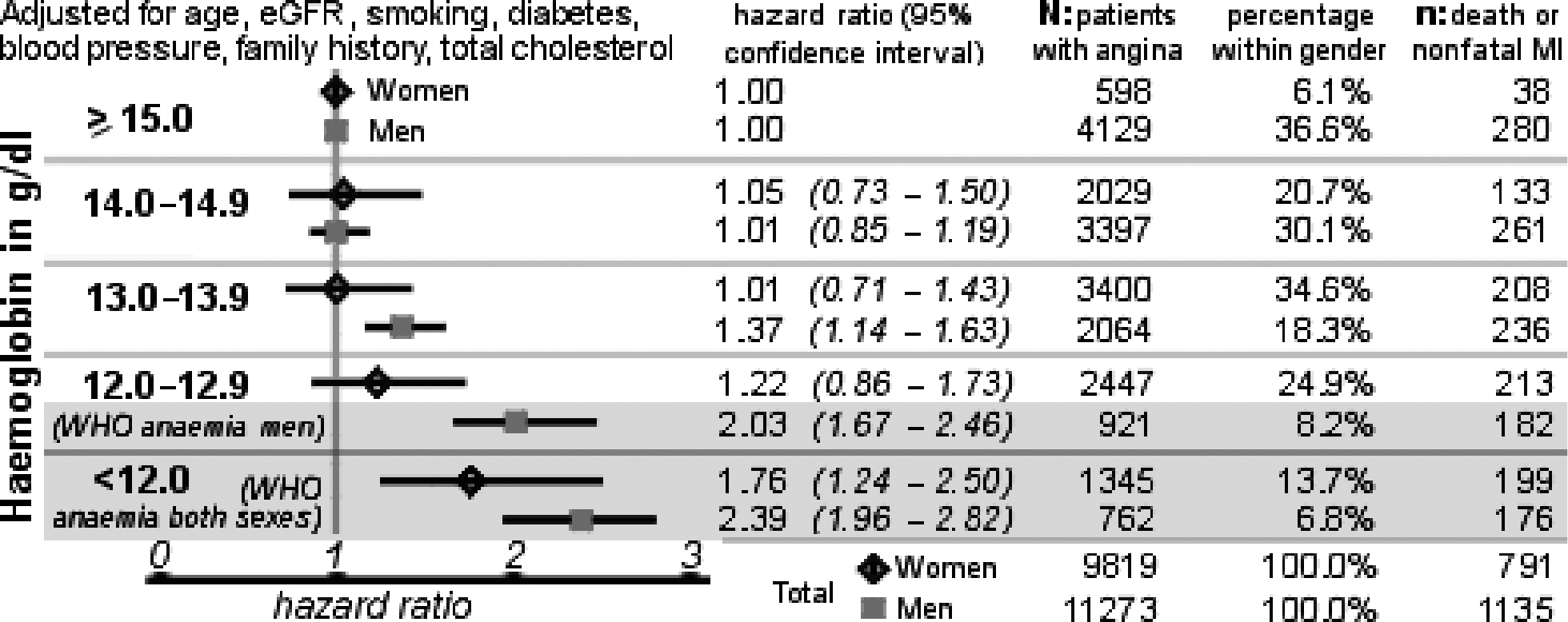
Results: There was no evidence that mild or moderate renal impairment increased risk; men with eGFR of 60–89 ml/min had slightly reduced risk (HR 0.76; 95% CI 0.60–0.97). The risk of events was increased only in the 2.2% of women and 1.6% of men with eGFR >30. By contrast for Hb, there was an inverse linear dose response effect particularly among men, with increased risk even among those with “normal” Hb values (>13 g/dl) (see figure). Among women, increased risk (HR 1.76) was confined to those with WHO defined anaemia (Hb <12 g/dl).
Conclusion: Independent of renal function, lower haemoglobin is associated with the prognosis of stable angina, which in men, but not women, extended into the normal range of values. These findings suggest sex-differences in the causal mechanisms for the transition from stable to acute coronary disease.
Hazard ratios for death or nonfatal MI
11 Dramatic change in demographic and clinical characteristics of patients undergoing inpatient cardiac rehabilitation in State Hospital for Cardiology
G Veress; I Berenyi; A Simon
State Hospital for Cardiology, Balatonfured, Hungary
The expanded therapeutic armory, more aggressive therapy for elderly patients, and changing demographics have significantly impacted the treatment and rehabilitation of coronary patients. This retrospective analysis looks at the changing patient population from January 1, 1999 to June 30, 2005 with regard to comobidities which may impact cardiovascular risk, in 49, 155 patients who participated in our institute's instutitional rehabilitative care. Temporal changes are indicated in 6 months periods.
Results: Patients' age (R=0.07, p>0.001, 0.39%/year), incidence of hypertension (R=0.98, p>0.001, 0.99%/year), and disorders of glucose regulation (R=0.96, p>0.001, 0.99%/year) increased. The incidence of angina pectoris (R=0.62, p>0.05, −0.28†/year) and the number of post-myocardial infarction patients (R=0.65, p>0.05, −0.64%/year) continuosly decreased. Conversely, the proportion of patients having percutaneous transluminal coronary angioplasty (R=0.98, p>0.001, 3.46%/year) or coronary artery bypass surgery (R=0.93, p>0.001, 2.16%/year) increased steeply.
The age of patients participating in phase II cardiac rehabilitation programs(18,515 patients) also increased (R=0.05, p>0.001, 0.36%/year), as did the proportion of women (R=0.75, p>0.01, 0.64%/year). There was a substantial increase in hypertension (R=0.95, p>0.001, 2.97%/year), and disorders of glucose regulation (R=0.61, p>0.001, 1.28%/year). The ratio of patients with angina (R=0.61, p>0.05, −0.35%/year) or myocardial infarction (R=0.90, p>0.001, −1.52%/year) decreassed. More patients had percutaneous transluminal coronary angioplasty (R=0.98, p>0.001, 5.78%/year increase) or coronary artery bypass surgery (R=0.85, p>0.001, 1.19%/year increase).
Conclusion: Dramatic temporal changes int he composition, comorbidities, and medical history of patients participating in cardiac rehabilitation programs mirror the great advances in Hungarian cardiology and underline new challenges for future cardiac rehabiltation teams.
12 Why have coronary heart disease mortality rates in Sweden halved between 1986 and 2002?
L Lena Bjorck1; A Rosengren1; K Bennett2; G Lappas3; S Capewell4
1Sahlgrenska Unversity Hospital/Ostra Department of Medicine, Goteborg, Sweden; 2Trinity Centre for Health Sciences, St James Department of Pharmacology and Therapeutics, Dublin, Ireland; 3Sahlgrenska University Hospital, Ostra Department of Medicine, Goteborg, Sweden; 4University of Liverpool Department of Public Health, Liverpool, United Kingdom
Purpose: Coronary heart disease (CHD) mortality rates have been decreasing in Sweden since the 1980s. We used the validated IMPACT CHD mortality model to examine how much of the decrease in Sweden between 1986 and 2002 can be attributed to medical and surgical treatments and how much to changes in cardiovascular risk factors.
Methods: The previously validated IMPACT mortality model was used to combine and analyse data on uptake and effectiveness of cardiological treatments and risk factor trends in Sweden. The main data sources were official statistics, national quality registers, published trials and meta-analyses, clinical audits and national population surveys. Sensitivity analyses were then conducted.
Results: Between 1986 and 2002, CHD mortality rates in Sweden decreased by 51.7% in men and 51.5% women 25 to 84 years old. This resulted in 12 345 fewer deaths in 2002. Some 38% of this decrease was attributed to treatments in individuals (including 12% to secondary prevention, 7% to heart failure treatments, 6% to initial treatments of acute myocardial infarction, and 4% to hypertension treatments) and 56% to population risk factor reductions (principally cholesterol, 38%; smoking, 10%; blood pressure, 7% and physical activity, 5%). Adverse trends were seen for diabetes, overweight and obesity.
Conclusion: More than half of the coronary heart disease mortality decrease in Sweden between 1986 and 2002 was attributable to reductions in major risk factors, principally a decrease in total serum cholesterol levels in the population along with reductions in smoking. These findings emphasize the value of a comprehensive strategy that promotes primary prevention such as tobacco control and a healthier diet plus physical activity. It also emphasizes the importance of effective evidence based medical treatments, especially secondary prevention.
13 Cardiovascular mortality trends in the old and new countries of the European Union
E Helis1; JG George Fodor2; P Zachar1; M Banic3; A Chockalingam4
1University of Ottawa Heart Institute Minto Prevention and Rehabilitation Centre, Ottawa, Canada; 2University of Ottawa Heart Institute Prevention And Rehabilitation Centre, Ottawa, Canada; 3Comenius University of Bratislava 2nd Department of Internal Medicine, Bratislava, Slovak Republic; 4Simon Fraser University Faculty of Health Sciences, Burnaby, Canada
Purpose: We are reviewing the mortality trends in the “new”, post-communist EU countries and compare them to the Western EU countries over a time frame of the past 35 years. We hypothesize about the possible determinants of the mortality differences.
Methods: Standardized mortality rates due to ischaemic heart disease (IHD) and cerebrovascular disease (CVD) were retrieved for 25 EU countries from the World Health Organization (WHO), European Health for All Database (HFA-DB). This information was reviewed for: i) Countries that entered the EU before 2004: Austria, Belgium, Denmark, Germany, Greece, Finland, France, Ireland, Italy, Luxemburg, Netherlands, Portugal, Spain, Sweden, United Kingdom and ii) Countries that entered the EU after 2004: Bulgaria, Czech Republic, Estonia, Hungary, Latvia, Lithuania, Poland, Romania, Slovakia, Slovenia. Data were retrieved for the time period from 1970 until most recently (after 2000).
Results: Mortality rates due to IHD and CVD in the “new” EU countries are approximately 2 times higher than in the “old” EU countries. The present large difference is not due to an increase of mortality in the Eastern countries but rather to a continuous, more rapid and accelerating reduction of mortality in the West since 1970.
Conclusion: The rapid decline of mortality in the Western countries is only partly due to decreased incidence rates and “lifestyle” changes. The prevalence of primary cardiovascular risk factors, with the exception of smoking, is not significantly different between Eastern and Western European countries. There is a higher use of invasive cardiac procedures as well as drug treatment in the West. The health expenditures in the West are significantly higher than in the “new” EU countries. Mental stress and life satisfaction play a more important role than it was formerly assumed in cardiac health and mortality outcomes.
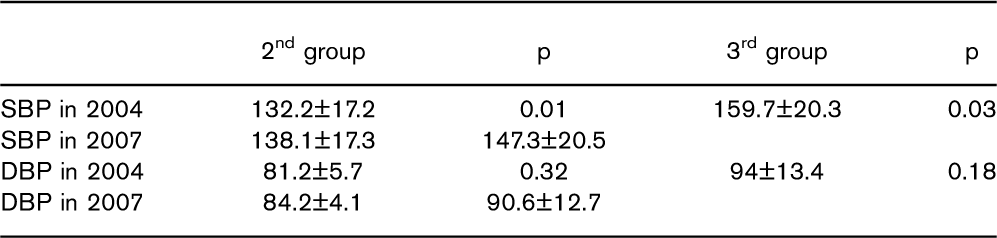
14 Weight gain contributes to the age-associated increase in blood pressure: the Doetinchem Cohort study
AMW Spijkerman; WMM Verschuren
National Institute of Public Health and the E Centre for Prevention and Health Services Res, Bilthoven, Netherlands
Purpose: To study the longitudinal association between the development over time of weight and BMI on the one hand and blood pressure levels on the other hand in the general Dutch population.
Methods: The Doetinchem Cohort Study is a longitudinal population-based cohort study. The study started in 1987 with the aim to investigate the impact of (changes in) lifestyle factors and biological risk factors on the incidence of CVD and other chronic diseases. A total of 7769 men and women aged 20–59 at baseline have been re-examined every five years. Data from the first three examinations are used. Weight, height, systolic and diastolic blood pressure (SBP and DBP) were measured at every examination. Blood pressure was measured twice and the mean of the two measurements was used in the analyses. Hypertension was defined as SBP=140 mmHg and/or DBP=90 mmHg and/or current use of antihypertensive medication. We used generalized estimating equations (GEE) to perform longitudinal linear regression analyses (proc GENMOD in SAS). Only people with complete data on weight, BMI and blood pressure for all three examination rounds were included (n=4637).
Results: The population consisted of 2211 men and 2426 women with a mean age at baseline of 40.2 (±9.9) yrs. The prevalence of hypertension at baseline was 17.0%. A total of 1210 normotensive individuals developed hypertension during follow-up. The mean change in weight between examination 1–2 and examination 2–3 was +2.4 (±3.0) kg, mean change in BMI +0.8 (±1.0) kg/m2, mean change in SBP +4.0 (±8.0) mmHg and mean change in DBP +2.1 (±5.5) mmHg. After adjustment for age, sex and use of antihypertensive medication, weight gain of 1 kg between two examinations was associated with a rise in SBP of 0.28 (0.25–0.31) and in DBP of 0.24 (0.22–0.26) mmHg (longitudinal linear regression coefficient (95% confidence interval)) and 1 unit (kg/m2) increase in BMI with 1.00 (0.91–1.09) mmHg SBP and 0.79 (0.73–0.85) mmHg DBP. The association between change in BMI and SBP and DBP was slightly stronger in men than in women: for SBP 1.04 (0.89–1.19) in men vs 0.94 (0.83–1.05) mmHg in women, for DBP 0.95 (0.84–1.05) in men vs 0.70 (0.62–0.77) mmHg in women.
Conclusion: About 20% of the observed increase in systolic blood pressure could be attributed to changes in BMI. Therefore, interventions aimed at weight loss or weight maintenance may also affect the development of elevated blood pressure in the general population.
15 Is the decline in coronary attack rates leveling off in Flanders?
C Vander Stichele1; D De Bacquer1; S De Henauw1; P Vannoote1; S Gevaert2; N Populier1; F De Boeck1; G De Backer1
1Ghent University Public Health, Ghent, Belgium; 2University Hospital Ghent, Ghent, Belgium
Purpose: To contribute to a better understanding of the dynamics of the epidemic of coronary heart disease.
Methods: From 1983 till 1992, the WHO has installed worldwide registers for acute coronary attacks in the framework of the MONICA project. In the population of the city of Ghent in Belgium, a decline was noted during that period both for fatal and non-fatal age-standardized attack rates. In 1999, a similar register was started in a more rural area of the country, in the region of Bruges. The two study populations consist of all inhabitants aged 25–74 years. The same criteria for defining cases-with different levels of certainty of diagnosis-were used as established by the MONICA project.
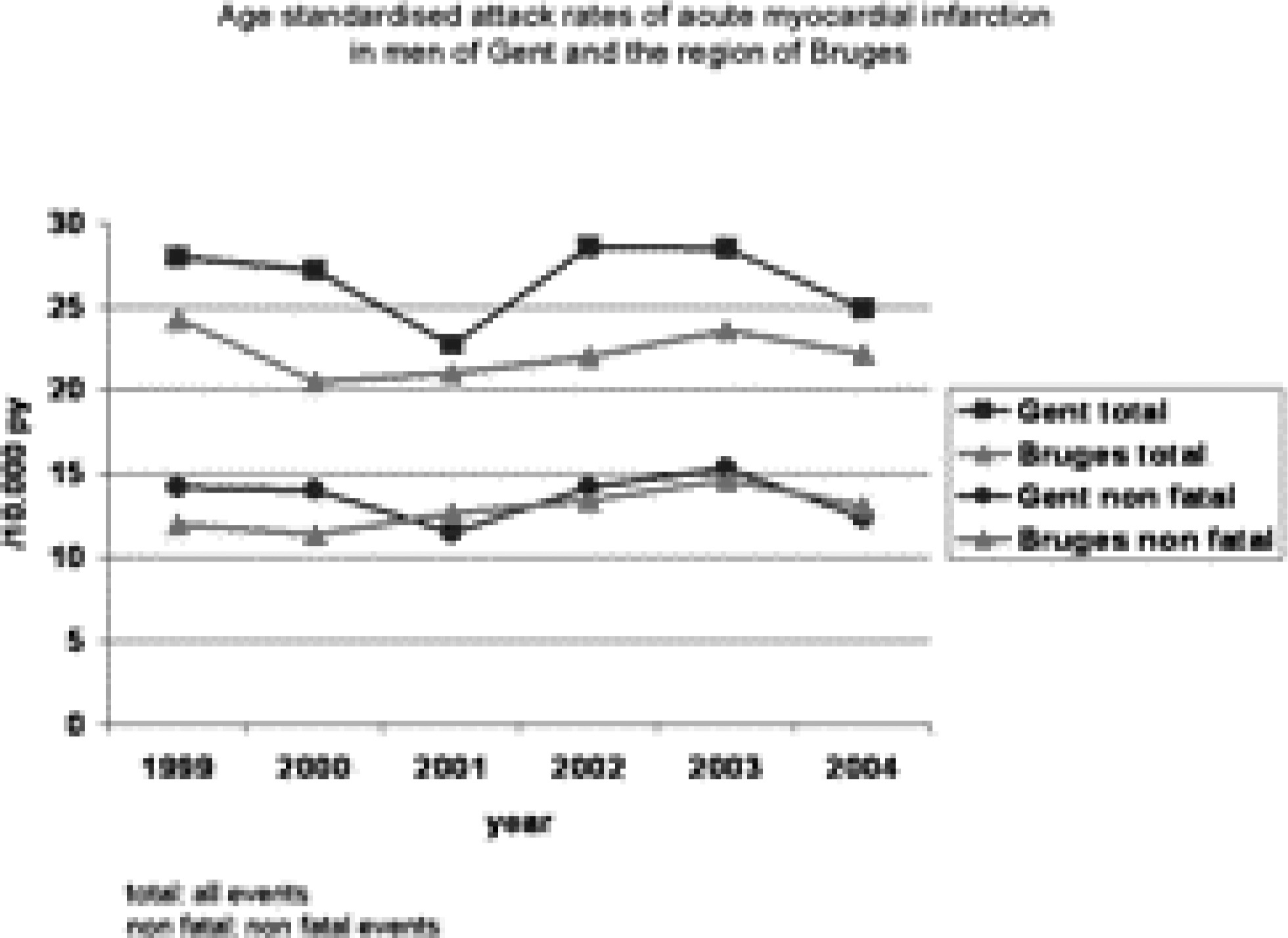
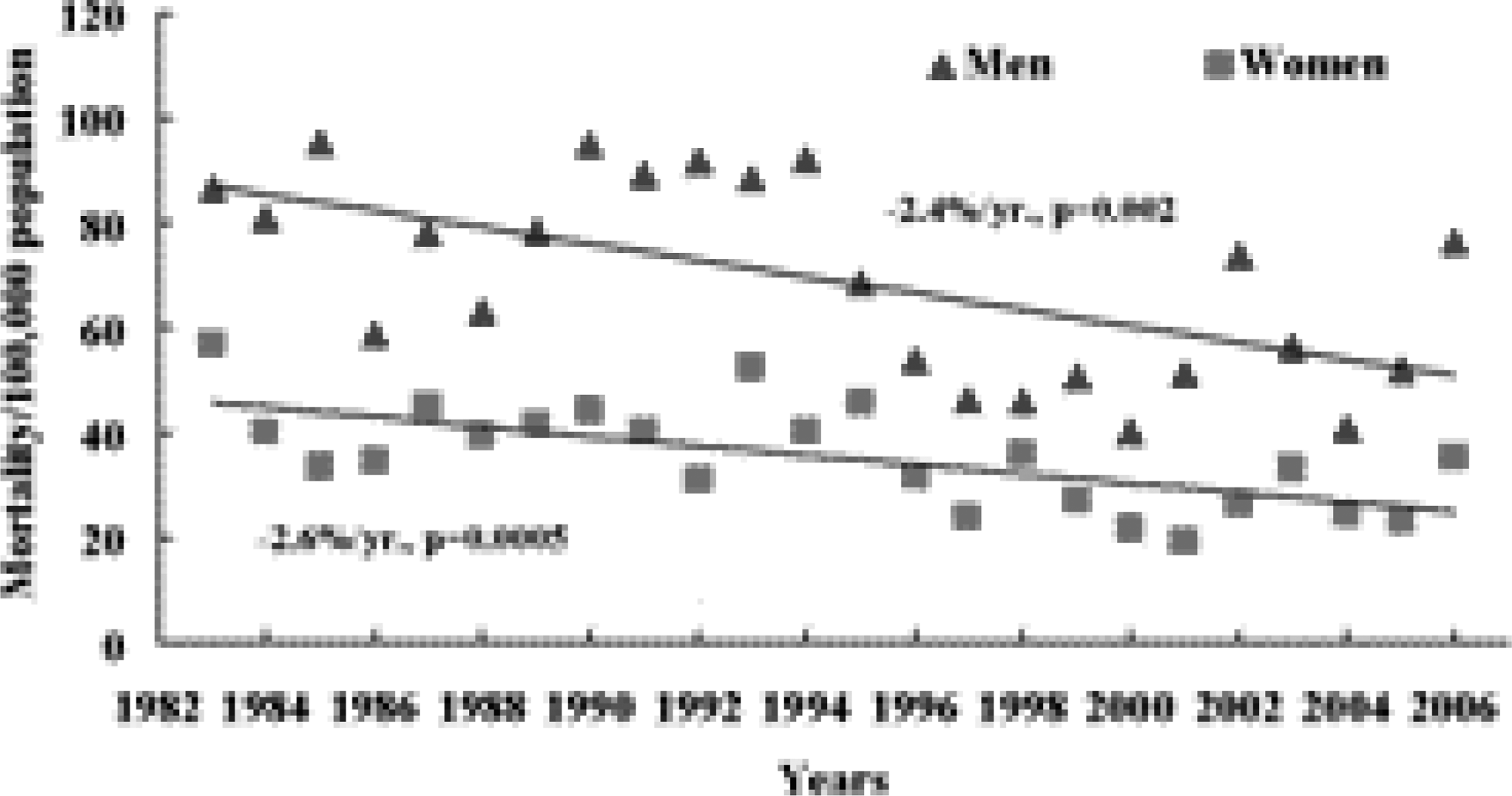
Results: The most recent data from 2003–2004 show an attack rate per annum of 27 per 10.000 personyears for men and of 9 per 10.000 personyears for women. The male/female ratio decreases from 4 to 2 with age. The 28-days-case fatality rate is still around 50%, with the highest percentages in the first hours following the start of clinical symptoms. Surprisingly, the results of 1999–2004 in both regions indicate that there is no longer a decrease of the age-standardized attack rates, both in the male and female population. In the figure the age-standardised attack rates are presented for all events and for non-fatal events in the male populations of the city of Ghent and of the region of Bruges.
Conclusion: Continuous monitoring of acute coronary events is indicated at the community level to describe precisely changes over time in event rates and in case fatality. The most recent trends in Flanders are challenging and need to be followed; if confirmed explanations should be searched in order to take action to reverse the unfavorable changes.
∗Monitoring of trends and determinants in cardiovascular disease
16 CHD death rates still decreasing in young adults in Sweden
J Berg; L Bjorck; K Dudas; A Rosengren
Sahlgrenska University Hospital/Ostra Medicine, Goteborg, Sweden
Purpose: Flattening mortality rates for coronary heart disease (CHD) among younger adults have been reported from the United Kingdom and from the USA, and has been attributed to increases in obesity and diabetes. The objective of our study was to examine recent trends in age-specific mortality rates from CHD and incidence of acute myocardial infarction (AMI) in Sweden, particularly those among younger adults.
Methods: We used individual-based mortality and hospital discharge data from 1987–2004 to calculate age-specific CHD mortality rates for Swedish adults aged 35 to 84 years. ICD-9 codes 410 to 414 were used for deaths occurring until 1996, and from 1997 and onwards ICD-10 codes I20 to I25. AMI was defined as first cases of 410 (ICD-9)/I21 (ICD-10) or CHD death.
Results: The crude decreases in CHD mortality over the 18-year period in men and women aged 35 to 44, 45 to 54, 55 to 64, 65 to 74, and 75 to 84 were −45%, −59%, −66%, −60%, and −49%. In women below 55 the decrease started later, but during the last half of the period, the decrease was as steep as for the men. AMI incidence among men decreased less, but again with no apparent flattening of trends, once changes in diagnostic methods after 2001 were taken into account. AMI incidence decreased among women aged 55 and over, but not among women below 55 years of age. There is, as yet, no apparent flattening in the decreasing trends in CHD mortality in any age group. Age-standardized CHD mortality rates in Sweden are still higher than in some Mediterranean countries like Italy or Spain but are on the same level as in Greece.
Conclusion: In Sweden, where overall obesity rates are still comparatively low, there is, at least until 2004, no apparent flattening in the decrease in CHD mortality rates in men or women, and Sweden can hardly any longer be described as a high risk country. More complex age-sex patterns are found for AMI incidence, with a decrease in younger men but not younger women.
17 Pace of change in coronary heart disease mortality in Finland, Ireland and the United Kingdom from 1985–2004
T O'hara1; K Bennett1; M O'flaherty2; S Jennings3
1Trinity Centre, St James's Hospital Department of Pharmacology and Therapeutics, Dublin 8, Ireland; 2University of Liverpool, L68 3GB Division of Public Health, Liverpool, United Kingdom; 3Health Services Executive Department of Public Health, Dublin 8, Ireland
Purpose: To examine the pace of change in coronary heart disease (CHD) mortality in Finland, Ireland and the United Kingdom from 1985 to 2004.
Methods: The percentage decrease in five-year average all age and under 65 year age standardised mortality rates from 1985–1989 to 2000–2004 was calculated for each country. Joinpoint regression analysis was used to analyse all age and under 65 year age standardised mortality rates to identify points (years) where the slope of the linear trend changed significantly. The pace of change in the CHD mortality rate was measured using annual percentage change (APC).
Results: The percentage decrease in five-year age standardised (under 65) CHD mortality rates was similar across all three countries and both genders except for Irish females, where the rate of change was greater (57.9%, 58.2% and 57.3% for males; 59.3%, 68.2% and 58.8% for females in Finland, Ireland and United Kingdom respectively). The percentage decrease in the all age rates was lower for Finnish males and females compared to their Irish and United Kingdom counterparts (40.3%, 46.5% and 47.1% for males; 33.6%, 44.2% and 45.3% for females in Finland, Ireland and United Kingdom respectively). There were different turning points in the downward trend in CHD mortality across the three countries varying from 1993 to 2002 (Figure). The annual percentage change (APC) in CHD mortality after the turning point was greatest for Irish males (all age (−7.3%) and under 65 year (−7.0%)) and Irish females (under 65 year (−10.6%)).
Conclusion: There were differences in the pace of change in CHD mortality among the three countries with turning points ranging from 1993 to 2002. Of the three countries, the pace of change was fastest in Ireland. The most likely explanations for the altered pace of change in CHD mortality are changes in CHD risk factors and treatments, implementation of cardiovascular health strategies, and economic changes. The combination of a favourable economic climate and strategic focus aimed at CHD risk factor reduction and access to treatments have the potential to influence pace of change in CHD mortality.
18 Heart rate as a marker of health state and cardiovascular risk in coronary patients - Outpatient based survey
J Bellwon1; A Wilkinson2; K Chlebus1; W Sobiczewski1; A Rynkiewicz1
1Medical University of Gdansk Ist Dept of Cardiology, Gdansk, Poland; 2Servier Polska, Warsaw, Poland
Objective: Heart rate values are associated with cardiovascular morbidity and mortality. Several questions regarding the clinical significance of a resting heart rate are still unanswered. The aim of our study was to evaluate weather heart rate reflects the quality of life and therapy in coronary patients.
Methods: An outpatient-based survey of 2253 coronary patients who visited primary care physicians (GP). There were 1247 men (55.3%) and 998 women (44.7%). Mean age was 65±10 years. Data on risk factors (age, gender, heart rate, blood pressure, BMI, waist circumference, lipids, glucose, renal function, smoking and family history), pharmacological and interventional therapy and angina episodes during the last month were obtained. All patients answered the EQ-5 questionnaire including EQ-VAS scale. EQ-VAS is a simple method of obtaining and scoring self-rating of current health status, the higher the VAS scores (0 to 100) the better the health state. The study was supported with unrestricted educational grant from Servier Poland.
Results: Angina episodes during the last month reported 2023 (89.9%) of patients. The mean number of angina episodes was 9±10 during the last month. The mean EQ-VAS was 56.7±16.6. The resting heart rate values did not correlate significantly the number of angina events per month r=0.04087 p=0.0572, but it inversely correlated significantly with EQ-VAS r=−0.12993 p>0.0001. Heart rate correlated with most of risk factors in univariant analysis. We have found significant positive correlation of resting heart rate with weight r=0.15162 p>.0001; body mass index r=0.16359 p>0.0001; waist circumference r=0.12038 p>0.0001; systolic blood pressure r=0.39566 p>0.0001; diastolic blood pressure r=0.40537 p>0.0001; total cholesterol r=0.25080 p>0.0001; LDL cholesterol r=0.15871 p>0.0001; fasting plasma glucose r=0.14485 p>0.0001 and significant inverse correlation with HDL cholesterol r=−0.05213 p>0.05.
Conclusion: Resting heart rate correlates significantly with EQ-VAS score as well as with a number of cardiovascular risk factors in coronary patients. Our results suggest that resting heart rate may be used as a very simple and easy to obtain marker of health state in ambulatory coronary patients.
19 Higher resting heart rate as an independent predictor of mortality in free living older adults the Three City Study
C Cohen1; P Ducimetiere1; JF Dartigues2; K Ritchie3; P Amouyel4; M Tafflet4; X Jouven4; C Tzourio5; JP Empana5
Aims: High resting heart rate (RHR), a simple marker of the autonomous system imbalance, has been consistently associated with higher mortality in middle-aged populations. This question has been addressed in the elderly in only a few studies of small sample sizes. We thus explored whether higher RHR was an indicator of higher mortality risk in a large population-based multicentre prospective cohort of older adults participants from the Three City Study.
Methods: The study population consisted of 7399 free-living older adults −2869 men and 4530 women- aged 65 years and more at time recruitment between 1999 and 2001, and who were free of permanent arrhythmias and pacemaker (n=1513). RHR was measured twice automatically (Dynamap) in a lying position after completion of the EKG at baseline examination. During the 6 years of follow-up, vital status was checked annually in the participant's family or GP. Causes of death were defined by an adjudication committee using any available information on the circumstances of death. In each gender, the hazard ratio (HR) for mortality according to RHR quintiles was estimated in a delayed entry time Cox proportional hazard model.
