457 Circulating adiponectin levels in patients with chronic heart failure: the effect of exercise training
AM Van Berendoncks; VY Hoymans; P Beckers; N Possemiers; CJ Vrints; VM Conraads
Antwerp University Hospital Cardiology, Edegem, Belgium
Background: The adipocytokine adiponectin is an insulin-sensitizing, anti-inflammatory and anti-atherogenic hormone. Contrary to other studied populations, high adiponectin levels have emerged as an independent risk factor for outcome in patients with chronic heart failure (CHF). Lifestyle adaptation restores reduced adiponectin levels in patients at risk for atherosclerotic disease. Modification of adiponectin levels in CHF patients has not been studied. We assessed circulating adiponectin concentrations in CHF patients and evaluated the effects of physical training.
Methods: Circulating adiponectin concentrations were measured using ELISA (Human adiponectin Quantikine Elisa, R&D systems) in 92 CHF patients and 10 healthy subjects. The effect of 4 months exercise training on adiponectin levels was studied in 63 patients out of this group. In addition, adiponectin was assessed twice (similar time interval) in an untrained control CHF group (n=29).
Results: Adiponectin levels were significantly higher in the CHF population (n=92, median age 58.7 years, range 27.2-80.5, 72% males) compared to healthy subjects (n=10, median age 55.0 years, range 38.0-85.0, 60% males) (10.855 mg/L±6.35 vs 6.577 mg/L±3.45, mean±SD, p=0.027). Adiponectin levels were related to heart failure severity (9.24±5.81 in NYHA I-II [n=47] vs 12.53±6.51 in NYHA III-IV [n=45], p=0.008).
Adiponectin concentrations measured at baseline in trained patients (n=63) were positively associated with NT-pro-BNP (r=0.488, p=0.01), HDL (r=0.400, p=0.01) and correlated negatively with BMI (r=-0.290, p=0.05), triglycerides (r=-0.501, p=0.01) and with exercise capacity (%VO2 peak: r=-0.236, p=0.070; maximal workload (r=-0.262, p=0.05).
Exercise training significantly reduced circulating adiponectin levels in CHF patients (11.122 mg/L±6.53 before, 10.566 mg/L±6.81 after training), whereas no changes were observed in the untrained control CHF group (10.077 mg/L±6.11 before, 11.111 mg/L±8.30 after similar time interval; p=0.044 for time × group interaction).
Conclusion: Circulating adiponectin concentrations are significantly higher in CHF patients compared to healthy subjects and increase in relation to disease severity. A pro-atherogenic risk profile is related to lower adiponectin levels, even in the presence of CHF. Physical training lowers circulating adiponectin levels.
458 The influence of physical training on left ventricular diastolic function and its relationship to exercise capacity in patients after myocardial infarction
I Korzeniowska-Kubacka; E Michalak; B Kusmierczyk-Droszcz; M Bilinska; R Piotrowicz
Institute of Cardiology Department of Cardiac Rehabilitation, Warsaw, Poland
Purpose: It remains uncertain whether exercise training program can improve the diastolic function in patients with CAD and diastolic LV dysfunction. Furthermore, the mechanisms of exercise capacity improvement after exercise training are not fully understood.
Nowadays, tissue Doppler echo (TDE) is a progress in LV diastolic function assessment. The aim of the study was to assess interval training effects on the diastolic left ventricular function (DLVF) and the relationship between diastolic LVF and exercise capacity in patients after MI.
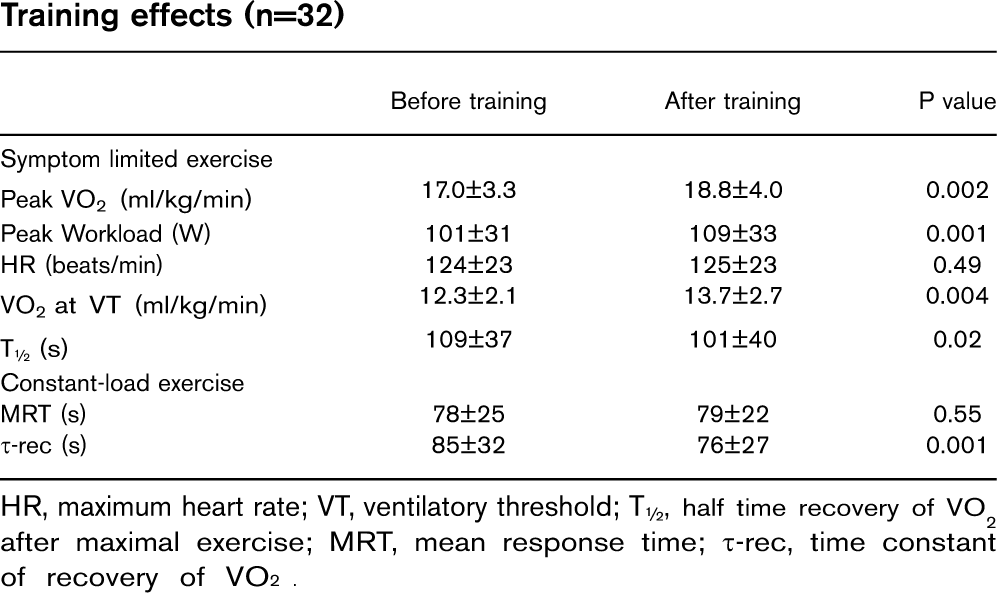
Methods: 22 male patients after MI, (mean age 56,6±7,5 years) with diastolic dysfunction in TDE and preserved systolic function participated in a 6-week interval training. All of them had cardiopulmonary exercise test (CET), TDE and TTE before and after the training cycle.
The following variables were measured: during CET - pVO2 (ml/kg/min), maximal workload (Mets), CET duration (min) and walking distance (m). During TDE: E'm-max velocity of lateral part of mitral annulus (m/s), A'-max velocity of lateral part of mitral annulus in atrial systole (m/s), E'm/A', E/E'm. During TTE: E-max velocity of early LV filling (m/s), A-max velocity of atrial filling (m/s), E/A, deceleration time (DT) (ms), IVRT - isovolumetric relaxation time (ms) The correlation between CET and TDE parameters was examined.
Results: After training program the following parameters improved significantly: CET duration increased from 12,08±1,83 to 13,37±1,22 (p=0,001), walking distance from 667,36±135,27 to 760,91±125,31 (p=0,001) and maximal workload from 7,01±1,32 to 7,7±1,28 (p=0,03). Moreover there was an increase in E'm/A' from 0,85±0,3 to 1,17±0,65 (p>0,05), and a decrease in E/E'm from 8,43±3,57 to 7,33±3,4 (p>0,05), both of which suggest an improvement of diastolic LVF. There was a negative correlation between increment of CET duration and A' (r=-0,399, p=0,05) and between A and CET duration (r=-0,409,p=0,05) and walking distance increment (r=-0,400,p=0,05). There was a positive correlation between E'm/A' and increment of CET duration (r=0,512, p=0,01).
Conclusion: 1. Systematic physical training after MI may have a beneficial effect on LV diastolic function in patients after MI and diastolic dysfunction. 2. Physical capacity improvement associated with interval training may depend on the improvement of diastolic LVF.
459 Three months of physical training improve left ventricular diastolic stiffness in chronic heart failure patients
G Malfatto1; G Branzi1; G Osculati2; P Valli1; F Ciambellotti1; G Parati3; M Facchini2
1Ospedale S Luca, Istituto Auxologico Italiano Divisione Di Cardiologia, Milano, Italy; 2Policlinico Multimedica IRCCS Cardiology, Sesto S Giovanni (Mi), Italy; 3Ospedale S Luca & Universita' Milano-Bicocca, Milano, Italy
Background: In long-term heart failure (HF), diastolic dysfunction is accompanied by abnormal neurohormonal control and progressive ventricular stiffness, whose occurrence significantly worsens the prognosis in all patients (pts). However, the analysis of diastole is complex, since it represents a sum of various phases determined by the balance between intrinsic ventricular characteristics and pressure gradients. According to a mathematical model, the passive diastolic properties of the left ventricle (i.e. its elastance=KLV) may be calculated by the formula: KLV=(70/[DT-20])22 mmHg/ml, where DT is the transmitral deceleration time obtained with Doppler echocardiography.
Purpose: The benefits of physical exercise in HF pts are well known. Training strongly affects both autonomic and neurohormonal regulation; despite its little effects on systolic function, it has been shown to improve left ventricular filling, i.e. the active diastolic phase. The effects of physical training on ventricular stiffness and passive diastolic properties, on the other hand, are poorly known, having been so far studied only in the experimental setting.
Methods: In 54 pts with chronic systolic heart failure (39 M, 15 F, 65 ± 10 years, NYHA 2.3+0.9, ejection fraction [EF] 32±5%), we analyzed the relationship between KLV and an index of neurohormonal derangement (=levels of Brain Natriuretic Peptide BNP), and investigated whether 3 months of physical training would interfere with diastolic stiffness. Twenty-seven patients (65±11 years, NYHA 2.3+0.5, EF 31±6%) were randomized to physical training, 27 patients were a control group. Before and after training we performed Doppler echocardiogram and cardiopulmonary stress test.
Results: At baseline, ventricular stiffness was significantly related to BNP levels (p>0.01) and to NYHA class (p>0.05). Training improved NYHA class and exercise performance and reduced BNP, while EF was unchanged. Moreover, a 27% reduction of elastance was observed (KLV 0.111+0.044 from 0.195±0.0811 mmHg/ml, p>0.01), whose magnitude was related to changes in BNP (p>0.05) and to KLV at baseline (p>0.01, Figure). No changes in KLV were observed in control pts after 3 months (0.192+0.115 from 0.195 +0.1211 mmHg/ml).
Conclusion: In HF, left ventricular diastolic stiffness is related to neurohormonal derangement and is modified by physical training. The improvement in left ventricular compliance could result from a slowing of the fibrotic process due to a better neurohormonal balance.
460 Effects of exercise training on systo-diastolic ventricular dysfunction in patients with hypertension: an echocardiographic study with tissue velocity and strain imaging evaluation
M Leggio1; L Sgorbini2; G Cruciani2; GR Cristinziani2; A Mazza3; MG Bendini3; F Leggio1; AP Jesi2
Purpose: New echocardiographic techniques, such as tissue Doppler imaging (TDI) and strain imaging (SI) have improved the assessment of systo-diastolic ventricular function in terms of accuracy and precision. A very interesting issue should be to examine, by means of these innovative echocardiographic tools, if exercise training could be able to improve the pattern of early mild systo-diastolic dysfunction frequently characterizing hypertensive patients. Therefore, aim of this study was the evaluation of left ventricular morphologic and functional parameters with traditional echocardiography, TDI and SI in patients (pts) with hypertension at baseline and at the end of a specific exercise training program for primary prevention of cardiovascular disease (CVD).
Methods: We evaluated 84 pts, mean age 58±10 years, 49 males, with treated hypertension who underwent a specific exercise training program, consisting in three exercise training sessions a week with endurance protocol on a treadmill or a cycloergometer. Systolic and diastolic blood pressure, heart rate and antihypertensive drug therapy were stable in the last 3 months; apart from familiar history of CVD, no others risk factors nor systemic diseases were represented in the study population. All pts were evaluated at baseline and at the end of the training program with traditional echocardiography, TDI and SI: for all pts, mean values of peak systolic, early diastolic and late diastolic velocities of the septal, lateral, inferior and anterior region of the mitral annulus were calculated; peak strain values of basal interventricular septum were also obtained.
Results: Base characteristics of the study population and traditional echocardiographic parameters showed no significant variations from baseline to the end of the program. About TDI parameters, mean values of peak systolic velocities were significantly increased (6.14±1.5 cm/s baseline, 7.13±1.8 cm/s end, p>0.01); mean values of peak early diastolic velocities were also significantly increased (6.08±1.6 cm/s baseline, 6.75±1.7 cm/s end, p>0.05); mean values of peak late diastolic velocities showed a trend to a decrease without reaching statistical significance (6.88±1.7 cm/s baseline, 6.48±2.0 cm/s end, p=0.06). About SI measures, peak strain values of basal interventricular septum were significantly increased (20.78±3.6% baseline, 24.56±3.9% end, p>0.01).
Conclusion: In our study, even if traditional echocardiography showed no differences, the positive effect of exercise training on left ventricular dysfunction in these pts (primary prevention) is demonstrated and emphasized by both TDI and SI.
461 Different pattern of modifications for haematopoietic and endothelial progenitor cells after a strenuous exercise in sedentary healthy men
F Cesari1; F Sofi1; A Capalbo1; N Pucci1; R Caporale2; AM Gori2; S Califano3; R Abbate3; GF Gensini4
1University of Florence Medical and Surgical Critical Care, Florence, Italy; 2Azienda Ospedaliero-Universitaria Careggi Central Laboratory, Florence, Italy; 3Institute of Sports Medicine, Florence, Italy; 4Don Carlo Gnocchi Foundation Onlus IRCCS, Florence, Italy
Introduction: Physical exercise has been reported to increase the number of circulating haematopoietic (HPCs) and endothelial progenitors cells (EPCs) in athletes and in moderately-trained subjects, but no data on the effect of exercise on the mobilisation of these cells in sedentary subjects are available. The aim of this study was to assess the effect of a maximal exercise test on HPCs and EPCs in a group of healthy sedentary men.
Methods: Twenty men with a median age of 34 (range: 22-40) years underwent to a maximal incremented graded treadmill test. The number of HPCs and EPCs were determined pre-exercise (T0), immediately at the end of the exercise test (T1) and 30 minutes after (T2). Peripheral blood HPCs were defined as CD34+, CD133+ and CD34+/CD133+ while EPCs were defined as CD34+KDR+, CD133+KDR+ and CD34+CD133+KDR+ by flow cytometry.
Results: HPCs showed a pattern of modification that included a significant (p>0.05) increase (CD34+: 4.31±3.1 vs. 3.14±1.7; CD133+: 4.3±3.1 vs. 3.1±1.6; CD34+/CD133+: 4.3±3.2 vs. 3.1±1.8 cells/L, for T1 and T0, respectively) for all the three types at T1, with a following significant decrease at T2 (CD34+: 2.9±1.7; CD133+: 2.9±1.7; CD34 +/CD133+: 2.9±1.7 cells/L; p=0.002). On the contrary, EPCs reported a specular pattern of modifications with a significant decrease immediately after the acute exercise (CD34+/KDR+: 0.06±0.04 vs. 0.08±0.06, p=0.04; CD133+/KDR+: 0.07±0.05 vs. 0.09±0.04, p=0.02; CD34+/CD133+/KDR+: 0.06±0.05 vs. 0.08±0.04, p=0.04 for T1 and T0 respectively), and a subsequent increase at T2, 30 minutes after the exercise (CD34+/KDR+: 0.08±0.05; CD133+/KDR+: 0.09±0.06; CD34+/CD133+/KDR+: 0.08±0.05).
Conclusion: In conclusion, we documented that intensive physical exercise has different effects in modifying HPCs' and EPCs' circulating levels. In fact, while HPCs significantly augmented immediately after the acute exercise, probably due to the increase of the leukocyte turnover, EPCs showed a significant decrease with respect to baseline, possibly determined by the release of inflammatory mediators that are highly produced during the acute phase of the exercise.
462 Effects of a 3 week exercise training program on a bicycle ergometer during phase II cardiac rehabilitation program: comparison of two different methods of determining the individual exercise intensit
D Bott1; C Busch1; T Abel1; K Sahin2; M Kohlmeyer3; A Seifert1; W Mayer-Berger1; B Bjarnason-Wehrens2
1German Sport University Institute for Cardiology and Sports Medicine, Cologne, Germany; 2University Hospital of Cologne Biostatistics, Informatics and Epidemiology, Cologne, Germany; 3Clinic Roderbirken, Leichlingen, Germany
Background: In Germany phase II cardiac rehabilitation (CR) is offered as a 3 week intensive CR program, mainly in a residential setting. Bicycle-ergometer-training is an obligate element of this program. In the study two methods of determining the exercise intensity were compared.
Methods: 285 Patient with coronary artery disease (251 men, 34 women, 49.7±7.5 years), were randomised into two groups. Group I performed the exercise training with a work load according to 60% of symptom limited heart rate reserve, group II with 60% of the work load achieved by 3.000 mmol/l lactate during the incremental bicycle ergo-spirometry. The amount of exercise measured as the metabolic rate during each exercise unit was kept equal in both groups.
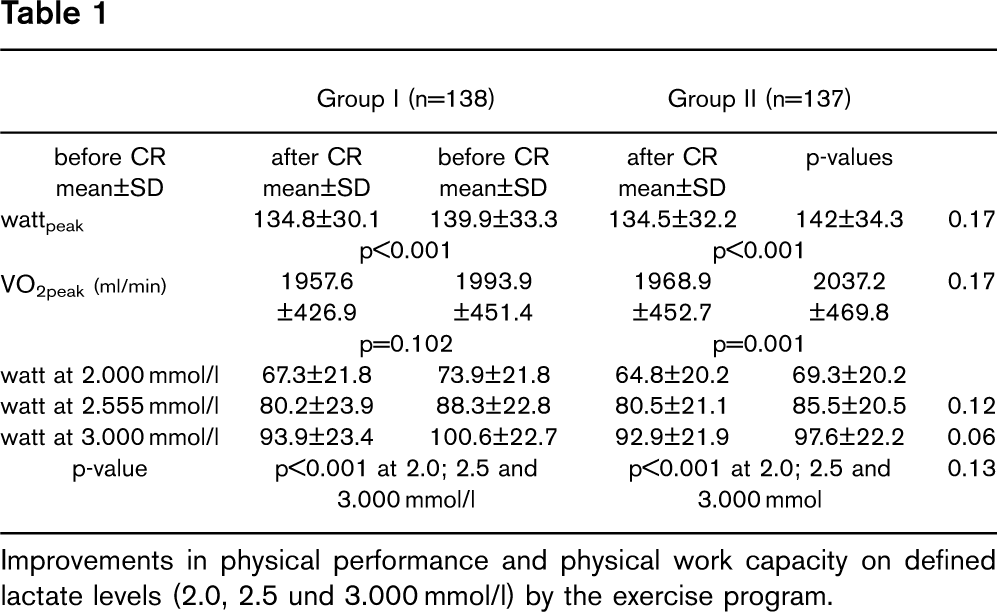
Results: During the 3 week CR the patients performed 10.7±1.1 exercise units on the bicycle ergometer. In Group I the mean exercise intensity was 24.5±21.5 watt (p>0,001) and the recommended heart rate 10.8±10 min-1 higher (p>0,001) than in Group II. The main outcomes are summarised in Table 1.
Conclusion: The results demonstrate that different methods of determining exercise intensity leads to significantly different exercise prescriptions. In both groups improvements in physical work capacity were achieved. Exercising with higher intensity did not result in better outcomes. These results indicate that to improve physical work capacity the total amount of exercise measured in metabolic rate per exercise unit is more important than the exercise intensity.
Group I (n=138)
Group II (n=137)
before CR
after CR
before CR
after CR
p-values
mean±SD
mean±SD
mean±SD
mean±SD
wattpeak
134.8±30.1
139.9±33.3
134.5±32.2
142±34.3
0.17
p>0.001
p>0.001
VO2peak (ml/min)
1957.6±426.9
1993.9 ±451.4
1968.9±452.7
2037.2±469.8
0.17
p=0.102
p=0.001
watt at 2.000 mmol/l
67.3±21.8
73.9±21.8
64.8±20.2
69.3±20.2
watt at 2.555 mmol/l
80.2±23.9
88.3±22.8
80.5±21.1
85.5±20.5
0.12
watt at 3.000 mmol/l
93.9±23.4
100.6±22.7
92.9±21.9
976±22.2
0.06
p-value
p>0.001 at 2.0; 2.5 and 3.000 mmol/l
p>0.001 at 2.0; 2.5 and 3.000 mmol
0.13
Improvements in physical performance and physical work capacity on defined lactate levels (2.0, 2.5 und 3.000 mmol/l) by the exercise program.
463 Comparison of endurance interval training on ergometer versus walking training in patients with heart failure in early phase after discharge
E Piotrowicz; R Baranowski; M Bilinska; A Wojcik; M Piotrowska; T Zielinski; R Piotrowicz
National Institute of Cardiology, Warsaw, Poland
The benefits of cardiac rehabilitation in patients (pts) with heart failure (HF) are well established. Now we are looking for an optimal and effective type of training.
Purpose: To compare the effectiveness of endurance interval training on an ergometer versus walking training in patients with heart failure in early phase after discharge.
Methods: The study group comprised 98 pts (59.6±9.3 years) with HF (NYHA II and III; EF>40%). After three weeks of clinical stability, the pts were randomized into two groups and underwent an 8-week endurance training. Group 1 (46 pts) underwent interval training on an ergometer. Group 2 (52 pts) underwent a specially prepared walking training. The programmed workload level for the two groups was 40%-60% of peak VO2. Fatigue was not to exceed 11 in Borg Scale. Training effectiveness was assessed by: delta distance in 6-minute walk test (δ6MWT), delta peak oxygen consumption (δpVO2), delta left ventricular ejection fraction (δEF) and improvement in NYHA class (δNYHA) as a result of comparing the distance covered in 6MWT, values of pVO2, EF and NYHA class from the beginning and the end of the program.
Results: The groups were comparable in terms of demographic data, baseline clinical and echocardiographic parameters and pharmacotherapy. The effectiveness of training in Group 1: δ6MWTwas 60±52 (m) - p=0.0001, δpVO2 was 1.2±2.5 (ml/min) - p=0.002, δEF was 1.6±4.2 (%) - p=0.02, δNYHA was 0.17±0.38 - p=0.004 The effective-ness of training in Group 2: δ6MWT was 44±57 (m) - p=0.001, δpVO2 was 1.9±2.6 (ml/min) - p=0.0001, δEF was 0.7±3.2 (%) - p=0.04, δNYHA was 0.38±0.49 - p=0.001. The differences between Group 1 and Group 2 were statistically insignificant in the following parameters: δpVO2, δ6MWT and δEF. The improvement in NYHA class was higher in Group 2 than in Group 1, and it was statistically significant.
Conclusion: 1. In HF pts in early phase after discharge walking training is as effective as endurance interval training on an ergometer. 2. The walking training seems a realistic strategy for HF pts.
464 Aerobic interval versus standard group exercise training after myocardial infarction
T Moholdt1; IL Aamot2; A Stoylen1; T Stolen1; I Granoien3; T Hole4; L Brattbakk5; T Graven3; U Wisloff4; S Slordahl4
1Norwegian University of Science & Technology Department of ciculation and medical imaging, Trondheim, Norway; 2St. Olavs Hospital, Trondheim, Norway; 3Aalesund Hospital, Alesund, Norway; 4Aalesund Hospital, Aalesund, Norway; 5Levanger Hospital, Levanger, Norway
Purpose: To determine the effect of group exercise training versus high intensity interval treadmill training upon peak oxygen uptake (VO2-peak) in myocardial infarction (MI) patients. Based on data from three hospitals in Norway, we wanted to compare usual care with an alternative exercise training model.
Methods: 107 MI patients referred to hospital based rehabilitation were randomised to standard group exercise training (n=71) or an interval treadmill protocol (n=36) in a 2:1 manner. Patients were recruited 2-12 weeks post MI. All patients were asked to meet for organized exercise training two times per week for 12 weeks and to exercise once weekly on their own. VO2peak was measured at baseline and again after 12 weeks. Patients randomised to group exercise participated in the usual exercise training program at the hospitals. The intensity of their exercise was supervised using heart rate monitors. The group exercise differed somewhat between the three hospitals. For the treadmill exercise patients each training sessions consisted of four times four minutes intervals at 85-95% of HRpeak with lower intensity periods in between.
Results: Eleven of the group training patients and five of the treadmill patients dropped out, so 91 patients were included in the analysis. VO2peak increased significantly in both groups, from 32.4 (SD 6.7) to 34.4 (SD 7.8) ml/min/kg (6.8%) in the group exercise training group and from 31.3 (SD 5.5) to 35.6 (SD 8.3) ml/min/kg (13,8%) in the treadmill group (both p>0.0001). The treadmill group had a statistical significantly larger increase (p=0.005). Also when analysed as intention to threat, the treadmill group had a larger increase (p=0.02).
Conclusion: High intensity interval treadmill training was more effective than the group exercise training after myocardial infarction. The results of this study may have implications on future organization of cardiac rehabilitation.
465 Importance of exercise training session duration in the rehabilitation of coronary artery disease patients
D Hansen1; P Dendale2; J Berger1; S Onkelinx1; I Reyckers1; A Hermans1; J Vaes1; V Reenaers1; R Meeusen2
1Vrije Universiteit Brussel Himan Physiology & Sportsmedicine, Brussels, Belgium; 2Virga Jesse Hospital Rehabilitation and Health Centre, Hasselt, Belgium
Purpose: In cardiac rehabilitation, 40 to 60-minute exercise training sessions are advised. However, because of the increasing coronary artery disease (CAD) prevalence and higher workload for cardiac rehabilitation centres, it remains to be established whether 40-minute exercise training sessions are equally effective as 60-minute exercise training sessions.
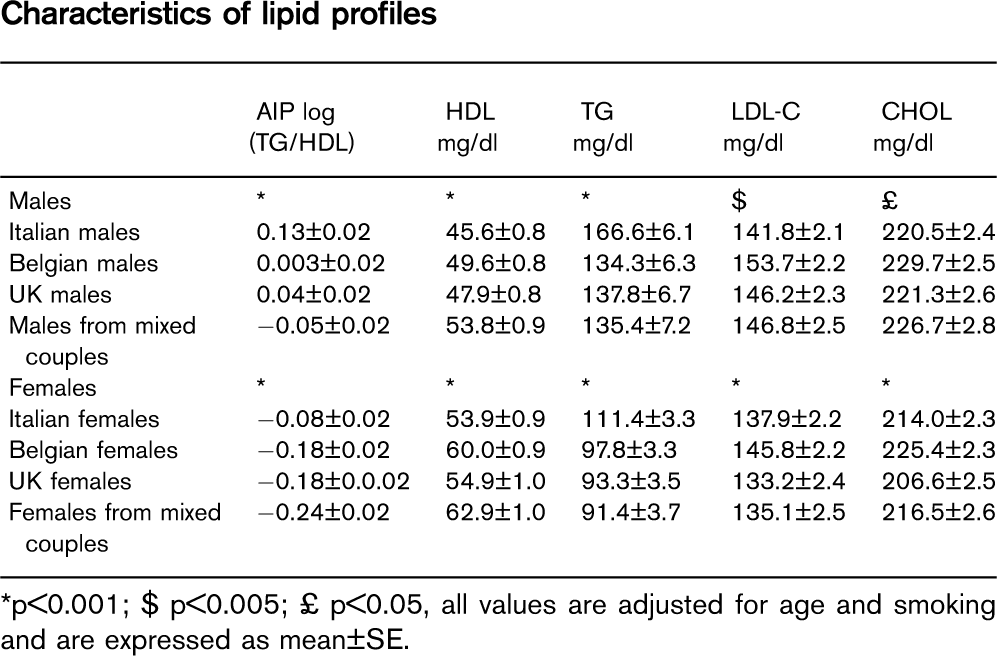
Methods: 134 CAD patients were included in a seven-week rehabilitation programme. All subjects exercised three days per week, at a heart rate corresponding to 65% of baseline VO2peak. Patients were randomised in two groups: 40-minute vs 60-minute exercise training sessions. Changes of body anthropometrics, peak exercise capacity and ventilatory threshold, blood plasma lipid profile and c-reactive protein level were assessed.
