145 Major life events and the risk of cardiovascular disease: findings from Copenhagen city heart study
H Petersen1; G Boysen2; E Prescott2
1Bispebjerg University Hospital Department of Cardiology, Copenhagen, Denmark
2Bispebjerg University Hospital Department of Neurology, Copenhagen, Denmark
Purpose: The aim of the present study was to describe whether major life events (LE) prospectively predict cardiovascular disease (CVD).
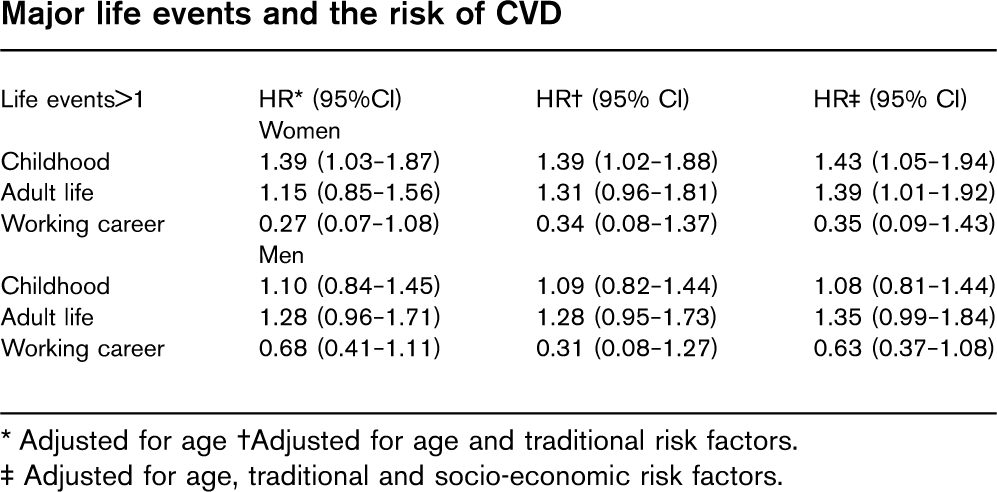
Methods: 9542 randomly selected adults without CVD were examined in The Copenhagen City Heart Study. Major LE were self-reported and categorised as related to childhood (parents with critical illness, unemployment or financial problems, family conflicts or placed away from home), working career (loss of job, lack of promotion or conflicts with colleagues, superiors or subordinates) or adult life (critical illness in close family, children with educational problems, conflicts with adult children, financial or marital problems). Endpoint was CVD defined as myocardial infarction or validated ischemic strokes both fatal and non-fatal. Hazard ratio (HR) for incidence of CVD was calculated for LE=1 and LE>1 using Cox proportional hazard model with LE=0 as reference.
Results: Adult LE>1 were associated with an adjusted increased risk of CVD in both genders, with a combined HR=1.37 (95% CI=1.10–1.71). Childhood LE>1 conveyed íncreased risk of CVD in women, but not in men (test for interaction with gender p=0.24). There was a trend towards lower risk associated with working related LE. When exploring each question, the item “Lack of promotion” seemed to be the “protecting” factor. There were no association between LE=1 and CVD.
Conclusion: The data suggest that major LE in childhood and adult life convey increased risk of CVD. To our knowledge, this is the first prospective study of the association between LE and CVD.
∗ Adjusted for age †Adjusted for age and traditional risk factors.
† Adjusted for age, traditional and socio-economic risk factors.
146 The catabolic-anabolic balance in the skeletal muscle: effects of an aerobic exercise program on protein catabolism in chronic heart failure patients
M Sandri1; S Gielen1; V Adams1; N Mangner1; R Hoellriegel1; S Erbs1; A Linke1; S Moebius-Winkler1; R Hambrecht2; G Schuler2
1University of Leipzig Heart Center, Leipzig, Germany
2Heart Center, Bremen, Germany
Background: Tagging structural proteins with organ-specfic E3-ligases is a key process in protein catabolism via the ubiquitin-proteasome pathway. RNF 28 (equivalent to Murf-1 in rats) is expressed in human skeletal muscle as a specific E3-ligase. We could previously describe an increased Murf-1 expression in a rat model of chronic heart failure (CHF) which is indicative of an accelerated protein catabolism.
Aim of this ongoing prospective randomized clinical trial is to establish the effects of a 4-week supervised bicycle ergometer training on RNF 28 expression in skeletal muscle biopsies of patients with stable CHF and healthy age-matched subjects.