Results: Median RHR (min-max) was 67.5 bpm (34–120.5) in men and 71 bpm (38–132) in women respectively. As expected, the use of beta-blockers was inversely related to the level of RHR in both genders. After 6 years of follow-up, there were 642 deaths (8.7%), 350 in men (12.2%) and 292 (6.5%) in women; 256 (42%) were due to cancer, 169 to cardiovascular causes (27.7%) and 193 (31.6%) to other causes. The risk of mortality increased gradually across the quintiles of RHR in men (p for linear trend>0.001) but less evidently in women (p for linear trend=0.07). The HR (95% CI) of mortality for the fifth over the first quintile of RHR was 1.76 (1.27–2.43) in men and 1.51 (1.05–2.16) in women respectively after adjutment for the study centre. Subsequent adjustment for conventional risk factors modified marginally the HR point estimates, but associations in women became borderline significant (p=0.09). In men, the findings were not influenced by age, while in women, significant association was observed in the eldest only (above the median, 77 years). Moreover, comparable associations were found for mortality due to cancer and to other causes in both genders; although the same trend was found for cardiovascular mortality, it was not statistically significant.
Conclusion: In a free-living population of older adults, higher RHR was associated with higher mortality not restricted to cardiovascular causes.
20 Resting heart rate (RHR) and total mortality in the normal population: the Copenhagen city heart study
GB Jensen1; MT Jensen2; J Marott3
1Copenhagen University Hospital Hvidovre Cardiology Dept, Hvidovre, Denmark; 2Copenhagen University Hospital Cardiology, Hvidovre, Denmark; 3Copenhagen University Hospital Bispebjerg Copenhagen City Heart Study, Copenhagen, Denmark
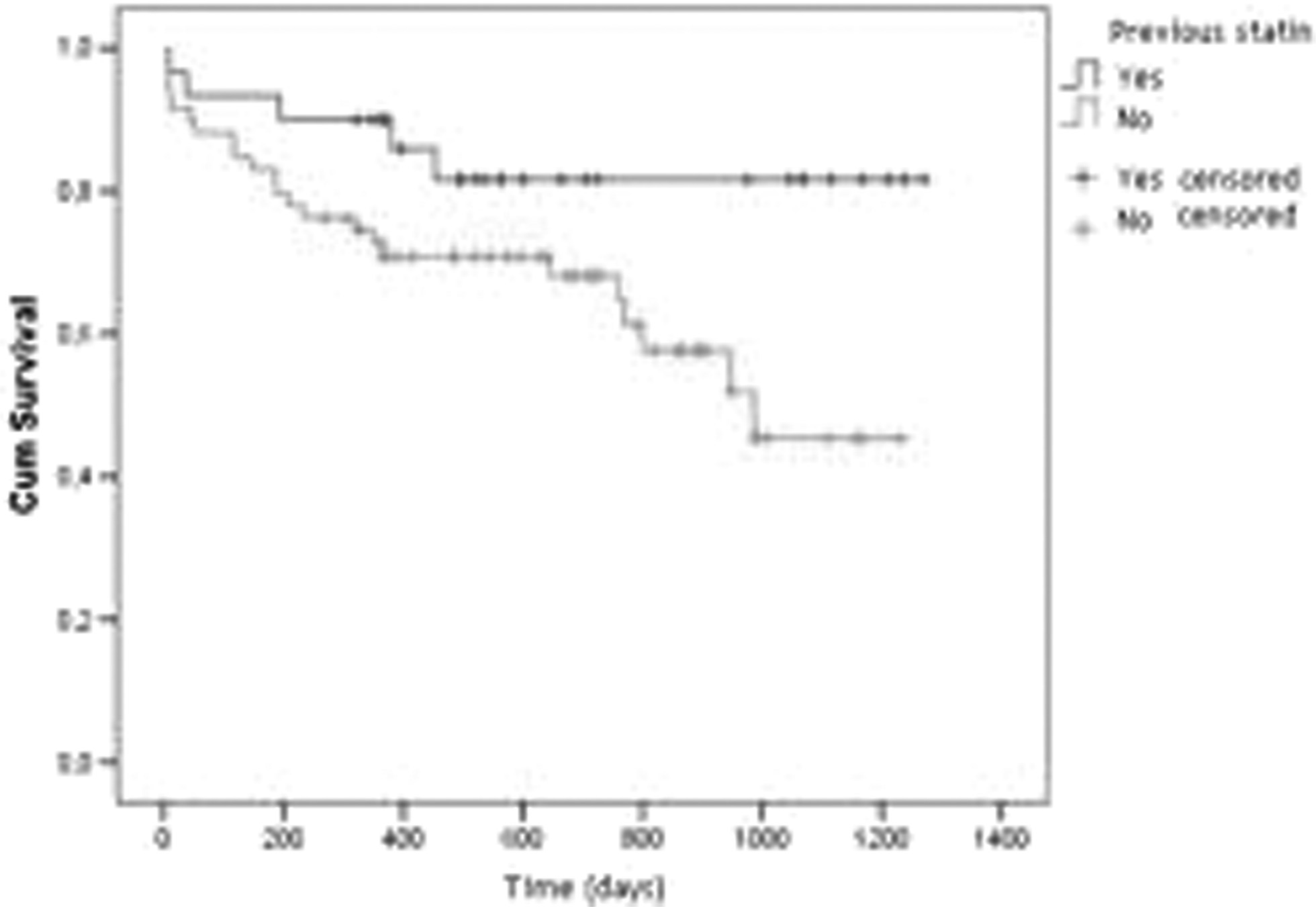
Background: Epidemiological and clinical studies have shown a positive association of RHR and all-cause mortality. RHR may be a proxy for underlying diseases or risk factors, but may also act independently, by promoting arterial stress and myocardial strain. The development of medicines acting directly on RHR by inhibiting the ion channel responsible for depolarisation of the sinus node has raised the possibility that RHR may be a target for primary prevention of mortality and morbidity.
Methods: The association between RHR and mortality was studied in the Copenhagen City Heart Study using Cox models. In 1976, 20,000 randomly selected men and women aged 20–90+ were invited to an examination including medical history, vital signs, blood samples, and 12-lead ECG from which RHR was determined. 74% responded. Follow-up (99.4%) was carried out by linkage to National Registers.
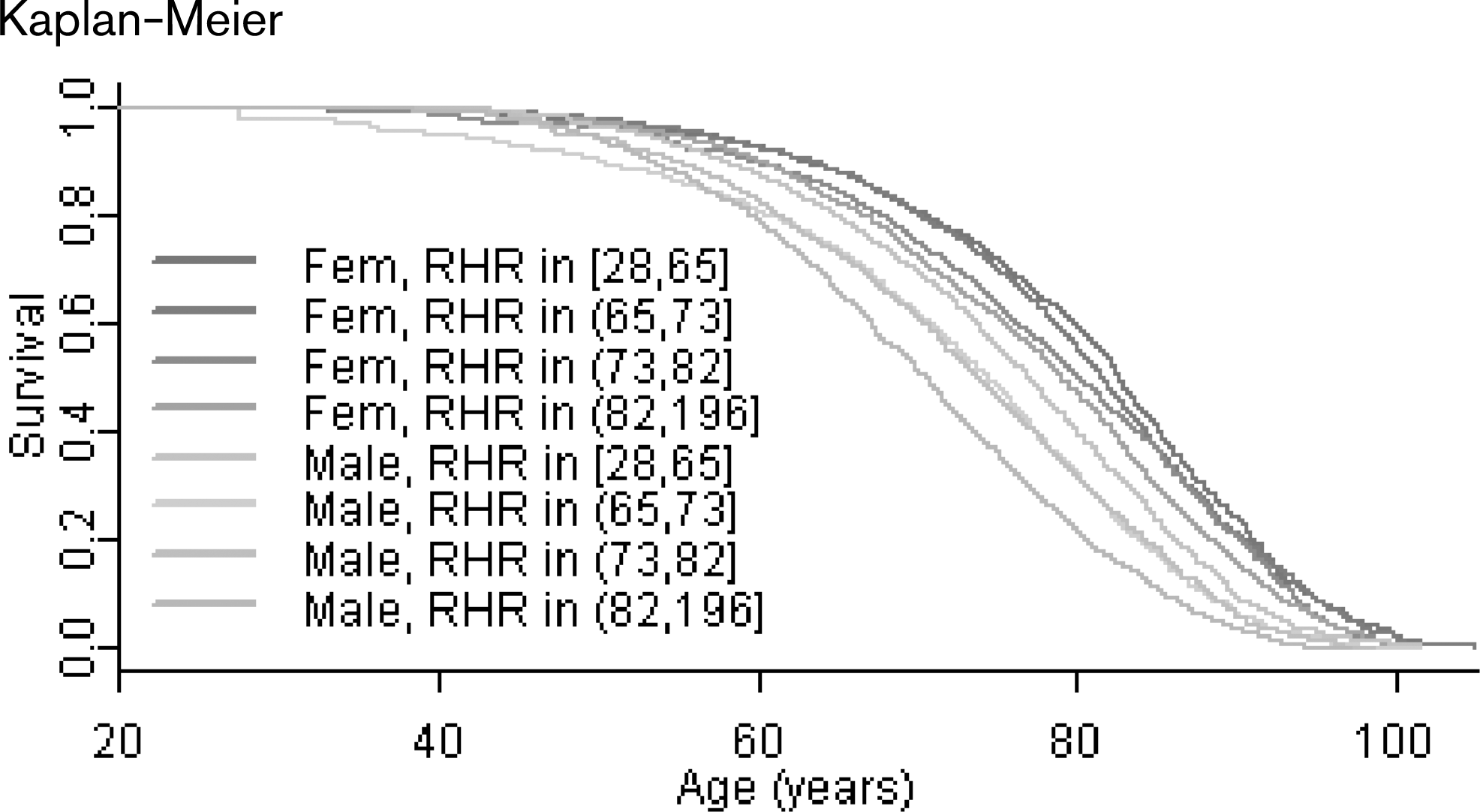
Results: 14,223 subjects participated in the study. Up to 2007, 9,094 deaths had occurred. The survival benefit in the lowest quartile compared to the quartile with highest RHR was about 6.5 years in males and 3.5 years in females (Fig 1). In a sex-stratified Cox model including RHR, physical activity, smoking, BMI, SBP, and triglycerides as exposure variables and which excluded 877 subjects with self-reported heart disease, stroke, diabetes, or ischemic ECG findings, RHR was an important risk factor for death. Increasing RHR with 1 BPM increased risk with 0.7% (CI 0.5–0.9, p>0.001). Removing deaths occurring within 5 years did not change the coefficients.
Conclusion: RHR is a highly significant independent predictor for death in the Copenhagen City Heart Study. The adjusted increase in risk for 1 BPM was 0.7%.
Perspective: RHR could potentially be a major focus for future preventive measures and pharmaceutical interventions.
Kaplan-Meier
21 Prognostic value of ambulatory heart rate revisited in 6928 subjects from 6 populations
TW Hansen1; L Lutgarde2; J Boggia3; L Yan4; M Kikuya5; K Bjorklund Bodegaard6; C Torp Pedersen7; H Ibsen1; JA Staessen5
1The Research Center for Prevention and Health, Copenhagen, Denmark; 2University of Leuven Studies Coordinating Centre, Division of Hype, Leuven, Belgium; 3Universidad de la Republica Departamento de Fisiopatologia, Hospital de C, Montevideo, Uruguay; 4University School of Medicine he Center for Epidemiological Studies and Cli, Shanghai, China, People's Republic of 5The Tohoku University Graduate School of Phar, Sendai, Japan; 6Uppsala University, Uppsala, Sweden; 7The Copenhagen University Hospital, Copenhagen, Denmark
Purpose: To investigate the multivariate-adjusted relation between mortality and cardiovascular outcomes in relation to 24-hour ambulatory heart rate.
Methods: We recorded 24-hour ambulatory heart rate in 6928 subjects (mean age 56.2 years; 46.5% women) enrolled in prospective population studies in Denmark, Belgium, Japan, Sweden, Uruguay, and China, and included in the International Database on Ambulatory blood pressure and Cardiovascular Outcome (IDACO). We excluded subjects on beta-blockers.
Results: Median follow-up was 9.6 years. In models including systolic ambulatory blood pres-sure and other risk factors, higher 24-hour heart rate was a predictor of total (n=850) and non-cardiovascular (n=493) mortality (P=0.003), but did not predict any of the cardiovascular outcomes (P=0.13). In similar models, higher nighttime heart rate predicted total, non-cardiovascular and cardiovascular (n=325) mortality (P=0.04). Furthermore, elevated night time heart rate predicted fatal and non-fatal cardiac events (n=439) (P=0.05), but not the combined cardiovascular outcome (n=805), coronary events (n=324), or stroke (n=363) (P=0.15). The daytime heart rate did not predict any of the outcomes (P=0.07). The results were consistent when we stratified according to gender, history of cardiovascular disease, or treatment with antihypertensive medication. However, there was a tendency that ambulatory heart rate was a better predictor in subjects younger than 60 years compared to the elderly part of the population.
Conclusion: In a general population, ambulatory heart rate was not a powerful predictor of cardiovascular outcomes. Only elevated nighttime heart rate was an independent predictor of cardiovascular mortality and cardiac events. With regard to mortality, the 24-hour and nighttime heart rate were positive related to total and non-cardiovascular death. Elevated heart rate during nighttime might be a sign of diminish sleep quality and could just be a marker of pre-existing or concurrent disease.
22 Control of cardiovascular risk factors: a secondary cardiovascular prevention and rehabilitation program
V Arrarte1; MD Sola1; M Garcia1; G Lopez1; I Lillo1; MA Lillo2; L Caballero1; C Lopez1; JM Climent1; F Sogorb1
1Hospital General Universitario de Alicante Cardiology, Alicante, Spain; 2Universidad de Alicante Inorganic Quemistry, Alicante, Spain
Purpose: Euroaction study states that in any hospital or in general practice a Secondary Prevention and Rehabilitation program could be carried out in order to improve control of cardiovascular risk factors in patients with coronary disease. During the present year, a program based on the principles that try to control the risk of ischaemic patients has been developed with the participation of a nurse and a physiotherapist.
Methods: Those patients with coronary disease which had been previously stabilised by medical or percutaneous treatment admitted to our service were closely monitored during 3 months. The monitoring consisted of eight informative sessions and an exercice program. Finally, during the medical consultation, the main cardiovascular risk factors (glycosylated hemoglobin levels, tabaquism, LDL, HDL, total cholesterol, triglycerides, Hypertension, exercice level, usual diet, weight, BMI and waist diametre) were again evaluated. A descriptive analysis of each of the risk factors (119 total patients) was performed, using as a reference the values for each parameter from Septembre 2007 European Prevention Guide.
Results: In our sample, 40% patients were hypertense and/or diabetic, 28% were smokers and 56% ex-smokers, exhisting a high level of sedentarism (72%). All patients were hypercholesterolemic and had, at least, two or three additional risk factors. After the three months of monitoring, 5% total weight loss was observed in 60% of the patients, motivated by the sustantial improvement in their diet and the exercice. Also, the number of patients who did not accomplish abdominal obesity criteria triplicated (from 9% to 27%) and the abdominal diameter was reduced in 95% of the patients. All these factors, together with the correct medication, improved total cholesterol, LDL, HDL and triglycerid levels (leading to prevention criteria changes from 28 to 76%, from 9 to 71%, from 67 to 86% and from 48 to 81%, respectively). Control of hypertense and diabetic patients was clearly improved, despite the fact that only 38% of diabetics could reach glycosylated hemoglobin levels below >6.55 mg/dl.
Conclusion: These results should encourage hospitals to pay attention to the prevention field since the cardiovascular risk in all patients has been decreased. We are sure that patients should be further in-centivated regarding diet, exercice and therapeutic learnt habits. We also consider that relatives participitacion is very important in this type of programs, since it is essential for patients motivation and leads the program to be accomplished.
23 Prevalence of traditional risk factors among patients with coronary heart disease
NK Dolidze1; G Chapidze1; S Kapanadze1; D Enquobahrie2; N Latsabidze1; M Williams2
1Emergency Cardiology Center Secondary Coronary Prevention, Tbilisi, Republic of Georgia; 2University of Washington, Seattle, United States of America
Background: It is well known that a substantial proportion of coronary events occurs in individuals without traditional risk factors. This claim implies that other factors play a significant role in coronary heart disease (CHD) and has led to considerable interest in nontraditional risk factors. The goal of the trial was to determine the prevalence of the 4 conventional risk factors (hypertension, diabetes, dyslipidemia, smoking) among patients with CHD.
Methods: The cross-sectional study was conducted among 367 patients (259 men, 108 women, mean age 58.1±7.8 years) visited the hospital during the months January through December 2006.
Results: Among patients with CHD 67.4% were hypertensive, 42.3% had diabetes, 76.7% had dyslipidemia, 70.3% were past or current smokers. It is noteworthy that at least 1 of the 4 conventional risk factors was present in 88.2% of men and 81.7% of women. The minority of patients with CHD lacked any of the 4 traditional risk factors. The majority of patients (41.2%) had multivessel disease. Left anterior descending artery was the most common coronary artery involved. Myocardial revascularization procedures – coronary artery bypass operation and percutaneous coronary intervention were used to manage most of the patients (71%), whereas conservative therapy was administered to 29%.
Conclusion: The 4 classical risk factors such as hypertension, diabetes, dyslipidemia and smoking were prevalent among patients with CHD. Although researches on nontraditional risk factors are very important, clinical cardiology and research efforts should place significant emphasis on the 4 traditional risk factors in reducing of first-ever or recurrent coronary events and generally, the epidemic of CHD.
24 Patients ruled out for acute coronary syndrome. Are they still at risk for future events?
K Martiadou, I Kanonidis, G Dadoush, M Papadimitriou, C Kagiadaki, GK Sakantamis1
Aristotle University of Thessaloniki. Hippokr 2nd University Department of Cardiology & CCU, Thessaloniki, Greece
Purpose: The study aims to evaluate the risk for subsequent coronary events in patients who presented typical clinical picture and were ruled out for acute coronary events.
Methods: The study included 57 patients who were admitted to the CCU of our department for acute coronary syndrome. No one of them had a history of previous coronary artery disease (CAD). Admission was made on clinical and ECG criteria which included (1) Typical anginal chest pain (2) Non specific ST and T-wave changes.
Immediate post admission evaluation showed good clinical evolution with relapse of clinical symptoms (pain) and no cardiac enzyme elevation (CPK-MB – Troponin).
Exercise ECG and SPECT study performed during the first week post admission were negative without signs of ischemia.
Patients were evaluated (post hoc) for classical risk factors including hypertension, smoking, diabetes mellitus and hyperlipidemia and were categorized according to the probability for future coronary events (Framingham Score) in three groups as follows:
Group A: High risk patients (patients having a ten year probability for events=20%).
Group B: Moderately High risk (patients having a ten year probability for events between 5% and 20%).
Group C: Low risk patients (patients having a ten year probability for events Additionally newer risk factors were also evaluated including C-Reactive protein (CRP), Erythrocyte sedimentation rate (ESR), Homocystein and Fibrinogen. Patients were treated according to the risk factors they presented plus aspirin 100 mg per os daily and were followed for subsequent coronary events in the 12 month post admission period.
Results: Of the 57 patients included in the study 21 belonged to Group A (high risk), 24 to Group B (moderately high risk) and 12 to Group C (low risk). During the 12 month post admission period 7 patients developed coronary events (5 STEMI and 2 NON STEMI). Of those 5 belonged to the high risk Group A and 2 to moderately high risk Group B. Of the newer factors CRP was the most valuable predicted factor. Six (6) out of seven (7) patients had a CRP higher than 5 mg/L.
Conclusion: Patients presenting with symptoms of acute coronary syndrome and are finally ruled out, still represent a group of relatively high risk for subsequent events. Risk score evaluation and CRP values are the most sensitive predictive factors for immediate events and must be evaluated to all members of this population.
25 Prevalence of cardiovascular risk factors on patients with aortic valve replacement included in comprehensive rehabilitation program
M Rada1; DE Velimirovici1; D Berceanu Vaduva1; S Dragan1; D Gaita1; A Schnabel1; G Mancas1; I Gogoasa2; S Mancas2
1Univ. of Medicine & Pharmacy Victor Babes Cardiac Rehabiltation Clinic, Timisoara, Romania; 2Univ. of Agricultural Sciences of Banat, Timisoara, Romania
Objective: To establish the influence of cardiovascular rehabilitation program on cardiovascular risk factors prevalence in patients with aortic valve replacement depending on the etiology of aortic valvulopathy.
Materials and methods: 76 patients with aortic valve replacement for aortic valvulopathy of diverse etiologies where included in the study. The evaluated cardiovascular risk factors at the study admission time and 6 month after surgery were as follows: BP=140/90 mmHg, BMI=30 kg/m2, TC=200 mg/dl, type 2 diabetes mellitus, smoking and ex-smoking state. Patients were recomanded to respect secondary prevention measures, including exercise programs or regular daily physical activity depending on the limits of individual effort tolerance and on the results at the effort test, with an accent to walking sessions. Statistical analysis: average±standard deviation, % lot, student t test.
Results: In the studied lot we remark the prevalence of degenerative etiology (61.84%) and secondly the reumatismal etiology of the aortic valvulopathy. 63.15% of patients were man. We remark a higher prevalence of the three traditional major risk factors (hypertension, hypercholesterolemia and smoking condition), especialy in aortic degenerative lesions. The benefit of secondary prevention measures on dinamics of cardiovascular risk factors evolution, quantified after 6 months from study admission, indicate a poor improvement of hypertension and obesity prevalence compared to early post surgery values, on the other han hand prevalence of hypercholesterolemia decreased from 28.94% to 18.30% (p>0.005), and the prevalence of smoker condition from 32.89% to 21.12% (p>0.005).
Conclusion: There is an evidence of higher prevalence for the three traditional major risk factors, especially for aortic valvular patients with degenerative lesions. This study demonstarte the major benefit of cardiovascular reabilitation programes and especially of secondary prevention measures on cardiovascular risk factor prevalence, first in rank for hypercholesterolemia and smoking status 6 months after randomisation, improving the cardiovascular risk score in patients with aortic valvulopathy.
26 Cardiovascular risk factors in young and elderly patients with acute coronary syndrome: a comparative study
F Kontari; TH Livieratos; AR Tziovas; PAN Koustas; GE Fagogenis; GE Kordosis
General Hospital of Agrinio Cardiology, Agrinio, Greece
Arteriosclerosis is the leading cause of cardiovascular morbidity and mortality around the world.
Purpose: To determine the presence of conventional cardiovascular risk factors in young patients with acute coronary syndrome and compare with those in elderly patients in order to achieve optimal planning of prevention.
Methods: The study included 446 patients aged 26–92 years admitted to a cardiologic clinic of a regional Greek hospital with acute coronary syndrome in a two-years study period from January 2005 to December 2006. Patients were classified according to their age in three groups: group A: 61 patients aged =45 years, group B: 183 patients aged 46–65 years and group C: 202 patients aged =66 years. We evaluated the prevalence of risk factors (smoking, dyslipidemia, hypertension, diabetes mellitus, family history of premature coronary disease) and compared three groups with each other.
Results: Out of all patients 72.5% were male. Prevalence of each cardiovascular risk factor in three groups A, B and C was as follows: Smoking 77%, 45.9%, 34.2%. Dyslipidemia 44.3%, 67.2%, 70.8%. Hypertension 6.5%, 68.3%, 88.6%. Diabetes mellitus 3.2%, 24.6%, 35.2%. In addition, 60% of group A had a family history of premature coronary disease. The prevalence of smoking decreased in the oldest group where as dyslipidemia, hypertension and diabetes mellitus increased in both B and C groups.
Conclusion: Our findings suggest that smoking and family history of premature coronary disease were the commonest risk factors in younger patients with acute coronary syndrome. Hypertension, dyslipidemia and diabetes mellitus were the commonest risk factors in elderly patients. As coronary heart disease(CHD) is one of the leading health threats worldwide it is fully justified to invest all efforts to prevention and to improve awareness of the CHD risks and morbidity in the population at large.
27 Awareness, treatment, and control of traditional CV risk factors in a founder population: the SardiNIA Study
A Scuteri1; M Orru'2; SS Najjar3; G Albai1; J Strait2; K Tarassov2; MG Piras1; M Uda1; A Cao1; EG Lakatta2
1UO Geriatria - INRCA, Roma, Italy; 2INN - CNR, Cagliari, Italy; 3Lab CV Sciences - NIA - NIH, Baltimore, United States of America
Although mortality from CV disease is declining, CV mortality and morbidity remain alarmingly high. This may recognize low control of traditional CV risk factor levels in the population. We investigated the effect of gender and age on the population burden of CV risk.
Methods: The SardiNIA Study was conceived as a study of a Sardinian founder population investigating the genetics of complex traits/phenotypes, including CV risk factors and arterial properties Over a 3 yrs period, 6,148 subjects were enrolled, comprising over 60% of those aged 14–102 in a cluster of 4 towns. Hypertension (HT) was defined as an average BP 140/90 mmHg or use of antiHT drugs. HT was considered treated if subjects reported use of antiHT drugs and controlled if BP was 65 years had their BP=140/90 mmHg, though 48.5% received treatment for HT. The rate of control of DM was similar across age groups, regarding approximately two thirds of the affected population. The use of lipid-lowering therapy was still very low, interesting less than one third of the subjects expecting a benefit from the treatment in subjects>65 years, the group with the highest treatment rate.
Conclusion: The present study also extended to a large Italian population of broad age range previous observation that a large number of subjects are not treated or are undertreated. This phenomenon is particularly striking for older subjects and it may reflect persistence of the (wrong) paradigm that at older age traditional CV risk factor are no longer significant determinants of CV events and that prevention is not effective at older ages.
28 Family history of cardiovascular disease risk factors: a population-based study in Switzerland
GO Wandeler1; A Chiolero1; FM Paccaud1; P Vollenweider2; G Waeber1; V Mooser3; D Hayoz1; A Pecoud4; M Murielle Bochud3
1Institute of Social and Preventive Medicine, Lausanne, Switzerland; 2CHUV Medicine, Lausanne, Switzerland; 3GlaxoSmithKline Medical Genetics, Philadelphia, United States of America; 4University of Lausanne Medical Outpatient Clinic, Lausanne, Switzerland
Purpose: There is limited quantitative information on the relationship between family history and the corresponding underlying trait. A better knowledge of the relationships between cardiovascular disease (CVD) risk factors and related family history may help assessment of CVD risk. We analyzed the association between blood pressure, fasting blood glucose and cholesterol levels and the corresponding family history.
Methods: Data were obtained from a population-based sample of 6102 participants (2903 men and 3199 women) aged 35–75 years from Lausanne (Switzerland). CVD risk factors were measured and CVD family history was self-reported, using a structured questionnaire.
Results: Among participants, 16.5%, 23.9% and 12.9% had a positive paternal, maternal and sibling history of hypertension, 9.0%, 10.5% and 6.5% of diabetes, and 13.9%, 12.7% and 10.0% of hypercholesterolemia, respectively. We observed that the paternal, maternal and sibling history was not known by 30.4%, 19.1% and 16.5% of the participants for hypertension, 8.7%, 4.5% and 5.7% for diabetes and 38.2%, 29.6% and 22.0% for hypercholesterolemia, respectively. For each CVD risk factor, a positive family history was strongly associated with higher levels of the corresponding trait (P>0.05), but not with the other traits. Mean adjusted systolic blood pressure, fasting glucose and cholesterol levels linearly increased with an increasing number of first-degree relatives with a positive history of hypertension (from 124.7±0.4 to 131.7 ± 1.3 mmHg for 0 to 3 relatives), diabetes (from 5.47±0.02 to 6.92 ±0.2111 mmol/L for 0 to 3 relatives) or hypercholesterolemia (from 5.53 ±0.02 to 6.01±0.1222 mmol/L for 0 to 3 relatives), respectively. Compared to participants with a negative family history of hypertension, those not knowing their family history had higher systolic blood pressure (127.1±15.0 vs 128.8±16.0 mmHg for the father, 127.0±14.9 vs 129.1 ±16.2 mmHg for the mother, and 127.3±14.7 vs 129.2±16.6mmHg for siblings, P>0.05). Analyses restricted to subjects who were unaware of their disease status (hypertension, diabetes or hypercholesterolemia) led to similar, although less strong, associations.
Conclusion: Family history of hypertension, diabetes and hypercholesterolemia was strongly associated with the corresponding trait. Many participants did not know their family history of hypertension and hypercholesterolemia. Not knowing family history of hypertension was associated with higher blood pressure. Family history is a powerful, specific and inexpensive screening tool to detect subjects at increased cardiovascular risk.
29 Gender differences in the implementation of secondary prevention after an acute coronary event: the EUROASPIRE Study
J Dallongeville1; D De Bacquer2; J Heidrisch3; G Debacker1; M Montaye2; P Amouyel1
1Lille, France; 2Gent, Belgium; 3Munster, Germany
Aim: Although ischemic heart disease rates are lower in women than in men until advanced age, the mortality rate after an acute coronary event is clearly higher in women than in men - especially at younger ages. Some of this gender-related difference has been attributed to worse cardiovascular risk factor profile and /or inadequate implementation of secondary prevention. The EUROASPIRE III survey provides an excellent platform to study these gender differences in depth. The goal of the present study was to compare the cardiovascular risk profile and disease management of men and women at least 6 months after an acute coronary event.
Method: Data from a representative sample of patients having experienced a recent coronary event before the age of 80 years were gathered in the period 2006–2007 through standardized methods from 22 European centers participating in the EUROASPIRE III study. A total of 8966 coronary patients (25.3% of women, range 11.5% to 35.7% between centers) were included in the analyses.
Results: Compared to men, women were slightly older (mean age 65.8y vs. 62.2y), had a lower level of education, and were more often included in the survey for ischemia and myocardial infarction (MI virtually no difference 19% vs. 20.6%) less often for CABG and PTCA. There was, in contrast, no difference in medical caregivers between men and women. The prevalence of current smoking was higher in men than women (19.3% vs. 11.0%). The prevalence of obesity (44.7% vs. 32.1%) was higher in women than in men. Self reported diabetes was more frequent in women than in men (30.4% vs. 22.6%), and less diabetic women than men were controlled with respect to HbA1c>777 mmol/l (and 6.555 mmol/l) (39.9% vs. 53.9%). The prevalence of hypertension (54.5% vs. 49.0%) was higher in women than in men at all age ranges. The rates of anti-hypertension treatment were similar in men and women, however, fewer women were reaching blood pressure targets than men, independently of age. Similarly, LDL-cholesterol levels and the prevalence of subjects with LDL-cholesterol levels = 333 mmol/L were higher in women than in men despite similar rates of prescription of lipid lowering agent.