Results: As a result of rehabilitation, peak exercise capacity, ventilatory threshold, and blood plasma lipid profile improved significantly in total population (P>0.05), without differences between subgroups (P>0.05). Body weight and waist circumference decreased significantly in total population (P>0.01), but with greater magnitude in the 40 vs. 60-minute exercise session group (P>0.05).
Conclusion: In the rehabilitation of CAD patients, 40-minute exercise training sessions are at least as effective for improving body anthropometrics, blood plasma lipid profile and exercise capacity, as compared to 60-minute exercise training sessions.
466 Effect of glycosaminoglycan - sulodexide on oxidative stress and inflammatory risk factors in post CABG patients enrolled into phase II cardiac rehabilitation program
M Bilinska1; J Wolszakiewicz1; M Duda2; J Janas1; R Piotrowicz1
1Institute of Cardiology Cardiac Rehabilitation, Warsaw, Poland; 2Medical Center of Postgraduate Education Physiology, Warsaw, Poland
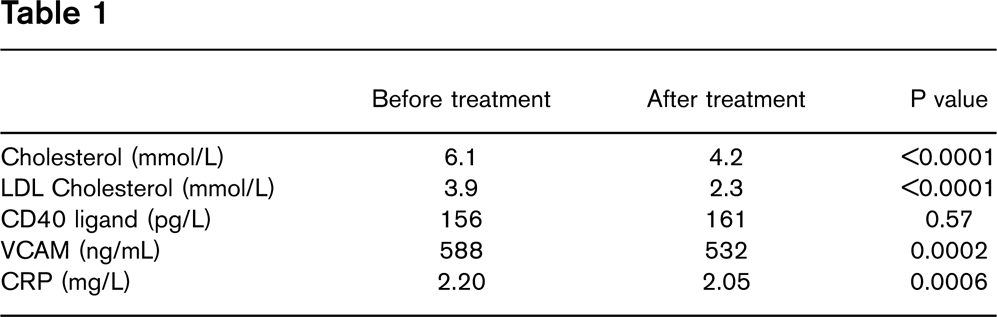
Background: A large number of studies suggest that oxygen free radicals play a major role in the pathogenesis of atherosclerosis. The purpose of this study was to determine the effect of short-term glycosaminoglycan-sulodexide administration on oxidative stress and proinflammatory risk factors in post CABG patients enrolled into eight-week phase II cardiac rehabilitation program.
Methods: Fifty six male patients (pts), mean age 55±6 ys, mean 2 months after CABG, with chronic stable angina, were randomized either to 8 weeks of sulodexide treatment, (SUL, n=28) or to a control group (n=28). Moreover, all pts received ACE-inhibitor, B-blocker, aspirin and statin. After baseline cardiopulmonary exercise test all pts underwent physical training, three times a week, at 60-70% of maximal estimated heart rate.
Isoprostanes (8-epi-PgF2alfa) as a sensitive index of lipid peroxidation and proinflammatory risk factors were measured in plasma samples collected at entry and at the end of the study.
Results: At entry all pts had comparable physical capacity (24,3±4,0 vs 25,1±3,6 ml/kg/min).
SUL treatment contributed to the more pronounced decrease in levels of 8-epi-PgF2alfa (77,4±38,3 vs 44,5±24,8 pg/ml, p>0.0001) comparing with controls (75,7±61,7 vs 68,3±59 pg/ml, p>0,05). However, levels of the remaining variables did not change significantly at the end of the study in both SUL and control groups: LDL cholesterol (2,72 vs 2,6999 mmol/l), triglyceride (1,49 vs 1,3999 mmol/l), uric acid (6,5 vs 6,22 mg/dl), homocysteine (12,9 vs 10,8 umol/l), fibrinogen (3,7 vs 3,6 g/l), hsC-reactive protein (0,16 vs 0,144 mg/l), leukocyte count (6,6 vs 6,3 x109/l), platelet count (194,4 vs 191,9 x109/l) and sedimentation rate (8,7 vs 8,44 mm/h).
Conclusion: During II phase of cardiac rehabilitation in post CABG patients with stable angina, short-term sulodexide administration had an additional antioxidant effect proven by a substantial decrease of 8-PGF2alfa.
467 The results of secondary coronary prevention in patients following bypass surgery
NK Dolidze; G Chapidze; Z Bakhutashvili; S Kapanadze; E Shengelia
Emergency Cardiology Center Secondary Coronary Prevention, Tbilisi, Georgia, Republic of
Background: Patients following bypass revascularization are at high risk for development of further coronary events. Ongoing atherosclerotic process may result in occlusion and stenosis of bypass grafts and native coronary arteries. Therefore, strategy of secondary coronary prevention is very important in such a category of patients.
Methods: 387 patients (349 male, 38 female, mean age 57±6.9 years) undergoing coronary artery bypass grafting (CABG) were enrolled in the study. Duration of the follow-up was 828±93 days. The primary end points were cardiac mortality rate and recurrent coronary events. The secondary end points were health-related quality of life, rehospitalization, repeat revascularization, low-density lipoprotein cholesterol (LDL-C) levels, left ventricular ejection fraction (LVEF) and prescribed drugs.
Results: Cardiac mortality rate was 2.06%, recurrent coronary events were observed in 3.87% patients. Rehospitalization was registered in 3.35% of cases, repeat revascularization - in 0.77% patients. Quality of life evaluation showed statistically significant improvement in almost all parameters. At the end of the follow-up target levels of LDL-C (less than 1000 mg/dl) were obtained in 74% of cases. There was significant increase in LVEF (p>0.05). The first line agents after CABG were aspirin and statins. Aspirin use was almost universal, 96% of patients received it. The use of statins was high enough − 84%.
Conclusion: According to our data on the basis of preventive strategies the mid-term results of CABG are satisfactory. The maintenance of results of CABG by the efforts of secondary coronary prevention is not less important than namely myocardial revascularization. Further follow-up is ongoing.
468 Effect of additional aerobic training during 4 week of cardiac rehabilitation in elderly patients after heart surgery
B Eder1; P Hofmann2; D Brandt3; R Pokan4; M Wonisch5
1Center for Cardiac Rehabilitation, St. Radegund, Austria; 2Human Performance Research Center; 3Graz, Austria; 4University of Vienna, Vienna, Austria; 5Center for Cardiac Rehabilitation, St. Radegund/Graz, Austria
Background: Early recovery of functional capacity after heart surgery is essential for a successful reintegration. Aim of this study was to assess the effects of intervention exercise (IG), (additional walking or cycle ergometer exercise) on exercise performance compared to a standard exercise rehabilitation program (control group, CG) after heart surgery in elderly patients.
Design: The trial consisted of 60 (32 male, 28 female) patients (mean age: 73.1±4.7), 12.2±4.9 days after heart surgery. Subjects were randomly assigned in 2 groups.
Methods: Subjects performed a symptom limited cardiopulmonary exercise test and a 6 min walk test (6-MWT). The MacNew questionnaire was used to assess quality of life (QOL). All tests were performed in a cardiac rehabilitation center before and after 4 wk of cardiac rehabilitation (CR). Both groups completed the standard exercise program (240 min/wk), IG completed an additional structured and regulated walking or cycle exercise training (210 min/ wk).
Results: At baseline, no significant differences for maximal (VO2peak, Pmax) and submaximal (6-MWT) exercise capacity were detected between IG group and CG. Global QOL was significantly higher in IG group. After 4 wk of CR, patients significantly improved in absolute values of cardiorespiratory testing, 6-MWT and QOL scores. Significant differences between groups were found post exercise for VO2peak (IG: 18.2±3.1 ml. kg-1.min-1; CG: 16.5±2.2∗ ml. kg-1.min-1), Pmax (IG: 72.2±16 W; CG: 60.7±15∗ W), (∗P>0.05), 6 minute-walking distance (IG: 454.8±76.3m; CG: 400.5±75.5∗ m), (∗P>0.05) and QOL.
Conclusion: Significant advantage of an additional exercise training compared to a standard rehabilitation training program in elderly patients after heart surgery was detected.
469 Phase one cardiopulmonary rehabilitation improves functional capacity and pulmonary function after coronary artery bypass graft surgery: a randomized trial
R Stein; CP Maia; AD Silveira; GR Chiappa; JP Ribeiro; Porto Alegre, Brazil
Background: Phase 1 cardiopulmonary rehabilitation (P1CRh) is widely recommended after coronary artery bypass surgery (CABG), however data are lacking regarding improvement in functional capacity and other cardiopulmonary measures.
Objective: To test the hypothesis that a postoperative P1CRh improves functional capacity, pulmonary function and respiratory muscle strength after CABG.
Methods: Twenty patients submitted to elective CABG were randomized to P1CRh or to control usual care. P1CRh included a 7-day program with respiratory exercises as well as cardiopulmonary and circulatory training. Before and 7 days after surgery, spirometry, manovacuometry, six-minute walk test (6MWT), and chest x-ray were performed. Thirty days after discharge all subjects underwent a maximal cardiopulmonary exercise testing and, pulmonary testing.
Results: Ten subjects were assigned to P1CRh and 10 to usual care. After randomization clinical characteristics were similar in the two groups. P1CRh resulted in significant improvement in maximal inspiratory and expiratory pressures measured at 7 and 30 days postoperative respectively (4.6±1.8 vs. 5±1.8 kPa; 6.1±2 vs. 6.9±2.6 kPa). Forced vital capacity (73±11 vs. 80.4±14 % predicted) and forced expiratory volume in one second improved only after 30 days (76±11 vs. 83±9% predicted). Distance walked in the 6MWT at day 7 was significantly higher in the P1CR group. Peak VO2 at day 30 was also higher (28%) in the P1CR group.
Conclusion: A 7-day P1CRh improves functional capacity, pulmonary function and respiratory muscle strength in patients submitted to coronary artery bypass surgery.
470 The results of a cardiac rehabilitation programme after coronary artery bypass surgery
K Pader; Budapest, Hungary
Objectives: Cardiac rehabilitation (CR) improves the clinical outcome of coronary artery disease (CAD) in general. We examined how the patients, who underwent coronary artery bypass surgery benefit from CR.
Methods: CR programme included a 3 weeks hospital phase, 9 weeks daily ambulatory phase. Patients had daily supervised exercise, weekly 2 times informative sessions about their disease, diet and smoking. A 6-minutes walking test was prepaired on the first day and before exmission in the hospital phase. The main risk factors were controled and the exercise capacity was measured with treadmill after 3 weeks and 12 weeks of the training process.
Results: In 2006 318 patients were admitted to our department after heart surgery. 251 (79%) of them underwent coronary artery bypass surgery, 159 (63%) participated in the CR, 45 (18%) were excluded because of age and medical reasons, 47 (19%) because of patient decision. There were no cardiac-events or significant medical complications during the exercise time at the 12 weeks follow up. There was a high percentage of compliance, 81% of all patients participated to the end and finished with closing examinations the 12 weeks training programme. A good control of main cardiovascular risk factors were achieved at 12 weeks: 87% of blood pressure control, 61% of LDL cholesterol levels, 59% of smoking cessation and 73% of weight and waist circumference reduction. Most of the patients (68%) increased exercise capacity. Mean increase in exercise capacity at 12 weeks was about 18% of basal capacity.
Conclusion: A CR for patients after coronary bypass surgery has a good compliance and acceptance and increases exercise capacity. In high percentage of patients can be achieved good secondary prevention results at 12 weeks follow up.
471 Cardiac rehabilitation after coronary artery bypass surgery: overcoming the barriers
M Worcester; B Murphy; P Elliott; R Higgins; A Goble
Heart Research Centre, Melbourne, Australia
Purpose: Routine referral to outpatient cardiac rehabilitation programs (CRP) is recommended by national and international expert authorities. Despite this, attendance at CRP is low, with reported levels of 37% to 66% in Australia. This low attendance has been attributed to patient factors. Little attention has been directed to referral methods and possible system failures. In the Cardiothoracic Surgical Unit at a major teaching hospital in Australia, routine referral occurs, with attention to assuring patient attendance if physically possible. This prospective cohort study audits the attendance rate of eligible patients and investigates the possible reasons for non-attendance.
Methods: A series of 184 patients who underwent coronary artery bypass graft surgery (CABGS) completed questionnaires pre-operatively. 170 (92%) of patients had their CRP attendance tracked after referral to CRP either at the parent hospital or elsewhere. Measures included CRP attendance and identification of reported sociodemographic, medical, psychosocial, cognitive and structural predictors of CRP non-attendance. Chi-squared tests and one-way ANOVAs were used to identify patient characteristics associated with CRP attendance. Variables associated with CRP attendance were then entered into a logistic regression analysis.
Results: The CRP attendance rate was 72%. Patients referred to CRP at the parent hospital were much more likely to attend than patients referred elsewhere to their nearest or most convenient CRP (OR=4.36; p=0.024). Travel time significantly predicted CRP attendance (OR=0.86; p=0.039). No other individual factor was significantly associated with CRP attendance in the logistic regression.
Conclusion: CRP attendance rate in this study was higher than previously reported for CABGS patients. The impact of individual patient factors is minimised when routine inclusive referral procedures are adopted, as in this case. The findings indicate that defined in-hospital recruitment and referral procedures, with a follow-up system to assure CRP attendance, minimised the effects of recognised common barriers to CRP attendance.
472 The benefit of physical training on haemodynamics in hypertensive patients
M Iurciuc1; D Gaita1; S Iurciuc1; C Avram2; S Ursoniu1; D Duda-Seiman1; S Dragan1; I Suceava1; O Fira-Mladinescu1
1University of Medicine Ambulatory Medicine, Timisoara, Romania
2Vest University Sport Medicine, Timisoara, Romania
Aim: To study the hemodynamic parameter and arterial stiffness before and after an rehabilitation program of 3 months.
Material and Method: We studied 120 patients with grade 2 of essential arterial hypertension with additional risk factor =2; under the same medication at least 3 month. They were at the target value of blood pressure (ESC/ESH 2003). This patients where evaluated clinically, paraclincicaly and by lab tests. We also evaluated the patients: by a stress exercise and by 24h blood pressure monitoring; before and after a rehabilitation program of 3 months. We study the hemodynamic parameters: Systolic blood pressure (SBP) diastolic blood pressure (DBP) mean blood pressure (MBP) pulse pressure (PP) heart rate (HR) at the office and by 24h blood pressure monitoring. We also studied the evolution of the SCORE risk and the ankle brachial index (ABI) before and after the rehabilitation program.
Results: After a 3 month physical training we obtained a decrease in: SBP from 134,9±5,3 to 130,7±5,1 mmHg (p=0.0112); SBP/24h from 119,86±4,11 mmHg to 113,70±4,033 mmHg (p=0.0013), DBP from 75,1±6,1 to 72,9±6,8 mmHg (p=0.0981); DBP/24h from 62,87±5,57 to 61,85±5.755 mmHg (p=0.1125) MBP from 93,4±5,88 mmHg to 94,0 ±6,1 mmHg (p=0.0981), MBP/24h from 81,86±5,36 mmHg to 79,80 ±4,933 mmHg (p=0.0045), PP from 58,79±8,79 to 55,33±7,722 mmHg (p=0.0382); PP/24h from 56,99±5.82 to 52,67±5.255 mmHg (p=0.0061).
Conclusion: Phisical exercise plays an important role in arterial compliance at hypertensive patients even with normal blood pressure value. Pulse pressure is significativly decreased at trained hypertensive person. At this kind of pations the only significativly results was at the ambulatory blood pressure monitoring (24 h). The physical training and life style changing offer a suplimentary decrease of hemodinamic and arterial stiffness parameters.
473 Cardiac rehabilitation in mild and moderate hypertensive Egyptian patients
F Aboul-Enein; A Zaky
Alexandria University, Alexandria, Egypt
Background: Hypertension is a major risk factor for coronary heart disease that affects over 25% of the Egyptian population. Non-pharmacological treatment especially aerobic exercise has been studied as a therapeutic measure for controlling hypertension.
The aim of this work was to study aerobic conditioning as a method of controlling mild to moderate hypertension in female Egyptian hypertensive patients.
Patients and methods: Patients with severe hypertension, uncontrolled diabetes, angina pectoris, and cerebrovascular stroke were excluded. 40 female hypertensive patients with mean age of 48±6.4 years and mean duration of disease 3.6±4.5 months were subjected to pre-exercising clinical evaluation and baseline stress ECG testing.
The program was individualized to restrict the patients to exercising aerobically; 50–70% of the maximum heart rate was considered the target zone. It lasted for eight weeks 3 sessions each, each session lasted from 20–30 minutes, during which patients were monitored for blood pressure and heart rate every 5 minutes to ensure that they exercised without reaching the anaerobic threshold. Exercise stress test was repeated at the end of the program to give an objective assessment of functional status.
Results: Follow-up assessment revealed significant reduction of resting heart rate (77.9±11.2 vs 73.9±9.4, P=0.009), systolic blood pressure (154.3±10.5 vs 131.5±10.1, P=0.005) and diastolic blood pressure (96.5 ±4.7 vs 85.8±3.6, P=0.04), with a significant decrease in resting RPP (215,345±19,472 vs 110,745±10,422, P=0.02). Stress test showed a significant reduction in peak systolic blood pressures and rate pressure product, in conjunction with significant increase in exercise time and METs achieved indicating better aerobic conditioning.
Conclusion: Treadmill walking is a feasible, safe, easy and effective aerobic training program that can control mild to moderate hypertensive Egyptian patients.
474 Low-intensity vs high-intensity exercise training improves glycemic control to a similar extent in obese, type 2 diabetes patients
D Hansen1; P Dendale2; M Beelen3; RAM Jonkers1; R Manders1; L Corluy2; A Mullens2; J Berger2; R Meeusen3; LJC Van Loon1
1Vrije Universiteit Brussel Human Physiology & Sportsmedicine, Brussels, Belgium
2Virga Jesse Hospital Rehabilitation and Health Centre, Hasselt, Belgium
3Maastricht University Movement Sciences, Maastricht, Netherlands
Purpose: Previously, 2 months of low-intensity (LI) and high-intensity (HI) exercise training were reported to be equally effective to improve glycemic control in obese, type 2 diabetes patients. However, considering the relatively short intervention period, the impact of training intensity over a more prolonged period remains to be established. Here, we assessed the clinical benefits of 6 months of either LI or HI endurance training, matched for energy expenditure in obese, type 2 diabetes patients.
Methods: A total of 37 male, obese type 2 diabetes patients (age 60 ±7y, BMI 31.3±3.77 kg/m2) participated in a 6-month endurance exercise training program. All subjects performed 3 supervised exercise sessions per week, either 55 min at 50% whole-body oxygen uptake capacity (VO2max) (LI) or 40 min at 75% VO2max (HI). Glycemic control, body composition, maximal workload capacity, and whole-body oxidative capacity were assessed at baseline and after 2 and 6 months of training.
Results: Endurance type exercise training lowered blood HbA1c levels, leg fat mass, and increased lean trunk muscle mass and VO2max (P>0.05), with no differences between the LI or HI trained group (P>0.05). However, trunk fat mass decreased to a significantly greater extent following HI exercise training, as compared to LI exercise training.
Conclusion: When matched for energy cost, LI exercise training is equally effective as HI training to improve glycemic control and augment whole-body oxidative capacity in obese type 2 diabetes patients.
475 Effect of Cardiac rehabilitation program on functional capacity following valvular heart surgery
R Ghalamghash1; B Goosheh1; A Emrani2; M Keyhani1; A Hosseini3
2Iran medical University Cardiac Rehabilitation, Tehran, Iran (Islamic Republic of)
3Modares University Cardiac Rehabilitation, Tehran, Iran (Islamic Republic of)
Background: The purpose of this study was to determine the effects of 4 to 6 weeks Cardiac Rehabilitation Program (CRP) on functional capacity improvement of patients six weeks following aortic and/or mitral valve replacement/reconstruction (AVR/MVR) surgery.
Methods: Fifteen experimental subjects were enrolled in the CRP. Functional capacity was estimated by oxygen uptake (VO2) during exercise tolerance testing (GXT) before and after the CRP. To determine the CRP mechanism and its effects on cardiac output, Left Ventricular Ejection Fraction (LVEF) was measured by manual and automatic echocardiography. Heart Rate (HR) and blood pressure (BP) as criteria to evaluate the patient's ischemic risk was measured. All measurement were performed before and after CRP sessions.
Results: Functional capacity and VO2 at the maximum stage of the GXT increased significantly for the participants (from 6.67 to 9.92 Metabolic Equivalents (METs), p>0.0001). Patient's LVEF increased significantly and at rest HR (from 92.86 to 84.40 bpm, p>0.003) and Systolic Blood Pressure (SBP) decreased significantly (from 113.33 to 104.000 mmHg, p>0.01) following CRP. No significant differences between before and after CRP were noted in Diastolic Blood Pressure (DBP) at rest (from 69.33 to 68.666 mmHg p=0.67, NS).
Conclusion: It was concluded that CRP strategies have positive effects on cardiac out put, functional capacity and patients functional class improvement in patients following aortic and/or mitral valve surgery.
476 Cardiac rehabilitation improves diastolic dysfunction after aortic valve replacement
A Yamaguchi; M Nagayama; H Watanabe; T Shimokawa; S Takanashi; T Sumiyoshi
Sakakibara Heart institude Cardiology Department, Tokyo, Japan
Background: Cardiac rehabilitation improves exercise tolerance without inducing left ventricular remodeling. Meanwhile whether cardiac rehabilitation improves diastolic dysfunction is yet to be proved.
Methods: We could research 343 patients who had aortic valve replacement due to aortic stenosis from December 2003 to December 2006. These patients were assessed their diastolic function by trans-thoracic echocardiography before the operation and 1 year after the operation. 62 patients had cardiac rehabilitation (who had cycle ergometry or treadmill at the exercise strength of the AT level more than two times per week for more than three months) and control group (n=281) did not have rehabilitation. We adopted E wave velocity, A wave velocity, E/A, E/e' to evaluate diastolic function. Furthermore we compared peakVO2/kg, AT, VE/VCO2, VO2/WR, peakVO2/HR before the operation and 6 months after the operation.
Results: Basal characteristics including age, gender, BNP, -blocker prescription, ACE/ARB prescription were not statistically different in both groups. Left ventricular ejection fraction (%) was 60±14 in rehabilitation group and 58±12 in control before the operation. E/e' was 17.6±6.9 in rehabilitation group and 18.2±6.6 in control before the operation, and 15.1±5.8 in rehabilitation group and 18.9±8.5 in control 1 year after the operation. We observed that systolic function immediately improved in both groups after the operation, and diastolic function was improved significantly in rehabilitation group after the operation (p=0.035). E/A and E wave velocity was not statistically different in both groups. PeakVO2/kg and AT also improved in rehabilitation group.
Conclusion: Cardiac rehabilitation improved diastolic function after aortic valve replacements due to aortic stenosis. Diastolic asynchrony of aortic stenosis is normalized later when hypertrophy and fibrosis regress. Cardiac rehabilitation may lead to short time to the improvement of diastolic function.
477 The effect of a selected functional electrical stimulation on thigh cross sectional area in anaesthetized and intubated cardiovascular patients
A Hermans1; J Berger1; P Dendale1; B Op'T Eijnde2; R Meesen1
1Virga Jesse Hospital Rehabilitation and Health Centre, Hasselt, Belgium
2Rehabilitation and Health Care Research Centr Department of Health Care, Hasselt, Belgium
Background and objective: It is well-known that long-term bed rest, such as in anaesthetized and intubated patients, induces massive muscle wasting/atrophy and thus reduces muscle functional capacity substantially and rehabilitation efficiency. Hence, any therapy that reduces muscle atrophy during prolonged inactivity may be of potential therapeutic interest.
Therefore, the present study aimed to investigate the impact of functional electrostimulation on muscle wasting/atrophy of the thigh in anaesthetized and intubated cardiovascular patients at ICU.
Methods: To evaluate muscle wasting/atrophy during inactivity, thigh perimeter was measured at baseline and following 7 days of anaesthetization and intubation in cardiovascular ICU patients. Furthermore, to evaluate therapy safety, blood saturation, systolic blood pressure, heart rate and respiration rate were evaluated before, during and after the treatment.
During ICU, the right legs of the participating patients received intermittent (5 phases, 5–8 min; frequency, 2–100 Hz; pulse duration, 250–330 μs) biphasic electrostimulation (ES, n=13) or control (CON, n=14) treatment. Every 3 days both study groups thigh perimeter was measured 5, 10 and 20 cm proximal to the upper edge of the patella of both legs.
Results: ES did not affect any of the observed cardiorespiratory parameters (p>0.05). Seven days of biphasic electrostimulation failed to reduce a reduction of thigh perimeter at 10 and 20 cm proximal to the upper edge of the patella. However, at 5 cm a thigh-perimeter-loss was completely prevented (p>0.05).
Conclusion: Electrical stimulation prevents reduction of thigh perimeter at 5 cm proximal to the upper patella edge following 7 days of intubation and anaesthetization of cardiovascular patients at ICU. Electrostimulation did not affect thigh perimeter at 10 and 20 cm proximal to the upper patella edge. Additionally, no influence of the electrical stimulation was shown on blood pressure, heart rate, respiration rate and blood saturation indicating that electrotherapy is a safe therapy.
