151 Usefulness of HDL-associated phospholipid levels as a predictor for the severity of coronary artery disease evaluated by multi-detector row computed tomography
R Mitsutake; S Miura; B Zhang; K Saku
Fukuoka University Hospital Cardiology, Fukuoka, Japan
Background: A relationship has been noted between lower levels of HDL-associated phospholipid and atherosclerotic coronary artery disease (CAD). The aim of this study was to assess the relationship between numerous lipidemic factors and severity of CAD as evaluated by multi-detector row computed tomography (MDCT).
Methods and Results: Subjects included 195 consecutive patients who underwent coronary angiography using MDCT because of suspected CAD. Coronary artery calcification (CAC) score and Gensini's score (GS) as evaluated by MDCT, platelet-activating factor acetylhydrolase (PAF-AH), free cholesterol (FC), phospholipid (PL), remnant-like lipoprotein particle-cholesterol (RLP-C), apolipoprotein (apo)-C, apo-B, apo-C3, apo-E, highly-sensitive CRP were determined. The number of the significant coronary vessel disease (VD) was determined using MDCT. The number of VD was significantly associated with HDL-C, HDL-associated HDL-C, HDL-associated PL, HDL-associated FC and RLP-C. Logistic regression analysis revealed that the number of VD was most closely correlated with HDL-C levels (p=0.02). GS was significantly associated with age, HDL cholesterol, hemoglobin A1c, HDL-associated PAF-AH, HDL-associated FC and HDL-associated phospholipid. Multivariate analysis revealed that GS was most closely correlated with HDL-associated phospholipid (p=0.02).
Conclusion: Lower levels of HDL-associated phospholipid may be an indicator and provide additional information regarding the severity of CAD compared with other lipidemic factors.
152 Alcohol consumption and the prevalence of hypertension in Czech Republic, Poland and Russia: cross-sectional analysis of the health, alcohol and psychosocial risk factors in East Europe (HAPIEE) Study
A Pajak; K Szafraniec; R Kubinova; S Malyutina; A Peasey; Y Nikitin; M Bobak
Jagiellonian University Medical College, WNoZ Department of Epidemiology and Population Studies, Krakow, Poland
National Institute of Public Health, Prague, Czech Republic
Institute of Internal Medicine, SB RAMS, Novosibirsk, Russian Federation; University College of London, London, United Kingdom
Background: The relation between alcohol consumption and hypertension (HT) has not been studied in Eastern Europe, where the drinking pattern differs from western populations.
Aims: To assess the relation between the pattern of alcohol consumption and prevalence of HT.
Subjects: Men and women aged 45–69 years, randomly selected from population registers in 6 Czech towns, Krakow (Poland) and Novosibirsk (Russia).
Methods: Alcohol consumption in the last year was ascertained by structured interview, including the graduated frequency questionnaire. Binge drinking was defined as drinking 100 g of ethanol per occasion less than once a week. Type of alcoholic beverage predominantly consumed was assessed when the amount of ethanol of beer, wine, or spirits corresponded to at least 75% of the total ethanol consumed. Blood pressure was measured by standard protocol. HT was defined as blood pressure>=140/90 mmHg. Participants with treated HT were excluded. Multiple logistic regression was used to estimate the relation between alcohol consumption and HT. All analyses were first conducted separately by country and sex; since there were no statistically significant interactions, data were then pooled.
Results: A total of 15,027 participants was included into the analysis. Czech men and women had the highest mean intakes of alcohol per year (3,420 and 585 g, respectively). Mean dose per drinking occasion was highest in Russian men and women (56 g and 25 g respectively). Prevalence of binge drinking was more than twice higher in Russia than in Poland and Czech Republic. The relation between alcohol consumption and HT was similar across the countries. Increase in daily intake of 20 g of alcohol was associated with 29% increase in HT prevalence. Compared to abstainers, those who consumed more than 40 g ethanol per occasion as well as those who consumed more frequently than twice per week had increased risk of HT (OR=1.61, 95% CI: 1.41–1.84 and OR=1.63, 95% CI: 1.41–1.87 respectively). Isolated groups of binge and regular drinkers who consumed equal amounts of alcohol per year had similar prevalence of HT. Analysis with different types of alcoholic beverages yielded the same impact on HT prevalence.
Conclusion: Strong relation between the total dose of alcohol and HT has been confirmed in previously unstudied populations with different drinking pattern. There was no protective dose of alcohol. The similarity of the associations between alcohol and consumption across countries, all types of alcohol beverages and regular vs. binge drinkers suggests that drinking pattern does not modify the effect of alcohol on hypertension.
153 Effect of a single exercise bout on the number and function of endothelial progenitor cells in patients with chronic heart failure
E Van Craenenbroeck; P Beckers; V Hoymans; N Possemiers; J Roeykens; C Vrints; V Conraads
Antwerp University Hospital Department of Cardiology, Edegem, Belgium
Purpose: Exercise training partially restores impaired endothelial function in chronic heart failure (CHF) patients. This beneficial effect might be mediated by the regenerative capacity of mobilized endothelial progenitor cells (EPC). Acute exercise results in a temporary increase in vascular oxidative stress. At low concentrations, reactive oxygen species (ROS) act as mediators of cell signalling and can alter key cellular functions. We studied the effects of a single bout of maximal exercise on the mobilization, function and oxidative stress in EPC of CHF patients.
Methods: Venous blood was obtained from 12 CHF patients (median left ventricular ejection fraction 33%, 83% males, median age 62 yrs) before and immediately after cardio-pulmonary exercise testing (median percentage of predicted VO2peak 86%). Circulating CD34+ and CD34+/VEGFR2+ cells were determined by flow cytometric analysis and expressed as percentages of lymphocytes. Peripheral blood mononuclear cells (PBMC) were cultured in an endothelial growth medium to generate early acLDL+/lectin+ EPC. For the detection of intracellular superoxide production, a dihydroethidium assay was performed and EPC senescence was detected by acidic β-galactosidase staining. Migratory activity towards VEGF and SDF1a was assessed using a modified Boyden chamber assay. Prior to exercise, endothelial function was evaluated at the level of the brachial artery (flow mediated dilation).
Results: Following exercise, EPC decreased with 53% (0.19 [0.02–0.62] vs. 0.10 [0.02–0.30] %, median and range, p=0.015), whereas CD34+ cell count did not change. Migratory capacity of EPC augmented by 30% after exercise (p=0.041). Additionally, cellular senescence was significantly accelerated in EPC cultures after exercise (28 [4–52] vs. 36 [3–52]%, median and range, p=0.016). This effect was associated with a significant increase of intracellular ROS production in post-exercise EPC (43 [26–75] vs. 50 [42–85]%, median and range, p=0.008). Impaired endothelial function at baseline correlated negatively with the production of ROS (r=– 0.83, p=0.42).
Conclusion: In CHF patients, the number of circulating CD34+/KDR + cells decreases acutely following exercise. Acute exercise induces premature senescence in cultured early EPC, possibly mediated by increased ROS production. Nevertheless, the migratory capacity of early EPC is improved. Although speculative, ROS induced upregulation of eNOS should be investigated as a plausible mechanism.
154 Vascular oxidative stress inhibits mobilization of circulating stem cells with endothelial progenitor capacity in mice
T Suvorava1; S Kumpf1; V Adams2; G Kojda1
1Heinrich Heine University Institute of Pharmacology, Duesseldorf, Germany
2University of Leipzig Heart Center Leipzig, Leipzig, Germany
Purpose: The number of circulating stem cells with endothelial progenitor capacity (EPCs) was reported to inversely correlate with the number of cardiovascular risk factors and is reduced in cardiovascular disease. Despite recent advances in EPC studies, the molecular mechanisms of EPC mobilization remain unclear. We sought to investigate the effects of increased vascular oxidative stress on exercise-induced EPCs mobilization.
Methods: Transgenic mice with a vascular-specific overexpression of catalase and reduced vascular levels of oxidative stress (cat++) and their transgene negative littermates (catn) were assigned to a sedentary group and a group undergoing moderate forced exercise training (15 m/min, 30 min, 5 days a week, 3 weeks). The number of EPCs in peripheral blood was measured by Fluorescence-Activated Cell Sorting (FACS) using anti-mouse CD3, Flk-1 and CD34, CD133 or Sca-1 antibodies. Additionally, the effects of different amounts of physical activity on EPC mobilization were investigated in sedentary (singularized), freely moving (6 mice per cage), voluntary (9.8±0.7 km/night) and forced (15 m/min, 5 days, 30 min/day) running C57BL/6 mice.
Results: There was no difference in circulating EPCs between sedentary and freely moving C57BL/6 mice (p>0.05, n=5). Three weeks of forced exercise training failed to mobilize EPCs defined as double positive for Flk-1 and CD34 or more immature hematopoeitic stem marker CD133 (p>0.05, n=5–9). Similarly, the number of EPCs was not different between sedentary and voluntary exercised groups (n=5–8, all p>0.05). FACS analysis of cat++ and catn peripheral blood revealed no effect of catalase overexpression on the basal level of circulating EPCs (p=0.68, n=8). Inhibition of catalase by 3 week treatment with catalase inhibitor aminotriazole (670 mg/kg in drinking water) strongly reduced the number of endothelial progenitors in blood of sedentary catn, and to a lesser extend also in cat++(p>0.05, n=5–8). When mice with vascular specific overexpression of catalase were subjected to the forced exercise training, the number of circulating EPCs was strongly increased (n=4–8, p>0.05). Furthermore, exercise-induced increase of circulating EPCs was completely abolished in cat++ treated with aminotriazole.
Conclusion: Hydrogen peroxide, an important component of vascular oxidative stress inhibits exercise-induced mobilization of EPCs. Dysregulation of the reactive oxygen species balance in the bone marrow vascular niche likely contributes to the impairment of important stem cell-induced endogenous vascular repair mechanisms in cardiovascular disease.
155 Contribution of novel biomarkers to incident stable angina and acute coronary syndrome. The PRIME Study
JP Empana1; F Canoui-Poitrine1; G Luc2; I Juhan-Vague3; D Arveiler4; J Ferrieres5; P Amouyel6; A Bingham3; A Evans7; P Ducimetiere3
1INSERM U909 Sudden Death and CV Epidemiology, Villejuif, France
2INSERM U545 Department of Atherosclerosis, Lille, France
3INSERM U626 Department of Hematology, Marseille, France
4Strasbourg MONICA Project Department of Public Health, Strasbourg, France
5Toulouse MONICA Project INSERM U558 Department of Epidemiology, Toulouse, France
6Lille MONICA Project INSERM U744 Department of Epidemiology, Toulouse, France
7Queen's University of Belfast Department of Public Health, Belfast, Ireland
Aims: To compare whether or not novel inflammatory and hemostatic biomarkers are more predictive of definite incident acute coronary syndrome (ACS) than stable angina (SA).
Methods: We used data from the PRIME Study, a prospective cohort of 9758 asymptomatic middle-aged men recruited in Northern Ireland and France between 1991 and 1993. A nested case-control study was established with the baseline plasma sample of 292 incident cases and 570 matched controls. Odds ratios (OR) for SA and ACS (unstable angina, non Q wave and Q wave myocardial infarction) were estimated by conditional logistic regression analysis.
Results: After 5 years of follow-up, 114 incident SA and 178 ACS were validated. After adjustment for traditional risk factors, higher circulating levels of hs-CRP, ICAM1, interleukin 6 and interleukin 18 were equally predictive of SA and ACS (all p-values of ORs comparison>0.05). In contrast, elevated levels of fibrinogen, von Willebrand factor and possibly higher level of D-Dimers and lower level of Tissue Factor Pathway Inhibitor were associated with ACS only. The comparison of the ORs showed statistically significant difference for von Willebrand factor only (OR 4th against 1st quartile=3.28 (1.67–6.45) for ACS vs. 0.89 (0.39–2.03) for SA; p z-test=0.016).
Conclusion: This is the first population-based study assessing the respective contribution of novel biomarkers to incident SA and ACS, and suggesting that higher level of von Willebrand factor is significantly more predictive of incident ACS than SA.
156 Physical activity, mortality and cardiovascular disease: Is domestic physical activity beneficial?
E Stamatakis; M Hamer
University College London Epidemiology and Public Health, London, United Kingdom
Purpose: Intense domestic physical activity (IDPA), such as vigorous housework and gardening, is heavily promoted by public health campaigns for the prevention of cardiovascular disease (CVD) but this recommendation is not supported by evidence. The aim of this study was to determine the independent effects of participation in IDPA on the risk for CVD (CVD death or non-fatal episode).
Methods: Interviewer-administered questionnaires assessed participation in at least moderate intensity physical activity (IDPA, walking and sports/exercises) among a population-representative sample of 16,144 adults (7,211 men) aged =35 years living in Scotland (UK). The sample consisted of participants from the 1995, 1998 and 2003 Scottish Health Survey (SHS). SHS records were linked to hospital episodes and death records up to September 2006. Survival analysis assessed the independent relationship between frequency of participation in IDPA for at least 20 minutes a time (none, less than/greater than sex-specific median) and risk for CVD (fatal/nonfatal combined). Analyses were adjusted for confounders (participation in other physical activity types, body mass index, social class, long-standing illness, marital status, smoking, family history of CVD mortality, and alcohol consumption). To minimise the effect of reverse causality, respondents with a CVD event before baseline examination were excluded.
Results: Survey response rates ranged from 77% to 83%. Higher IDPA was inversely related with risk for all-cause mortality in both men (multivariate RR=0.77; 95% CI 0.61–0.99 for those in the top IDPA group compared to those with no IDPA) and women (0.66, 0.50–0.88). In both sexes, IDPA was unrelated to the risk for CVD (M: p=0.3; W: p=0.7). Total physical activity (including IDPA) was unrelated to CVD (M: p=0.2; W: p=0.4) but there was a clear dose-response effect when IDPA was excluded from the calculations (M: 0.75, 0.57–0.98; W: 0.65, 0.47–0.89 for top tertile). IDPA did not appear to confer any protection when older adults (=60 yrs) were considered separately.
Conclusions: IDPA makes a large contribution to overall physical activity levels but does not seem to offer primary protection against CVD. These results suggest that CVD-preventing physical activity promotion may need to focus on moderate intensity physical activities other than those performed in and around the household.
157 Variation in energy expenditure in locomotor activities: impact on achieving physical activity guidelines
J Hussey; S Langford; J O'Dwyer
Trinity College Physiotherapy, Dublin, Ireland
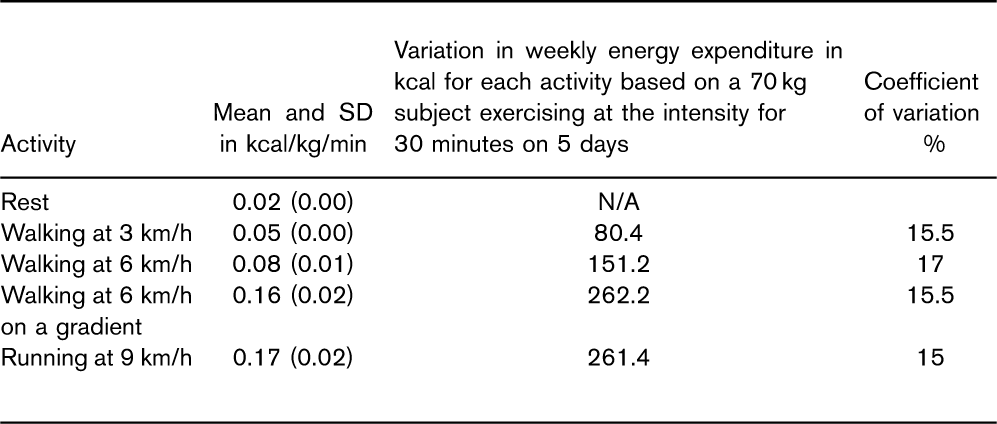
Purpose: Physical inactivity is responsible for much of the imbalance in energy expenditure leading to overweight and obesity. The current guidelines for physical activity are that adults accumulate a minimum of 30 minutes of at least moderate intensity physical activity on five days of the week. It has been found that the energy expenditure required to perform activities does change with age and pubertal status and is highly variable in adolescent girls. The aim of this study was to investigate the variation in energy expended in 30 minutes of walking/running at three different speeds and what this would translate into over one week if performed on five days.
Methods: Participants in this study were healthy young adults aged 18–30 years who were subjects in a study validating two accelerometers against the gold standard of energy expenditure. The activities evaluated were: walking at 3 km/h, brisk walking at 6 km/h, brisk walking at 6 km/h on an incline of 10% gradient, and running at 9 km/h. In addition resting energy expenditure was measured. Expired respiratory gases were collected and oxygen consumption was measured on a breath by breath basis using a mobile ergospirometry system.
Results: Twenty subjects participated in the study (10 M, 10 F). The mean (SD) age was 26.2 (3.7) years and BMI was 23.7 (3.2). Table 1 presents the data for the energy expended in kcal/kg/min for each activity measured and the estimated weekly variation in terms of kcal based on a 70 kg individual exercising at that speed for 30 minutes on five days of the week.
Conclusion: The variation in energy expenditure may influence the examination and prescription of physical activity. The effect of this variation means that some individuals may need to engage in more activity than others to achieve similar benefits.
Activity
Mean and SD in kcal/kg/min
Variation in weekly energy expenditure in kcal for each activity based on a 70 kg subject exercising at the intensity for 30 minutes on 5 days
Coefficient of variation %
Rest
0.02 (0.00)
N/A
Walking at 3 km/h
0.05 (0.00)
80.4
15.5
Walking at 6 km/h
0.08 (0.01)
151.2
17
Walking at 6 km/h on a gradient
0.16 (0.02)
262.2
15.5
Running at 9 km/h
0.17 (0.02)
261.4
15
158 Use of composite cardiovascular risk calculator before initiating statins for primary prevention
P Prashanth Raju; GK Rao; R Bhamidipati; H Rammohan; R Antony; G Davis
University Hospital Aintree Cardiology Dept., Liverpool, United Kingdom
Purpose: Statin therapy is a well established treatment for Hyperlipidemia. While initiating statin for primary prevention, apart from lipid profile, consideration should be given to age, sex, smoking history and blood pressure as per Joint British Societies (JBS) guidelines. JBS guideline recommends primary prevention treatment with statins for hypercholesterolemia if the calculated cardiovascular risk is more than 20% over 10 years. Aim of this study was to look into the appropriateness of Statin prescription in a tertiary centre.
Methods: We retrospectively analysed 500 consecutive patients who were prescribed statins over four month period. We excluded patients who met secondary prevention criteria. From electronic records and case notes, we collected the following parameters - sex, age, diabetes, total cholesterol, HDL, blood pressure and history of smoking. We used Joint British Societies Cardiovascular Disease Risk Prediction Chart to calculate 10 year composite risk. Prescription when risk of=20% (high risk group) or after 6 months life style modification when risk was between 10–19% was considered appropriate.
Results: 51 patients were treated for primary prophylaxis out of 500 patients (10%). Out of these, 7(14%) patients had 10 year composite cardiovascular event risk of more than 20% (high risk) hence receiving appropriate therapy. The mean cholesterol level was comparable in both high and low risk groups (6.07 and 5.3888 mmol/L respectively, P=0.22). The highest total cholesterol in the low risk group was 7.7 mmol/L.
Conclusion: Only 14% of patients received statin therapy appropriately for primary prevention and rest were prescribed inappropriately. Total cholesterol, TC: HDL ratios on itself were poor predictors of high 10 year cardiovascular event risk. The Joint British Societies Cardiovascular Disease Risk Prediction Charts or similar risk scoring tools should be used before initiating statins in primary prevention. This approach would not only identify the group of patients who would benefit most from statins but also limit the side effects due to inappropriate use.
159 Preparticipation physical activity screening: a unique opportunity for CV risk primary prevention and risk reduction programs
MT Lira1; ML Solivelles2
1Chilean Society of Cardiovascular Nursing, Santiago, Chile
2Santiago, Chile
A Preparticipation Evaluation Program (PPEP) for new members of one of the two biggest gyms in Chile was proposed and developed by Registered Nurses with experience in CV health.
Methods: A questionnaire to evaluate physical activity readiness, health status, demographic data and health related behaviors was applied to every new member of the gym. Blood Pressure (BP), Total Cholesterol (TC), Blood Glucose (BG) Body Mass Index (BMI) and Waist Circumference (WC) were measured using standardized methods. Members were stratified by the european CV risk chart model and referred for further medical evaluation based on decisional algorithms elaborated by a multidisciplinary team based on clinical guidelines. All of them also received personalized self-care nursing counseling tailored to findings. For the analysis, normal values were determined according to International Guidelines.
Results: Since this program started in March 2005, 1,725 persons have become new members, 121 of them preferred a direct MD staff evaluation. Data of 1,604 members (92.9%) is presented. Mean age was 34 ±10 y. and 51% were women. Unawareness of own values of BP, TC and BG was 13%, 41.6% and 15.6% respectively. The prevalence of CVRF was: current smoking 44%, abnormal TC 30%, abnormal Systolic BP 10%, abnormal Diastolic BP 7.1%, abnormal BG 12.8% and Obesity 11.8%. CV risk stratification in those who could be estimated by the model (age 30 or more, n=968) identified 8.1% members with moderate risk and 1% with high risk of developing a cardiovascular event within the next 10 years. A total of 41% of the members needed MD referral according to decisional algorithms: 35.5% of them to nutriologist due to metabolic disorders, 24.3% to internal medicine for respiratory or cardiovascular further evaluation and 40% to traumatologist.
Discussion: This PPEP enabled apparently healthy adults to be aware of their unknown CV risk parameters values, to identify people with untreated CVRF, including the diagnosis of Diabetes Mellitus in 4 unaware persons and also contributed to identify a significant number of persons that needed to start, adjust or restart abandoned treatment for another glucose disorders, dyslipidemia, hypertension or obesity. Current prevention guidelines preconize that every effort should be made to identify people at CV risk, to improve awareness and to implement risk reduction strategies. We believe that this scenario is an important opportunity for comprehensive and routine prevention programs that go beyond current settings.
160 Modification of caridac risk factors using a primary prevention programme-a six month follow up
C English; I Gibson; P Nash; J Crowley; K Daly
University College Hospital Cardiology, Galway, Ireland
Purpose: Coronary heartdisease is the single most common cause of death in Ireland. The aim of this study was to identify those athigh risk of cardiovascular disease in the community and whether once offprimary prevention advice would result in a significant reduction in modifiblerisk factors.
Methods: “Heart Smart” is an ongoing community based cardiovascular prevention programme in the west of Ireland. Individuals over forty years of age with one or morecardiac risk factors that had never had previous cardiovascular assessment were included in the programme. People who had attended their General Practitioner(GP) for a cardiac risk assessment over the previous year and whose blood pressure(BP) and lipid profile were at recommended target levels were excluded. The programme included an initial assessment of cardiac risk factors (lipid profile, bloodpressure, body mass index (BMI), glucose, and lifestyle risk factors). Onceoff lifestyle advice was givenusing motivational techniques. All patients with elevated lipids, blood pressure or glucose levels were referred to their GP and were invited to attend fora six month follow up assessment.
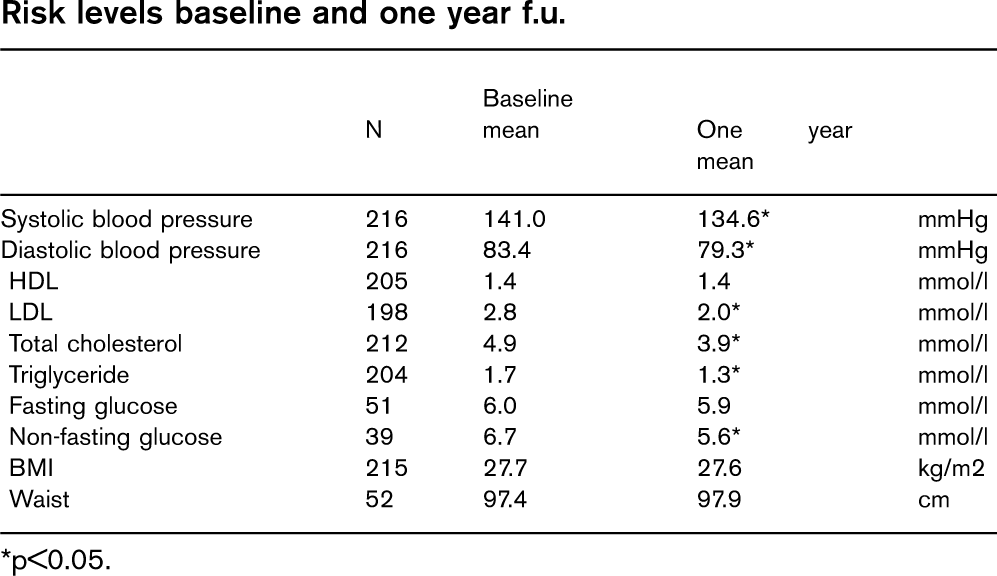
Results: 1928 risk assessments were conducted between 2005 and 2006. There was a high prevalence of risk factors among the population assessed; 40% had a BP>140/90 mmHg, 53% had a total cholesterol>5 mmol/l, 18% were smokers, 65% had a BMI>25> mmkg/m2 and 28% did not exercise. 14% ofindividuals were identified as having over a 5% 10yr risk of fatal CVD with 40% in the 1–4% risk group. GPfollow up was arranged for over 70% of individuals. From the total number of assessments, 695 high risk individuals were identified and invited for follow up. Of these, 436 attended with a response rate of 63%. 58% ofindividuals attended their GP as advised. At 6 month follow up, 67.7% showed overall reductions in cholesterol with 25% reaching target levels. Recommendedtarget BP levels were reached by 26%. The number of people participating inexercise doubled in six months with 71% reporting improvements in diet and 42% reporting improvements in exercise levels.
Conclusion: Although only one primary prevention advice session was conducted, significant reductions in BPand cholesterol levels, and increases in the number of participants in exercisewere seen at six month follow up. The results show that even if time and resources are limited for one thorough motivational session may result in significant improvements in modifible cardiovascular risk factors. The reluctance of a large number of individuals tofollow up with their GP highlights the importance of a community primary prevention programme.
161 Multi-factorial lifestyle intervention in the general population. Changes at five years follow-up in dietary habits and cardiovascular risk factors. The Inter 99 Study
UN Toft1; LK Kristoffersen2; S Ladelund1; C Lau3; C Pisinger1; L Ovesen4; K Borch-Johnsen4; T Jorgensen1
1Research Centre for Prevention and Health Glostrup University Hospital, Glostrup, Denmark
2Research Center for Prevention and Health, Glostrup, Denmark
3Steno Diabetes Center, Gentofte, Denmark
4Slagelse Hospital Department of Gastroenterology, Slagelse, Denmark
Purpose: To investigate the effect of an intensive lifestyle intervention on long-term changes in dietary habits and cardiovascular risk factors in a general population.
Methods: The study was a randomized controlled intervention study. From a general population of 61,301 individuals, aged 30 to 60 years, a random sample was drawn (n=11,708) and invited for a screening programme. Participation rate was 52% (6,091 of 11,708). Participants received individual life-style counselling. Individuals at high risk of ischemic heart disease were furthermore offered life-style counselling in groups. The intervention was repeated for high-risk individuals after one and three years. At five-year follow-up all participants were invited for health examination. A control group was drawn (n=5,264) from the remaining study population and followed by questionnaires. Dietary habits were measured by a validated 48-item food frequency questionnaire and changes were analysed by multilevel repeated measurement analyses with random effects.
Results: At five-years follow-up the intervention group compared to the control group had significantly increased their intake of vegetables (P=0.005) and unsaturated fats(P=0.02) and decreased the intake of saturated fats(P=0.003). No significant effect was found on fish and fruit intake at five-year follow-up. Increased intake of vegetables and fruits and decreased intake of saturated fat was significantly inverse associated with changes in Non-HDL plasma cholesterol, weight and waist circumference, adjusted for sex, age, changes in physical activity, smoking and energy intake.
Conclusion: The lifestyle intervention improved long-term intake of vegetables and fats in a general population and dietary improvements were inverse associated with biological and anthropometric risk factors.