Conclusion: The results of the present study show gender-specific differences in prevalences of cardiovascular risk factors after an acute coronary event. Despite similarities in pharmacological treatment, women reach less often the therapeutic goals of BP and LDL-cholesterol and HbA1c among diabetic patients. These results suggest that women and men may not benefit equally from the same care after an acute coronary event.
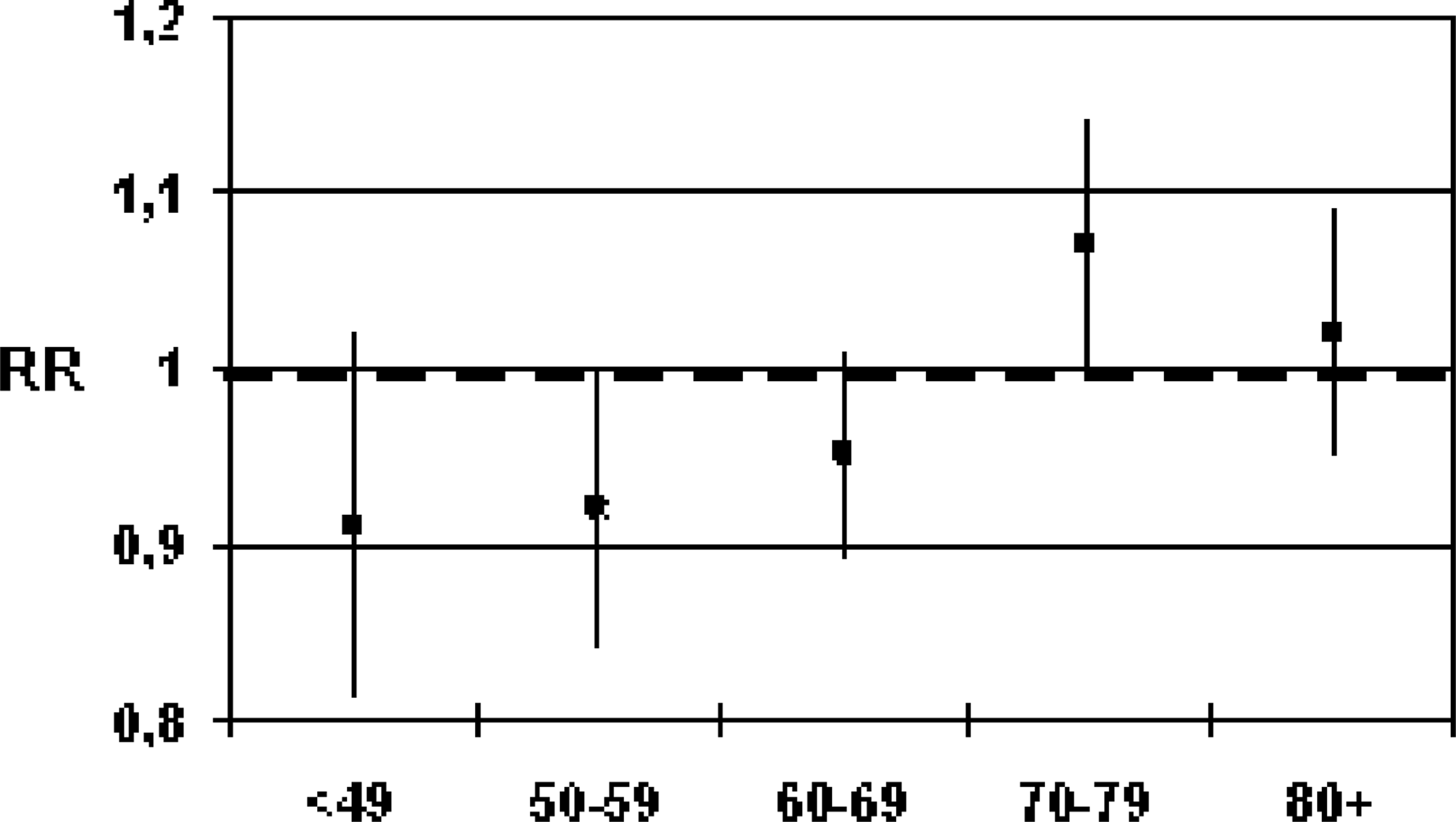
30 (WITHDRAWN) Short- and long-term case fatality in 15 873 patients hospitalized with a first acute myocardial infarction, 1972–2001 the Western Norway Cardiovascular Disease Register
J Langoergen1; J Igland2; SE Vollset2; M Averina3; JE Nordrehaug1; GS Tell3; LM Irgens4; OK Nygaard1
1Haukeland University Hospital Dep. of Heart Disease, Bergen, Norway; 2University of Bergen The Western Norway Cardiovascular Disease Reg, Bergen, Norway; 3University hospital of Northern Norway, Tromsoe, Norway; 4Norwegian Institute of Public Health The Medical Birth Registry, Bergen, Norway
Purpose: To analyse trends over three decades in short- and long-term case fatality after hospitalization for a first episode of acute myocardial infarction (AMI).
Methods: The Western Norway Cardiovascular Disease Register has recorded data collected from Haukeland University Hospital in Norway during 1972 to 2001. The data were linked with the National Causes of Death Registry to obtain information about causes of death and date of death. Case fatality trends were examined using logistic regression.
Results: A total of 10 389 men and 5 484 women with a first AMI were identified. From the first (1972–81) to the last (1992–2001) decade, mean age increased significantly from 66.8 to 69.4 years. In the same period, crude 28-day case fatality declined from 34.9 % to 20.9 % in men and from 43.6 % to 27.7 % in women, whereas crude 10-year case fatality declined from 72.6 % to 56.4 % in men and from 82.7 % to 68.7 % in women (all p-trend >0.0001). After adjustment for age and decade, overall 28-day, 1-year and 10 year case fatality comparing the last with the first decade were 0.41 (0.38–0.45), 0.39 (0.36–0.42) and 0.34 (0.31–0.39), respectively. 10-year case fatality was significantly lower in women than in men (OR=0.88; 95 % CI 0.80–0.97). When stratifying the population in two age groups (>and<60 years), the difference between women and men was only significant in patients aged>60 years (OR=0,80; 95 % CI 0,72–0,89) and not in patients aged >60 years (OR=1,05; 95 % CI 0,85–1,29).
Conclusion: Before the introduction of new biomarkers in the diagnostic criteria of AMI, short- and long-term prognosis after hospitalization for a first AMI have improved substantially during the last 30 years in both sexes. In elderly patients, long-term case fatality is significantly lower in women than men.
31 Agreement between self-reported cardiovascular diagnoses and medical records in patients with coronary heart disease
C Prugger; J Wellmann; H Birke; R Dittrich; U Keil; J Heidrich
University of Muenster Epidemiology and Social Medicine, Muenster, Germany
Purpose: Self-reported diagnosis may be an important source of information and reflects patients' awareness and knowledge of a disease. The present study investigates agreement between self-reported cardiovascular diagnoses and medical records in a sample of patients with coronary heart disease (CHD).
Methods: The EUROASPIRE III study in the region of Muenster, Germany, was conducted among patients aged 18 to 79 years with established CHD. Patients were interviewed and examined at least six months after their cardiac event. The interview contained a detailed section on pre-existing cardiovascular conditions such as myocardial infarction (MI), coronary revascularization (PTCA and CABG), angina, stroke, transient ischemic attack (TIA) and peripheral artery disease (PAD). Interview data were compared to medical records using kappa statistics.
Results: Overall, 551 patients participated in the study. Mean age was 63.3 (+/−9.1) years and 21% of the study population were female. Agreement between self-reported diagnosis and medical records was highest for CABG (kappa 0.92, 95% confidence interval (CI) 0.88–0.97) and stroke (kappa 0.85, 95% CI 0.73–0.98). Agreement for MI (kappa 0.67, 95% CI 0.59–0.74), PTCA (kappa 0.69, 95% CI 0.62–0.75) and PAD (kappa 0.67, 95% CI 0.56–0.79) was less pronounced. Agreement was poor for angina (kappa 0.22, 95% CI 0.13–0.32) and very poor for TIA (kappa −0.01; 95% CI-0.01–0.00). We did not observe substantial differences between age groups. For most diagnoses, agreement was lower in women compared to men.
Conclusion: Major diagnoses such as CABG or stroke showed good agreement between self-reports and medical records. Diagnoses with more ambiguous symptoms such as angina or TIA showed only poor agreement. This may be due to both, lacking self-report and inadequate medical documentation. However, awareness and documentation of these diagnoses are of utmost importance since they are often precursors of a major event and offer an opportunity to prevent disease progression.
32 Gender dependent trends in coronary event and mortality rates in French registers in the period 1997–2003
D Arveiler1; A Wagner1; M Montaye2; A Bingham3; JB Ruidavets4; B Haas1; P Amouyel3; J Ferrieres2; P Ducimetiere4
1Epidemiology Dpt-EA1801, L Pasteur University Department of Epidemiology and Public Health, Strasbourg, France; 2INSERM, U744, Pasteur Institute of Lille, Lille, France; 3INSERM, U780, Paris-Sud University, Villejuif, France; 4INSERM, U558, Paul Sabatier-Purpan University, Toulouse, France
Purpose: Whereas consistent downward trends in both myocardial infarction (MI) and coronary mortality rates were observed in the WHO MONICA Project from 1985 to 1994 in France as in other western countries, little information is available concerning more recent years. A possible levelling off is currently hypothesized.
Methods: Since 1997, Lille, Strasbourg and Toulouse MONICA registers have carried on recording MI episodes, coronary deaths, and deaths with insufficient data according to the WHO original protocol, except for non fatal MI, now recorded from hospital discharge files. A two-week annual concordance with MONICA MI diagnosis did not show any appreciable change during the period 1997–2003 for which complete validated data are presently available.
Over 7 years, 12601 total events (age 35–64), among which 5278 deaths, were identified in the three regions. Gender- and age-specific population numbers were estimated in each region and each year from national demographic statistics, and annual event and mortality rates and their ratio (28-day case fatality) were obtained. Linear trends with the period were estimated by Poisson regression for rates and logistic regression for case fatality.
Results: Age- and region-adjusted mortality rates decreased significantly in men and the mean relative annual change (−2.5%, p=0.001) was equally due to a decreasing event rate (mean relative annual change=−1.2%, p=0.015) and 28-day case fatality (mean relative annual change=−1.3%, p=0.07). Conversely, mortality and event rates both slightly increased in women (mean relative annual change=+1.0% for each rate, not significant), without any linear trend in case fatality.
Consistent trends with the general pattern were observed in Lille and Strasbourg for both genders. In Toulouse, however, age-adjusted mortality and event rates did not change in men during the period but both indicators were importantly rising in women (more than 4%/year) although at the limit of significance.
Conclusion: In France, whereas CHD mortality and event rates were still decreasing during the period 1997–2003 in men, a plateau was already reached in women. Toulouse (a low risk population) seemed somehow to precede this evolution, with steady rates in men and increasing ones in women.
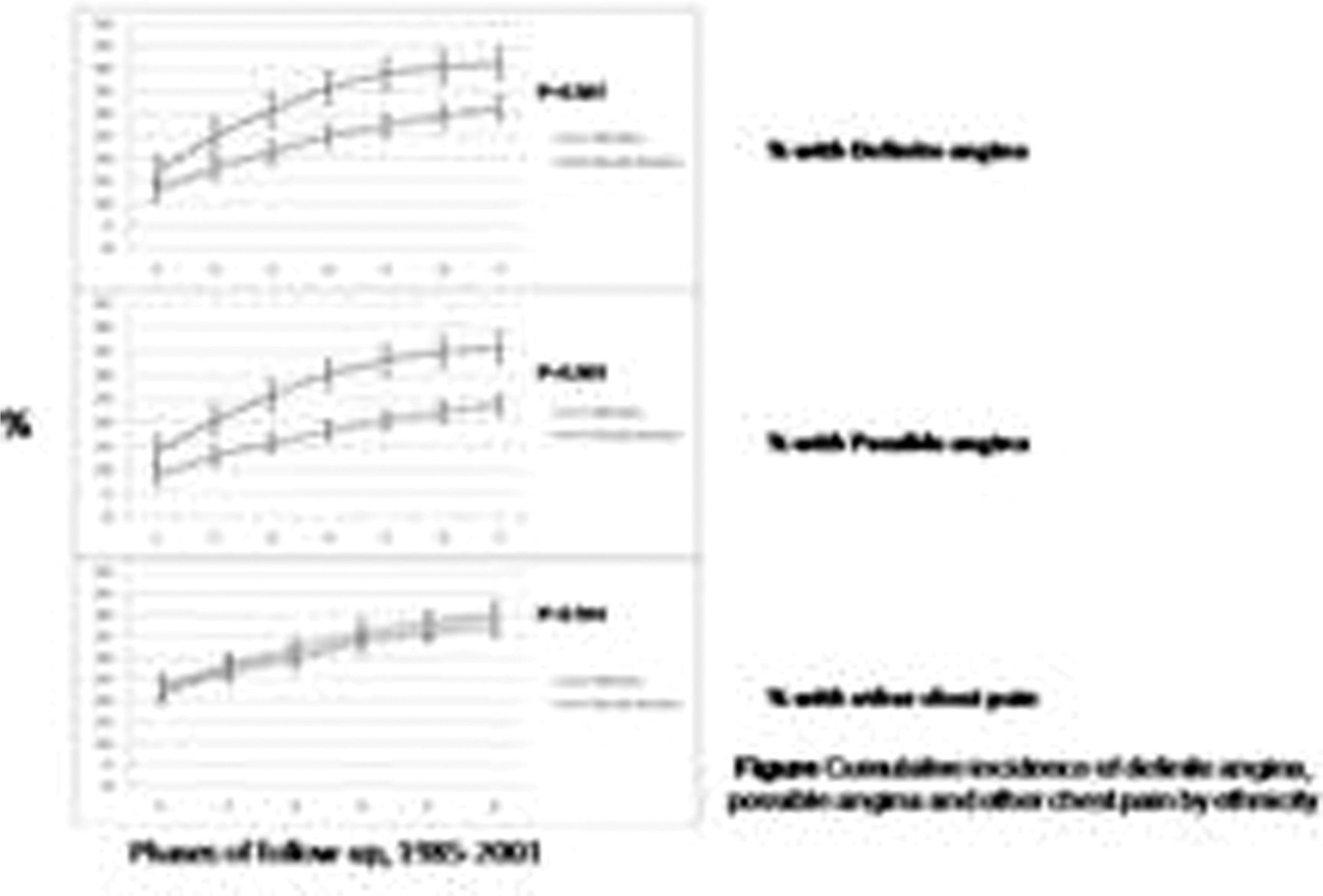
33 The incidence, character and prognosis of angina in South Asian and European populations
MJ Zaman1; M Shipley; M Stafford1; E Brunner1; M Marmot1; AD Timmis2; H Hemingway2
1University College London Department of Epidemiology And Public Health, London, United Kingdom; 2Barts and The London Hospitals Cardiology, London, United Kingdom
Background: Higher coronary death rates in South Asians compared to whites populations may be the result of a higher incidence of disease. Incident rates of angina are as yet unknown in South Asians and the utility of the Rose questionnaire [RQ] for angina in them has been questioned due to the atypical nature of their pain.
Objective: To determine cumulative incidence of angina in South Asians compared to whites in the Whitehall II cohort study and to examine the prognosis of differing forms of chest pain by ethnicity.
Methods: Prospective cohort study of all non-industrial civil servants aged 35–55 years who worked in the London offices of 20 civil service departments [9195 whites and 560 South Asians].
Outcomes: Chest pain was categorised as ‘definite’ angina, ‘possible’ angina and ‘other’ [non-Rose-possible] using the RQ. The outcome was a measure of coronary death and non-fatal myocardial infarction (NFMI) at 18 years.
Results: There was a higher cumulative incidence of definite [41.2% vs 31.3%, z=2.71, p=0.007] and possible angina amongst South Asians compared to whites. South Asians did not demonstrate a higher cumulative incidence of other types of chest pain. [42.8% vs 43.1%, z=0.07, p=0.944] In both ethnic groups, angina predicted coronary outcomes [fully-adjusted HR 2.94 (1.59,5.43) in South Asians with definite angina]. Other chest pain did not predict coronary outcomes in either ethnic group pain.
Conclusion: South Asians demonstrated a higher cumulative incidence of angina of a cardiac nature than whites. Angina, as ascertained by the Rose questionnaire, was predictive of coronary events. Our findings demonstrate that South Asians have a genuinely increased incidence of prognostically-significant angina, and that the Rose questionnaire can be used in South Asians to predict prognosis.
34 Incidence of unrecognized myocardial infarction the MONICA-Catalonia Study
S Menendez1; L Balana1; G Paluzie2; T Puig3; I Balaguer-Vintro4
1Institute of Health Studies, Barcelona, Spain; 2Consorci Maresme, Calella, Spain; 3Hospital Sant Pau Epiodemiology, Barcelona, Spain; 4Barcelona, Spain
Purpose: Unrecognized myocardial infarction has an increased probability of cardiovascular complications hence it is important to assess its frequency in the general population. The aim of this study is to report ten-year incidence of unrecognized myocardial infarction (UMI) in men and women aged 25 to 64 years at baseline.
Methods: The target population were the adult residents aged 25 to 64 years of a well defined geographical area. A stratified random sample of 2,571 subjects (75% response rate) taken from municipal population registers was examined for cardiovascular risk factors in 1986–88. This cohort was followed up for ten years and re-examined in 1996–97 (attendace rate 75%, 997 women, 934 men). Risks factor were measured following the WHO-MONICA manual of operations. In both examinations a 12- lead resting electrocardiogram (ecg) was taken and coded by the Minnesota code by two independent observers who were blind to any characteristics of the subjects. An UMI was defined if the person had no Minnesota Q-wave code in the baseline ecg, and a second ecg at ten-years with Minnesota code 1-1 or 1–2 except 1-2-6 and 1-2-8 plus no other evidence of known acute coronary syndrome assessed either by Rose questionnaire, self-report by the subject on interview in both exams, or absence of an acute MI registered in the MONICA population register.
Results: During the ten year period, 32 UMI occurred, giving a ten-year incidence of 9,3 per 1 000 in women and 15,7 per 1 000 in men. This represents approximately three quarters as much as diagnosed definite AMI in the same population, although is lower than the incidence found in other Northern European longitudinal studies. Incidence increased with age in both sexes. Subjects with UMI were less often smokers, but were more often hypertensive and diabetic and had lower level of education than subjects with no UMI.
Conclusion: The burden of AMI in this population is higher than described beforehand, as a high proportion of MI's remain clinically unrecognized. As their prognosis is worse according to other studies, intensified preventive efforts addressed to subjects likely to suffer these type of coronary events seems warranted.
35 Out-of-hospital mortality from ischemic heart disease in Kaunas middle-aged population according to the IHD register in 2001-2005
G Bernotiene; R Radisauskas; D Sidlauskiene; L Gogelis
Institute of Cardiology Population Studies, Kaunas, Lithuania; M. Riomeris University Institute of Forensic Kaunas Division, Kaunas, Lithuania
Purpose: The aim of the study was to evaluate trends in out-of-hospital mortality from IHD in Kaunas middle-aged (25–64 years) population during 2001 to 2005 according to the Ischemic Heart Disease Register's data.
Methods: The primary source of data was Kaunas population-based Ischemic Heart Disease Register. The data was collected according to the requirements of the WHO program MONICA. Only deaths due to IHD that occurred out-of-hospital were analyzed in this study. Trends in rates were analyzed using the method of linear regression on logarithms of the age-standardized by World population out-of-hospital mortality from IHD. The regression coefficient multiplied by 100 is given as an average yearly change.
Results: According to the IHD Register the out-of-hospital mortality from IHD during the analyzed years amounted 579 Kaunas middle-aged (25–64 years) residents: 493 (85.1%) men and 86 (14.9%) women. During the analyzed period, out-of-hospital mortality from IHD was on the average 108.7/100,000 among Kaunas men aged 25–64 years, meanwhile among women the corresponding rate was 8 times lower (13.2/100,000). Among middle-aged men the rate of out-of-hospital mortality from IHD during 2001–2005 years was tended to increase by 9.5% per year (p=0.06). Among women of the same age the corresponding rates during the analyzed period increased statistically significantly by 14.0% per year (p=0.02). The most changes in out-of hospital mortality from IHD were defined among 25–64 aged women with previous acute myocardial infarction (AMI): during the analyzed period out-of-hospital mortality from IHD tended to decrease on the average 13.6% per year (p=0.054), meanwhile the corresponding rates among men of the same age tended to increase by 9.9% per year (p=0.3).
Conclusion: Among middle-aged men the rate of out-of-hospital mortality from IHD during 2001–2005 years was tended to increase, meanwhile among 25–64 aged women was increasing statistically significantly.
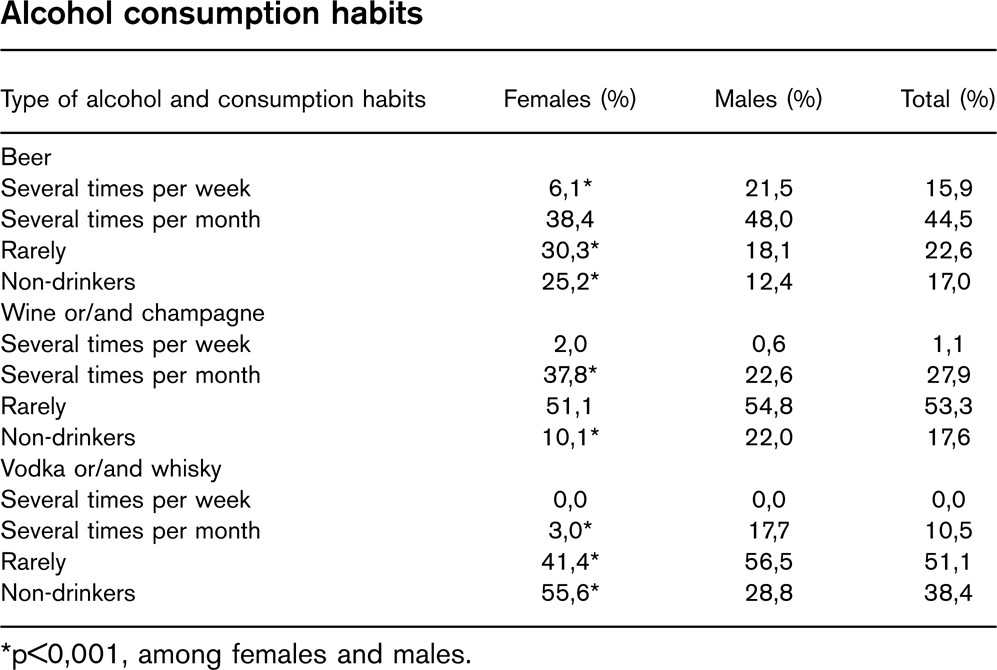
36 Alcohol consumption habits among Lithuanian students
A Janusauskas
Mykolas Romeris University Faculty of Public Security, Kaunas, Lithuania
Aim of Investigation: To investigate the main features of alcohol consumption of students.
Object of Investigation: 576 students of faculty of public security: 201 females and 375 males (99.3% of all the students, who entered Faculty in 2000–2006).
Methods of Investigation: The standardised questionnaire was created in faculty of public security. The analysis of the main features of negative influential factors for students’ health was based on informants’ answers to particular questions. The data of the investigation was analysed according to statistical methods.
Results of Investigation: It was found out that only 17% of students do not drink beer at all (25.5% of females and 12.4% of males, p>0.05). Approximately the same number of students (17.6%) does not drink wine and champagne at all (10.1% of females and 22% of males, p>0.001), 38.4% of students do not drink any strong drinks (55.6% of females and 28.8% of males, p>0,01). Every third female and every fifth male declared themselves as non-drinkers of any alcohol.
Conclusion: According to our study data, males mostly often drink more beer and strong alcohol drinks, whereas females prefer wine and champagne.
Alcohol consumption habits
Type of alcohol and consumption habits
Females (%)
Males (%)
Total (%)
Beer
Several times per week
6,1∗
21,5
15,9
Several times per month
38,4
48,0
44,5
Rarely
30,3∗
18,1
22,6
Non-drinkers
25,2∗
12,4
17,0
Wine or/and champagne
Several times per week
2,0
0,6
1,1
Several times per month
37,8∗
22,6
27,9
Rarely
51,1
54,8
53,3
Non-drinkers
10,1∗
22,0
17,6
Vodka or/and whisky
Several times per week
0,0
0,0
0,0
Several times per month
3,0∗
17,7
10,5
Rarely
41,4∗
56,5
51,1
Non-drinkers
55,6∗
28,8
38,4
∗p>0,001, among females and males.
37 Independent association of cigarette smoking and heavy alcohol consumption with cardiovascular risk factors in men and women from the Moli-sani project
S Costanzo; A Di Castelnuovo; F Zito; A De Curtis; R Di Giuseppe; A Arcari; L Rago; MB Donati; G De Gaetano; L Iacoviello
Catholic University Research Laboratories, Campobasso, Italy
Purpose: To investigate the association of cigarette smoking, heavy alcohol consumption and their interaction with major cardiovascular risk factors in an Italian population.
Methods: The Moli-sani Project is an on-going epidemiologic cohort study, on men and women, aged=35 years, randomly recruited from the general population of Molise, a Southern Italian region. From March 2005 to July 2007, 10,994 subjects were enrolled. After exclusion of subjects with previous cardiovascular and malignant disease, or under treatment for hypertension, diabetes or dyslipidemia, former drinkers or former smokers, 4,653 apparently healthy subjects (mean age±SD=49.7 ±10.2 years, 41% men) were analyzed. Using logistic regression adjusted for age, body mass index, menopause, alcohol consumption and cigarette smoking we compared those who smoked cigarettes or consumed alcohol with those who did not, and calculated the odds ratio (OR) (95% confidence interval (CI)) for the major cardiovascular risk factors.
Results: In men who smoked 11–20 or>20 cigarettes/day, compared with non-smokers, the OR(CI) of having the following laboratory values were as follows: total cholesterol=2400 mg/dl 1.5(1.1–1.9) and 1.6(1.1–2.3), respectively; HDL-cholesterol>400 mg/dl 1.7(1.3–2.4) and 3.6 (2.4–5.4), LDL-cholesterol=1600 mg/dl 1.4(1.0–1.8) and 1.1(0.7–1.7), triglycerides=2000 mg/dl 1.7(1.2–2.3) and 3.7(2.5–5.4). In women, who smoked 11–20 cigarette/day, the corresponding OR(CI) were the following: high total cholesterol 1.5(1.1–2.0), high LDL-cholesterol 1.7 (1.2–2.4), high triglycerides 2.8(1.8–4.7). The OR of low HDL-cholesterol were 2.6(1.5–4.5), 2.4(1.2–4.9), 8.3(2.7–26.4) in women who smoked 1–10, 11–20,>20 cigarettes/day, respectively. In men who consumed>40 grams/day of alcohol, compared with non-drinkers, the OR(CI) were: high total cholesterol levels 2.7(1.7–4.3), low HDL-cholesterol 0.3(0.2–0.5), high LDL-cholesterol 1.6(1.0–2.6), high triglycerides 1.8(1.1–2.9), glucose=1000 mg/dl was 1.5(1.0–2.1). In women who consumed>20 grams/day of alcohol the adjusted OR of high total cholesterol was 1.4(1.1–1.9) and high glucose 1.4(1.0–1.9). Neither in men nor in women, interactions between high alcohol consumption (>20 grams/day in women, >40 grams/day in men) and smoking>10 cigarettes/day, on the association with any cardiovascular risk factor could be found.
Conclusion: Although heavy alcohol consumption increased HDL-cholesterol with a potential protective effect on coronary heart disease, its adverse effect on all other major cardiovascular risk factors was similar to that of smoking>10 cigarettes/day.
38 Effects of Italian smoking regulation on rates of hospital admission for acute myocardial infarction: evidence of effect modification by age
F Francesco Barone-Adesi; L Vizzini; F Merletti; L Richiardi
University of Turin Unit of Cancer Epidemiology, Turin, Italy
Objective: Recent studies carried out in Italy and USA have shown a reduction of hospital admissions for acute myocardial infarction (AMI) after the introduction of regulations banning smoking in public places. Using data from the Piedmont Region, Italy, we had previously estimated a reduction of 11% in the first five months after the introduction of a national ban (January 2005), limited to individuals aged less than 60. We have updated our previous study in order to evaluate longer term effects of the ban. Furthermore we estimated the possible reduction in AMI attributable to a smoking ban by the decrease in acute effects of passive smoking.
Methods: Rates of admission for AMI in Piedmont from 2001 to 2006 were analysed using regression models allowing for long term trends and seasonality. The expected decreases in AMI incidence due to regulations banning smoking in public places by the prevention of acute effects of passive smoking were calculated assuming different scenarios of prevalence of active smoking, relative risk of AMI after acute exposure to passive smoking, and population average hours at increased risk of AMI per week after exposure to passive smoking.
Results: A reduction of hospital admissions for AMI among persons aged less than 60 was still evident 18 months after the introduction of the smoking ban in Italy (Rate Ratio, 0.91; 95% confidence interval, 0.85–0.98). No effect was found among persons aged at least 60. Simulations of the possible acute effects of passive smoking showed that, although up to 30% reduction may theoretically occur, a decrease of 5% to 10% is more likely.
Conclusion: These results suggest that smoke-free policies may result in a short-term reduction in admissions for AMI.
39 Five year incidence of Cardiovascular Disease; the ATTICA Study
DB Demosthenes B Panagiotakos1; C Chrysohoou2; C Pitsavos1; L Papadimitriou1; Y Lentzas1; Y Skoumas1; C Stefanadis1
Objectives: The 5-year incidence of cardiovascular disease (CVD) and its determinants, in a sample of men and women from Greece, was evaluated.
Methods: From May 2001 to December 2002, 1514 men and 1528 women (>18 y) without any clinical evidence of CVD, living in Attica area, Greece, were enrolled in the ATTICA study. In 2006, a group of experts performed the 5-year follow-up (941 of the 3042 (31%) participants were lost to follow-up). Development of CVD (coronary heart disease, acute coronary syndromes, stroke, or other CVD) during the follow-up period was defined according to WHO-ICD-10 criteria.