478 The first experience of passive physical training in patients with pulmonary hypertension
AN Sumin1; NA Snytskaya2; OG Arhipov2
1Kemerovo Cardiologic Center Cardiology Department, Kemerovo, Russian Federation
2Sanatorium Topaz, Mysky, Russian Federation
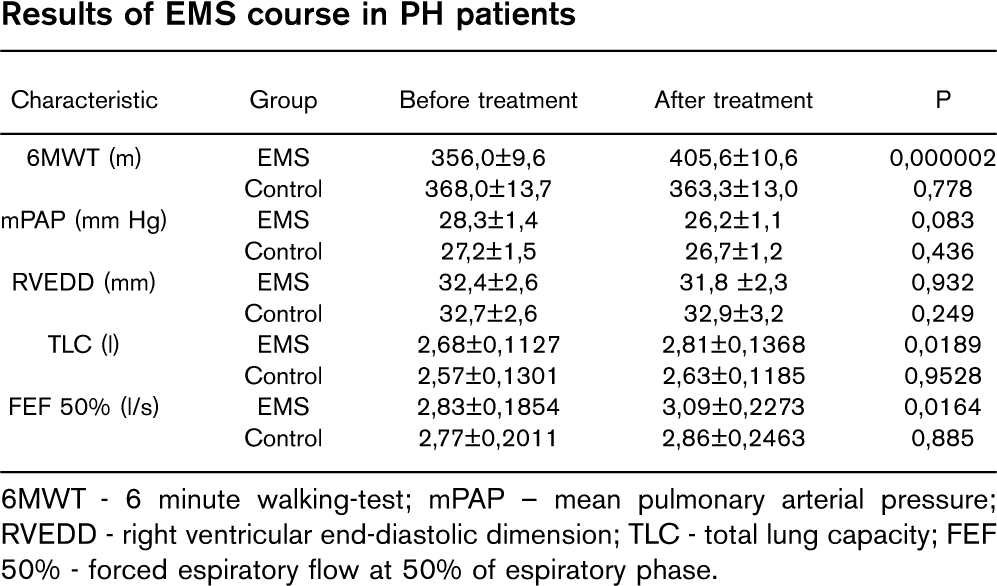
Pulmonary hypertension (PH) is associated with restricted physical capacity and a poor prognosis because of right heart failure. Usual physical training may have a negative impact on such patients. Electrical stimulation of skeletal muscles (EMS) could represent an alternative for patients with chronic heart failure, but at the patients with PH was not applied.
The objective of the our study was to evaluate the effectiveness and safety of EMS in patients with chronic PH. We examined 101 patients (59±1,1 yrs) with secondary PH. In control (n=47) the patients received the usual program of rehabilitations, in the EMS group (n=54) there was an additional EMS course. At baseline and after 3 weeks of the rehabilitation, all patients underwent a 6 minute walking-test (6MWT) and bicycle ergometric test (VEM). Estimation of a functional condition of skeletal muscles was determined with static (STAT) and static-dynamic tests (SDT) of flexors and extensors of lower extremity (LEF and LEE). EMS sessions were carried out 2 times a day for 30 minutes within 10 days.
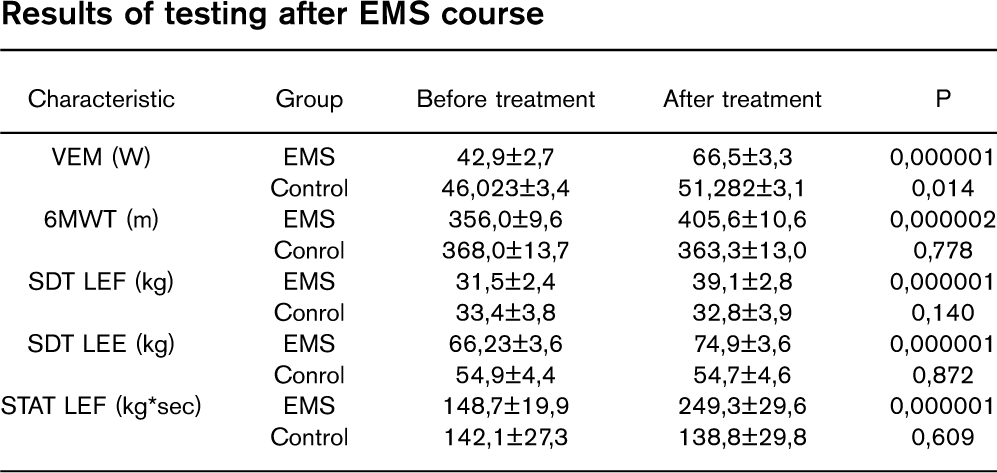
Results: According to static-dynamic tests after the course of EMS there was a substantial growth of muscles strength. In EMS group significant increases were observed in maximal VEM workload and distance 6MWT (see table).
Thus, passive physical trainings with EMS result to an significant increase of tolerance to physical loading due to increasing of force and endurance of skeletal muscles. This method deserves the further application for rehabilitation of patients with a chronic PH.
Results of testing after EMS course
Characteristic
Group
Before treatment
After treatment
P
VEM (W)
EMS
42,9±2,7
66,5±3,3
0,000001
Control
46,023±3,4
51,282±3,1
0,014
6MWT (m)
EMS
356,0±9,6
405,6±10,6
0,000002
Conrol
368,0±13,7
363,3±13,0
0,778
SDT LEF (kg)
EMS
31,5±2,4
39,1±2,8
0,000001
Conrol
33,4±3,8
32,8±3,9
0,140
SDT LEE (kg)
EMS
66,23±3,6
74,9±3,6
0,000001
Conrol
54,9±4,4
54,7±4,6
0,872
STAT LEF (kg∗sec)
EMS
148,7±19,9
249,3±29,6
0,000001
Control
142,1±27,3
138,8±29,8
0,609
479 French registry of acute aortic dissection admitted in cardiac rehabilitation center after surgical treatment
S Corone1; N Odjinkem1; MC Iliou2; T Farrokhi1; P Meurin3; B Pierre4; JM Feige5
1Centre Medical Bligny Readaptation Cardiaque Department, Briis Sous Forges, France; 2Hopital Broussais, Paris, France; 3Les Grands Pres 77174, Villeneuve Saint Denis, France; 4IRIS, Marcy L'etoile, France; 5Clinique Rhone Durance, Avignon, France
Background: After surgical treatment of acute type I dissection, a part of the aorta remains dissected. There is no consensus concerning the possibilities of physical activity for these postoperative patients.
Methods and results: This study is a registry to analyse the feasibility of a benefit-risk study. Thirty-three patients aged 55 (±9,3) were enrolled and followed from the admission in cardiac rehabilitation center up to 1 year clinically and by CT scan. The exercise training program, not standardized, included sessions of callisthenics, respiratory exercise, walking and cycling. During sessions (15,4±11), blood pressure was monitored and the exercise level was set for a Borg scale level of 11,1±1,6 (“moderate”). In 25% the blood pressure at maximum exercise was under 1500 mmHg, 1600 mmHg for 50% and for the last 25% it raised up to 1700 mmHg.
We observed 3 complications that needed a re-operation of the thoracic aorta during the rehabilitation stay (in 2 patients), an aortic valve replacement at 5 month and 3 cases of late ischemic complications but no death, no cerebral attack and no myocardial infarction. At exercise testing (cycle/10watts/mn), the maximal load improved from 63watts to 95 (13 subjects). Among 19 patients able to work, 10 returned to their job.
Conclusion: The first step of this registry allows thinking about a standardized exercise program to assess. Rest blood pressure, maximum exercise blood pressure and the initial thoracic descending aorta diameter appeared to be basic parameters.
480 A novel coronary heart disease risk evaluation and communication program improves modifiable risk factors in patients with hypertension: the REACH OUT study
L Erhardt1; JS Benner2; RA Moller3; N Rajicic3; SB Cherry1; Z Gaciong4; ES Johnson1; MCJM Sturkenboom5; J Garcia-Puig6; X Girerd7
1Lund University, Malmo, Sweden; 2IMS Health, Falls Church, Virginia, United States of America; 3Pfizer Inc, New York, New York, United States of America; 4The Medical University of Warsaw, Warsaw, Poland; 5Erasmus University Medical Center, Rotterdam, Netherlands; 6La Paz University Hospital, Madrid, Spain; 7Hopital Pitie Salpetriere Service d'endocrinologie metabolisme, Paris, France
Purpose: This analysis of the Risk Evaluation And Communication Health Outcomes And Utilization Trial (REACH OUT) assessed changes in modifiable CHD risk factors in patients receiving a non-drug intervention (INT) program to evaluate/communicate predicted CHD risk.
Methods: REACH OUT was a 6-month, prospective, controlled, cluster-randomized, multinational study. Hypertensive patients (45–64 y) with no CVD or diabetes, and Framingham 10-year CHD risk ≥10%, received INT or usual care (UC). Following baseline assessments, INT physicians were told patients' predicted CHD risk and advised patients according to a risk evaluation/communication program. UC physicians received baseline laboratory values, but were not told patients' predicted risk, and provided UC only. Changes in risk factors and predicted modifiable CHD risk (% risk in excess of that for a non-smoker of the same age, sex, and antihypertensive treatment status with “normal” BP and cholesterol), were determined at baseline and Month 6. Percentages of patients at treatment goals were also determined.
Results: Mean modifiable risk was reduced by 55% with INT (192 to 87%, n=524), and 47% with UC (221 to 117%, n=461; P=0.034 for INT vs. UC at Month 6, after adjusting for baseline values). Changes in risk factors contributing to reductions in predicted modifiable risk were greater among INT than UC patients: systolic BP was reduced by −20.3 vs. −15.44mmHg (P=0.001; baseline=1577mmHg INT; 1599mmHg UC), and total cholesterol by −6.3 vs. −4.4% (P=0.073; baseline=5.999 mmol/L in both groups), for INT vs. UC. At screening ∼50% of patients smoked; among these patients smoking cessation was higher with INT (29%) than UC (21%; P>0.05). Among INT patients, 48% met BP goal (>140/900 mmHg), 52% LDL-C goal (>3.444mmol/L), and 25% both goals, vs. 32%, 43%, and 14% of UC patients (P=0.003, P=0.005, P=0.002, respectively, INT vs. UC). Although weight was not considered in the Framingham calculation, weight was reduced significantly more with INT than UC (−1.1 vs. −0.44kg; P=0.015). Improvements with INT compared with UC do not appear to be related to increases in medication use, which were similar in both groups, but may be due to better adherence to medications/lifestyle changes.
Conclusion: Reductions in modifiable risk factors and predicted modifiable CHD risk were larger in patients receiving a risk evaluation/communication program than with UC. However, residual modifiable risk remained in both groups; additional therapeutic intervention to further lower CHD risk in patients with multiple modifiable risk factors is therefore required.
481 Change in cardiovascular risk factors prevalence through comprehensive cardiac rehabilitation program in patients with aortic valve replacement with and without CABG
DE Velimirovici1; M Rada1; D Berceanu Vaduva1; S Dragan1; D Gaita1; A Schnabel1; G Mancas1; I Gogoasa2; S Mancas2
1Univ. of Medicine & Pharmacy Victor Babes Cardiovascular Rehabilitation Clinic, Timisoara, Romania; 2Univ. of Agricultural Sciences of Banat, Timisoara, Romania
Objective: To establish the impact of comprehensive cardiovascular rehabilitation program on prevalence of risk factors in patients with aortic valve replacement and associated CABG.
Methods and materials: 96 patients where included in the study, from which 76 with aortic valve replacement (group A) and 20 with aortic valve replacement and associated CABG (group B). The prevalence of man was 63.54% and the average age was 68±7 years. We studie the prevalence of the following cardiovascular risk factors: BP=140/90 mmHg, BMI=30kg/m2, TC=200mg/dl, type 2 diabetes mellitus, smoking and ex-smoking condition. Phase II of cardiovascular rehabilitation program emphasizes the importance of safe physical activity and consisted of 12 weeks of exercise training: the first 2 weeks- in hospital with daily sessions (30min/day), and the next 10 weeks -out-patient rehabilitation with three sessions per week (30min/session), with an efort level (target heart rate) between 70–80% from the maximum heart rate achieved during the effort test. It subsequently was emphasized the importance of walking sessions (phase III RC). The purpose of the study was to determine the effectiveness of secondary cardiac prevention programs, by evaluating risk factors prevalence 6 months after surgery. Statistical analysis: average ±standard deviation, %ot, student t test.
Results: This study demonstrate that aortic valvular patients with associated coronary artery disease (group B), had a higher prevalence of studied risk factors, compared to the A- group. Six months after randomization, the prevalence of hypercholesterolemia decrease from 40% to 23,52% (p>0,001) in B- group and from 28,94% to 8,30% (p>0,005) on A- group, and the prevalence of active smokers was 21,12% on A-group versus 11,76% on B- group. We remark a significant statistical decrease in prevalence of smoking in both groups, considering the prevalence of active smokers of 32,89% in A- group and of 35% in B- group at the time of inclusion.
Conclusion: Aortic valve lesions associated with coronary artery disease have a higher prevalence of cardiovascular risk factors than isolated aortic valve lesions. Arterial hypertension, hypercholesterolemia and smoking modify through their prevalence the cardiovascular risk profile of patients with aortic valvulopathy. Comprehensive cardiovascular rehabilitation programs lead to improvement of major cardiovascular risk factors prevalence.
482 Effects of cardiac rehabilitation in Germany: metaanalysis of the effects from national and international trials
O Mittag1; S Schramm2; A Hueppe2; T Meyer2; H Raspe2
1University Medical Center of Freiburg Quality Management and Social Medicine, Freiburg, Germany; 2University of Luebeck Institute of Social Medicine, Luebeck, Germany
Cardiac rehab in Germany is offered as an inpatient treatment lasting 3 weeks. Evidence for this kind of health care is poor, due to the focus on observational cohort studies only. Reliable evidence for the effectiveness of cardiac rehab is solely available from international RCTs, and applies to outpatient programs lasting 6 to 12 weeks or longer.
We conducted a systematic search for relevant German studies (1990-2004). International studies were selected from recent metanalyses. Intra-group effect sizes were computed for national studies and international treatments and controls separately. In the following, medium-term (12 months) results are presented.
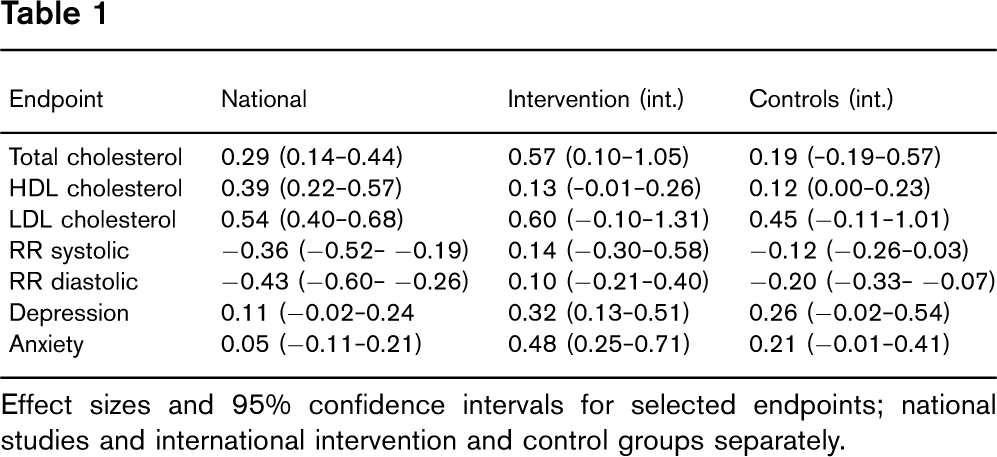
77 national cohort studies were identified. Results of these studies were compared to the effects in the treatments (IG) and controls (CG) of 40 international RCTs. Table 1 shows the effect sizes for selected endpoints.
Except for HDL, no statistically significant differences as to lipids were found. For blood pressure the effect sizes differ significantly with lower effect sizes in the national studies. Effect sizes for depression and anxiety in the national studies are lower compared to international IGs. Poor results as to blood pressure control in Germany are known from other research. But low effect sizes for changes in depression and anxiety in German cardiac rehab trials have not been reported so far. It seems likely that short term programs are less effective than interventions lasting for six weeks or longer as far as psychological outcomes are concerned. Further analyses will be conducted with special attention to moderating variables such as age, gender, and program duration.
Endpoint
National
Intervention (int.)
Controls (int.)
Total cholesterol
0.29 (0.14- 0.44)
0.57 (0.10–1.05)
0.19 (−0.19–0.57)
HDL cholesterol
0.39 (0.22–0.57)
0.13 (−0.01–0.26)
0.12 (0.00–0.23)
LDL cholesterol
0.54 (0.40–0.68)
0.60 (−0.10–1.31)
0.45 (−0.11–1.01)
RR systolic
−0.36 (−0.52- −0.19)
0.14 (−0.30–0.58)
−0.12 (−0.26–0.03)
RR diastolic
−0.43 (−0.60- −0.26)
0.10 (−0.21–0.40)
−0.20 (−0.33- −0.07)
Depression
0.11 (−0.02–0.24
0.32 (0.13–0.51)
0.26 (−0.02–0.54)
Anxiety
0.05 (−0.11–0.21)
0.48 (0.25–0.71)
0.21 (−0.01–0.41)
Effect sizes and 95% confidence intervals for selected endpoints; national studies and international intervention and control groups separately.
483 Association of physical activity with all-cause and cardiovascular mortality - a meta-analysis
M Nocon; T Hiemann; F Muller-Riemenschneider; F Thalau; S Roll; SN Willich
Charite University Medical Center Institute For Social Medicine, Epidemiology, Berlin, Germany
Purpose: Over the past decades, numerous large cohort studies have attempted to quantify the protective effect of physical activity on cardiovascular and all-cause mortality. The aim of our review was to provide an up-to-date overview of study results.
Methods: In a systematic MEDLINE search conducted in May 2007, we included cohort studies that assessed the primary preventive impact of physical activity on all-cause and cardiovascular mortality. We report risk reductions based on the comparison between the least active and most active population subgroups, with the least active population subgroup as the reference group. Random-effect models were used for meta-analysis.
Results: A total of 33 studies with 883,372 participants were included. Follow-up ranged from 4 to over 20 years. The majority of studies reported significant risk reductions for physically active participants. Concerning cardiovascular mortality, physical activity was associated with a risk reduction of 34% (95% confidence interval, 29%–39%). All-cause mortality was reduced by 33% (28%–37%). Studies that used patient questionnaires to assess physical activity reported lower risk reductions than studies that used more objective measures of fitness.
Conclusion: Physical activity is associated with a marked decrease in cardiovascular and all-cause mortality in both men and women, even after adjusting for other relevant risk factors.
484 Effects of drug, biobehavioural and exercise therapies on heart rate variability in coronary artery disease: a systematic review
RP Nolan1; P Jong1; SM Barry-Bianchi2; TH Tanaka3; JS Floras3
1University Health Network/Univ. of Toronto Cardiology, Toronto, Canada; 2University Health Network Behavioural Cardiology Research Unit, Toronto, Canada; 3Tsukuba University of Technology, Tsukuba, Japan
Purpose: Heart rate variability (HRV) is reported as a surrogate index for clinical outcome in trials of secondary prevention strategies for coronary artery disease (CAD), but a standardized guide for interpreting HRV change is not established. We evaluated HRV change in trials with CAD patients who received conventional medications (beta- or calcium channel blockers, angiotensin converting enzyme inhibitors), biobehavioral treatment (psychotropics, biofeedback, relaxation) or exercise training.
Methods: Medline, Pubmed, Psycinfo, the Cochrane database and Embase were searched until July 2007, without language restriction. We identified 33 randomized controlled trials. Two reviewers independently abstracted all trials using a standardized form. A hierarchy of frequency and time domain HRV indices defined outcome.
Results: A random effects model yielded an overall pooled standardized mean difference (SMD) between treatment and control groups of moderate magnitude across treatment classes, based on a composite of time and frequency domain indices (SMD=0.40, p>0.0001), or only time or frequency indices (SMD=0.37 and 0.43 respectively, both p>0.0001). This change was equivalent to an increase in SDNN of 9.0 ms [95% Confidence Interval (CI), 7.3, 10.7 ms] or a relative increase of 15.9% (95% CI, 13.2, 18.6%). To detect HRV change of this magnitude, a hypothetical trial would require a sample size of 660 subjects for conventional medications or 1232 subjects for all treatment classes.
Conclusion: Pharmacologic, biobehavioral and exercise strategies for secondary prevention of CAD significantly increase HRV. This review provides a framework to assist efforts to evaluate the contribution of HRV change to CAD prognosis.
485 Evaluation of two new methods for continuous cardiac output assessment during exercise in patients with congestive heart failure
HMC Kemps1; HJM Thijssen1; G Schep1; BTHM Sleutjes2; WR De Vries2; AR Hoogeveen2; PFF Wijn1; PA Doevendans3
1Maxima Medical Centre, Veldhoven, Netherlands; 2Eindhoven University of Technology, Eindhoven, Netherlands; 3University Medical Centre, Utrecht, Netherlands
Purpose: This study investigated in patients with congestive heart failure (CHF) the reliability of 2 continuous cardiac output measuring methods at rest and during exercise: an arterial pulse contour analysis method (PulseCO), calibrated at rest by an indicator dilution method (LiDCO), and a impedance cardiography technique (Physioflow), using the Fick method as a reference.
Methods: Ten male CHF patients (New York Heart Association class II-III) were included. At rest, cardiac output measurements obtained by LiDCO and Physioflow were compared with the direct Fick method. During exercise PulseCO, calibrated by LiDCO, and Physioflow were compared with the continuous Fick method. Exercise, performed on a cycle ergometer in upright position, consisted of light and moderate constant-load (CL) exercise at 30% and 80% of the ventilatory threshold and a symptom-limited (SL) exercise test.
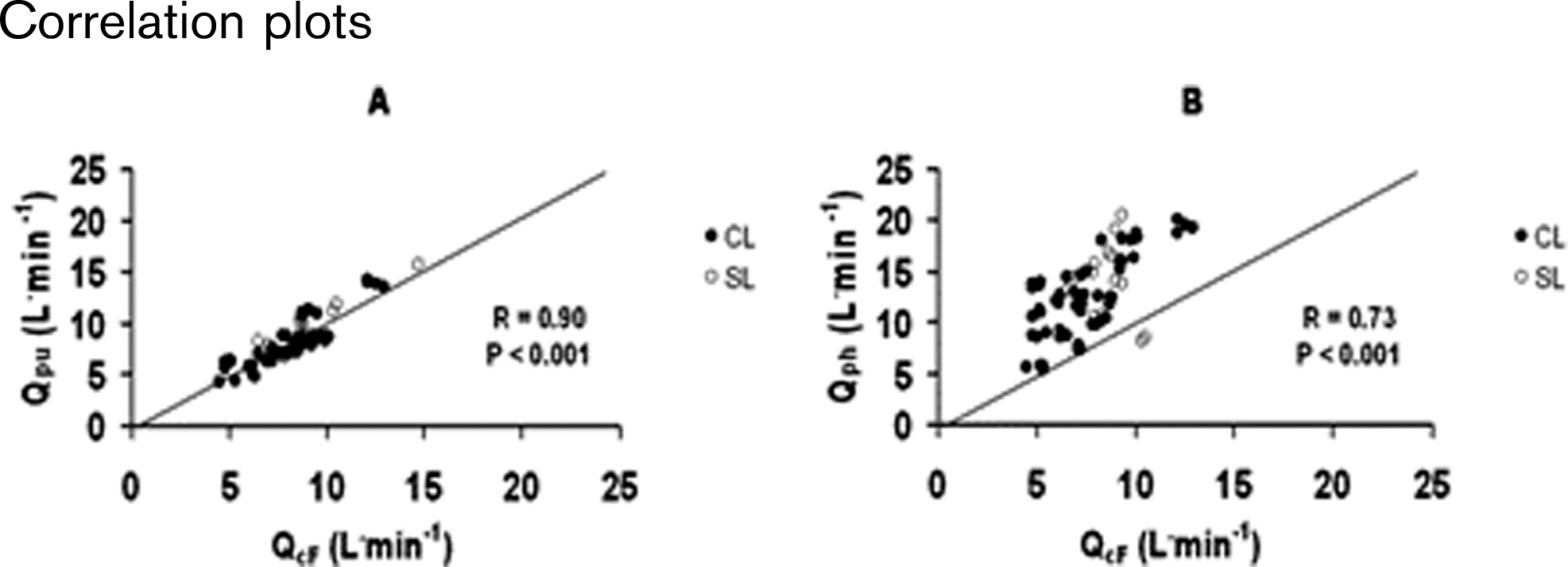
Results: At rest, LiDCO showed good agreement with the direct Fick method, while Physioflow systematically overestimated reference values (bias±limits of agreement (LOA), −1%±28% and 48%±60% respectively). During exercise, both PulseCO (Qpu) and Physioflow (Qph) correlated significantly with the continuous Fick method (QcF) (Figure). In contrast with Physioflow, PulseCO showed good agreement with the continuous Fick method (bias±LOA, 2%±28% and 48%±52%, respectively). Exercise-related within-patient changes of cardiac output assessed by both PulseCO and Physioflow showed clinically acceptable agreement with reference values (bias±LOA: 2%±26% and −2%±36%, respectively).
Conclusion: PulseCO, calibrated by LiDCO, provides accurate measurements of cardiac output during exercise in CHF patients. Although Physioflow overestimates cardiac output, this method may still be useful to estimate changes during exercise.