162 Cardiovascular disease primary prevention strategies: the prevention paradox in CUORE Project
S Giampaoli1; C Donfrancesco1; S Panico2; D Vanuzzo3; M Ferrario4; G Cesana5; L Pilotto1; R Sega5; L Palmieri2
1Istituto Superiore di Sanita', Rome, Italy
2Universita' degli Studi Federico, Naples, Italy
3Centro per la Prevenzione Cardiovascolare, Udine, Italy
4Universita' degli Studi dell'Insubria, Varese, Italy
5Universita' degli Studi Milano-Bicocca, Monza, Italy
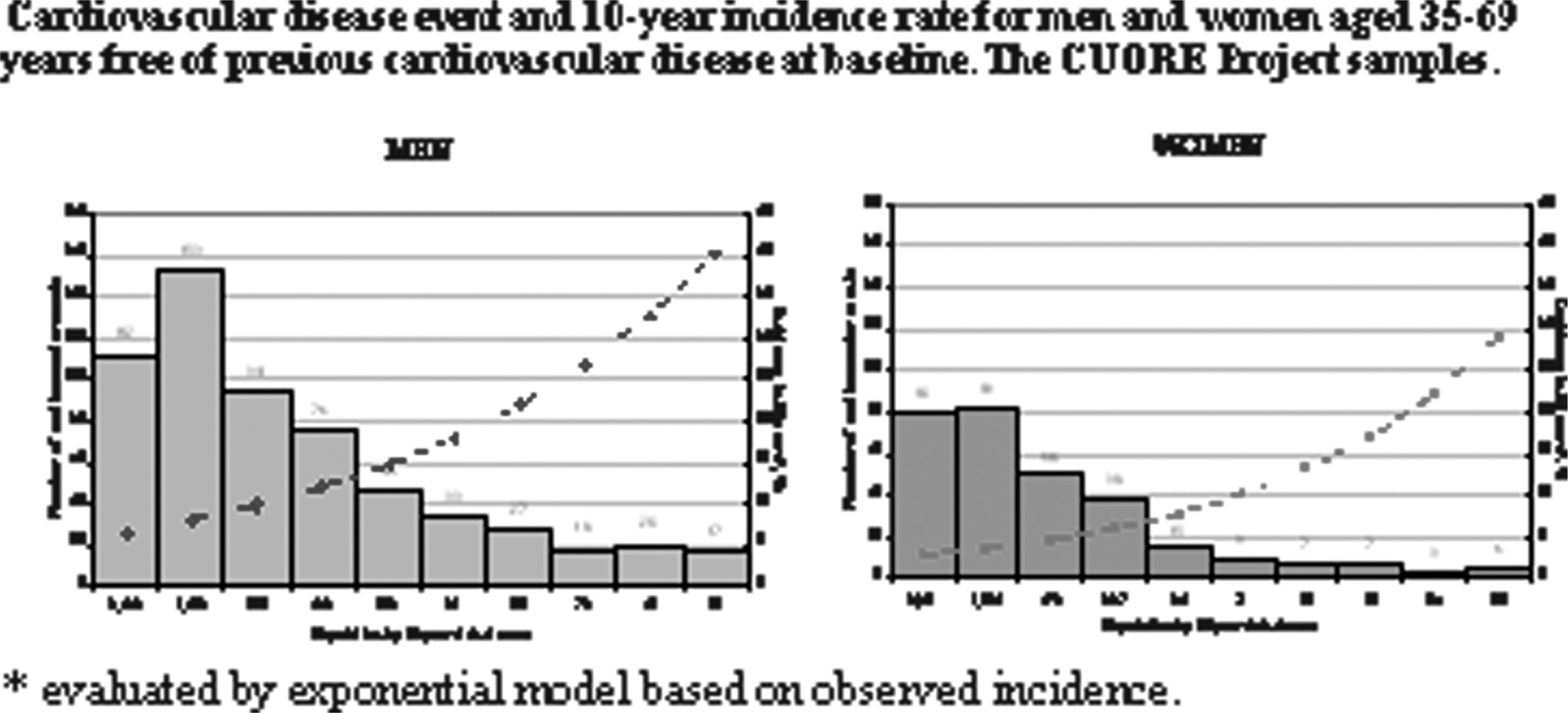
Purpose: The identification of cardiovascular disease risk is a key step to reduce modifiable risk factors in primary prevention, from lifestyle changes to pharmacological treatments. In Italy, risk score assessment has been recently introduced in primary care. The aim is to compare the reapplication of risk score to the population of the CUORE Project from which risk equations were estimated, and compare it with the event occurrence over 10 year of follow-up.
Methods: The CUORE Project equations for risk prediction were re-applied to the population of the CUORE Project (11,354 women, 5,898 men ages 35–69 without previous cardiovascular disease at baseline); risk was subsequently subdivided in ten equal classes and incidence in each class was computed.
Results: In the first risk class (lower risk), 112 events occurred among 3,433 men and 80 among 9,331 women, while in the last class 17 among 55 men and 6 among 22 women. Men belonging to last class, have risk 9.4 times higher than those in the first class; for women this ratio is 30.0. In absolute terms, the majority of events do not occur in individuals at high risk, but in those at intermediate or low risk; paradoxically, the latter, being more numerous than high risk individuals, develop, in absolute terms, a greater number of events (Figure).
Conclusion: Prevention strategies, to be fully effective, that means make CVD endemic-not epidemic, should address the whole population, not only high risk persons, and to increase as much as possible the prevalence of low risk reducing risk factors values through healthy lifestyle in those individuals who are still not high risk and keeping risk factors at a favourable level over lifetime in those at low risk.
163 The role of exercise test after primary percutan coronary intervention
J Bakai1; M Lukacs2; 1State Rehabilitation Institution Dept. of Cardiology, Sopron, Hungary
2State Rehabilitacion Institution Department of Cardiology, Sopron, Hungary
Background: The role of exercise test (ET) performed in patients with acute myocardial infarction (AMI) treated with primary percutan coronary intervention (PCI) is less well established.
The aim of our study was to evaluate the impact and aspect of performing of ET on the patient's rehabilitation process.
Materials and methods: Retrospectively collected data of patients with primary PCI taking part inpatient rehabilitation between January and July 2007. 212 patients were studied. The average age was 61?9 years. An ET was performed in 92 (43.4%) cases. The revascularization was complete in 131 (61.8%) patients, incomplete in 81 (38.2%) patients. Of patients with complete revascularization ET was performed to a greater extent than patients with incomplete revascularization (59.5% vs. 27.2.%). The most common reasons of inability to perform ET were heart failure in 31(25.8%) patients, significant non cardiac disease in 28 (23.3%) patients, arthrosis in 19 (15.9%) patients, advanced age in 36 (30.0%) patients, non compliance in 6(5.0%) patients.
Conclusion: In the modern era of aggressive reperfusion therapy the rehabilitation aspect of exercise testing often neglected, however it should remain a preferred option for the patients in the individually tailored rehabilitation.
164 Oxygen uptake kinetics after exercise and coronary artery disease
H Haruki Itoh1; T Maeda1; A Tajima2; K Omiya3; N Osada2; T Aizawa3; K Wasserman4
1Sakakibara Heart Institute Cardiology, Tokyo, Japan
2The Cardiovascular Institute Exercise Labo, Tokyo, Japan
3St. Marianna Univ. Cardiology, Tokyo, Japan
4Harbor-UCLA Medical Center Respiratory and Critical Care Physiology, Torrance, California, United States of America
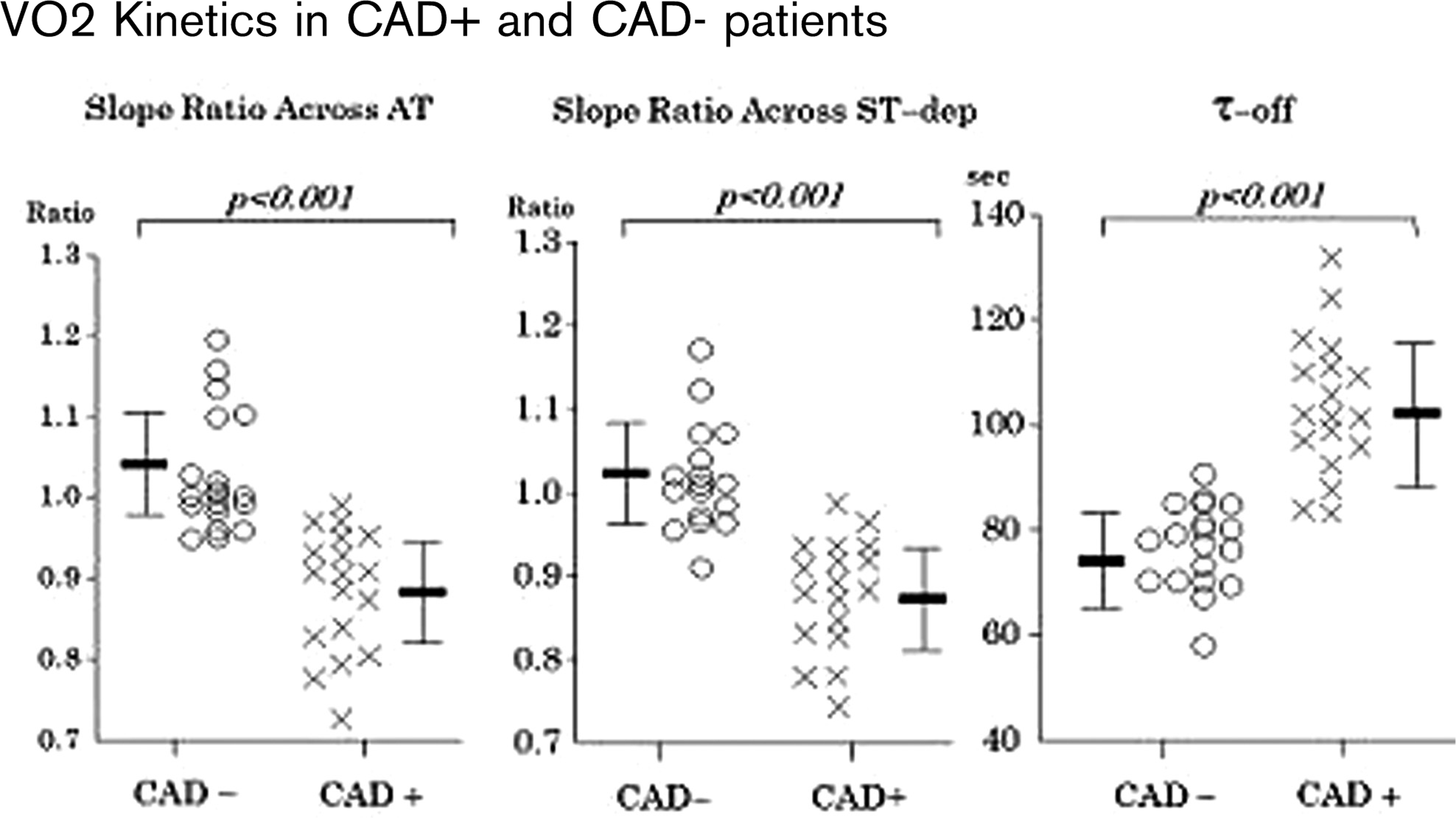
Objective: When myocardial ischaemia develops during exercise, oxygen uptake (VO2) fails to track work rate increase and the gas exchange changes reflect increased anaerobiosis. Our aim was to determine if the myocardial ischaemic would be accompanied by delayed recovery VO2 kinetics via the slowed exercise VO2 kinetics in patients with coronary artery disease (CAD).
Method: Thirty nine patients who showed significant ST depression during treadmill exercise underwent cardiopulmonary exercise testing (CPET) with a cycle ergometer. The change in increase in O2 uptake relative to increase in work rate (?VO2/?WR) from below to above anaerobic threshold (AT) and 11 mm ST depression point (ST-dep) were measured. Measurements performed are the ratio of ?VO2/?WR across AT and ST-dep transitions, the time constants of VO2 during recovery (Tau-off), and stress radio-isotope scintigraphy and coronary angiography were done within 2 weeks after CPET. Patients were divided into CAD positive (CAD+) and CAD negative (CAD-) groups, based on coronary angiography.
Results: In CAD+ patients, ?VO2/?WR decreased above AT and ST-dep in contrast to CAD-patients. The ratio of ?VO2/?WR above compared to below AT or ST-dep were reduced in CAD+. Tau-off in CAD+ (103.1 ±13.0 sec) was greater than that of CAD- (76.5±8.7 sec) and showed positive correlations to the ischaemia score from radio-isotope scintigraphy. These parameters improved in patients who underwent coronary bypass surgery.
Conclusions: Exercise and recovery VO2 kinetics were slowed when myocardial ischaemia was provoked by exercise. Measurement of exercise and recovery VO2 kinetics improve the accuracy of the exercise ECG diagnosis of CAD.
VO2 Kinetics in CAD+ and CAD- patients
165 Shuttle walk test predicts completion of a cardiac rehabilitation programme and subsequent cardiovascular admissions at 1 year
JM Warnock1; P Pardeep Jhund2; P Macintyre1
1University of Glasgow Department of Sports and Exercise Medicine, Glasgow, United Kingdom
2University of Glasgow Heart Failure Research Group, Glasgow, United Kingdom
Purpose: Assessment of exercise capacity is important prior to commencing a cardiac rehabilitation programme (CR) after a myocardial infarction. Whilst maximal symptom limited treadmill exercise testing (ETT) provides accurate prognostic information it is relatively expensive to conduct. The incremental shuttle walk test (SWT) is a possible inexpensive and reproducible alternative. We sought to determine if performance in the SWT predicted completion of CR and subsequent cardiovascular readmissions to hospital at 1 year following completion of CR.
Methods: This study examined 891 men and 410 women in the Have a Heart Paisley Study in Paisley, UK, who completed a SWT prior to CR. These individuals had undergone ETT and had failed to achieve 8 metabolic equivalents. The SWT was conducted according to the standard published protocol. Subsequent cardiovascular admissions (myocardial infarction, angina, heart failure and chest pain) recorded in the Scottish Morbidity Record Scheme (which records all discharges from hospitals in Scotland) for each patient in the cohort were retrieved using the corresponding ICD-10 codes. Age and sex adjusted logistic regression models were used to determine if performance in the SWT predicted completion of CR. Cox's regression was used to determine whether performance in the baseline SWT predicted cardiovascular admissions to hospital at 1 year.
Results: The mean age of men and women was 61 and 64 years respectively (p=0.2). Baseline metabolic equivalents achieved during ETT and number of shuttles walked during a pre-cardiac rehabilitation SWT were positively correlated (R=0.49, N=505, p>0.0001). 289 patients did not complete the CR. The age and sex adjusted odds of completing CR increased with increasing number of shuttles walked in the pre rehabilitation SWT, OR 1.02 (95%CI 1.01–1.03, p>0.0001). During 1 year follow up, 139 individuals were readmitted for a cardiovascular cause. After adjustment for age and sex, increasing number of shuttles walked in the pre-cardiac rehabilitation SWT led to a reduction in the hazard of readmission at 1 year, HR=0.98 (95% CI 0.97–0.99, p>0.0001) per shuttle walked.
Conclusion: We have demonstrated that performance in the SWT prior to commencing a CR predicts not only completion of the CR (independently of sex and age), but also predicts cardiovascular readmissions within 1 year of the completion of the programme. This finding may allow the SWT to be used to identify moderate and low risk groups who may be suitable for home or community based cardiac rehabilitation programmes.
166 Effects of exercise training on prognostics indices of cardiopulmonary exercise testing
G Deboeck; P Lejeune; M Lamotte; S Huez; P Van Den Borne; D Decanniere; JP Degaute; M Renard; Brussels, Belgium
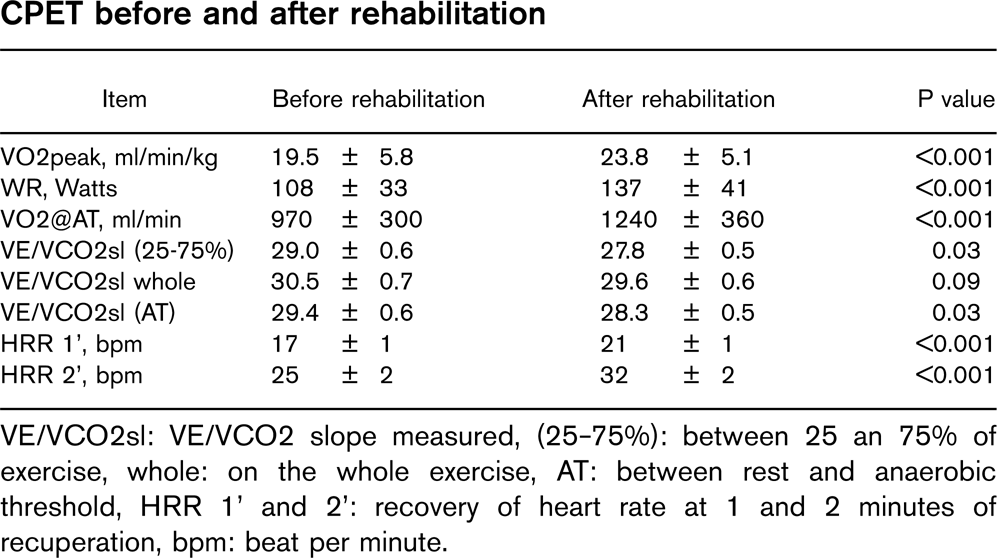
Purpose: Exercise training is known to improve work rate (WR), peak oxygen consumption (VO2peak) and oxygen consumption at anaerobic threshold (VO2@AT) that are crucial and classical indices of survival and quality of life in heart disease. Since a couple of years, other indices like Heart rate recovery (HRR) and VE/VCO2 slope in chronic heart failure were shown to be good indicators of survival. We so aimed to know whether these indices were modified by exercise rehabilitation in cardiac patients.
Methods: 76 patients (58±11 years, 60 males) were referred for exercise rehabilitation (high intensity interval training and resistive training, 3 times a week for a period of 3 months, 39±13 sessions) after myocardial infarct, coronary artery bypass or valvular surgery replacement, or chronic heart failure. Maximal cardiopulmonary exercise testing (CPET) was performed before and after rehabilitation. VO2peak, peak WR and VO2@AT were assessed as primary indices of improvement. HRR after 1 and 2 minutes of CPET, VE/VCO2 slope measured between 25 and 75% of exercise test, between rest and anaerobic threshold and on the whole exercise test were measured as new indices of survival.
Conclusion: This study confirm the evidence of a benefit on exercise capacity from physical rehabilitation (peak WR, VO2peak and VO2@AT) in cardiac patients. We also note significant changes in VE/VCO2 slope and HRR. The importance of those changes in relationship to prognosis has to be further evaluated.
CPET before and after rehabilitation
Item
Before rehabilitation
After rehabilitation
P value
VO2peak, ml/min/kg
19.5 ± 5.8
23.8 ± 5.1
>0.001
WR, Watts
108 ± 33
137 ± 41
>0.001
VO2@AT, ml/min
970 ± 300
1240 ± 360
>0.001
VE/VCO2sl (25–75%)
29.0 ± 0.6
27.8 ± 0.5
0.03
VE/VCO2sl whole
30.5 ± 0.7
29.6 ± 0.6
0.09
VE/VCO2sl (AT)
29.4 ± 0.6
28.3 ± 0.5
0.03
HRR 1', bpm
17 ± 1
21 ± 1
>0.001
HRR 2', bpm
25 ± 2
32 ± 2
>0.001
VE/VCO2sl: VE/VCO2 slope measured, (25–75%): between 25 an 75% of exercise, whole: on the whole exercise, AT: between rest and anaerobic threshold, HRR 1' and 2': recovery of heart rate at 1 and 2 minutes of recuperation, bpm: beat per minute.
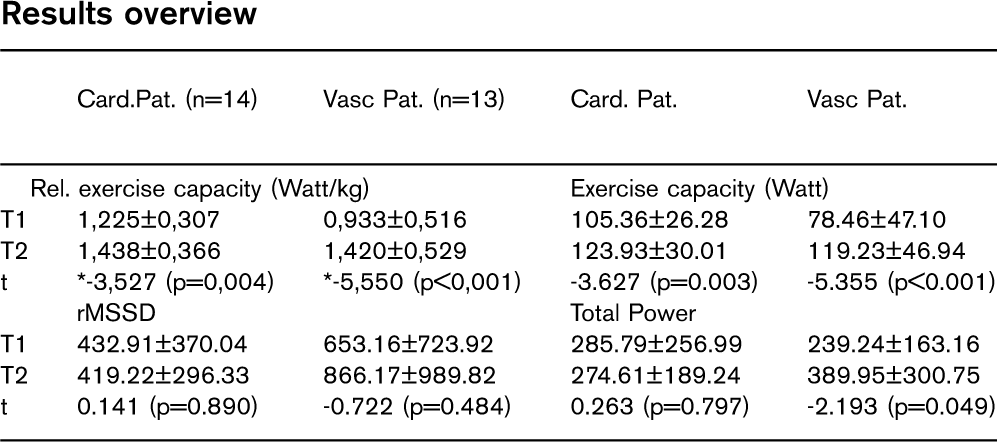
167 Effects of a 21-day-ambulatory rehabilitation program on heart rate variability in either cardiac or vascular patients
J Latsch1; JA Wegener2; B Bjarnason-Wehrens2; DB Gysan3; S Tuerk3; HG Predel3
1German Sport University Institute of Cardiol, and Sportsmedicine, Cologne, Germany
2German Sports University Institute of Cardiology and Sportsmedicine, Cologne, Germany
3AmKaRe Cardiac Rehabilitation, Cologne, Germany
Topic: Heart Rate Variability (HRV) represents functional aspects of the autonomic nervous system (ANS). It also has proven to be a strong predictor of acute cardiac death or exacerbation. Our topic was to evaluate a change of HRV parameters in patients of a cardiologic or angiologic ambulatory rehabilitation program.
Methods: A total of 27 patients in a three week ambulatory rehabilitation program were examined. 14 cardiac patients (CP) and 13 vascular patients (VP) (f=5; m=22, Age 59,15yrs; height 172,8 cm, weight 85,8; BMI 28,6 kg/m). HRV Measurement was performed by using “supine-upright-supine” test before and after the program.
Results: There were no significant changes in anthropometric. The patients exercise capacity improved significantly in CP (p=0.003) and in VP (p>0.001). HRV parameters showed mostly tendencial but not singnificant improvements: NN time elevated from 0.883±0.123 ms to 0.893±0.156 ms (p=0.711) in CP and 0.824±0.120 ms to 0.837 ±0.141 ms (p=0.547) in VP. RMSSD showed a tendential increase in VP and Total Power increased significantly in VP. LF/HF ratio changed slightly towards LF-portion (p=0.328 in CP and p=0.826 in VP). There was a positive correlation between increased exercise capacity and NN elevation (r=0.438) which was even more remarkable in VP (r=0.577).
Discussion: Rehabilitation strategy caused functional and medical improvements in both patient groups The averagely older VP showed higher profits. HRV did only improve reservedly. Adjustments of the ANS did not happen within a short period of three weeks. Patients would probably show improved HRV results after a continous lifestyle change over two or three month.
Introduction: Hypertension is a well-known risk factor for cardiovascular disease. The 2007 European Guidelines recommend reducing blood pressure levels below 140/90 mmHg (130/80 mmHg for diabetics). Confirmation of hypertension is necessary before embarking on life-long medication that may cause unwanted side effects. Accurate diagnosis and monitoring of hypertension depends on reliable blood pressure measurement. Early intervention, patient education and lifestyle modification are essential for effective management of hypertension. Ambulatory blood pressure monitoring (ABPM) provides more representative values of BP than clinical measurements and makes it possible to determine the efficacy of treatment. This study explores the benefit of 24-hour ABPM in assisting CR staff with decisions regarding the implementation and modification of antihypertensive therapy.
Methodology: The indications for ABPM included a clinical BP>140/90 mmHg (>130/80 mmHg for diabetics) consistently over a period of 3 weeks pre and post exercise. ABPM was performed on a sample of 46 patients, 72% male and 28% female, mean age 63 years over a 10 month period. Space Labs software analysed the results.
Results: Of the total sample, 76% (n=35) had pre-existing hypertension and 20% (n=9) had diabetes mellitus. ABPM recorded normal blood pressure results for 33% (n=15), avoiding unnecessary changes in anti-hypertensive treatment. White coat hypertension was diagnosed in 7% (n=3). Medication change was required in 59% (n=27). Follow up included clinical BP monitoring until completion of CR. Post medical intervention, follow-up clinical BP measurements demonstrated 26% (n=12) BP>140/90 mmHg, 15% (n=7) of diabetic patients, BP>130/80 mmHg. As a result 41% (n=19) had repeat ABPM. 58% (n=11) were controlled and 42% (n=8) required further medication changes. Follow up for these 8 patients included one referral to GP and the remainder with general cardiology clinics at the hospital. 3 were rebooked for ABPM.
Conclusion: Fifty nine percent of attendees in Phase 3 CR over a 10 month period demonstrated uncontrolled hypertension despite anti-hypertensive medication. 70% were controlled with medication changes, lifestyle advice and follow up. This study demonstrates the clinical value of ABPM in CR not only in selecting patients for treatment but also in assessing the effects of treatment.
169 Prevalence and improvement of impaired glucose tolerance in patients with coronary heart disease during a short term inpatient rehabilitation program
U Eherer; M Wonisch
Cardiac Rehabilitation Center, St. Radegund, Austria
Introduction: Patients with coronary heart disease (CHD) have a high prevalence of undiagnosed glucose intolerance (IGT) or diabetes mellitus. On the other hand, long term lifestyle modification can improve glucose metabolism. It is unclear, however, if short term lifestyle interventions has any effect on IGT or diabetes mellitus. Aim of our study was to show the prevalence of IGT in patients with CHD and to examine the effect of a short term inpatient rehabilitation program in patients with CHD and IGT.
Methods: 235 consecutive patients with CHD without known diabetes mellitus and normal fasting glucose passed an oral glucose tolerance test (OGTT) according to the WHO criteria. Then all patients underwent an inpatient rehabilitation program consisting of an endurance training program combined with a low cholesterol diet. At the end of the program OGTT and exercise test were repeated.
Results: Thirtyfour patients (15%) had an IGT, 4 patients (=0.02%) were identified as diabetics. After 18±4 days of the inpatient rehabilitation program we observed a significant (p>0.05) improvement of the 2h-value of the OGTT (164±25 vs. 151±288 mg/dl), a reduction in weight (80±14 vs. 78±13 kg) and an increase in the maximal workload (87±34 vs. 111±33 W) of the exercise test. Three of the 4 (75%) identified diabetics changed to IGT, 12 patients with IGT (35%) normalised their glucose tolerance.
Conclusion: Our findings confirm the high prevalence of IGT in patients with CHD and normal fasting glucose. Furthermore, our study show that even a short-term inpatient rehabilitation program can improve a pathological glucose metabolism in these patients substantially.
170 Effect of NT-pro BNP level on results of six-month cardiac rehabilitation in elderly patients with previous ACS
M Sobieszczanska1; D Kalka1; A Bak2; A Chorebala1; E Metner1
1Wroclaw Medical University, Wroclaw, Poland
2Cardiac Rehabilitation Center ‘Medar’, Wroclaw, Poland
Purpose: Analysis of relation between NT-pro BNP serum level measured 72 hours after the ACS occurrence and change of effort tolerance induced by cardiac training in elderly patients.
Methods: Ambulatory six-mont rehabilitation comprised a 45-min cycloergometer training (ERGOLINE system) with the 4-min interval loads (50% of those established during the ECG exercise testing) increasing with time and broken by the 2-min rest with 10 Watt load (3x/week), with generally improving exercises (2x/week). Serum level of NT-pro BNP was determined using Elycsys 1010 and Elycsys 2010. E.170 analyzers.
Material: A group of 75 patients (34 females and 41 males) at age of 69–72 years (mean: 72.4±3.4) with previous ACS. Results: It was shown that there was no statistically significant correlation (r=0.139; NS) between improvement of effort tolerance, assessed as a prolongation of exercise treadmill test duration, and serum level of NT-pro BNP measured 72 hours after ACS in elderly patients.
171 EuroSCORE as a predictive factor for different types of postoperative care and cardiac rehabilitation after cardiac and thoracic aortic surgery
V Goeber; H Saner; JP Schmid; T Carrel
Inselspital, Bern, Switzerland
Background: The number of older patients (pts) and pts with significant comorbidities in cardiac surgery is increasing whereas improved surgical methods and postoperative medical care allow for earlier QJ; discharge. The aim of this study was to assess predictive characteristics leading to different types of postoperative care and cardiac rehabilitation (cr) after cardiac surgery.