Results: The 5-year incidence of CVD was 11.0% in men and 6.1% in women (p>0.001); the case fatality rate was 1.6%. Multi-adjusted logistic regression analysis revealed that increased age (odds ratio per year=1.09, p=0.04), waist-to-hip ratio (odds ratio=5.07, p=0.02), hypertension (odds ratio=4.53, p=0.001), diabetes (odds ratio=4.53, p=0.001) and C-reactive protein levels (odds ratio per 1 mg/dl=1.31, p=0.02), were the most significant baseline bio-clinical predictors of CVD. Furthermore, increased education level and greater adherence to the Mediterranean diet (among 35–65 y old subjects) were associated with lower CVD incidence (odds ratio per 3-years of school difference=0.83, p>0.001 and odds ratio per 1/55 units in diet score=0.94 p>0.001), irrespective of various potential confounders.
Conclusion: Aging, central fat, hypertension and diabetes, inflammation process, low social status and abstinence from Mediterranean diet, seem to predict CVD events within a 5-year period.
40 Predictors of early onset of coronary artery disease in Polish women
B Lubiszewska; G Broda; P Kurjata; E Ksiezycka; W Piotrowski
Institute of Cardiology Coronary Artery Disease Department, Warszawa, Poland
Background: During last 10 years the rise in coronary artery disease (CAD) in younger women has been observed. Pathophysiology of premature coronary artery disease in women is not well understood. Emerging data suggest a unique risk profile in women.
Objective: To identify and quantify risk factors contributing to early onset of coronary artery disease in women.
Methods: Case-control study of 282 women with early onset of established CAD (acute MI, angiografically confirmed angina or revascularization before 55 years of age) enrolled between April 2005 to April 2007, and 328 age-matched healthy controls, selected from the National Health Survey – WOBASZ study.
Results: Multivariable logistic regression model showed that cigarette smoking, menopausal status, impaired fasting glucose level (=110 mg/dl) (IFG) or diabetes, hypertension, waist circumference=88 cm, hsCRP, and educational level were significant and independent determinants of early onset of CAD in women. The highest ORs were observed for early menopause (OR- 11.2; 95% CI- 6.2–20.0), IFG or diabetes (OR 4.3; CI-2.4–7.6), smoking (OR-4.5; CI-2.7–7.3) and hypertension (OR-2.0; CI-1.3–3.3). Other factors increased the risk of premature CAD in women of about 30–60%.
Conclusions: The presence of early menopause, impaired fasting glucose or diabetes, cigarettes smoking and hypertension were main predictors of premature CAD in women.
41 High ten year risk for fatal cardiovascular disease in ambulatory daily practice patients in Belgium
L Missault; N Witters2; J Imschoot1
1St Jan Hospital Cardiology, Brugge, Belgium; 2Brussels, Belgium
A cross-sectional evaluation of the ten year risk for fatal cardiovascular disease in a cohort of 12,637 evaluable consecutive patients aged=50 years representative for the Belgian population visiting their GP was performed including the SCORE system. A total of 6846 (54%) male and 5768 (46%) female subjects were included.
4161 (33%) patients were actual smokers.
Although 61% of patients were treated with at least one antihypertensive drug, mean systolic blood pressure was 141+/-15 mmHg with no difference between sexes on the whole although in the higher SCORE risk groups blood pressure was higher in females. Stage I hypertension was present in 43% of patients, stage II in 13% and stage III in 3%.
Categorisation of patients according to absence or presence of hypercholesterolemia was left at physician's perception. 40% of patients were considered normocholesterolemic. In the group of patients with hypercholesterolemia, total cholesterol level was 242+/-355 mg/dl suggesting that only very high cholesterol is considered relevant by physicians. After reclassification according to European Guidelines for cholesterolemia, patients with perceived hypercholesterolemia turned out to be normocholesterolemic in 0.4%, untreated hypercholesterolemic in 23.3% and undertreated hypercholesterolemic in 76.3%. Virtually 0% of patients (N=3) was correctly treated.
BMI>30 was found in 41% and abdominal obesity was present in 50% with no difference between sexes.
Diabetes was present in 2434 patients (19.5%) equally distributed between sexes. Of all patients, 3466 (27.4%) had suffered at least one vascular event and 2336 (18.5%) were>75 year. Patients with diabetes, personal history of vascular event and/or age>75 years are considered at high risk as such and these patients were thus excluded from the risk analysis according to the SCORE table. In the remaining 6383 (50,5%) patients, the 10 year fatal cardiovascular risk according to the Belgian SCORE table was determined as follows: 750 (11.75%) showed a risk of >2%; 1733 (27.15%) a risk of 2–4%; 2316 (36.28%) a risk of 5–9% and 1584 (24.82%) had a risk of 10% or more.
This survey shows that despite simple, clear, credible guidelines and a very accessible health system in Belgium the 10-year fatal cardiovascular risk remains very high (>5%) even in a professional medical environment of daily practice. Smoking and obesity remain highly prevalent and require further sensibilisation. Blood pressure is inadequately treated in more than half of the subjects and medical management of hypercholesterolemia is disappointing despite good accessibility to antilipemic drugs.
42 The role of health examination surveys in determining priorities for CVD prevention: experience from the UK
P Primatesta
University College London Epidemiology & Public Health, London, United Kingdom
Background: Priorities for cardiovascular disease (CVD) prevention can be determined by looking at changes over time in CVD prevalence and CVD risk factors and assessing cardiovascular risk using data from Health Examination Surveys (HESs).
Methods: The HESs in the UK (separately in England and Scotland) have been running since the early ‘90s, in sociodemographically representative samples of the non-institutionalised population (drawn yearly from the Postcode Address File). Data are collected at two home visits: an interviewer's visit (when a questionnaire is administered to collect information on socio-demographic data, risk factors and medical history) and a nurse visit (when several physical measurements are taken).
Results: While trends in ischaemic heart disease remained stable over the last 10 years, data from the Health Survey for England suggest an increase in stroke prevalence in the population in England. Annual monitoring of obesity (both generalised and abdominal) showed a rapid increase over the last 10 years. In adults aged 16–64 the percentage of obese (BMI>30 kg/m2) increased in England by over 50%, and similar changes were observed in Scotland. By projecting obesity to the year 2012, further increases were predicted. The prevalence of diabetes also increased in all age groups, and the prevalence of hypertension (using a standardised definition) was 30.5% in 1994 and 30.4% in 1998, compared with 34.2% in 2003; with awareness, treatment and control rates all substantially increasing over time. Only small changes in levels of dyslipidaemia were seen since 1998 (in 2003 69.9% of adults had a total cholesterol>= 5 mmol/l vs. 67.5% in 1998), but use of lipid-lowering treatment has more than doubled and control rates have increased by approximately fourfold. In people without CVD the risk profile (10-year CVD risk>=20%) varied by sex and age, with older men more likely to be at high risk due to a combination of risk factors.
Conclusion: The results from Health Surveys can be used to set public health targets, establishing a baseline for monitoring changes. The information collected can enable health monitoring and scientific research.
43 Equivalence of subclinical atherosclerosis measurements to cardivascular death for evaluating risk factor impact: the REFINE Reykjavik study
T Aspelund; B Thorsson; V Gudnason
Icelandic Heart Association Biostatistics Unit, Kopavogur, Iceland
Background and aim: Conventional risk estimates do not allow for the necessary stratification for people with moderate risk. In 2006 we embarked on a new population based study, REFINE Reykjavik Study, of men and women aged 35–70, adding ultrasound studies of the carotids to identify subclinical atherosclerosis on top of conventional risk factor measurements. The aim of this investigation is to examine the relationship between conventional risk factors and subclinical atherosclerosis and compare it to relationships seen in the Reykjavik Study Risk Score and the European SCORE for 10-year risk of fatal coronary heart disease.
Methods: The first 2000 participants in the ongoing were used for analysis. Ultrasound measurements for evaluation of clear evidence for atherosclerosis by plaque formation was carried out.
Results: Plaque was found in 14% of men and 11% of women, strongly associated with age. Odds ratios for plaque in the REFINE Reykjavik Study compared to hazard ratios for fatal coronary heart disease from the Reykjavik Study and SCORE according to smoking status, blood pressure and cholesterol levels are shown in the Table.
Conclusion: Ultrasound of the carotids revealing subclinical atherosclerosis shows the same relationship with conventional risk factors on a population level as do both the Reykjavik Study and the European SCORE study. This suggests vascular disease can be studied at a population level long before conventional endpoints materialize. REFINE Reykjavik Study can therefore be used to potentially identify new risk factors for cardiovascular disease.
HR for fatal CHD and OR for plaque
Risk Factor
Reykajvik HR
SCORE HR
REFINE OR
Current Smoker
2.11
2.03
3.49
Systolic BP (10 mmHg)
1.23
1.20
1.25
Cholesterol (mmol/L)
1.34
1.27
1.27
Hazard ratios for fatal coronary heart disease from the Reykjavik Study and the SCORE project in comparison with odds ratios for Plaque in the REFINE Reykjavik Study.
44 Contribution of conventional risk factors to incident stable angina and acute coronary syndrome in middle-aged men: the PRIME Study
F Canoui-Poitrine
I Juhan-Vague2; D Arveiler3; J Ferrieres4; P Amouyel5; A Bingham6; P Ducimetiere3; JP Empana3
Purpose: To test whether conventional coronary heart disease (CHD) risk factors and antihypertensive treatment were more predictive of first stable angina (SA) than first acute coronary syndrome (ACS).
Methods: We used data from the PRIME Study, a prospective cohort of 9,758 asymptomatic middle-aged men recruited in Northern Ireland and France between 1991 and 1993. Using a logistic multinomial regression model, we estimated and compared the odds ratios (OR) for first SA and first ACS, taking men who remained free of CHD during follow up as the reference group.
Results: After 5 years of follow-up, 114 first SA and 178 first ACS were validated. Diastolic blood pressure (adjusted OR=1.36 95% Confidence Interval (CI): 1.18–1.57 for SA versus 1.04 95% CI: 0.87–1.26 for ACS; p for comparison between ORs= 0.028) and possibly cigarette smoking (adjusted OR=2.09; 95% CI: 1.44–3.05 versus. 1.30; 95% CI: 0.83–2.03; p for comparison between ORs=0.09) were more predictive of first ACS than first SA. The opposite trend was found for antihypertensive treatment (adjusted OR=2.24, 95% CI: 1.42–3.53 for SA versus. 1.29, 95% CI: 0.85–1.97 for ACS, p for comparison between ORs =0.03). Consistent findings were found for β-blockers and calcium-channel blockers.
Conclusion: This multicenter large cohort study suggests that diastolic blood pressure and possibly cigarette smoking were more predictive of incident ACS than SA while the opposite was found for antihypertensive treatment. These results support the hypothesis that SA and ACS as a first manifestation of CHD may not share entirely the same risk factors.
45 Predictive accuracy and usefulness of calibration of the ESC SCORE in Switzerland
P Pedro Marques-Vidal1; N Rodondi2; M Bochud1; A Pecoud2; D Hayoz3; F Paccaud2; V Mooser4; G Waeber5; P Vollenweider1
1Inst. Univ. de Medecine Sociale et Preventive UPC, Lausanne, Switzerland; 2University of Lausanne Cardiovascular Prevention Clinic, Lausanne, Switzerland; 3Centre Hospitalier Universitaire Vaudois Medicine, Vascular Medicine, Lausanne, Switzerland; 4GlaxoSmithKline Medical Genetics, Philadelphia, United States of America; 5Centre Hospitalier Universitaire Vaudois Medicine, Internal Medicine, Lausanne, Switzerland
Background: Prevention of cardiovascular disease (CVD) at the individual level should rely on the assessment of absolute risk using population-specific risk tables.
Objective: To compare the predictive accuracy of the original and the calibrated SCORE functions regarding 10-year cardiovascular (CV) risk in Switzerland.
Design: Cross-sectional, population-based study (5,773 participants aged 35–74).
Methods: The SCORE equation for low risk countries was calibrated based on the Swiss CVD mortality rates and on the CVD risk factor levels from the study sample. The predicted number of CVD deaths after a 10-year period was computed from the original and the calibrated equations and from the observed CV mortality for 2003.
Results: According to the original and calibrated function, 16.3% and 15.8% of men and 6.8% and 8.2% of women, respectively, had a 10-year CVD risk>5%. There was a strong agreement between the two functions: kappa was 0.767 for men, 0.784 for women, both p>0.001. Both risk functions adequately predicted the 10-year cumulative number of CVD deaths: in men, 71 (original) and 74 (calibrated) deaths, for 73 deaths when using the CVD mortality rates; in women, 44 (original), 45 (calibrated) and 45 (CVD mortality rates), respectively. Relative to the original function, the calibrated function classified more women and fewer men at high risk. Moreover, the calibrated function gave better risk estimates among subjects aged over 65.
46 Comparison of the efficacy of Polish risk score (PSR) with the common used scores in the group of Polish patients of highest risk underwent surgical revascularization
PK Okonski1; M Banach2; J Zaslonka1; R Jaszewski1
11st Chair of Cardiology and Cardiac Surgery, Lodz, Poland; 21st Chair of Cardiology and Cardiac Surgery Department of Cardiology, Lodz, Poland
Introduction: Commonly used scores of surgical risk in cardiac surgery were founded as a result of wide multicenter researches, however in none of them Polish patients were included. Thereby the aim of our study was to select the most important risk factors in Polish population patients, and to compare the created SCORE with the internationals scores (EUROSCORE and Cleveland Clinic Foundation) commonly used in Polish departments of cardiac surgery.
Materials and methods: The research was performed prospectively in 12 Polish cardiosurgical centers, in the group of 4653 patients (male: 74.19% and female: 25.81%) aged between 29–87 years (mean: 61.64±9.17), subjected to isolated surgical revascularization. The inclusion criteria to the group of patients of highest risk were as follows: =10 points in PSR SCORE (n=200),=6 pt. in EUROSCORE (n=1094), and=7 pt. in Cleveland Clinic Foundation score (CCF) (n=291).
Results: The efficacy of scores was evaluated with the application of AUC - area under the receiver operating characteristic (ROC) curve. The obtained results for the particular scores in these three groups of high risk patients were as follows: PSR group: PSR–0.755, EURO-SCORE-0.686, CCF-0.609; EUROSCORE group: PSR-0.758; EUROSCORE-0.717; CCF-0.602; CCF group: PSR-0.908; EUROSCORE-0.793; CCF-0.706.
Conclusion: Irrespective of the score on the basis of which the highest risk patients were selected, the highest ROC curve with the largest area under the curve was calculated for PSR SCORE. It incontestably means that PSR SCORE discriminates the Polish patients against deaths in the most significant way.
47 National health examination surveys in Europe
H Tolonen1; K Kuulasmaa2; M Chaudhury3; S Conti4; S Graff-Iversen4; L Grotvedt4; P Primatesta5; G Rago1; M Verschuren6; L Viet2
1National Public Health Institue Dept. of Health Promotion and Chronic Disease, Helsinki, Finland; 2National Public Health Institute, Helsinki, Finland; 3University College London, London, United Kingdom; 4Istituto Superiore di Sanita, Rome, Italy; 5Norwegian Institute of Public Health, Oslo, Norway; 6National Institute for Public Health and Envi, Bi Ithoven, Netherlands
Health information is needed for the planning and evaluation of prevention programmes as well as for the planning of health policies at the country level. Some health information is available through official statistics (e.g. total mortality, cause specific mortality, hospital admissions) but for example the prevalence of hypertension or obesity in the population can only be obtained only through population based health examination surveys.
Health examination survey (HES) is a population based survey where the required information is collected through questionnaires and at least some physical and biological measurements (e.g. blood pressure, test of functional capacity and blood samples) are included. Feasibility of a European Health Examination Survey (FEHES) Project is assessing the feasibility of carrying out a standardized national HES in all EU countries and prepares a proposal for their implementation. The Project is carried out within the Public Health Programme of the European Commission.
According to the results of FEHES, in period 2000–2007, national HES among adults were conducted in 13 EU countries. For years 2008–2012, 17 countries have active plans for some form of national HES. Contact persons in the European countries have indicated that HES is an important source of health data in their country and that international comparability of the data is desirable.
The most recent internationally comparable data on chronic disease risk factors in the populations is from the WHO MONICA Project, which ended over 10 years ago. Since that there has not been an international coordination for standardized HESs and for their quality control and evaluation. This has created a shortage of comparable health information in Europe. The opportunity to standardize the forthcoming national HESs and to evaluate their success in order to facilitate HESs in other countries should not be missed.
48 Distribution profile of CV risk factors and their calculation by means of computer-assisted scores: comparative analysis of the ESC, Framingham- and PROCAM-Scores in the framework of the PreFord Study
S Tuerk; J Joachim Latsch; B Bjarnason-Wehrens; HG Predel
German Sports University Institute of Cardiology and Sports Medicine, Cologne, Germany
Topics: The PreFord Study is a multicenter prospective cohort study to evaluate guideline based risk management on primary prevention of CVD. The objective of the trial was to evaluate the results of the initial screening phase.
Methods: In a cross case analysis the CV risk profile of 4810 employees (724 female, 46,6±13,2y, 166,2±7,1 cm, 70,1±13 kg, BMI 25,4±4,6 kg/m2; 4086 male 44,8±10,5y, 178,8±7,5 cm, 86,9±13,4 kg, BMI 27,2±3,9, kg/m) was assessed through systematic screening. The ESC score (10 year risk of a fatal CV event) was implemented for the evaluation. The subjects were sub-grouped according to ESC risk results: Risk group (RG) I: 0–1%, RG II: 1–5%, RG III:>5% individual risk. In the following the ESC-Germany-Score, the PROCAM-Score, and the Framingham-Score were also applied to the data record for comparison (risk stratification defaults were considered).
Results: 14,8% of all subjects (16–84 y, 16.1% of the male and 7% of the female) were classified into the RG III by ESC-Score, thus exhibiting a high risk for the occurrence of an acute CV event (RG II: 36,5%, RG I: 48,7%). For a comparison of the Scores the collective had to be reduced on a calculable age span (40–65y, n=2920).
Discussion: The regional European ESC-Score (Score-Germany) seems to estimate the German population more precisely, more so than the “high risk” Score of the ESC. The Framingham-Score proves to be unsuitable, as the trial population is based on the data from the USA, who are all older than 30 years. In the context of a prevention study with existing high CV risk, the necessity for a life-style intervention should particularly be highlighted. Thus the ESC-Germany-Score appears to be the most suitable Score model.
Score-Model
ESC-Score
Germany-Score (ESC)
PROCAM
Framingham
Riskgroup
I
%
26,1
31,5
85,9
61,6
n
669
827
2145
1610
II
%
56,7
55,8
10,3
31,2
n
1453
1464
256
814
III
%
17,2
12,7
3,8
7,2
n
441
334
96
188
Distribution of risk groups I-III in % after the Score models ESC, ESC-Germany, PROCAM and Framingham. n=2920, age 40–65 years.
49 Effects of smoking on lipids and apolipoproteins in healthy people
WM Masson; DA Siniawski; P Sorroche; W Scordo; L Casanas; J Krauss; AM Cagide
Hospital Italiano, Buenos Aires, Argentina
Background: Changes in plasma lipoproteins levels could be one of the mechanisms by which smoking increases cardiovascular risk. In our region there is not much information about how smoking affects levels of plasma lipoproteins and apolipoproteins.
Objetive: Establish the effects of smoking on plasma lipoproteins, Apolipoprotein A1 (A) and Apolipoprotein B (B) in a healthy young population.
Methods: The A, B and lipoproteins levels (HDL-C, total cholesterol and triglycerides) were determinated in samples obtained of blood givers. The levels of lipoproteins (n=205) and apolipoproteins (n=403) according to the presence or absence of smoking were analyzed.
Results: 403 patients were recruited. Patients with diabetes, hypertension, a history of cardiovascular disease or lipid-lowering therapy were not included. Mean age±SD: 36±12 years, 67% men. Baseline characteristics of the population are shown in a Table 1. The A and HDL-C levels were higher in nonsmokers than in smokers (A:151±32 mg/dL vs. 144±30 mg/dL, p>0.05; HDL-C: 52±18 mg/dL vs. 46±11 mg/dL, p>0.05). The B and total cholesterol levels were similar in both groups (B: 93±25 mg/dL vs. 92±29 mg/dL, p=NS; Total cholesterol: 194±40 mg/dL vs. 196±45 mg/dL, p=NS). Triglycerides level was greater in smokers, although this difference was not statistically significant (124±91 mg/dL vs. 99±78 mg/dL, p=NS). The correlation between HDL-C and A in our population was good (r=0.85).
Conclusion: In this young and healthy population, smoking decreased plasma levels of HDL-C and A. These findings could be related to the increase in cardiovascular risk in smokers.
Smokers (n=139)
Nonsmokers (n=264)
Age (mean±SD)
35±12
37±12
Male (%)
65
67
Body mass index (mean±SD)
25.71±4
25.75±4
Baseline characteristics of the population.
50 Atherogenic dyslipidemia - Does it matter?
N Antonio; Coimbra, Portugal
Background: The atherogenic dyslipidemia (AD) is characterized by 3 lipid abnormalities: increased triglycerides, decreased HDL levels and the presence of small dense LDL cholesterol particles. This lipid triad is a common, but modifiable, feature in persons with premature coronary heart disease.
Purpose: To characterize the clinical features associated to AD and evaluate the impact of AD on severity and short-term prognosis of acute coronary syndromes (ACS) patients.
Methods: We retrospectively analyzed 851 patients consecutively admitted for ACS, in a single coronary care unit. Patients were divided into two groups: A) 268 patients with AD (triglycerides>1500 mg/dl and HDL>40 in men or >466 mg/dl in women) and B) 583 patients without AD.
Results: Patients with AD had more diabetes, obesity, smoking habits and metabolic syndrome and significantly higher levels of apoprotein B (Apo B). Affected patients were significantly younger, had significantly lesser levels of peak Troponin I, better systolic cardiac function and higher levels of creatinine clearance. However, there were no significant differences in length of stay, number of vessels with significant stenosis, prevalence of STEMI or inhospital mortality between groups. Multivariate logistic regression analysis showed that Apo B, diabetes, glycosylated haemoglobin (HbA1c) and metabolic syndrome are independent preditors of AD. In order to detect the better marker of AD among ACS patients, a receiver-operating characteristic (ROC) analysis was performed. Apo B exhibited the greater accuracy and the best performance, with an optimal value of cut-off point of 94.55 mg/dl (sensitivity 72.9%, specificity 59.5%), in prediction of AD.
Conclusion: Although younger and with some features associated with better prognosis, patients with AD have the same severity of coronary stenosis and short-term prognosis as patients without AD. The fact that older patients had less AD than younger suggests that AD is associated with a worse life expectancy, indicating the need for early and intensive preventive measures. Apo B seems to be reliable to identify AD and individuals with Apo B higher than 94.55 mg/dl may benefit from stronger lipid-lowering intervention.
51 Evaluation of high-density lipoprotein cholesterol goals in patients with diabetes and coronary artery disease presenting with acute coronary syndromes
CN Lourenco; R Teixeira; N Antonio; S Monteiro; F Goncalves; P Monteiro; L Goncalves; M Freitas; LA Providencia
Coimbra University Hospital Cardiology, Coimbra, Portugal
Purpose: Current guidelines recommend a more aggressive target related to lipid profile for patients with diabetes and coronary artery disease (CAD). High-density lipoprotein cholesterol (HDL-C) is an independent risk factor for CAD. However, more focus has been given on LDL cholesterol. Moreover, 60 or 70% of events still occur despite remarkable reduction of LDL cholesterol and the effects of the standard drugs to treat dyslipidemia have a variable and often non satisfactory effect over HDL levels. The aim of this study is to evaluate the HDL-C profile of patients with acute coronary syndrome (ACS) and previously known diabetes mellitus or coronary artery disease.
Methods: Retrospective analysis of 898 consecutive patients hospitalized in a single coronary care unit between May 2004 and July 2007, and who had simultaneously known diabetes and coronary artery disease. Patients were divided in two groups, each one in two subgroups: 1) HDL>40 and >40 mg/dl for men; 2) HDL>45 or >45 mg/dl for women.
Results: The mean value of HDL was 40.56 mg/dl for men and 43.74 mg/dl for women; 53.2% (n=341) presented HDL >40 mg/dl in the first group, whereas 59.5 (n=153) presented HDL >45 mg/dl in the second one. When comparing the groups, we found that both groups with lower levels of HDL have a higher incidence of diabetes mellitus, HbA1c, triglycerides and lower total cholesterol, LDL and ApoA levels. Also they presented more on high TIMI score. While woman with low HDL levels had more often previous myocardial infarction and atrial fibrillation, men with low HDL levels had more complex coronary lesions. No differences between the two groups were found related to age, incidence of arterial hypertension, previous treatment with statin, type of ACS, cerebrovascular disease, myocardial necrosis markers levels, Killip class, renal function, rate of complications or death.
Conclusion: We can conclude that the majority of these patients were not meeting the recommended goals for the HDL, although a significant part of them were on statin. Because low HDL and the atherogenic dyslipidemia are firm risk factors for ACS, probably this lipid profile contributed for ACS in this population, particularly in those with normal LDL values. Every effort should be made for all this high risk patients to meet target HDL values, by lifestyle modification and/or using more specific target drugs.
52 Lipid levels in patients admitted with myocardial infarction to a regional cardiology centre 2000–2006: is there an association with declining prevalence of ST elevation myocardial infarction?
PJ Scott; V Kodoth; R Noad; JC Murphy; JR Bennett; P Mckavanagh; C Owens; G Manoharan; AAJ Adgey
Royal Victoria Hospital Cardiology, Belfast, United Kingdom
Purpose: Hypercholesterolemia is a major risk factor for coronary artery disease. Revised Joint British Society Guidelines 2005 (JBS-2) have recommended lower LDL and total Cholesterol with higher HDL cholesterol targets for both primary and secondary prevention. We reviewed trends in fasting lipid levels of patients admitted with Myocardial Infarction (MI) to our centre.
Methods: Fasting lipid profiles were analysed in patients admitted with an MI from January 2000 to December 2006 (n=1346). We also compared patients with ST elevation myocardial infarction (STEMI) and Non-ST elevation myocardial infarction (NSTEMI) to determine if lipid levels differed.
Results: On admission, average total Cholesterol decreased from 5.20 mmol/L in 2000 to 4.68 mmol/L in 2006 (p=0.026) and LDL Cholesterol from 3.11 mmol/L to 2.52 mmol/L (p=0.009). HDL Cholesterol rose from 1.11 mmol/L in 2000 to 1.30 mmol/L in 2006 (p=0.006). STEMI patients had significantly higher total Cholesterol (5.12 mmol/L vs 4.80 mmol/L; p>0.001), LDL (3.0 mmol/L vs 2.75 mmol/L; p>0.001) and lower HDL (1.20 mmol/L vs 1.24 mmol/L; p=0.161) when compared with those admitted with NSTEMI. The number of STEMI patients admitted fell from 221 in 2000 to 72 in 2006 (p>0.001). A significant linear correlation existed between the average number of STEMI patients admitted and the associated Cholesterol: HDL ratio for that year (p=0.011).
Conclusion: Our study reveals a reduction in lipid profile values on admission from 2000 to 2006. We also noted that patients admitted with STEMI had a higher total Cholesterol, LDL and lower HDL than NSTEMI. Current guidelines for primary and secondary prevention of coronary heart disease has led to more fastidious usage of anti-lipid medications which has had a significant impact on the reduction of cholesterol on patients admitted with MI. The previously documented fall in patients admitted with STEMI is further highlighted in our study, and we propose is linked with the associated fall in average cholesterol levels.
53 Trends in arterial hypertension and mortality from stroke among middle-aged Kaunas population during 1983–2006
D Sopagiene; A Tamosiunas; R Reklaitiene; R Radisdauskas; K Jureniene
Institute of Cardiology, Kaunas, Lithuania
Purpose: Of this study was to evaluate prevalence of arterial hypertension among Kaunas population aged 35–64 and stroke mortality trends during 1983–2006.
Methods: Four independent surveys in 1983–1984, 1986–1987, 1992–1993, and 2001–2002 were carried out in random samples of men and women aged 35–64 involving 2413, 1762, 1231 and 1403 persons, respectively. The risk factors were defined within the framework of the WHO MONICA study (Multinational Monitoring of Trends and Determinants in Cardiovascular Disease). The source of stroke mortality data among population aged 35–64 years was the official mortality statistics. The age-standardized rates were calculated by the direct method using the European population as a standard.
Results: During the study period the mean values of systolic blood pressure decreased among men. Among women decreased both mean values of systolic and diastolic blood pressure, however the prevalence of hypertension has decreased only among women by 11.9% (from 51.3% to 39.4%, p>0.001) with no significant changes among men. According to the official mortality statistics data, during the study period, the average rate of mortality from stroke was 68.99/100,000 for men and 35.39/100,000 for women. During the study period trend analysis showed a significant decline in mortality rates from stroke among Kaunas population by 2.5%/yr., p=0.0003 (by −2.4%/yr., p=0.002 in men and −2.6%/yr., p=0.0005 in women).
Conclusion: The decreasing trend in the prevalence of arterial hypertension has been assessed in Kaunas middle-aged women during 1983–2002 years. Despite the decreasing trends during 1983–2006 in the mortality rates from stroke among Kaunas population, programs or strategies targeted to control levels of arterial blood pressure are still needed.
Mortality trends from stroke in Kaunas
54 Tissue Doppler and strain imaging evaluation of obesity-related adjunctive systo-diastolic ventricular dysfunction in patients with hypertension
M Leggio1; L Sgorbini2; G Cruciani2; GR Cristinziani2; A Mazza3; MG Bendini3; F Leggio1; AP Jesi2
Purpose: Obesity is an independent risk factor for the development of heart failure, even after accounting for other co-morbid conditions that cluster with it, such as above all hypertension. In this context, application of innovative echocardiographic techniques like tissue Doppler imaging (TDI) and strain imaging (SI) has been largely extended, in order to improve the assessment of systo-diastolic ventricular function. Thus, aim of this study was the evaluation of left ventricular morphologic and functional parameters with traditional echocardiography, TDI and SI in patients (pts) with hypertension compared to pts with hypertension and obesity.
Methods: We evaluated 190 pts, mean age 56±11 years, 94 males, affected by essential hypertension and divided according to their body mass index (BMI) in Group 1 (BMI>30, 96 hypertensive pts without obesity) and Group 2 (BMI=30, 94 hypertensive pts with obesity). The 2 groups were matched in age, sex, heart rate, systo-diastolic blood pressure, medical therapy; apart from familiar history of cardiovascular disease, no others risk factors nor systemic diseases were represented in the study population. All pts were evaluated with traditional echo-cardiography, TDI and SI: for all pts mean values of peak systolic, early diastolic and late diastolic velocities of the septal, lateral, inferior and anterior region of the mitral annulus were calculated; peak strain values of basal interventricular septum were also obtained.