Correlation plots
486 Isovolumic relaxation time monitoring during the stress-echo is a new method of non-invasive assessment of the left ventricular diastolic reserve
A Bobrov; S Shulenin; N Hyshova
Military Medical Academy Propaedeutics, Saint Petersburg, Russian Federation; Almazov's cardiology research institute, Saint Petersburg, Russian Federation
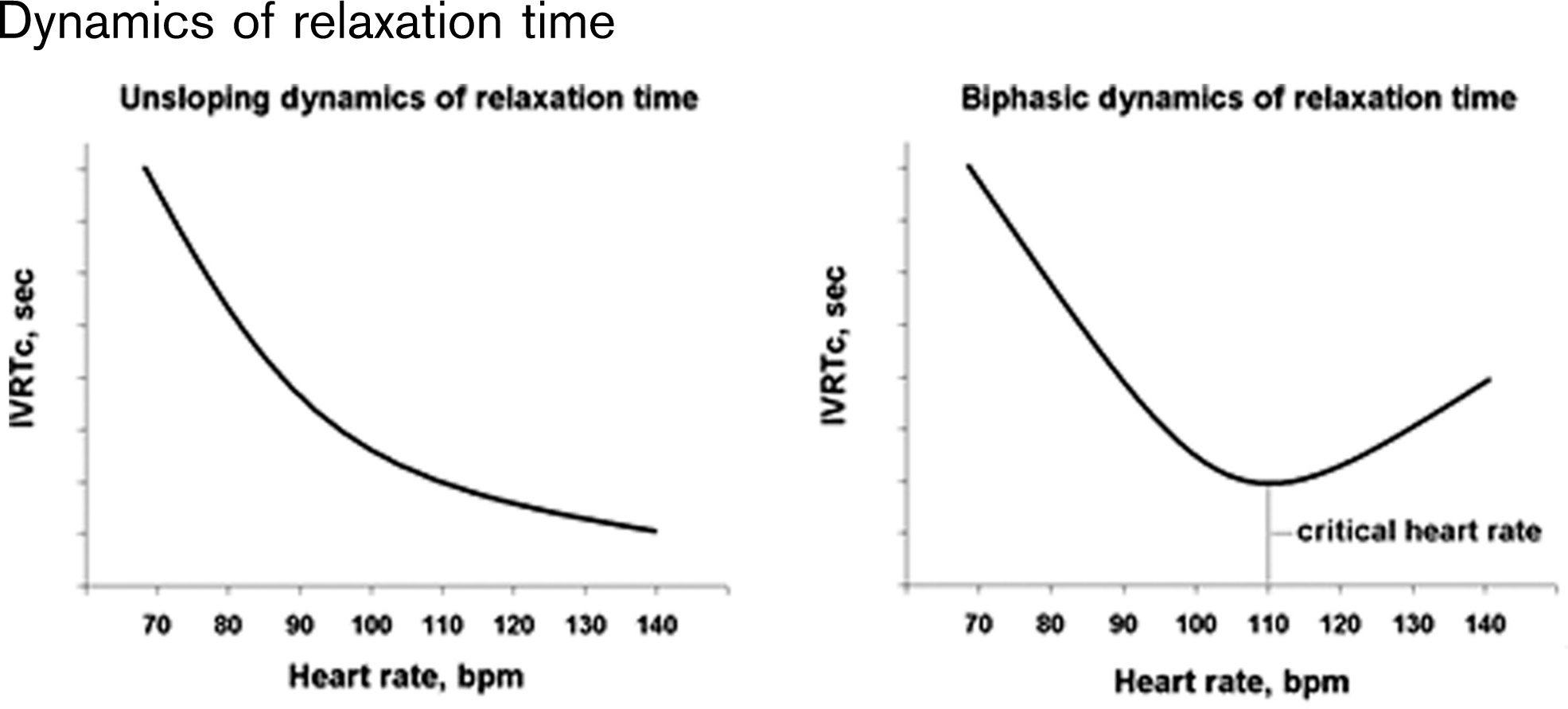
Purpose: In healthy men the exercise leads to increasing of the heart rate and decreasing of relaxation time right up to the maximal heart rate. Increasing of relaxation time during heart rate growth identifies the decompensation of the heart relaxation. This condition we can observe in patients with heart failure.
Method: To assess the possibility of diastolic reserve evaluation we propose a new method. During the stress test with the help of continuous wave Doppler the blood flow in the left ventricular is registered. Isovolumic relaxation time (IVRT) is calculated on the heart rate 70, 80, 90, 100, 110, 120, 130, 140 bpm. To correct the influence of heart rate on relaxation time we use Bazett formula (IVRTc=IVRT/square root of RR interval).
Results: In healthy men stress leads to increasing of the heart rate and decreasing of relaxation time index right up to the maximal heart rate. In men with heart failure there is increasing of relaxation time during heart rate growth. Cardiac frequency at which IVRTc starts its ascending limb called critical heart rate (Figure). If there is no possibility to access exercise test we propose to use dobutamine stress echo. We enrolled 20 patients with mild stable angina (with biphasic IVRTc curve) referred for the exercise stress-echo with cycling and dobutamine. Means of critical heart rate were identical in each stress group (p>0.05). Correlation between the values of critical heart rate during cycle and dobutamine tests was strong (r=0.92, p>0.05).
Conclusion: Noninvasive estimation of isovolumic relaxation time during the exercise stress-echo can evaluate diastolic heart reserve. A biphasic IVRTc pattern during the exercise stress echo identifies diastolic heart failure. Cycle and dobutamine stress echo are equivalent in detecting of diastolic reserve.
Dynamics of relaxation time
487 Cardiac power output measurements in patients on left ventricular assist devices, explanted (recovered) patients and those with severe heart failure
D Jakovljevic1; G Donovan1; D Nunan1; R Bougard2; R George2; M Yacoub3; E Birks3; D Brodie1
1Buckinghamshire New University Research Centre for Society and Health, Chalfont St Giles, United Kingdom; 2Royal Brompton and Harefield NHS Trust Transplant ECG, Harefield, United Kingdom; 3Magdi Yacoub Institute, Heart Science Centre Cardiology, London, United Kingdom
Purpose: It has been demonstrated that left ventricular assist devices (LVADs) can in many patients prevent the need for subsequent transplantation. Cardiac power output (CPO) is a direct indicator of overall cardiac function and can play a major role in risk stratification and prognosis in heart failure. We aimed to assess CPO in patients implanted with LVADs, those explanted due to myocardial recovery and in those with severe heart failure.
Methods: Measurements during exercise testing were undertaken using non-invasive, inert gas, rebreathing haemodynamic and respiratory gas procedures. They were performed on 39 patients 16 severe heart failure (HF) patients (age 45+3 yrs), 10 implanted LVAD (IMP) patients (age 39±12 yrs) and 13 explanted LVAD (EXP) patients (age 40±13 yrs).
Results: Peak CPO was significantly higher in the EXP than the HF and the IMP patients (HF, 1.61±0.51; IMP 2.03±0.65; EXP 2.51±0.62 W; p>0.001) as was peak cardiac output (HF, 7.6±2.2; IMP, 10.4±1.6; EXP, 12.3±3.3 l.min-1; p>0.001). Peak CPO was not significantly different between HF and IMP patients. At rest there was a non significant difference in cardiac power output between the HF, IMP and EXP patients, whereas cardiac output in the IMP group was higher compared with the HF group (5.3±1.8 vs. 4.2±1 l.min-1, p>0.05). Mean arterial blood pressure at rest and at peak exercise was not significantly different between the HF, IMP and EXP patients.
Conclusion: Our data suggests that peak cardiac power output is a useful tool in patients receiving LVADs. A peak CPO of 1.96 W is considered to be a ‘cut-off’ value for good and poor prognosis in heart failure, therefore IMP and particularly EXP patients appear to have better prognosis than HF patients. It appears that cardiac power output is a useful physiological marker of heart failure severity and can guide management of LVAD patients.
488 Exercise-induced left ventricular systolic and diastolic dysfunction in patients with essential hypertension and normal cardiac function at rest
I Korzeniowska-Kubacka; E Florczak; A Klisiewicz; B Dobraszkiewicz-Wasilewska; R Piotrowicz
Institute of Cardiology Department of Cardiac Rehabilitation, Warsaw, Poland
Purpose: Seismocardiography (SCG) can be used to monitor changes in cardiac function during exercise test (EXT) based on systolic and diastolic cardiac time intervals.
The aim of the study was to assess SCG usefulness for early diagnosis of left ventricular systolic and diastolic dysfunction in patients with essential hypertension and normal systolic and diastolic function at rest.
Methods: The study population consisted of 63 patients (pts) with hypertension aged 43±8 years with normal systolic and diastolic function at rest based on ECHO and 30 healthy volunteers aged 34±7 years. All of them had undergone a symptom limited exercise test (EXT) on cycloergometer. SCG was done simultaneously with EXT. The measurements included: workload in Watts, duration of EXT in minutes, HR and BP at rest and effort from EXT as well as left ventricular systolic and diastolic time intervals in ms - PEP, IVCT, LVET, IVRT, PEP/LVET, MPI=((IVCT+IVRT)/LVET), g value, from SCG. The results were analysed statistically by the t-Student test. The value of p>0.05 was accepted as statistically significant.
Results: In hypertensive pts we observed elongation of PEP from 111±13 to 112±13 IVRT from 55±13 to 59±18 (p=ns), shortening of LVET from 308±20 to 295±20 (p=0.004) and increase of PEP/LVET from 0.36±0.06 to 0.38±0.07(p=0.04) and g value from 44±16 to 82±31(p>0.001) during exercise SCG. Then we assessed subgroup of 30 pts with hypertension and comparable age with healthy volunteers.
In comparison with the healthy controls, a total myocardial performance observed in the group of hypertensive pts was worse i.e., MPI was higher=0.38±0.11 vs 0.26±0.1 (p=0.001) and the diastolic dysfunction was observed in the form of IVRT prolonged during exercise from 56±12 to 60±19 ms. Moreover longer IVRT 60±18 vs 38±16 ms (p>0.001) and lower g value 87±29 vs 106±19 (p>0.01) were found during exercise in comparison to healthy subjects.
Neither were statistically significant differences between both groups found in terms of physical capacity: workload 155±30 vs 168±28, EXT duration 9±2 vs 9±2; p=ns.
Conclusion: 1. Hypertensive patients developed systolic and diastolic dysfunction during exercise SCG. 2. A worse total myocardial performance observed in hypertensive patients during exercise SCG in comparison to healthy subjects. 3. Seismocardiography may be a useful method for early diagnosis of left ventricular systolic and diastolic dysfunction.
489 Cardiac rehabilitation in left ventricular diastolic dysfunction: effect on cardiac function and functional capacity
J Murakami; H Adachi; H Tsurugaya; S Ohshima; K Taniguchi
Gunma Prefectural Cardiovascular Center Cardiology, Maebashi, Gunma, Japan
Background: Exercise training improves functional capacity in patients with systolic dysfunction, but the role of exercise training in diastolic dysfunction is unclear. We sought to evaluate whether the exercise training would influence on left ventricular diastolic dysfunction.
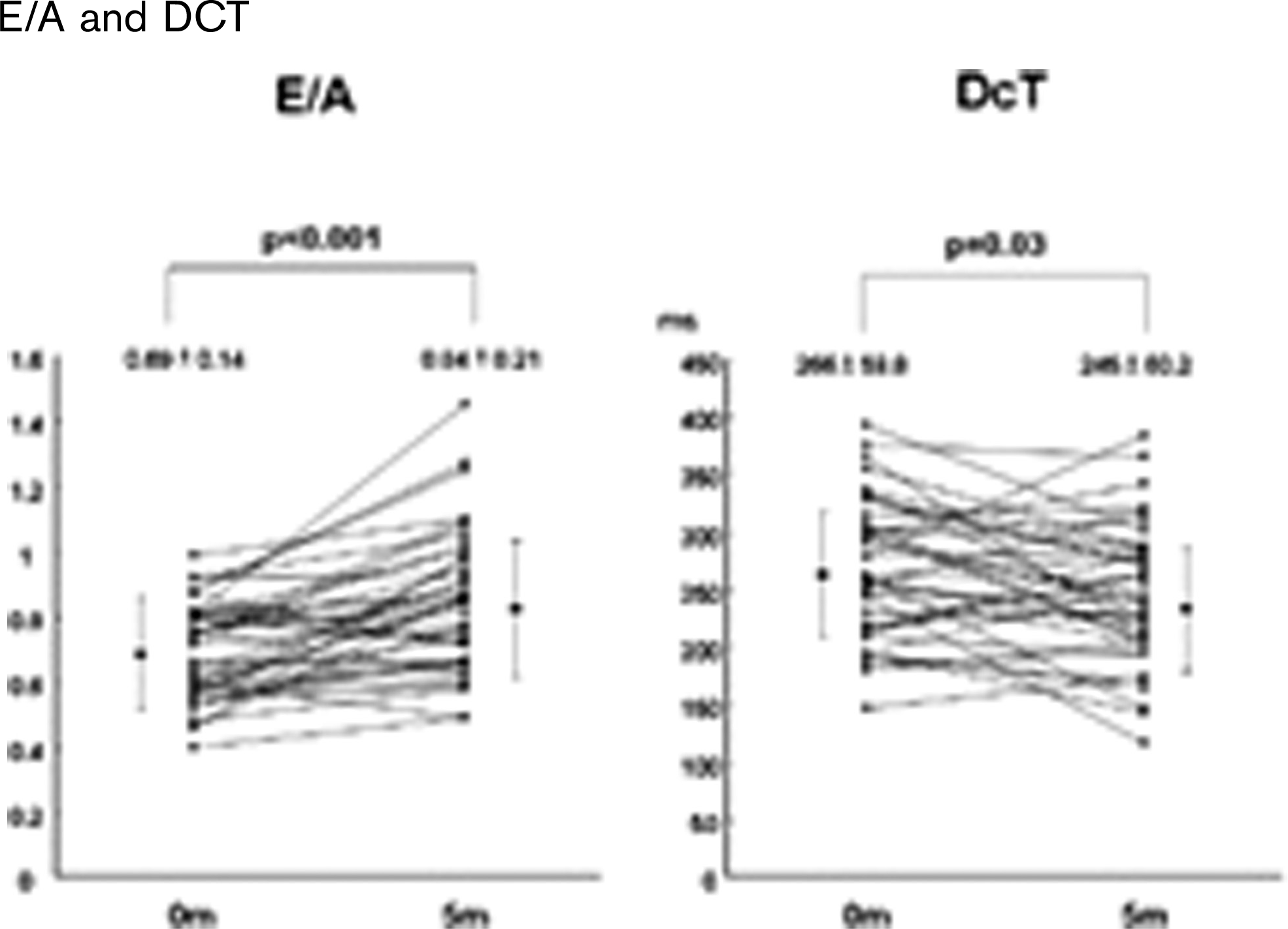
Methods: Forty patients with diastolic dysfunction (abnormal relaxation pattern) and without systolic dysfunction (ejection fraction>45%) were studied. Cardiopulmonary exercise testing and echocardiographic measurements (ejection fraction, left atrial diameter, transmitral flow velocity, tissue doppler imaging) were performed at baseline and after 5 months follow-up of cardiac rehabilitation.
Results: The patients' diagnoses were 9 myocardial infarctions and 31 angina pectoris. There was no event in any patients during the follow-up period. Peak VO2 (p>0.001), AT (p>0.001), peak O2 pulse (p>0.001), early/atrial (E/A) mitral flow ratio (p>0.001), and mitral annular velocity: E' (p>0.001) were significantly increased and deceleration time (p>0.05) was significantly decreased after cardiac rehabilitation. The change in E/A ratio was correlated with changes in peak VO2 (r=0.33, p>0.05) and slope of VE/VCO2 (r=-0.41, p>0.01).
Conclusion: In patients with coronary heart disease, cardiac rehabilitation improves left ventricular dysfunction. Amelioration of exercise tolerance may, in part, be attributed to this improved left ventricular diastolic dysfunction.
E/A and DCT
490 Implementation of a screening program for obstructive sleep apnea in phase II cardiac rehabilitation: feasibility and results
Y Korenfeld; FS Kuniyoshi; P Kayembe; VK Somers; R Thomas; RW Squires; SM Caples; L Braaten; F Lopez-Jimenez
Mayo Clinic Division of Cardiovascular Division, Rochester, United States of America
Background: Obstructive sleep apnea (OSA) has been recognized as a risk factor for cardiovascular disease and mortality. OSA is generally underdiagnosed and untreated. The aim of this study was to determine the feasibility and efficacy of implementing a screening program for OSA in phase II cardiac rehabilitation and to estimate the risk for OSA in this population.
Methods: From the 535 patients enrolled in phase II cardiac rehab from June 1, 2005 to August 31, 2007, we screened 376 (70%) patients for OSA risk using the Berlin questionnaire. From those, we excluded 18 who denied access to use their medical record for research, 16 who had already been diagnosed with OSA and 23 with incomplete data. We report the results from the reminder 319 patients who fulfilled inclusion criteria for this analysis and were classified as low vs. high risk for OSA. Patients considered at high risk for OSA were referred for either overnight oximetry or to a sleep specialist. We assessed the yield and feasibility of a screening program to detect patients at high risk for OSA, patient compliance with referral to a Sleep Clinic and the percentage of patients ultimately diagnosed with OSA with polysomnography.
Results: Mean patient age was 63±12 years, and mean BMI was 29±66 kg/m2. 70% were male, 20% had diabetes, 65% hypertension and 58% had experienced a recent myocardial infarction. Two hundred patients (62%) had a high risk for OSA based on the questionnaire. Of these, 151 (75%) were referred for further evaluation, and 14% could not be referred because they prematurely discontinued participation in cardiac rehabilitation. Only 106 (70%) patients referred for further OSA evaluation actually followed through and attended the evaluation, with 29 (27%) undergoing an overnight polysomnography and 73 (69%) undergoing an overnight oximetry first, followed by polysomnography if needed. Out of the 106 patients who underwent an OSA evaluation, 41 (39%) were found to have OSA with an apnea-hypopnea index=5.
Conclusion: Implementation of a simple screening program for OSA in phase II cardiac rehabilitation is feasible with minimal incremental resources. Screening for OSA in this setting is justified given the high prevalence of patients at risk for OSA. A significant percent of patients at risk for OSA decline further evaluation, suggesting that their perceived risk for OSA and its consequences may be low.
491 Changing patterns of chronic heart failure treatment in British primary care
RW Morris1; SL Hardoon1; M O'flaherty2; I Petersen1; A Islam1; PH Whincup3; S Capewell3
1University College London Primary Care & Population Sciences, London, United Kingdom; 2University of Liverpool, Liverpool, United Kingdom; 3St George's University of London, London, United Kingdom
Purpose: Over 10 million people in European countries suffer from heart failure. Recommendations and treatment guidelines have been produced by the European Society of Cardiology, but little is known about the extent to which these are followed. We used data from a British primary care database (THIN: The Health Improvement Network), including over 300 general practices, to examine patterns of treatment for patients with heart failure from 1991 to 2005. Of particular interest was increased prescribing for evidence-based therapies, including spironolactone following the RALES trial published in 1999.
Methods: Patients with diagnostic Read codes for heart failure were followed for use of various treatments prescribed by their general practitioners. Rates of treatment usage during the year following diagnosis were calculated for loop diuretics, aldosterone blockers (including spironalactone), beta blockers, angiotensin converting enzyme inhibitors (ACEIs) and angiotensin II blockers. Rates were compared according to time period (1991-9 versus 2000-5), age (under 75 years vs 75+), sex, and whether a diagnosis of myocardial infarction (MI) was also recorded.
Results: 29,135 subjects had a diagnosis of heart failure over the whole period. Usage of all drugs increased over the period from 1991 to 2005, from 62% to 79% for loop diuretics, from 41% to 62% for ACEIs, from 10% to 29% for beta blockers, from 6% to 17% for aldosterone blockers, and from 2% to 11% for angiotensin II blockers. All therapies were more commonly prescribed for subjects with previous myocardial infarction, than for those without. All therapies (except angiotensin 2 inhibitors) were more commonly prescribed among men than women, and all therapies (except loop diuretics) were more commonly prescribed for patients aged under 75 years. For example, the odds ratio for aldosterone blocker treatment was 0.86 (95%CI 0.79–0.92) for women compared with men, 0.81 (0.76–0.88) for subjects aged 75 or over compared with those aged under 75, 1.28 (95%CI 1.17–1.39) for those with previous MI compared with those without, and 3.08 (95%CI 2.81–3.37) for those presenting from 2000 onwards, compared with those presenting earlier.
Discussion: Substantial increases have occurred in several evidence-based therapies for heart failure in primary care settings in the UK between 1991 and 2005. However all patients groups remain under-treated, in particular women, older subjects, and those with no history of myocardial infarction.
492 Early diastolic filling pattern determined left ventricular dysfunction and remodeling in patients six month after first myocardial infarction
V Celic1; M Dekleva1; M Colic2; J Suzic3; N Radivojevic1; N Kostic3; Z Caparevic3
1University Clinical Centre Dr Dragisa Misovic Department of echocardiography, Belgrade, Serbia; 2Institut for Cardiovascular Diseases Dedinje Invasive cardiology, Belgrade, Serbia; 3Belgrade, Serbia
Background: Different courses of left ventricle (LV) remodeling after first myocardial infarction (MI) are followed with various aspect of LV dysfunction. Two dimensional Doppler echocardiography and tissue Doppler imaging (TDI) are well established methods for the assessment of systolic and diastolic function. Serial clinical studies indicate that velocity propagation of early diastole (Vp), independent of loading conditions, facilitates accurate diastole assessment. But role of Vp in remodeling process and prognostic value for LV systolic dysfunction after MI are not already well known. Aim of this study were to determine the ability of Vp to predict severe permanent LV remodeling and dysfunction six months after first MI.
Methods: Two dimensional Doppler echocardiography with Color M-mode Echocardiography was performed within first week of hospitalization, and after one, three and six months in 77 consecutive patients with first MI. Patients were divided into group A with mild (N=52) and group B with severe LV remodeling (N=25).
Results: Optimal cut of value of Vp ≤30 cm/sec could identify patients at high risk of severe remodeling after MI (p=0,04) and also predct occurance of severe diastolic dysfunction in both groups of postinfartion patients (p=0,04). Significant correlation was found between severity of LV remodeling and systolic dysfunction after six months follow up (p=0.005). Therefore ≤25 cm/sec could also predict systolic dysfunction in group B (p=0,02). Early peak filling velocity divided by Vp (E/Vp) >2 had a significant predictive value for development of systolic dysfunction (sensitivity 64%; p=0,002) and moderate or severe diastolic dysfunction (sensitivity 66%; p=0,002) in both groups over six months following MI.
Conclusions: Flow propagation velocity after MI is useful and predictive, superior to other Doppler measurements, for severe early and late LV remodeling. Progressive decrease of Vp is valuable tool for prediction of systolic heart failure in patients with severe remodeling after MI. Changing of Vp and E/Vp during LV remodeling could indicate the course of diastolic dysfunction. Slope of early propagation of blood into the LV is strong predictor not only for diastolic dysfunction but for severe LV remodeling and systolic dysfunction in patients after MI.
493 Evaluation of exercise tolerance and quality of life in patients treated with cardiac resynchronisation therapy
E Smolis-Bak; M Wojcicka; T Chwyczko; I Kowalik; B Kazimierska; R Dabrowski; H Szwed
Institute of Cardiology II Department of Coronary Artery Disease, Warsaw, Poland
Baseline: Cardiac resynchronisation therapy (CRT) gains growing importance in treatment of patients with severe congestive heart failure.
Purpose: Evaluation of exercise tolerance and quality of life of patients treated with CRT.
Methods: We investigated 24 patients after successful CRT implantation: 8 women and 16 men aged 34–75 years (av. 62,3±9,5). All patients underwent complex rehabilitation during hospitalization after CRT. Before and 6 months after the procedure we performed cardiopulmonary exercise test to evaluate patients' exercise tolerance. All subjects completed Nottingham Health Profile (NHP) quality of life questionnaire. We analized: (1) oxygen uptake - VO2 (ml/kg/min), (2) quality of life aspects: values of energy (E), pain (P), physical capability (PC), emotional reactions (ER), sleep disorders (SD), social alienation (SA), employment possibilities (EP), homework (HW), social life (SL), family life (FL), sexual activity (SA), hobby (H) and freetime (FT).
Results: After 6 months after CRT implantation patients performed better in CPX achieving higher VO2: (11,8±3,5 before vs 15,4±3,6 after CRT, p>0,001), following quality of life aspects have improved, respectively: E (2,9±0,3 vs 2,0±1,2, p>0,002), PC (4,3±2,3 vs 3,0±2,0; p>0,005), ER (5,2±1,8 vs 3,7 ±2,6; p>0,01). We did not observe any statistical significance in number of patients with problems in EP (46% vs 46%), HW (67% vs 67%), SL (58%vs50%), FL (33% vs 21%), SA (54% vs 71%), H (42% vs 42%) and FT (50% vs 54%).
Conclusion: (1) CRT implantation improves exercise tolerance. (2) CRT improves some aspects of quality of life (E, AL, ER) (3) Further improvement in exercise tolerance and other aspects of quality of life after CRT requires particular care of patient from physicians, physioterapists and psychologists side.
494 Exaggerated peripheral chemoreflex response in heart failure with inspiratory muscle weakness
JP Ribeiro; CC Callegaro; FL Schneider; ENS Pires; JV Silveira; L Marini; D Martinez
Hospital De Clinicas De Porto Alegre Cardiology Division, Porto Alegre, Brazil
Introduction: The peripheral chemoreflex is involved in the genesis of abnormal breathing patterns in patients with chronic heart failure (CHF). We have previously shown that inspiratory muscle training improves the ventilatory response to exercise in CHF and inspiratory muscle weakness, however it is not known if inspiratory muscle strength influences peripheral chemoreflex responsiveness.
Objective: To test the hypothesis that patients with CHF and inspiratory muscle weakness may present abnormal peripheral chemoreflex responsiveness.
Methods: We studied 7 patients with CHF and inspiratory muscle weakness (maximal inspiratory pressure >70% of predicted for age and sex) and 5 with normal inspiratory muscle strength, but with similar age and functional capacity. Peripheral chemoreflex was evaluated by single-breath CO2 test, in which subjects inspired 13% CO2 during a single breath (mean±SD coefficient of variation for different days 13±11%), with the measurement of ventilation as well as end-tidal partial pressure of CO2 response in the subsequent 20 seconds.
Results: As by protocol, patients with normal inspiratory muscle strength showed a greater maximal inspiratory pressure (114±7 cmH2O) than patients with inspiratory muscle weakness (64±6 cmH2O). Peak oxygen consumption was not significantly different in patients with (23±5 ml/kg.min) and without inspiratory muscle weakness (19±3 ml/kg.min). Peripheral chemoreflex response to single-breath CO2 test was significantly greater in patients with inspiratory muscle weakness (0.11±0.02 l/min. Torr) than those with normal inspiratory muscle strength (0.07±0.02 l.min/Torr-). Peripheral chemoreflex response was inversely correlated with maximal inspiratory muscle pressure (r=-0.60, p>0.05).
Conclusion: Inspiratory muscle weakness contributes to increased peripheral chemoreflex response in heart failure patients.