Methods: In this prospective cohort study data of all cardiac and thoracic aortic surgery pts over a period of 6 months were evaluated before, during and after cardiac and thoracic aortic surgery. EuroSCORE has been used to predict perioperative mortality, intensity of postoperative care and cr. According to clinical progress and complications we stratified pts on postoperative day 3 to 7 for treatment in a low intensity care unit (defined as: mobile within pts room, none drainage, cardiac monitoring or central venous line, blood pressure check twice/d, infusion with no more than 2 drugs, ward round 3-times per week).
Results: Complete data from 475 pts (345 males, 130 females; mean age 65.1 years) have been collected. Preoperative EuroSCORE was in the range of 0–16 (mean 5.5). 269 (56.6%) of 475 pts could be treated in a low intensity care unit. Nine of these pts suffered from postoperative complications (atrial fibrillation and flutter, pericardial effusion, mild postoperative delirium) but made a good recovery. EuroSCORE was highly predictive for low complication rate in pts treated in the low intensity care unit (p>0.05) and for subsequent ambulant cr (p>0.05). Furthermore EuroSCORE >4 was predictive for the need of inpatient cr (p=0.002).
Conclusions: EuroSCORE is a very helpful tool to predict both intensity of postoperative care and cr in pts undergoing cardiac surgical procedures.
172 The changing of the cognitive functions of the patients in the early fase after ACBG operation
K Szalay; E Simon; E Princz
State Rehabilitation Center Cardiorehabilitation Department I., Sopron Hungary
Purpose: The basic fact in our research was, that in the early phase after operation (8–10 days) the self-sufficiency and the motion is quickly impoving, meanwhile the power of memory, the orientation in place and time is still incomplete.
Methods: We searched the cognitive functions of the researched patients with using the Modificated Mini Mental State Examination (MMMSE) + Cortical status (C) test on the 8±2 day after operation (at the beginning of the rehabilitation program) and on the 30±2 day after operation (at the end of the rehabilitation program).
Men and women in the age of 45–65 were participating in the search. We don't search patients after the age of 65, because the risk of impairment in their cognitive funcions (dementia) is extremely high between the average population due to special literature facts.
During the rehabilitation program the patients participate in:
• Individual and small group exercise trainings
• Supportive psychological therapy
• Lifestyle guidance after risk stratification
• Regular individual and small group education
• Daily routin complation and controllation
We divided the searched patients into two groups: ECC group and off-pump group.
We compared our results to the similar age and gender cronic heart disease patients without heart operation.
Results: 1. The cognitive functions of the ACBG operated patients were impaired in the first days after op.
2. Remarkable improvement in the cognitive functions was showed during rehabilitation program, but it isn't yet on the average level of the similar age and gender cronic heart disease patients.
3. It showed differences between the ECC group and the off pump group: by the off pump group established less level of impairment of cognitive functions, and greater improvement.
Conclusion: The rehabilitation has a good influence not only on the physical power, but on the change of the cognitive functions too. Persumably, the surgery on the beating heart (off-pump) is affecting the cognitive functions less negative and their recovery is more spectacular in the first weeks after op.
Plans in the future: Working together with heart surgery departments to measure the cognitive functions before ACBG op. Compared to this result is definable the changing of the cognitive functions at the early postoperative fase (8 days after surgery), at the end of the rehabilitation program (30 days after surgery) and late postoperative phase (6 month, 1 year, 2 years, 3 years after surgery).
173 Sexual dysfunction before and after cardiac rehabilitation
J Schumann; M Zellweger; M Divalentino; S Piazzalonga; A Hoffmann
University Hospital Basel Suisse Cardiology, Basel, Switzerland
Background: Sexual dysfunction is common in cardiovascular patients. The aim of our study was to assess sexual function during cardiac rehabilitation in relation to various medical variables.
Methods: Analysis of all patients (pts) participating in a 12-week exercise-based outpatient cardiac rehabilitation program (OCR) between april 1999 and august 2007. In addition to medical history and risk factors, exercise capacity (ExC) was measured before and after OCR. Sexual function was assessed using a standardized questionnaire before and after OCR (5 items: problems with or change of sexual activity, decrease in libido, problems due to exertion during intercourse, problems with virility or orgasm, no activity at all).
Results: Of the 2032 pts, 959 were excluded because of incomplete data. Of the remaining 1073 pts (15% female, mean age 62) 2/3 had PCI, 1/4 had coronary bypass surgery (CABG) and 1/10 had valvular surgery. The prevalence of cardiovascular risk factors was: hypertension 55%, hyperlipidemia 69%, diabetes 15%, smoking 44% and family history 36%; 90% were on betablockers.
No sexual activity at all was indicated by 23% of the pts. No problems with sexual activity was indicated by 42% at baseline and 40% after OCR. Male pts showed an increase of specific problems (virility and orgasm) during OCR from 18 to 23% (p>.0001).
In a stepwise multivariate regression analysis we found the following independent positive and negative predictors of sexual problems after OCR: female gender (hazard ratio (HR) 0.569, 95% confidence interval (CI) 0.373–0.868, p>.009); CABG (HR 1.457, CI 1.058–2.005, p=.021); age (HR 1.033, CI 1.018–1.048, p>.0001); baseline ExC (HR 0.995, CI 0.990–0.999, p=.022); and improvement of ExC (HR 0.994, CI 0.989–0.999, p=.027).
There was no relation of LVEF or diabetes to sexual function.
Conclusion: Sexual dysfunction is present in over half of the patients undergoing outpatient cardiac rehabilitation with no overall improvement during OCR. Age, gender, CABG, ExC and its improvement are independent predictors of sexual function after OCR.
174 Influence of exercise training on physical capacity, autonomic cardiac regulation and inflammatory markers in post CABG patients
M Kosydar-Piechna; M Bilinska; B Foss-Nieradko; J Wolszakiewicz; R Piotrowicz
Institute of Cardiology Cardiac Rehabilitation, Warsaw, Poland
Background: There is literature suggesting that regular training improves exercise capacity and prognosis in patients with chronic angina. However, the influence of aerobic, short-lasted training on physical capacity, heart rate variability (HRV) and inflammatory markers in post-CABG patients has not been extensively studied.
Methods: Sixty males, mean age 55±6 ys, mean 2 months after CABG, were randomized to either 6 weeks of exercise training, three times a week, at 60–70% of maximal estimated heart rate (training group, TG, n=30) or to a control group (n=30). At baseline and at the end of the study the following examinations were performed: (1) exercise stress test; (2) 24 h Holter monitoring; (3) plasma levels of inflammatory markers.
Results: Physical capacity increased significantly only in TG pts: exercise duration from 759±98 to 827±76 sec (p>0.01) and max workload in METs from 7.6±1.4 to 8.1±1.5 (p>0.05). Only in TG pts mean 24-h heart rate decreased significantly from 69±7 to 62±8 beats/min (p>0.05). However, there were no significant differences in time (SDNN: 132.65 vs 128.9 ms, p=ns) and frequency domain indexes (LF: 255.41 vs 253.56 ms2, p=ns; HF: 179.89 vs 180.41 ms2, p=ns) of HRV in both groups. Moreover, only in TG pts significant improvement in the following inflammatory markers was found: leukocyte count (7.3 vs 6.2 x109/l, p>0.01), sedimentation rate (13.2 vs 6.88 mm/h, p>0.05) and fibrinogen (4.1 vs 3.3 g/l, p>0.05). C-reactive protein level tended to be lower in the TG group (0.57 vs 0.166 mg/l, p=0.056).
Conclusion: (1) Short period of aerobic training improved physical capacity and reduced levels of proinflammatory risk factors in post-CABG patients. (2) Autonomic tone did not change significantly after training.
175 Cardiac rehabilitation vs. immediate hospital discharge after acute coronary artery disease (CAD): a prospective 12 month follow-up study
B Schwaab1; A Waldmann2; A Katalinic2; B Poppe3; A Sheikhzadeh4; H Raspe3
2Institut of Social Medicine University of Schleswig Holstein, Luebeck, Germany
3General Practioner General Medicine, Luebeck, Germany
4Segeberger Kliniken Cardiology, Bad Segeberg, Germany
Purpose: The evidence of cardiac Rehabilitation (Rehab) is not yet fully settled as even recent meta-analysis predominantly included smaller and older studies without acute revascularisation and without modern secondary preventive medication.
Methods: In a multicentre randomised controlled trial, 1.474 patients (pts.) with acute CAD were included to investigate the impact of telemedicine on chronic CAD: 679 pts. were included immediately at discharge from the hospital (Hosp), 795 pts. after three week in-patient Rehab. All pts. had acute coronary angiography and were followed for one year. As Hosp pts. were included 11,3±3 days (median 11) earlier than Rehab pts., events in the Hosp group were counted from day 12.
Results: At entry, Rehab pts. were older (64±10 vs. 62±10 years; p>.001), had more congestive heart failure (64 vs. 40%; p>.001), three vessel disease (51 vs. 31%; p>.001), carotid stenosis (8 vs. 4%; p=.004), renal insufficiency (10 vs. 7%; p=.036) and a lower LV-EF (54 vs. 58%; p>.001). Telemedicine device prescription, gender, atrial fibrillation, peripheral artery disease, diabetes, obesity, hypertension, education, marital and social status were similar in groups. Rehab pts. had more β-blockers (88 vs. 75%; p>.001), ACE-inhibitors (81 vs. 70%; p>.001), lower LDL-C (102±35 vs. 121 ±477 mg/dl (median 96 vs. 116); p>.001) and a higher proportion of non-smokers (44 vs. 38%; p=.024). There was no difference in platelet inhibition, anticoagulation and statin therapy (81 vs. 79%). The primary combined endpoint of all-cause mortality, acute myocardial infarction (AMI), coronary revascularisation and hospitalisation occurred in 32.6% of Rehab pts. and in 38.7% of Hosp pts. (p=.014; absolute risk reduction (ARR) 0.0615, relative risk reduction (RRR) 16%, number needed to treat (NNT) 17). AMI (1.8 vs. 3.8%, p=.015; ARR 0.0207, RRR 54%, NNT 49) was reduced. Revascularisation (4.2 vs. 5.4%), hospitalisation (33.6 vs. 38.0%) and all-cause mortality (2.1 vs. 2.4%) were similar between groups. After multivariate analysis, the primary endpoint was still significant: OR 0.716 (95% CI 0.575–0.892; p=0.003) giving a RRR of 28% in favour of Rehab therapy.
Conclusion: Although Rehab pts. were older and sicker at entry, cardiac Rehab substantially reduced relevant clinical endpoints within one year. With a very low NNT, cardiac Rehab is highly effective and should be advised to all suitable patients with acute coronary artery disease.
176 Effect of comprehensive cardiac rehabilitation versus usual care on myocardial infarction. Three years results of the DANREHAB Trial
ADO Zwisler1; AMB Soja2; S Rasmussen3; M Frederiksen1; C Gluud4; L Iversen1; B Sigurd1; M Madsen3; J Fischer-Hansen1
1Bispebjerg Hsopital Cardiac Rehabilitation Unit, Copenhagen, Denmark
2Bispebjerg Hospital Cardiac Rehabilitation Unit, Copenhagen, Denmark
3National Institute of Public Health, Copenhagen, Denmark
4Rigshospitalet Copenhagen Trial Unit, Copenhagen, Denmark
Purpose: Literature propose that aggressive focus on modification of risk-factor-related lifestyle as part of comprehensive cardiac rehabilitation can help patients to achieve behavioural changes leading to decrease in the long-term coronary recurrence risk. In a randomised clinical trial on comprehensive cardiac rehabilitation we found improvement in lifestyle and risk factors after 12-months and reduction in total acute bed-days, but no effect on death, myocardial infarction, or first-time readmission due to heart disease. We now report the effect of comprehensive cardiac rehabilitation after 3 years.
Methods: A centrally randomised clinical trial comparing cardiac rehabilitation with usual care. Cardiac rehabilitation was offered as a comprehensive, individually tailored, multidisciplinary program in accordance with current guidelines. Of 1614 eligible patients 770 were randomised (47%): 380 to cardiac rehabilitation and 390 to usual care. Mean age was 65 years; 36% were women; 12% had congestive heart failure, 58% had ischaemic heart disease and 30% had high risk for ischaemic heart disease. A composite register-based primary outcome measure at 3 year follow-up included total mortality, myocardial infarction, or first acute readmission due to heart disease. We used Cox-regression to analyse time-to-event, and Poisson-regression to analyse length-of-stay.
Results: We found no significant difference in the composite register-based outcome measure at 3 year follow-up (46.1% vs. 48.7%; RR 0.92, 95% CI 0.75 to 1.13; p=0.40). During the 3 year follow-up myocardial infarction occurred among 3.7% in the cardiac rehabilitation group and 6.9% in the usual care group (RR 0.52, 95% CI: 0.28 to 1.00, p=0.049). There was no significant difference when looking separately at the two other outcome meassures: total mortality and time to first acute read-mission due to heart disease. Among the 73% patients who where readmitted during the 3 year period, the cardiac rehabilitation group tended to have a non-significantly lower total number of readmissions (1262 vs. 1467; p=0.10), and significantly fewer total acute bed-days (4974 vs. 7237, p=0.04).
Conclusion: Comprehensive cardiac rehabilitation seems to significantly reduce myocardial infarction and total acute bed-days compared with usual care. The lower event rate of myocardial infarction after 3 years may reflect the effect of lifestyle changes and improved risk factor control demonstrated at 12 month. The patients will be followed long term to examine whether the effect on myocardial infarction translates into beneficial effect on the primary outcome as well.
177 Cardiac rehabilitation outcome in primary PTCA and CABG
Z Eysymontt1; U Kniezyk2; Z Baczek1; A Bukowska-Kluska1; E Blaszczak3
1Silesian Centre of Rehabilitation Cardiac Rehabilitation Department, Ustron, Poland
2Silesian Centre of Rehabilitation Cardiac Rehabilitation Department, Ustron, Poland
3Silesian Medical University Medical Biophysics Department, Katowice, Poland
Purpose: The aim of the study was to estimate the impact of a 2–3 week inpatient cardiac rehabilitation program on physical capacity, quality of life and symptoms of depression and anxiety. Another aim was to compare 2 groups – after primary PTCA and after CABG. The third aim was to estimate the impact of ejection fraction, age and awaiting time (from intervention till rehabilitation) on rehabilitation outcome.
Methods: 143 inpatients in two intervention groups: 75 patients after primary PTCA (20 women, 63 men; aged 37–74) and 68 patients after CABG (13 women, 68 men, aged 28–77) with measured ejection fraction (EF) where evaluated during a stress test (physical capacity - PC) and with 2 quality of life questionnaires – SF-36 health survey (only CABG group), MCNEW Quality of Life after Myocardial Infarction (QLMI) and with the Beck scale of depression (BECK) and Spielberger scale of anxiety as a state (STAI) during the first 3 days. The Rehabilitation programme (2 weeks - PTCA, 3 weeks - CABG) included individually chosen physical excercise, psychoeducation and relaxation training. Two days before departure all the patients where examined with the same questionnaires and scales. CABG patients were also examined during the second stress test.
Results: In CABG group PC increased (23% in METS, 31% in WAT, 25% longer stress test), SF-36 increased 9%, QLMI increased 17%, BECK decreased 22% and STAI decreased 3%. In PTCA group QLMI increased 19%, BECK increased 2%, STAI decreased 8%. The differences in changes of QLMI, BECK, STAI between both groups are insignificant due to large ingroup variability. The outcome in CABG group was independent from the EF, age and awaiting time. In PTCA group EF correlated significantly with QLMI outcome (−0,28) and with BECK outcome (−0,25).
Conclusion: The rehabilitation programme helped to increase patients' physical capacity, health and heart related quality of life, to manage with depression and anxiety regardless of the kind of intervention. The outcome is independent from age and awaiting time. The patients after PTCA with a higher ejection fraction had lower outcomes in heart related quality of life and depression symptoms. Thus, inpatient cardiac rehabilitation brings fewer effects to patients with a high physical capacity. More examination should be done about group differences in rehabilitation outcomes, ingroup variability and rehabilitation programme for high physical capacity patients after primary PTCA.
178 The effects of early cardiac rehabilitation program acute myocardial infarction
R Rudko; J Smialek; M Pasowicz; R Kolasa-Trela; I Witkowicz; M Misiak
The John Paul II Hospital, Krakow, Poland
Background: It was suggested that complex cardiac rehabilitation improves prognosis after myocardial infraction.
Objective: The study aimed to evaluate the effects of early cardiac rehabilitation program in patient with myocardial infarction treated with primary percutaneous coronary intervention (PCI).
Methods: The studied group comprised of 50 patients aged 58.7±10.8 y who underwent primary PCI due to acute myocardial infarction. Within 30 days after the procedure all patients underwent early cardiac rehabilitation program for 8 weeks (3 sessions per week). The following parameters were obtained and compared before and after the rehabilitation: workload during treadmill test (METs), ejection fraction (measured with echochadiography and magnetic resonance), end-systolic and end-diastolic left ventricular volume (measured with magnetic resonance) and BNP level.
Results: Exercise capacity improved significantly after early cardiac rehabilitation (8.3±2.1 vs 9.5±1.9 METs, p>0.001). It was accompanied by a significant decrease in end-diastolic left ventricular volume (145.1 vs 136.0 ml/m2, p=0.0384) and BNP level (814.3 vs 228.0, p>0.01). However, there was no significant difference in ejection fraction measured both with echocardiography (54.0 vs 54.3%, p - NS) and magnetic resonance (55.5 vs 57.4%, p - NS) as well as in end-systolic left ventricular volume (64.7 vs 64.3 ml/m2, p - NS) before and after the rehabilitation.
Conclusion: The study suggests that the improvement in exercise capacity after early cardiac rehabilitation in patients with myocardial infarction treated with primary PCI is associated with decrease in end-diastolic left ventricular volume and BNP level but not to left ventricular ejection fraction. This might be explained by a decrease in left ventricular wall tension.
179 Increase in exercise training one year after the participation in a 4-week comprehensive cardiac rehabilitation program: a case-control study
OE Borstad; G Skoglund; CM Stenbakken; J Grimsmo
Feiringklinikken (The Feiring Clinic) Dept. of rehabilitation, Feiring, Norway
Objectives: One of the goals of cardiac rehabilitation is to get the participants to exercise lifelong. The aim of this study was to assess to what extent exercise training is maintained after a follow-up of 1 year in patients participating in a cardiac rehabilitation program (CRP) versus patients not participating.
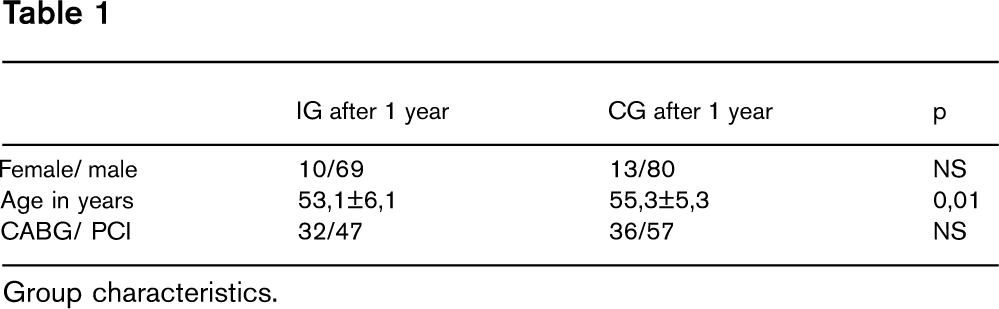
Methods: Ninety-eight participants under the age of 62 were included into the intervention group (IG). During the 4-week-rehabilitation-stay they participated in 35 different exercise lessions and were maximal exercise tested before and after CRP. They were given advise how to continue to train at home. Seventy-nine participated in the follow-up study. The control group (CG) was draught out from patients from treated at the same time as IG. They were matched by gender, age, social status and procedure (‘PCI’ or ‘CABG’). Both IG and CG undewent a maximal exercise test after one year and answered questionnaires about training. Group characteristics are shown in Table 1.
Results: At follow up IG had unchanged body mass index (BMI) from baseline and there was no difference between IG and CG groups (mean 29,0 kg/cm2 vs. 28,4; NS). Only 2 subjects in IG reported that they did not exercise at follow-up versus 10 before CRP. In CG 8 subjects did not exercise one year after treatment. IG significantly increased self-reported training time in hours from baseline to follow-up (2.9±2.3 vs. 4.4±2.2; p=0–0001) but they did not exersice harder than before (p=0.3). They reported both significantly more training hours per week (4.4±2.2 vs. 3.4±2.2; p=0.0001) and harder training (p=0.0001) than CG. No significant difference was found between the groups in VO2max in ml/kg/min after one year (29.0±7.7 vs. 27.3±6.3; p=0.1). However, IG significantly increased VO2 max from start of CRP (27.0±6.5) to one year after (p=0.0001), but they had a decline from the end of CRP (30.3±7.6; p=0.001).
Conclusion: One year after CRP the participating subjects exercised harder and more hours per week than the control group, but we did not find any difference between the groups in maximal oxygen uptake.
IG after 1 year
CG after 1 year
p
Female/male
10/69
13/80
NS
Age in years
53,1±6,1
55,3±5,3
0,01
CABG/PCI
32/47
36/57
NS
Group characteristics.
180 Early stationary rehabilitation favorably influences exercise tolerance in patients after an acute coronary syndrome treated with invasive methods
I Przywarska; E Deskur-Smielecka; S Borowicz-Bienkowska; M Wilk; A Brychcy; PE Dylewicz
University School of Physical Education Cardiac Rehabilitation, Poznan, Poland
The aim of the study was to compare the results of 3 different models of early rehabilitation in patients after an invasively treated acute coronary syndrome: 1) short-term stationary rehabilitation (Group S), 2) short-term stationary rehabilitation followed by 3-month hospital-based, ambulatory rehabilitation (Group SA), and 3) 3-month hospital-based, ambulatory rehabilitation (Group A).
Material: Sixty patients aged 54.9±8.13 (mean±SD), 5–14 days after an acute coronary syndrome treated with primary PCI acute coronary syndrome were randomly assigned to group S, SA or A.
Method: Exercise tolerance and quality of life were assessed before entering a rehabilitation program and after 3 months.
All patients performed a treadmill exercise test using a modified Bruce protocol and had quality of life measured with EuroQoL visual analogue scale (VAS).
Rehabilitation programs: stationary rehabilitation - training sessions 5 times per week for 3 weeks; ambulatory rehabilitation - training sessions 2–3 times per week for 3 months.
Training program included calisthenics (30 min/day), cycle ergometer training of interval or continuous mode and intensity of 50% of heart rate reserve (15–20min/day), and Nordic Walking 3 km/day.
Results: Mean exercise tolerance and quality of life before entering the rehabilitation program did not differ between the study groups. During the study period, exercise tolerance increased significantly from 7.8±2.81 to 9.5 ±3.99 METs (p>0.01) in group S and from 7.3±1.96 to 10.8±2.37 METs (p>0.001) in group SA, while the increase in group A was not significant (7.9±3.00 before vs. 9.5±3.08 METs at 3 months; p=0.1). Mean VAS result increased significantly from 68±17 to 74±17 p>0.01) in group S and from 72±16 to 80±11 (p=0.02) in group SA, and remained unchanged in group A (76±10 vs. 75±15; p=0.99). No differences between the groups in exercise tolerance and quality of life at 3 months were found.
Conclusion: Favorable effects of short-term stationary rehabilitation on exercise tolerance and quality of life parameters in patients after an acute coronary syndrome remain for at least 3 month after completing the rehabilitation program. Continuation of the program with 3-month hospital-based, ambulatory rehabilitation seems to not result in further improvement in exercise tolerance.
181 Exercise training in patients with chronic ischemic heart disease: influence on quality of life depending on sex
J Siegelova1; J Pochmonova2; L Mifkova2; V Chludilova2; A Havelkova2; P Vank2; B Fiser2; P Dobsak2
1Masaryk University, Head of Department, Department Functional Diagnostics And Rehabitation, Brno, Czech Republic
2Masaryk University Department. Functional Diagnostics and Rehabitation, Brno, Czech Republic
Aim of the study: The study was aimed at evaluation of quality of life, physical performance and parameters of capacity of the transport system of oxygen that we monitored in the group of men and in the group of women with chronic ischemic heart disease (CHIHD) before and after the combined exercise training (aerobic combined training with resistance elements).
Methodology: We examined 85 men (mean±SD) at the age of 62±10 years (without myocardial infarction) with ejection fraction (EF) 49 ±10% diagnosed by echocardiography and body mass index (BMI) 27 ±4 kg.m-2, and 19 women at the age of 64±7 years (without myocardial infarction) with EF 46±8% diagnosed by echocardiography and body mass index BMI 29±4 kg.m-2 before and after aerobic training combined with resistance exercises (12 weeks, three times a week). We compared the parameters of capacity of the transport system of oxygen (VO2SL ml.min-1, VO2SL.kg-1 ml.min-1.kg-1), maximum achieved symptom-limited load (WmaxSL W, WmaxSL.kg-1 W.kg-1), and subjective perception of quality of life by means of the questionnaire of quality of life (Seattle Angina Questionnaire, SAQ 1–5).
Results: In the group of men (CHIHD) we have found (before versus after) a significant change in WmaxSL (113±33 v. 123±35 W; p>0.01), WmaxSL.kg-1 (1.3±0.4 v. 1.4±0.4 W.kg-1; p>0.01), VO2SL (1692±412 v. 1834±45 ml. min-1.; p>0.01), VO2SL.kg-1 (20±5 v. 22±6; p>0.01), MET (5.7±1.4 v. 6.2±1.7; p>0.01), points in the questionnaire of quality of life SAQ1 (81±19 v. 85±16; p>0.01), SAQ2 (80±22 v. 86±16; p>0.01), SAQ3 (83±16 v. 88±14; p>0.01), SAQ4 (88±16 v. 93±10; p>0.01), SAQ5 (67±17 v. 74±17; p>0.01). In the group of women (CHIHD) we have recorded significant changes in rest VO2SL (1135±155 v. 1215±184; p>0.05), VO2SL.kg-1 (15.1±2.4 v. 16.3±2.4; p>0.05), MET (4.4±0.7 v. 4.7±0.6; p>0.05), SAQ1 (69±20 v. 75±16; p>0.01), SAQ2 (78±18 v. 88 ±16; p>0.05), SAQ3 (77±21 v. 84±17; p>0.01), SAQ4 (90±12 v. 94±9; p>0.05), SAQ5 (63±21 v. 72±17; p>0.01).
Conclusion: The twelve-week aerobic training combined with resistance exercises in patients with CHIHD improves capacity of the transport system and subjective perception of quality of life in all evaluated spheres both in men and in women with CHIHD. Men, moreover, achieved a significant improvement of the maximum performance, also of the performance related to kilogram of the mass, of initial heart rate and maximum systolic pressure. Supported by the research task of – MSM 0021622402.
182 Beneficial effects of the early, short-term and multi-profile stationary rehabilitation of hypertensive patients after ACS
S Borowicz-Bienkowska; E Deskur-Smielecka; I Przywarska; M Wilk; PE Dylewicz
University School of Physical Education Rehabil. Hospital - Cardiac Rehabilitation, Poznan, Poland
Data from EUROASPIRE III study show that effects of secondary prevention in patients with IHD are especially unsatisfactory in patients with arterial hypertension.
The aim of our study was to estimate to what extent the early multi-profile rehabilitation improves knowledge of patients about the blood pressure and corrects their blood pressure values, and also to what extent the early multi-profile rehabilitation improves knowledge about the healthy nutrition and if it modifies their nutritional habits.
Material: 40 patients with the arterial hypertension aged 57±9 (mean ±SD) who 1–2 weeks after ACS were put on stationary, multi-profile rehabilitation course for 2–3 weeks, which essential element was educational programme directed towards informing on the disease and recommendation on healthy nutrition.
The method: Before the beginning of rehabilitation, routine diagnostic procedures were done including BP measurements, and analysis of diet composition was performed. The survey questionnaire was also applied being related to such items like knowledge about the disease and the risk factors, information on own blood pressure, and knowledge about the proper values of blood pressure. The investigation was repeated 3 months after the end of rehabilitation.