Methods: A total of 50 CHF-patients and 60 healthy subjects were prospectively randomized to 4 weeks of supervised bicycle ergometer training at 50 to 70% of the individual heart rate reserve 4 times 20 min/day or to a control group. Before and after the training intervention a maximal spiroergometry and echocardiography were performed. Skeletal muscle needle biopsies were obtained from the vastus lateralis muscle.
Expression of the E3 ligase Murf-1 and TNF were quantified by real-time PCR and standardized for 18S-rRNA.
Results: (1) CHF patients (age 60.3±2.9 years, BMI 28.9±1.7, LV-EF 27.4±1.7%): After four weeks of bicycle ergometer training VO2max increased from 14.9±3.3 to 18.1±4.7 ml/min/kg, p>0.01 versus control, and LV-EF increased from 26.8±4.6 to 33.1±5.5% (p=0.001 vs. control). Skeletal muscle Murf-1 expression was significantly higher as compared to HS at baseline. After the training intervention Murf-1 expression decreased from 0.49±0.21 to 0.22±0.07 rel. units (p>0.05) and TNF-expression decreased from 79±7.1 to 44.7±5.9 rel. (p>0.001) units while remaining unchanged in the control group.
(2) Among healthy subjects (age 64.7±2.7 years, BMI 26.2±0.5, LV-EF 63 ±0.8%) bicycle ergometer training increased VO2 max from 20.3±2.1 to 27.9.2±1.3 mL/kg min (p=0.01). In the training group no changes in Murf-1 and TNF-expression were observed in comparison to control patients.
Conclusion: Two key messages emerge from this prospective randomized study: (1) CHF is associated with both inflammatory and catabolic activation in the skeletal muscle as indicated by higher baseline Murf-1 levels among CHF patients. (2) Training cuts the elevated E3-ligase expression by half within only four weeks of intervention.
These findings extend the current knowledge of how physical activity readjusts the catabolic-anabolic balance in CHF. The prevention of muscle atrophy may be an important factor explaining the prognostic benefits of training in CHF.
147 Regular physical exercise training induces neovascularization in the skeletal muscle in patients with severe chronic heart failure as a sign of endogenous tissue regeneration
R Hoellriegel1; S Erbs1; A Linke1; V Adams1; S Gielen1; M Sandri1; N Mangner1; R Hambrecht2; G Schuler2
1University of Leipzig - Heart Center Department Of Cardiology, Leipzig, Germany
2Klinikum Links der Weser Cardiology, Bremen, Germany
Bone marrow-derived stem cells are known to contribute to endogenous tissue regeneration. In patients (pts) with chronic heart failure (CHF) the number of circulating endothelial progenitor cells (EPC) is known to be reduced contributing to an impaired regenerative capacity of the skeletal muscle.
Aim of the present study was to determine, whether physical exercise training influences capillary density in the skeletal muscle through activation of EPCs in pts with CHF and whether this impact on exercise capacity.
Methods: 37 pts with CHF (LVEF 24±2%, NYHA class IIIb) were randomized to 6 months of exercise training (30 min bicycle ergometer training daily at 50–60% of maximal work load) or sedentary lifestyle (control). At begin, after 3 and 6 months, blood samples and a biopsy of the vastus lateralis muscle were obtained, and a spiroergometry, as well as an echocardiography were performed. The number of circulating CD34/KDR+ EPCs was detected using FACS analysis. Capillary density was quantified by immunohistochemistry.
Results: As a result of the training intervention the number of CD34/KDR + EPCs in the blood increased by 83% after 3 months and by 79% after 6 months (p>0.05 for δ after 3 and 6 months versus begin and control). This was associated with an improvement in capillary density by 14% after 3 months and 15% after 6 months (begin: 1.49±0.02; 3 months: 1.70±0.02; 6 months: 1.71±0.03 capillaries/ muscle fibre; p>0.05 for 3 and 6 months versus begin and control). This training-induced augmentation in capillary density was accompanied by an improvement in peak oxygen uptake by 16% after 3 months (from 15.3±0.8 to 17.8±0.8 ml/min/kg) and by 24% after 6 months (to 19.0±0.7 ml/min/kg; p>0.05 for 3 and 6 months versus begin and control).
Moreover, left ventricular ejection fraction increased from 24.1±1.2% to 33.5±1.4% after 3 months and to 38.9% after 6 months (p>0.05 for 3 and 6 months versus begin and control). All above mentioned parameters remained unchanged in the control group.