495 Correlation between shortage, functional capacity and quality of life in patients with ischemic cardiopathy and variables with the highest value to mesure functionality
M Parra; F Ortun; A Aunon; A Segura; I Cote; N Caparos; R Figuera; M Martin
Hospital Mutua de Terrassa Rehabilitation, Terrassa, Spain
Purpose: Finding the correlation between variables used to evaluate patients suffering from ischemic cardiopathy (IC), and detection of relevant variables when measuring their functional capacity (FC).
Methods: samples from IC patients assessed in the rehabilitation department between June 2006 and October 2007 to enter a training program. Chosen variables were: ejection fraction (EF), functional questionnaires [DASI- reduced version (DASIr) and Veterans Specific Activity Questionnaire (VSAQ)], exercise tests [six-minute walk test (6MWT)] and ergometry with gas analysis (EGA) and Health Related Quality of Life (HRQoL) questionnaires [Seattle Angina Questionnaire (SAQ), Velasco- Del Barrio (VB)]. NYHA based on VO2 in anaerobic threshold (AT) classification was applied to analyse the capacity of variables to differentiate between clinical functionality levels.
Statistics: Bivariate correlation and ANOVA.
Results: 68 patient samples, 94% of those maleswith an average age of 58 years. A strong correlation (p>0.01) has been found between the following variables:
- Age, risk, VO2 peak, Anaerobic Threshold time (ATt), 6MWT.
A weak correlation (p>0.05) appears between the following variables:
- EF, Age, AT, exercise time in EGA (tEGA).
- VSAQ, VO2 in AT.
- BMI, AP, phSAQ, tEGA, WT6m.
Variables with differences found between the NYHA levels are DASIr (p=0.001), VO2 peak, ATt, pulse O2 (PO2), tEGA and 6MWT (all p>0.001).
Conclusion: - EF shows a weak correlation with functionality and no correlation with HRQoL.
- DASIr and mVB reflect functional capacity better than VSAQ and phSAQ, respectively.
- It is important to point out that BMI and AG show a correlation with functionality and HRQoL.
- It is important to point out that VB and SAQ show no correlation with functional capacity variables.
- DASI, AT, VO2 peak, PO2, tEGA and WT6m have been selected as the election parameters to measure the functional capacity.
496 Dyspnea in cardiac patients: role of clinical features and systolic and diastolic function
IP Clements; DO Hodge; CG Scott
Mayo Clinic Cardiology, Rochester, United States of America
Background: Dyspnea is a common symptom in patients with cardiac disease. This study was undertaken to define the clinical and hemodynamic features associated with dyspnea.
Methods: Clinical and hemodynamic parameters, including left ventricular (LV) end-diastolic and end-systolic volumes (ml/m2), ejection fraction (EF) and early LV peak filling rate (PFR, ml/m2/s) were assessed in 778 cardiac patients (aged at least 45 years) undergoing resting equilibrium radionuclide angiocardiography (ERNA). Two groups of patients were analyzed; 404 patients with LVEF >0.50 and 374 patients with LVEF >0.50.
Results: When LVEF >0.50, 26% of patients had dyspnea and the presence compared to absence of dyspnea was associated with few clinical correlates; prior myocardial infarction and revascularization were less likely (p=0.03), LV end-diastolic (82±35 vs 93±41) and end-systolic (33±17 vs 38±19) volumes were smaller (p=0.003) but LVEF (0.63±0.10 vs 0.62±0.01) and PFR (221±131 vs 243±130) were similar as were the incidences of delayed, normal and restrictive filling (47%, 46% and 8% vs 41%, 49% and 10% respectively). When LVEF >0.50, 34% of patients had dyspnea (p=0.01, LVEF >0.50 vs LVEF >0.50) and presence compared to absence of dyspnea was associated with less frequent prior myocardial infarction (p=0.0002) and revascularization (p=0.01) and more frequent valve disease (p=0.002) and cardiomyopathy (p>0.0001); LV end-diastolic (173±93 vs 134±66, p>0.0001), end-systolic (127±84 vs 87±56) volumes and PFR (273± 149 vs 214 ±97, p>0.0001) were greater and LVEF (0.29±0.11 vs 0.37±0.09, p>0.0001) was smaller and the incidence of delayed filling decreased, normal filling was unchanged and restrictive filling tripled (36%, 47% and 17% vs 51%, 43% and 6% respectively, p=0.0006). Logistic regression analysis showed that LVEF, PFR and volumes rather than clinical variables predicted dyspnea when LVEF >0.50; when LVEF >0.50 dyspnea was independent of all the recorded variables.
Conclusion: Dyspnea was associated with LV systolic and diastolic dysfunction when LVEF >0.50; whereas when LVEF >0.50 dyspnea may be caused by factors other than LV systolic and diastolic dysfunction.
497 The hypercapnic ventilatory response predicts poor survival in patients with severe heart failure
H Tsurugaya; H Adachi; J Murakami; S Oshima; K Taniguchi
Gunma Prefectural Cardiovascular Center Dep. of Cardiology, Maebashi, Gunma, Japan
Background: Recently, it was reported that the VE-VCO⊂2 slope is a marker of poor prognosis for patients with moderate to severe chronic heart failure (CHF). However, the mechanisms of increased exercise ventilation have not yet been still clear, but hyper responsivity of chemoreceptors and ergoreceptors may take part in the mechanism. For this reason, in some studies, a mutual relationship between chemoreceptors and VE-VCO⊂2 slope was clarified, and it was investigated whether chemosensitivity become the predictor of poor prognosis in patients with severe heart failure. However, in most of papers, hypoxic ventilatory response was used as an indicator.
Purpose: We investigated whether the hypercapnic ventilatory response (HCVR) predicts cardiac events in patients with CHF using Kaplan-Meier analysis.
Methods: We monitored fifty-one patients with CHF (mean age 63±9 years, left ventricular ejection fraction (LVEF) was 30.2±8.2). HCVR was assessed using rebreathing of carbon dioxide. Subjects rebreathed through a 6-liter bag containing a hypercapnic gas mixture to induce the hyperpnea responses to hypercapnia activation (7% CO⊂2/ 93% O⊂2). We defined HCVR was expressed in liters per minute per mmHg of CO2 (L/min/mmHg). Subjects were divided into two groups according to HCVR (Group L; >3 L>min−1 >mmHg−1, Group H;>3). BNP, peak-VO2 and VE-VCO2 slope were evaluated and the cardiac events were followed for sixteen months.
Results: Twenty-two cardiac events (5 deaths and 18 re-hospitalization) occurred within the observation period. Group H had significantly lower cardiac event-free rate (33.3%) than Group L (79.2%, p>0.005). Peak VO2 in Group H (16.3±3.6ml>min−1>kg−1) was significantly (p>0.05) lower than that of Group L (18.8±4.6). VE-VCO⊂2 slope was higher (p>0.01) in Group H (38.4±8.6) as compared with that in Group L (29.4±4.4). BNP of Group H (286±246) was significantly (p>0.05) higher than that of Group L (104±115).
Conclusion: We conclude that the hypercapnic ventilatory response is associated with lower exercise tolerance in CHF patients. HCVR can be a prognostic indicator of cardiac events in CHF.
498 Cardiorespiratory responses during maximal graded exercise in obese subjects
LA Riani Costa
DML Prado
A Murad Neto
Diagnosticos da America Cardiology, Sao Paulo, Brazil
Purpose: Excessive body fat content profoundly influences on aerobic fitness. Moreover, an increase in body fat produces direct effects on components of oxygen delivery chain. For instance, obese subjects (OS) typically demonstrate greater resting cardiac output, stroke volume and expanded plasma volume. The aim oh this study was to evaluate whether cardiorespiratory responses during maximal graded exercise are different in OS comparing to lean subjects (LS).
Methods: Thirty eight male subjects were divided into 2 groups: 18 OS (40.0±2.3 years, 102.0±3.44kg, 175.4±1.8 cm, BMI 32.4±0.55 kg/m2) and 20 LS (36.2±2.3 years, 69.7±2.33kg, 176.7±2.8 cm, BMI 22.6±0.55kg/m2) and performed a ramp progressive exercise test until exhaustion on treadmill. The cardiorespiratory responses during graded exercise test were analyzed between two groups using two-way (group by time) analysis of variance. In the case of significance, Sheffé's post-hoc comparison was used to determine differences between groups. A P value of >0.05 was considered statistically significant.
Results: Data are presented in the table as mean±SE.
Conclusion: OS have greater values for absolute cardiorespiratory variables than LS. However, for relative cardiorespiratory variables, OS showed lower values. In summary, these findings suggest that elevated body mass produces higher absolute metabolic activity, but excess fat body weight reduces the positive impact in exercise performance and cardiovascular health.
Rest
AT
RCP
Peak
Interaction
HR (bpm)
OS
65,9±2,5
127,7±3,8
159,9±4,7
178,2 ±3,7
NS
LS
64,7±2,2
130,6 ±3,0
166,8 ±2,1
184,4±2,0
SBP (mmHg)
OS
123,6
152,5
177,5
189,7
NS
±2,9
±3,9
±5,8∗
±5,8
LS
113,3 ±2,9
145,0 ±3,8
161,5 ±3,7
175,5±4,0
O2pulse (mL/bpm)
OS
5,4±0,3
16,8±0,7∗
19,4±0,9∗
19,3±0,9∗
>0,05
LS
3,8±0,2
14,6±0,6
15,8±0,5
15,7±0,6
VO2 (L min−1)
OS
0,3±0,0
2,1±0,1
3,1±0,1∗
3,4±0,2∗
>0,05
LS
0,2±0,0
1,9±0,1
2,6±0,1
2,9±0,1
VO2 (mL kg−1.min−1)
OS
3,4±0,2
21,5±1,1∗
30,5±1,5∗
33,7±1,3∗
>0,05
LS
3,5±0,1
27,5±1,2
38,1±1,1
41,8±1,3
NS, not significant; AT, anaerobic threshold; RCP, respiratory compensation point; ∗different from LS (P>0.05).
499 Value of non ST-segment exercise test variables in patients with diabetes mellitus
Purpose: Recent research based on large patients population has demonstrated that there are much stronger ergometric predictors of cardiovascular events than ST-segments.
Studies focused on non-ST segment variables in exercise testing (exercise capacity, chronotropic response, heart rate recovery) in diabetics are lacking.
Methods: We compared exercise time, chronotropic and blood pressure response in 1172 patients undergoing exercise testing with Bruce protocol (mean age: 60.72±11.30; males 61.60%). 83 (7%) were diabetics; mean age: 64.37±8.44 vs 60.44±11.44 of non diabetic patients; males: 56 (67.47%) vs 665 (61.06%). Diagnostic tests were 48 (58%) in diabetics (vs 686; 63%). BMI was 28.87±3.94 in diabetics (vs 27.13 ±5.14).
Results: Features of exercise testing parameters in diabetic patients (vs non diabetics) are listed in the Table.
Conclusion: Preliminary results of this study highlight that non-ST variables (exercise capacity, chronotropic response, heart rate and blood pressure recovery) are significantly different in diabetic compared to non diabetic patients.
Further studies would be useful to evaluate the prognostic significance of these differences.
Comparison of exercise test parameters
Diabetics
Normals
P
83 (7%)
1089 (93%)
EXERCISE TIME (min)
4.84±2.49
5.96±2.60
0.00016
HR MAX (bpm)
124.40±21.14
130.73±21.83
0.01
1st min HR rec (bpm)
106.41±20.06
109.59±20.74
ns
HR decr 1st min rec (beats)
17.98±10.05
21.15±9.76
0.005
SBP MAX (mmHg)
174.16±19.55
173.60±22.64
ns
SBP 3rd min rec (mmHg)
153.13±19.01
1477±19.42
0.014
SBP 3rd min rec/ SBP MAX (%)
88.47±10.63
85.65±9.88
0.013
500 64-row Multi-Detector Computed Tomography(MDCT) in assessment of right ventricle remodeling in patients with atrial fibrillation(AF) compared with parameters obtained in Cardio-Pulmonary Exercise Test
M Zagrodzka1; S Szmit2; L Szumowski3; E Szufladowicz1; G Opolski2; F Walczak1
1WIM Radiology, Warsaw, Poland; 2Warsaw Medical University Cardiology, Warsaw, Poland; 3Institute of Cardiology, Anin, Poland
Background: There is no data assessing remodeling of the right ventricle (RV) in patients with atrial fibrillation (AF), and cardiovascular parameters reflecting their clinical condition.
Aim: The aim of the study was to compare right and left heart morphology with cardio-pulmonary exercise test (CPET) parameters in patients with AF before RF ablation.
Material and methods: 20 patients (49±14 y) before RF ablation due to AF had 64-VCT performed before ablation to assess right and left ventricle morphology and function and pulmonary veins. Results were correlated with clinical signs of heart failure established in CPET.
Results: 17 patients had RV>LV, 6 patients had RAV>LAV. Results of cardiopulmonary parameter correlations are presented in Table 1. In Mann-Whitney U test: 1. Patients with LV>130ml had significantly higher PetCO2 (p=0.03) and significantly lower VE/VCO2 (p=0.0475) 2. Patients with RV>167ml had significantly higher VO2peak (p=0.003), VEmax (p=0.03), VO2AT (p=0.0026), PetCO2 (p=0.0015) and significantly lower VE/VCO2 (p=0.0002), VE/VO2 (p=0.003), PetO2 (p=0.03) 3. Patients with VO2AT>11ml/kg/min. had significantly smaller LV (p=0.048) and RV (p=0.0099) 4. Patients with impaired ventilation with regard to perfusion (VE/VCO2>29) had significantly smaller area LIV (p=0.035), smaller LV (p=0.003) and RV (p=0.0001) 5. Patients with impaired CO2 diffusion PetCO2>40 mmHg had significantly smaller RV (p=0.01).
Conclusion: 1. Right ventricular volume correlates with all cardiopulmonary sufficiency parameters stronger than LV. 2. Cross section area of left inferior pulmonary vein (LIV) seems to be important for pulmonary circulation in patients with AF. 3. Patients with AF before RF ablation, without increase in ventricular volumes have significantly worse exercise tolerance and dysfunction of pulmonary circulation.
501 Anaemia accentuates the phenomenon of post-exercise hypotension
O Georgopoulou; M Koskolou; G Megas; S Athanasopoulos; N Geladas; National & Kapodistrian University of Athens, Athens, Greece
Purpose: Although post-exercise hypotension has been studied extensively, it is not known how this phenomenon is affected by anaemia, since enhanced vasodilation in the periphery is expected in this condition due to the suggested vasodilatory effect of low hemoglobin concentration [(Hb)]. The purpose of this study was to explore how differences in (Hb) affect post-exercise hypotension and the associated cardiovascular response.
Methods: Seven women (22.6±3 yrs) with normal values of hemoglobin and hematocrit [(Hb)=14±0.4 g/dl, and Hct=41.7±1.0%] and seven women (24.4±1.6 yrs) with mild anaemia [(Hb)=11.3±0.6 g/dl and Hct=35.3±1.4%] participated in the study. Resting values were taken for 30 min in supine position. Afterwards the participants performed exercise on a cycle ergometer at 70% of VO2max for 30 min, followed by 60 min of supine recovery. Arterial pressure [systolic (SP), diastolic (DP), mean (MAP)], total peripheral resistance (TPR), cardiac output (CO), stroke volume (SV) and heart rate (HR) were monitored using a photo-plethysmographic device.
Results: Upon exercise cessation, systolic pressure dropped (p>0.05) and remained lower than resting values for 25 min in both groups. Mean arterial pressure was lower than pre-exercise baseline values (p>0.01) for the first 15 min of recovery period only in anaemic women, while DP was lower only for the first 5 min of recovery in the same group. TPR was lower from rest values till the 45th min and 20th min of recovery in anaemic and non-anaemic women, respectively (p>0.05). From the 10th min of recovery onwards the values of TPR were lower in anaemic than non-anaemic women (p>0.01). CO was higher than pre-exercise values the first 5 minutes of recovery in both groups (p>0.01) but was different between groups from the 20th till the 60th minute of recovery. The higher CO in anaemic compared to non-anaemic women (p>0.01) was due to higher SV, since postexercise HR was not different between groups.
Conclusion: These findings suggest that the magnitude of post-exercise hypotension is affected by hemoglobin concentration. It is more profound in mild anaemic, as a result of a greater reduction in TPR, than in non-anaemic women. The lower TPR in the anaemic group insinuates that there is a greater vasodilation in this group persisting after exercise, which cannot be completely offset by the higher CO, leading to an enhanced post-exercise hypotension.
502 Impaired oxygen kinetics in thalassemic patients
I Vasileiadis1; P Roditis1; ST Dimopoulos1; O Papazachou1; D Sakellariou1; A Tasoulis1; V Ladis2; A Aessopos2; G Pangalis2; S Nanas1
1Cardiopulmonary Rehabilitation Center, Evgenidio Hospital, University of Athens, Greece; 2Thalassemia Unit, Department of Pediatrics, University of Athens, Greece
Background: It has been shown reduced exercise capacity in patients with β-thalassemia major (TM). The disease affects all the systems responsible for blood gas exchange during exercise. Precise pathophy-siological mechanisms for this exercise intolerance have not been definitely clarified.
Aim of the study: To assess exercise capacity in patients with β-thalassemia major and no clinical or echocardiographic evidence of cardiac disease and estimate oxygen uptake kinetics during submaximal, constant work-load exercise, to explore possible pathophysiology of the expected limited patients' response.
Methods: The study consisted of 12 patients (7 males/5 females) and 10 healthy controls (6 males/4 females). Patients had no clinical evidence of cardiovascular or respiratory disease and normal echocardiographic indices and were under intensive transfusion treatment to maintain hemoglobin level> 10 g/dl. Patients and controls performed incremental, symptom limited CPET on a cycle ergometer with evaluation, breath by breath, of oxygen uptake, carbon dioxide output and ventilation. Also, they performed constant work-load exercise test; the load was set at 70% of the value of the WR achieved at the anaerobic threshold. Phase 1 of on-transient oxygen kinetics was evaluated by time from start of exercise until the sharp decline of respiratory exchange ratio and phase 2 by the time constant of the response from the end of phase 1 until steady-state.
Results: Exercise capacity was markedly reduced in TM patients comparing to controls, as assessed by peak oxygen uptake (22.28±7.37 vs 28.76±4.77 ml/kg/min, p>0.05) and anaerobic threshold (13.14±2.71 vs 17.42±2.55 ml/kg/min, p=0.002). There was no difference in oxygen cost of work at peak exercise (11.73±1.88 vs 12.58±1.94 ml/min/watt, p=ns) suggesting normal oxygen availability for the required energy production. Ventilatory response to exercise was normal. Interestingly, cardiodynamic phase at the onset of submaximal, constant work-load exercise was the same in TM patients and controls (24.62±7.29 vs 23.62±9.55 sec, p=ns) while time constant of phase 2 in patients was significantly prolonged (42.81±11.98 vs 32.59±8.77 sec, p>0.05).
Conclusion: In TM patients, it is not cardiac function or other reason affecting oxygen availability, the limiting factor for the reduced exercise capacity but rather “defective” muscle intracellular, metabolic control mechanisms.
503 Fine motor abilities in children with congenital heart diseases (CHD) compared to healthy peers
S Schmitz1; S Dordel2; D Bott2; S Schickendantz3; N Sreeram1; K Brockmeier1; B Bjarnason-Wehrens3
1Institute for Cardiology and Sports Medicine German Sport University, Cologne, Germany; 2Inst for School Sports & School Development German Sport University, Cologne, Germany; 3Department of Pediatric Cardiology Cologne University Hospital, Cologne, Germany
Purpose: The aim of this study was to evaluate fine motor development in children with congenital heart diseases (CHD) compared to healthy peers.
Methods: A sample of 77 children (41 boys, 36 girls, mean age 8.1±1.2 years), representing the entire spectrum of CHD, was compared to a control group (CG) of 147 healthy children (77 boys, 70 girls, mean age 8,2±1.1 years). The MLS - Motor Performance Series, was used to measure fine motor abilities. The following 5 factors of fine motor abilities were analysed: aiming, hand unrest/tremor, precision of armhand movements, rate of arm and hand movements, wrist-finger speed. For statistical analysis, one-factorial and multiple variance analyses were used.
Results: The CHD-children-group scored lower by all measured factors compared to healthy peers. Trey scored significantly lower by the factor hand unrest/tremor (p=0.003) and the factor precision of arm-hand movements (p=0.020) compared to the CG. CHD-Children in status after open heart surgery (n=40) scored lower in the factor hand unrest/ tremor (p= 0,051), those who didn't require open heart surgery (n=37) scored lower in the factor hand unrest/tremor (p= 0.061) as well as in the factor precision of arm-hand movements (p=0.054) compared to CG. Depending on the presence and/or degree of residual sequelae the CHD-children were divided into two groups (A: no or mild residual sequelae (n=45), B: significant residual sequelae (n=26)). Children with significant residual sequelae scored significant lower in the factor precision of arm-hand movements (p=0.050) than healthy peers. Conclusion: These results demonstrate deficits in the fine motor development of children with CHD compared to healthy peers. This was especially seen for the fine motor abilities hand unrest/ tremor and precision of arm-hand movements. The Results indicate that the status after open heart surgery, as well as the presence and/or degree of residual sequelae may influence fine motor development of children with congenital heart disease. Preoperative persistent low cardiac output, acidosis, and/or hypoxia as well as the duration of hypothermic circulatory arrest during surgery may contribute to this.
504 Impact of different levels of school exercise on fitness, motoric skills and body mass index in children
C Walther1; K Drechsler1; S Fikenzer2; L Gaede1; M Sonnabend1; J Gnann1; M Busse2; G Schuler1
1University of Leipzig - Heart Center Cardiology, Leipzig, Germany; 2University of Leipzig - Institute of Sports M, Leipzig, Germany
Background: The prevalence of childhood obesity is continuously increasing in western countries counting for about 25% of school children. A major contributing factor is the decline of physical activity which can be observed in school children of every age. The importance of physical activity for prevention of cardiovascular disease is closely linked to cardiovascular health, fitness level and psychosocial behaviour. Aim of this trial is to teach a health-conscious life-style, to improve physical activity and to reduce obesity in school children with additional exercise lessons.
Methods: Eleven 6th-grade classes (277 children) of three different high schools in Leipzig were randomized to an intervention group (IG) with daily school exercise lessons for 1 year (1Y) and a control group (CG) with regular school sports (2 hours per week). Three classes (45 children) of a high school with special focus on competitive sports and physical education served as reference group (PE). At baseline and after 1 year the following investigations were performed: bioelectric impedance analysis, treadmill exercise test with spirometry and a standardised questionnaire on sport and leisure behaviour of the children. Motor abilities were determined by a body gross motor development test for children (Koerperkoordinationstest fuer Kinder; KTK).
Results: At begin mean body mass index (BMI) was significantly lower in children of PE (16.8±0.5 kg/cm2) compared to children of IG (18.1 ±0.2 kg/cm2) and CG (18.4±0.3 kg/cm2), however 12% of children in IG and 13% of children in CG had a BMI over the 97th percentile, compared to 2% of children in PE. At the end of one year, children of IG and CG showed a significant improvement of their motor abilities. In addition an improvement of exercise capacity could be observed in IG and CG after 1Y, however maximal oxygen consumption (VO2max) in children of IG was significantly better compared to children of CG (46.8±0.5 ml/min/kg in IG vs. 42.2±0.8 ml/min/kg in CG, p>0.001), but did not reach values of children of PE (56.23±1.2 ml/min/kg, p>0.01).
Conclusion: The results of this trial demonstrate, that already in childhood, regular school exercise lessons have a positive influence on exercise capacity and motor abilities. Therefore, to prevent the negative consequences of physical inactivity and overweight/obesity early intervention to support exercise and movement is recommended.
505 Physical activity estimated in Cardio-Pulmonary Exercise Test (CPET) in patients with WPW pattern in ECG: time for new definition of symptomatic WPW syndrome?
S Szmit1; S Stec2; P Balsam1; M Futyma3; K Dudek1; P Kulakowski3; G Opolski2
1Medical Univeristy of Warsaw 1st Department of Cardiology, Warsaw, Poland; 2Postgraduate Medical School Department of Cardiology, Warsaw, Poland; 3Asclepios Clinic, Rzeszow, Poland
Purpose: The diagnosis of Wolf-Parkinson-White (WPW) syndrome is reserved for patients who have both ventricular pre-excitation and symptoms related paroxysmal tachycardia such as chest pain, dizziness, palpitations, syncope or feeling short of breath.
The aim of the study was to comparison results of Cardio-Pulmonary Exercise Test (CPET) with electrophysiological characteristic in patients with WPW pattern in ECG
Materials: 20 patients (mean age 33years) with recognized in ECG WPW pattern underwent CPET (ZAN 680) on treadmill with Rampe protocol: The organic pulmonary vessels, lung and heart diseases have been excluded in chest X-ray (or Computed Tomography) and in echocardiography.
Results: 1. Patients with intermittent ventricular pre-excitation had significant lower equivalent ventilation for oxygen and end tidal pressure for oxygen (VE/VO2 and PetO2, p>0,05).
2. Patients with SVT in anamnesis had significant lower time and load of exercise, VCO2 production, ventilation (VE) and higher VD/VT (ratio of dead space and tidal volume) (for all p>0,02).
3. Patients with refractory of accessory atrioventricular pathway higher than refractory of physiological pathway had significant lower VT (tidal volume, p=0,0008), VCO2 production and peak oxygen consumption (p>0,005), oxygen consumption at anaerobe threshold (VO2AT, p=0,04), lower time of exercise (p=0,01) and load of exercise (p=0,005) and higher VD/VT (p=0,0038).
4. The significant lowest exercise tolerance in CPET had the patient with septal and inferior locus of accessory atrioventricular pathway and with refractory of accessory atrioventricular pathway higher than refractory of physiological pathway (lowest time and load of exercise, VO2peak, VO2AT, VE, VT, RER=VCO2/VO2, highest VD/VT, p>0,001) - these patients after successful atrioventricular radio-frequency ablation showed significant improvement of exercise tolerance in CPET.
Conclusion: Locus and refractory of accessory atrioventricular pathway and manifest ventricular pre-excitation were related with worse results of Cardio-Pulmonary Exercise Test and could be additional indication for RF ablation in patients with WPW pattern.