Results: BMI was 26.9±4.6 in Group 1 and 35.7±5.2 in Group 2 (p>0.001). Traditional echocardiographic parameters showed no significant differences between the 2 groups, with the only exception of left ventricular mass; however, left ventricular mass index was similar in both groups. About TDI parameters, mean values of peak systolic and early diastolic velocities were significantly decreased in Group 2 (respectively 5.55±1.4 cm/s vs. 6.46±1.3 cm/s, p>0.01; 5.69±1.5 cm/s vs. 6.42±1.4 cm/s, p>0.05); mean values of peak late diastolic velocities were increased without reaching statistical significance in Group 2 (7.24±1.9 cm/s vs. 6.80±2.3 cm/s, p=0.08). About SI parameters, peak strain values of basal interventricular septum were also significantly decreased in Group 2 (18.24±3.2% vs. 21.12±2.9%, p>0.01).
Conclusion: In hypertensive pts obesity is related to a higher level of systo-diastolic left ventricular dysfunction. In our study, TDI and SI revealed and highlighted that even if obesity tends to cluster with hypertension, its presence is related to a significant worsening of the left ventricular dysfunction observed in hypertensive patients.
55 Elevated blood pressure in children of patients with premature coronary heart disease: relation to own and parental risk factors
MV Konnov; LM Dobordzhginidze; AD Deev; NA Nikolai Gratsiansky
Institute of Physico-Chemical Medicine Center for Atherosclerosis, Moskva, Russian Federation
Purpose: To elucidate associations between prehypertension (preHT) and/or hypertension (HT) in children of patients with premature coronary heart disease (onset before 55 years) and their own and parental risk factors.
Methods: We examined members of 219 families. There were 231 parents-probands aged 32–63 years and 278 their own children aged 5–36 years. In children aged =17 years we used definitions of HT and pre HT of the NHLBI 4-th report on diagnosis, evaluation, and treatment of high blood pressure (BP) in children and adolescents. In older offsprings we used JNC 7 criteria. In analysis of children aged =17 years HT and preHT were combined and designated “high BP”.
Results: High BP was found in 22/116 (19%) of children aged 5–17 years. According to logistic regression analysis high BP was independently associated with higher own body mass index (BMI) and smoking of proband: odds ratio (OR) of top tertile BMI (=21.2 kg/m) vs 2 bottom tertiles (>21.2 kg/m) was 6.73 (95% confidence interval [CI] 2.16–21.00; ?=0.001); OR of having smoking vs nonsmoking parent-proband was 1.65; 95% CI 1.01–2.70; ?=0.045. HT was found in 24/162 (14.8%) children aged 18–36 years. Independent significant own predictors of HT were fasting serum glucose, BMI and total cholesterol (TC). OR top vs bottom tertiles of plasma glucose (=5.03 and =4.5999 mmol/l), BMI (=25.3 and =21.4 kg/m) and TC (=5.25 and =4.3777 mmol/l), were 12.1 (95% CI 2.56–57.16; ?=0.002), 11.4 (95% CI 2.32–56.04; ?=0.003) and 6.48 (95% CI 1.58–26.51; ?=0.009), respectively.
Among characteristics of parent-proband heart rate (HR) and systolic (S) BP were independently significantly related to offspring HT: OR top vs bottom tertiles of HR (=76 vs =64/min) and SBP (=135.0 vs =116.55 mm Hg) were 4.51 (95% CI 1.34–15.20; ?=0.015) and 3.75 (95% CI 1.04–13.55; ?=0.043), respectively.
Conclusion: HBP and HT in children of patients with premature CHD were associated with own metabolic risk factors (BMI in both age groups, and fasting glucose and TC in adult children). Association of HT with parental elevated BP was found only on children older than 17 years.
56 Prevalence, treatment and control of hypertension in Portugal: insights of the VALSIM study
N Cortez-Dias; S Martins; A Belo; MM Fiuza
Portuguese Society of Cardiology, Lisbon, Portugal
Purpose: To estimate the prevalence of hipertension (HT) in the portuguese adult population, and to determine the overall and regional level of treatment and control in subjects followed in primary care setting.
Methods: Descriptive cross-sectional study (VALSIM Study) performed in a primary care setting representative of all regions of Portugal. Patients (pts)>18 years consulting their general practicioner irrespective of the reason for consulting, were asked to participate. After informed consent, a questionnaire was used to collect sociodemographic, clinical and laboratory data, and blod pressure (BP) was measured after a 5-minute seated rest. HT was defined as systolic BP (SBP)=140 mmHg or diastolic BP (DBP)=90 mmHg or use of antihypertensive medication (aHT). Multivariate regression analysis was used to estimate the odds ratio of HT and non-controlled HT by age, gender and region.
Results: A total of 16,333 pts were analised (59±14 years; 61% women). The age and sex-adjusted prevalence of HT was 43.4% (M:43.5%, F:43.25%). Prevalence rose with age in both sexes. In pts>70 years there was a male preponderance, but this trend was reversed in older pts. Geographical variation in HT prevalence was found: lowest in Azores (35.8%), highest in Alentejo (53.5%) and lower in litoral districts. Among the group of hypertensive pts, 78.6% were on aHT medication but only 37.5% had their BP controlled and 10.33% had SBP=180 mmHg or DBP=110 mmHg. The proportion of hypertensives under treatment was higher in women (M:77.2%; F:79.8; p>0.01) and had regional variation, highest in Azores (90.6%) and lowest in Madeira (63.7%). The proportion of pts receiving 1-, 2-, 3- and >3 aHT agents was 43.6%, 38.3%, 14.5% and 3.6% respectively. The most frequently aHT therapies used were: monotherapy with angiotensin receptor blockers (ARB, 15.7%), ACE-inhibitors (ACEI, 14.7%), diuretics (D, 5.8%), calcium chanel blockers (CCB,7.5%) ARB+D (12.6%), ACEI+D (12.4%) and ARB+D+CCB (3.7%). The proportion of uncontrolled HT was significantly higher in men (OR:1.14, p>0.001), older pts and in residents of Madeira (77.9%) and North region (70.1%). An inverse correlation was found between the proportion of uncontrolled HT by region and the probability of being treated with monotherapy in that region (OR:0.71; CI 95% 0.65–0.77), independently of the aHT classes most frequently used.
Conclusions: These results show that HT is highly prevalent and underscore the need to develop national strategies to improve prevention, detection and treatment, particularly in those regions where the proportion of uncontrolled HT is significantly higher.
57 Clustering of cardiovascular risk factors in prehypertension and hypertension in a Korean general population: Atherosclerosis risk of rural area in Korea general population (ARIRANG) study
M-S Ahn; JY Kim KH Lee; BS Yoo; SH Lee; JH Yoon; KH Choe; YJ Youn; SY Kim
Wonju Christian Hospital Dept of Cardiololy, Wonju, Korea, Republic of Wonju College of Medicine Yonsei University cardiology, Wonju Kangwondo, Korea, Republic of
Background and objective: Risk factors such as dyslipidemia, hyperglycemia, and obesity are more frequent in hypertensive than in normotensive subjects. Recognition that cardiovascular risk factors often cluster together has focused attention on the concept of total cardiovascular risk. Information regard to the associations between hypertension and cardiovascular risk factors in Korean general population is limited. We investigated the associations between hypertension and cardiovascular risk factors in Korean general population.
Methods: The study subjects were enrolled 6,191 Korean adult subjects (2,659 men, 3,532 women) from the five rural areas of the Korean genomic rural cohort (KGRC), an ongoing epidemiologic study conducted on a representative senior population. We excluded subjects with treatment of diabetes mellitus, hypertension, and hyperlipidemia. and We divided into three (normotension, prehypertension and hypertension) groups by JNC7. Cardiovascular risk factors were defined as smoking, abdominal obesity (waist circumference>90 cm in male, >85cm in female), low HDL-cholesterol (>40 mg/dL), high LDL-cholesterol (>160 mg/dL), diabetes mellitus (fasting blood glucose=126 mg/dL) and high CRP (>1 mg/dL). The metabolic syndrome (Mets) was defined according to the modified ATP III and IDF criteria.
Conclusion: Increasing blood pressure frequently clusters with other cardiovascular risk factors, such as obesity, diabetes mellitus and dyslipidaemiametabolic syndrome.
Risk facors according to blood pressure
N. of Additional
Normotension
Prehypertension
Hypertension p
risk (%)
(n=1238)
(n=2324)
(n=2329)
0
28.1
25.9
24.5
1
35.4
36.4
32.9
2
25.7
25.2
28.3
3
8.8
10.5
11.2
4
1.9
2.0
3.1
The clustering of risk factors with among study groups are shown table (P=0.001)
58 Obesity, metabolic syndrome and blood pressure control: insights of the VALSIM study
N Cortez-Dias; S Martins; A Belo; MM Fiuza
Portuguese Society of Cardiology, Lisbon, Portugal
Purpose: The aim of this study was to determine the prevalence of obesity and metabolic syndrome (MS) in patients (pts) with hypertension (HT) and to evaluate the relationship between obesity, abdominal obesity (AO), MS and blood pressure (BP) control.
Methods: Descriptive cross-sectional study (VALSIM Study) performed in a primary care setting representative of all regions of Portugal. Pts>18 years consulting their general practicioner irrespective of the reason for consulting, were asked to participate. HT was defined as systolic BP=140 mmHg or diastolic BP=90 mmHg or use of antihypertensive medication. Obesity was determined by body mass index (BMI): normal weight (NW: 18.5–24.9 kg/m2), overweight (OW: 25–29.9 kg/m2) and obese (OB: 30 kg/m2). AO was defined as waist circumference (WC) was greater than 102 cm in men and 88 cm in women. MS was defined by NCEP-ATP III criteria. Multivariate regression analysis was used to estimate the odds ratio of HT and non-controlled HT by age, gender, BMI, WC or MS.
Results: A total of 16,333 pts were analised (59±14 years; 61% women). The age and sex-adjusted prevalences were: HT 43.4% (M: 43.5%, F: 43.25%); MS 29.4% (M: 27.5%; F: 31.4%); OW 39.6% (M: 45%; F: 34.8%) and OB 26.7% (M: 25.3%; F: 28.4%). Both the prevalence of HT and MS rose with age in both sexes: in pts>70 years there was a male preponderance, but this trend was reversed in older pts. Obesity and AO were significantly more prevalent in women. When evaluating pts according to categories of BMI, greater levels of BP were found as weight increased (from 129.6/75.4 to 140.5/82 mmHg; p>0.001). The overall prevalence of HT among obese subjcts almost doubled that observed in NW population (NW: 41.1%; OW: 61.4%; OB: 74.4%). Likewise, HT prevalence was also increased among subjts with AO [70.6% vs 47%; p>0.001; OR 2.71, 95% confidence interval (CI) 2.54–2.9] or MS (75.7% vs 45.5%; p>0.001; OR 3.45, CI4.46-4.03), being high BP the most frequent MS component. On the other hand, the control of BP decreased as weight increased (BMI in controlled /uncontrolled HT was 29.1/29.6; p>0.001). Besides, AO and MS were also associated with worse control of BP (AO: OR 1.7, CI 1.58–1.84; MS: OR 1.93, CI 1.76–2.11).
Conclusion: These results show a strong association between obesity, AO, MS and HT, as well as between those cardivascular risk factors and BP control and therapeutic needs.ese results show that HT is highly prevalent and underscore the need to develop national strategies to improve prevention, detection and treatment, particullarly in those regions where the proportion of uncontrolled HT is significantly higher.
59 Effect of BMI on antihypertensive treatment: meta-analysis of 41625 observations
FA Allaert
University Hospital Medical Evaluation Dept., Dijon Cedex, France
Objective: Study the effect of BMI (Normal>25, overweight 25 to 30 and obese<=30) on the rate of blood pressure control by anti-hypertensives at >140 mmHg and >90 mmHg.
Material and methods: Meta-analysis of 9 identically designed observational studies conducted in general practice including an enrolment visit and a follow-up visit within 2 to 3 months following anti-hypertensive treatment. Given the large number of studies involved, antihypertensives prescribed alone or in combination reflect their overall use in general practice.
Results: The meta-analysis was performed on 41625 observations of patients aged 63±11 years of whom 55% were male. Of these, 54% were of normal weight, 26.3% were overweight and 19.7% were obese. Blood pressure parameters were SBP 162±11 mmHg and DBP 93±7 mmHg at enrolment and respectively 142±10 mmHg and 82±7 mmHg after 3 months of follow-up, for respective reductions of 21±12 mmHg and 11±8 mmHg and a normalization rate of 61.7%. The normalization rate did not vary as a function of sex but decreased significantly with age going from 69.9% before age 50 to 49.3% after age 80; and with BMI going from 63.7% in patients of normal weight to 61.1% in overweight and 56.7% in obese patients. After adjusting for weight and sex, logistic regression analysis highlights the independent role of weight, with an odds ratio of 87 [0.82; 0.92] (p>0.0001) for excess weight and 0.70 [0.66; 0.75] (p>0.0001) for obesity.
Conclusion: BMI, which is a recognized risk factor for hypertension, also appears statistically to limit the effect of antihypertensive treatment.
60 Nondippers have higher incidence of abnormal exercise blood pressure response cardiac and carotid structure diastolic dysfunction and metabolic profile in pre-hypertensive and hypertensive men
A Pittaras1; AJ Manolis2; JP Kokkinos3; V Kolovou2; A Giannelou2; A Papada2; PF Kokkinos1
1Athens, Greece; 2Asklipieion Voulas Hospital Cardiology, Athens, Greece; 3VA & Georgetown University Medical Centers Cardiology, Washington Dc, United States of America
Background: The increasing use of ambulatory blood pressure (BP) monitoring (ABPM) has uncovered the people with abnormal sleep-waking BP patterns called as nondippers and considered as of higher cardiovascular risk. Nondipper data related to exercise BP profile, left ventricular and carotid structural changes, diastolic dysfunction and metabolic profile in hypertensive and especially in pre-hypertensive men is limited.
Methods: We assessed left ventricular structure and diastolic function by echocardiography, carotid intima-media thickness (IMT) by carotid ultrasound, the exercise BP response by treadmill test (Bruce), the day-night BP variation by ABPM and metabolic profile by blood chemistry. We included 563 middle-aged men (51±11 yrs) free from heart disease, medication and smoking. Men who had less than a 10% drop in BP at night are referred to as nondippers (n=120). Men with SBP: 120–139 mmHg or DBP:80–89 mmHg are referred as pre-hypertensives (n=316).
Results: After statistical analysis for dippers and nondippers, the nondippers were older (54±8 vs 50±11, p=0.000), had increased left ventricular mass index (LVMI) (130±25 vs 122±29, p=0.015), the size of aortic root (p=0.000) and left atrium (p=0.05) as well as the IMT levels. Exercise BP response was increased in nondippers (SBP (p=0.000) and DBP (p=0.001). Nondippers had worse diastolic function [A wave (p=0.000), E/A ratio (p=0.001) and deceleration time (DT) (p=0.05)]. Nondippers had significantly worse metabolic profile (lipid, glucose and uric acid levels). Analysing the pre-hypertensives (n=316), again, all the above variables were less favourably different significantly for the nondippers (p=0.000).
Conclusion: Nondippers in pre-hypertensive and hypertensive men have higher incidence of abnormal exercise BP response, LV mass, carotid IMT, diastolic function and metabolic profile. This group represents a progressive increase in the cardiovascular risk for target organ damage and important clinical information especially in the pre-hypertensive population.
61 The association of orthostatic hypotension and medication use in the British women's heart and health study
S Kamaruzzaman1; H Watt2; C Carson2; S Ebrahim2
1London School of Hygiene & Tropical Medicine Non Communicable Disease Unit, EPH, London, United Kingdom; 2London School of Hygiene & Tropical Medicine Medical Statistics Unit, London, United Kingdom
Purpose: Antihypertensive drugs are widely used in the prevention of cardiovascular diseases but may have adverse side effects, particularly in older people. To determine the association between Orthostatic Hypotension (OH) and medication use, and the implications of polypharmacy in a community dwelling population of older women.
Method: The British Women's Heart and Health Study cohort comprises of 4286 women aged 60–79 years from 23 towns in Britain. Data was collected using nurse interviews, questionnaires and medical record reviews. Odds Ratio (OR) for OH was calculated using conditional logistic regression analyses, adjusted for town of residence and potential confounding factors such as age, disease variables, social class, smoking, body mass index excessive alcohol consumption and other medications. OH was defined as a drop of 20mmHg or more in systolic blood pressure and/or a drop of 10 mmHg in diastolic blood pressure. OH status was based on differences between the average of two sitting and two standing measurements, all taken at one minute intervals.
Results: The prevalence of OH is 18.6% (95% CI 17.4, 19.9) showing a significant trend with increasing age, diabetes and hypertension. OH was significantly associated (p>0.0001) with the number of medications taken, especially antihypertensive ones. This was seen with thiazide diuretic use as well as being on any blood pressure medication, in particular beta blockers, alpha adrenoceptor blockers and drugs affecting the renin-angiotensin system. There is a weak suggestion that women taking respiratory system drugs have an increased prevalence (14% vs. 11%, p=0.02)
The risk of OH is significant in those taking alpha adrenoceptor blockers after adjusting for confounding factors, OR 1.89 (95% CI 1.09, 3.25). In similarly adjusted odds of OH, taking beta blockers and respiratory system drugs both independently confer an approximate one third increase in the risk of OH with an OR of 1.37 (1.07,1.74) and 1.36 (1.02,1.81) respectively.
Conclusion: The prevalence of OH was moderately high in this population of older women, being greater among diabetics and hypertensives. There was an association between OH and number of drugs as well as type of drugs received, in particular antihypertensives. Prevention programmes should monitor adverse drug side effects, particularly in older people.
62 Arterial hypertension and myocardial infarction risk among truck drivers
V Malinauskiene; V Dulskiene; A Azaraviciene
Institute of Cardiology of Kaunas University Environmental Epidemiology, Kaunas, Lithuania
Purpose: Studies in Western societies have confirmed that professional drivers are at increased myocardial infarction (MI) risk, though the exact reasons have not yet been stated. The objective of our study was to investigate the effect of occupational and lifestyle risk factors on the risk of first MI among professional truck drivers.
Methods: We conducted a case-control study among men aged 25–64 who were residents in Kaunas in 1997–2000. We identified MI cases (n=448) from the MI hospital register and controls (N=1777) without clinical diagnosis of ischemic heart disease. We obtained information on potential MI risk factors through a personal interview using standardized questionnaires for both groups. We interviewed 60 truck drivers in the cases' group and 108 controls. We used the Swedish version of the demand-control questionnaire to assess the effect of job strain on first MI risk. We conducted the logistic regression analysis to evaluate the adjusted odds ratios for definite risk factors for truck drivers.
Results: We found that age-adjusted odds ratio of MI for truck drivers was 2.36; 95% CI 1.67–3.35. After adjustment for education, smoking, arterial hypertension and obesity the odds ratio of MI was 2.26; 95% CI 1.58–3.24. After adjustment for job strain it decreased to 1.8; 95% CI 0.96–5.22. The logistic regression analysis within the subgroup of professional drivers showed that the adjusted odds ratio of MI for arterial hypertension was 3.20; 95% CI 1.57–6.55. The adjusted odds ratio for smoking was 2.48; 95% CI 1.12–5.49; for job strain it was 2.91; 95% CI 1.23–6.98.
Conclusion: We found that occupational and lifestyle risk factors influence the increased risk of MI among truck drivers. Arterial hypertension showed a significant effect on first MI risk. Arterial hypertension regulation methods would be of importance in heath promotion strategies among truck drivers.
63 Prevalence, awareness, treatment and control of hypertension in a primary health care region
L Donmez; O Yasar; S Kantar
Akdeniz University Public Health Department, Antalya, Turkey
Aims: Control of the hypertension may decrease the mortality of CVDs in the population. Determination of the status of secondary preventive efforts (early detection and intervention) may contribute to solution of the problem. In this study, we aimed to determine the prevalence, awareness, treatment and control of hypertension.
Methods: Population based smaple of 120 people aged 40 years and older in a primary health care region in Antalya, selected by cluster sampling method. A questionnaire was performed and their blood pressures were measured. Hypertension was defined as “sistolic blood pressure (SBP)>140 and/or diastolic BP>90”.
Results: Thirtynine people were aware that they had hypertension. Of this hypertensive 39 people, 17.9% (7 people) were not being treated by antihypertensive medication. Of the 32 people who were being treated, 46.9% (15 people) were under controlled, but 53.1% (17 people) had high BP. Of the 81 people who has never recognized as hypertensive, 19.8% (16 people) had high BP. Overall hypertension prevalence was 33.3% (7+17+16=40 people).
Conclusion: Hypertension is a major public health problem in the study region. Some of people do not aware of their hypertension. Alhough some people aware of their hypertension, they are not being treated and/or are being treated uneffectively. Screening programmes may be useful to find new cases and performing the suitable treatment may decrease of the complications in the population.
64 Admission blood pressure predicts coronary anatomy but not outcome in hypertensive acute coronary syndrome patients
R Baptista; E Jorge; R Teixeira; C Negrier; N Antonio; S Monteiro; S Costa; P Monteiro; M Freitas; LA Providencia
University Hospital Cardiology Departement, Coimbra, Portugal
Backgound: There are few studies evaluating the effect of a previous his-tory of hypertension on the outcomes of an acute coronary syndrome (ACS).
Objective: To determine, in previously hypertensive patients admitted with an ACS, if those with high blood pressure at admission had poorer outcomes than those normotensive at admission.
Population and methods: A total of 1084 previously hypertensive patients admitted with ACS were studied and divided in two groups: A (normotensive at admission −365 patients) and B (hypertensive −719 patients). Prognostic variables were determined during admission and at discharge. All patients with shock were excluded.
Results: Group B patients were more often men (66.3% vs 33.7%, p>0.01). There were no differences regarding age, familiar history of cardiovascular disease, dyslipidaemia, smoking, previous myocardial infarction, coronary artery disease or congestive heart failure. Personal history of diabetes was associated with higher blood pressure at admission, with an odds ratio (OR) of 2.355 (p>0.001), as was female gender (OR 1.430 p>0.01), obesity (OR 1.612 p>0.001) and previous stroke (OR 2.534 p>0.001). Group B patients were more likely to receive beta-blockers (β-B) (OR 1.458 p=0.039), calcium channel blockers (OR 2.884 p>0.001) and ACE inhibitors (ACEi) (OR 2.632 p=0.001) on admission. On discharge, this trend is maintained, with the former receiving more β-B (OR 1.473 p=0.010) and ACEi (OR 1.629 p=0.005). Group B patients were also more likely to have a normal coronary angiogram (OR 1.685 p=0.035) and no significant stenosis (OR 1.685 p=0.035). No difference was found between groups regarding intra-hospital death and complication rates. At a mean 19-month follow-up, odds-ratios for adverse cardiovascular events and death were equivalent in the two populations.
Conclusion: In ACS patients previously hypertensive, admission blood pressure is a predictor of coronary anatomy, but is not a useful tool to predict in-hospital or post-discharge outcome.
65 Gender peculiarities of left-ventricular myocardium hypertrophy in patients with essential hypertension
E Myasoedova; S Myasoedova; TM Ndoumi
Ivanovo State Medical Academy Faculty therapy and occupational diseases, Ivanovo, Russian Federation
Purpose: To reveal specific factors affecting left-ventricular myocardium mass index (MMI) in women and men with essential hypertension (EH).
Methods: We observed 101 patients with EH aged 18 to 57 years: 63 women (mean age (±SD) 43.42±8.81 years) and 38 men (mean age (±SD) 40.18±10.51 years). Patients have no history of myocardium infarction, stroke or diabetus mellitus; individuals with inflammatory processes and abnormal erythrocyte sedimentation rates (ESR) were excluded from the study. All patients underwent echocardiography with subsequent MMI calculation. C-reactive protein (hsCRP), total cholesterol (TCh), triglycerides (TG) plasma level, concentration of desquamated endotheliocytes in plasma (DE), global antioxidant plasma activity (GAA), and ESR were assessed. Data are presented as mean ±SD.
Results: Though systolic and diastolic blood pressure levels were lower (p>0.05) in women than in men (149.18±13.36/94.75±9.63 mmHg and 159.6±21.52/99.54±11.44 mmHg, respectively), groups had equal frequency of left-ventricular myocardium hypertrophy and comparable MMI's. No distinctions in body mass index (BMI) were found between groups; however abdominal obesity prevailed in women (p>0.001). Smoking (p=0.009) was more frequent in men than in women. Men had higher SCORE index (p>0.001) than women. hsCRP, DE and GAA did not differ between the groups; TG levels were higher in women as compared to men (p>0.05).
Gender peculiarities were found to affect MMI in our EH patients: in men MMI correlated to ESR (r=0.56, p=0.01), hsCRP (r=0.48, p>0.001), GAA (r=0.646, p=0.02) and DE (r=0.65, p=0.03), in women – to age (r=0.45, p>0.01), EH anamnesis duration (r=0.44, p=0.001), BMI (r=0.41, p>0.001), waist circumference (r=0.48, p=0.002), TCh (r=0.29, p=0.03) and SCORE index (r=0.29, p=0.03). We found that age and waist circumference were significantly associated with MMI in women in a multiple regression model (adjusted R2=0.23), while ESR, GAA, hsCRP and DE were weighty in men cohort (adjusted R2=0.35).
Conclusion: The development of left ventricular myocardium hypertrophy in EH, evidently, has gender peculiarities. In women MMI is mostly affected by metabolic factors, while in men subclinical inflammation and endothelial dysfunction seem to be more influential. Thus, we confirm that gender peculiarities of left-ventricular mass increase should be considered in prevention and treatment of EH patients.
66 Correlation between left ventricular mass and extension of coronary disease in hypertensive patients
R Musetescu; E Belu; AE Musetescu; D Toader; A Gavrila; DD Ionescu
University Hospital Cardiology Department, Craiova, Romania; University Hospital, Craiova, Romania
Purpose: An increase in left ventricular mass (LVM) represents a compensatory response of hypertensive heart to augmented loading conditions. Risk factors such as: diabetes mellitus, dyslipidemia, obesity accelerate the increase of left ventricular mass (LVM) in patients with primary hypertension and therefore may contribute to the increase of cardiovascular morbidity and mortality.
The aim of this study was to measure LVM in hypertensive patients with coronary disease and the relationship with risk factors such as: diabetes mellitus, dyslipidemia and obesity.
Methods: We studied 36 hypertensive patients (20males and 16 females), aged between 36–72 years, whom were admitted for elective coronary arteriography by clinical examination, standard 12 ECG leads, echocardiography - left ventricular mass (LVM) was calculated using the formula 0.8[1.04(IVS+LVPW+LVDD)3-LVDD3]+0.6g, with IVS-interventricular septum, LVPW-left ventricular posterior wall, LVDD-left ventricular diastolic diameter. Risk factors were considered: diabetes mellitus by fasting plasma glucose>1266 mg mg/dl, dyslipidemia LDLC>1300 mg mg/dl,(>100 mg/dl for diabetic patients or with coronary heart disease), HDL<400 mg mg/dl, triglycerides>2000 mg mg/dl (>150 mg/dl for diabetic patients), obesity, BMI>30 Kg/m2.
Results: 1. Coronary lesions in hypertensive patients were present in 77.77%, 50% single vessel disease, 75% two vessel disease and 81.18 % three vessel disease. 2. In hypertensive patients with increased LVM>149 g in males and 125 g in females, coronary lesions were present in 85.71%, 53.84% in those with multivessel disease. 3. Correlation with risk factors: hypertensive patients with increased LVM had three coronary lessions in 78.26% when associated diabetes mellitus, 70.83% in those with dyslipidemia and 70% in in those with obesity.
Conclusion: 1. The ability to identify hypertensive patients at high risk for coronary heart disease may be improved through echocardiographic assessment of left ventricular mass. 2. Higher values were associated with the extent of coronary disease and well correlated with the presence of risk factors: diabetes mellitus, dyslipidemia and obesity.
67 Effectiveness of treatment in the elderly hypertensive patients with left ventricular hypertrophy and dyslipidemia
S Vatinian; S Gurgenyan; K Nikoghosyan
Institute of Cardiology Arterial Hypertension, Yerevan, Armenia; Institute of Cardiology, Yerevan, Armenia
Objective: Hypertension and dyslipidemia are common conditions, that both contribute synergistically to cardiovascular risk. Several anti-hypertensive drugs and statins have been shown to decrease the cardiovascular risk. The aim of this study was to evaluate the efficacy of two antihypertensive agents (ACE inhibitor perindopril with calcium channel blocker amlodipine) with or without statin (atorvastatin) in the elderly patients with essential hypertension and dyslipidemia.
Methods: Fifty eight elderly patients (30 males and 28 females, aged 65–77 years) with mild to moderate essential hypertension, left ventricular (LV) hypertrophy (LV mass index>125 g/m2 for men and>110 g/m2 for women) and dyslipidemia: total cholesterol (TC)>190 mg/dl, low-density lipoprotein cholesterol (LDL-C)>115 mg/dl were randomly assigned to perindopril 44 mg mg daily and amlodipine 55 mg mg daily (group A – 29 patients) or perindopril 44 mg mg daily and amlodipine 55 mg mg daily with atorvastatin 20 mg daily in combination (group B–29 patients). Echocardiography was performed at baseline and after 12 months of therapy. The parameters of LV hypertrophy were evaluated. LV mass, indexed by body surface area, was estimated according to Devereux with use of Penn Convention. TC was measured from fasting plasma samples obtained at baseline and at the end of the study. LDL-C was calculated by the Friedewald formula. Statistical comparisons were performed by 2-tailed Student's t test for quantitative parameters.
Results: Blood pressure was lowered in both groups to less than 140/90 mmHg. At the end of the study 44,8% patients with atorvastatin (group B) achieved the European TC goal of >190 mg/dl and LDL-C goal of >115 mg/dl. In the patients without atorvastatin (group A) TC and LDL-C were no significantly lower than at baseline (from 240.7±33,5.6 mg/dl to 228.4±23.11 mg mg/dl and from 153.5±15.8 mg/dl to 141.7±12.5 mg/dl, respectively, p=ns). At the end of the study LV end diastolic diameter and LV wall thickness significantly decreased in both groups. LV mass index reduced from 159.9±6.8 g/m2 to 138.7±3.1 g/m2 in group A (p>0,01) and from 161.8±7.6 g/m2 to 134.2±2.7 g/m2 in group B (p>0,001).
Conclusion: Statins may cause vasodilatation by restoring the endothelial dysfunction. So, simultaneous treatment of concomitant hypertension and dyslipidemia with antihypertensive drugs, wich preserves lipid metabolism, and statins is a highly effective strategy for the patients with high cardiovascular risk.