Results: In preliminary investigations it was found that 61% patients could not give the correct values of systolic BP and 47% of diastolic BP, while these percentages dropped respectively to 19% and 22% (p>0,005) after 3 months. 9.5% patients at the end of rehabilitation, and 19.5% subjects 3 months after discharge home had SBP=140 or/and DBP=90 mmHg.
Among the preferences considered in the context of nutritional decisions, the number of patients declaring taking into account fat content of product increased significantly from 45.9 to 69.6% (p>0,005), and the number of patients checking a salt content in products increased from 43.2% to 64.9%. Also beneficial tendencies were observed in the diet composition, which were expressed by a lower total caloricity (from 2324±503 kcal to 1967±601 kcal, p>0.02), a decrease in the cholesterol content (from 605.5±344.99 mg to 369.6±203.77 mg, p>0.03), and the decrease in the content of saturated fat acids in total daily caloric intake from 12.7% to 10.8%.
Conclusion: Early, short-term and multi-profile cardiac rehabilitation after ACS of patients with arterial hypertension improves their knowledge, brings about beneficial change in patients' nutritional habits, as well as it probably has a favorable effect on a control of the arterial blood pressure in majority of patients.
183 Short-term, early stationary rehabilitation improves functional fitness and quality of life in patients after an acute coronary syndrome
M Wilk; E Deskur-Smielecka; S Borowicz-Bienkowska; I Przywarska; PE Dylewicz
University School of Physical Education Cardiac Rehabilitation, Poznan, Poland
Decreased functional fitness is a common problem in subjects after an ACS, and may deteriorate quality of life.
Purpose: To assess whether early stationary rehabilitation may influence functional fitness and quality of life in patients after an ACS.
Methods: Study population consisted of 61 subjects (mean age 57±9 yrs, 47 males) enrolled in early, stationary rehabilitation after an ACS. Rehabilitation comprised moderate-intensity endurance training on cycle ergometer, calisthenics and Nordic Walking (5 times per week, total 10 sessions). At discharge, 16 patients (group A) volunteered an ambulatory, hospital-based training program (sessions twice a week) for another 3 months. The remaining 45 patients (group B) were given instructions to maintain physical activity. On admission, at discharge and 3 months thereafter functional fitness was assessed with selected elements of the Fullerton's Functional Fitness Test Battery, and quality of life was measured with EuroQoL visual analogue scale (VAS).
Results: After the stationary rehabilitation, functional fitness and quality of life parameters improved in both groups (group A: 6MWT from 514±99 m to 583±120 m [p>0,001], Arm curl from 19,3 ±5,4 reps to 23,40±3,7 reps [P>0,01], 8-ft from 5,5±0,8 s to 5,2±0,5 s [ns], VAS from 72±16 to 78±3 [ns; P=0,059], in group B: 6MWT from 502±113 m to 551±123 m [P>0,001], Arm curl from 18,5 ±4,8 reps to 21,5±6,5 reps [P>0,001], 8-ft from 5,7±1,2 s do 5,1±1.0 s [P>0,001], and VAS from 68±17 to 76±17 [P>0,001]). For all parameters and both study groups, the results after 3 months were significantly better than on admission, but did not differ from the ones obtained after the stationary rehabilitation (group A: 6MWT 569±106 m, Arm curl 23,7±3,8 reps, 8-ft 4,9±0,7 s, VAS 80±11, in group B: 6MWT 562±164 m, Arm curl 20,7±4,7 reps, 8-ft 5,2±1,0 s, VAS 74 ±17). Between-group analysis revealed that Arm curl in group A was significantly better than in group B (P=0,03). A moderate, but significant (P>0,05) correlation between VAS results and functional fitness parameters (correlation coefficient for 6MWT: 0,24, for 8-ft: −0,26, and for Arm curl: 0,3).
Conclusions: Short-term, early stationary rehabilitation significantly improves functional fitness and quality of life, which effects lasts for at least 3 months. Functional fitness parameters weekly correlate with quality of life. Prolongation of the rehabilitation with hospital-based ambulatory program does not cause further improvement in functional fitness, with the exception of upper body endurance.
184 Metabolic effects of a very short-term, early stationary rehabilitation in patients after an acute coronary syndrome (ACS) - results of a 3-month follow-up
E Deskur-Smielecka; M Wilk; S Borowicz-Bienkowska; I Przywarska; J Karolkiewicz; L Pilaczynska-Szczesniak; P Dylewicz
University School of Physical Education Dept of Cardiac Rehabilitation, Poznan, Poland
Background: It is unknown what is the shortest duration of a rehabilitation program (RP) sufficient to induce changes in metabolic risk factors and blood pressure (BP), and how lasting are these effects.
Purpose: 1. To assess lipids and insulin resistance, and BP in patients after an ACS before, at the end and 3 month after a very short-term, early stationary RP. 2. To compare the efficacy of such RP with a short-term stationary followed by a 3-month ambulatory, centre-based RP.
Methods Study population: 61 subjects (age 57±9 yrs, 47 males; 41 with hypertension) 5–24 days after an ACS. Stationary RP: moderate-intensity endurance training, calisthenics and Nordic Walking (5 times per week, total 10 sessions), and education on risk factors and recommended lifestyle changes. At discharge, 16 patients (group A) volunteered an ambulatory, hospital-based training program (twice a week) for another 3 months. The remaining 45 patients (group B) were given instructions to maintain healthy lifestyle. Serum lipids, fasting glucose and insulin were measured on admission (Term I), at discharge (Term II) and after 3 months (Term III). Atherogenic index of plasma (AIP) and insulin resistance index HOMAIR were calculated.
Results: Significant changes in metabolic parameters and BP are shown in the table. Between-group analyses: HOMAIR at Term I and II, and systolic BP at Term III were lower in group A (respectively: P>0,05, P>0.05, BP: 117±12 vs. 129±19, P>0,01).
Conclusion: Patients after an ACS have better lipid and insulin resistance parameters at 3 months after a very short-term, stationary RP than before rehabilitation. Prolongation of the RP with a 3-month hospital-based ambulatory program does not improve the metabolic effects, but may prevent an increase in systolic BP observed in non-participants.
Group
Term I (mean ±SD)
Term II (mean ±SD)
Term III (mean ±SD)
ANOVA
Term vs. III
Term II I vs. III
A
AIP
0,33 ±0,17
0,29 ±0,19
0,20 ±0,24
0,0468
>0,05
ns
B
TC (mmol/l)
4,40±0,90
4,16±0,76
4,03±0,85
0,0489
>0,05
ns
HDL (mmol/l)
1,23±0,34
1,28±0,33
1,39±0,36
0,0032
>0,01
ns
AIP
0,33± 0,22
0,32 ±0,19
0,25±0,23
0,0015
>0,01
>0,05
HOMA-IR
3,53±2,11
3,99±2,68
3,29±2,6
0,0294
ns
>0,05
Systolic BP
121±17
120±11
129±19
0,0047
ns
>0,01
Diastolic BP
77±9
78±9
82±12
0,0142
ns
ns
185 Is there any correlation between physical activity before Acute Coronary Syndrome and the effects of six-month cardiac rehabilitation?
D Kalka; M Sobieszczanska; W Pilecki; A Bak; A Chorebala; E Metner
Wroclaw Medical University, Wroclaw, Poland; Cardiac Rehabilitation Centre ‘Medar’, Wroclaw, Poland
Purpose: Evaluation of possible relation between physical activity before ACS and adaptation to effort during cardiac training.
Methods: Ambulatory rehabilitation comprised a 45-min cycloergometer training (ERGOLINE system) with the 4-min interval loads (50% of those established during the ECG exercise testing) increasing with time and broken by the 2-min rest with 10 Watt load (3x/ week), with generally improving exercises (2x/ week). A physical activity profile was assessed retrospectively for 20 years before ACS with the Framingham questionnaire using metabolic equivalent (MET).
Material: A group of 75 patients (12 females and 63 males), aged 43–63 years (mean: 55. 4±4.4) with previous ACS.
Results: Analysis of possible correlation between the value of Index Framingham, which for the examined patient group was of 55.6±4.12, and the increase of MET value measured during the pre-rehabilitation and post-rehabilitation ECG treadmill testing, which was of 2.12±1.2, revealed that the level of physical activity before the ACS episode had no significant influence on the effort tolerance obtained in result of cardiac rehabilitation cycle.
186 A mixed method study, analysing the factors and reasons for non-attendance and drop out at a phase III cardiac rehabilitation programme
2Trinity College School of Nursing, Dublin, Ireland
Purpose: The purpose of the study was to examine the factors and reasons contributing to non-attendance at phase III cardiac rehabilitation after enrollment and dropping out after commenement.
Methods: The study was a single site study. A mixed method design was used. A telephone survey was carried out of the patients who enrolled and subsequently did not attend or dropped out of a programme (n=80). Patients were asked to say why they could not attend the programme. A convenience sample from these patients was selected for semi-structured interviews (n=7). The interviews identified the factors that contributed to their non-attendance or drop out from the programme. Analyses of the demographics of the total cohort and the results of the survey were carried out using the statistical package SPSS. Pearson's chi-squared analysed the demographic factors that influenced the attendance, non-attendance and non-completion. The qualitative data was analysed using a priori themes and a template analytical approach using the computerized package “Nvivo 2”.
Results: Of the 267 patients who enrolled in the cardiac rehabilitation programmes over the time course of the study, 70% completed the programme, 11% did not attend the programme and 19% did not complete the programme. The clients that did not attend or complete, were significantly more likely to be manual or unskilled workers (P=0.029) or smokers (p=0.000). There was no significant difference among the three groups when factors such as age, gender and co-morbidities including depression were analysed. The survey revealed that the most common reason cited by those who dropped out was “illness” (33%). The most common reason cited by those not attending after enrolling was “not interested” (24%). The follow up interview findings of the factors that influenced their drop out or non-attendance were categorized into three major categories: physical, psychological & organizational. Further exploration of the physical theme revealed that these reasons could be categorised into health reasons, access difficulties and difficulties with exercise. The main psychological reasons were classified as depression, issues relating to self and stress and the main organisational reasons were education; issues with the cardiac rehabilitation programme, the health system and work.
Conclusion: The patients that did not attend or complete, were more likely to be manual or unskilled workers and smokers. Patient cited illness as the most common reason for dropping out of the programme and not interested as the most common reason for not attending the programme after enrolling.
187 Assessment of a national rehabilitation programme for patients after cardiovascular diseases in a developing country
E Rivas-Estany; JA Alvarez Gomez; JD Barrera Sarduy; S Sixto Fernandez; LM Rodriguez Nande; C Kesser Garcia
Institute of Cardiology and Cardiovascular Su Cardiac Rehabilitation, Havana, Cuba
Cardiovascular diseases are the leading cause of death in Cuba, a developing LatinAmerican country, since more than 40 years ago, with a high prevalence and a negative social-economic repercussion. A national and comprehensive cardiac rehabilitation (CR) program developed at community level has been implemented all over the country since 1989. The principal aim of this report has been to analyze and compare the last two years results of the implementation of this CR program.
In this study were included all patients with the diagnosis of acute myocardial infarction, unstable angina pectoris or after coronary angioplasty (PTCA), aorto-coronary bypass or valvular surgery discharged alived in the 23 hospitals involved in the Cuban Cardiological Network, sponsored by the Health Ministry.
The program included the three phases for comprehensive CR considered by the World Health Organization, also it were included changing life style measures and physical exercises at target training heart rate determined through previous exercise stress testing. Chi-square test was used to analyze the qualitative comparable results.
10611 patients were included in the study in 2006 of whom 5202 (49%) were enrolled in the CR program. 52,4% of myocardial infarction patients were included in the CR program, 28% of angina and PTCA patients and 79% of coronary and valvular surgery patients. In 2005 were included in CR Phase I a higher number of patients than in the last year (14977 vs 8477, p>0,05), nevertheless more patients received psychological support and outwork medical follow-up in 2006. It was observed only a tendency to a higher number of exercise stress test, with diagnostic or evaluative purpose, performed in 2005 compared with the following year (22955 vs 19088, p= n.s.).
The best results of the comprehensive CR program were observed in the hospitals and community centers of the western region of the country, where Havana, the capital is located in. It was concluded that the national CR program in Cuba is a reality, nevertheless it is required to increase its development in some regions of the country-side.
188 Rehabilitation preference among the elderly
B Oerkild1; M Frederiksen2; J Fischer Hansen1; E Prescott1
1Bispebjerg Hospital Department of Cardiology, Copenhagen, Denmark
2Bispebjerg Hospital Department of Cardiology, Rehabilitation Unit, Copenhagen, Denmark
Background: Participation in cardiac rehabilitation programs decline with increasing age despite the fact that older patients have the highest morbidity and relative mortality. Establishing of a home-based rehabilitation program may increase patient referrals, enhance uptake and reduce drop-out.
Objective: To investigate the cardiac rehabilitation preferences of elderly patients admitted with a new event of ischaemic heart disease. Design: Patients =65 years with ischaemic heart disease admitted to the cardiac unit at Bispebejerg Hospital over a period of 3 consecutive months were asked to fill in a questionnaire. It included questions of whether the patients would accept to participate in a cardiac rehabilitation program after being discharged, of the reasons for rehabilitation refusals and questions about preference of cardiac rehabilitation type if offered the choice between home-based and centre-based programs.
Results: A total of 209 patients (65–91 years) with a new event of ischaemic heart disease were admitted. Of these, 27% (n=57) were not eligible to fill in the questionaire because of confusion, serve illness or language difficulties. Of the 152 patients who answered, 43% (n=66) refused participation in a centre-based rehabilitation program. The main reasons for this refusal were reported to be the time and transportation burden associated with participation (62%) or because patients were not interested in risk factor intervention and hence life style changes (29%). However, 20% of the refusers would be interested in a home-based rehabilitation program if given the choice and 70% did not know if they would accept such an offer. Overall, of the 152 patients who answered the questionnaire 20% would choose home-based rehabilitation, 32% would choose centre-based rehabilitation and 47% did not know which of the two programs to choose.
Conclusion: Home-based cardiac rehabilitation is considered an attractive/acceptable alternative by some elderly patients who refuse centre-based programs indicating that inclusion of a home-based rehabilitation offer will increase the overall rehabilitation participation rate.
189 Medical treatment and secondary prevention in greek outpatients with established coronary heart disease
T Livieratos; PAN Koustas; AR Tziovas; FO Kontari; AL Patsilinakos; GE Fagogenis; GE Kordosis
General Hospital of Agrinio Cardiology, Agrinio, Greece
Secondary prevention measures for coronary heart disease are effective in reducing coronary morbidity and mortality.
Purpose: To evaluate the overall achievement of goals in the control of risk factors in secondary prevention in patients with established coronary heart disease and assess drug prescription relative to published therapeutic guidelines.
Patients and Method: The study included 185 consecutive patients=75 years of age from outpatient cardiology clinic of a regional Greek hospital. All patients were identified after coronary artery bypass grafting, percutaneous transluminal coronary angioplasty (PTCA), admission for myocardial infarction or admission for myocardial ishaemia. The targets for control were: blood pressure >140/90 mmHg in the general population and >130/80 mmHg in diabetics; LDL-cholesterol >100 mg/dl and no smoking habits. We also evaluated prescriptions for cardiovascular drugs.
Results: Out of all patients 74.5% were male, mean age 65±8 years; 73% were hypertensive, 77.8% dyslipidemic and 30.8% diabetics; 35.6% achieved target blood pressure; 33% achieved LDL-cholesterol=100 mg/dl and current smoking was present in 28% (45% were former smokers while 27% were never smokers). Regarding use of cardiovascular drugs, 91.3% of patients receiving aspirin, 47.5% other antiplatelet medication, 64.3% angiotensin-converting enzyme, 63.8% b-blockers, 80.5% statin, 42.7% calcium channels blockers, 25.4% angiotensin receptor blockers and 40% diuretics. Finally, nitrates were used by 41.6% of patients.
Conclusion: Our study shows a high prevalence of modifiable risk factors in Greek patients with coronary heart disease. Despite the frequent use of appropriate cardiovascular drugs only a minority of these patients achieved the recommended goals.
190 Improving cardiac rehabilitation in Finland: the access to cardiac rehabilitation of the CHD patients in the Pirkanmaa hospital district
A Leimumaki1; K Hautamaki-Lamminen2; P Eljaala1; J Saarnisto3; M Salonen3; T Sisto3; J Taurio3; V Virtanen3; M Rantala1
1Finnish Heart Association, Pirkanmaa, Tampere, Finland
2University Central Hospital Heart Centre, Tampere, Finland
3Orivesi Health Care Centre, Tampere, Finland
Background: Reliable figures have not been available of the access to cardiac rehabilitation in Finland or in Finland's different hospital districts. The Finnish Heart Association has been engaged in collecting data by asking health care professionals in hospitals and health care centres during the years 1991, 1994 and 2006, and according to those results less than 10% of CHD patients receive CR after discharge in Finland. The total population in the Pirkanmaa Hospital District is 467 000 i.e. about 10% on Finland's total population. The Heart Centre of the Pirkanmaa Hospital District diagnoses and treats all acutely ill cardiac patients and all those who need complex cardiological or cardiosurgical examination or treatment. We wanted to study the access to CR in this effectively acting Hospital District in Finland.
Methods: A cohort sample of 300 CHD patients were retrospectively and randomly identified from hospital records treated in years 2005–2006 for their CHD at the Heart Centre of the Pirkanmaa Hospital District. 100 of the patients were selected from the Tampere region, 100 from the upper Pirkanmaa region and 100 from the Kolmostie region to study the effect of the distance from central hospital on the access to CR. The data was collected according to the Cardiac Rehabilitation Audit Standards 2004.
Results: The mean age on the sample was 70.4 years (SD 10.8), and 70% of patients were male. Of the whole sample almost all received phase I CR, and even 50% of the CHD patients received phase II CR. The male sex (p>0.01) and the younger age (>70 years, p>0.0001) of the patients as well as the shorter distance from the central hospital (p>0.0001) affected the access to the phase II CR. Operatively treated patients (CABS, p>0.01) were more likely to achieve phase II CR than PCI treated patients. Phase III CR was available only for a very few patients.
Conclusion: The access to CR may vary a lot in Finland according to the different hospital districts. In Finland the main effort should be focused on getting audit system to increase the access and quality of CR as has been successfully been done e.g. in Sweden. Secondly, more equal access to CR should be guaranteed for cardiac patients despite of their sex, age or place of living.
191 The importance of phase I cardiac rehabilitation and evaluation of its performance in Tehran city hospitals
R Ghalamghash1; B Goosheh2; A Hosseini2; A Bazrafshan2; M Keyhani3
3Iran Medical University Biometry, Tehran, Iran (Islamic Republic of)
Background: There are limited studies related to the inpatient phase of cardiac rehabilitation on complete performance and importance point of view. The main goal of this study is evaluation and discussion about the amount of regards to importance and performance phase I cardiac rehabilitation in Tehran city hospitals.
Methods: Eleven hospitals among the governmental and non-governmental ones which have cardiac surgery sections were chosen randomly. To gain the main purpose of study, we used a questionnaire that was prepared according to American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR) guideline. The questionnaires were sent to head of the cardiac rehabilitation department by the educated personals in a two weeks period. These forms have been contained of ten specialized questions with different scores about evaluating the quality of phase I cardiac rehabilitation performance and attentions to it. The scores were used in SPSS software to analysis the data.
Results: The results showed that only 10% of the hospitals with cardiac surgery section, had a relatively complete plan of phase I cardiac rehabilitation according to AACVPR guideline (P=0.07). These results were lower than the international standards, where as in some of them, the scores were about zero.
Discussion: According to the importance of phase I as a main goal in cardiac rehabilitation program and its direct effect on participation of the patients in the last phases of cardiac rehabilitation, it is suggested to pay more attention in planning, processing and performing this phase.
Rate of cardiac rehabilitation companents performance
Rate (%)
Title
Abbreviation
No.
9
Cardiac rehabilitation group
CRGs
1
18
Functional capacity measurement
FCM
2
18
Progressive exercise therapy programs
PEPs
3
54
Group exercise therapy
GE
4
9
Risk stratification
RS
5
0
Exercise testing
ET
6
18
Secondary prevention programs
SPPs
7
36
Psychological programs
PSPs
8
54
Nutrition programs
NUTPs
9
18
Second phases programs
2edPs
10
192 Drug secondary prevention in postmenopausal women with cardiovascular disease
A Sitar-Taut1; M Cebanu1; DT Dumitru Tudor Zdrenghea2; D Pop1; D Petrovai1
1 Univ. of Med. And Pharm. Cardiology, Cluj-Napoca, Romania
2Univ. of Med. And Pharm. Dept of Cardiology, Cluj-Napoca, Romania
Background and purpose: It is known that women with cardiovascular disease are under treated, including drug treatment. This aspect was less studied with respect to drugs used for secondary prevention.
Methods: In an urban Romanian community there was studied a representative sample of 150 postmenopausal women with ischaemic heart disease. We considered the secondary prevention by drugs. The results were compared with those registered in a similar sample of 150 men aged > 55 years with ischaemic heart disease. The study was carried out using general practitioner's files.
Results: In according to literature, there were considered as preventive drugs: antiplatelet agents, statins, beta blockers and ACEI. Aspirin was used in 56.4% of the women and 72.5% of the men (p>0.05), ACEI in 69.1% and 79.8% (p>0.05), beta blockers in 69.1% and 74.3% (p>0.05) and statins in 48.9% and 48.6% (p>0.05). Even if they don't represent preventive drugs, a significant percent of the patients were treated with nitrates (36.2% women, 43.1% men p>0.05) and with calcium channel blockers (31.9% women and 19.3% men p>0.05). The results show that antiplatelet drugs are underused in ischaemic patients, but especially in women. The use of other preventive drugs categories is close to that reported in the literature for East Europe, but if the utilization of beta blockers and statins is almost equal in men and women, ACEI are less used in women. The maximum use of preventive drugs in women was registered after acute myocardial infarction (beta blockers-85.7%, statins-50%, aspirin-60.7%, ACEI-75%). In turn, the myocardial revascularization by CABG and PCI is low in both groups, but much less in women than in men: CABG 1.1% in women, 4.6% in men p>0.05, PCI 5.3% in women and 13.8% in men p>0.05.
Conclusion: In postmenopausal women with ischaemic heart disease the secondary prevention by drugs is similar with that applied in men, except aspirin and ACEI, which are underused.
193 Mortality and causes of death up to 8 years after outpatient cardiac rehabilitation
M Di Valentino; MT Maeder; S Jaggi; J Schumann; K Sommerfeld; S Piazzalonga; A Hoffmann
University of Basel Cardiology, Basel, Switzerland
Purpose: Little data exist about long-term prognosis of patients (pts) completing outpatient cardiac rehabilitation (OCR). The aim of this study was to determine the mortality rate and assess the causes and predictors of death after cardiac rehabilitation.
Methods: Analysis of 2146 consecutive pts completing a 12-week exercise-based OCR between March 1999 and March 2007. Medical data were assessed at the beginning of OCR. Median follow-up was 46 months (interquartile range 22–71). Date and cause of death were obtained from general practitioners and hospital records.
Results: During the study period 74 pts (87% male) died after a median of 29 months (interquartile range 17–49). 93% of pts had coronary artery disease and 15% had valvular heart disease, 48% had undergone PTCA, 37% coronary artery bypass grafting (CABG) and 8% valve surgery. The mortality rate was 0.9% per year for all causes and 0.34% per year for cardiovascular causes. In comparison to survivors, non-survivors were older (65±12 vs 60±11 yrs), had lower LVEF (51±15 vs 55±16%), lower exercise capacity (69±17 vs 79±20% of predicted value), and there was a higher prevalence of CABG, diabetes and hypertension (all differences p>.05). Multiple logistic regression analysis revealed the following independent predictors of death: Exercise capacity (odds ratio (OR) 0.14, 95% confidence interval (CI) 0.04–0.47; p=.002), diabetes (OR 2.03, CI 1.20–3.42; p=.008), angina (OR 1.80, CI 1.08–2.99; p=.024), and age (OR 1.05, CI 1.02–1.07; p>.001).
Conclusion: Patients after successful OCR have an excellent long-term prognosis. Mortality is due to cardiovascular causes in less than half of the cases and is associated mainly with low exercise capacity, diabetes and residual ischemia, and to a lesser extent with age, CABG and ventricular function.
194 Effect on physical activity of a multifactorial intervention study for prevention of ischaemic heart disease (Inter99): results from 5-years follow-up
LVH Smith1; T Jorgensen2
1Research Centre For Prevention And Health Glostrup Hospital, Glostrup, Denmark
2Research Centre for Prevention and Health, Glostrup, Denmark
Purpose: Knowledge about the long-term effect on physical activity (PA) of multiple behavioural risk factor interventions to prevent ischaemic heart disease (IHD) is sparse. This study aims to examine the effect of a randomized multifactorial intervention on change in PA from baseline to 5-years follow-up.
Methods: The intervention group (group A) was a random sample of 11.708 men and women aged 30 to 60 years living in Copenhagen County, Denmark. Tthe control group (group C) was a random sample of 5264 men and women. At baseline 6091 persons from group A and 3324 persons from group C participated. Group A was invited for a health examination, an assessment of their absolute risk of developing IHD and individualized lifestyle intervention. Participants who were at high risk of developing IHD were also offered diet/physical activity group counselling. High-risk persons in group A were re-invited to a health examination and lifestyle counselling after 1 and 3 years and low risk persons answered a mailed questionnaire. At 5-year follow-up all baseline participants were re-invited. Group C answered a mailed questionnaire at baseline and at 1, 3 and 5-years follow-up. Data was analysed using longitudinal linear regression models with random effects. Main outcome: change in PA from baseline to 5-years follow-up.
Results: Among men with a low baseline PA level, participants in group A had increased their PA level significantly more than participants in group C after 5 years (increase in PA: group A: 109 min/week (95% CI: 99–120 min/week); group C: 63 min/week (95% CI: 49–77 min/week)). Also among all men, irrespective of their baseline PA level, the intervention had a beneficial effect when compared to group C (increase in PA: group A: 5 min/week (95% CI: −2–12 min/week); group C: −28 min/week (95% CI: −37–19 min/week)). There was no significant intervention effect on PA after 5 years in either women with a low PA level at baseline (increase in PA: group A: 98 min/week (95% CI: 88–108 min/week); group C: 95 min/week (95% CI: 83–108 min/week)) or in all women (increase in PA: group A: −3 min/week (95% CI: −10–4 min/week), group C: −8 min/week (95% CI: −17–0 min/week). The intervention effect differed according to educational level. Details on this will be presented.
Conclusion: The intervention seemed to have a beneficial long-term effect on PA level among men. There was no effect among women.
195 Sustainability in the secondary prevention
W Mayer-Berger1; M Martin Kohlmeyer1; M Redaelli2; G Buescher3; B Schwitalla1; KW Lauterbach2
Purpose: Worldwide cardiovascular diseases lead to an increase of burden of disease with high morbidity and mortality followed by a significant growth of health expenditures.
Meanwhile the providing in the secondary prevention has remained behind expectation. Studies of the rehabilitation research showed that the sustainability of therapy-success achieved during this period is insufficient.
Methods: Our present study is a unicentric, prospective, randomised and controlled clinical trial. It is designed for 18 months with 600 patients. The intervention consists of telephonic reminders after a unit of 3 weeks inpatient rehabilitation (each month during the first three months after the unit followed by once in three months till the end of the study after 18 months) and an one day additional training in our clinic 6 months after the end of the inpatient care. For the outcome measurement the following parameters were taken at the beginning and at the end of the study: blood pressure, BMI, triglyzerides, total cholesterol, LDL cholesterol, HDL cholesterol, HbA1c as well as the status of smoking. Likewise the intima-media thickness of carotids is measured following international standards. The quality of life is quantified with EUROQOL and HADS. The study ends with the identification of the pensionary status.
Results: The average age amounts to 49 years at the beginning of the study (n=600). 89% of the participants are male, 72% have a low-grade education. After 18 months 8 patients of the control group (7 of them proved to be cardiac) and none of the interventional group have died. Significant differences concerning morbidity get clear: 13 patients of the control group were retired since the beginning of the study, 3 patients of the intervention group (p>0,05).