506 Heart rate response to incremental maximal exercise is a useful tool in evaluating cardiovascular performance and aerobic capacity
LA Riani Costa1; DML Prado1; RMR Dias2; A Murad Neto1
1Diagnosticos da America Cardiology, Sao Paulo, Brazil; 2University of Sao Paulo Public Health, Sao Paulo, Brazil
Purpose: Functional capacity is related with clinical aspects of cardiovascular health, diagnosing subclinical cardiovascular disturbances and supporting rehabilitation programs. Heart rate (HR) response to exercise is depressed in sedentary and cardiac patients while health and trained people shows higher chronotropic response. The aim of this study was to investigate the exercise elevation in HR as percentual changes related to the basal, correlating with classical markers of cardiovascular health and aerobic capacity.
Methods: 197 subjects without diagnosis of cardiovascular diseases (37.3±11.3 years, BMI 25.5±4.2 Kg/m2) performed a maximal cardiopulmonary test on treadmill. We analyzed HR, oxygen consumption (VO2) and oxygen pulse in rest, ventilatory thresholds (L1 and L2), peak of exercise and recovery. To test the hypothesis that HR response identify different cardiovascular performances, subjects were divided into two groups by the mean chronotropic response to resting HR (178,8%). Variables selected in a whole group analysis with Pearson's correlation test were compared between the groups using Student's t test (p>0,05).
Results: The results are presented in the table as mean±sd.
Conclusion: HR response to exercise as percentual elevation related to the basal is a useful tool in evaluating cardiovascular performance, positively correlated with cardiovascular health and aerobic capacity. Subjects with higher chronotropic response have higher levels of aerobic fitness and work capacity, higher ventricular function and increased vagal tonus in rest and recovery phase.
Variables
HR response >178,8%
HR response >178,8%
p
Resting HR (bpm)
58.8±6.5
75.0±8.8
>0,001
VO2L1 (ml. Kg−1.min−1)
26.6±6.5
21.3±6.4
>0,001
VO2L1 (%max predicted)
61.4±14.6
54.3±15.2
0,001
VO2L2 (ml. Kg−1.min−1)
36.7±6.8
30.0±78
>0,001
VO2L2 (%max predicted)
84.8±16.1
76.2±18.1
0,001
VO2Peak (ml. Kg−1.min−1)
40.4±7.1
33.4±78
>0,001
VO2Peak (%max predicted)
93.3±17.1
84.9±18.1
0,001
Oxygen Pulse (%max pred)
94.2±17.1
85.1±19.4
>0,001
HR decline 2min recovery (bpm)
53.7±10.9
44.4±9.8
>0,001
Maximal Power (watts)
566.1±21 7.4
429.2±183.3
>0,001
507 Arrhythmogenic risk of exercise stress testing
A Malai; R Rosu; D Zdrenghea; E Bogdan; The Rehabilitation Hospital, Cluj-Napoca, Romania
Purpose: Last decades the indication of exercise stress testing (ET) enlarged, being used for diagnosis and evaluation of the majority of cardiovascular patients. In the same period, the prevalence of arrhythmia increased, supporting a reevaluation of the arrhythmogenic risk of exercise stress testing.
Methods: We studied 1110 consecutive ET, indicated for diagnosis or evaluation. There were excluded the subjects with arrhythmias at rest, immediately before ET. There were took into account tachyarrhythmia and conduction disturbances, during and ten minutes after ET and were correlated with cardiovascular risk factors, etiology of cardiovascular disease and LEVF.
Results: We studied, 589 females and 521 males, aged 55,25±9,78 years, with ischemic cardiopathy (64,1%), dilated cardiomiopathy (4,1%), other cardiovascular disease (8,92%), healthy subjects (22,88%). A number of 421 of all p were addressed to ET for diagnostic reason. Arrhythmia were registered during ET in 21,2% of cases and after effort in 13,0% and conduction disturbances during and after ET in 2,2%. Exercise arrhythmia were represented by ventricular premature beats (VPB) in 13%, ventricular tachycardia in 1,1%, supraventricular extra-systoles 6,7% and atrial fibrillation 0,4%. VPB weren't more frequent in ischemic cardiopathy (13,1% vs 12,8%, p=0,14), except old myocardial infarction (24,5% vs 10,7%, p>0,01) and they were registered in 48% of with LVEF >40% (vs 11,7% p with LVEF>40%, p>0,01). The correlation with left ventricular performance was also supported by the high incidence of VPB in dilated cardiomiopathy (71,1%). A correlation was also registered with dyslipidemia (20% vs 8,7%, p>0,01), hypertension (19,7% vs 10,8%, p>0,01), obesity (29,1% vs 9,8%, p>0,01). Post effort, VPB are considered to have an increased arrhythmogenic risk. They were more frequent in p. with ischemic cardiopathy (7% vs 1%, p>0,01), dyslipidemia (19,6% vs 8,1%, p>0,01) hypertension (6% vs 0%). The small percent of with ventricular tachycardia don't offer the possibility of any correlation. For supraventricular extrasystoles, the only correlation was registered with LVEF (25% in patients with LVEF>40% vs 7% in LVEF>40%, p>0,01), suggesting they represent a sign of depressed left ventricular systolic performance and increased mean atrial pressure.
Conclusion: The arrhythmogenic risk of ET is low, being represented mainly by VPB correlated with left ventricular performance, old myocardial infarction and some cardiovascular risk factors. In turn, no cardiac arrhythmic death was registered during exercise stress testing.
508 Significant difference in maximal heart rate in fit and unfit boys
EA Skaug1; AB Johnsen2; U Wisloff2; O Ellingsen2
1Norwegian council of cardiovascular research, Trondheim, Norway; 2Norwegian university of science & technology Sirculation and medical imaging, Trondheim, Norway
Introduction: Previous studies indicate that fit persons have lower maximal heart rate compared to unfit individuals, but the literature is conflicting. The aim of the present study was to determine maximal heart rate in the 25% best fit (highest VO2max/peak) compared to the 25% most unfit (lowest VO2max/peak) from a population of 600 healthy Norwegian adolescents.
Methods: 600 healthy adolescents (278 boys and 322 girls) between 13 and 19 years old were included from a middle school and a neighbouring college in a small city in Norway. Systolic and diastolic blood pressure, weight and height were measured, and all went trough a limited interview with a physician. All included performed a 10 minute warm-up before VO2m/p(VO2max/peak) and maximal heart rate was measured during an individualized treadmill protocol. 277 boys and 312 girls reached VO2m/p.
Results: Mean maximal heart rate was found to be 203±7 for unfit boys, 198±8 for fit boys, 199±8 for unfit girls, and 199±7for fit girls. Mean VO2m/p for unfit boys were 50.0±4.4 ml/kg/min, for fit boys 72.5±4.3 ml/kg/min, for unfit girls 40.2±4.0 ml/kg/min, and for fit girls 58.0±4.3 ml/kg/min. Using the 1-way ANOVA we found the difference in maximal heart rate between unfit and fit boys to be significant (p>0.005) Conclusions: The fit boys had a significant lower maximal heart rate compared to the unfit boys. 61% of the fit boys had a VO2m/p higher than 70 ml/kg/min, and were considered to be athletes (6% had a VO2m/p higher than 80 ml/kg/min). Among the unfit boys we found 42% with VO2m/p lower than 50 ml/kg/min (which in Norway is considered to be the “mean” value for a 20 year old man). 28% of the fit girls had a VO2m/p higher than 60 ml/kg/min, and 36% had a lower than 40 ml/kg/min. So there were overall more homogeneity among the girls, and a greater difference between the two groups of boys compared. This can explain why we did not find a correlation in the girls. Physical exercise or genetic basis may be the reason for the difference we found in the boys, but this is still unclear.
509 Exercise-induced abnormal pulmonary arterial pressure response in young athletes: normal physiology or precursor of endothelial damage?
T Moller1; K Peersen1; PM Fredriksen2; H Holmstrom1; E Thaulow1
1Vestfold Hospital Pediatric Department, Toensberg, Norway; 2Rikshospitalet University Hospital Clinic of Rehabilitation, Oslo, Norway
Introduction: Pulmonary arterial pressure (PAP) is considered to remain nearly unchanged during exercise. Earlier studies have shown an abnormal rise in PAP during exercise in endurance-trained professional athletes.
Methods: A group of 68 healthy volunteers (age 14 to 25 yrs) were studied by cardiopulmonary exercise testing, echocardiography at rest and during supine cycling with target heart rate 160-min. Eight individuals with extremely high (>2 SD) maximal oxygen uptake were defined as highly endurance-trained athletes (ETA). Their data were compared to 16 age- and gender-matched normal trained individuals (NTI).
Results: At rest, right ventricular performance as measured by tricuspid annulus plane systolic excursion (TAPSE) was equal in both groups (mean 23/23). Exercise peak systolic PAP raised above 500 mmHg in 6 of 8 ETA (mean 48, median 55, range 17 to 66) but only in 1 (511 mmHg) of 16 matched NTI (mean 31, median 31). The difference is statistically significant (p=0.008 [−28.8,-4.8]).
Discussion: The mechanism of abnormal PAP elevation in high cardiac output situations may be due to pulmonary blood flow beyond dilative capacity in the pulmonary vascular system. Pressure levels above 355 mmHg are commonly considered to damage pulmonary endothelium and to be a possible precursor of permanent pulmonary hypertension. Young athletes with abnormal PAP response may have high pressure load in their pulmonary vessels several hours a day for years while maintaining their endurance training program.
Conclusion: Non-professional highly endurance-trained individuals show abnormal pulmonary pressure response during exercise. The common definition of normal range in pulmonary arterial pressure may have to be reconsidered.
510 Limited relationship between blood pressure and VO2max in a healthy, adolescent population
S Aspenes; U Wisloff
Faculty of Medicine, NTNU Department of Circulation and Medical Imaging, Trondheim, Norway
Purpose: There exists an inverse relationship between adolescent fitness and CVD risk factors, and prospective studies have demonstrated how adolescent's fitness is inversely associated with adult CVD risk factors. Most studies use an estimate of maximal oxygen uptake (VO2max), and investigations of true VO2max and CVD risk factors is sparse. The purpose of the present study was to determine whether there is a close relationship between blood pressure and VO2max in a healthy adolescent population.
Methods: 612 healthy participants between 13 and 20 years were included from a middle school and a college in Nord-Trøndelag, Norway. Height, weight and blood pressure was measured using standard procedures and VO2max measured during an individualized treadmill protocol. Results: 501 participants reached VO2max. Independent samples t-test revealed a significant difference (p>0.01) in diastolic blood pressure between the lowest and highest female quartile of VO2max. No other differences were found.
Conclusion: Regarding former studies the significant difference in diastolic blood pressure between first and fourth quartile of VO2max is not surprising. However, it is surprising that a similar difference is not evident for any other parameter. It should be noted that the first female quartile is closest to former investigations. There is no reason to believe any systematic bias occurred regarding these elevated VO2max-values. Thus, in a healthy, fit adolescent population there is only a limited relationship between VO2max and blood pressure.
Characteristics and findings
Female
Male
N
251
250
Age
16.7±1.8
16.6±1.9
Height (cm)
166.0±6.1
176.2±9.1
Weight (kg)
57.9±9.0
679±14.6
BMI
21.0±2.8
21.7±3.4
Systolic BP
124±12
133±13
Diastolic BP
78±8
78±9
VO2max
49.6±7.3
61.5±8.9
1. quartile
41.1±3.4
50.2±4.3
4. quartile
59.4±4.3
72.8±4.3
VO2max in mL >kg−1 >min−1.
511 Asynchrony in dilated cardiomyopathy versus ischemic cardiomyopathy: Doppler Tissue Imaging study
A Serag1; A Serag2; S Shalaby2
1Cairo, Egypt; 2Menoufyia university Cardiology, Shebein El Kom, Egypt
Ventricular asynchrony is common in patients with ischemic or non ischemic cardiomyopathy. Accurate assessment of it is of utmost importance to identify patients that will benefit from cardiac resynchronization therapy.
Aim: To assess the utility of (DTI) in detection of ventricular asynchrony in patients with ischemic and non ischemic cardiomyopathy.
Methods: 40 patients with ischemic cardiomyopathy with a mean age of 57±9 years and 29 patients with dilated cardiomyopathy with a mean age of 56±8 years. 15 sex and age matched volunteers as a control group with a mean age of 57±3 years. All groups were examined by DTI to measure the pre-contraction time (from the beginning of QRS to the beginning of systolic S wave), the time to peak (from the beginning of the QRS to the peak of systolic wave S), the time to early diastole (from the QRS to the beginning of the E wave).
Results: Fifteen patients with ischemic cardiomyopathy had significant right coronary lesions, evidenced by coronary angiography. There was a highly significant prolongation of the measured parameters in the myopathic groups than the control group. There was significant prolongation of the time to peak S wave between the lateral and septal wall of the LV in both patients groups (356.7±3 vs. 248.7±3, p>0.0001 and 281.8±3 vs. 207.2±2, p>0.0001 respectively). This means an intraventricular asynchrony in both patients groups. Also, there was significant difference between the lateral wall of the RV and the lateral wall of the LV as regard time to S wave (214.1±2 vs. 323.9±9, p>0.0001) in patients with no significant right coronary affection indicating interventricular asynchrony in those patients. However there was no significant difference between lateral wall of the RV and lateral wall of the LV in patients with right coronary affection (332.1±3 vs. 331.3±5, p>0.05 respectively). There was no significant difference between the time to peak systolic wave of the studied LV segments in patients with wide and narrow QRS in both patients groups.
Conclusion: DTI tracing allows precise assessment of intra and interventricular asynchrony. The inter-ventricular asynchrony may not be evident in patients with dilated cardiomyopathy and ischemic cardiomyopathy with significant lesions in the left and right coronary system as the two ventricles are affected with nearly equal prolongation of the different time intervals. Ischemic heart disease can be suggested as a cause of cardiomyopathy by the presence of inter-ventricular asynchrony. Also, the presence of intra-ventricular asynchrony is not dependant on the width of QRS complex.
512 Improved ventricular-arterial coupling after 4 weeks of exercise training in patients with chronic heart failure
M Sandri1; S Gielen1; V Adams1; N Mangner1; R Hoellriegel1; S Erbs1; A Linke1; S Moebius-Winkler1; R Hambrecht2; G Schuler2
1University of Leipzig Heart Center, Leipzig, Germany; 2Heart Center, Bremen, Germany
Background: The concept of ventricular-arterial coupling implies that LV-function is determined by the three factors left ventricular diastolic, left ventricular systolic and arterial elastance. We have previously documented an improvement in endothelial and systolic LV-function in patients with chronic heart failure (CHF) after 6 months of exercise training (ET).
It remains, however, unclear, how shorter ET periods may affect endothelial, systolic and diastolic ventricular function as echocardiographic parameters related to ventricular arterial coupling in patients with CHF. Methods: In this ongoing study we randomized 50 patients with stable CHF (age 58.3±3.1 years, EF 27.7±2.1%, VO2max 15.1±3.9ml/kg∗min) to a training or a control group (C). Patients in the training group exercised 4 times a day at 50 to 70% of the individual heart rate reserve for 4 weeks under supervision. At baseline and after 4 weeks the E/A ratio and septal/lateral E'/A' velocities were determined by echocardiography with tissue Doppler. Exercise capacity was measured by ergospirometry and flow-mediated dilatation (FMD) was assessed by high-resolution radial ultrasound.
Results: After only 4 weeks of ET oxygen uptake at peak exercise increased from 14.7±2.9 to 18.5±3.6 ml/min/kg, (p>0.01 vs. C) in training subjects. Left ventricular ejection fraction improved from 26.9 ±3.6 to 32.0±4.5% (p>0.05 vs. C) in patients of the training group while it remained unchanged in the control group. E/A-ratio mended from 0.59±0.22 to 0.84±0.29 (p=0.01 vs. C) in training patients. Lateral E' velocities increased from 4.5±0.6 to 7.3±1.4 cm/s in training patients (p>0.05 vs. C). FMD of the radial artery improved from 9.5 ±2.7 to 14.3±3.2% (p>0.01 vs. C) as a result of ET.
Conclusion: Only 4 weeks of endurance training are highly effective with significantly improved FMD accompanied by an emended systolic and diastolic LV-function. We hypothesise that the improvement in LV-EF in training patients may be caused by a corrected ventricular-arterial coupling: ventricular diastolic relaxation and effective endothelial function are ameliorated resulting in an augmentation of stroke volume.
513 The anti-inflammatory effect of moderate physical training early after myocardial infarction
V Persic; A Ruzic; B Miletic; V Pehar-Pejcinovic; Z Jovanovic; Thalassotherapia Opatija Cardiology and Cardiac Rehabilitation, Opatija, Croatia
Purpose: The inflammatory process is defined as one of the leading pathophysiological constituents of generalized atherosclerotic disease, its development, progression and acute complications. The basal cytokine values as well as acute phase reactants are clearly connected with the incidence of myocardial infarction, its course and long-term outcome. It is also well known that regular physical activity has a positive effect on mild inflammation in certain cardiovascular conditions, although the mentioned effect in the early post infarction period has not been sufficiently studied. The purpose of this study was to determine the effect of physical training on levels of pro-inflammatory and anti-inflammatory cytokines at rest and their inducibility during the submaximal exertion early after the myocardial infarction.
Methods: Sixty consecutive patients aged 60±10 years were included in the 3-week cardiac rehabilitation program following acute myocardial infarction (AMI). The average period passed from the AMI was 7.08±1.60 days. The patients were randomized in the group with standard treatment and in the group with additional aerobic physical training of a moderate intensity prescribed according to the initial ergospirometry test result. Beside a thorough clinical monitoring, serum cytokine levels (TNF-a, TNF-aSR1, IL-8 and IL-10) and acute phase reactants (hsCRP, fibrinogen) were determined while resting or on submaximal exertion in the beginning and in the end of the monitoring.
Results: The early period after AMI is characterized by elevated levels of pro-inflammatory cytokines and acute phase reactants. Training induced a significant decrease in hsCRP, fibrinogen, TNF-aSR1 and IL-8 basal concentrations and more significant increase of IL-10 values at rest. TNF-a levels were not significantly altered in both group. The reactivity of examined markers during the final load test showed significantly higher decline of hsCRP in trained patients, while TNF-aSR1 decreased in trained and increased in non-trained patients. The decline of fibrinogen and IL-8 during the final load test was statistically more significant in the trained patients. Conclusion: The early period after AIM is characterized by a persistent inflammatory condition which gradually regresses using standard treatment procedures. During the same period, the moderate physical training expresses an additional anti-inflammatory effect possibly improving the coronary risk profile.
514 Physical rehabilitation of patients with severe chronic heart failure
G Arutyunov; A Rylova; O Volgina; Moscow, Russian Federation
Purpose: Current approach to administration of exercise to patients with CHF leaves open many issues such as tactics of selecting an optimal regimen of exercise depending on the patient's baseline condition, and exercise safety in patients with high functional classes. Aim of study was evaluating the efficacy and safety of exercise in patients with III-IV NYHA.
Methods: Study enrolled 311 patients with III-IN NYHA of ischemic genesis who were randomized to two groups. After having adjusted the drug therapy and stabilized the condition, patients of group 1 (n=127) exercised at least 5 times weekly. Patients of group 2 (n=184) refused of exercise, and they received only drug therapy. Exercise regimen was selected depending on the patient's baseline condition. Patients with IV NYHA performed exercise for inhalatory and exhalatory muscles using resistance to the air flow during inhalation and exhalation created by special instruments. Patients with III NYHA combined respiratory exercise with walking. Results of 6-min walking test, blood norepinephrine (NE) and angiotensin II, rate of hospitalization for decompensated CHF, and death rate were controlled every 3 months. Follow-up duration was 12 months.
Results: All patients of group 1 showed a significant increment of 6-min walking test results in 12 months (>0.02); IV NYHA was replaced for III NYHA in 14 patients, and IV NYHA was replaced for III NYHA in 19 patients. Exercise tolerance was impaired in patients of group 2: III NYHA was replaced by II NYHA in 26 of them. At enrollment and after 12 month, blood NE significantly increased from 4.78±2.51 nmol/l to 7.65±1.73 nmol/l and from 4.87±1.6 nmol/l 7.32±1.94 nmol/l, respectively, >0.05 in patients of group 1 during exercise. Resting blood level of NE slightly increased from 4.73±2.7 nmol/l to 7.21±2.4 nmol/l. Patients of group 2 showed some increase in NE level from 4.73±2.7 nmol/l to 7.21±2.4 (>0.05). Levels of II remained steady in group 1 throughout the study (154.7±12.33 ng/l at baseline and 167.2±19.88 ng/ml (>0.05) after 12 months), whereas in group 2 these parameters increased from 152.3±13.66 ng/l to 273.3±18.44 ng/l (>0.05). During the follow-up period, 37 (29.1%) and 76 (41%) hospitalizations for decompensated CHF occurred in groups 1 and 2, respectively, >0.05. Numbers of fatal cases were 23 (18.1%) and 48 (26.08%) respectively, >0.05.
Conclusion: Addition of systematic exercise to drug therapy stabilizes the state of neuro-hormonal systems in patients with III-IV NYHA, improves clinical condition of patients, and reduces the rate of decompensation and fatal cases.
515 Intensity determination of interval aerobic exercise training programmes in CHF patients
L Karatzanos1; A Georgantas1; S Dimopoulos2; J Venetsanakos1; 5 Drakos1; S Gyftopoulos2; M Anastasiou-Nana1; G Mansolas2; C Georgopoulos2; S Nanas2
1Cardiopulmonary Rehabilitation Centre, ‘Evgenidion’ Hospital, University of Athens, Greece; 2‘Alexandra’ Hospital, University of Athens, Greece
Introduction: Aerobic exercise training has been an important means of rehabilitation in CHF patients. ‘Steep ramp test’ (SRT), which consists of 3 min unloading pedaling on a cycle ergometer followed by 25 watt increases every 10 secs up to exhaustion, has been suggested as a test to determine intensity of interval aerobic regimes. The aim of this study was to investigate the effects of SRT application on determining and read-justing the intensity of interval aerobic training in CHF patients.
Methods: Thirty one stable CHF patients, 24 male/7 female [(M±S) age: 53.5±10.3 yrs, VO2peak: 14.2±2.2 ml/kg/min], participated in an exercise training program for 12 weeks, 3 times/week. Participants were randomly assigned to either aerobic or combined group, which included aerobic and strength training. Aerobic training was performed in interval type (30 sec effort-60 sec rest) on cycle ergometers. Intensity was set at 50% SRT (WSRT). Both regimes were of the same duration. All the subjects performed a CPET to assess VO2peak and maximum power output (Wmax) and a SRT before and after the program. Additional SRTs took place every 6 sessions (2 weeks) to readjust the intensity of the aerobic exercise.
Results: A small, but significant difference (p>0.05) was observed between Wmax and WSRT at the beginning of the program (95.8±21.7 vs. 105.8±23.7 watt, respectively). Performance at SRT seemed to improve up to 6th week (18 sessions), with no significant alterations thereafter (Table 1). No differences were observed between the two groups (p>0.05). WSRT relative improvement during the program (11.3±6.8%) found to be correlated with pre-WSRT (r=0.57, p>0.05). No correlation was observed between WSRT absolute improvement (22±10 watt) and pre-WSRT (p>0.05). Significant improvements (p>0.05) also found in V02peak (from 14.2±2.2 to 16.4±3.4 ml/kg/min) and Wmax (from 95.8±21.7 to 110.8±28.2 watt).
Conclusion: SRT, in comparison to power output determined with CPET, seemed to determine intensity of aerobic interval training to higher levels. Performing SRT during a 12-week exercise training program also seemed to improve intensity. The necessity of SRT in intensity determination and readjustment of aerobic interval programs need to be further investigated
SRT performance alterations
pre
1
2
3
4
5
post
212±13
223±12
235±12
242±10∗
246±13∗
246±11∗
254±10∗
∗significant compared to ‘pre’ (p>0.05).
516 Beneficial effects of exercise training in patients with heart failure regardless of training modality
A Hoffmann; P Gnehm; HP Brunner-La Rocca; J Schumann; M Di Valentino; P Rickenbacher; Univ. Hospital, Basel, Switzerland
Background: Exercise training has proven to be beneficial in patients with heart failure but a debate is ongoing whether steady state or interval training protocols should be used.
Methods: Patients with heart failure entering a 12-week outpatient exercise based rehabilitation program were randomly assigned to either an interval protocol (IP) or a steadystate protocol (SS). Three sessions per week were held where in addition to warm-up gymnastics and relaxation the pts were trained on bicycle ergometers for 25 minutes at either 67% of their max. work capacity (as measured in a steep ramp protocol) with repeated intermittent bouts of 40 sec load / 60 sec rest (IP) or at 50% peak exercise capacity (as determined during a standard ergometry ramp test) (SS). Pts were examined at the beginning and after 12 weeks (exercise tests, six minutes walking tests, BNP).
Results: There were 29 pts in the IP and 18 pts in the SS group. Diagnoses were coronary disease in 55% and cardiomyopathy in 45%. Age (mean±SD: 60±14 vs 63±16), gender (m/f 24/5 vs 14/4), and LV function (LVEF 25±5 vs 27±5%) were not different between the groups. Exercise capacity increased equally in both groups (IP: 116±29 to 124±33; SS: 99±30 to 111±39 Watt, p=0.012). In the six minutes walking test increased distances were measured in both groups (IP: 440±71 to 466±82 m; SS: 447±73 to 510±80 m; p=0.005). BNP levels decreased in both groups (IP: 651±495 to 442±322; SS: 387±422 to 263±255 pg/ml; p=0.017). The incidence of cardiac complications (symptomatic arrhythmias or need for treatment interventions) was significantly higher in the SS group (7/18 vs 2/29, p=0.007).
Conclusion: Beneficial effects on exercise capacity, walking distance and BNP levels were observed during a 12 week rehabilitation program with both SS and IP training modalities. However in the group with IP the rate of complications necessitating treatment interventions was lower. This may be an indication of better long term tolerance of IP exercise training.
517 Maintain - Randomized controlled trial of a 12 months low intensity exercise-training program in chronic systolic heart failure
E Prescott1; R Hansen2; F Dela3; A Teisner2; B Oerkild2; H Nielsen2
1Bispebjerg University Hospital Cardiology Department, Copenhagen, Denmark; 2Amager University Hospital Cardiology Department, Copenhagen, Denmark; 3University of Copenhagen Department of Biomedical Sciences, Copenhagen, Denmark
Background: Short term physical training programmes have been shown to be beneficial in heart failure patients but there is a lack of studies following unselected patient-groups for longer duration with maintenance training programs to defer deconditioning.