68 Blood pressure changes in systematicaly exercising middle-aged persons
J Svanishvili; N Chabashvili; Z Sopromadze; E Tataradze
Tbilisi State Medical University Medical Rehabilitation and Sports Medicine, Tbilisi, Georgia, Republic of
Purpose: The purpose of our study was to investigate effects of systematic physical exercises on blood pressure (BP) level changes in middle-aged persons.
Methods: BP changes were investigated on 50 to 60 years old individuals (156 females and 70 males) during four years. By the level of BP they were divided into three groups: I group included persons with normal BP (average value 125/72–130/75 mHg), II group – persons with high BP (average value 155/88–156/85 mmHg) and III group – persons with low BP (average value 99/66–98/67 mmHg). These groups were performing systematic physical exercises two or three times per week during four years. Investigated persons did not take any BP normalizing medications.
Results: Among persons who initially had normal BP no significant changes were obtained at the end of the study - systolic blood pressure (SBP) became 125±1.2 among females and 130±3.5 among males and diastolic blood pressure (DBP) became 76±0.7 among females and 76±1.7 among males. In hypertensive persons BP significantly decreased: SBP − 132±2.4 among females and 143±3 among males; DBP − 80±1.3 among females; 81±1.2 among males. In persons with hypotension BP reached physiological norm: SBP − 117±1.5 among females and 117±1.7 among males; DBP − 73±0.7 among females and 70±1.1 among males.
Conclusion: From the results of our study we can conclude that systematic physical exercises facilitate normalization of BP and therefore they should be used as one of the basic treatments in persons with hypertension and hypotension.
69 Changes of antihypertensive treatment compliance and blood pressure control in patients with arterial hypertension during the recent three years
PA Zelveian; KA Ordyan; GA Podosyan; AA Potosyan
Institute of Cardiology Preventive Cardiology, Yerevan, Armenia; Armenian Medical Association, Yerevan, Armenia
“Blood Pressure Screening and Survey in Yerevan Adult Population” study was conducted in 2004. A cross-sectional survey and screening were performed among 748 randomly selected subjects. In 2007 121 patients with arterial hypertension (HT) were selected by the method of proportions differences and undergone to re-screening.
Purpose: The aim of this study was to find out the changes in the antihypertensive treatment compliance and blood pressure (BP) control of patients with HT.
Methods: After obtaining informed consent of these patients, at home visit, trained interviewers measured their BP and interviewed them using friendly-constructed questionnaires. BP was measured according to ESC/ESH guidelines. Treatment was defined as regular use of anti-hypertensive medications. Successful BP control was defined as systolic BP (SBP) >140 mmHg and diastolic BP (DBP) >90 mmHg at the time of visit. The sample was divided into four groups depending on whether the subjects took antihypertensives in the past or not and whether they take them currently. 1st group: received antihypertensives in the past and continue to receive now, 2nd group: discontinued anti-hypertensive treatment, 3rd group: didn't take antihypertensives, but now take, 4th group: never receive antihypertensive treatment. The intergroup comparison was made between past and last BP mean values.
Results: In 2004 from the sample only 23 patients with HT received antihypertensive treatment (31%) and BP was controlled only in 39% them (12.2%). Due to re-screening results 45 patients received anti-hypertensives (60.8%), and of those being treated 44.4% were effectively controlled (27%). As shown in the table below the compared past and last BP mean±std values of 1st and 4th groups didn't significantly differ (p>0.05), meanwhile SBP of the 2nd and 3rd groups differ significantly (p>0.05).
Conclusion: The follow-up results show that during the past three years the compliance to antihypertensive treatment as well as the number of controlled hypertensives has increased twice.
2nd group
p
3rd group
p
SBP in 2004
132.2±17.2
0.01
159.7±20.3
0.03
SBP in 2007
138.1±17.3
147.3±20.5
DBP in 2004
81.2±5.7
0.32
94±13.4
0.18
DBP in 2007
84.2±4.1
90.6±12.7
70 Effect of a comprehensive multidisciplinary lifestyle modification program on blood pressure
A Ziv1; S Pintov2; Y Sandhaus1; D Keret1; O Vogel1; K Wolkomir1; S Efrati1
1Asaf Harofeh Medical Center Integrated Medicine, Beer Yakov, Israel; 2Soraski School of Medicine Public Health, Tel Aviv, Israel
Rationale: Elevated blood pressure is a result of environmental and genetic factors. Commonly used approaches such as the DASH diet address only some of the environmental factors. An educational self management approach encompassing a comprehensive multidisciplinary method which addresses diet, sedentary lifestyle, stress, social and habitual factors may improve blood pressure control. A diet low in protein and rich in whole grain rice which has been used in traditional folk nutrition to reduce blood pressure was used in this study.
Purpose: To Compare the effect on blood pressure of Comprehensive Approache to Lower Measured Blood Pressure (CALM BP), a patient self management educational program, to the Dietary Approaches to Stop Hypertension (DASH) recommendations.
Methods: A total of 49 outpatients with uncomplicated mild to moderate arterial hypertension were randomized to 16 weeks (2–4 hour weekly sessions) of either CALM BP program or DASH program. DASH program sessions included a 45 minute group walk, a 30 minute lecture including dietary instructions and a group meal. CALM BP program sessions included the above with an addition of a one hour relaxation session, one hour guided group discussion on stress management and a 10 minute audio CD used for a daily Qi Gong breathing meditation. Participants in both groups received educational manuals with daily lifestyle instructions and questionnaires which were reviewed weekly by the study staff. Ninety-two percent of the patients were receiving antihypertensive medication. Primary outcome measures were mean 24-hour ambulatory blood pressure levels after the intervention. Primary endpoint was defined as blood pressure dropping below 120 mmHg systolic or 80 mmHg diastolic for over two days. Measurements for all patients included 24-hour ambulatory blood pressure, weight, physical exam, blood work, arterial stiffness and were conducted at the beginning and at the end of the study.
Results: 45 patients completed the trial (24 with CALM BP, 21 with DASH). A total of 24 patients achieved the primary endpoint: 16 (66.7%) from CALM BP group and 8 (33.3%) from DASH group (P=0.032). These patients were instructed to reduce blood pressure medication due to symptomatic hypotension. The most significant blood pressure reductions occurred during weeks two and three of the intervention. At the end of the intervention period no significant differences in mean group blood pressure measurement were observed between the groups.
Conclusion: In the current study CALM BP program was significantly superior DASH program in reducing blood pressure medication.
71 Difference in clinical characteristics, self rated sleep and day-time sleepiness between hypertensive patients with or without risk of obstructive sleep apnoea -a pilot study in a primary care setting
A Brostrom1; A Stahlkrantz2; J Albers2; F Nystrom3; O Sunnergren4; F Uhlin5; E Svanborg6
1Clinical Neurophysiology, IMH Medicine and Health Sciences, Linkoping, Sweden; 2Pulmonary Medicine County Hospital Ryhov, Jonkoping, Sweden; 3Internal Medicine, IMH Medicine and Health Sciences, Linkoping, Sweden; 4Ear, Nose and Throat County Hospital Ryhov, Jonkoping, Sweden; 5Nephrology, IMH Medicine and Health Sciences, Linkoping, Sweden; 6Neuroscience and Locomotion, IKE Clinical and Experimental Medicine, Linkoping, Sweden
Introduction: Obstructive sleep apnoea (OSA) is a prevalent, but often undiagnosed health problem. OSA is linked to hypertension (HT), as well as increased cardiovascular (CV) morbidity and mortality. Studies have shown that long term CPAP (continuous positive airway pressure) treatment in patients with severe OSA can reduce risks for both fatal and nonfatal CV events. OSA still remains undiagnosed in many individuals. An early identification of individuals at risk of OSA can therefore be of great importance.
Purpose: To describe the prevalence of patients who suffers from high risk of OSA at a HT-clinic, as well as to compare how clinical characteristics, self-rated sleep and excessive daytime sleepiness (EDS) differs in HT-patients with or without high risk of OSA.
Method: A descriptive design was used. A total of 46 consecutive patients (40% men) with diagnosed HT (> 140/90), were enrolled from the registry (defined as having this diagnosis) in a primary care setting. Data regarding risk of OSA (Berlin sleep apnoea questionnaire), sleep and insomnia (Minimal insomnia scale), EDS (Epworth sleepiness scale) and clinical characteristics were collected during a visit at the clinic.
Results: A total of 72% of the included patients met the Berlin sleep apnoea questionnaires criteria to suffer from high risk of OSA. Patients with high risk of OSA reported higher prevalence of loud (p>0.01) and frequent snoring (p>0.0001), more complaints from others regarding snoring (p>0.0001), more witnessed apnoeas (p>0.05), and higher frequency of non restorative sleep (p>0.0001) compared to patients without high risk of OSA. No significant differences were found regarding systolic or diastolic blood pressure, total sleep time, EDS, BMI, neck circumference, waist hip ratio, levels of body fat, lipids-, creatinine-, or blood glucose levels between the groups.
Conclusion: This pilot study indicates that above 70% of all patients with HT at a HT-clinic might suffer from a high risk of OSA. Knowledge of how clinical characteristics differ between patients with or without high risk for OSA can help primary care physicians to identify patients at risk and may motivate to preventive interventions.
72 Efficiency of blood pressure control in type 2 diabetes mellitus suffered from hypertension
G Simonyi; JR Bedros; M Medvegy
Ferenc Flor Hospital Cardiometabolic Center, Kistarcsa, Hungary
Earlier investigation showed that in Hungary the effective blood pressure (BP) control about 30% of hypertensive patients. The European Society of Hypertension suggests that BP should be reduces to at least below 140/90 mmHg and to lower values, if tolerated, in all hypertensive patients. In cases of hypertension combined with diabetes mellitus target BP should be at least >130/80 mmHg.
Our aim was to determine the proportion of successful target BP among patients with diabetes mellitus.
Patients and methods: In this study for 4 years we investigated our in-patients to following parameters: gender, age, duration of diabetes (type 2) and hypertension, systolic and diastolic BP, calculated the mean arterial pressure (MAP) and pulse pressure (PP).
Results: In this period we investigated 4112 patients. Among this patients had 668 diabetes mellitus. All of them suffered from hypertension too. 432 women, age 68.33±11.31 (35–91) years. The mean duration of diabetes mellitus was 12.340±8.63 (1–42) years and the mean duration of hypertension was 12.68±8.73 (1–41) years. The systolic BP was 142.56±20.85 (102–206) mmHg, diastolic BP was 84.56±10.54 (62–124) mmHg. The MAP was 104.63±12.32 (73.33–147.67) mmHg and PP was 57.45±15.45 (20–110) mmHg. The successful rate of target BP (>130/80 mmHg) was only 19.56% (128 patients).
Conclusion: Our results showed that BP pressure control for majority of diabetic patients was unsuccessful. Because of hypertension and diabetes are relevant risk factors for cardiovascular events we need turn our attention to achieving target BP of these patients too.
73 Prognosis of acute STEMI treated with primary PCI in patients with Metabolic Syndrome/Insulin Resistance Syndrome
Z Babic1; M Pavlov1; N Bulj1; M Weber2; V Nikolic-Heitzler2; V Mitrovic1
1UH Sestre milosrdnice Coronary Care Unit, Zagreb, Croatia; 2Kerckhoff Klinik Cardiology Departement, Bad Nauheim, Germany
Purpose: American Association of Clinical Endocrinologists (AACE) and American College of Endocrinology (ACE) published in 2003 the definition of Metabolic Syndrome/Insulin Resistance Syndrome as modification of mostly used NCEP ATP III and WHO definitions. The definition recognised some limitations of two previous definitions and expanded it with associated disorders and individuals considered at risk. Using AACE/ACE definition authors evaluated prognosis of acute STEMI treated with primary PCI in patients with Metabolic Syndrome/Insulin Resistance Syndrome.
Methods: 395 patients who suffered acute STEMI and were treated with primary PCI in Kerchoff Klinik have been divided in two groups (with or without Metabolic Syndrome/Insulin Resistance Syndrome) and compared according to their prognosis. The prognosis was evaluated using intrahospital reinfarction, re-PCI and mortality rate, as well as MACE (restenosis, reinfarction, cardiac and non-cardiac rehospitalisation, mortality, CABG and CVI rate) during follow-up. The analysis was performed using Pearson Chi-Square and Fisher's Exact Test in SPSS for Windows 15 program.
Results: The average age of investigated patients was 63.0 years, 70.3 % of them were male, they were hospitalized between March 31st 2003 and April 3rd 2005, follow-up was made six months after initial hospitalization. 192 of them fulfilled criteria for Metabolic Syndrome/Insulin Resistance Syndrome and they had higher incidence of MACE in general (30.9 vs. 28.3 %), intrahospital reinfarction (1.0 vs. 0.5%), as well as cardiac re-hospitalisation (28.1 vs. 25.9 %), restenosis (19.3 vs. 13.3 %), mortality (6.3 vs. 6.2 %) and CVI (1.6 vs. 0.5 %) during follow-up. 193 patients who did not fulfill this criteria had higher incidence of intrahospital mortality (0.5 vs. 0.0 %), as well as reinfarction (1.6 vs. 0.5%), non-cardiac re-hospitalisation (6.7 vs. 5.2 %) and CABG (5.7 vs. 5.2 %), during follow-up. None of these differences reached statistical significance.
Conclusion: Using AACE/ACE definition for Metabolic Syndrome/Insulin Resistance Syndrome authors did not find significant influence of this syndrome on prognosis in six month period of time of patients who suffered acute STEMI and were treated with primary PCI.
74 Is an invasive strategy useful in women with non-ST acute coronary syndrome?
R Paiva Cardoso Teixeira1; C Lourenco2; R Baptista2; E Jorge2; N Antonio2; S Monteiro2; S Costa2; P Monteiro2; M Freitas2; LA Providencia1
1Coimbra, Portugal; 2Coimbra University Hospital Cardiology Departement, Coimbra, Portugal
Background: Previous investigators have reported gender differences in the management of patients with acute coronary syndrome (ACS). The majority of trials comparing an invasive strategy with a conservative one for the management of unstable angina (UA) and non ST elevation myocardial infarction (NSTEMI) have demonstrated a benefit for men. Nevertheless, in females results have been conflicting and no consensus has yet been settled.
Purpose: To assess the impact of an invasive versus a conservative strategy in the in-hospital outcome in women admitted for UA/NSTEMI.
Material and methods: Retrospective analysis of 347 female patients admitted to a single coronary unit between May 2004 and July 2007. Patients were divided in 2 groups, group A (n=197) - conservative strategy; and group B (n=150) - invasive strategy.
Results: Group A was older (74.49±10.15 vs 66.23±11.62, p>0,001), had higher incidence of type 2 diabetes (36.2 vs 23.6%, p=0.029), atrial fibrillation, and received more diuretics during hospital stay. Patients in this group also had significantly higher inflammatory markers, lower creatinine clearance (50.7±32.8 vs 63.1±35.3, p>0.001), decreased ejection fraction (52.83±9.59 vs 56.65±8.29, p=0.001) and shorter hospital stay (4.6±2.4 versus 5.2±2.6, p=0.017).
Group B had more previously known coronary heart disease (71.1 vs 59.3%, p=0.023), presented more often on Killip class I (84.6 vs 70.1, p=0.002), had lower TIMI risk scores, received more anti-platelet therapy and at discharge were more often on B-blocker and dual anti-platelet therapy. There were no differences between groups concerning previous medications and cardiac biomarkers. The type of strategy used in this population did not significantly influence in-hospital mortality, morbidity and readmission rates, which were similar in both groups.
Conclusion: Our results support the hypothesis that women may not benefit as much as men from an invasive strategy in the setting of an UA/NSTEMI. Long-term follow-up of this population will enable us to determine the long-term outcome of both these groups. In the meantime, adequate risk/benefit evaluation is critical in both male and female patients to ensure optimization of short and long-term prognosis after an ACS.
75 Are we treating the right non-ST acute coronary syndrome patients with an invasive strategy?
R Paiva Cardoso Teixeira1; R Baptista2; C Lourenco2; N Antonio2; E Jorge2; S Monteiro2; S Costa2; P Monteiro2; M Freitas2; LA Providencia2
1Coimbra, Portugal; 2Coimbra University Hospital Cardiology Departement, Coimbra, Portugal
Background: In addition to medical therapy in the acute setting of unstable angina (UA) or non ST acute myocardial infarction (NSTEMI), revascularization plays an important role in determining prognosis. Nevertheless there is still debate over the benefit of an invasive versus conservative strategy in the short and long-term UA/NSTEMI outcome.
Purpose: To compare in-hospital outcome of an invasive versus a conservative strategy in the setting of UA/NSTEMI.
Materials and methods: Retrospective analysis of 1103 patients admitted to a single coronary unit between May 2004 and July 2006, with UA/NSTEMI. Patients were divided in 2 groups: A (n=528) - conservative strategy; B (n=575) - invasive strategy.
Results: Group A patients were older (71.28±11.52 vs 63.46±11.30, p>0.001), more frequently female (37.3 vs 26.1%, p>0.001), diabetic (31.2 vs 25.6%, p=0.044), with more frequent past history of acute myocardial infarction and atrial fibrillation. They also presented with lower creatinine clearance, hemoglobin, lower ejection fraction (50.47±11.04 vs 54.67±9.98, p>0.001) and higher inflammatory markers and were more frequently treated with ACE inhibitors and diuretics before admission. The in-hospital mortality was significantly higher on this group (5.9 vs 1.9%, p=0.001).
Group B had more smokers, more frequent history of percutaneuos coronary intervention, higher total and LDL cholesterol, presented with lower Killip class and lower TIMI scores. They were more frequently treated with anti-platelet therapy and at discharge were more often on B-blocker and dual anti-platelet therapy.
There were no differences between groups regarding body mass index, cardiac biomarkers, in-hospital complications and hospital stay.
Conclusion: Despite some imbalances between groups, in our population invasive strategy decreased in-hospital mortality. This result reinforces the need for proper clinical evaluation at hospital admission, in order to define the best therapeutic strategy for each UA/NSTEMI patient.
76 Gender-based therapy discrimination in acute coronary syndromes
N Antonio; NS Monteiro; C Lourenco; R Teixeira; R Baptista; E Jorge; P Monteiro; L Goncalves; M Freitas; LA Providencia; Coimbra, Portugal
Purpose: Previous investigators have reported gender differences in the management of patients with acute coronary syndromes, but the impact of these differences on prognosis remain unclear. Our aim was to assess gender differences in management and outcome in patients with non-ST-elevation ACS (NSTE-ACS).
Methods: Prospective, observational study of 449 patients consecutively admitted for NSTE-ACS, in a single coronary care unit with 1 year follow-up. Patients were divided in two groups: females (n=161) and males (n=288). We compared demographic characteristics, treatment and 1-year outcomes between groups.
Results: Women were significantly older with worse renal function but presented a shorter in-hospital duration of stay. Regarding risk factors, women had higher rates of hypertension but were less frequently smokers (Table 1). Women were less submitted to coronary angiography (40.4% vs 58.7%; p>0.01) and received less drug eluting stents (14.3% vs 30.9%) compared to men. Females had more often normal coronary arteries (29.2% vs 14.8%, p>0.05). At discharge, they were undertreated in terms of beta-blockers (79.5% vs 84.4%, p>0.05) and clopidogrel (31.1% vs 50.3%, p>0.05). There was no significant gender differences neither in in-hospital mortality nor in re-infarction rates at 1-year. However, women tended to have a higher mortality at 1-year (19.0% vs 10.5%, p>0.078).
Conclusion: NSTE-ACS women are older and have more co-morbid illness, being less likely to receive evidence-based therapies. This may explain their worse 1-year outcome and should lead to a reinforcement in the use of evidence-based strategies in NSTE-ACS women.
Women
Men
P
Age (years)
71.5±11.2
66.0±11.4
>0.01
In-hospital stay (days)
5.0±2.4
5.6±3.0
>0.05
Creatinine Clearance (ml/min)
56.1±33.0
70.2±34.7
>0.01
Hypertension
85.2%
75.4%
>0.05
Smoking Habits
5.0%
15.7%
>0.01
NSTEMI/UA
79.1%/20.9%
73%/27%
n.s.
GP IIb/IIIa inhibitors
43.5%
56.3%
>0.01
Baseline characteristics.
77 Glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: does age make any difference?
CN Lourenco; R Teixeira; N Antonio; S Monteiro; S Costa; F Goncalves; P Monteiro; L Goncalves; M Freitas; LA Providencia
Coimbra University Hospital Cardiology, Coimbra, Portugal
Purpose: Age is a major determinant of outcomes in the setting of acute coronary syndromes (ACS), although community studies reveal a significantly lower use of cardiovascular medications among elderly patients. Glycoprotein (GP) IIb/IIIa inhibitors reduce the acute ischemic complications but the risk of bleeding may also be increased with these agents, particularly in elderly patients. Furthermore, limited trial data is available to guide the care of older adults and outcome is unknown, particularly with newer medications. The aim of this study was to compare in-hospital outcome of elderly patients who were treated or not with intravenous GP IIb/IIIa antagonists.
Methods: Retrospective analysis of 515 patients hospitalized for ACS, aged over 75. Patients were divided in two groups: A (n=354) or B (n=161) if they were treated or not with IIb/IIIa antagonists.
Results: Group A patients were younger (79.91±3.29 vs 81.66±4.45Y, p>0.001), had higher TIMI score, higher troponin I and ApoA levels, were more often treated with inotropics agents during hospitalization and had higher incidence of minor bleeding (hemoglobin drop 3–5 g/dl) (22.0 vs 10.8%, p=0.008). They also had a lower incidence of cerebrovascular or peripheral arterial diseases, nephropathy, recent hospitalization for heart failure, previous treatment with diuretics and were discharged more often on ezetimibe and oral antidiabetics. There were no differences between groups regarding gender, cardiovascular risk factors, Killip class, type of ACS or coronary anatomy, in-hospital treatment other than GP IIb/IIIa antagonists or inotropics agents, creatinine levels, ejection fraction, platelets levels or weight. Furthermore no differences were found regarding incidence of major bleeding (4.0 vs 1.7 %, p=0.249), hospital stay or in-hospital outcome (complications − 14.8 vs 10.3 %, p=0.148; mortality − 11.8 vs 12.4 %, p=0.840). Multivariate analysis showed that GP IIb/IIIa antagonists use was the only independent predictor of minor bleeding (p=0.011, OR=2.501).
Conclusion: In this elderly population GP IIb/IIIa antagonists use was associated with minor bleeding with no impact on outcome in a short term. Because of this similar outcome between the two groups and lack of benefits of these agents in reducing ischaemic events in this population, this study questions the need for GP IIb/IIIa antagonists use in a high risk elderly population. Further studies with longer follow-up are needed to determine the risk/benefit ratio of these agents in the elderly.
78 Can the creatinine clearance predict bleeding complications in acute coronary syndrome patients?
N Antonio; C Lourenco; S Monteiro; R Teixeira; E Jorge; F Goncalves; P Monteiro; L Goncalves; M Freitas; LA Providencia; Coimbra, Portugal
Background: Renal dysfunction is directly associated with a high cardiovascular mortality in acute coronary syndrome (ACS) patients and it is also frequently associated to other bleeding risk factors, like diabetes, ageing and several clotting disorders. Data of the impact of renal dysfunction on bleeding complications and ACS outcomes are sparse, since in most trials renal dysfunction is an exclusion criteria, so that patients with kidney disease are under-represented.
Purpose: To assess the impact of creatinine clearance (CrCl) at the time of hospital admission on bleeding complications and short-term prognosis after an ACS.
Methods: Retrospective analysis of a database containing 1552 consecutive patients admitted to a single coronary care unit for ACS (May 2004 to July 2006). CrCl values were available in 65% of patients. This population (n=1009) was stratified by quartiles of admission CrCl: Q1, >44 ml/min; Q2, 44–64 ml/min; Q3, 64–87 ml/min; Q4, =87 ml/min. Demographic and clinical characteristics, medication use, and in-hospital outcomes were compared for patients within the different quartiles of creatinine clearance.
Results: Patients with renal dysfunction were older, more likely to be women and presented to hospital with more comorbidities (heart failure, hypertension, diabetes, atrial fibrillation) than those with normal renal function. Patients in Q1 tended to have a significantly lower body mass index, lower admission haemoglobin, LDL cholesterol and triglycerides. Patients with worse renal function received less IIb/IIIa inhibitors, clopidogrel and aspirin; nonetheless they showed significantly higher rates of in-hospital bleeding complications (haemoglobin drop>3 g/dl) (Q1:17.5%; Q2:10.4%; Q3:13.7%; Q4:8.9%, p>0.05). In-hospital mortality was also significantly higher in patients with lower levels of CrCl (Q1:10.8%; Q2:5.6%; Q3:2.4%; Q4:2.1%, p>0.001). In univariate analysis, female gender, age =57.5, BMI =28.3, diabetes mellitus, hypertension, Killip class>1, LVEF =49.5 %, heart rate =78.5 and CrCl =48.5 ml/min were associated with higher bleeding complications. However, in a multivariate analysis the only independent predictors of in-hospital bleeding were female gender and diabetes.
Conclusion: The risk of major bleeding episodes increases as renal function worsens in ACS patients. However, in our study, CrCl could not be identified as independent predictor of in-hospital bleeding. These data reinforce the importance of optimal risk/benefit management in ACS patients, especially in patients with high bleeding risk, like older diabetic females.
79 Bleeding complications in acute coronary syndromes patients: predictors and outcomes
CN Lourenco; R Teixeira; N Antonio; S Monteiro; S Costa; F Goncalves; P Monteiro; L Goncalves; M Freitas; LA Providencia
Coimbra University Hospital Cardiology, Coimbra, Portugal
Purpose: Bleeding is the most frequent non-ischaemic complication observed in the management of acute coronary syndromes (ACS) and several studies have shown a strong impact on prognosis. Can we identify the patients more prone to have this complication and prevent their poor outcome? The aim of this study was to find predictors of bleeding complications and to analyze their in-hospital outcome, among an ACS population.
Methods: Retrospective analysis of 1141 patients hospitalized for ACS. We analyzed both the occurrence of minor (hemoglobin drop 3–5 g/dl-n=151) and major bleeding (hemoglobin drop>5 g/dl-n=28). When compared with patients without this complication, those with minor bleeding presented more often with ST elevation myocardial infarction, left anterior descendent (LAD) stenosis, higher myocardial necrosis markers, C-reactive protein, fasting glucose; they were treated more often with levosimendam and glycoprotein IIb/IIIa inhibitors (32.7vs22.8%,p=0.029), had longer hospital stay (6.6±4.7 vs 4.9±2.8days, p>0.002) and higher heart rates. Moreover, they had lower platelets, left ventricular ejection fraction(55.38±18.2 vs 60.66±16.28%, p=0.010) and lower creatinine clearance (60.7±41 vs 66.8±35.6 mL/min, p=0.03) and they were less likely to have normal coronary anatomy. There were no significant differences between the two groups regarding in-hospital outcomes. Multivariate analysis showed that previously known coronary artery disease (p=0.043, OR=0.585) and LAD stenosis (p=0.049; OR=1.744) were the only independent predictors of minor bleeding. When comparing patients with major bleeding with those with less important bleeding we found that the first group was more obese (69.2 vs 49.6%, p=0.048), had higher myocardial necrosis markers, C-reactive protein, fasting glucose and maximum creatinine (2.6±1.7 vs 1.6±1.22 mg/dl, p>0.001) levels, lower platelets, required more often IIb-IIIa inhibitors (42.9 vs 23.8%, p=0.045) and levosimendam, had longer hospital stay (6.7±4.3 vs 5±3.1 days, p=0.021), higher in-hospital complications (26.9 vs 4.8%, p>0.001) and mortality (17.9vs6.0%, p=0.027) rates.
Conclusion: Bleeding occurred in more severe disease requiring more often aggressive treatment including IIb-IIIa inhibitors, in renal failure and glucidic dysmetabolic patients. Although minor bleeding had not impact on outcome, major one was associated to a dismal in-hospital outcome. Every effort should be made to early identify this higher risk patients and to prevent this complication by choosing the safer drug and by using it in appropriate dosages for the shortest time possible, according to risk/benefit evaluation.
80 Effect of rapid access chest pain clinic a target led tariff attracting service on service delivery to angina patients
AO Molajo1; CE Metcalfe2
1Royal Albert Edaward Infirmary Cardiology, Wigan, United Kingdom; 2Royal Albert Edward Infirmary Informatics, Wigan, United Kingdom
Introduction and Purpose: The Angina Specialist Nurse Service (ASNS) was established in 2000 to provide an open access service for patients with established angina (EA) in between clinic attendance and to support non cardiologist physicians when patients with acute coronary syndrome with non ST elevation (NSTEMI) and unstable angina (UA) are admitted under their care. The Rapid Access Chest Pain Clinic (RACPC) is a target led government initiative set up in 2002 for the early diagnosis and management of patients with new onset chest pain; patients with known angina were excluded. It attracts a special tariff and has a two-week time limit from referral to attendance. Patients from the RACPC were also referred to the ASNS. There was no increase in the staffing of the ASNS with the introduction of this new service.
Methods: Data on 5205 patient episodes of EA and RACPC were analysed to measure: 1. Referral patterns to the ASNS from 2000 to 2006. 2. Readmission up to 30 days, up to six months and up to 12 months. 3. The Influence of source of initial referral (RACPC and EA) to the ASNS on readmission rates from 2000–2006.
Results: Data for assessed variables were available in 96% of patient episodes. Referrals to the ASNS were 350, 264, 279, 222, 314, 345 and 279 from 2000 to 2006 respectively. Of these 350, 264, 183, 86, 175, 164, and 124 were patients with EA. In 2000 350 of 686 (52%) patients with EA were referred to the ASNS compared to 124 of 815 (15%) in 2006. Readmissions with NSTEMI and UA in these patients were 20%, 22% 12%, 17%, 7%, 6% and 2% from 2000 to 2006.
96, 136, 139, 181, and 155 patients were referred to the ASNS from the RACPC. Readmissions rates in these patients were 3%, 2%, 6%, 3% and 4% from 2002 to 2006 respectively. In 2002, 96 of 686 (14%) RACPC patients was referred to the ASNS. In 2006, 55 of 815 (7%) were referred.
Conclusion: 1. The ASNS reduced readmission rates in patients with angina.
2. Patients with EA are at high risk of readmission.
3. Readmission rates are low in RACPC patients with new onset chest pain.
4. With increasing referral of RACPC patients to the ASNS less of the patients with EA are being referred to the service.
5. The competing demand for the ASNS of the low risk RACPC patients may reduce access from the patients with EA who have a higher risk for readmission.