After 18 months the patients of the intervention group show a favourable but not significantly improved risk profile. Concerning the intima-media thickness (p>0,05) and quality of life (p>0,05) the same patients show significant improvement.
Conclusion: Even in the high risk group (young mainly male patients with low social status) sustainability is within reach by using simply, psychosocially arranged ambulant aftercare which leads to a decreased number of mortality, a significant decrease of morbidity and at the same time a significant increased quality of life. It is remarkable that these results were gained without achieving the recommended target values of the classic risk factors of the evidence based practice guidelines. The intima-media thickness however showed a significant growth in the control group.
196 Three years experience with a nurse led atherosclerotic secondary prevention clinic
HT Jorstad; TPW Kamphuisen; JJ Doornenbal; B Van Den Lienden; EBCH Stecher; CH Putto; RJG Peters
Academic Medical Centrum Cardiology Department, Amsterdam, Netherlands
Objectives: To assess the effectiveness of uniform standardized secondary prevention on patients who have suffered a complication of atherosclerotic disease by specialized nurses on (i) lifestyle components (smoking cessation, medication usage, exercise and healthy diet); (ii) standardized goals on hypertension, dyslipidemia, blood glucose and Body Mass Index (BMI).
Methods: 231 patients referred to the outpatient Nurse Led Prevention Clinic (NLPC) were included in this observational study. The primary end point was change in risk factor levels between baseline and one year follow-up. Other end points were medication adherence and the percentage of patients within target range. Data was obtained from postal questionnaires and review of case notes at baseline and one year follow-up.
Results: The mean age of patients at baseline was 61.8 years and the mean follow-up was 1.2 years (response rate 54%). At one year follow-up there was a significant improvement in systolic blood pressure (SBP), diastolic blood pressure (DBP), LDL, total cholesterol, triglyceride and non-fasting glucose. The improvement in HDL, BMI, waist and fasting glucose was not significant. Statin adherence increased from 78.5% to 97.9%. There was also a significant rise in number of patients on or below target for the risk factors SBP, DBP, HDL, LDL, total cholesterol and triglycerides. The improvement in self reported risk factors exercise and healthy food choices was also significant.
Conclusion: NLPCs have the potential to improve the clinical management of cardiovascular risk factors.
Risk levels baseline and one year f.u.
N
Baseline mean
One mean
year
Systolic blood pressure
216
141.0
134.6∗
mmHg
Diastolic blood pressure
216
83.4
79.3∗
mmHg
HDL
205
1.4
1.4
mmol/l
LDL
198
2.8
2.0∗
mmol/l
Total cholesterol
212
4.9
3.9∗
mmol/l
Triglyceride
204
1.7
1.3∗
mmol/l
Fasting glucose
51
6.0
5.9
mmol/l
Non-fasting glucose
39
6.7
5.6∗
mmol/l
BMI
215
27.7
27.6
kg/m2
Waist
52
97.4
97.9
cm
∗p>0.05.
197 Alternative delivery models of cardiac rehabilitation: description and patient characteristics
H Tulloch; S Black; P O'farrell; L Morrin; P Robbins; R Reid; A Pipe
University of Ottawa Heart Insitute Prevention and Rehabilitation, Ottawa, Canada; Ottawa Heart Institute, Ottawa, Canada
Purpose: Chronic underutilization of cardiac rehabilitation programs (>20% of eligible patients) and long wait times for CR program initiation (i.e., >75 days), led to restructuring our cardiac rehabilitation program to improve access and better meet the needs of cardiac patients. Program changes included: an automatic referral process, systematic triage to programs based on need, and increased program capacity through the development of a variety of program length options. The purpose of the present research is to describe the CR program streams and respective patient characteristics.
Methods: Five CR program streams will be described: 1) Brief - exercise evaluation and tailored home exercise program without supervision; 2) Case-managed home program-3 on-site appointments, individual home exercise program without supervision, and weekly telephone contact; 3) 4 week on-site program; 4) 8 week on-site program; and 5) 12-week on-site program. Participants (N=1952) included all patients enrolled in CR between April 2006 and October 2007. Participants completed questionnaires on program entry measuring demographic variables, cardiac risk factors, comorbidities, depression, anxiety, and quality of life. Anthropometric measurements and fasting lipid profile were also performed. Analysis of Variance was used to examine the differences between the participants in each stream on each of the variables under study.
Results: The most prevalent stream (38% of participants) was the 8-week on-site program, followed by the case-managed home program (22%), the brief program (14%), the 12-week on-site program (13%), and the 4-week on-site program (13%). As expected, significant differences were observed on many of the variables under study (ps>.05). Specifically, participants in the 12-week on-site program tended to be older, less educated, have more comorbidites, have elevated risk factors, experience more depression and anxiety, report lower quality of life, and included more women than the other streams. The brief and 4-week program tended to attract younger patients who were more active before their cardiac event.
Conclusion: The program restructuring was designed to provide the right program to the right patient at the right time in the right place for the right cost. We found that patient profiles varied across the program streams, indicating appropriate triaging to alternative models of CR. Future research on the differential effects of CR options on health outcomes over time is warranted.
198 EUROACTION: do couples attending a hospital based multidisciplinary family cardiovascular prevention and rehabilitation programme share the same risk factors? Do they change together?
C Jennings1; T Collier2; A Mead1; J Jones3; A Holden2; S Connolly2; K Kotseva2; D De Bacquer4; G De Backer4; D Wood2
1Imperial College London, London, United Kingdom
2London School of Hygiene and Tropical Medicin, London, United Kingdom
3Brunel University, London, United Kingdom
4University of Ghent, Ghent, Belgium
Purpose: EUROACTION a multidisciplinary programme managing CHD patients and families to the European targets for CVD prevention.
Methods: Correlation between couples for CVD risk factors at initial assessment (IA) and for changes from IA to 1 year were assessed by Pearson correlation coefficients.
Results: 645 couples attended the IA (78% of eligible) and 419 (65%) at 1 year. Correlations for CVD risk factors between patients and partners are shown in Table. At 1 year quintiles of change in patients for waist (Q1 most, Q5 least) concorded with mean change in partners (figure).
Conclusion: Couples attending the IA shared the same risk factors. At 1 year changes in waist, BMI, BP and TC correlated between patients and their partners. Patients who made the most changes were more likely to be associated with partners who also made most changes. These results support the principal of family based CVD prevention.
IA
Change at 1-year
WC (cm)
r=0.12
p=0.004
r=0.22
p>0.0001
BMI (kg/m2)
r=0.22
p>0.0001
r=0.21
p>0.0001
SBP (mmHg)
r=0.20
p>0.0001
r=0.13
p=0.008
DBP (mmHg)
r=0.18
p>0.0001
r=0.15
p=0.002
TC
r=0.20
p=0.007
r=0.21
p=0.03
LDL
r=0.16
p=0.04
r=0.15
p=0.14
Glucose
r=0.14
p=0.07
r=0.13
p=0.18
Waist Circumference (cm)
199 Comparison of two questionnaires measuring quality of life
A Hoffmann; I Arrigo; K Sommerfeld; S Piazzalonga; M Lefkovits
Background and aim: Multiple instruments are available for assessing quality of life (QoL) in cardiac patients. The aim of this study was to compare the german, “PLC” and the german version of the, “MacNew” questionnaires for detecting changes in a cohort of patients followed for one year after cardiac rehabilitation.
Patients and methods: Two hundred and twenty eight patients (33 female, mean age 61 yrs) were prospectively followed after completion of a cardiac rehabilitation program. Both questionnaires were administered at baseline and at the one year follow-up evaluation. The PLC (QoL profile for chronic diseases; Siegrist et al) has 40 items converted into 6 scales ranging from 0–4; the MacNew (Höfer et al) has 27 items, converted into 4 scales ranging from 1–7.
Results: The scores obtained are shown in the table.
With the MacNew significant positive changes could be measured from baseline to follow-up in all scales, whereas with the PLC the physical domain only showed a significant change in the same patients.
Conclusion: The MacNew questionnaire is more sensitive than the PLC to detect changes in quality of life among cardiac patients after rehabilitation. The number of items used in a questionnaire seems to be less important than the number of steps in the answering scale.
Quality of life scores
Scale
Baseline
Follow-up (1 year)
p-value
PLC physical capacity
2,85±0,72
3,05±0,63
8,1 E-5
PLC psychol. functioning
2,72±0,64
2,71±0,71
ns
PLC pos. mood
3,23±0,71
3,25±0,74
ns
PLC neg. mood
3,05±0,54
3,10±0,61
ns
PLC social functioning
3,31±0,62
3,29±0,65
ns
PLC social wellbeing
3,09±0,54
3,13±0,57
ns
MacNew global
5,70±0,73
5,97±0,72
1,74 E-8
MacNew physical
5,71±0,82
6,03±0,76
2,20 E-9
MacNew emotional
5,70±0,83
5,87±0,84
1,10 E-3
MacNew social
5,85+0,79
6,24±0,69
1,30 E-12
200 HAPIEE study: effect of obesity and overweight on the quality of life and perceived health in Lithuanian population of Kaunas city
M Baceviciene; A Tamosiunas; R Reklaitiene; R Radisauskas; E Daugeliene
Institute of Cardiology, Kaunas University of Department of Population Studies, Kaunas, Lithuania
Purpose: The aim of this study was to examine the prevalence of overweight and obesity among Lithuanian men and women aged 45–72 and to investigate the relationship between body mass index (BMI), quality of life (QOL) and perceived health.
Methods: The HAPIEE study comprises for random samples from Russia, Poland, the Czech Republic and Lithuania (Kaunas city). Lithuania joined the project in 2006. Sample was randomly selected from the population register of Kaunas city. Planed size of the total sample is 7000 men and women aged 45–72. In this study we used the data of 4297 participants: 1923 men and 2374 women examined up to June 2007. Response rate for this period was 55.2%.
The normal body weight was defined as BMI 18.5–24.9 kg/m2, overweight – BMI 25.0–29.9 kg/m2 and obesity – BMI =30.0 kg/m2. The direct method was used for age standardization using European population as a standard.
Results: Overweight was less prevalent among women than among men (35.9% and 45.7%, respectively, p>0.001). 31.6% of men and 41.5% of women were obese (p>0.001). Among men the relationship between QOL and BMI was not found (Pearson Chi-Square=7.3, p>0.05). Women with obesity had significantly lower QOL: 50.4% of obese women rated their overall QOL as very bad or bad and 39.5% - as good or very good (p>0.05).
Women with BMI>25.0 kg/m2 more often reported very good and good perceived health than average or poor and very poor (26.4%, 17.8% and 14.5%, respectively, p>0.001). Obese and overweight men and women more often rated their health as average, bad and very bad than good or very good (p>0.01). There were no statistically significant differences of subjective health ratings in men with BMI>25.0 kg/m2.
Conclusion: Obese and overweight persons aged 45–72 comprise more than 70% of Lithuanian population. Persons with obesity had significantly lower perceived health and QOL. This relationship should receive more attention in clinical care and research as excess body weight is usually related with co-morbid illness and even more impaired health and QOL. The impact of chronic diseases linked to obesity on the QOL will be investigated in future HAPIEE project studies.
201 Quality of life in early old age and mortality in Eastern European population
H Pikhart1; A Nicholson1; R Kubinova2; A Peasey2; M Bobak2; M Marmot2
1UCL Epidemiology And Public Health, London, United Kingdom
2NIPH, Prague, Czech Republic
Background: Quality of life has been extensively studied in western populations but there is lack of data from non-western countries. For this presentation, we investigated the relationship between quality of life in early old age and mortality from all causes and from cardiovascular diseases (CVD).
Methods: The baseline survey for the HAPIEE study examined random sample of middle-aged men and women in 6 cities of the Czech Republic. A total of 3,508 individuals aged 50 years and more answered questions on quality of life in early old age (measured by the CASP-19 instrument), socio-economic circumstances and other covariates. The cohort was followed-up for mortality (mean follow-up 3 years, maximum 4.3 years). The CASP-19 score was divided into quartiles and the association with mortality was assessed using Cox regression modelling.
Results: By the end of 2006, there were 142 deaths from all-causes and 47 from CVD. There was a strong and statistically significant association between CASP-19 and all-cause and CVD mortality. Those in the highest quartile of CASP-19 score had 4-fold reduction in risk of all-cause mortality and 5-fold reduction in risk of CVD mortality (HR=0.25 for all-cause mortality and 0.19 for CVD mortality). Mortality (both all-cause and CVD) increased with decreasing CASP-19 scores (p-value for linear trend in HR >0.001 for all-cause mortality and 0.006 for CVD mortality). There was no gender difference in the association between quality of life and all-cause mortality; for CVD, the small number of female deaths does not allow evaluation of interactions. Adjustment for various measures of health status and cognitive functioning at baseline did not substantially reduce the effect of CASP-19 on mortality
Conclusion: CASP-19, a measure of quality of life in early old age, strongly predicts all-cause and CVD mortality in this sample of the Czech population. This association remains significant when physical health, cognitive functioning and social circumstances at baseline are taken into account.
202 Factors, which influence on quality of life of the patients with angina pectoris
A Ibatov
Moscow Medical Academy Cardiology, Moscow, Russian Federation
Purpose: to study relation of quality of life and emotional status of the patients with ischemic heart disease (IHD).
Methods: 277 patients with IHD (176 men and 71 women) from 36 till 67 years (average age 55.2+7.2 years) were examined. All patients had angina pectoris (11-1V functional class). A level of depression was estimated by Beck's Depression Scale Inventory (BDI), level of state and trait anxiety - by Spielberger questionnaire for State-Trait Anxiety Inventory (STAI), quality of life - by Seattle Angina Questionnaire of quality of life (SAQ).
Results: The level of state anxiety was 43.4+1.2 scores (from 20 till 76 scores). The level of trait anxiety was 47.3+0.9 scores (from 36 till 67 scores). The level of depression was 14.9+0.9 scores (from 2 till 45 scores). The score of Physical limitation scale SAQ negatively correlated with function class of angina pectoris (r= −0.46 p>0.01), level of depressive disorders on a scale Beck (r= −0.29 p>0.01). The score of Angina stability scale SAQ negatively correlated with a level of depression (r= −0.21 p>0.01). The score of Angina frequency scale SAQ negatively correlated with the of angina pectoris function class (r= − 0.35 p>0.01). The score of Treatment satisfaction scale SAQ negatively correlated with a level of state and trait anxiety (r= −0.37 p>0.01 and −0.29 p>0.01, respectively), level of depression (r= −0.24 p>0.01). The score of Disease perception scale SAQ negatively correlated with a level of state and trait anxiety (r= −0.36 p>0.01 and −0.33 p>0.01) and level of depressive disorders (r= −0.38 p>0.01). Total score scale of quality of life SAQ negatively correlated with a degree of coronary atherosclerosis (r= −0.12 p>0.05; not significant), function class of angina pectoris (r= −0.48 p>0.01), level of state and trait anxiety (r= −0.26 and −0.21), and level of depression (r= −0.38 p>0.01). Influence of various factors on quality of life was examined by factorial ANOVA analysis. Total score scale of quality of life SAQ was influenced the function class of angina pectoris (F=18.7; p=0,0000), level of trait anxiety (F=13.3; p=0.000003), degree of depression (F=11.1; p=0,00003), level state anxiety (F=10.1; p=0.00006), smoking (F=5.4; p=0.02), age of the patient (F=4.4; p=0.012), degree of coronary atherosclerosis (F=3.5; p=0.017).
Conclusion: Life quality of the patients with angina pectoris more depends on the function class of angina pectoris, level of depression and anxiety, than from the degree of coronary atherosclerosis.
203 Relationship between quality of life and cardiovascular risk factors: a population based study in Lithuania
M Baceviciene; R Reklaitiene
Institute of Cardiology, Kaunas University of Department of Population Studies, Kaunas, Lithuania
Purpose: This study aimed to identify the impact of the cardiovascular risk factors on the quality of life (QOL) among middle-aged Lithuanian population.
Methods: A representative random sample of 1403 Kaunas city (Lithuania) men and women aged 35–64 years and stratified by age and sex was examined in 2002. QOL was assessed by the self-administered World Health Organization Quality of Life 100 (WHOQOL-100) questionnaire. To detect cardiovascular risk factors objective health examination and face-to-face interview were performed. To assess which factors affect QOL a multivariate analysis was performed.
Results: WHOQOL-100 showed high reliability and high convergent and discriminant validity results therefore the WHOQOL-100 is a suitable instrument for evaluating QOL.
Increasing age had a negative impact on both men's and women's QOL in most of the WHOQOL-100 domains. Overweight (BMI 25.0–29.9 kg/m2) and obese (BMI = 30kg/m2) men had by 69% and 77%, respectively, lower probability of rating their overall QOL worse as compared to men with BMI>25.0 kg/m2, whereas obesity had a negative impact on men's QOL in the independence domain as compared to ones with BMI >25.0 kg/m2 (OR=1.87; 95% CI=1.11–3.16). Obesity for women increased the odds of having worse QOL in the psychological and independence domains as compared to women with BMI of >25.0 kg/m2. Smoking increased the probability of having worse QOL in the environment and psychological domains for both men and women as compared to non-smoking ones. Inadequate physical activity was associated with worse QOL among women. Moderate-to-heavy alcohol consumption was associated with lower risk of having worse QOL in the physical domain (by 40%) among women and in the independence domain among both men and women by 54% and by 42%, respectively, as compared to light alcohol consumption. Indeed in the social relationships domain, moderate-to-heavy alcohol consumers had a higher probability of rating their QOL worse as compared to the light consumers among women (OR=1.62; 95% CI=1.11–2.35). CHD increased the probability of scoring lower in the independence domain for men (OR=1.84; 95% CI=1.09–3.10) and for women (OR=1.67; 95% CI=1.06–2.62) as compared to ones without CHD. Diabetes had a negative impact on men's overall QOL and health (OR=1.78; 95% CI=1.09–2.89).
Conclusion: Health perception and QOL are significantly affected by a clinical situation characterized with cardiovascular risk factors. An inverse relationship between BMI and overall QOL was found in a male population.
204 Is the Mac New quality of life questionnaire a useful diagnostic and evaluation instrument for cardiac rehabilitation?
V De Gucht1; S Maes1; R Goud2; I Hellemans3; N Peek3
1Leiden University Health Psychology, Leiden, Netherlands
2University of Amsterdam Medical Informatics, Amsterdam, Netherlands
3Free University of Amsterdam Health Sciences, Amsterdam, Netherlands
The MacNew quality of life questionnaire is used as the standard for psychosocial assessment in Dutch cardiac rehabilitation centres. This study investigates its sensitivity (differentiating capacity between diagnostic disease categories, gender and age) at entry (T1) and at the end (T2) of cardiac rehabilitation as well as the responsiveness of the MacNew during this period. Data was used from 6288 cardiac rehabilitation patients at T1 and 1654 at T2.
Results: show that the total MacNew as well as the three (physical, emotional, social) subscales have high internal consistencies, and differentiate well and in the expected direction at T1 between diagnostic groups (heart surgery, acute coronary syndrome, stable angina, internal cardio defibrillator (ICD) and heart failure patients), gender and age. The MacNew also proves to be an adequate evaluation instrument for cardiac rehabilitation, since all scales are responsive enough to capture changes over this period. At T2 however, the MacNew looses some of its sensitivity, partly because of ceiling effects. It is suggested to complement the assessment of the MacNew both at T1 and T2 with a brief anxiety and depression measure, which is valid, sensitive and responsive for cardiac rehabilitation patients.
205 Impact of diabetes on quality of life results in patients with stable angina treated by coronary angioplasty
I Uchmanowicz1; K Loboz-Grudzien1; L Sokalski2
1Medical University Public Health Department, Wroclaw, Poland
2Marcinak's Hospital Cardiology, Wroclaw, Poland
Introduction: Patients with diabetes (D) have an increased incidence of coronary heart disease (CHD) which leads to an increased requirement for percutaneus coronary intervention (PCI). Angina limits normal activities, thus it has a negative impact on quality of life (QOL). There are still controversies regarding the impact of diabetes on QOL. The aim of this study was to assess whether D influences the quality of life.
Methods: Data were collected from 60 patients. They were divided in two groups: I/ 30 patients with CHD with coexisting D type 2 (men age:61,3), and II/ 30 non-diabetic (nD) patients with CHD (mean age: 60,3). We measured changes in patient QOL using SF-36 questionnaire
Results: The D and nD patients were found to have statistical differences in respect to: demographic factors, clinical variables, and cardiac risk factors. In general, D reported lower QOL outcomes than nD patients. Among analysed variables, for patients with D only a level of education was associated with higher Physical Component Summary (PCS) and Mental Component Summary (MCS) results at 6 months follow-up: (α-coefficient:4,89 (95% CI: 4,55,4,23; p>0,34), and (α-coefficient: 0,82, 95% CI: 0,06, 1,58; p>0,76), respectively. With lower PSC results: older age>65: α -coefficient: 3,54, 95% CI: 2,56, 4,52; p>0,98), more single persons α -coefficient: 2,56, 95% CI:1,59, 3,53; p>0,97), higher the Canadian Cardiovascular Society's classification (CCSS) class (α -coefficient: 4,49, 95% CI: 3,85, 5,13; p>0,64), lower left ventricular ejection fraction (α-coefficient: 6,39, 95% CI 5,4,7,38; p>0,99). Lower MCS results at 6 month-follow up were associated with: older age>65 (α-coefficient: 3,18, 95% CI: 3,3,36), p>0,18), more single persons (α-coeficient: 2,58, 95%: 1,76, 3,4, p>0,82), more retired patients (α-coefficient: 1,03, 95% CI: 0,48,1,58; p>0,55).
Conclusion: 1/ Diabetes mellitus itself is not a significant determinant of the QOL results after PCI.
206 Aerobic capacity and LV ejection fraction are predictive of life quality in heart failure
LV Athanasopoulos; A Dritsas; DV Cokkinos
Onassis Cardiac Surgery Center 1st Cardiology Department, Athens, Greece
Purpose: This study was conducted to determine which echocardiographic and laboratory variables are predictive of quality of life (QoL), as derived from approved heart failure specific QoL questionnaire scores.
Methods: Measurements were taken of peak VO2 derived from exercise tredmill testing, plasma N-terminal prohormone of BNP (NT-proBNP) and echocardiographic markers (LVEF, LA, LVDD, LVSD) in 62 patients with CHF. Patients also completed the Minnesota Living with Heart Failure Questionnaire (MLHF). The positively skewed NT-proBNP values were log-transformed.
Results: The (mean±SD) MLHF score was 22.4±13. The peak VO2 was 19.6±5.5 ml/kgr/min and the LVEF was 30.8±6.8%. Median value and interquartile range of NT-proBNP was 495.5 pg/ml (178.8–1247.5). On linear regression analysis and after adjusting for age and sex the variables that were significantly predictive of MLHF score were: peak VO2 [β(SE)= −1.136 (0.265), p>0.001], LVEF [β(SE)= −0.949 (0.216), p>0.001], LA [β(SE)=0.807 (0.23), p=0.001] and logNT-proBNP [β(SE)=8.391 (2.572), p>0.01]. On multiple linear regression and after adjusting for age and sex the only variables that continued to be predictive were peak VO2 [β(SE)= −0.806 (0.37), p>0.05] and LVEF [β(SE)= −0.577 (0.288), p=0.05]. On stepwise multiple regression analysis, the only variable that entered the model was LVEF [β(SE) = −1.008 (0.239), p>0.001] accounting for 25% of the variability of the MLHF score.
Conclusion: Aerobic capacity and LVEF are predictive of poor quality of life as measured by MLHF.
207 Serum collagen type I degradation peptides correlate with quality of life in chronic heart failure patients
S Chatzikyriakou1; DN Tziakas1; GK Chalikias1; DA Stakos1; A Thomaidi1; DF Floros1; K Mitrousi1; AE Lantzouraki1; H Boudoulas2
1Democritus University of Thrace University Cardiology Department, Alexan-droupolis, Greece
2Academy of Athens Center for Clinical Research, Biomed Research, Athens, Greece
Introduction: Chronic heart failure (CHF) is characterized by structural alterations and functional limitations. One of the major determinants of heart failure-associated structural alterations is abnormal extracellular matrix (ECM) metabolism. Circulating levels of collagen type I degradation peptides have been proved to correlate with cardiac ECM changes. On the other hand, previous studies have shown that quantification of functional limitations in CHF can be assessed using the “Minnesota Living with Heart Failure Questionnaire” (MLHFQ). With the present study, we investigated the correlation between the levels of collagen-derived serum degradation peptides and the quality of life (QOL) scoring using the MLHFQ, in CHF patients during a period of six months follow up.
Methods: We recruited 124 stable CHF patients (88 men, 67±12 years), NYHA class II-IV with an ejection fraction of 39±13% attending our Outpatient Heart Failure Clinic, during a routine follow up visit and after their CHF stable status was confirmed. Both on recruitment and at six month follow up, we assessed serum concentrations of the carboxy-terminal telopeptide of collagen type I (CITP), index of collagen type I degradation, by commercially available immunoassay. We, also, assessed their physical, emotional, social and mental dimensions of their quality of life using the MLHFQ. All patients were under standard treatment for CHF. MLHFQ score was assessed as dichotomous variable using its median value as cut-off point (score=45) as this level is considered to represent a clinically relevant score associated with good or poor QOL. Patients presenting with symptoms or signs of acute decompensation of their stable CHF status during the follow-up, were excluded from the study.
Results: CHF patients with low MHLFQ score (associated with good QOL) were characterized with a more pronounced increase (p=0.049) in CITP levels (+0.122 ng/ml 95% CI +0.06 to +0.166 ng/ml) during the 6 months follow up compared to patients with high MHLFQ score (associated with poor QOL) (+0.066 ng/ml 95% CI −1.6 to +0.144 ng/ml). Conclusion: The present study showed that in patients with CHF, good QOL as assessed with MHLFQ score is characterized by increased collagen type I degradation during a follow-up of 6 months. These findings suggest that possibly quality of life in heart failure is associated with alterations of cardiac ECM remodelling. Therefore circulating levels of collagen metabolism may represent a novel therapeutic and prevention target in heart failure setting.
208 Quality-of-life score, NYHA validity class and exercise parameters: different tools to grade heart failure
MGJ Gademan; R Van Wamelen; JCW Haest; MJ Schalij; EE Van Der Wall; CA Swenne
Leiden University Medical Centre, Leiden, Netherlands; Leiden, Netherlands
Background: NYHA validity grading characterizes the severity of chronic heart failure (CHF) according to the exercise intensity at which complaints arise. The exercise related questions of the Minnesota Living with Heart Failure Questionnaire (MLWHFQ) assess the impact of restricted exercise capacity on the quality of life. Hence, both grading systems probe other dimensions of the CHF related exercise limitations. It is, however, not known how much agreement exists between the NYHA validity class and the MLWHFQ physical subscore and which of these two scores relates best to major exercise-test derived parameters.
Purpose: To investigate the mutual relationship of the NYHA validity class, the MLWHFQ physical subscore and the objectively measured exercise capacity in patients with CHF.
Methods: We studied 117 CHF patients (91M/26F, age 62.5±10.0, NYHA I-III, LVEF 31.0±8.7) who successively visited our heart failure outpatient clinic. All patients completed the MLWHFQ and performed a symptom-limited exercise test and a 6-minute walk test (6MWT). Pearson rank correlations were computed between exercise testing variables, MLWHFQ full score, MLWHFQ physical subscore (questions 2–7 and 12–13) and NYHA class.
Results: MLWHFQ physical subscore and NYHA class correlated significantly (P>0.01; r=0.60). The MLWHFQ physical subscore also correlated significantly with the MLWHFQ full score (r=0.90), 6MWT (r= −0.51), oxygen uptake efficiency slope (r= −0.32), VE/VCO2 slope (r=0.32) and VO2 peak (r= −0.27). NYHA class correlated significantly with the MLWHFQ full score (r=0.53), 6MWT (r= −0.42), VO2 peak (r= −0.37), oxygen uptake efficiency slope (r= −0.35) and VE/VCO2 slope (r=0.33).