Methods: Randomized controlled study examining the efficacy of an 8 week training program with in-hospital training twice a week followed by either a home-based maintenance exercise program with group training sessions every 2 weeks for 12 months, or usual care, in patients with systolic heart failure (Left ventricular ejection fraction (LVEF).
Results: 43 of 66 patients completed the study. Drop out was characterized by low exercise capacity and high co-morbidity at baseline. The initial 8-weeks training program was associated with significant improvement in all of the functional tests. With the exception of STS, there was a significant decline in functional tests after 14 months in both groups. There was a trend towards beneficial effect of intervention compared with control in maximum exercise capacity (p=0.06) but no difference in SMWT, ISWT or STS. In a multivariate regression with adjustment for baseline exercise capacity, LVEF, angina, bodymassindex and history of hypertension, there was a significant effect of the maintenance intervention on maximum exercise capacity at 14 months with a difference in decline between groups of 8.25 watts (SE 2.53, p=0.002). After 14 months the intervention group had better glycemic control and lover inflammatory markers.
Conclusions: A low cost maintenance program is feasible in unselected patients from a hospital setting. The program could not prevent loss of exercise capacity but reduced the loss significantly in comparison with a control group and had added beneficial effect on glycemic control and markers of inflammation. Further studies are needed that focus on maintenance training programs that are available to an unselected patient group.
518 Physical training accelerates post-exercise oxygen uptake kinetics in patients with chronic heart failure
H M C Kemps1; WR De Vries2; SL Schmikli2; ML Zonderland2; AR Hoogeveen1; HJM Thijssen1; G Schep1
1Maxima Medical Centre, Veldhoven, Netherlands; 2University Medical Centre, Utrecht, Netherlands
Purpose: To evaluate the clinical usefulness of O2 kinetics to assess training effects in CHF patients.
Methods: In a prospective semi-crossover design, 32 CHF patients (NYHA class II/III) were randomized to an intervention group (n=16), that performed a 12-wk training program (cycle interval and resistance training), or to a control group (n=16) that started this program after a 12-wk control period. Training effects were expressed as changes in peak workload, peak O2, O2 at the ventilatory threshold (VT), and O2 onset and recovery kinetics at submaximal and maximal cycle ergometry.
Results: During symptom-limited exercise, peak workload, peak VO2, and VO2 at the VT were increased significantly after training (Table 1). Only VO2 at the VT showed a significant training-related between-group change (P=0.02).
Concerning O2 kinetics, both the time constant of O2 recovery after submaximal exercise (τ-rec) and the recovery half-time of peak VO2 decreased after training (Table 1), whereas only τ-rec showed a significant between-group change (P=0.005). In contrast to the assessment of VT (percentage of failure: 13%), assessment of τ-rec was successful in all patients.
Conclusion: Training effects in CHF patients were manifested consistently at a submaximal exercise level in improvements of τ-rec and VO2 at the VT. Since τ-rec could be better assessed, this parameter can be recommended in clinical practice for evaluation of training effects in CHF patients.
Training effects (n=32)
Before training
After training
P value
Symptom limited exercise
Peak VO2 (ml/kg/min)
17.0±3.3
18.8±4.0
0.002
Peak Workload (W)
101±31
109±33
0.001
HR (beats/min)
124±23
125±23
0.49
VO2 at VT (ml/kg/min)
12.3±2.1
13.7±2.7
0.004
T1/2 (s)
109±37
101±40
0.02
Constant-load exercise
MRT (s)
78±25
79±22
0.55
τ-rec (s)
85±32
76±27
0.001
HR, maximum heart rate; VT, ventilatory threshold; T1/2, half time recovery of VO2 after maximal exercise; MRT, mean response time; τ-rec, time constant of recovery of VO2.
519 (WITHDRAWN) Postexercise blood flow in chronic heart failure: evidence for enhanced systemic endothelial function
R Stein; D Umpierre; PJC Vieira; RS Moraes; EL Ferlin; JP Jorge; P Ribeiro
Hospital De Clinicas De Porto Alegre, Porto Alegre, Brazil
Background: Chronic lower-limb exercise training improves endothelial function in non-trained vascular beds in patients with chronic heart failure (CHF) and improves autonomic balance.
Objective: To test the hypotheses that (1) CHF patients would present changes in blood flow and flow-mediated vasodilation responses in the non-exercised limb after a single session of cycle exercise, and (2) that they could have less parasympathetic drive following the exercise.
Methods: Thirteen CHF patients (mean±SEM, left ventricular ejection fraction 34±3%) and 13 healthy controls participated in two sessions, on different days, in random order: (1) a 25-min period seating at rest and, (2) a 25-min submaximal exercise session. Measurements of heart rate, blood pressure, and venous occlusion plethysmography forearm blood flow and flow-mediated dilation were made before and after (immediately, 10, 30, 60 min, and 24 h) each session. Heart rate variability (HRV) and ambulatory blood pressure monitoring (ABPM) were assessed during the 24 h following each session.
Results: CHF patients had no changes in the mean blood pressure throughout the protocols, whereas mean blood pressure was reduced up to 60 min after exercise in controls (pre-exercise, 90±22 mmHg vs. postexercise, 86±22 mmHg). In CHF patients, forearm blood flow was increased and forearm vascular resistance was reduced immediately after exercise, while these changes were two-fold higher and sustained up to 30 min after exercise in controls (P>0.001). Flow-mediated vasodilation showed a significant increase up to 30 min after exercise in both groups (CHF: 13.5±1 vs. 16±1 ml/min.100ml; controls: 14.4±1 vs. 16.8±1 ml/min.100ml). Indices of HRV were similar after both sessions in CHF patients, while controls showed less parasympathetic modulation up to 24 h after the exercise (P>0.05). Twenty four-hour ABPM showed no significant changes between the two experimental days for both groups.
Conclusion: A single submaximal cycle exercise session results in less vagal activity and sustained increase in forearm blood flow in healthy individuals, but not in patients with CHF. Despite the blunted postexercise vascular responses, patients with CHF respond to a single cycle exercise session with improved endothelium-dependent vasodilation.
520 Inspiratory muscle training improves distribution of bood flow to resting and exercising limbs in heart failure
JP Ribeiro; GR Chiappa; BT Roseguini; PJC Vieira; CN Alves; A Tavares; ER Winkelmann; EL Ferlin; R Stein
Hospital De Clinicas De Porto Alegre Cardiology Division, Porto Alegre, Brazil
Background: Previous clinical trials have shown that inspiratory muscle training results in improved functional capacity of patients with chronic heart failure (CHF) and inspiratory muscle weakness, but the mechanisms of these effects are not known.
Objective: We tested the hypothesis that inspiratory muscle loading could result in exaggerated peripheral vasoconstriction in resting and exercising limbs and that inspiratory muscle training could attenuate this effect in patients with CHF and inspiratory muscle weakness.
Methods: Eighteen patients with CHF and weakness of inspiratory muscles (maximal inspiratory pressure >70% of predicted) and 10 healthy volunteers participated in the study. Inspiratory muscle loading was induced by the addition of inspiratory load of 60% of maximal inspiratory pressure, while blood flow to the resting calf (CBF) and exercising forearm (FBF) were measured by venous occlusion plethysmography. For the patients with CHF, measurements were also made after a 4-week program of inspiratory muscle training.
Results: With inspiratory muscle loading, CHF patients presented a more marked reduction in resting CBF (mean±SD 55±12 vs. 14±5%, P>0.01%) and showed an attenuated rise in FBF (6.9±2.0 vs 11.2±1.1 ml/min.100ml; P=0.01) when compared to controls. After 4 weeks of inspiratory muscle training, CHF patients improved resting CBF (1.19 ±0.3 vs 2.0±1.0 ml/min.100ml; P=0.01) and exercise FBF (6.9±2.0 vs 9.8±2.8 ml/min.100ml; P=0.01) with inspiratory muscle loading.
Conclusion: In patients with CHF and inspiratory muscle weakness, inspiratory muscle loading results in marked reduction of blood flow to resting and exercising limbs. Inspiratory muscle training improves blood flow redistribution in these patients.
521 Gender comparison of long term outcomes of a disease management and rehabilitation program designed for congestive heart failure patients
L Houston-Feenstra; K Jutzy; JR Chiong
Loma Linda University Medical Center Cardiology Department, Loma Linda, United States of America
Purpose: Compare long-term outcomes of a comprehensive disease management and rehabilitation program (CDMR) vs. standard of care in both men and women with CHF.
Methods: This study compares four groups of patients followed for 36 months post hospital discharge; all groups received training in the management of CHF in the hospital and were discharged on appropriate medication regimens. Two groups were identified as Intervention: Group A (15 men average age: 59.9) and Group B (6 women average age 64.08) participated in a 12-week CDMR program and the two other groups identified as Control: Group C (36 men average age 61.3) and group D (12 women average age 62.2) returned to standard follow up care for CHF. Groups A and B participated in CDMR received an individualized program including use of medications, effective sodium balance and symptom identification. Rehab patients returned 3 times per week for 12 weeks.
Conclusion: Both genders participating in CDMR program demonstrated long-term improvement in medication adherence and smoking cessation. They also had significantly fewer CHF related Hospitalizations, ED visits and improved survival at 36 months compared to Controls.
Results
Men Control (group C)
CMDR (group A)
Baseline
36 mos.
P value∗
Baseline
36 mos.
P Value∗
Smoking
25%
9%
0.001
13%
9%
0.02
Beta Blocker
69%
91%
0.032
87%
91%
N/S
ACE
67%
69%
N/S
80%
91%
0.021
Hospitalizations
3
4.364
0.03
2
0.364
0.0002
ED Visits
3
3.091
N/S
4
0.091
0.001
Deaths
0
3
0.001
0
0
N/S
Results: Women Control (group D)
CMDR (group B)
Baseline
36 mos.
P value∗
Baseline
36 mos.
P Value∗
Smoking
42%
40%
N/S
50%
0%
0.0002
Beta Blocker
100%
100%
N/S
100%
100%
N/S
ACE
100%
80%
0.02
98%
100%
N/S
Hospitalizations
2
3.143
0.004
2
0.167
0.001
ED Visits
1.67
2.429
0.032
2
0
0.0001
Deaths
0
0
N/S
0
0
N/S
522 Electrical stimulation of skeletal muscles in patients witn chronic right ventricular disfunction: influence on right ventricular function and pulmonary function
The breathlessness of patients with pulmonary hypertenson (PH) during exercise can be related to the relative hypoperfusion of their well-ventilated alveoli. Recently a beneficial effect of standardized exercise training in patients with severe PH was demonstrated. We have assumed, that electrical stimulation of skeletal muscles can be used in rehabilitation of the PH patients.
The objective of the present investigation was to evaluate the influence of EMS course on right ventricular function and pulmonary function in PH patients.
We examined 101 patients (59±1,1 years) with secondary PH. In control group (n=47) the patients received only the usual program of rehabilitations, in the EMS group (n=54) there was an additional EMS course. At baseline and after 3 weeks of the rehabilitation, all patients underwent a 6 minute walking-test, spirometry and echocadiography. EMS sessions were carried out 2 times a day for 30 minutes within 10 days.
Results: The passive trainings with EMS have resulted to increase of distance of six-minute walking, TLC and FEF 50% at spirometry and tendency to decrease of pulmonary arterial pressure in Doppler echocadiography (see Table).
Thus, the EMS course resulted to the significant increase of exercise tolerance, improvement of pulmonary functiom and some improvement of right ventriculsr function. Use of EMS deserves the further application in rehabilitation of the PH patients.
Results of EMS course in PH patients
Characteristic
Group
Before treatment
After treatment
P
6MWT (m)
EMS
356,0±9,6
405,6±10,6
0,000002
Control
368,0±13,7
363,3±13,0
0,778
mPAP (mm Hg)
EMS
28,3±1,4
26,2±1,1
0,083
Control
27,2±1,5
26,7±1,2
0,436
RVEDD (mm)
EMS
32,4±2,6
31,8±2,3
0,932
Control
32,7±2,6
32,9±3,2
0,249
TLC (l)
EMS
2,68±0,1127
2,81±0,1368
0,0189
Control
2,57±0,1301
2,63±0,1185
0,9528
FEF 50% (l/s)
EMS
2,83±0,1854
3,09±0,2273
0,0164
Control
2,77±0,2011
2,86±0,2463
0,885
6MWT − 6 minute walking-test; mPAP - mean pulmonary arterial pressure; RVEDD - right ventricular end-diastolic dimension; TLC - total lung capacity; FEF 50% - forced espiratory flow at 50% of espiratory phase.
523 Description of a sample from ischemic cardiopathy patients assessed in the second phase of a cardiac rehabilitation program: analysis of changes after the training program
M Parra; F Ortun; A Aunon; A Segura; I Cote; N Caparos; R Figuera; M Martin
Hospital Mutua de Terrassa Rehabilitation, Terrassa, Spain
Purpose: Description and analysis of changes produced in a sample of patients with ischemic cardiopathy (IC) who followed a training programme (TP).
Methods: Description of a sample of patients with IC assessed by the rehabilitation department between June 2006 and October 2007, and analysis of changes produced among those who completed the TP. The described variables are: risk, functional questionnaires [DASI- reduced version (DASIr) and Veterans Specific Activity Questionnaire (VSAQ)], Exercise trials [Six-minute Walk Test (6MWT) and ergometry with gas analysis (EGA)] and Health Related Quality of Life (HRQoL) questionnaires [Seattle Angina Questionnaire (SAQ), Velasco- Del Barrio (VB)]. Statistics: conventional descriptive analysis, ANOVA, paired t-test and MANOVA.
Results: 68 patients, average age 58 years, 94% male. According to risk levels, 33.8% were considered mild, 55.9% moderate, and 10.3% severe. The average results are: -DASIr 20.9, VSAQ 6.7.
-6MWT 458 metres, EGA VO2 peak 19.2 ml/k/min (5.5 METs), exercise time (ET) 10 minutes, Anaerobic threshold time (ATt) 8.1 minutes with VO2 AT 15.1 ml/k/min.
Among the 39 patients who completed the TP, 39.5% are mild, 52.6% moderate, and 7.9% severe. With regard to functional parameters, all groups present significant changes (p>0.05) in DASI, 6MWT, VO2peak, ET and ATt. VSAQ improves only significantly in the group of mild and moderate patients. Regarding HRQoL changes, only the mild group improves significantly (p>0.05) in health, mobility, leisure and work time, and general dimensions of the VB questionnaire.
Due to the reduced size of the severe group, it has only been possible to analyse the changes following the TP between mild and moderate group. There are no significant differences in the magnitude of change between these groups.
Conclusion: -DASIr, 6MWT, VO2 peak, ET, ATt capture the beneficial effects of TP in the majority of patients. -VB and SAQ do not seem to be able to reflect the beneficial effects of a TP. -TPs provide similar functional benefits in patients with slight and moderate risk levels.
524 Derangement of hypothalamus-pituitary-adrenal axis in patients with severe chronic heart failure
L Jasiukeviciene1; DA Vasiliauskas1; A Kavoliuniene2; R Grybauskiene3; V Grizas3; J Janenaite1; V Tumyniene3
1KMU Institute of Cardiology Institute of Cardiology, Kaunas, Lithuania; 2Kaunas University of Medicine Hospital Department of Cardiology, Kaunas, Lithuania; 3KMU Institute of Cardiology Institute of Cardiology, Kaunas, Lithuania
Introduction: Chronic fatigue and chronic fatigue syndrome are characterized as disorder of hypothalamus-pituitary-adrenal axis which in definitive stages is definable as exhaustion of adrenal function and atrophy of adrenal glands. Long-term internal sympathetic activity in patients with chronic heart failure and its impact on cardiorespiratory function is underestimated.
We assessed the hypothesis that chronic fatigue severity is related not only to left ventricular dysfunction, and that long-term internal sympathetic activity in patients with moderate-to-severe chronic heart failure impacts on a hypothalamus-pituitary-adrenal axis.
Methods: One hundred and ten patients with III-IV class (NYHA) chronic heart failure filled in chronic fatigue questionnaires MFI-20L (100 point scale), DUFS and DEFS (9 point scales each) and underwent Doppler echocardiography and cardiopulmonary exercise testing, underwent a.m. and p.m. blood cortisol and plasma NT-proBNP analysis. Regression analysis relating neurohumoral and cardiorespiratory findings to MFI-20L scale of overall and physical fatigue results was performed, and Spearman's rank correlation coefficients were calculated.
Results: Fifty patients with III class (NYHA) scored 45.8±25.5 points, and sixty patients with IV class (NYHA) − 58.8±28.8 points of overall chronic fatigue according to MFI-20L questionnaire scale. In patients with III (NYHA) class a.m. blood cortisol concentration was normal (552.1±95.111mmol/l), and p.m. blood cortisol concentration was diminished within normal range -(289.5±149.222 mmol/l). In patients with IV (NYHA) class a.m. blood cortisol concentration was normal (410.1±175.111 mmol/l), and p.m. blood cortisol concentration was insufficiently diminished -(355.6±160.333 mmol/l). Chronic fatigue had a significant and moderate relation to age and ventilating equivalent VE/VCO2, significant and moderate inverse relation to blood cortisol concentration, and weak relation to left ventricular ejection fraction and plasma NT-proBNP concentration.
In conclusion, chronic fatigue is ubiquitous and pronounced in patients with III-IV class (NYHA) chronic heart failure, resulting in lack of motivation to act and poor self-care. Insufficient decrease in p.m. blood cortisol concentration in patients with IV (NYHA) class chronic heart failure is a sign of derangement in hypothalamus-pituitary-adrenal axis in patients with long-term cardiovascular organic disease.
525 Impaired creatinine clearance is associated with higher likelihood of development systolic heart failure in post acute coronary syndrome patients; the Hellenic acute heart failure case-control study
C Chrysohoou1; P Aggelopoulos2; C Pitsavos1; L Papadimitriou1; G Metallinos1; C Liantou1; A Aggelis1; D Marayiannis1; E Tsiamis1; C Stefanadis1
1Glyfada, Greece, 2Athens, Greece
Background: The relationship between renal dysfunction and mortality in patients with myocardial infarction, as well as with heart failure, has been extensively investigated. However, data about the role of renal function on the occurrence of heart failure in patients with an acute coronary syndrome are limited. Therefore, we sought to investigate whether renal insufficiency is an independent predictor for systolic heart failure among latter patients.
Methods and Results: During 2006-2007, 144 male (65±14 years) and 50 female (71±12 years) post acute coronary syndrome patients who developed systolic heart failure after the cardiac event and 129 males (64±12 years) and 51 females (67±10 years) without developing heart failure after the coronary event, were included in the study. Participants were age and sex matched and consequently selected. Detailed information regarding their medical records, anthropometric data, physical activity and smoking habits were recorded. Those who developed systolic heart failure had lower body mass index, higher prevalence of myocardial infarction than unstable angina, higher initial serum levels of troponin-I, higher uric acid levels, more advanced coronary level disease, lower prevalence of physical activity and higher prevalence of diabetes mellitus. Creatinine clearance rates were estimated by the Cockcroft-Gault formula. Eight percent of patients presented at the hospital with severe renal dysfunction, 30% with moderate and the other 62% with normal. Patients with moderate or severe renal dysfunction were older, had lower body mass index, lower prevalence of smoking and higher prevalence of arterial hypertension and diabetes mellitus, compared to those with normal renal function. Moreover, moderate and severe renal insufficiency continues to be prognostic factor for systolic heart failure; while a increase per 10 units of creatinine clearance decreases the risk of developing heart failure by 26%, even after controlling for potential confounders.
Conclusion: We demonstrated that creatinine clearance rate is an important independent predictor of systolic heart failure after an acute coronary event. Therefore, patients with acute coronary syndromes complicated by renal dysfunction should receive more aggressive medical care.
526 An association of diabetes or hyperglycemia and increased level of lipid peroxidation with stroke and myocardial infarction in elderly men
DI Luksiene1; LR Cerniauskiene1; L Margeviciene1; A Tamosiunas1; A Norkus2
1Institute of Cardiology Laboratory of population Studies, Kaunas, Lithuania; 2Institute of Endocrinology, Kaunas, Lithuania
Stroke is a deadly and disabling disease that preferentially afflicts older adults; it shares common risk factors with myocardial infarction (MI), such as diabetes and oxidative stress.
The aim of this work: To evaluate the association of stroke and MI with diabetes, hyperglycemia and increased level of lipid peroxidation in elderly men from Kaunas urban population investigated in 1995-1996. Subjects and methods: In this work we used data of 525 men aged 65-84 years. Previous stroke and MI were determined according to epidemiological criteria. History of stroke was based on answers to following interview question: “Has a doctor ever told you that you had a stroke?”. Previous MI was determined according to answers of responders to question: “Has a doctor ever told you that you had a heart attack?” and/or changes on electrocardiogram coded by Minnesota codes as 1-1 or 1-2. All stroke and MI cases were verified using all possible medical documentation (hospital discharge records, domiciliary care records of outpatient departments and etc.). 30 men had stroke, 65 men had MI. Diabetes mellitus was determined by persons answer to question: “Has a doctor ever told that you have diabetes?” and/or glucose level =11.111 mmol/l after 2 hour glucose laod (75 g). Glucose concentration was determined in capillar blood by individual glucometer. Hyperglycemia was evaluated as fasting glucose =6.111 mmol/l. Lipid peroxidation marker malondialdehyde (MDA) was measured by fluorimetrical method and increased level was evaluated as =5.5 micromol/l.
Results: The average of age for men who had stroke or MI (N=89) was not different to age for men without stroke or MI (N=436): 73.5±4.64 years and 72.9±4.10 years respectively (p>0.05). Among men who had stroke or MI the rate of diabetes or hyperglycemia (a) and the rate of increased level of MDA (b) were significantly higher than among men without stroke and MI (1.8 and 1.4 times accordingly): (a) 25.8% vs. 14.7% (p>0.05), (b) 46.6% vs. 32.9% (p>0.05). Among men who had stroke or MI the rate of persons with complex of those risk factors (diabetes or hyperglycemia and increased level of MDA) was 2.2 times higher than among persons without stroke and MI: 12.4% vs. 5.7% (OR 2.28; 95%CI 1.01-5.08; p=0.048).
Conclusion: In elderly men diabetes or hyperglycemia and increased level of lipid peroxidation marker MDA are directly associated with cardiovascular diseases - stroke and MI.
527 White blood cell count is independenly related to occlusive atherosclerosis of lower extremities in patients with diabetes
NV Polenova; AD Deev; DV Abramkin; IS Yavelov; NA Gratsiansky
Institute of Physico-Chemical Medicine Center for Atherosclerosis, Moskva, Russian Federation
Purpose: To elucidate factors associated with low ankle-brachial index (ABI) in patients with diabetes mellitus, impaired glucose tolerance, or impaired fasting glucose with and without coronary heart disease.
Methods: We examined 182 patients with diabetes (n=155), impaired glucose tolerance (n=17), or impaired fasting glucose (n=7). ABI was =0.9 in 47/182 patients (25.8%). We analyzed history, demographic parameters, anthropometric data (body mass index, waist circumference), levels of plasma high and low density lipoprotein cholesterol (HDLCH and LDLCH), triglycerides, degree of glycemic control, presence of signs of atherosclerosis of other localization.
Results: ABI was =0.9 in 47/182 patients (25.8%). Patients with ABI =0,9 were older, more often had history of myocardial infarction (p=0.006) or vascular surgery (p>0.0001), symptoms of heart failure (p=0.04), claudication(p>0.001), and ultrasound sings of carotid artery stenosis (p>0.001). They also had higher leukocyte count (p=0.009). Leukocyte count above 7.5103/mm3 compared with that =7.5103/mm3 was associated with 3 fold increase of odds ratio (OR) 2.96 [95% confidence interval (CI) 1.5-6.0, p=0.03]. Factors independently related to ABI =0,9 were age (OR 1.1; 95% CI 1.02-1.14; P=0,01), history of smoking (OR 2.2, 95% CI 1.34-3.74, p=0.01), and leukocyte count (OR 1.3; 95% CI 1.06-1.62, p=0.02). None of biochemical parameters including characteristics of glycemia control was related to the presence of decreased ABI.
Conclusion. In this group of patients with type 2 diabetes besides such classical factors as age and smoking white cell count but not lipids were associated with low ABI - an established marker of atherosclerosis of lower extremities.
528 Systemic level of C-reactive protein and incident coronary heart disease among free-living older adults: the Three City Study
C Straczek1; P Ducimetiere1; M Tafflet1; JF Dartigues2; K Ritchie3; P Amouyel4; C Tzourio5; JP Empana6
1Inserm U909 Sudden Death and CV Epidemiology, Villejuif, France; 2INSERM U593, Bordeaux, France; 3INSERM E0361, Montpellier, France; 4INSERM U508, Lille, France; 5INSERM U708 Department of neuroepidemiology, Paris, France; 6Inserm U909 Sudden Death and CV Epidemiology, Paris, France
Purpose: In the past decade, systemic inflammatory markers have emerged as independent risk indicators for coronary heart disease (CHD). Even though older adults experience a higher CHD incidence, epidemiologic data on C-reactive protein (CRP) from this population are scarce and inconsistent. We therefore examined the association of systemic CRP level with incident CHD events among older adults participants from the Three City Study.
Methods: The Three City Study is a French population-based multicentre prospective study including 9294 free-living older adults aged >65 years who were recruited between 1999-2001 from the electoral rolls of three French cities for an extensive examination. Incident CHD events were checked annually and after the completion of 4 years of follow-up, a case cohort study was undertaken. The baseline plasma samples of 199 incident CHD events and of a random sample of 1083 subjects from the initial cohort without previous CHD were thawed for the measurement of several proteins. High sensible CRP (hs-CRP) was measured by enzyme linked immunosorbent assays. Subjects with baseline hs-CRP above 10 mg/l (n=98) were excluded from the analysis. Hazard ratios (HR) of hs-CRP for CHD were estimated by a Cox proportional hazard model adapted to the case cohort study design, using hs-CRP below 33 mg/L as the reference category.
Results: Among the random sample, 65.4% of the study participants had hs-CRP below 33 mg/L and 27.6 % between 3-100 mg/L. Hs-CRP was correlated with body-mass index (BMI), low HDL cholesterol, high triglyceride levels, and fasting glycaemia in the random sample. The HR of higher hs-CRP for CHD was 1.65 (95%CI: 1.17-2.33) after adjustment for age, sex and the study centres. Additional adjustment for BMI, HDL and LDL cholesterol, diabetes, hypertension, smoking status and statin use did not materially change the HR point estimates (1.55; 1.05-2.29). There was no significant interaction with LDL cholesterol or gender, although association tended to be stronger in women (1.89; 1.03-3.49) compared to men (1.40; 0.84-2.37; p for interaction=0.50). In a subset of 950 participants who had Doppler ultrasound examination of the carotid arteries at baseline, higher hs-CRP remained predictive of CHD independently of carotid plaque presence or higher intima-media thickness.