81 Pre-treatment with statins reduced cardiovascular complications in acute coronary syndrome diabetics with heart failure
ES Azenha Balhau Jorge; R Baptista; R Teixeira; C Negrier; N Antonio; S Monteiro; S Costa; P Monteiro; M Freitas; LA Providencia
Coimbra, Portugal; University Hospital Cardiology Department, Coimbra, Portugal
Background: Previous studies have suggested possible cardio-protective effects of statins beyond lipid lowering. Their utility in diabetic patients with heart failure admitted with acute coronary syndrome (ACS) is less well known.
Objectives: To determine, in a group of diabetics admitted with ACS and with systolic heart failure (LVEF>40%), if those previously treated with statins differ from patients who were not, regarding epidemiological profile, clinical presentation and prognosis.
Methods: A total of 51 consecutive diabetic patients with LVEF>40% admitted with ACS were evaluated. Clinical follow-up was available for 40 patients (78.4%), with a mean duration of 18 months. Patients with follow-up were then divided in two groups: A - not previously taking statins (26 patients − 51.0%) and B - already medicated with statins on hospital admission (25 patients − 49.0%).
Results: There were no significant differences between the two groups in age, gender, family history, smoking, and stroke. Personal history of hypertension, myocardial infarction, coronary artery disease, previous PCI, were more frequent in diabetics previously treated with statins. These patients were more likely to receive ACE inhibitors, β-blockers, nitrates and aspirin. No difference was found between groups regarding intra-hospital and follow-up mortality. However, clinical follow-up showed that diabetics previously with statins therapy have a significantly lower incidence of cardiovascular complications than diabetics not previously taking statins (33.3% versus 68.2%, p=0.028).
Conclusion: Although with worse risk profile, ACS diabetic patients with LV dysfunction previously treated with statins have a significantly lower complication rates during follow-up period. However, the two groups do not differ in intra-hospital mortality, maybe due different etiology of deaths (probably heart failure for intra-hospital mortality and coronary heart disease for long term outcomes).
82 Trends in survival following an acute myocardial infarction in the UK in relation to changes in prescribing of evidence-based medication in primary care
S Hardoon1; P Whincup2; I Petersen2; A Islam2; S Capewell3; R Morris2
1University College London Primary Care and Population Sciences, London, United Kingdom; 2St George's, University of London Division of Community Health Sciences, London, United Kingdom; 3University of Liverpool Division of Public Health, Liverpool, United Kingdom
Purpose: To investigate recent time trends in post 28-day survival following a first myocardial infarction (MI) and to examine the role of changes in prescribing of relevant medication in these case-fatality trends.
Methods: Data came from The Health Improvement Network (THIN), a representative UK-wide longitudinal primary care database comprising regularly updated data on patient diagnoses and prescriptions. Data from 219 general practices covering a period from 1991 to 2004 were used. First-MI patients were identified from medical diagnoses. Those patients who were alive at least 28 days after the MI were included (n=14548). Medication use was determined from prescriptions recorded in the six months following the MI. The extent to which trends in prescribing of medication could explain post 28-day survival rates was estimated by combining estimates of the trends in use of the different medications and trend in case-fatality following the MI over the 14 year time period with trial evidence on the effectiveness of the medications.
Results: The case-fatality rate in the first year following an MI, given survival to 28 days, fell by 3.1% per annum, corresponding to a decline of 35%, 95% CI (20 to 49), over the 14 years from 1991 to 2004. Meanwhile, prescribing in the first six months following an MI increased significantly: lipid-lowering drugs increased from 3.3% of patients receiving treatment in 1991 to 91.6% in 2004; odds ratio per annum increase in calendar time: 1.72 (1.68 to 1.75), beta-blockers increased from 29.4% of patients in 1991 to 75.1% in 2004; odds ratio 1.21 (1.19 to 1.22), ACE inhibitors increased from 13.8% to 83.8%; odds ratio 1.31 (1.29 to 1.32), and anti-platelet drugs increased from 48.7% to 92.2%; odds ratio 1.21 (1.20 to 1.23). Based on a relative risk of 1-year case-fatality in MI patients of 0.89 from trial data, the increase in prescribing of anti-platelet drugs over the 14 years is consistent with a 5% decline in case-fatality and can therefore statistically explain approximately 14% of the 35% case-fatality decline. Similarly, lipid-lowering drugs explain approximately 30%, ACE inhibitors explain approximately 32% and beta-blockers explain approximately 32% of the decline.
Conclusions: One-year case-fatality rates in patients surviving at least 28 days after a first MI have declined by approximately one third in 14 years. Much of this decline might be attributed to the considerable increases in primary care prescribing of evidence-based medications to MI patients, in particular lipid-lowering drugs, beta-blockers and ACE inhibitors.
83 Variations between 230 hospitals in gender differences in statin prescribing after myocardial infarction - The Myocardial Infarction National Audit Project (MINAP)
JL George1; R Chen1; A Timmis2; G Feder3; S Eldridge2; H Hemingway3
1University College London Epidemiology and Public Health, London, United Kingdom; 2Barts and the London NHS Trust Cardiology, London, United Kingdom; 3Queen Mary University of London Unit of General Practice and Primary Care, London, United Kingdom
Background: It is not known to what extent individual hospitals vary in the underuse of secondary prevention medication by gender.
Purpose: To determine the nature and extent of hospital variation between all acute hospitals in one country in gender differences in statin prescribing on discharge following MI.
Methods: 180,138 patients (33.2% female), aged 35–94, admitted between 01 Jan. 2003 and 31 Dec. 2006 with a final diagnosis of ST segment elevation Myocardial Infarction (STEMI) (44.5%) or non-STEMI as recorded in the UK Myocardial Infarction National Audit Project (MINAP). The main outcome measure was odds ratios (OR) for prescribed statins in women compared to men for each of the 230 acute hospitals in England & Wales.
Results: When all hospitals were analysed together, we observed lower use of statins in women; OR 0.85 (95% CI 0.83–0.87), as has widely been reported in the literature. However, this aggregated analysis concealed wide variability between hospitals, with hospital-specific ORs ranging from 0.13 (0.03–0.64) to 1.71 (0.89–5.54). The funnel plot was symmetrical with a similar number of hospitals lying above and below the 95% control limits (See Figure).
Conclusions: Prescribing of statins in women compared to men varied substantially between hospitals. As hospitals provide a locus for accountability and performance management, factors affecting hospital variation in receipt of evidence-based care demand investigation.
84 Pre-treatment with statins improves outcome in acute coronary syndrome patients with heart failure
ES Azenha Balhau Jorge1; R Baptista2; R Teixeira2; C Negrier2; N Antonio2; S Monteiro2; S Costa2; P Monteiro2; M Freitas2; LA Providencia2
1Coimbra, Portugal; 2University Hospital Cardiology Departement, Coimbra, Portugal
Background: Previous studies have suggested possible cardio-protective effects of statins beyond lipid lowering. Their utility in the setting of heart failure remains uncertain.
Objective: To determine, in a group of patients admitted with acute coronary syndrome (ACS) and with systolic heart failure (LVEF>40%), if those previously treated with statins differ from patients who were not, regarding epidemiological profile, clinical presentation and prognosis.
Methods: A total of 142 consecutive patients with LVEF>40% admitted with ACS were evaluated. Clinical follow-up was available for 107 patients (75.0%), with a mean duration of 18 months. Patients with follow-up were then divided in two groups: A - not previously taking statins (n=67) and B - already medicated with statins on hospital admission (n=40). RESULTS: There were no significant differences between the two groups in age, gender, family history, hypertension, smoking, personal history of diabetes mellitus and stroke. Personal history of dyslipidaemia, myocardial infarction, coronary artery disease, PTCA, CABG and recent hospitalization were more frequent in patients previously treated with statins. These patients were more likely to receive ACE inhibitors, β-blockers, nitrates and aspirin. No difference was found between groups regarding intra-hospital death and complication rates. However, clinical follow-up showed that patients previously on statins were more likely to survive an ACS (OD 0.225; p=0.004) - figure 1. Multivariate analysis also showed that age>70 y and Killip class at admission>1 were independent predictors of mortality during follow-up (c-statistic 0.822).
Conclusion: Although with worse risk profile, ACS patients with LV dysfunction previously treated with statins have a significantly better medium-term outcome.
85 Effect of glycemic control at the acute phase on later onset of left ventricular enlargement after myocardial infarction
J Tomono; H Adachi; H Tsurugaya; J Murakami; S Oshima; K Taniguchi
Gunma Prefectural Cardiovascular Centre Div. of Cardiology, Maebashi, Gunma, Japan
Background and Purpose: Hyperglycemia during acute phase of myocardial infarction (MI) is reported to result in poor prognosis. Although, onset of left ventricular remodeling is regarded as one of the predictive parameters of poor prognosis, the relationship between acute management of glycemic control and left ventricular enlargement (LVE) in these patients is not well studied. We quantified the relationship between the glycemic control during intensive care unit (ICU) stay and the left ventricular enlargement at the chronic phase.
Methods: Consecutive 20 anterior acute MI patients with successful reperfusion therapy since April 2007 were enrolled. Blood sugar (BS) level at the 2nd day of admission into ICU was regarded as a parameter of acute phase glycemic control. Left ventricular end diastolic diameter (LVEDD) was measured at the acute phase (within 3 days post-AMI) and at the chronic phase (4–6 months later) by echocardiography.
Results: Mean BS level in ICU was 179.5±75.66 mg/dl varying from 1000 mg/dL to 4344 mg/dL. LVEDD increased significantly (16.6±22.8%, p>0.01) from 44.6±6.00 mm in acute phase to 51.3±6.55 mm at the chronic phase. Increasing ratio of LVEDD was positively related with glycemic control in acute phase (r=0.44). Both the thickness of Intraventricular septum (IVST) and posterior wall thickness (PWT) decreased at the chronic phase as comparing with acute phase (IVST: 11.0±1.9 vs. 10.1±2.33 mm, p>0.05, PWT: 10.7±1.9 vs. 10.1±1.55 mm, p>0.05).
Conclusion: It was revealed that the left ventricular enlargement at the chronic phase is enhanced as the glycemic control is poor at the acute phase in patients with acute myocardial infarction. Tight BS level control at this phase is important to prevent the left ventricular remodeling.
LVDD increase vs. Plasma Glucose
86 Global risk factors management one year after acute coronary syndrome: the GIANINA survey
G Galuscan; JL Georges; S Gardenat-Leboidre; G Gibault-Genty; L Stefas; JJ Maspoli; J Schwob; B Livarek
Hopital Andre Mignot Cardiology, Le Chesnay, France
Purpose: Secondary prevention is a key strategy for reducing levels of coronary heart disease, but a gap between guidelines and practice remains. The aim of this double-part survey was to evaluate the improvement in secondary prevention 1 year after acute coronary syndrome (ACS) in real life, between 1999 and 2005.
Methods: Two surveys of almost similar design were performed in 1999 and 2005. In each survey, unselected consecutive patients (pts) suffering from ACS (N=112 hospitalized in 1998, and N=110 in 2004) were evaluated at admission, and 1 year after hospitalization, for the risk factors, lifestyle, and achievement of therapeutic goals recommended by the most recent guidelines. Follow-up (FU) data were obtained by mail and phone contact with patient, general practitioner and cardiologist, and medical laboratory when appropriate.
Results: (∗p>0.05; ∗∗p>0.0001). At 1-year FU (N=192 survivors with FU), smoking cessation (87% in 1999 vs 89% in 2005) and obesity (body-mass index>30 kg/m, 13% vs 19 %, resp) did not vary significantly. Blood pressure was controlled (>140/90 mmHg, excepted in diabetics in 2005 >130/80 mmHg) in 65 vs 80%∗, and was associated with an increased use of antihypertensive drugs (Beta-Blockers 52% vs 75%∗∗, ACE inhibitors or ARB 17% vs 64%∗∗). The goals for LDL cholesterol were achieved in 47% of pts in 1999 (>3.444 mmol/L) and in 76% in 2005 (>2.666 mmol/L)∗∗. Use of statin therapy (59% vs 87%∗∗) and statin dose-regimen also increased. The rate of pts with normal fasting glycemia (>777 mmol/L) decreased from 1999 to 2005 (90% vs 81%), despite increased use in antidiabetic drugs (4% vs 34%∗∗). In 2005, HbA1C was measured in 64% of the diabetic pts, but the goal (HbA1C>6.5%) was achieved in only 29%.
Mean number of controlled risk factors was 3,96±1,52 in 1999 vs 4,94±1,83 in 2005∗∗, and prevalence of pts with> 5 controlled risk factors at 1 year increased from 15% to 44%∗∗.
Conclusions: These results, drawn from unselected consecutive patients managed in real life, demonstrate an improvement in secondary prevention 1 year after ACS, between 1999 and 2005, despite strengthened guidelines for blood pressure and LDL cholesterol levels. Control of obesity and diabetes remains unoptimal.
87 Angiotensin II receptor 1 blockade reduces lipoprotein-induced AT1 expression and oxidative stress
H Morawietz; RA Catar; G Muller; C Goettsch; CG Ziegler; AW Krug
University of Technology Dresden Dept. Vasc. Endothelium And Microcirculation, Dresden, Germany
Purpose: Cardiovascular risk factors like oxidized low-density-lipoprotein (oxLDL) and angiotensin II (Ang II) can increase formation of reactive oxygen species in endothelial cells. However, interactions of both risk factors and impact of AT1 receptor blockade on lipoprotein-induced oxidative stress and endothelial function is currently not well understood.
Methods and Results: In this project, impact of native and oxidized LDL (nLDL, oxLDL) on Ang II receptor expression and formation of reactive oxygen species was analyzed in primary cultures of human umbilical arterial endothelial cells (HUAEC). Native and oxLDL (25–100 g/mL) induced already after 1 h AT1 (100 g/mL, nLDL: 329±69%, oxLDL: 366±56%, P>0.05 vs. control) and AT2 (100 g/mL, nLDL: 185±36%, oxLDL: 275±12%, P>0.05 vs. control) receptor mRNA expression in HUAEC. Increased AT1 and AT2 mRNA expression could also be observed after 3 for up to 24 h. These findings were confirmed by Western blotting. Both lipoproteins increased intracellular AT1 receptor immunofluorescence in HUAEC. Native LDL and oxLDL activated MEK/ERK and p38 MAPK pathways (ELISA, western blot) in HUAEC. Furthermore, oxLDL induced the oxLDL receptor LOX-1 and toll-like receptor 4 expression in HUAEC (RT-PCR, western blot). Induction of both Ang II receptors by oxLDL could be reduced by preincubation with AT1 receptor antagonist candesartan. OxLDL induced in contrast to native LDL superoxide anion formation in HUAEC (chemiluminescence). AT1 receptor blockade prevented lipoprotein-induced oxidative stress in HUAEC like SOD. This was not mediated by regulation of expression of major endothelial NAD(P)H oxidase subunit Nox4. In murine aortic rings, oxLDL-induced vascular superoxide anion formation was reduced by AT1 blockade. Furthermore, AT1 blockade prevented impaired endothelial function (increase of log EC50 values and impaired max. relaxation by oxLDL measuring acetylcholine-induced relaxation in phenylephrine-preconstricted vessels).
Conclusion: Augmented vascular oxidative stress and endothelial dysfunction in response to lipoproteins involves induction of the AT1 receptor. Our data suggest a novel vasoprotective mechanism of AT1 receptor blockade in hypercholesterolemia.
88 ACE inhibitors in the therapeutic regimens of patients with cardiovascular diseases
N Gotcheva1; B Georgiev1; V Baytcheva1; D Gotchev2; D Avramov2; M Vasseva-Hazan2
1National Heart Hospital, Sofia, Bulgaria; 2Military Medical Academy, Sofia, Bulgaria
Over the past years, ACE inhibitors (ACE-i) became the most widely used medication. Large clinical studies made them a class of first choice in the treatment of hypertension, HF and in the prevention of target organ damage. Some large studies confirmed the advantages of their use in patients with coronary heart disease (CHD).
The aim of the present study was to evaluate the preferences to use ACE inhibitors in the treatment of hypertension, CHD, heart failure (HF), and for cardio-vascular (CV) prevention.
Materials and methods: In 2007, using an anonymous questionnaire, we evaluated the preferences for cardioprotective therapy among 259 GPs taking care of 65717 patients with CVD, 45 out-of-hospital cardiologists for their 20 101 CVD patients, and 77 in-hospital specialists treating patients with CVD. The study is a part of the project named BULPRAKT HEART study.
Results: GPs' preferences were as follows:
In the treatment of hypertension, 95% of GPs used ACE-i; in patients with CHD, ACE-i were used by 78% of them; in HF patients, ACE-i were used by 88%; and for CV prevention 91% of GPs used ACE inhibitors. Enalapril is the most commonly used ACE inhibitor.
The preferences of out-of-hospital specialists were as follows:
In the treatment of hypertension, 89% of physicians used ACE-i; in patients with CHD, ACE-i were used by 67% of them; in HF patients, ACE-i were used by 67%; and for CV prevention 89% of physicians used ACE-i. Enalapril is the most commonly used ACE-i, except for HF patients, for which lisinopril is more commonly preferred.
The preferences of in-hospital physicians were as follows:
In the treatment of hypertension, 96% of physicians used ACE-i; in patients with CHD, ACE-i were used by 80% of them; in HF patients, ACE-i were used by 87%; and for CV prevention 91% of physicians used ACE-i. Enalapril is the most commonly used ACE-i.
Conclusion: ACE inhibitors are the most widely used drugs for prevention and treatment of CVD. Within the class, enalapril was the most commonly used. Their usage of ACE-i is most common in the treatment of hypertension, followed by the treatment of HF and in target organ protection. Although the indications for use in CHD were not very clear, a substantial proportion of the physicians included them in the wide therapeutic regimen for patients with CHD. Physicians included predominantly enalapril and not ACE-i with evidence for CV advantages from large trials. There is a need of a better clarification of the preventive effects of the class, as well as a clear delineation of their protective effects beyond blood pressure control.
89 Secondary prevention of coronary artery disease (CAD) by lipid lowering therapy: treatment status with respect to target values in the disease management program (DMP) CAD North Rhine
B Hagen1; I Schwang2; R Griebenow1; L Altenhofen3; W Hass2
1Zentralinstitut DMP - Projektbuero, Koeln, Germany; 2Krankenhaus Koeln-Merheim Medizinische Klinik II der Universitaet Koeln, Cologne, Germany; 3Zentralinstitut DMP-Projektbuero, Cologne, Germany
Aim: Current guidelines recommend an LDL cholesterol of >1000 mg/dl (2,666 mmol/l) for the secondary prevention of CAD. The DMP leaves all treatment decisions at the discretion of the treating physician, who has to participate in a structured survey with feedback of the data (of his own vs. all patients) at regular intervals. We have analyzed whether age, gender, morbidities and prescription rates are correlated with the levels of LDL cholesterol achieved in the DMP.
Results: By the end of June 2007 108.559 patients with proven CAD have been included into the DMP CAD, of whom in 73.509 patients values of LDL cholesterol have been documented: age=70±10 years, female 35%, arterial hypertension 79%, myocardial infarction 37%, diabetes mellitus 34%, lipid disorders (unclassified) 68%, percutaneous coronary intervention (PCI) 39%.
Conclusion: Independent from whether target values for LDL cholesterol are achieved or not there are no clinically relevant differences between age and gender groups and in the subgroups of patients post MI, with diabetes or prior PCI. Prescription rates for statins are associated with age and gender and are higher in those achieving target values for LDL cholesterol.
Results and treatment patterns
Women
Men
Age (years)
=55
=76
=55
=76
LDL cholesterol=1000 mg/dl (I, a)
83±14
83±14
81±15
81±15
n
559
3.038
1.877
5.169
LDL cholesterol>1000 mg/dl (II, a)
137±32
140±32
134±29
132±27
n
954
7.571
2.947
7.338
Post myocardial infarction (I)
84±12
83±14
81±15
81±15
Post myocardial infarction (I)
131±29
137±31
132±27
131±26
Diabetes mellitus (I)
81±16
81±16
78±17
79±15
Diabetes mellitus (II)
133±31
139±32
135±30
133±29
PCI (I)
84±13
82±14
81±15
81±15
PCI (II)
131±32
137±30
132±28
130±27
Lipid lowering drugs (I, %)
77,3
73,9
86,8
78,3
Lipid lowering drugs (II, %)
61,3
52,0
76,7
58,9
Except for age, n and lipid lowering drugs all data given as mean±1 standard deviation, a:=2,58666 mmol/l.
90 Association of age and gender with the treatment patterns of patients with coronary artery disease (CAD): results from the disease management program (DMP) CAD North Rhine
B Hagen1; I Schwang2; R Griebenow1; L Altenhofen2; W Hass2
1Zentralinstitut DMP-Projektbuero, Cologne, Germany; 2Krankenhaus Koeln-Merheim Medizinische Klinik II der Universitaet Koeln, Cologne, Germany
Aim: The DMP defines a set of consented treatment targets (for blood pressure etc.), leaving the treatment decision free to the treating physician, who has to participate in a structured survey with feedback of the data (of his own vs. all patients) at regular intervals. Participation is voluntary but honored for by the health insurance companies. By the end of June 2007 108.559 patients with proven CAD have been included. We have analyzed in how far age and gender are correlated with the treatment strategies and the extent to which the treatment targets are achieved.
Conclusion: Prognostically important medications are significantly less often prescribed in female and/or elderly patients. Prescription behavior for platelet inhibitors and ACE inhibitors is stronger associated with gender than with age of patients. Age is stronger associated with the prescription of beta blockers and lipid lowering drugs.
Results and treatment patterns
Women
Men
Age (years)
=55
=76
=55
=76
n
2.312
16.782
6.932
18.857
Hypertension
66,8
84,3
67,6
80,0
Post myocardial infarction
34,0
28,3
46,1
40,2
Sys. blood pressure=140 mmHg
21,7
37,6
21,9
32,3
Beta blockers (BB)
77,2
69,5
84,6
73,9
ACE inhibitors (ACE-I)
54,5
62,4
64,1
65,8
LDL cholesterol>1000 mgmg/dl (a)
63,1
71,4
61,1
58,7
Lipid lowering drugs
63,7
55,6
78,7
64,5
NYHA II-IV
32,3
44,1
38,2
47,5
NYHA II-IV, BB + ACE-I
70,4
50,5
76,6
53,0
Platelet inhibitors
76,2
79,5
87,1
84,9
Except for age and n all data given as %, a:=2,58666 mmol/l; NYHA, New York Heart Association heart failure class.
91 Stable angina pectoris: comparison of trends in symptoms and diagnosed cases of angina from 1991 to 2003 with trends in MI mortality
A Aitsi-Selmi; M Shipley; H Hemingway
University College London Epidemiology and Public Health, London, United Kingdom
Background: It is unclear from current data whether the prevalence of angina follows the same trend as MI mortality. We compare time trends in the prevalence of angina symptoms and diagnosed cases of angina from 1991 to 2003 with MI mortality.
Methods: Five national cross sectional samples. N=70,206 responders (mean response proportion 72%); n=2,131 angina cases identified using the standardised seven item Rose angina questionnaire. National mortality data were used to analyse time trends in MI mortality. Age adjusted coefficients and standard errors of change in the log odds per year were calculated. Outcomes measured were prevalence of i) angina symptoms measured using the Rose questionnaire; ii) self-reported diagnosis of angina; and mortality from MI (ICD-9 code 410; ICD-10 code I21-22).
Results: Over the twelve year period the prevalence of angina symptoms declined from 3.6% to 2.5% (age adjusted annual percentage decline −3.4% [−2.0%, −4.8%] in women and −4.2% [−2.6%, −5.8%] in men). The rate of decline did not differ by age, ethnicity or social class. The rate of decline was much lower (by about half, p>0.001), compared to that observed for MI mortality (age adjusted annual percentage decline −7.3% [−7.0%, −7.5%] in women and −8.1% [−7.0%, −7.5%] in men). The prevalence of angina diagnosis did not change during the same period, nor did the percentage of Rose cases diagnosed.
Conclusion: Over a twelve year period, the prevalence of diagnosed angina remained constant, and angina symptoms showed a much lower rate of decline compared with MI mortality. This has implications in terms of a shift in emphasis in service provision and research into aetiological factors from MI to angina.
Trends in stable angina, 1991–2003
92 Preventive cardiovascular risk strategies based on interaction between occupational medicine and primary care
M Cabrera; E Calvo; MA Sanchez; A Garcia; A Fernandez; M Ruiz; JC Sainz; C Fernandez-Labandera; A Galvez; J Roman
Ibermutuamur Proyectos Sanitarios, Madrid, Spain
Introduction and aim: Workers are young and “healthy” people, with low use of health services and scarce prevention programs for them. During the routine medical check-ups workers were informed about their cardiovascular risk profile and healthy cardiovascular lifestyle measures. They were also given a letter to their General Practitioner (GP) to report on the worker's risk level. Telephone surveys were performed to evaluate the workers degree of awareness of the recommendations given and the extent of lifestyle changes. The present study was aimed to assess the interaction between the Occupational Medicine preventive measures and the Primary Care follow-up.
Materials and methods: Three telephone surveys with structured questionnaires, on the 1st, 4th, and 8th month after the checkup, were performed on 3,085 moderate/high cardiovascular risk workers.
Results: First call showed that 67.81% (n=2.092) subjects were smokers, 86.74% (n=2.670) had read the preventive recommendations; 71.35% (n=2.116) knew some of their cardiovascular risk factors (48.51% high blood pressure, 57.96% dislipidemia, 39.73% smoking, 6.69% diabetes, 14.52% obesity, 1.82% previous cardiovascular disease), 30.90% (n=951) workers knew their cardiovascular risk level. 6.86% workers (n=211) tried to quit smoking during the first month and 13.16% (n=405) over the next six months. 37.23% (n=1.146) had not this intention. 5.43% workers (n=167) gave up smoking and 17.35% (n=534) remained non-smokers. 49.77% workers (n=1.532) gave the letter to the GP, with the result of: 29.01% (n=893) diet advise, 9.2% (n=283) antihypertensive treatment prescription, 9.3% (n=286) lipid lowering treatment, 0.94% (n=29) antidiabetic treatment, 0.36% (n=11) antiplatelet treatment, and 1,88% (n=58) antitobacco treatment. Nineteen cardiovascular events occurred (3 of them were mortal). Second call showed that 21% (n=104) workers gave up smoking and 1% (n=6) workers with the intention of giving up smoking had achieved it at the time of the third call.
Conclusion: There was a good level of knowledge about their cardiovascular risk amongst workers; half of interviewed workers informed their GPs, who prescribed therapeutic treatments and healthy cardiovascular lifestyle measures. Preventive synergy actions between Occupational Medicine and Primary Care contribute to an early, and effective, cardiovascular risk prevention.
93 The evaluation of secondary students' knowledge about cardiovascular diseases, their risk factors and prevention possibilities
A Kusiak; P Palacz; L Klima; P Kusak; D Czarnecka; Krakow, Poland
Introduction: The ESC guidelines from 2007 regarding the prevention of cardiovascular diseases aim at assisting those at low risk of CVD to maintain this state lifelong, and to help those at increased total CVD risk to reduce it. At the ACC congress in 2006 the attention was drawn to the fact that the prevention should also be applied to groups of children and young people.
Objective: The objective was to raise young people's awareness of cardiovascular diseases, their risk factors and prevention possibilities.
Methods: We have prepared a presentation addressed to Polish students of I and II form of secondary schools (16-17-year olds). Before and after the presentation, 419 students have filled in a questionnaire which was composed by us and consisted of questions connected with cardiovascular diseases, their risk factors and prevention possibilities.
Results: Before the presentation, 67% of the respondents have indicated heart diseases as the most common cause of death; after the presentation, the number has risen to 96% (p>0.01). The number of respondents identifying LDL cholesterol as the substance escalating atherosclerosis has reasonably risen (52% vs 88%, p>0.01). After the presentation, 99% of the respondents were able to determine healthy person's level of blood pressure correctly (before 88%, p>0.01). The number of respondents defining the heart attack correctly has risen by 13%, and indicating anaerobic exercises as the form of exercise the least profitable for the circulation system by 24%.
Conclusion: The level of Polish secondary students' knowledge about cardiovascular diseases, their risk factors and prevention possibilities is good. But is is also vital to improve and supplement this knowledge. It is important to create new educational programmes addressed to this particular age group.
94 Repeated education of patients with II-IV FC CHF: results of 2-year follow-up
GP Arutyunov; AV Evzerikhina; Moscow, Russian Federation
Patient education generally follows a certain schedule including several contacts between physician and patient and dispensing of training materials to patients. The degree of learning and its effect on clinical condition of patients remains unclear.
Purpose: Evaluating the effect of repeated education after 12 months of follow-up on therapy compliance and number of visits to clinic.
Methods: Study included 80 patients with II-IV FC CHF randomized to a group of traditional education or a group of interactive training and control of knowledge (28 and 42 patients). All patients had CHF of ischemic genesis and received a standard therapy. Patients of the first group received a standard therapeutic education including 3 lessons 40 minutes each before discharge with subsequent outpatient follow-up. In the second group situational tasks and interactive testing were used in addition n to the standard education. After 12 months of follow-up, group 2 patients were additionally divided into two subgroups (A and B). Follow-up of subgroup A was continued, whereas subgroup B underwent repeated training (3 lessons 40 minutes each). All patients received literature containing methodical recommendations. Testing was performed every 3 months and on study completion.
Follow-up period lasted for 24 months. Knowledge survival (10-score scale), compliance to the standard drug therapy, rate of hospitalization, and rate of visits to clinic were evaluated in all groups.
Results: Baseline assimilation of knowledge was scored 8.7 and 9.2 respectively, in both groups; at one year of follow-up, assimilation of knowledge was significantly lower (4.5 vs. 7.5 in group of active education). When subgroups of group 2 were compared after 24 months of follow-up, knowledge survival was significantly higher in subgroup B (8.1 vs. 6.7 in subgroup A). Compliance to treatment was also significantly higher in group 2 than in group 1 (90% vs. 60% respectively) at 12 months and in subgroup B than in subgroup A (91% vs 82% respectively) at 24 months. Number of visits to clinic reduced in both groups after 12 months to 1.1 (not signif) in group 1 and to 0.35 in group 2 (?>0.05). After 24 months the number of visits to clinic increased to 0.8 per month in subgroup A and remained unchanged (0.35 per month) in subgroup B. After 24 months, number of visits to doctor's office increased from baseline to 1.8 per months in group 1.
Conclusion: Education of patients repeated every 12 months increases survival of knowledge. Degree of knowledge survival is significantly related with compliance to therapy and number of visits to clinic.