Conclusion: Although the MLWHFQ physical subscore and NYHA class correlated significantly, their association is rather weak (r∗∗2=0.36). The associations between, on one hand, the NYHA class and the MLWHFQ physical subscore and, on the other hand, the exercise capacity parameters were considerably weaker (r∗∗2>0.26). In conclusion, the NYHA class, MLWHFQ physical subscore, and exercise capacity are only weakly associated. As a consequence, these measurements cannot replace each other and are all needed for a complete evaluation of heart failure severity.
209 (WITHDRAWN) Health status in patients treated with CRT: modulating effects of personality
A Schiffer1; J Denollet2; SS Pedersen1; H Broers3; JW Widdershoven3
Purpose: Cardiac resynchronisation therapy (CRT) is a promising treatment in chronic heart failure (CHF), but a subgroup of patients still report impaired health status, cardiac symptoms and feelings of disability. We examined (1) whether CHF patients treated with CRT improved in patient-centred outcomes and functional capacity, and (2) whether personality traits exerted a stable effect on these outcomes over 2 months.
Methods: 31 CHF patients treated with CRT (65% male;mean age 70±8), completed the Type D Scale (negative affectivity, i.e. tendency to experience negative emotions, and social inhibition, i.e. tendency to inhibit self-expression), the Minnesota Living with Heart Failure Questionnaire (disease-specific health status) and the Health Complaints Scale (cardiac symptoms, perceived disability), and performed the 6-minute walking test (functional capacity).
Results: There was general improvement in disease-specific health status (p>.001), cardiac symptoms (p=.001), perceived disability (p>.001), and functional capacity (p=.007) over 2 months. However, high negative affectivity patients reported significantly lower disease-specific health status (p=.046), and more cardiac symptoms (p=.035) and perceived disability (p=.015), as compared to low negative affectivity patients. There was no significant main effect for negative affectivity on functional capacity. High negative affectivity patients still reported lower disease-specific health status (p=.06) and significantly more perceived disability (p=.04), when adjusting for left ventricular dysfunction, gender and age. The effects of negative affectivity on patient-centred outcomes, as measured by Cohen's effect size index, were moderate to large compared to small effects for gender.
Conclusion: Patient-centred outcomes improved over a 2-month period in patients treated with CRT, but negative affectivity exerted a stable, negative effect on health status, cardiac symptoms and perceived disability. Personality traits should be taken into account when evaluating effects of CRT.
210 Changes on health related quality of life following an acute coronary syndrome in patients participating on a cardiac rehabilitation programme
N Casanovas1; P Cabero2; L Recasens2; J Marti2; J Punti1; E Guillaumet1; JR Guma1; R Baga1; R Serrat2; J Bruguera2
1Hospital de Sabadell Cardiology, Sabadell, Spain
2Hospital del Mar Cardiology, Barcelona, Spain
Purpose: To describe changes in health related quality of life (HRQOL) after an acute coronary syndrome (ACS) in patients attending a cardiac rehabilitation programme (CRP) depending on their participation or not on a supervised exercise training programme.
Methods: All patients admitted to our hospital for an ACS during 2003 and 2004 were evaluated to participate in our CRP. 62 patients were finally included in the study. Main reasons for exclusion were age, impossibility to complete an exercise stress test or patient rejection. All patients received an specific educational programme including nutritional, physical activity and smoking cessation counselling. Patients were randomized to a monitored exercise training programme (group 1: 32 patients) or not (group 2: 30 patients). There were no statistical differences in main basal clinical characteristics between groups. HRQOL was assessed with the Medical Outcome Trust Short Form (SF-12) questionnaire that was distributed at baseline and at months 6 and 12 of follow-up.
Results: Scores for the results of the SF-12 questionnaire were calculated following the norm-based scoring algorithm. Results are expressed with the two summary scores: physical component summary (PCS) and mental component summary (MCS). Table 1 shows the results in both groups with no statistical differences at baseline and at follow-up.
All patients showed a significant and persistent increase on both mental and physical component summaries at 6 and 12 months. Baseline scores were similar to those found in other published studies.
Conclusion: No differences on HRQOL were found on patients participating on a CRP with or without an exercise training programme after an ACS. Although all patients showed a significant improvement on HRQOL, PCS was under the mean for general population even after 12 months of the ACS.
GROUP 1
GROUP 2
P
PCS-Baseline (mean±SD)
41,81 (9,25)
40,68 (10,01)
ns
MCS-Baseline (mean±SD)
46,68 (12,05)
46,46 (11,18)
ns
PCS-6 months (mean±SD)
44,77 (8,62)
45,38 (11,47)
ns
MCS-6 months (mean±SD)
49,31 (10,79)
51,88 (10,21)
ns
PCS-12 months (mean±SD)
47,13 (8,58)
46 (9,47)
ns
MCS-12 months (mean±SD)
50,25 (10,6)
53,20 (10,19)
ns
Health related quality of life at baseline and at follow-up.
211 Quality of life predictors in secondary prevention of coronary heart disease
O Mayer Jr1; J Simon1; M Galovcova2; J Bruthans2; R Cifkova2
1Charles University, Medical Faculty 2nd of Internal Medicine, Plzen, Czech Republic
2Institute of Clin. and Experimental Medicine Department of Preventive Cardiology, Prague, Czech Republic
Purpose: Psychosocial and physical well-being represents important goal of medical care. We aimed to identify the psychosocial and somatic predictors of quality of life (QoL) in patients with chronic coronary heart disease (CHD).
Methods: 476 patients with clinical CHD, 373 males and 103 females, mean age 62.7±0.39 were included into a cross-sectional study. QoL was evaluated using standardized SF36 questionnaire. The large set of potential predictors were included into step-wise logistic regression. Impaired QoL (defined as SF Score>50) was used as dependent variable (separately in physical and mental health dimensions by SF36 scoring system). Following variables were included into full model: age, gender, current smoking, moderate alcohol intake (44–308 g weekly), raised blood pressure (<140/90), raised LDL cholesterol (<2.5), diabetes (glucose<7 or antidiabetic treatment), metabolic syndrome (by current IDF definition), subclinical or over hypothyroidism (TSH<4.1) and hyperthyroidsm (TSH>0.4), anxiety and depression by Hospital Anxiety and Depression Score (<7 of score), overt or subclinical heart failure (BNP<150), reported angina pectoris (by Rose Questionnaire) and treatment with betablockers, ACE inhibitors or statins.
Results: The variables entering significantly the regressions are given on Table 1 as odds ratio and 95% confidence intervals.
Conclusion: Anxiety and depression, heart failure and angina pectoris were identified as most power-full factors adversely influencing both, mental and physical dimensions of QoL. These factors should be intervened by specific treatment.
Independent variables:
Mental health
Physical health
Anxiety
8.75 (4.57–16.75)
5.25 (2.76–10.0)
Depression
4.23 (2.37–7.57)
3.79 (2.17–6.60)
Angina pectoris
2.16 (1.08–4.34)
6.85 (3.49–13.4)
Heart failure
2.57 (1.46–4.52)
1.73 (1.02–2.93)
Moderate alcohol intake
0.46 (0.26–0.82)
0.54 (0.32–0.89)
212 Life quality estimation by Duke Activity Status Index questionnaire in patients after aortic valve replacement
DE Velimirovici; M Rada; S Dragan; CA Sarau; DM Duda-Seiman; A Schnabel; M Berceanu; FI Cobzariu; G Mancas; S Mancas
Univ. of Medicine & Pharmacy Victor Babes Cardiovascular Rehabilitation Clinic, Timisoara, Romania
Objective: to establish the benefit of post operatory cardiovascular rehabilitation program on functional capacity and on quality of life for patients after aortic valve replacement.
Materials and methods: we used the Duke Activity Status Index (DASI) questionnaire to assess the quality of life; DASI was developed generally for adults with cardiovascular pathology. Duke index is evaluated on a semi continuous scale with possible scores between 0 and 58.2. Maximal scores indicate a good physical capacity, and a score of 0 points reflects the inability to carry out usual activities of daily living. 82 patients were divided in 2 groups: training group (A) – 43 patients and control group (B)-39 patients. The two groups of patients completed a self-administered questionnaire to determine the quality of life, at the time of inclusion and after 3 months (the end of phase II of cardiovascular rehabilitation).
Results: and discussions: to obtain a better quantification, scores were grouped as fallows: 0–18; 19–26; 27–32; 33–42; 43–50; 51–58. Albeit there is a predominance of low DASI scores at study admission time-24,39% (score 0–18), after 3 months we remark a proportion of the patients with higher DASI scores −52,05% (score 51–58), demonstrating a significant improvement of functional capacity in patients with aortic valve replacement. After 3 months of physical training the patients improved their DASI score with 66.78% (from 27.85 at study admission time to 46.45 at the end of phase II RC). In the control group, we remark a less significant improvement of the score- 35.65% (from 25.52 at the time of inclusion to 34.62 after 3 months). Gender differentiated analyze for DUKE score discloses the most evident improvement for male training group, from 32,8 to 52,3, (p>0,001), versus female training group with an improvement from 22,9 to 33,8 (p>0,01).
Conclusion: DASI score that reflect physical condition and health self-esteem have a more favorable evolution in patients that participate to cardiovascular rehabilitation programs versus sedentary subjects. Physical training contributes to the increase of functional capacity and quality of life. Gender differentiated analyze for DASI evolution scores discloses the most obvious progress in male patients included in cardiovascular rehabilitation program.
213 Physical training efficiency on life quality evaluation by short form 36 questionnaire in patients after aortic valve replacement
M Rada; DE Velimirovici; S Dragan; DM Duda-Seiman; CA Sarau; A Schnabel; M Berceanu; FI Cobzariu; G Mancas; S Mancas
Univ. of Medicine & Pharmacy Victor Babes Cardiac Rehabiltation Clinic, Timisoara, Romania
Objective: evaluation of life quality amelioration at the end of phase II of cardiovascular rehabilitation, using Short Form 36 questionnaire (SF 36) for patients after aortic valve replacement, SF 36 is the most used questionnaire for evaluation of life quality for patients after cardiac surgery.
Methods and Materials: monitoring of cardiac rehabilitation program effects on life quality for 82 study included patients was performed by assessing the two questionnaire components physical (PSC36) end mental (MCS-36) at admission and after 3 months (the end of phase II of cardiovascular rehabilitation). Synopsis estimation of the two components was effectuated on internet site www.sf-36.org/demos/SF-36html. To quantify obtained data, an original score with limits between 0 and 100 was utilized: 0-the powerless and 100 the best possible health condition. Study eligible patients were divided in two groups: training group (A) – 43 patients and control group(B) – 39 patients.
Results and Discussions: at the beginning of the study, the physical component (PCS-36) had lower score comparative to the mental score (MCS-36) in patients with aortic valve replacement included in cardiovascular rehabilitation program, and also in the control group, because of physical decoditioning secondary to preoperatory disease. After phase II of cardiac rehabilitation program we remark a favorable evolution of the PCS-36 component (from an average value of 33,67±16,2 to 60,45±23, p>0,0001). Contrarily, PCS-36 amelioration on B-group was less obvious: from 28,82±18,2 to 44,45±25,1 after 3 months (p>0,001). Regarding the MCS-36 component, A-group patients had obtained more significant statistical results from 47,31±27,5 to 62,35±32,4 (p>0,01), compared to the B-group from 41,3±22,41 to 51,3±24,2 (p>0,05).
Conclusion: the actual purpose of cardiac rehabilitation program is not only life prolongation, but also to enhance the quality of life that becomes one of the leading goal. Albeit in both groups lifestyle changes according to guideline recommendations were preserved, patients who benefit from individual and standardized physical training had a significant improvement of physical condition and functional capacity, also of mental condition, compared to the control group.
214 Modifications of cardiopulmonary capacity are not associated with changes in quality of life in patients with congenital heart disease
N Ehlert; J Hess; A Hager; Munich, Germany
Objective: The intention of surgical and medical treatment is to improve the cardiovascular status and exercise ability. However, do improvements of exercise ability also result in a better quality of life?
Patients and Methods: 194 patients (85 female, 109 male, age 14–81 years) with various congenital heart defects were investigated twice. At each time, they completed the SF-36 quality of life survey and, afterwards, they performed a symptom-limited cardiopulmonary exercise test. In-between the two tests, 48 patients had a change in their medicational regime, 34 open heart surgery, 10 a catheter intervention, and 102 had no changes in their medical management for at least 6 month.
Results: Patients were classified into 3 groups. 47 patients showed an increase in peak oxygen uptake for more than 10%, in 88 patients it remained similar (±10%) and in 53 patients it declined for more than 10%.
Comparing the 3 groups, there were no significant changes in any of the scales of quality of life. Even in self-reporting physical functioning, there was no difference between those three groups. (Kruskal-Wallis test p=.909).
Conclusion: Improvements or worsening of physical exercise ability do not automatically result in an improvement or worsening of quality of life and have to be evaluated and analyzed separately. Patients with congenital heart disease do not recognize objective measurable improvments or worsening of their capacity in their subjective evaluation.
215 The association of cardiovascular autonomic neuropathy in type 2 diabetic patients with vascular structural changes
I Bondar; O Shabelnikova
Novosibirsk State Medical University Endocrinology Department, Novosibirsk, Russian Federation
Background and Aims: Cardiovascular autonomic neuropathy is important cardiovascular risk factor. The aim of was study to evaluate carotid intima-media thickness in type 2 diabetic patients with autonomic neuropathy and without. Carotid intima-media thickness with cardiovascular standard reflex testis in these subjects was compared.
Materials and Methods: 95 type 2 diabetic patients (30M/65F, age 53,4±5,4 (SD) years) were examined, including 70 patients (22M/48F, age 54,0±5,6 years) with the cardiovascular autonomic neuropathy (group 1) and 25 patients (8M/17F, age 51,8±4,5 years) without autonomic neuropathy (group 2). Right and left common carotid artery stiffness indices were assessed with noninvasive ultrasound method in both groups. A five standard cardiovascular reflex test battery, as proposed by Ewing, was performed in both groups.
Results: The difference in the intima-media thickness was statistically significant in the patients with type 2 diabetes with cardiovascular autonomic neuropathy (1,28±0,155 mm) as compared to the patients with type 2 diabetes without autonomic neuropathy (1,17±0,199mm) (?=0,004). Stenosis of the common carotid artery was revealed in 29 (41%) patients with type 2 diabetes with cardiovascular autonomic neuropathy and in 2 (8%) patients without autonomic neuropathy (?=0,037). Carotid intima-media thickness correlated significantly with cardiovascular reflex respiratory test (?=0,03).
Conclusion: The results of the study indicate that cardiovascular autonomic neuropathy in patients with type 2 diabetes is associated with vascular structural changes. These data suggest the role of autonomic neuropathy on development of cardiovascular disease in diabetes.
216 Decreased plasma levels of soluble receptor for advanced glycation end-products in type 2 diabetes mellitus: association with oxidative stress and metabolic control
F Santilli1; E Devangelio1; G Formoso1; P Ferroni2; L Bucciarelli3; N Michetti2; C Clissa2; G Ciabattoni2; A Consoli2; G Davi2
1University of Chieti, Chieti, Italy
2IRCCS San Raffaele, Rome, Chieti, Italy
3University of Milan, Milan, Italy
Purpose: Advanced glycation end-products (AGEs) contribute to diabetic vascular complications by engaging the AGE receptor (RAGE). A soluble RAGE form (sRAGE) can act as a decoy domain receptor thus decreasing AGE cellular binding. Aim of the study was to compare sRAGE plasma levels in patients with type 2 diabetes (T2DM) vs age-matched nondiabetic subjects. We also investigated whether improving metabolic control affects sRAGE and asymmetric dimethylarginine (ADMA) levels in T2DM.
Methods: A cross-sectional comparison of sRAGE, ADMA levels (index of endothelial dysfunction), and urinary 8-iso-PGF2a (marker of oxidative stress) was performed between 86 T2DM patients and 43 controls. In addition, 24 of 86 patients with newly-diagnosed diabetes and 12 of 86 patients in poor metabolic control were re-evaluated for sRAGE and ADMA levels after 12 weeks of treatment with an hypoglycemic agent or with insulin, respectively.
Results: Plasma sRAGE levels were significantly lower and ADMA levels were significantly higher in T2DM as compared to controls (P>0.0001). HbA1c was inversely correlated with sRAGE and directly correlated with ADMA. Urinary 8-iso-PGF2a correlated directly with both sRAGE (Rho= −0.332; P=0.009) and ADMA levels (Rho=0.253; P=0.047). Improvement in metabolic control achieved by oral agents (n=24) or insulin (n=12) resulted in a significant increase in sRAGE levels [1044 (942–1317) pg/mL vs. 786 (620–992) pg/mL, P>0.0001] and a significant decrease in ADMA levels [0.88 (0.76–1.1) micromol/L vs 0.75 (0.54–0.86) micromol/L, P>0.0001)] (Figure).
Conclusion: Poor glycemic control reduces sRAGE levels, in association with enhanced oxidative stress and endothelial dysfunction in T2DM. We thus suggest that sRAGE might serve as an endogenous protection factor in T2DM.
217 Association between autonomic function and incidence of type 2 diabetes in healthy Korean men
SY Jae1; KS Heffernan2; B Fernhall1; MK Lee3
1University of Seoul Sports Informatics, Seoul, Korea, Republic of
2University of Illinois at Urbana & Champaign Kinesiology and Community Health, Champaign, United States of America
3Samsung Medical Center Department of Medicine, Seoul, Korea, Republic of
Impairment of autonomic nervous system activity is associated with the development of type 2 diabetes in westernized society. Insulin secretion capacity is genetically lower in Asian individuals than in Caucasians. Whether autonomic impairment contributes to the development of diabetes across ethnic groups is unknown. We hypothesized that slow heart rate recovery (HRR) after exercise testing, indicative of decreased autonomic nervous system activity, would be an underlying causal factors in the development of type 2 diabetes in 1813 healthy Korean men. HRR was calculated as the difference between maximum heart rate during the exercise test and heart rate 1 minute after cessation of the exercise test. During an average of 6.4-years of follow-up, 64 (3.5%) subjects developed type 2 diabetes. The unadjusted relative risk (RR) of developing incident diabetes in the slowest HRR quartile had a 3.13 (95% CI, 1.28–7.65) compared with the highest HRR quartile. However, these relationships were no longer significant after adjustment for risk factors (RR=2.28, 95% CI, 0.87–5.95). Similar results were observed when HRR was studied as a continuous variable (RR=1.00, 95% CI, 0.97–1.04).
These results suggest that slow HRR after exercise is associated with development of type 2 diabetes but this relationship was dependent on confounding factors in healthy Korean men. Further studies are needed to clarify this association.
218 Association of high sensitivity C-reactive protein with hyper-triglyceridemic waist in patients with type 2 diabetes
H Rosolova; B Petrlova; J Simon
University Hospital in Pilsen 2nd Medical Department, Pilsen, Czech Republic
Purpose: Type 2 diabetes (DM2) patients have enormously high cardiovascular (CV) risk. High sensitive C reactive protein (hs-CRP)=33 mg/l has been found as a significant biomarker of CV risk. Aim of this cross-sectional study was to find cardio-metabolic risk factors responsible for increased CV risk in DM2 patients stratified by hs-CRP level.
Methods: 417 DM2 patients without any inflammatory disease were included; personal history, physical examination and 12-h fasting venous blood taking were done. Plasma glucose, glycosylated hemoglobin, lipids, apolipoproteins A, B and fibrinogen were evaluated using standard biochemical methods; hs-CRP was estimated by imunoturbidimetry. Metabolic syndrome (MS) was diagnosed by the NCEP III criteria. Standard statistical methods were used for data analysis.
Results: 217 (52%) males and 198 (48%) females with DM2 were 66±9 y. old. About 80% of diabetics with MS had higher level of hs-CRP (3,8 ±3,22 mg/l) than diabetics without MS (2,5±2,66 mg/l) (p>0,001). No association was found between standard risk factors (BP, smoking, cholesterol) and hs-CRP. Plasma triglycerides, apolipoprotein B, fibrinogen and waist appeared significant independent variables for hs-CRP=33 mg/l (dependent variable).
Conclusion: In those DM2 patients with concomitant metabolic syndrome, hypertriglyceridemic waist appeared as a major factor for increased CV risk.
219 The ageing process of the heart: relation between changes in body weight and left ventricular geometry and function - The MONICA/KORA-Study
J Stritzke1; MRP Markus1; W Lieb1; A Luchner2; A Doering3; U Keil4; HW Hense3; H Schunkert2
1University of Luebeck Medical Clinic II, Luebeck, Germany
2University of Regensburg Clinic for Internal Medicine II, Regensburg, Germany
3GSF ResearchCenter for Environment and Health Institute of Epidemiology, Neuherberg, Germany
4University of Muenster Institute of Epidemiology and Social Medicine, Muenster, Germany
Background: The gain in weight observed in many individuals during ageing may promote left ventricular (LV) hypertrophy and diastolic dysfunction. However, it remains unclear whether attention to weight maintenance may have beneficial effects on LV remodeling. We evaluated the relation between weight changes and left ventricular volume and pressure load as well as consecutive alterations of LV geometry and function during ten years of follow-up.
Methods: A total of 1005 individuals (aged 25 to 74 years) who originated from a gender and age stratified random sample of German residents of the Augsburg area were examined by standardized echocardiography at baseline and again after ten years. The associations between weight changes and long-term changes of systolic blood pressure (BP), stroke volume (SV), LV end-diastolic diameter (LVEDD), wall thickness (WT), LV mass (LVM), and left atrial (LA) diameter were assessed. Mean relative changes and odds ratios were calculated by statistical models adjusting for gender, age, body height, systolic blood pressure and body weight at baseline.
Results: After ten years of follow-up 305 individuals presented with a loss of body weight (mean loss 3.5+/-3.4 kg on average), whereas 700 subjects presented with an increase of body weight (mean increase 5.4+/-4.7 kg). Changes in LV volume and pressure load associated with ageing by 10 years were significantly different in the two groups. Specifically, individuals with weight gain displayed higher increases in BP (+7.7% [CI-95% 6.6, 8.7] vs. +4.7% [3.2, 6.3], p=0.003) and SV (+6.1% [4.2, 7.9] vs. +1.7% [−1.0, 4.3], p=0.007). Additionally, this group also presented with higher increase in WT (+8.1% [7.0, 9.2] vs. +5.9% [4.3, 7.5], p=0.024), LVEDD (+0.8% [0.2, 1.4] vs. −0.6% [−1.5, 0.2], p=0.008), LVM (+11.9% [10.4, 13.5] vs. +6.5% [4.3, 8.8], p>0.001) and LA (+2.5% [1.7, 3.3] vs. −0.9% [−2.1, 0.2], p>0.001), as compared to individuals with weight loss.
Consequently, the risk for incident left ventricular hypertrophy (OR 2.5 [1.5–4.3], p=0.001) and incident diastolic dysfunction (OR 1.9 [1.1-3.4], p=0.023) was significantly higher in individuals presenting with an increase in body weight.
Conclusion: Prospectively, weight gain is associated with an increase in LV volume and pressure load independent of confounding factors. As a result LV remodeling was accelerated in participants with significant weight gain upon follow-up. In addition, increases of left ventricular mass attributable to ageing were also detectable in the weight loss group, but to a significant lesser extent.
220 Long-term effects of various physical activity levels in preventing obesity and metabolic syndrome in middle-aged men
W Drygas; M Kwasniewska; T Kostka; A Jegier; M Pasowicz
Medical University Lodz Department Prev. Med., Lodz, Poland
Background and aim: Regular physical activity is considered as an effective method in preventing overweight and obesity and to influence positively several metabolic risk factors. There are only few studies analyzing longitudinal effects of various training programs in middle-aged subjects. The aim of the study was to assess the influence of leisure-time physical activity level (LTPA) on the prevalence of obesity and metabolic syndrome (MS) in long-term observation.
Methods: Between 1977 and 2004 a group of 305 men aged 30–59 years participated in regular health status examinations (detailed interview, physical examination, blood pressure, glucose and lipids profile, anthropometric measurements, exercise tests). According to self-reported LTPA all participants were divided into three groups: sedentary (S) (LTPA>1000 kcal/wk), moderate (M) LTPA (LTPA between 1000–2000 kcal/week) and highly (H) active group (LTPA>2000 kcal/week). In the subgroup of men with the highest aerobic capacity indices calcium scoring was performed using 64-slice computed tomography (MSCT) and Agatston's algoritm.
Results: Mean values of body weight, BMI and body fat increased in all groups compared however the mean values in H group are more favourable as compared with sedentary and moderate LTPA group. Only H group was able to maintain BMI value about 25,0 and to increase significantly HDL (51,7 vs. 56,66 mg/dl) in the follow-up. At final examination we diagnosed obesity (BMI= or> 30,0 kg/m2) in 23,3% of sedentary men, 20,0% of moderate activity and 12,% of highly active group. Frequency of obesity increased above twofold in sedentary individuals (10,8 vs 23,3). Metabolic syndrome (MS) as defined by ATP III has been diagnosed by 26,6% of sedentary, 23,1% of moderate and only 8,4% of highly active middle-aged men at final examination. In the group of men with the highest aerobic capacity at final examination (VO2max>35 ml/min/kg) prevalence of obesity increased form 2,4% to only 3,5%, and there were no cases of MS.
Conclusion: Prevalence of obesity and metabolic syndrome development depends on leisure time physical activity volume in middle-aged men. High aerobic capacity is strong protective factor in development of obesity and metabolic syndrome even more important than leisure time energy expenditure related to the training.
221 Evidence-based reduction of predicted cardiovascular risk after bariatric surgery: a systematic review
JA Batsis; A Romero-Corral; ML Collazo-Clavell; MG Sarr; RJ Thomas; V Somers; F Lopez-Jimenez
Mayo Clinic Medicine, Rochester, United States of America
Background: Obese patients have an increased prevalence of cardiovascular (CV) risk factors which improve with bariatric surgery, but whether long-term CV events or mortality are decreased remains ill-defined. The purpose of this study was to use previously published risk models applied to both a validation cohort in addition to a theoretical test group based on studies obtained from a systematic review of previously published studies related to long-term predicted CV risk after bariatric surgery.
Methods: Our validation cohort consisted of a population-based historical cohort of 197 bariatric surgery undergoing Roux-en-Y gastric bypass and 163 non-operative patients identified through the Rochester Epidemiology project, a linkage system allowing for complete ascertainment of a patient's medical record. We applied the Framingham and PROCAM risk scores to calculate 10-year CV risk. A search of Medline resulted in 4 studies related to obesity, bariatric surgery, and CV risk factors relevant to our analysis that we used to form a theoretical test group. Using mean values of major CV risk factors at baseline and their change at follow-up, we calculated 10-year CV risk to compute directionality and trends among these diverse cohorts.
Results: In our validation cohort, absolute 10-year Framingham risk was lower at follow-up in the operative group (7.0 to 3.5%; p>0.001) as compared to the non-operative group (7.1 to 6.5%; p=0.13), with an intergroup change of risk of 3.0% (p>0.001). PROCAM risk in the operative group risk decreased from 4.1 to 2.0% (p>0.001), whereas the non-operative group exhibited only a modest decrease (4.4 to 3.8%; p=0.08). Using mean data from the validation study, the trend and directionality in risk was similar in the operative group (−1.1%), but was 0.5% greater at follow-up in the non-operative group. The theoretical test group studies also confirmed directionality of CV risk with estimated relative risk reductions for bariatric surgery patients ranging from 24.0–60.5% using the Framingham algorithm compared to reductions of 8.3–61.5% using PROCAM. One study demonstrated an increase in CV risk at follow-up (7.7 to 11.8%), the direction which normalized once age-independent scores were utilized.
Conclusion: Bariatric surgery offers considerable improvement in CV risk factor control in obese patients and in risk prediction scores for the incidence of CV events using standard risk models. Risk improvement may be underestimated because models do not include body weight in their algorithm, and therefore ignore potential benefit beyond improvement in CV risk factors.
222 The I CARE study targeting a major killer of diabetic patients
U Milman1; C Shapira2; S Blum3; AP Levy3
Clalit Health Services, Haifa district Research Unit, Haifa, Israel
2Clalit Health Services, Haifa, Israel
3Technion-Israel Institute of Technology Vascular Laboratory, Haifa, Israel
Purpose: The Haptoglobin (Hp) gene is polymorphic in man with two classes of alleles denoted 1 and 2. The Hp 2 allelic protein product provides inferior anti-oxidant protection compared to the Hp 1 allelic product. Several cross sectional and retrospective studies have suggested that the Hp 2–2 genotype may be a major determinant of susceptibility to cardiovascular events in diabetic individuals and also, that anti-oxidants may reduce cardiovascular events in diabetics. We sought to examine this relationship in a prospective, randomized, double blind, placebo controlled clinical trial.