Conclusion: In patients with severe chronic heart failure regular exercise training leads to a neovascularization in the skeletal muscle. This training-induced endogenous tissue regeneration might be partially the result of an augmentation of the number of circulating endothelial progenitor cells and is associated with an improvement in exercise capacity.
148 The relative importance and conjoint effects of obesity and physical inactivity on the development of insulin resistance and metabolic syndrome: fatness or fitness?
E Ingelsson; J Sundstrom; U Riserus; K Michaelsson; L Byberg; J Arnlov
Uppsala University Department of Public Health and Caring Sciences, Uppsala, Sweden
Purpose: Obesity and physical inactivity are related to development of insulin resistance, but their relative importance and conjoint effects are unclear.
Methods: We assessed body mass index (BMI) and self-reported leisure time physical activity (PA) in 672 50-year-old men free from diabetes and metabolic syndrome (MetS). In these participants of the community-based Uppsala Longitudinal Study of Adult Men (ULSAM), we evaluated insulin sensitivity with euglycemic insulin clamp technique and the prevalence of MetS according to the modified NCEP criteria at age 70. We performed multivariable linear (insulin sensitivity at age 70 as dependent variable) and logistic regression (MetS at age 70 as dependent variable) models with BMI, PA, and homeostasis model assessment insulin resistance (HOMA-IR) at baseline as independent variables. Further, the same models were analyzed using four categories by BMI above or below median, and low (sedentary or moderate) or high (regular or athletic) PA at baseline.
Results: In multivariable models including BMI, PA, and HOMA-IR at baseline, both BMI (β, –0.25mg/kg bodyweight/min per 1 kg/m2 increase; P>0.0001) and PA (adjusted least square means, 5.2, 5.2, 5.4, and 6.3 mg/kg bodyweight/min in individuals with sedentary, moderate, regular, and athletic PA, respectively; P=0.002 for trend) were significant predictors of insulin sensitivity at age 70. BMI at baseline was significantly associated with MetS at age 70 in a multivariable model (odds ratio [OR], 1.27; P>0.0001), whereas PA was not. When categorizing individuals into four groups by BMI and PA at baseline, insulin sensitivity at age 70 decreased significantly over the categories in a model adjusting for HOMA-IR at baseline (adjusted least square means, 5.9 [low BMI/high PA]; 5.7 [low BMI/low PA]; 5.0 [high BMI/high PA]; and 4.5 [high BMI/low PA] mg/kg bodyweight/min, respectively; P>0.0001 for trend). The multivariable-adjusted ORs for MetS at age 70 were 1.3 (low BMI/low PA), 3.8 (high BMI/high PA), and 3.9 (high BMI/low PA) using the low BMI/high PA group as reference (P>0.0001 for trend).
Conclusion: In our community-based sample of middle-aged men, BMI and PA were independent and additive predictors of insulin resistance after 20 years of follow-up. Although obesity and physical inactivity may increase insulin resistance and metabolic risk by partly independent pathways, the role of obesity appears to be more important than a sedentary lifestyle. Nevertheless, our results highlight the importance of targeting both fatness and fitness to achieve improved public health.
149 Re-evaluating Rose: benefits of population and high risk prevention strategies
MT Cooney; AL Dudina; IM Graham
Adelaide Meath Hospital Cardiology, Dublin, Ireland
Background: “A large number of people exposed to a small risk may generate more cases than a small number exposed to a high risk” - G. Rose, 1985. This concept is the basis for the population prevention strategy which aims to shift the whole distribution of exposure in a favourable direction. The high risk strategy directs the most aggressive risk factor modification towards those at highest risk. Manuel et al recently suggested that the population strategy no longer applies and is substantially less effective than high risk strategies. However, this was evaluated assuming a population strategy with a reduction in population cholesterol of only 2%, no change in other risk factors and a high risk strategy with a 100% uptake of risk factor screening.
Purpose: Evaluation of the benefit of population and high risk strategies with varying levels of population risk factor reductions and uptake of screening programs.