95 Are CVD prevention programmes “value for money”? Modelling the cost-effectiveness of the “keepwell” programme (Scotland)
K Lawson
University of Glasgow Research Fellow, Glasgow, United Kingdom
Purpose: The Scottish government launched a national pilot programme of CVD preventative care called ‘Keep Well', in 2006. This programme is aimed at socio-economically deprived patients aged 45–64, who are considered at high risk of a CVD event. While there is a significant evidence-base regarding specific CVD prevention interventions, there is a lack of research into the cost-effectiveness of prevention programmes as a whole, which can consist of multiple, diverse and simultaneous interventions. Given limited public resources and competing demands for funding, it is increasingly necessary to demonstrate “value for money.” As part of an evaluation of Keep Well, we are developing an appropriate cost effectiveness model. In addition to establishing the cost-effectiveness of the Keep Well programme, the model aims to develop a case for the collection of follow-up patient data, which is not currently planned.
Methods: To project the effectiveness of Keep Well we draw upon peer-reviewed literature to estimate the likely reduction of CVD events over a 10-year horizon. Results will then be extrapolated to estimate total life years gained, and increased longevity will be adjusted for morbidity to produce a “Quality Adjusted Life Year” (QALY). Programme costs will be collated, together with cost changes resulting from differences in CVD events. Costs and benefits associated with Keep Well will be compared to the counterfactual of no prevention programme to generate an incremental cost/ QALY (ratio). This can be compared with other medical interventions to assess whether Keep Well is relatively good “value for money” and should be rolled out nationally.
There is likely to be significant uncertainty regarding the cost-effectiveness of Keep Well. To reduce uncertainty, “Value of Information” techniques will be used to determine the potential worth of further research, to identify key information gaps. This will allow the estimation of the potential value associated with the collection of follow-up patient data. This value can be compared with the cost of collecting this data to determine if this could be an efficient use of research resources.
Results and Conclusion: Preliminary results will be presented at the conference. Key issues include the functional form used to capture the complexity of Keep Well. The study will illustrate and make recommendations for the use of cost-effectiveness modelling for CVD prevention programmes.
96 How are coronary heart disease policies made? A qualitative study of the role of scientific evidence in decision-making
D Taylor-Robinson; B Milton; F Lloyd-Williams; MO Flaherty; S Capewell
University of Liverpool Division of Public Health, Liverpool, United Kingdom
Purpose: To explore the role of scientific evidence in the decision-making processes that inform coronary heart disease (CHD) policy-making.
Methods and Design: Qualitative study using semi-structured interviews. Participants: 33 CHD policy and decision makers purposively sampled from the UK National Health Service (at national, regional and local level), academia and voluntary organisations. Analysis: FRAME-WORK analysis using N-VIVO software. Interviews were transcribed, coded and emergent themes identified.
Results: Few participants described linear decision-making processes which follow pre-determined stages. Most participants described a more complex, even ‘chaotic' policy-making process. Scientific evidence was just one factor affecting decisions. The ability of decision-makers to respond to scientific evidence was often limited by a number of factors: short time frames and horizons for decision making; the pre-determined nature of health service spending patterns; and the lack of robust tools for synthesising disparate sources of information at different population levels. Some participants described the ways in which scope for innovation or responsiveness to evidence was ‘at the margins'. Some participants highlighted the difficulty of advocating for primary prevention due to the perceived lack of evidence of effectiveness. Political influences were described as especially important.
Conclusion: Significant barriers limit the application of evidence in the decision-making process. Evidence is just one of many factors that influence CHD policy and commissioning. However, an increased understanding of these processes may facilitate the development of tools to better support evidence-based decision-making to improve population health.
97 The health knowledge of persons suffered from diabetes: do they have better knowledge on prevention?
A Piwonska1; W Piotrowski1; W Bielecki2; K Kozakiewicz3; J Gluszek4; U Biela5; T Zdrojewski6
Purpose: Insufficient knowledge of CVD risk factors (RF), unawareness of diseases and their complications cause the significant limitation of prevention effectiveness. The group of persons suffering from diabetes is still growing all around the world. We evaluated the awareness of own CVD RF and the knowledge concerning hypertension (HT) and CVD prevention methods in persons with diabetes.
Methods: Data came from the polish population sample − 14769 persons (6977 men and 7792 women), aged 20–74, screened in 2003–2005. We analyzed how many persons were familiar with their blood pressure (BP), body mass (BM), HT complications and CVD prevention methods and prepared a health knowledge score.
Results: Out of screened persons 489 of men (7%) and 459 of women (6%) had diabetes. Persons with diabetes, both men and women, were significantly older, more often suffered from coronary artery disease (CAD), hypertension (HT) and hyperlipidemia (HLP). Out of persons that said they knew their BM, about 50% of men and women gave their BM exact to 2 kg and majority correctly classified their BM as normal or overweight/obesity (there were no significant differences between diabetic and non-diabetic persons). There was a difference between diabetic and non-diabetic persons in knowledge on their actual BP and ability to classify it to the normal or high category (diabetic persons more often classified their BP correctly). In general, persons with diabetes had better knowledge on complications of untreated HT (especially men). The most often mentioned HT complications were stroke and myocardial infarction. The knowledge on prevention methods was worse in diabetics or did not differ significantly between persons with and without diabetes. Higher physical activity, smoking cessation and healthy life style were the most often mentioned prevention methods. In general, health knowledge of diabetic was better than knowledge of non-diabetics men (score 1.87±1.26 vs 1.73±1.19, p=0.0374). In women population there was the opposite situation (score 1.89±1.20 vs 2.12±1.23, p>0.0001).
Conclusion: Knowledge concerning awareness of risk factors, hypertension complications and CVD prevention methods was insufficient in persons with diabetes. Diabetic persons had better knowledge on hypertension complications and did not differ in the knowledge on prevention methods than the rest of the population.
98 Octogenarians undergoing cardiac surgery: long-term outcome and quality of life
A Viana Tejedor; FJ Dominguez; M Moreno; L Pena-Conde; P Salinas; A Sanchez-Recalde; S Jimenez-Valero; R Moreno; E Lopez De Sa-Areses; JL Lopez-Sendon; Madrid, Spain
Background: The increase in life expectancy in western countries in the last decades has resulted in a significant gradual increasing number of octogenarians referred for cardiac surgery. Since health care resources are limited, there is a need for critical evaluation of the long-term surgical outcome and quality of life in the elderly. The aim of this study is to identify the factors influencing perioperative outcome in octogenarians and to determine mid and long term survival and the quality of life after cardiac surgery.
Methods: We evaluated 150 patients aged 80 years and over who underwent cardiac surgery at our institution in the last 26 years. We analyzed clinical and epidemiological variables included in the European System for Cardiac Operative Risk Evaluation (EuroSCORE), in-hospital morbidity and mortality, mid and long survival and quality of life after cardiac surgery.
Results: Mean age was 82.7±2.5 years and 72 (48%) were men. Fifteen patients (12.6%) were in NHYA functional class I, 21 (17.6%) in class II, 48 (40.3%) in class III and 35 (29.4%) in class IV prior to surgery. Thirty-three patients (36.3%) underwent emergent surgery, 70% of them due to a postinfarction ventricular rupture. The 30-day mortality rate was 27.5%, with a mean hospital stay of 16.5 days (13–27). Emergent procedure, NYHA functional class IV, chronic renal failure and previous myocardial infarction were independent predictors of in-hospital mortality. Mean follow up was 72.2±9.9 months with survival rates of 87.3% after one year and 57% after 5 years respectively. Late postoperative quality of life in our 53 long-term survivors was significatively better than prior to surgery. NYHA functional class improved from 2.52 to 1.48. Most survivors (97.7%) confess personal feelings of performance in age-and role-specific activities and feel satisfied with present quality of life.
Conclusions: Cardiac surgery in octogenarians is associated with increased in-hospital mortality rate and longer hospital stay. Our findings support that cardiac surgery can be performed in a selected elderly population with good long term survival and quality of life.
99 Prevalence of overweight and obesity in iron-deficient Iranian adolescent girls
MH Eftekhari1; H Mozaffari-Khosravi2; F Shidfar3
1Shiraz University of Medical Sciences Schoopl of Health, Nutrition Department, Shiraz, Iran (Islamic Republic of); 2Shahid Sadougi university of Medical sciences Nutrition, Yazd, Iran (Islamic Republic of); 3Iran university of Medical sciences Nutrition, Tehran, Iran (Islamic Republic of)
Background: Many Iranian adolescent girls are iron deficient, but it is unclear whether iron deficiency is associated with other nutritional risk indicators.
Objective: To investigate the association between iron deficiency and weight status (measured as BMI) among a reprehensive sample of adolescent girls.
Methods: A cross-sectional study was performed in a region of southern I.R. Iran. 431 iron-deficient participants (with or without anemia) were selected by systematic random sampling among all students in grades 1 to 4 from high schools for girls. Blood samples were collected and assayed for hemoglobin, hematocrit, serum ferritin, iron and total iron binding capacity. Anthropometric assessments included measurement of weight and height. Body mass index was calculated according to age and gender-specific BMI growth charts for children 2 to 20 years of age.
Results: 15.3% were at risk for overweight and 9.3% were overweight. The severity of iron deficiency increased as BMI increased from normal to at risk for overweight and to overweight. Iron deficiency anemia was most prevalent among overweight adolescent than at risk for overweight and normal weight adolescents (32%, 21%, and 18%, respectively).
Conclusions: The results of this study showed an inverse association of BMI with serum ferritin. Overweight adolescents demonstrated an increased prevalence of anemia. Because of potentially harmful effects of iron deficiency, obese adolescents should be routinely screened and treated as necessary.
100 Prevalence of obesity and overweight in English 11–16 year olds: between-group differences in selected cardiovascular disease risk factors
G Sandercock; C Voss
University of Essex Centre for Sports and Exercise Science, Colchester, United Kingdom
Purpose: Recent English data regarding prevalence rates of obesity and overweight in 11–16 year olds are available from an ethnically diverse sample within London. These data are valuable, showing prevalence of obesity and overweight of approximately 6% and 18% respectively. The primary aim was to determine the prevalence of obesity and overweight, according to International Task Force on Obesity (IOTF) criteria, in a sample taken outside London, including volunteers from rural areas with an ethnic mix more representative of England. The secondary aim was to determine between-group differences in: waist circumference, physical activity, aerobic fitness, and blood pressure, according to weight classification.
Methods: Mass, stature, BMI, and systolic blood pressure (SBP) were measured in 2795 volunteers (1457 boys) aged 11–16 yrs in the East of England. Physical activity was assessed by 7-day recall (PAQ-A) and aerobic fitness by 20 m shuttle-run test (20 m SRT). BMI was converted to IOTF classification. SBP and 20 m SRT were converted to age- and sex-specific percentile scores. Between-group differences were analysed using one-way ANOVA with post hoc Tukey tests.
Results: The sample was broadly representative of England in terms of ethnic mix (88% White British, 3% Black, 4% Asian, 5% from other or mixed backgrounds) and residential distribution (83% urban). 6% of volunteers were obese and 19% were overweight. There were significant main effects for IOTF classification across all dependent variables. Waist circumference percentile was higher (p>0.001) in obese (88±19) and overweight (86±18) groups compared with the normal weight group (56±27). Aerobic fitness percentile was lower (p>0.001) in obese (28±21) and overweight (39±22) compared with the normal weight group (56±26). SBP was higher (p>0.001) in obese (74±26) and overweight (72±28) compared with the normal weight (65±28) group. Physical activity was significantly (p>0.02) lower in the obese group compared with the normal weight group.
Discussion: Prevalence of obesity and overweight in the East of England is similar to that found in London. There is a strong, graded, association between BMI classification and a number of other cardiovascular risk factors in English schoolchildren.
101 Heart Disease Prevention in juvenile obesity: the protective effects of an aerobic Exercise Program
MB Rossetti1; AR Brasil2; AM Silveira2; PPF Filho2; RR Britto2; RC Norton2
1Catholic University of Minas Gerais PHYSICAL THERAPY, Belo Horizonte, Brazil; 2Federal University of Minas Gerais Pediatrics, Belo Horizonte, Brazil
Juvenile obesity and physical inactivity, which have reached epidemic proportions worldwide, are important risk factors for atherosclerosis and other cardiovascular morbidities. Being related to systemic inflammation, both conditions have received wide scientific attention. Recently, higher levels of C-reactive Protein were observed in obese adults and children.
Purpose: Foccused on early prevention, it was hypothesized that a programme containing medical, nutricional and psycological counselling, plus supervised physical activity sessions, would generate cardioprotection for overweight children and adolescents.
Methods: This prospective clinical trial studied parallel groups of overweight children and adolescents (n=45), from 6 to 16 years old, of both sexes and with a body mass index above>85th percentile. The control group (n=18) was given the traditional medical treatment aiming on lifestyle changes. The intervention group (n=27) underwent, beyond the standard recommendations, a supervised moderate intensity aerobic exercise program, three times a week, for 12 weeks. Estimates os oxygen consumption (VO2 max) from the Rockport Walking Test, time spent to perform the test (T, minutes), serum levels of ultra-sensitive C-reactive Protein (us-CRP), total colestherol to high density lipoprotein ratio (TC:HDL) and percentual body fat (%BF) were obtained for the two groups, before and after the study period. It was used the Student T-Test and multivariated analysis to check the differences obtained within and between groups (p>0.05).
Results: The intervention group obtained various benefits recognized as cardioprotective: increase in VO2 max (p=0,0001) and decreases in % BF (p=0,0001), TC:HDL ratio (p=0,005), us-CRP levels (p=0,0001), T (p=0,0001), BMI (p=0,003), while the control group had increases in the inflammatory marker us-CRP (p=0,0027), without alterations in the other variables of interest.
Conclusions: A supervised exercise programme should be an essential component of multidisciplinary approachs for treating juvenile obesity, due to its important antinflammatory and metabolic roles
102 Mode of transport to school and prevalence of risk factors for cardiovascular disease in English schoolchildren
C Voss; G Sandercock
University of Essex Centre for Sports and Exercise Science, Colchester, United Kingdom
Purpose: The aim of this study was to illustrate the relationship between mode of transport to school and prevalence of risk factors for CVD, such as low aerobic capacity, sedentary lifestyle (by physical activity (PA)), elevated systolic blood pressure (SBP) and central adiposity (by waist circumference (WC)) in English schoolchildren.
Methods: Two-thousand two-hundred and twenty-four English schoolchildren (1131 boys, 11–16 years) were recruited as part of the ongoing East of England Healthy Heart Study. After gaining parental consent, aerobic capacity (20m shuttle run test) was assessed and scores expressed as percentiles. PA was established through PAQ-A; SBP was measured and categorised as normal or elevated, and WC (cm) was measured and classified as normal, overweight or obese by percentiles.
Results: Mode of transport was: 8% cycle, 51.2% walk, 21.9% public transport, 18.9% car. ANOVA showed significant variance by mode of transport for aerobic capacity (F=4.9238, p=0.002), physical activity (F=12.356, p=0.000) and waist percentile (F= 4.450, p=0.004). No significant variance was identified for SBP (F=1.644, p=0.177). Post hoc analysis (Tukey) showed significantly better aerobic capacity in cyclist than in those driven to school (p=0.010) and between public transport users and those driven (p=0.005). Physical activity levels were significantly lower in all modes of transport when compared to the cyclists (p>0.001). WC was significantly lower in cyclists than in walkers (p=0.043) and those driven by car (p=0.003).
Conclusion: Based on our findings, it can be concluded that English children that cycle to school are more likely to have better aerobic capacity, enjoy an active lifestyle and have a more desirable central fat distribution than their peers. Interestingly, no similar association was found in those walking to school. The exercise intensity associated with cycling may be a mediation factor in this association. Driving children to school is associated with poor aerobic capacity, lower physical activity and undesirable central body fat distribution compared to their peers.
103 24-hours blood pressure monitoring in healthy Slovak children and adolescents - a multicenter study
A Jurko (Jr)1; E Cizmarova2; D Schwartzova3; E Ondriskova4; M Minarik5; I Tonhajzerova6
1Martin Faculty Hospital Dept. of Pediatric Cardiology, Martin, Slovak Republic; 2Pediatric Cardiology Pediatric Cardiology, Bratislava, Slovak Republic; 3Pediatric Cardiology Pediatric Cardiology, Kosice, Slovak Republic; 4Pediatric Cardiology Pediatric Cardiology, Myjava, Slovak Republic; 5Anestesiology Anestesiology, Zilina, Slovak Republic; 6Department of Physiology Department of Physiology, Martin, Slovak Republic
Introduction: Ambulatory blood pressure monitoring [ABPM] is a valuable and irreplaceable diagnostic tool for juvenile hypertension. Until now, there are no ABPM reference levels in healthy children and adolescents and there is no categorization of juvenile hypertension based on this method, in Slovakia.
Purpose: Measurement of normal ABPM levels in healthy children in Slovakia in dependence on body height and sex.
Methods: Study involved 826 children and adolescents [437 boys and 389 girls] at the age from 10 to 19 years. There were 80 children in each age group. Children originated from the cities of Bratislava, Martin and Kosice. Rural population were represented by children from Myjava. All children included in the study were healthy, without taking any medications. The measurements were done according to the same protocol and with the same type of blood pressure machine [BP One, Medatron], in all centers. The cuff size was adjusted according to the age of the child. The blood pressure has been measured every 20 minutes during the day and every 40 minutes during the night. Calculated were minimal, maximal and average blood pressure levels for all age categories, specifically for girls and boys.
Results: Systolic blood pressure is increasing significantly with increasing body height. The increase is more significant in boys than girls. The 50th percentile of systolic blood pressure in boys is increasing from 104 mmHg to 114 mmHg and in girls from 104 mmHg to 110 mmHg. The 50th percentile of diastolic blood pressure is 69±8 mmHg and does not depend on body height or sex. During night, there was 11 % drop in systolic blood pressure in both sexes and 21 % drop in diastolic blood pressure [22 % in boys and 19 % in girls].
Conclusion: This multicenter study provides normal ABPM levels in healthy children in dependence on body height and sex in Slovakia.
104 Overweight, hypertension and lipid disorders in the Siberian adolescent population: prevalence, interrelations and familial aggregation
D Denisova; YUP Nikitin; L Zavjalova; S Burakova
Institute of Internal Medicine, Novosibirsk, Russian Federation
Overweight, high blood pressure (BP) and lipid disorders in childhood are considered as risk factors for CVD in adulthood. The combination and familial aggregation of these factors in children and adolescents aggravates the predictive risk.
The aim of the study was to evaluate the prevalence and interrelations of overweight, elevated BP and high total cholesterol (TC) in Siberian adolescents, as well as the presence of its familial aggregation.
Methods: Four cross-sectional surveys of representative samples of school children aged 14–17 during 1989–2003 were carried out in Novosibirsk (Russia). Total sample was 2569 (1214 males). Body mass index (BMI, kg/m), systolic, diastolic BP and TC were measured. Diet was estimated using 24-hour dietary recall. The mail questionnaire for parents with the information on blood pressure, height and weight was used.
Elevated BP for adolescents was estimated using NHBPEP 4th report criteria, for parents - using JNC-7 criteria. Adolescent's overweight registered using IOTF criteria, parent's overweight - using WHO criteria (BMI=25 kg/m). Prevalence of high TC was evaluated with NCEP-peds criteria.
Results: Prevalence of prehypertension in adolescents was high in both gender groups: 40% in boys and 26% in girls (P>0.01); hypertension − 14% in boys and 10% in girls. Overweight registered in 11% boys and 13% girls. Frequency of high TC (>2000 mg/dl) was 13, 5% in males and 22% - in females. Self-reported prevalence of parents' hypertension was 24% among fathers and 18% among mothers, but 53% of both mothers and fathers had overweight. Distribution of BMI percentiles and the prevalence of elevated BP within each BMI percentile category were estimated. A linear rising of high BP prevalence in adolescents as BMI increased from 5th to 95th percentile was demonstrated. Prevalence of elevated BP was 5-fold increased in boys and 3-fold increased in girls from lowest BMI to highest. In addition, elevated BP was registered twice more often in overweight adolescents. Significant regression coefficients for TC controlled by age and gender were revealed with BMI, diastolic BP and triceps skinfolds. Associations of parents' and children's BP and BMI levels were revealed. Among adolescents of hypertensive mothers elevated BP registered twice more often compared with normotensive mother' children. Parents of overweight adolescents had BMI higher than parents of adolescents with normal BMI.
Conclusion: Revealed associations of BP, TC and BMI in adolescents and familial aggregation of these factors underscore the importance of controlling adiposity, BP and lipid profile early in life.
105 Overweight-cosmetic defect or serious potential threat to the heart in children?
I Schusterova1; J Saligova2; M Kuchta3; L Potocnakova2; I Riecansky4
1East Cardiovascular Institute Kosice Cardiovascular Surgery Department, Kosice, Slovak Republic; 2Children Faculty Hospital, Kosice Preventive Cardiology, Kosice, Slovak Republic; 3Children Faculty Hospital, Kosic, Kosice, Slovak Republic; 4Slovak Medical University, Faculty of Cardiol, Bratislava, Slovak Republic
Overweight precede obesity and from 60 to 80% children with overweight become later obese. Aim of our study was to investigate the impact of grade of obesity assessed by BMI percentiles (overweight=85 and >95 BMI percentile; obesity=95 BMI percentile) on diastolic function in children and adolescents.
Methods: Two-dimensional ultrasound, M-mode imaging and pulsed wave conventional Doppler measurements were compared in 22 (mean age 13.5±1.2 years) obese and overweight subjects and 24 age- and gender matched lean controls to assess cardiac structure and function at rest.
Ambulatory blood pressure (BP) monitoring (ABPM) was performed and lipids level established.
Intima-media thickness (IMT) was measured ultrasonographically.
Results: Left ventricle mass (LVM) positively correlated with waist circumferences (WC), left atrial diameter (LAD) (p>0.0001), casual and mean day systolic BP (p>0.001), body weight, height and BMI (p>0.0001) as well as with deceleration time of early transmitral blood flow velocity (DT) and relative wall thickness (RWTh) (p>0.05). DT positively correlated with body weight (p>0.02). Isovolumetric relaxation time (IVRT) positively correlated with interventricular septum (IVS) and relative wall thickness (RWTh) (p>0.02) and peak A flow velocity with WC (p>0.05), triacylglycerol level (p>0.03) and BMI percentil (p>0.002). Statistical differences between obese, overweight and normal weight children were found besides expected parameters as body weight and BMI percentiles also in WC (p>0.0001), casual systolic and diastolic BP (p>0.01; p>0.05), mean systolic 24 h BP (p>0.05) and TAG level (p>0.01). Differences in echocardiographic parameters were present in IVS (p>0.05), posterior wall thickness (p>0.01), left ventricle enddiastolic (p>0.005) and endsystolic diameter (p>0.05) and volume (p>0.05). LVM and LVM by height2.7 (LVMIV) (p>0.05) and peak A flow velocity (p>0.01) were significantly higher and E/A ratio lower (p>0.05) in obese and overweight. Comparing only obese and normal weight children moreover mean IMT (p>0.05) were higher and HDL cholesterol (p>0.05) lower and LAD (p>0.05), IVRT (p>0.05) and DT (p>0.05) were increased in severe obese children.
Conclusion: Obesity and overweight in children and adolescents are accompanying not only by some metabolic disorders, increased BP, IMT and LVM but also some indexes of diastolic function are impaired. Overweight which precedes obesity is associated with some of these abnormalities so it is important to begin prevention as soon as possible when only overweight or mild obesity is present.
106 Influence of an 8 month additional school sport program on parameters of anthropometry an exercise capacity in obese basic school children: the K.i.S.-Project
J Latsch; L Wedig; J Buschmann; HG Predel
German Sports University Institute of Cardiol and Sportsmedicine, Cologne, Germany
Topic: Overweight and obesity in young children are beyond the major health related topics of the next decades. In early age children are predisposed for their future health status. Obese childrens risk for consecutive CVD is highly elevated in comparison to normal weight children. Besides socio-economic factors as well as educational aspects overweight, obesity and physical inactivity have major influence on future health behaviour and status.
Methods: We examined a total of 853 children in 10 basic schools in the Cologne/Bonn area twice within one school year, only 694 children participated in both investigation dates. Herein were 345 girls and 349 boys, age 7,71±1,27 yrs, height 131,5±9,1 cm, weight 31,5±8,6 kg, BMI 17,8±3,3 kg/m2. Additionally an individual staging into BMI-percentiles was accomplished, obesity was diagnosed in case of 97 or higher percentile. At time 1 a total of 12,8 % were obese. The examination panel contained several motoric, functional, cardiac, vegetative and health related topics. To investigate on exercise capacity the children performed the “6 minutes-running-test”. During the following school year all children volunteered in an extra school sport program once daily.
Results: At time T2 (after 6-7 month) children grew on average by 3,5 cm, gained about 2 kg of weight with an BMI increase of 0.14 kg/m2. A portion of 11,8% were obese at T 2. 10,4% were obese at T1 and T2 1,4% were not obese on T1. Obese children (OC) had no significant change in BMI (p=0,567) independently of the gender between T1 and 2, T1: 24,2 kg/m2 (m: 24,3; f: 24,1) vs. T2: 24,3 kg/m2 (m: 24,5; f: 24,0). Non obese children (NOC) achieved a significantly higher “6 min-running-test” result (T1: NOC 810,0±120,5m vs. OC 702,5±107,6m) (T2: NOC 815,4±125,5m vs. OC 709,2±109,9m). There was neither a significant difference in maximum heart rate between NOC and OC nor in recovery phase one and three minutes after finishing the running test.
Discussion: Compared to average age related “6-min-running-test” results the majority of the tested children were below this, only 3% in T1 and 3,9% in T2 achieved results above average. The tested collective was under average in terms of physical fitness. A portion of 13% obese children seems comparably representative. An additional hour of physical exercise in school every day could not effect a reduction of average weight or significant increase of running capacity. The KiS Project was not meant to be an anti obesity program but a concept to generally elevate basic school childrens daytime or scholl based activity.
107 Children and youth need better education on CVD prevention and health promotion at school
L Matwiejczyk; M Bogowicz; M Krawczyk; K Chwojnicki; A Ignaszewska-Wyrzykowska; B Wyrzykowski; T Zdrojewski
Medical University of Gdansk Department of Hypertension And Diabetology, Gdansk, Poland
Purpose: Wrong beliefs and unhealthy habits, often “acquired” in childhood and adolescence from family, society and media have potential influence on future problems in prevention and treatment of cardiovascular diseases (CVD) on individual and population level. The aim of this study was to evaluate both health status as well as habits and knowledge on CVD risk factors in youths from best secondary schools from large cities area in Poland.
Methods: 155 high school students (65 girls, 90 boys) aged 16-17 from Gdansk, Gdynia and Sopot answered 43 questions and underwent anthropometrical (BMI, circumference of predominant arm, waist and hips) and blood pressure measurements.
Results: Most of the students (83%) considered their health as relatively good or very good. There were 23% of active smokers and 11% of ex-smokers. Although 80% of active smokers confirmed that tobacco can cause heart diseases, only 26% pointed out smoking as one of the most important risk factors. Vegetables and fruits were indicated as most valuable ingredients of a healthy diet by 95% of respondents. Nevertheless, almost nobody ate 4-5 portions of fruits or vegetables a day. Half of students (51%) did physical exercise less than 3 times a week. When asked about diseases and complications caused by untreated hypertension, 43% of respondents didn't give any answer. Sixty five percent of students didn't know what are the highest values of normal blood pressure. In 9,4% of cases students' Body Mass Index (BMI) was 25 kg/m2 or higher, and in 2,6% − 30 kg/m2 or higher. High normal blood pressure was found in 13% of subjects, and identical figure was found to have increased blood pressure.
Conclusion: Unhealthy lifestyle of examined youths who will build the elite of the society in future, namely: low physical activity, unhealthy diet, high tobacco intake and poor knowledge on CVD risk factors need urgent comprehensive, regular educational and behavioral action, preferably as a special training in schools.
108 Exercise-induced abnormal pulmonary arterial pressure response in adolescents and adults with atrial or ventricular septal defect
T Moller1; E Pettersen2; K Peersen2; PM Fredriksen1; H Holmstrom1; E Thaulow1
1Vestfold Hospital Pediatric Department, Toensberg, Norway; 2Rikshospitalet University Hospital Department of Cardiology, Oslo, Norway
Introduction: The European Heart Survey on Congenital Heart Disease described follow-up data in 902/634 adult patients with isolated atrial or ventricular septal defect (ASD or VSD). The reported prevalence of pulmonary hypertension was 18% in both closed ASD and closed VSD which was surprisingly high. However, the study recruited patients from specialised centres with a selection towards difficult cases. Our study aims to examine a representative population-based group of young patients with isolated ASD or VSD. The main focus is pulmonary hypertension or its postulated precursor, abnormal pulmonary pressure response (AR) during exercise.
Methods: The study comprises 49 patients with either isolated VSD or ASD, whose defects were assumed hemodynamically insignificant or surgically closed early in life. The patients were recruited among all patients born between 1982 and 1993 from two regions in Norway. They are matched against 62 healthy controls with same age and gender. Cardiovascular exercise testing (treadmill protocol) and echocardiography at rest and during supine cycling (target heart rate 160-min) are performed.
Results: Treadmill testing showed normal (Gaussian) distribution of age-corrected maximal oxygen uptake (VO2peak) for both groups expressed by VO2peak Z-score related to a Norwegian normal standard. Highly endurance-trained volunteers with a Z-score > 2 were excluded. There was a significant lower mean Z-score of VO2peak in the patient group (−1.65, −5.2 to 1.3) as compared to the normally trained controls (mean −0.12, −4.5 to 1.8).
Echocardiography showed a significant lower right ventricular performance measured by tricuspid annular plane systolic excursion (TAPSE) (p>0.001, means patient/control 18.4/23.0 [−6.1,-3.0]). There were no cases of pulmonary hypertension at rest in the patient group.
Exercise echocardiography rendered assessable registrations of tricuspid regurgitation jet velocity in 45/49 patients and in 60/62 controls.
20 of 45 patients (44%) and 11/60 controls (18%) had PAP above 40 mmHg during exercise. Eight patients (18%) but only one control (2%) had PAP above 50 mmHg during exercise. The PAP did not differ between genders and no correlation was found between TAPSE and PAP.
Conclusion: Young patients with small untreated or surgically closed isolated ASD or VSD have lower exercise capacity and lower right ventricular performance than healthy individuals. About one out of five patients has pathologic pulmonary pressure load above 50 mmHg during exercise. The long-term implications of these findings have to be investigated.