Methods: 3054 diabetic individuals, 55 years of age or older, were screened for Haptoglobin genotype and composite the I CARE Registry (NCT00448487). 1434 diabetic individuals from the registry, with the Hp 2–2 genotype, were randomized to either vitamin E or placebo for the I CARE Study (NCT00220831). We divided the entire cohort into 4 groups: Hp 1–1, Hp 2–1 and Hp 2–2 randomized to vitamin E or placebo. The primary outcome of the study was the composite of cardiovascular death, non-fatal myocardial infarction and stroke. Events were ascertained by reviewing all hospitalizations of study participants. Adjudication of events corresponding to study outcomes was based on the hospitalization discharge summaries. All registry patients completed two years follow up. All treatment decisions regarding routine care remained at the discretion of the individual's primary care physician.
Results: The prevalence of cardiovascular disease in this study cohort at baseline was 25%. Patients were well balanced for all baseline characteristics. Event rate was 2.1%, 2.0% and 4.7% in individuals with Hp 1–1, 2–1 and 2–2 randomized to placebo respectively (HR 2.4, p=0.001). Event rate in Hp 2–2 individuals randomized to vitamin E was 2.2%, remarkably similar to that of Hp 1–1 and Hp 2–1 individuals.
Conclusion: This study suggests that Hp genotyping may be useful to identify a large subgroup of high risk diabetic individuals who could derive cardiovascular benefit from a very inexpensive treatment. Such an approach to determine who should receive vitamin E appears warranted based on several meta-analyses showing that vitamin E may be harmful when given indiscriminately to all individuals.
223 Estimating the cardiovascular mortality burden attributable to the European Common Agricultural Policy on dietary saturated fats
F Lloyd-Williams1; M O'Flaherty1; M Mwatsama2; C Birt1; R Ireland1; K Lock1; S Capewell1
1University of Liverpool Division of Public Health, Liverpool, United Kingdom
2Heart of Mersey, Liverpool, United Kingdom
Purpose: To estimate the burden of cardiovascular disease within 15 European Union countries (prior to the 2004 enlargement), as a result of excess dietary saturated fats attributable to the Common Agricultural Policy.
Methods: A spreadsheet model was developed to synthesise data on population, diet, cholesterol levels and mortality rates. A conservative estimate of a reduction in saturated fat consumption of just 2.2 g was chosen, representing 1% of daily energy intake. The fall in serum cholesterol concentration was then calculated, assuming this 1% reduction in saturated fat consumption was replaced with 0.5% monounsaturated and 0.5% polyunsaturated fats. The resulting reduction in cardiovascular and stroke deaths were then estimated by multiplying the predicted change in the CHD death rate for the estimated cholesterol fall, by the actual number of CHD deaths in Europe and in the individual countries. A probabilistic sensitivity analysis was conducted.
Results: Reducing saturated fat consumption by 1% and increasing mono-unsaturated and poly-unsaturated fat by 0.5% each would lower blood cholesterol levels by approximately 0.0666 mmol/l, resulting in 6868 fewer coronary heart disease deaths (minimum estimate 878, maximum estimate 7796) and 2138 fewer stroke deaths (minimum estimate 1045, maximum estimate 3244) (Table 1) each year. Of this total, 3158 (minimum estimate 408, maximum estimate 3601) were CHD premature deaths (under 75 years) and 836 (minimum estimate 814, maximum estimate 1267) were stroke premature deaths. The excess deaths burden was greatest in France, Italy, Spain and the UK.
Conclusion: The cardiovascular disease burden attributable to the Common Agricultural Policy appears substantial. Furthermore, these calculations were conservative estimates, and the true mortality burden may be higher.
224 Long-term fish consumption is associated with better 30-day prognosis of patients who had had an Acute Coronary Syndrome
G Pounis1; DB Panagiotakos1; C Chrysohoou2; P Aggelopoulos1; G Metallinos1; L Papadimitriou1; C Pitsavos1; C Stefanadis3
1Harokopio University, Athens, Greece
2Athens, Greece
3Cardiology Dept, Athens Medical School, Athens, Greece
Background: The role of fish consumption in secondary prevention of cardiovascular disease (CVD) is not yet fully understood. In this work we sought to investigate the relationship between long-term consumption of fish in short-term prognosis of patients who had an Acute Coronary Syndrome (ACS).
Methods: 293 consecutive patients (65±12 years), with discharge diagnosis of ACS were enrolled, during 2006–2007. All participants were asked about their frequency of intake of fish that are frequently consumed in Greece. The assessment of n-3 and n-6 fatty acids intake was performed using local and national food composition tables. 30-day after discharge, all patients were re-examined and main outcome of interest was death or re-hospitalization due to CVD.
Results: The 30-day CVD event rate was 23.1%, while the case fatality rate was 2.0%. Multivariate logistic regression analysis, controlling for several confounders revealed that fish intake above 7 portions/week is associated with 83% decrease of the risk for a recurrent event (OR=0.17, 95% CI 0.04–0.80). Moreover, high n-3 and n-6 fatty acids intake above 8.8 g/week and 13.2 g/week, respectively, is associated with 83% and 79% reduction on the likelihood of recurrent events (OR=0.17, 95% CI 0.04–0.81, p=0.03 and OR=0.21, 95% CI 0.05–0.97, p=0.05). Calcium intake from fish, above 77555 mg/week is also associated with 79% reduction in 30-day coronary risk (OR=0.21, 95% CI 0.05–0.93, p=0.04).
Conclusions: Dietary habits that include adequate quantities of fish consumption seem to prevent cardiac patients from another CVD event, short after their first episode.
225 Food patterns analysis and the Metabolic Syndrome: the ATTICA study
DB Panagiotakos1; C Pitsavos2; C Chrysohoou1; Y Skoumas1; C Stefanadis1
1Harokopio University, Athens, Greece
2Athens Medical School, Athens, Greece
Background: Dietary habits have been associated with the prevalence of the metabolic syndrome (MS). We evaluated the associations between foods or food patterns and the characteristics of the MS were evaluated.
Methods: During 2001–2002, 1514 men (18–87 years old) and 1528 women (18–89 years old) without any clinical evidence of cardiovascular disease were randomly enrolled, from the Attica region in Greece. Dietary habits were evaluated using a semi-quantitative, food-frequency questionnaire. Characteristics of the MS (i.e. blood pressure, waist circumference, glucose, triglycerides and High Density Lipoprotein cholesterol) were also measured. Principal Components Analysis was applied to extract dietary patterns from 22 foods or food groups. Multivariate regression analysis evaluated the associations between the extracted dietary patterns and characteristics of the MS.
Results: Six components were derived explaining 56% of the total variation in intake. Component 1 was characterized by the consumption of cereals, fish, legumes, vegetables and fruits (explained variation 19.7%); component 2, characterized by the intake of potatoes and meat (explained variation 11.7%), component 6, characterized by alcohol intake (explained variation 4.8%), while the other components were mainly characterized by the consumption of dairies and sweets. After adjusting for various confounders, component 1 was inversely associated with waist circumference, systolic blood pressure, triglycerides, positively associated with HDL-cholesterol levels, and inversely with the likelihood of the MS (odds ratio=0.87, p=0.013), while components 2 and 6 were positively correlated with the previous indices, and the likelihood of having the MS (odds ratio=1.13, p=0.004 and odds ratio=1.26, p=0.001).
Conclusion: A dietary pattern that includes cereals, fish, legumes, vegetables and fruits was independently associated with reduced levels of clinical and biological markers linked to the MS, while meat and alcohol intake showed the opposite results.
226 Alcohol, beer, wine, spirits, drinking patterns and obesity
M Bobak1; R Kubinova2; S Malyutina3; A Pajak4; M Marmot4
1University College London Department of Epidemiology and Public Health, London, United Kingdom
2National Institute of Public Health, Prague, Czech Republic
3Institute of Internal Medicine, Novosibirsk, Russian Federation
4Jagiellonian University, Krakow, Poland
Background: Uncertainties remain about the effects of different alcoholic beverages and drinking patterns on obesity. Anecdotally, beer has long been seen as more obesogenic than wine or spirits but empirical data on this important public health question are sparse and contradictory. Similarly, little is known about whether episodic drinking has similar effects as regular intake. The objective of this work was to investigate the association between body mass index (BMI) and waist-hip ratio (WHR) in large cohorts in populations with different drinking patterns and beverage preferences.
Methods: The HAPIEE Study is being conducted in Novosibirsk (Russia), Krakow (Poland) and six cities of the Czech Republic. Random population samples of men and women aged 45–69 years were invited to participate (overall response rate 61%). Anthropometric indices were measured in a clinic. Intake of beer, wine spirits and total alcohol in the last week was assessed by a questionnaire. Data collection was standardised across study centres. Analyses were done separately in men (n=13,519) and women (n=15,075), first in the full sample and then in subjects who drank exclusively beer, wine and spirits; we controlled for age, country, education, physical activity, cholesterol and smoking.
Results: In men, BMI was not associated with intake of beer, wine, spirits or total alcohol. By contrast, WHR was positively associated with weekly intake of beer, spirits and total ethanol but not wine. In women, intake of each beverage and total alcohol intake was inversely associated with BMI and, of marginal significance, positively with WHR. The magnitude of statistically significant effects was modest, not exceeding 0.004 units of WHR (positive effect) and 0.5 units of BMI (negative effect) per 100 g of ethanol per week. Beverage-specific results were similar in the full data and in subjects who were exclusive drinkers of specific beverages. There was a statistically significant effect of binge drinking pattern, which was independent from the weekly intake; men and women who drank>80 g of alcohol per single drinking occasion at least once a month had WHR 0.008 (p>0.001) and 0.012 (p=0.013) units, respectively, higher than those who did not report episodic drinking.
Conclusion: WHR, but not BMI, was positively associated with intake of beer, spirits and total alcohol but the effects were too small to be of practical significance. The positive association of binge drinking with WHR, which was independent from weekly drinking volume, may be of relevance to the discussion about the link between heavy drinking and the metabolic syndrome.
227 Adherence to a Mediterranean Diet and the risk of incident hypertension
F Valencia Serrano1; JM Nunez-Cordoba2; M Bes-Rastrollo2; A Alonso3; MA Martinez-Gonzalez3
1Hospital Virgen de la Victoria Cardiology, Malaga, Spain
2University of Navarra Preventive Medicine and Public Health, Pamplona, Spain
3University of Minnesota Epidemilogy and Community Health, School of P, Minneapolis, United States of America
Objective: To determine whether the adherence to a Mediterranean Diet (MeDiet) pattern is associated with a reduction in the risk of incident hypertension (HT) in a large prospective dynamic Mediterranean cohort (the SUN study).
Methods: Incidence of HT was ascertained in 11.243 subjects without previous history of HT, diabetes, cancer or known cardiovascular disease enrolled in the SUN Study. Dietary information at baseline and incidence of HT biennial were assessed with previously validated questionnaires. Adherence to a MeDiet pattern was evaluated according to a 10 point scale that resumes the main components of this diet, as reported by others. The total Mediterranean-diet scale ranged from 0 (minimal adherence to the traditional MeDiet) to 9 (maximal adherence). Participants were grouped into 4 categories of adherence: low (score:0–2), low-moderate (score:3–4), moderate-high (score:5–6) and high (score:7–9). Cox proportional hazard models assessed the risk of incident HT among categories of adherence to MeDiet, simultaneously controlling for several other known risk factors for HT.
Results: In a follow up of 60,203 persons-years, 505 new cases of HT were ascertained. After multivariate adjustment women with a moderate-high adherence to a MeDiet pattern showed a reduced risk of incident HT compared with those with the lowest adherence (HR=0.59, CI (95%) 0.38–0.93). No category of adherence was associated with a reduction in the risk of hypertension in men, see Table 1.
Conclusion: These results suggest that a moderate-high adherence to a Mediterranean diet pattern is associated with a lower risk of incident HT in women but not in men.
SCORE
0-2
3-4
5-6
7-9
Women
Incident cases
39
75
65
26
Person-years
6674
15342
12960
3722
Multivariate HR
1 (ref.)
0.69 (0.46-1.03)
0.59 (0.38-0.93)
0.69 (0.39-1.23)
(95% CI)
Men
Incident cases
36
102
114
48
Person-years
3798
7831
7320
2555
Multivariate HR
1 (ref.)
1.15 (0.79-1.71)
1.26 (0.83-1.92)
1.31 (0.78-2.17)
(95% CI)
Hazard ratios (95% CI) of hypertension according to categories of adherence to the traditional Mediterranean diet and gender.
228 Fish consumption is associated with lower likelihood of heart failure in post acute coronary syndrome patients: a case-control study
C Kastorini1; DB Panagiotakos2; C Chrysohoou1; G Metallinos1; S Athanasopoulou1; Y Barbetseas1; C Pitsavos1; C Stefanadis3
1Athens, Greece
2Harokopio University, Athens, Greece
3Cardiology Department Athens Medical School, Athens, Greece
Background: Heart failure is recognised as a major and escalating public health problem in industrialized countries with ageing populations. Dietary habits have long been associated with the development of acute coronary syndromes (ACS); however, fish intake seems to play a controversial role in this relationship. The aim of the present work was to evaluate the association between fish consumption with the development of heart failure in patients who had had an ACS.
Methods: During 2006–2007, 144 male (65±14 years) and 50 female (71±12 years) post ACS patients who developed heart failure soon after the cardiac event and 129 males (64±12 years) and 51 females (67±10 years) without heart failure, were included in the study. Participants were age and sex matched and consequently selected. Detailed information regarding their medical records, anthropometric data, physical activity and smoking habits were recorded. Nutritional habits were evaluated using a semi-quantitative food-frequency questionnaire. Multiple logistic regression analysis estimated the odds ratio (OR) of developing heart failure by the frequency of fish consumption, after taking into account the effect of several confounders.
Results: Moderate consumption of fish (1–2 times/week) was reported by 57.7% of patients who did not develop heart failure and by 47.4% of patients who developed heart failure after the cardiac event. Multi-adjusted analysis revealed that fish consumption 1–2 times/week was associated with 74% (95% CI 0.07–0.92) lower likelihood of developing heart failure, compared to no/rare consumption, after adjusting for age, sex, obesity, smoking, exercise, education status, clinical presentation and history of ACS, hypertension, hypercholesterolemia and diabetes.
Conclusion: Fish consumption according to the nutritional guidelines for the general population seems to offer significant protection against the development of heart failure in post ACS patients.
229 Vegetables consumption is associated with lower likelihood of heart failure in post acute coronary syndrome patients: a case-control study
C Kastorini1; DB Panagiotakos2; C Chrysohoou1; G Metallinos1; S Paspaliari1; S Brilli1; C Pitsavos3; C Stefanadis2
1Athens, Greece
2Harokopio University, Athens, Greece
3Cardiology Department Athens Medical School, Athens, Greece
Background: Fruits and vegetables have long been associated with the prevention of acute coronary syndromes (ACS). However, their influence on cardiovascular system in patients with heart failure has rarely been investigated. The aim of this work was to evaluate the association between fruits and vegetables consumption with the development of heart failure in patients who had had an ACS.
Methods: During 2006–2007, 144 male (65±14 years) and 50 female (71±12 years) post ACS patients who developed heart failure soon after the cardiac event and 129 males (64±12 years) and 51 females (67±10 years) without heart failure, were included in the study. Participants were age and sex matched and consequently selected. Detailed information regarding their medical records, anthropometric data, physical activity and smoking habits were recorded. Nutritional habits were evaluated using a semi-quantitative food-frequency questionnaire. Multiple logistic regression analysis estimated the odds ratio (OR) of developing heart failure by the frequency of fruits and vegetables consumption, after controlling for the effect of several potential confounders.
Results: Multi-adjusted analysis revealed a consistent inverse relationship with vegetables consumption and the likelihood of developing heart failure, compared to no/rare consumption. In particular, after adjusting for age, sex, obesity, smoking, exercise, education status, clinical presentation and history of ACS, hypertension, hypercholesterolemia and diabetes, we observed that 1–2 times/week was associated with 73% lower likelihood of heart failure (95% CI 0.08–0.97), 3–5 times/week was associated with 77% lower likelihood of heart failure (95% CI 0.06–0.83), and 5+ times/week was associated with 78% lower likelihood of heart failure (95% CI 0.05–1.05). No significant association was found between fruits intake and development of heart failure after an ACS episode.
Conclusion: Vegetables intake seems to offer significant protection against the development of heart failure in post ACS patients.
230 Nutritional quality of the meals at workplace canteens in Finland
S Raulio1; M-L Ovaskainen1; E Roos2; R Prattala2
1National Public Health Institute (KTL), Helsinki, Finland
2Folkhalsan Research Center, Helsinki, Finland
Purpose: There is a long tradition of having a lunch at workplace canteen in Finland; on average half of all Finnish employees eat at the canteen regularly. Well planned mass catering at workplace could since have major effects on public health, well-being, and nutrition education of employees. Little is known, however, about the nutritional quality of meals eaten at the canteens, or the nutritional contribution of those lunches to employees' diet as a whole.
The aim of this study was to examine the nutritional quality of the meals of Finnish employees at workplace canteens.
Methods: Dietary data were collected for 2007 adults by using a computer-assisted 48-h dietary recall in the national FINDIET 2002 survey. Employed Finns aged 25–64 years were included in this study (279 men and 330 women).
Results: Lunches of those male employees, who ate at workplace canteen, contained more (g/MJ) wheat bread (p>0.003), fresh vegetables (p>0.001), vegetable foods (p>0.014), and boiled potatoes (p>0.021), than did lunches of those, who did not eat at canteen. Women, instead, ate more fresh vegetable (p>0.001), poultry (p>0.045), and salad dressings (p>0.009) when eating at canteen. The choices that were made during the lunch had only a weak association with the composition of the employees' diet as a whole. Among men, fresh vegetables (p>0.001), as well as salad dressings (p>0.001), and among women salad dressings (p>0.001), were used more commonly on the daily basis by those, who ate at canteen. Even though differences in food selection between eating places were quite clear, differences in nutrition intake were modest. Male employees, who preferred to eat at canteen, got more carotenoids (p>0.029), carbohydrates (p>0.049), and energy (p>0.015), but less protein (p>0.041) from their lunches than did those, who did not eat at canteen at all. Women got more fat (E%) (p>0.001), but less carbohydrates (E%) (p=0.021), and sugar (E%) (p>0.001) from the lunches that were eaten at canteen compared to those eaten elsewhere.
Conclusion: Even though the nutritional differences of the meals between eating places were modest, eating regularly at workplace canteen improved the composition of the lunches of Finnish employees by increasing their vegetable intake substantially.
231 LDL-c, HDL-c and glucose optimization using phytonutrient combination therapy in diabetes
PJE Verdegem; B Horne; I Martinez
Unicity International Research And Development, Orem, United States of America; Blue Mesa Medical Center, Katy, United States of America
Introduction: Phytonutrient therapy options to management of lipid and glucose parameters in diabetes is gaining popularity among patients. Monotherapy with dietary ingredients has shown positive effects, but with limited clinical relevance. Our research focuses on using a phyto-nutrient combination in optimizing lipid and glucose parameters. All four ingredient groups have individual data supporting their use for optimizing lipoprotein fractions in hypercholesterolemia. This pilot study evaluates their combined efficacy in type-II diabetes.
Methods: A group of 34 subjects with established type-II diabetes and hypercholesterolemia added the product to their diet. The drink was taken thrice daily 15–20 minutes before meals. The fiber drink consists of viscous soluble fiber, minerals, vitamins, policosanol, phytosterols, an aqueous Chrysanthemum morifolium extract and vitamins and minerals at or close to the RDA level. The ingredients combine 4 mechanisms to lipid lowering, including bile acid sequestration, dietary absorption inhibition, and HMG-CoA reductase inhibition. Lipid and glucose parameters were measured at baseline, 4 and 8 weeks.
Conclusion: BiosLife, a phytonutrient combination drink, shows potential in optimizing parameters associated with cardio vascular disease risk in type-II diabetes. These findings are in line with previously reported clinical results. The fiber component has reduced the postprandial glucose levels and the resulting lower HbA1c levels indicate natural option to improve diabetes management.
Results
Parameter
Inclusion at BL
BL (mg/dl)
t=8 wks (mg/dl)
change (%)
p-value
LDL-c
All
127
104
−18.3
>0.05
LDL-c
>160
197
141
−28.9
>0.005
HDL-c
All
46
48
+3.5
n.s.
HDL-c
>40
35
40
+14.4
n.s.
TG
All
182
143
−21.3
n.s.
TG
>150
242
163
−32.5
>0.05
Glu
All
162
134
−17.3
>0.05
Glu
>175
218
155
−28.9
>0.05
HbA1c
All
7.2
6.6
−9.4
>0.05
HbA1c
>8
9.2
7.8
−15.8
>0.05
HbA1c measurements after 12 weeks.
232 Quantitative effects on coronary heart disease risk of replacing trans fats by other fats
R Clarke1; D Mozaffarian2
1Clinical Trial Service Unit Nuffield Department of Clinical Medicine, Oxford, United Kingdom
2Harvard Medical School Division of Cardiovascular Medicine, Boston, United States of America
Purpose: Reduced consumption of trans fatty acids (TFA) is desirable to lower coronary heart disease (CHD) risk. In practice, partially hydrogenated vegetable oils (PHVO), that contain both TFA and other fatty acids, must be replaced with alternative fats/oils. We performed quantitative estimates of CHD effects of replacing PHVO with alternative fats/oils based on (a) randomized dietary trials and (b) prospective observational studies.
Methods: We performed meta-analyses of (a) effects of TFA on blood lipids and lipoproteins in controlled dietary trials and (b) associations of habitual TFA consumption with CHD outcomes in prospective cohort studies. Based on these results and corresponding findings for SFA, MUFA, and PUFA, we calculated effects on CHD risk for replacing 7.5% of energy from different PHVO formulations (containing 20%, 35%, or 45% TFA) with butter, lard, palm, or vegetable oils.
Results: In controlled trials, each 1% energy replacement of TFA with SFA, MUFA, or PUFA, respectively, decreased total/HDL-C by 0.31, 0.54, and 0.67; ApoB/ApoA-I by 0.007, 0.010, and 0.011; and Lp(a) by 3.76, 1.39, and 1.111 mg/L (p>0.05 for each). We also included possible effects on CRP of TFA vs. other fats from one trial. Based on these risk factor changes in controlled trials, CHD risk would be variably decreased by different fats/oils replacing 20% TFA PHVO (range: −3.3% [butter] to −10.3% [canola]); 35% TFA PHVO (−12.1% [butter] to −16.1% [canola]); or 45% TFA PHVO (−17.7% [lard] to −19.8% [canola]). In prospective cohort studies, each 2% energy replacement of TFA with SFA, MUFA, or PUFA, respectively, would lower CHD risk by 17%, 20%, or 24%. Based on these associations in observational studies, CHD risk would be variably decreased by different fats/oils replacing 20% TFA PHVO (−1.8% [butter] to −22.2% [soybean]); 35% TFA PHVO (−15.1% [butter] to −32.8% [soybean]); or 45% TFA PHVO (−22.7% [butter] to −38.8% [soybean]). Comparing the calculated risks from trial vs. cohort evidence, the effects on total/HDL-C, ApoB/ApoA-I, Lp(a), and CRP in the trials explained most (65–80%) of the cohort-calculated risk reduction for animal fats, but only ∼50% of the cohort-calculated risk reduction for vegetable oils.
Conclusion: Effects on CHD risk of removing PHVO in foods will vary depending on the PHVO formulation and replacement fat/oil. Prior discrepancies between estimates from controlled dietary trials vs. prospective cohort studies are at least partly explained by considering effects of TFA on multiple risk factors.
233 Effects of salt substitution on blood pressure using clinical and home measurements in hypertensive patients: a double-blinded randomized controlled trial
L Zhao; J Hu; X Li; Y Wu
Cardiovascular Institute And Fu Wai Hospital Dept of Epidemiology, Beijing, China, People's Republic of; Ningxia Medical College Public Health, Yinchuan, China, People's Republic of; Cardiovascular Institute and Fuwai Hospital Epidemiology, Beijing, China, People's Republic of; 4Peking University, School of Public Health Epidemiology, Beijing, China, People's Republic of
Objective: To evaluate the effect of salt substitution on blood pressure (BP) using clinical and home measurements in hypertensive patients.
Methods: A total of 220 patients with SBP ≤140 mmHg or/and DBP ≤90 mmHg at two, aged 57.3±10.4 years, took part in this double-blinded randomized controlled trial. Participants were required to have no clear established contra-indication to the use of the study salt substitute, such as use of a potassium-sparing medication or significant renal impairment. The regular salt or salt substitution (65% sodium chloride, 25% potassium chloride, 10% magnesium sulphate) was randomized allocated to two groups during one-year trial. Both clinical and home BP were measured with automatic electronic devices HEM770A at baseline, month 3, 6, 12. Spot first morning urine samples were collected at baseline, month 6, 12. Blood sample was collected at baseline, month 3, 12. The evaluation of taste was recorded at baseline, month 6, 12 months using 100 mm visual analogue scales for saltiness, flavor and overall liking by consuming a standard soup.
Results: 213 of the 220 subjects was completed the trial. All participants in the salt substitution group and 98% of the controls “all” or “nearly all” used study salt. The magnitude of SBP reduction was 5.33 mm Hg (95% confidence interval [CI], 1.0 to 9.5) for office SBP and 4.22 mm Hg (95% CI, 1.3 to 7.0) for SBP at home at the end of the trial in the salt substitution group compared with the regular salt group. There were no detectable differences between groups for DBP during the trial. In addition, the reductions of SBP were found both in the subgroups with taking the same anti-hypertensive drug and with no drug use during the trial. Urinary sodium concentration and sodium-potassium ratio were significantly lower and urinary potassium concentration was significantly higher in the salt substitution group than those in the regular salt group during the intervention (all p>0.05). Serum electrolytes, urinary nitrogen were not significantly different between two groups. There were no detectable differences between 2 groups at any time point in the perception of the soup provided, in terms of saltiness, liking or overall acceptability.
Conclusion: Replacing regular salt by a low sodium, high potassium, high magnesium salt could offer a simple, practical, well accepted, and valuable non-pharmacological approach to lowering SBP in Chinese hypertensives.
234 Using a fiber and phytonutrient combination therapy to control hypercholesterolemia in an African American community
L Njord1; R Njord1; PJE Verdegem1; W Cooper2
1Unicity International Research and Development Department, Orem, United States of America
2Wellstar Kennestone Hospital Surgery, Atlanta, United States of America
Introduction: African Americans living in the American south are the highest risk ethnic group for heart disease, the leading cause of mortality in the United States. Currently, statin medications are the most common intervention used by physicians to mitigate hypercholesterolemia. There are some patients who cannot or will not take statin medications due to associated side-effects or desire to use diet-based products to improve health. This study evaluates a fiber and phytonutrient combination therapy to mitigate moderate hypercholesterolemia in an African American population in Roswell, GA.
Methods: 85 subjects were enrolled from an African American community living in Roswell, GA. Each participant added the supplement containing a total of 6.6 g of soluble dietary fiber, 1.67 g phytosterols, 122 mg mg policosoanol, 255 mgmg Chrysanthemum morifolium and a mixture of vitamins and minerals close to the RDA level to their diet, split into 2 portions taken shortly before their two largest meals. Participants' lipid levels were evaluated at four, eight and twelve week intervals. They were advised not the change their lifestyles, including diet.
Discussion and conclusion: The enriched fiber and phytonutrient dietary supplement was shown to be effective in lowering LDL-M and triglyceride levels while raising HDL levels simultaneously. The test product was shown to be most effective in groups with HDL levels >400 mg mg/dl, TG levels>1500 mg mg/dl and LDL-M levels>1600 mg mg/dl in 8 to 12 weeks, providing patients an alternative for cholesterol control.