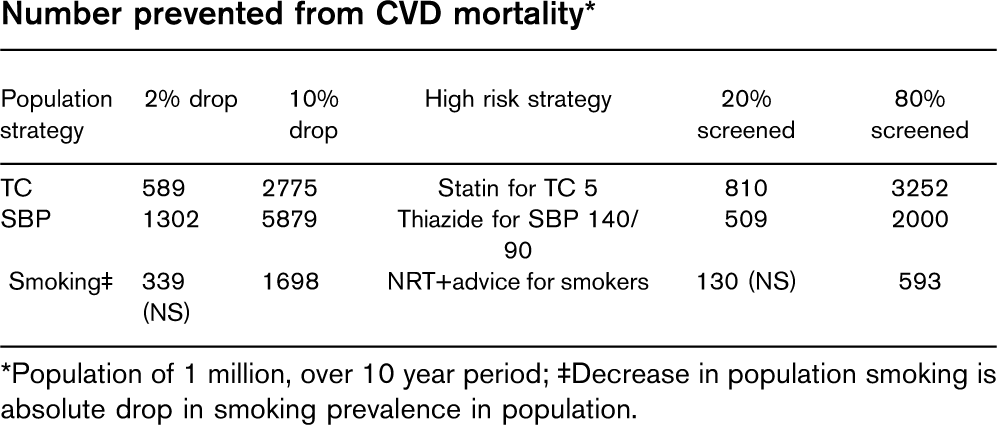
Methods: The Systematic Coronary Risk Evaluation (SCORE) dataset was used (high risk countries only), including over 112,000 people. SCORE risk was calculated for each individual (10 year risk of CVD mortality). This was re-calculated after reduction of each individual's risk factor levels (cholesterol (TC) blood pressure (SBP) and smoking) by a given percentage. The difference between these is the percentage prevented from dying of CVD in a 10 year period. This estimates the benefit of various population strategies. For the high risk strategies, those at high risk (ESC definitions) were considered to be “treated” with statin if TC 5 mmol/l, thiazide if SBP140/90 mmHg and NRT/advice if smokers. The relative risk reduction (as estimated in meta-analyses) was applied to their SCORE and the difference calculated.
Results: The table shows the benefit of sample population and high-risk strategies.
Conclusion: Population and high risk prevention strategies are complementary. The levels of screening uptake and reductions in risk factor levels achieved should be considered when evaluating strategies for prevention.
∗Population of 1 million, over 10 year period; ‡Decrease in population smoking is absolute drop in smoking prevalence in population.
150 Marked repolarisation changes in highly trained athletes of african/afro-caribbean (black) origin: Overlap with and differentiation from hypertrophic cardiomyopathy (HCM)
M Papadakis1; C Edwards1; JC Rawlins1; S Basavarajaiah1; S Gati2; S Sharma1
1King's College Hospital & Lewisham Hospital Cardiology, London, United Kingdom
2Queen Elizabeth Hospital Cardiology, London, United Kingdom
Objectives: Electrocardiographic (ECG) repolarisation changes affecting ST segments and T waves are well recognised and relatively common in black athletes (BA). Certain anomalies, specifically deep (–0.2 mV) T-wave inversions are also common in HCM, the commonest cause of death in young athletes and warrant further investigation. The precise overlap relating to the prevalence and distribution of T wave inversions between BA and individuals with HCM is unknown but has important implications with regard to the European Society of Cardiology and International Olympic Committee recommendations, implementing ECG as part of preparticipation screening of all competitive athletes. The aim of this study was to compare ECG repolarisation changes seen in BA and patients with HCM.
Methods: The ECGs of 198 asymptomatic and normotensive BA (21% with echocardiographic evidence of physiological left ventricular hypertrophy; 13–166 mm) were compared to those of 53 individuals with unequivocal HCM.
Results: Individuals with HCM had a higher prevalence of deep T wave inversions (–0.2 mV) compared with BA (64% vs 18%; p>0.001). There were also significant differences in the distribution of T wave inversions between the two groups. Deep T wave inversions in contiguous inferior and/or lateral leads were more common in HCM compared with BA (85% vs 17%; p>0.001), whereas deep T wave inversions, confined, in V1–V4 were more common in BA compared with HCM (83% vs 15%; p>0.001). Deep T wave inversions in HCM were associated with concomitant ST segment depression in 56% of individuals versus none of the BA (p>0.001). In contrast T wave inversions in BA were commonly associated with ST segment elevation (69%). Left atrial enlargement and pathologic Q waves were observed in 68% and 25% of individuals with HCM but in none of the BA.
Conclusion: Deep T wave inversions are present in almost 20% of BA therefore pre-participation screening with ECG using current criteria would result in unnecessary investigations in an unacceptable number of BA. However, the distribution of deep T wave inversions, the pattern of ST segments and the presence or absence of voltage criteria for left atrial enlargement and/or pathological Q waves help identify those BA who may have HCM. Black athletes exhibiting: (1) T wave inversions in the inferior and/or lateral leads, (2) T wave inversions associated with ST segment depression, (3) voltage criteria for left atrial enlargement and/or (4) pathological Q waves warrant further investigations for HCM.