Results
week 8
week 12
Parameter
Subgroup
BL
t=8 N
%
p
BL
t=12
N
%
p
TC
Total
189
214
55
13.2
>0.001
180
202
39
12.2
>0.01
TC
>200
238
251
23
5.5
ns
239
236
14
−1.3
ns
HDL
Total
45
48
55
6.7
ns
44
44
39
0.0
ns
HDL
>40
32
41
24
28.1
>0.001
33
42
21
27.3
>0.01
TG
Total
157
119
55
−24.2
>0.01
154
128
39-16.9
ns
TG
>150
261
159
21
−39.1
>0.001
277
149
14
−46.2
>0.01
LDL-M
Total
135
126
55
−6.7
ns
125
130
39
4.0
ns
LDL-M
>160
189
155
14
−18.0
>0.01
191
167
8
−12.6
ns
235 Effect of short-term consumption of bread obtained by a selected healthy Italian grain variety on lipid, inflammatory and haemorheological variables: an intervention study
F Sofi1; F Cesari1; AM Gori1; L Mannini1; M Lenti1; L Ghiselli1; S Benedettelli1; V Vecchio1; R Abbate1; GF Gensini2
1University of Florence Medical and Surgical Critical Care, Florence, Italy
2Don Carlo Gnocchi Foundation Onlus IRCCS, Florence, Italy
Objective: Epidemiological studies have strongly suggested that dietary habits play a crucial role in the prevention of cardiovascular disease. In particular, consumption of fruits, vegetables, and grains has been associated with reduced risk of chronic diseases, mainly due to their content of compounds with antioxidant activity. However, beneficial capacity of different grains varies substantially in relation to cultivar and location of the varieties. The aim of this study was to evaluate the influence of short-term dietary intake of bread obtained by a selected variety of grain grown in Tuscany, Italy, and found to be naturally rich in antioxidants and B-group vitamins on biomarkers related to the atherosclerotic process.
Methods: Twenty subjects (9 F; 11 M) with a median age of 39.5 years (range: 21–61) were studied. After a run-in period, the subjects followed for 10 weeks a diet containing 150 g/die of bread obtained by the test grain (Test period) and for the same period a diet containing commercially available bread of the same quantity (Placebo period). We evaluated lipid profile (total cholesterol, HDL-cholesterol, LDL-cholesterol and triglycerides) inflammatory markers [highly-sensitive C-reactive protein (hsCRP), interleukin-6 (IL-6) and interleukin-8 (IL-8)], circulating and red blood cells' folate, and haemorheological profile [whole blood viscosity (WBV), plasma viscosity, erythrocytes' filtration rate (EF)] before and after dietary intervention.
Results: A general linear model for repeated measurements after adjustment for age, and gender was conducted. The test period determined a significant improvement of total cholesterol (pre: 211.1±44.9 vs. post: 196.5±44.44 mg/dL; p=0.01), and LDL-cholesterol levels (pre: 133.7±33.1 vs. post: 120.9±36.66 mg/dL; p=0.02), whereas no significant changes during the placebo period have been observed. With regard to haemorheological parameters, the test period significantly decreased all the parameters investigated, namely WBV at high (pre: 26.1±2.2 vs. post: 24.8±3.3; p=0.01) and low shear rates (pre: 5.9±0.4 vs. post: 5.7±0.4), as well as EF (pre: 8.4±3.1% vs. post: 9.1±2.8%; p=0.009) with respect to the placebo period that showed no significant changes.
Conclusion: Dietary short-term intake of bread obtained by a grain naturally rich in antioxidants and B-group vitamins seems to impose favourable biochemical changes, with regard to lower circulating levels of markers of atherosclerosis, such as lipid parameters, and haemorheological variables.
236 To study the role of H2S in the initial stage of atherosclerosis
S Barsainya; Ahmedabad, India
Background: H2S [Hydrogensulfide] was recently suggested to be a possible endogenous gasotransmitter in physiological concentration produced from homocysteine. For the purpose of understanding its possible role in pathogenesis of atherosclerosis, we explored the effect of H2S on carotid artery injured rats.
Objective: To study the role of H2S in the initial stage of atherosclerosis in rats.
Materials and Methods: Rats fed on atherogenic diet for 1 week underwent left carotid artery injury induced by thin metallic wire. Atherogenic diet was continued and on the next day of injury, treatment of NaHS [H2S donor] was given for another 3 weeks. Total 4 weeks later, blood was collected and carotid artery was removed for various observations.
Results: Carotid artery lesion index was significantly less in H2S treated group [0.13±0.09] when compared with control group [3.94±0.89] P value >0.05.
Mean serum homocysteine levels were significantly higher in H2S treated group [7.85±0.19 mol/L] when compared with control group [5.45±0.065 mol/L] P value >0.005.
Conclusion: H2S is directly acting as a antiatherosclerotic in the presence of high homocysteine levels probably due to antiproliferative activity or it might be due to antioxidant or vasodilator activity.
237 Differential effects on IGF-1 expression in myocardium and skeletal muscle of wild type and mdx -/- mice after voluntary exercise
N Mangner; S Gielen; S Sandri; R Hoellriegel; V Adams; G Schuler
University Leipzig - Heart Center Department of Cardiology, Leipzig, Germany
Purpose: Both clinical and experimental data show conflicting results with regard to exercise recommendations in hereditary muscle dystrophy: On the one hand overloading of diseased muscle fibres may accelerate disease progression, on the other hand myocardial affection by dystrophy may limit the cardiac training response. Aim of this study was to examine cardiac and skeletal muscle adaptations to voluntary wheel running in mdx -/- mice (MDX), an animal model of Duchenne muscular dystrophy vs. C57/Bl6 wild type (WT) with regard to local IGF-1 expression.
Methods: Six months old WT and MDX were assigned to 4 weeks of voluntary wheel running (VR) or to nonexercised control group (C). Running distance was recorded daily. After 4 weeks body and heart weight were measured and myocardium, M. extensor digitorum longus (EDL) and M. soleus (SOL) were collected. IGF-1 was quantified as ratio of IGF-1 to 18S-RNA by quantitative rt-PCR.
Results: WT ran a longer distance than MDX (5.71±0.36 vs. 4.27±0.18 km/d, p>0.01). Relative heart weight increased both in WT by 16.1% and in MDX by 10.2% after VR, but was significantly higher in the WT training group (p>0.01 vs. C and WT vs. MDX).
Sedentary MDX and WT showed comparable expression levels of IGF-1 in myocardium. VR resulted in an increase of myocardial IGF-1 expression from 0.25±0.04 to 0.69±0.19 in WT (p>0.05) whereas it remained unaffected in MDX.
Sedentary MDX showed higher expression levels of IGF-1 in EDL and SOL than WT (0.79±0.19 vs. 0.23±0.04 and 1.66±0.49 vs. 0.53±0.08, p>0.01). VR resulted in an increase of IGF-1 expression from 0.23±0.04 to 0.53±0.12 in EDL of WT (p>0.05) whereas remaining unchanged in SOL. No changes of IGF-1 expression in EDL or SOL of MDX were detectable after VR.
Conclusion: Both WT and MDX developed a cardiac hypertrophy in response to voluntary wheel running which was more distinct in WT MDX exhibited a compensatory higher baseline anabolic activation (by local IGF-1 levels) in EDL and SOL as compared to WT Contrary to WT animals MDX were not capable to further increase IGF-1 expression in response to voluntary running. These data indicate a significantly limited capacity of MDX to respond to exercise training with IGF-1 mediated physiological hypertrophy.
238 Intracellular molecular effects of insulin resistance in subjects with metabolic syndrome
DA Assanelli1; EP Pasini2; VF Flati3; DR Rizzoni4; EP Porteri5; GC Corsetti6; SS Speca5; RB Bianchi1
1Chair of Sport Medicine Medical and Surgical Sciences, Brescia, Italy
1Salvatore Maugeri Foundation, IRCCS Medical Center Lumezzane, Brescia, Italy
3Department of Experimental Medicine University of LAquila, Laquila, Italy
4Chiar of Internal Medicine University of Brescia, Brescia, Italy
5Chair of Internal Medicine University of Brescia, Brescia, Italy
6Chair of Human Anatomy University of Brescia, Brescia, Italy
Aim of the study: It is widely accepted that intracytoplasmic insulin signaling is impaired in the presence of insulin resistance. However, most available data have been obtained in animal models while in humans, the only available data were obtained using invasive approaches (namely muscle biopsies). The aim of this study was to develop a new method of insulin signaling evaluation from peripheral lymphocytes in order to investigate the alterations of the proteins involved in insulin signaling in patients with metabolic syndrome.
Patients and Methods: We investigated 10 consecutive patients with metabolic syndrome (MS), as well as 10 normal controls (N). The metabolic syndrome was defined according to the US National Cholesterol Education Program Adult Treatment Panel III guidelines. Blood samples (20 ml) were taken from all participants. Total mononuclear cells were isolated from peripheral blood by density gradient centrifugation. Insulin signaling was evaluated by Western blot analysis of the proteins involved. Finally, the optical densities of blot bands were determined by using a computer-assisted densito-meter.
Results: In the lymphocytes of patients with MetS, there were significantly fewer insulin receptors as well as other proteins involved in insulin signaling, such as mTOR, p-p70S6K1 and p-4EBP1 (a regulator of protein synthesis in the lympho/monocyte). This would suggest profound alterations in the post-receptor mechanism involved in signal transduction. Native IRS-1 (Insulin-receptor substrate) tended to increase in patients with MetS probably as a compensatory mechanism, which was further confirmed by an increased trend of the Serine 636–639 phosphorylated (inactive) form of IRS-1 (p-IRS-1).
Conclusion: The evaluation of insulin signaling in human lympho/monocytes is both feasible and relatively easy. In patients with MetS an evident impairment of insulin signaling can be observed, with a significantly reduced expression of the protein cascade, from insulin receptor to mTOR, p-p70S6K1 and p-4EBP1. Our proposed method has the additional advantage of allowing the evaluation of the time-course of the alterations in insulin signaling and the possible effects of therapeutic interventions.
239 The effect of chronic neuronal nitric oxide synthase inhibition on vascular function and structure of rat thoracic aorta
S Cacanyiova; F Kristek
Institute of Normal & Pathological Physiology Vascular Disorders Etiopathogenesis, Bratislava, Slovak Republic
Purpose: Studies in hypertensive humans showed an abnormal nitric oxide (NO) activity associated with hypertension and a lot of experimental studies revealed important role of constitutively expressed NO-synthase (NOS) isomers: endothelial (eNOS) and neuronal (nNOS) in cardiovascular control. However, to recognise the contribution of NO generated by nNOS to cardiovascular regulatory mechanisms still remains the subject of research. In this study the function of nNOS was studied by comparing the effects of chronic treatment by the selective nNOS inhibitor 7-nitroindazole (7-NI) with that by the general NOS inhibitor NG-nitro-L-arginine methylester (L-NAME) on systolic blood pressure (BP) and on reactivity and morphological changes of rat thoracic aorta (TA).
Methods: Male 10 weeks old Wistar rats were divided into groups: controls (n=10), L-NAME (rats received L-NAME 50 mg/kg b.w./day in drinking water/6 weeks) and 7-NI (rats received 7-NI 10 mg/kg b.w./day in drinking water/6 weeks). BP was measured using plethysmographic method. For functional study the relaxant responses to acetylcholine (ACh) and contractile responses to noradrenaline (NA) on isolated TA were recorded. For morphological study the geometry of TA was measured using light microscopy.
Results: After 6-weeks lasting treatment BP was increased in L-NAME group but it was not affected in 7-NI group. Relaxation of TA induced by ACh (10–9–10–5 M) was inhibited in L-NAME group compared to controls. The treatment with 7-NI also decreased ACh-induced relaxation but this depression was significantly smaller than in L-NAME group. The contraction of TA to exogenous NA (10–9–10–5 M) was augmented in L-NAME group compared to controls. The treatment with 7-NI shifted the dose-response curve to NA to the right so indicating the inhibition of contraction. Morphometry showed the opposite effects of treatment with two inhibitors. Wall thickness and wall cross-sectional area of TA were increased in L-NAME group whereas in rats chronically treated with 7-NI it was revealed the decrease in both parameters.
Conclusion: General inhibition of NO led to the increase of BP which correlated with impaired endothelial function, arterial wall hypertrophy and increased vascular contraction. However, chronic treatment with 7-NI did not modify BP and revealed hypotrophic effect on arterial wall associated with decreased smooth muscle sensitivity to contractile stimuli. These results suggest that biological activity of NO derived from two constitutive forms of NOS (nNOS, eNOS) could participate in regulation of cardiovascular tone by distinct mechanisms.
240 The mechanisms involved in the positive inotropic and vasodilator action of amylin on isolated rat hearts
Z Kaygisiz1; H Ciftci2; N Erkasap3; T Koken4; T Gunduz1; M Ikizler3; T Kural3
1Eskishir Osmangazi University, Medical Faculty Physiology Dept., Eskisehir, Turkey
2Eskiehir Osmangazi Universty, Medical Faculty Department of Anatomy, Eskiehir, Turkey
3Eskiehir Osmangazi Universty, Medical Faculty Department of Physiology, Eskisehir, Turkey
4Kocatepe Universty, Medical Faculty Department of Biochemistry, Afyon, Turkey
Amylin is a 37 amino acid peptide secreted from beta cells in the pancreatic islets of Langerhans. Plasma concentration of amylin is increased in type II diabetes mellitus and hypertension. The involvement of extracellular Ca2+ influx into cardiomyocytes, protein kinase C (PKC), protein kinase A (PKA) and Ca2+ release from the sarcoplasmic reticulum (SR) in the positive inotropic effect of amylin has not been investigated. The role of nitric oxide (NO) in the vasodilator effect of the peptide has not been studied. We have hence investigated the underlying mechanisms of amylin-induced positive inotropy and vasodilation. Isolated rat hearts were perfused under constant flow condition by nonrecirculating Langendorff technique. Coronary perfusion pressure, heart rate and left ventricular developed pressure as an index of contractility and +dP/dtmax were measured. Rat amylin at concentration 100 nM significantly decreased coronary perfusion pressure, increased heart rate, left ventricular developed pressure and +dP/dtmax (p>0.001). The peptide also significantly enhanced tissue nitrite level. (p>0.01). The amylin-induced positive inotropic effect was not changed by H-89 (50 M), a PKA inhibitor. Diltiazem (1 M), a L-type Ca2+ channel blocker and ryanodine (10 nM), a SR Ca2+ release channel opener suppressed completely whereas staurosporine (100 nM), a potent PKC inhibitor suppressed partially amylin-induced positive inotropic effect. Our results suggest that rat amylin may produce vasodilator, positive chronotropic and positive inotropic effects. NO may be a mediator in vasodilation. Ca2+ entry via L-type Ca2+ channels, Ca2+ release from SR through ryanodine-sensitive Ca2+ channels and activation of PKC may be involved in the positive inotropy.
241 Effects of hyperbaric oxygen treatment on experimentally induced hypercholesterolemia
PB Brkic; TJ Jovanovic; AM Mitrovic
School of Medicine Institute of Physiology, Belgrade, Serbia
Purpose: General problem of circulatory system is the impaired function of the blood vessel system. The anatomic and the subsequent functional malformations or conversely, first the functional alterations that lead to pathoanatomic changes of blood vessels at different levels of circulatory system result both in disorder of the segment responsible for local oxygen and nutrient supply and the one accountable for discharge of carbon dioxide excess and end products of metabolism as well as the whole circulatory system. In this study we have tried to establish the effect of hyperbaric oxygen (HBO) treatment, on the extent of diet-induced accumulation of lipid oxidation products in rabbit plasma and tissues, and the extent of progression and regression of atherosclerotic lesions in the rabbit aorta.
Methods: Animals were divided in three groups. First group was control group (n=7). Animals in this group were fed with regular rabbit diet. Animals in two experimental groups A (n=7) and B (n=7) have been submitted to cholesterol-rich diet, for 10 weeks. After 10 week period, animals in both experimental groups were switched to regular diet. During the period of next two weeks animals from the experimental group A have received HBO treatment (14 HBO treatments 2,5 ATA 70 min).
Results: As expected, cholesterol-rich diet induced sever hypercholesterolemia. HBO treatment had little or no effect on plasma cholesterol concentrations. We have also found, in the plasma of the experimental animal the substation reduce high density lipoprotein fraction. But significant reduction in the accumulation of cholesterol in the aortic segments was noticed on the preparations taken from the animals from the group A compared to the similar preparations from the group B. In spite the fact that HBO treatment did not have effect on the rate of plasma cholesterol decline, it significantly accelerated aortic lesion regression, as it has been shown on the histology tissue preparation. On the histology tissue preparation from the experimental group A, reduction in the remodeling process of the myocardium were also shown.
Conclusion: On the basis of these result we can assume that repeated (even relatively short), exposure to HBO induces an antioxidant defense mechanism (or mechanisms), that is (are) responsible for retarding the development of atherosclerotic lesions.
242 Hypotrophic effect of neuronal NO-synthase inhibition on the heart and vessel wall
F Kristek; S Cacanyiova; M Gerova
Institute Normal and Pathological Physiology Laboratory vascular disorders etiopatogenesis, Bratislava, Slovak Republic
Purpose: It is generally accepted that chronic NO deficiency, due to eNOS inhibition, resulted in sustained increase of blood pressure (BP) and cardiac and arterial wall hypertrophy. It has been demonstrated that 7-nitroindazole (7NI) a selective inhibitor of nNOS did not provide, contrary to eNOS inhibition, unequivocal effect on the efficiency of the cardiovascular system. Moreover, the studies devoted to the structural alterations of the heart and vascular system after chronic nNOS inhibition are completely missing.
Methods: We follow the effect of chronic nNOS inhibition on the cardiovascular system of Wistar rats. Two groups of ten weeks old Wistar rats were used: control animals (n=10) and animals (n=10) receiving 7-NI in a dose 10 mg/kg b.w./day in drinking water for 6 weeks. BP was measured by the plethysmographic method. At the end of the experiment the animals were anaesthetized and perfused with a glutaraldehyde fixative (120 mmHg), heart and carotid artery (AC) were excised and AC was processed for electron microscopy. Geometry of the artery: wall thickness (intima+media) – WT, inner diameter – ID, cross sectional area (intima+media) – CSA, and WT/ID ratio was measured in light microscopy. Volume densities (percentage from the arterial wall) of tunica intima (TI), smooth muscle cells (SMC), and extracellular matrix in tunica media (ECM) were assessed in electron microscopy using point counting method. CSAs of TI, SMC, and ECM were calculated. Results: 7-NI administration did not increase BP (112±2.2 mmHg controls vs. 118±1.9 mmHg in 7-NI). Both heart weight and HW/BW ratio (2.89±0.11 vs. 2.48±0.10, p>0.01) were decreased. WT, CSA, and WT/ID ratio were significantly (p>0.01) decreased (33.41 ±0.91 m vs. 25.86±0.91 m, 86560±1600 m vs. 67920±2200 m, 4.25 ±0.21 vs. 3.20±0.13, respectively). ID did not change. Evaluation of VD and CSAs of individual parts of the arterial wall revealed: (i) VD of TI did not change between groups, CSA of TI was decreased (9400±340 m vs. 6510±530 m, p>0.01), (ii) both VD and CSA of SMC were decreased (53.00±0.76% vs. 42.29±1.18%, p>0.01, 45880±660 m vs. 28720±800 m, p>0.01, respectively), (iii) VD of ECM in media was increased (35.92±1.00% vs. 47.06±1.14%, p>0.01) and CSA of ECM did not changed.
Conclusion: Our data, for the first time revealed that the long-term nNOS inhibition, contrary to long-term eNOS inhibition, evoked cardiac and arterial wall hypotrophy. The hypotrophy of arterial wall was due to decrease of smooth muscle cell mass. Surprising effect of nNOS inhibition on structure of cardiovascular system needs further experiments.
243 Angiotensin receptor blockers improve insulin signalling and reduce microvascular rarefaction in the skeletal muscle of spontaneously hypertensive rats
DA Assanelli1; DR Rizzoni2; EP Pasini3; VF Flati4; LFR Rodella5; CDC De Ciuceis6; GC Corsetti4; RR Rezzani4; SS Speca7
1Chair of Sport Medicine University of Brescia Medical and Surgical Sciences, Brescia, Italy
2Chair of Inter Medicine University of Brescia Medical and Surgical Sciences, Brescia, Italy
3Salvatore Maugeri Foundation, IRCCS Medical Center of Lumezzane, Brescia, Brescia, Italy
4Department of Experimental Medicine University of l Aquila, L'aquila, Italy
5Department of Human Anatomy University of Brescia, Brescia, Italy
6Department of Internal Medicine University of Brescia, Brescia, Italy
7Department of Experimental Medicine, University of L Aquila, L Aquila, Italy
Objective: Spontaneously hypertensive rats (SHR) are an example of an animal model of genetic hypertension associated with insulin resistance. The aim of this study was to investigate insulin signalling in the heart and in the skeletal muscle of SHR, as well as to evaluate the effects of renin-angiotensin system blockade.
Design and Methods: We investigated 6 untreated SHR of 12 weeks of age and 6 age-matched normotensive Wistar-Kyoto controls (WKY). In addition, 6 SHR were treated for 8 weeks with the angiotensin receptor blocker olmesartan (OLM), and 6 SHR with the ACE inhibitor enalapril (ENA). The heart and a skeletal muscle (quadriceps femoris) were promptly dissected and frozen. Insulin signalling was evaluated by Western blot analysis of involved proteins; in addition, micro-vessel density (MVD) was evaluated by immunohystochemistry.
Results: Blood pressure values were normalized by both OLM and ENA. In the heart, only mild differences in the expression of proteins involved in the insulin signalling were observed between the groups. On the contrary, in the skeletal muscle of untreated SHR, we noted a significant reduction of insulin receptor, of insulin-receptor substrate −1 (IRS-1), and of p-mTOR. The treatment with OLM normalised insulin signalling including expression of glucose transporter 4 (GLUT4), while the treatment with ENA was ineffective for the insulin receptor, and less effective than OLM on the IRS-1, p-mTOR and GLUT4. There was a significant reduction in MVD in the skeletal muscle of SHR compared with WKY, and was completely prevented by both OLM and ENA.
Conclusion: These results suggest that changes in insulin signalling occur in untreated SHR, especially in the skeletal muscle, while they are less evident in the heart. In the skeletal muscle, insulin signalling was restored by OLM, while ENA was less effective. Effective anti-hypertensive treatment with OLM or ENA was associated with a prevention of microvascular rarefaction.
244 The origin and differentiation potential of smooth muscle cells in coarctation of the aorta-neonatal type
I Vukovic1; A Aleksic2; NN Arsenijevic1; AA Aleksic2
1Faculty of Medicine Institute of Histology and Embryology, Kragujevac, Serbia
2KBC Zemun Cardiology, Belgrade, Serbia
The vascular malformation responsible for coarctation is a prominent posterior infolding (“shelf”) which, in some cases may extend around the entire circumference of the aorta.
We investigated the smooth muscle cells phenotype in aortic intimal thickening, presence of inflamatory cells and condition of the elastic tissue.
We examined samples of coarctation segments excised at surgery from 10 patients with ages from 2 days to 1 year. Section of 5 m thickness were stained with orcein and immunocytochemical staining using a LSAB/HRP+kit (Dako). We were used those primary antibodies: a-smooth muscle actin-a-SMA, vimentin, desmin, myosin haevy chains-MHC, CD45, S-100 and PCNA.
At all samples is noticed focal intimal thickening on the posterior aortic wall, with accumulation of smooth muscle cells. Smooth muscle cells (SMC) show immunoreactivity on a-SMA and vimentin, but not on desmin or MHC. In inner media on the posterior wall is noticed a large number of PCNA- and S100- positive cells and in outer media one layer of MHC- and desmin- positive cells.
In all studied samples the immunocytochemical examination revealed the presence of dedifferentiated smooth muscle cells which expresse a-SMA and vimentin, with a lack of expression of desmin and MHC. Results also showed an increase of the cell number in intima followed by proliferated smooth muscle cells in inner media and absence of inflamatory cells. This finding suggests that proliferation of the smooth muscle cells, their synthecic activity and increase of the cell number could lead to intimal thickening on the posterior wall.
245 Calcium handling in atrial myocytes: effects of exercise training and heart failure
T Skoglund1; R Rosbjorgen1; T Stolen1; MA Hoydal1; U Wisloff2
1Trondheim, Norway
2Norwegian University of Science and Technolog Circulation And Medical Imaging, Trondheim, Norway
Background: The dependence of cardiac function on the contribution of atria becomes increasingly important with age and exercise. In place of the T-tubules, which is a central structure for normal excitation-contraction coupling in LV-myocytes, atrial cells have prominent SR elements, which have been described as ‘Z-tubules’. The lack of T-tubules in atrial myocytes means that depolarization provokes calcium signals that largely originate around the periphery of the cells. To engage the contractile machinery, the calcium signal must propagate centripetally deeper into the cells. At present nothing is known about the effect of exercise training upon calcium handling in atrial cells.
The aim of the present study was to study the calcium transients in single atrial myocytes from rats with post-infarction heart failure and study the effect of exercise training.
Methods: Single atrial cells from rats with post-infarction heart failure (controls, interval-trained and moderately trained) loaded with the Ca2 + indicator, fluo-3. The Ca2+-transients were studied using confocal line-scan.
Results and Conclusion: The method for studying atrial calcium handling is now established, and in ventricular cells, we observed a near synchronous SR Ca2+ release throughout the cell results in a horizontal band of fluorescence in a linescan image transverse to the longitudinal axis of the cell. In contrast, the rise in [Ca2+]i was asynchronous in atrial cells (figure, horizontal line indicate action potential). Quantitative data comparing the adaptation to aerobic interval training, moderate continuous exercise in rats with post-infarction heart failure will be available before May 2008.
Atrial (left) and LV Ca2+ transient
246 Effects of ischemic postconditioning on inward rectifier potassium current and action potential of rats ventricular myocytes
L Yang; Z-Y Fan; X-C Yang; X-L Liu; L Liu
Chaoyang Hospital, Capital Medical University Heart Center, Beijing, China, People's Republic of
Background: Brief periods of ischemia performed just at the time of reperfusion can reduce infarct size and arrhythmia, a phenomenon called “ischemic postconditioning (IPC).” After reflow, enhancement of inward rectifier potassium current (IK1) has been involved in reperfusion arrhythmia. We hypothesized that postconditioning may modulate IK1.
Purpose: To investigate the effects of IPC on the current density of IK1 and action potential of rats ventricular myocytes.
Methods: Intervention of rats hearts was performed ex vivo using Langendoff perfusion instrument. Control hearts underwent 150mim of perfusion and without ischemia. The ischemia/reperfusion (I/R) hearts underwent 30min of ischemia and 120min of reperfusion. Post-conditioning consisted of 3 episodes of 30s of ischemia and 30s of reperfusion performed after 30s of reflow after the prolonged ischemia. Ventricular myocytes were singly isolated and soaked with collagenase. The current densities of IK1 and action potential of single rat ventricular myocytes were recorded by whole-cell path-clamp technique. Eight cells were enrolled in each group.
Results: With test potential of 0.5 Hz and −120mV, −90mV, −60mV, −30mV, and +50mV, the current densities of IK1 (pA/pV; absolute value) in IPC group were less than that in I/R group (−7.20±2.54 vs −12.37±3.50, −2.86±1.10 vs −3.99±0.94, −0.42±0.22 vs −0.69±0.14, 0.70±0.34 vs 1.05±0.35, 1.23±0.46 vs 1.81±0.58, respectively, each of them P>0.05), whereas no significant alteration between IPC group and control group. The resting membrane potential (RMP) of IPC group was lower than that in I/R group [(−80.03±3.68) mV vs (−68.39±3.10) mV, P>0.001]. The Action Potential Amplitude (APA) of IPC group was higher than that in I/R group [(119.91±3.12) mV vs (91.71±4.70) mV, P>0.001]. Action Potential Duration (APD), APD20, APD50, and APD90 (ms) of IPC group were longer than that in I/R group (119.91 ±3.12 vs 91.70±4.70, 17.80±1.42 vs 16.35±1.32, 45.17±3.29 vs 40.88 ±3.30, 87.04±6.58 vs 81.76±6.61, respectively, each of them P>0.05), whereas no significant alteration between IPC group and control group.
Conclusion: IPC reduces the current density of IK1, which contributes, at least in part, to APD prolongation, RMP decrease, and APA increase of rats ventricular myocytes during the period of reperfusion after ischemia.