Conclusion: The present study provides evidence that higher systemic hs-CRP is a risk marker of incident CHD over 4 years in a free-living older adult population. The respective contribution of hs-CRP and other inflammatory biomarkers from different pathways should be further assessed in this population.
529 The relationship between apolipoprotein A-I and B, lipids and Lp(a) in patients with or without coronary heart disease
L Agoston Coldea; LD Rusu; R Pais; L Poanta; T Mocan; ML Ruse
University of Medicine and Pharmacy Cluj, Cluj-Napoca, Romania
Purpose: Recent evidences show that apolipoprotein B and apoB/apoA-I ratios is a better indicator for coronary risk than the conventional lipid profile. Several studies showed that an elevated plasmatic level of lipoprotein(a) [Lp(a)] is a good predictor for coronary risk. Based on already existing literature data, we intended to study the relationship between apolipoprotein A-I and B, lipids and Lp(a) in patients with or without coronary heart disease.
Methods: We performed a transversal „cross-sectional“ study which included 208 patients (males and females) aged between 37-75 years, with or without myocardial infarction according to coronarograhy criteria. We measured the anthropometric and cardiovascular risk parameters. The dosage of the lipids fractions was done by enzymatic method and those of the Lp(a) and apoA-I and apoB was measured by immunoturbidimetric method from Roche.
Results: The group with myocardial infarction had higher values of plasmatic levels of Lp(a) (0.37±0.28 vs. 0.29±0.23 g/L, p >0.001), apoB (1.13±0.40 vs. 0.84±0.28 g/L, p>0.0001) and of the apoB/apoA-I ratio (0.77±0.37 vs. 0.68±0.20, p >0.001) than those without coronary heart disease. Multivariate analysis performed with adjustments for cardiovascular risk factors, showed that the levels of Lp(a), apoB and apoB/apoA-I ratios remained as significant and independent cardiovascular risk factors. The correspondent Receiver Operator Curve shape suggested a good reliability in the diagnose of coronary heart disease for the apoB/apoA-I ratio (under curve area=0.756, p>0.0001), apoB (0.664, p>0.0001), Lp(a) (0.652, p>0.0005) and apoA-I (0.571, p>0.05). ANOVA analysis showed the significant correlation of Lp(a), apoB and of the apoB/apoA-I ratio with the severity of the coronary heart disease.
Conclusions: Our results indicates that Lp(a), apoB and the apoB/apoA-I ratio are independent coronary risk factors, being superior to conventional lipids. We suggest the use in clinical practice of the apoB/apoA-I ratio and of the Lp(a) as a marker for cardiovascular risk assessment in clinical practice.
530 Endothelial haemostatic markers in members of families with familial combined hyperlipidemia
D Karasek; H Vaverkova; M Halenka; L Slavik; D Novotny
University Hospital 3rd Department of Internal Medicine, Olomouc, Czech Republic
Purpose: The aim of this study was to evaluate the plasma levels of endothelial haemostatic markers - von Willebrand factor (vWF), plasminogen activator inhibitor-1 (PAI-1), tissue plasminogen activator (t-PA) and soluble thrombomodulin (sTM) - in asymptomatic, non-smoking members of families with familial combined hyperlipidemia (FCH). We investigated the association between these factors and the intima-media thickness (IMT) of the common carotid artery, selected risk factors of atherosclerosis and markers of insulin resistance.
Methods: 82 members of 29 FCH families were divided into two groups: HL (probands and hyperlipidemic first-degree relatives, n=47) and NL (normolipidemic first-degree relatives, n=35). The control groups C-HL (n=20) and C-NL (n=20) consisted of sex- and age-matched healthy individuals. IMT was measured by ultrasound at a far wall of both common carotid arteries.
Results: Compared with healthy controls, hyperlipidemic subjects had significantly higher levels of vWF (146.4±73.2% versus 112.2±29.4%, p>0.05), of PAI-1 [102.4(83.0-117.0) ng/ml versus 63.5(31.8-87.3) ng/ml, p>0.01] and of t-PA [5.1(2.5-7.9) ng/ml versus 3.4(1.4-5.8) ng/ml, p>0.05]. They had increased IMT, which correlated with vWF (r=0.29, p>0.05). Their normolipidemic relatives had significantly higher levels of vWF (137.2±42.8% versus 106.6±24.0%, p>0.01) and of PAI-1 [75.3(53.2-92.0) ng/ml versus 48.6(37.4-85.9) ng/ml, p>0.05]. Levels of vWF, PAI-l and t-PA were independently associated with several markers of insulin resistance.
Conclusion: Asymptomatic members of FCH families have increased endothelial haemostatic factors - vWF, PAI-1, t-PA, which are associated with insulin resistance. VWF correlates with morphological vascular changes, detected by the increase of IMT, presented in only hyperlipidemic subjects.
531 Clinical and angiographic implications of peripheral neutrophilia in acute st-segment elevation myocardial infarction
MF Elnoamany; Shebin Elkom, Egypt
Background: Inflammation associated with acute ST-segment elevation myocardial infarction (ASTEMI) is frequently marked by a peripheral leukocytosis and relative neutrophilia (RN). This process has been associated with a higher risk of acute clinical ischemic events and adverse angiographic (AA) findings.
Objectives: To examine the association between hospital admission peripheral total leukocyte count (TLC) and the neutrophil percentage (NP) and subsequent development of congestive heart failure (CHF) and AA outcomes in patients with ASTEMI.
Methods: The study enrolled 152 patients admitted to the coronary care unit with ASTEMI. Blood samples were collected for assessment of total and differential leukocyte counts and cardiac enzymes. Outcome measures included clinical episodes of CHF with confirmatory chest roentgenogram findings and/or echocardiographic evidence of contractile dysfunction. Coronary angiograms were performed conventionally, and Thrombolysis In Myocardial Infarction (TIMI) flow grade of the infarct-related artery (IRA) was assessed.
Multivariable regression analysis was performed to examine the relation between TLC, NP, and the development of CHF in the first 4 days after ASTEMI and TIMI flow grade of IRA while controlling for baseline characteristics and early therapeutic interventions.
Results: 49% of the studied population had admission TLC>11X 10 9/L, 55.9% had NP>65%, and 56.7% had lymphocyte count >25 %. CHF developed in 92 patients (60.5%) of the study population. Of those (who developed CHF), 80 (87%) patients had RN(neutrophil count>65%), 71 (77.2%) patients had TLC>11X 10 9 / L, 64 (69.6%) patients had creatine phosphokinase (CPK) level>600 U/L compared with 5 (8.3%) patients, 4 (6.7%) patients & 24 (40%) patients, respectively in whom CHF did not develop (60 patients). A relatively strong negative correlation was detected between NP and TIMI flow grade (r=-0.66, p>0.001). In multivariable analysis, RN was found to be a highly significant independent predictor of both IRA (TIMI grade 0/1 flow) [odds ratio(OR) 2.1; 95% confidence interval(CI) 1.6 to 8.7], and subsequent development of CHF (OR 4; 95% CI 1.9 to 8.6).
Conclusion: RN on admission to the hospital in patients with ASTEMI is significantly associated with the early development of CHF and impaired epicardial flow. This association may help in the identification of individuals at high risk who might benefit from more aggressive therapeutic and/or interventional reperfusion to prevent or reduce the risk of CHF.
532 Heart rate variability and silent myocardial ischemia as indices of cardiac autonomic neuropathy in hypertensive diabetes patients
T Akhobadze; R Kurashvili; L Dzneladze; M Dundua; E Shelestova; K Paghava; R Tsvariani, Georgian Diabetes Center, Tbilisi, Georgia, Republic of
Background and Aims: Type 2 diabetic (T2DM) patients (pts) with hypertension have increased risk of cardiac mortality, including sudden death (SD). The risk is especially high in non-dippers. Cardiac autonomic neuropathy (CAN) is considered to be an independent risk factor for cardiac mortality in T2DM pts. The aim of the study was to asses CAN data - heart rate variability (HRV), QTc interval dispersion (QTs), silent myocardial ischemia (SMI) in non-dipper T2DM pts.
Material and Methods: We supervised 2 groups of hypertensive T2DM pts (n=116): dippers (D n=61. 32 m/29f, mean age 54+11.3 yrs), non-dippers (ND, n=55. 29 m/26f, mean age 55+9.8.yrs) In all pts 24-h ambulatory ECG and BP monitoring were performed. Time domain HRV parameters and SMI episodes were assessed on Holter ECG. QTcd was measured on surface ECG. CAN severity was evaluated using Eving's five standard tests (severe CAN-scores 7-10, moderate - scores 4-6, mild- scores 2-3, no CAN - scores 0-1). Duration of diabetes, HbA1c, plasma lipids were also assessed.
Results: ABPM values fore 24h BP in D and ND were142.3+12.1/89.9+9.1 mmHg and 144,1+10.7/92.6+9.33 mmHg (p=0,262/0,117), for daytime 144.9+8.3/90.7+11.1 mmHg and 146.2+9.4/93.9+11.3 mmHg (p=0,971/0,127) and for night-time 127.1+12.3/ 78.9+9.4 and 137.9+9.9/89.7+13.11 mmHg (p=0,000/0,000). HRV parameters -SDNN (0.104+0.046 vs 0.131+0.029, p=0,000), and Triangular index (24.3+8.3 vs 33.7+9.1 p=0,000) were significantly lower in ND compared to D. Prolongation of QTcd was statistically evident in ND (58.3+11.1 vs 45.3+11.3msec p=0,000) SMI episodes were more frequently found in ND, compared to D (44.8% vs 26.3%). We revealed following CAN prevalence in the study groups: severe 12.7% (D), 26.5% (ND), moderate 33.3% (D), 44.1% (ND), mild 44.1%(D) 26.5 (ND), no CAN 9.8% (D), 2.9% (ND). Severe and moderate CAN were more frequently observed in ND compared to D. There was significant difference in diabetes duration (13.1 vs 5.3 yrs, p=0,000) and HbA1c values (6.1±0.19 vs 7.2±0.31, p=0.000) between the goups.
Conclusion: Non-dipper pts showed association with CAN parameters. Our date suggest that relative sympathetic overactivity due to predominantly parasympathetic neuropathy might be responsible for the higher night blood pressure, lower HRV, and QTcd prolongation. CAN correlates to diabetes duration and glycemia levels. Autonomic function should be studied as part of cardiovascular risk assessment in diabetic pts with hypertension. 24-h ECG and BP monitoring and CAN tests may help to identification diabetics with poor prognosis.
533 Association of early chronic kidney disease with inappropiate left ventricular mass in hypertensive subjects
A Huerta1; MF Landecho1; I Colina1; I Alberola1; JM Araquistain1; O Beloqui1; J Diez2
Purpose: Inappropriate left ventricular mass (iLVM) has been defined as the excess LVM for the amount needed to sustain stroke work. The appropriateness of LVM to cardiac workload may be calculated by the ratio of observed LVM to the value predicted for an individual's sex, height, and stroke work at rest. iLVM is thought to be a condition that represents a phase of transition from compensatory LVM hypertrophy towards heart failure; thus the iLVM identifies individuals with an increased cardiovascular risk profile. Since even mild renal dysfunction is associated with an increased cardiovascular risk, we have studied, in hypertensive subjects, the relationship between early phases of chronic kidney disease (E-CKD) and the presence of iLVM.
Methods: 334 asymptomatic hypertensive subjects (mean age 50±0.5 years range 22 to 82 years, 78% males) with estimated GFR>60 ml/min∗1.73m2 entered the study. E-CKD was considered as the stages 1 and 2 of the K/DOQI CKD classification, that characteristically maintain normal GFR (>60 ml/min∗1.73m2) with an increased uACR (>177 mg/g in males and>255 mg/g in females).
Using echocardiographyc parameters, iLVM has been defined as observed LVM/predicted LVM>128%.
Results: Twenty-eight percent of patients exhibited iLVM. The prevalence of E-CKD in iLVM cases (37.9%) was significantly increased in comparison with hypertensive patients without iLVM (25.5%, p=0.025). Furthermore, the prevalence of iLMV in subjects with E-CKD (37.1%) appeared significantly higher than in cases with normal renal function (24.9%, p=0.025). Finally, after adjustment for age, sex, body mass index, systolic blood pressure and diabetes, E-CKD remained independently associated with iLMV, with and OR of 2,42 (95% CI 1.32-4.44, p=0.004).
In conclusion in hypertensive subjects, the presence of early stages of chronic kidney disease favors the development of iLMV, thus contributing to the increased global cardiovascular risk in these patients.
534 Can haemoglobin at admission predict short-term prognosis in Acute Coronary Syndrome patients?
N Antonio; S Monteiro; C Lourenco; R Teixeira; R Baptista; F Goncalves; P Monteiro; L Goncalves; M Freitas; L A Providencia; Coimbra, Portugal
Purpose: Anaemia is associated with worse prognosis in various conditions; however few studies have specifically examined its impact in acute coronary syndrome (ACS) patients. We aimed to assess the impact of baseline haemoglobin (Hb) in short-term prognosis of patients with ACS.
Methods: Retrospective analysis of a database containing 1552 consecutive patients admitted to a single coronary care unit for ACS (05/2004 to 07/2006). Baseline Hb were available in 84% of patients. This population (n=1303) was stratified by quartiles of Hb concentration: Q1,>10.8 g/dL; Q2,10.8-12.3 g/dL; Q3,12.3-13.3 g/dL; Q4, >13.3 g/dL.
Results: Hypertension and diabetes were more common in lower quartiles of Hb, while the proportion of cigarette smokers and physical inactivity increased with increasing Hb levels. Patients in lower quartiles of Hb showed higher proportions of previous congestive heart failure, peripheral artery disease and stroke. Anaemic patients tended to be significantly older, with significantly lower body mass index, lower LDL and triglycerides and worse renal and cardiac function. Patients in Q1 had significantly higher levels of peak troponin I and glucose (Table 1). Anaemic patients had significantly higher length of stay (Q1:6.1±4.4; Q2:5.2±3.0; Q3:4.9±2.7; Q4:4.3±2.1, p>0.001), in-hospital complications (Q1:10.5%; Q2:4.9%; Q3:3.5%; Q4:2.3%, p>0.001) and mortality (Q1:9.8%; Q2:6.3%; Q3:4.1%; Q4:3.6%, p>0.001). In multivariate analysis, independent predictors of in-hospital mortality were age75 and Killip class>1, but not anaemia. However, Hb>10.8 g/dl was an independent predictor of in-hospital morbidity as were age65.5 and Killip class>1.
Conclusion: In ACS patients, anaemia is associated with more co-morbidities, such as diabetes and renal failure.
Low baseline Hb can accurately predict in-hospital morbidity, but not in-hospital mortality
Baseline characteristics according to haemoglobin quartiles
Q1
Q2
Q3
Q4
p
Age
73.4±10.1
70.2±10.8
65.4±12.1
61.6±12.5
>0.001
BMI
26.6±3.8
27.0±4.0
27.0±4.0
28.1±4.1
>0.001
CrCl
47.3±32.6
59.7±32.4
74.0±32.9
83.2±48.4
>0.001
Tn I
37.0±57.0
35.0±67.0
34.0±60.0
28.0±52.0
>0.001
Glucose (dl)
177.2±123.7
154.5±78.4
153.5±69.3
142.9±62.0
>0.001
535 Meaning of mean platelet volume in acute coronary syndromes
A Tejedor; E Lopez De Sa-Areses; JR Rey-Blas; E Armada; J Ruiz-Cantador; L Pena-Conde; F Rivero-Crespo; D Dobarro; MC Gomez-Rubin De Celix; JL Lopez-Sendon; Madrid, Spain
Purpose: The quantification of mean platelet volume (MPV) is a simple method of assessing platelet function. Larger platelets are more active and have increased prothrombotic potencial. Previous studies have shown that in patients with acute corononary syndrome (ACS), MVP is higher than in patients with stable angina. The objective of this study is to determine whether increased MPV constitutes a simple association in patients with ACS or it could be a determinant factor in the setting of ACS (because it means platelet activation).
Methods: We evaluated MPV of the patients admitted between August 1st, 2006 and March 31st, 2007 with acute myocardial infarction (AMI). We compared MPV determined on arrival to the emergency department with a prior sample of MPV determined at least one week before (mean platelet life), non related with an ACS.
Results: During this period, 329 patients with AMI were admitted to the acute cardiac care unit. Patients with concomitant infective diseases, chronic haemodyalisis and AMI related to percutaneous intervention were excluded. Of the remaining patients, 138 had a prior determination of MPV. Previous analysis were obtained with a mean of 229 days (CI 63-622 days). MPV prior to admission was 8.6 fl and 8.4 fl on admission (NS). Only 6.6% had identical MPV, in 46.3% MPV was larger and in 44.2% smaller in the prior analysis than in the one obtained at the time of the hospitalization.
Conclusion: Although increased MPV is associated to ACS, it is not a determinant factor in the acute phase of the clinical event and we should consider it just a biological marker of risk for AMI.
536 Atherogenic Index of Plasma in European countries at different cardiovascular risk: a report from the IMMIDIET study
B Vohnout1; F Zito1; J Arnout2; FP Cappuccio3; M Van Dongen4; M De Lorgeril5; V Krogh6; A Siani7; MB Donati1; L Iacoviello1
1Catholic University Research Laboratories, Campobasso, Italy 2Katholieke Universiteit, Leuven, Belgium; 3Warwick Medical School Coventry, United Kingdom; 4Maastricht University, Maastricht, Netherlands; 5UFR de Medecine et Pharmacie, La Tronche, France; 6National Cancer Institute, Milan, Italy; 7National Research Council, Avellino, Italy
Cardiovascular (CV) risk in Europe is apparently distributed in a north-to-south gradient. Atherogenic Index of Plasma (AIP) - log(TG/HDL) in mmol/l, reflects distribution of particle sizes in HDL, LDL and VLDL. AIP is additive to other CV factors and increases with increasing CV risk. We compared AIP in European populations at different predicted CV risk.
Methods: 542 Italians (271 couples), 536 Belgians (268 couples), 526 English subjects (UK, 263 couples), and 207 mixed couples living in Belgium and formed by a member of Italian origin and their spouse of Belgian origin participated to a population-based cross-sectional study. Couples aged 30-60 years were recruited randomly from general practice.
Results: In contrast to predicted low CV risk in Italians, we found the highest AIP in Italian men and women (Table). LDL and cholesterol (TC) in Italian men were however lower compared to the other populations. Similarly, Italian women, showed LDL and TC lower than Belgian women. Both men and women from mixed couples showed the most favorable AIP values.
Conclusion: Our data on AIP does not support the hypothesis of north-to-south gradient of CV risk. Although low LDL and TC were found in Italians, the highest AIP levels suggest a higher proportion of atherogenic LDL and VLDL subpopulations compared to the other two European populations. Differences in AIP between Italians and mixed couples support the importance of trans-cultural life-style changes in control of CV risk.
Characteristics of lipid profiles
AIP log (TG/HDL)
HDL mg/dl
TG mg/dl
LDL-C mg/dl
CHOL mg/dl
Males
∗
∗
∗
$
£
Italian males
0.13±0.02
45.6±0.8
166.6±6.1
141.8±2.1
220.5±2.4
Belgian males
0.003±0.02
49.6±0.8
134.3±6.3
153.7±2.2
229.7±2.5
UK males
0.04±0.02
47.9±0.8
137.8±6.7
146.2±2.3
221.3±2.6
Males from mixed couples
−0.05±0.02
53.8±0.9
135.4±7.2
146.8±2.5
226.7±2.8
Females
∗
∗
∗
∗
∗
Italian females
−0.08±0.02
53.9±0.9
111.4±3.3
137.9±2.2
214.0±2.3
Belgian females
−0.18±0.02
60.0±0.9
97.8±3.3
145.8±2.2
225.4±2.3
UK females
−0.18±0.0.02
54.9±1.0
93.3±3.5
133.2±2.4
206.6±2.5
Females from mixed couples
−0.24±0.02
62.9±1.0
91.4±3.7
135.1±2.5
216.5±2.6
∗p>0.001; £p>0.005; £ p>0.05, all values are adjusted for age and smoking and are expressed as mean±SE.
537 High plasma adiponectin is related to low functional capacity in patients with chronic heart failure
I Laoutaris; I Vasiliadis; A Dritsas; S Mavrogeni; MS Kallistratos; A Manginas; A Chaidaroglou; D Degiannis; D Panagiotakos; DV Cokkinos
Onassis Cardiac Surgery Center 1st Cardiology Department, Athens, Greece
Purpose: Plasma adiponectin is associated with cachexia and increased mortality in chronic heart failure (CHF). We evaluated the relation of adiponectin with exercise capacity in patients with CHF.
Methods: In 57 patients (age 57.2±11.9 yrs, BMI 29.2±4.11 kg/m2 LVEF 28±8%) and in 17 healthy matched controls, plasma adiponectin and NT-proBNP were measured. All patients underwent cardiopulmonary exercise testing and 2-dimensional echocardiography. In 37 patients, the 6 min walk test (6MWT) was also conducted.
Results: Both adiponectin and NT-proBNP levels were elevated in CHF compared to controls (26.9±19.8 vs. 14.2±5.9, μg/ml, p>0.01), (1059.2±1109.1 vs. 360.5±91 pg/ml, p>0.001), respectively. Adiponectin correlated positively with NYHA functional class (r=0.434, p>0.001), NT-proBNP (r=0.574, p>0.001) and inversely with peak VO2 (r=-0.474 p>0.001) and 6MWT distance (r=-0.398, p>0.05) independent of age, sex, BMI, LVEF. Adiponectin values>27.8 μg/ml showed 81% sensitivity (sn) and 79% specificity (sp) for detecting peakVO2>14 ml/kg/min (AUC=0.80, p>0.01). Adiponectin values>31 μg/ml showed 80% sn and 78% sp for detecting peak VO2>10 ml/kg/min (AUC=0.86, p>0.01). Adiponectin values>30 g/ml showed 86% sn and 87% sp for detecting walking distance>300m (AUC=0.90, p>0.001).
Conclusion: High adiponectin level was independently associated with reduced exercise capacity and may have a place as an index to identify low functional class CHF patients.
538 An association of a low grade albuminuria measured by urine albumin creatinine ratio with metabolic syndrome in non-diabetic general population: Atherosclerosis risk of rural area in north general
1Wonju Christian Hospital Department of Cardiololy, Wonju, Korea, Republic of; 2Wonju College of Medicine Yonsei University Cardiology, Wonju Kangwondo, Korea, Republic of
Background: Microalbuminuria is a prognostic marker for cardiovascular risk regardless of the presence of diabetes. However, data are limited with regard to the relationship between low-grade albuminuria (below the microalbuminuria threshold) and metabolic syndrome (MetS) in non-diabetic individuals. We investigated an association between albuminuria below 30 g/mg and MetS in Korean non-diabetic general population.
Methods: The study subjects were selected from a Korean Genomic Rural Cohort, an ongoing epidemiologic study conducted on a representative senior population (age>40 years) of Koreans. It enrolled 2,600 nondiabetic general population (mean age; 56 years; male; 40%) with low grade urinary albuminuria (spot urine albumin creatinine ratio [UACR] >30 μg/mg). We examined associations among MetS itself, its components and UACR values.
Results: The prevalence of MetS was 24.3% (male; 19.2%, female; 27.6%). The UACR values as a continuous variable were significantly correlated with the components of MetS, systolic blood pressure (beta=0.06, p=0.003), total cholesterol (beta=0.059, p=0.003), triglyceride (beta=0.078, p>0.001), HDL-cholesterol (beta=-0.085, p>0.001) and fasting blood glucose (beta=0.046, p=0.019). The multivariate logistic regression showed the UACR as a continuous variable were independently associated with MetS (odd ratio, 1.02; 95% CI, 1.005 to 1.034, p=0.008).
Conclusion: UACR values even in below >30 μg/mg are independently associated with MetS itself and its components in Korean general population.
539 Update of the Portuguese familial hypercholesterolemia study
AM Medeiros1; AC Alves1; S Silva1; M Mafalda Bourbon2
1Instituto Nacional de Saude Dr. Ricardo Jorge Cardiovascular Research Unit, Lisboa, Portugal; 2Instituto Nacional de Saude Dr Ricardo Jorge Centro de Biopatologia, Lisboa, Portugal
Introduction/Aim: Familial hypercholesterolaemia (FH) is an inherited disorder of cholesterol metabolism characterized by defective clearance of plasma LDL that results in increased circulating LDL-cholesterol, leading to premature atherosclerosis and coronary heart disease (CHD). FH is caused mainly by mutations in LDL receptor (LDLR) gene but missense mutations in APOB or PCSK9 genes also cause a similar phenotype. Portugal should have about 20 000 cases of FH but this disorder is severely under diagnosed in our country. Since 1999 the “Portuguese FH Study” has studied more than 800 individuals with the collaboration of clinicians countrywide. The major aim of this study is the molecular study of patients with clinical diagnosis of FH.
Methods: Blood samples were collected from 259 unrelated patients with clinical diagnosis of FH and 562 (affected and unaffected) relatives. LDLR gene was analysed by PCR, DHPLC and/or direct sequencing and MLPA. Fragments corresponding to exon 26 and exon 29 of the APOB gene and the 12 exons of the PCSK9 were analysed by PCR and direct sequencing.
Results and Conclusion: Sixty four different mutations in the LDLR gene were detected in 288 individuals, 38 previously described and 26 exclusive of the Portuguese population. Two of these patients were homozygous and 2 patients were compound heterozygous. Additionally, 9 subjects carried the APOB3500 mutation and 1 carried a non described APOB mutation (Y3533C). Three had a PCSK9 mutation and presented the most severe phenotype. The molecular identification of FH patients is important for the correct identification of the disease and is useful to establish the most adequate treatment in order to prevent premature CHD common in these patients.
540 Functional characterization of missense mutations found in Portuguese patients with a clinical diagnosis of familial hypercholesterolemia
M Bourbon1; S Silva2; AC Alves2; D Patel3; AM Medeiros2; MA Duarte3; AK Soutar3
1Instituto Nacional de Saude Dr Ricardo Jorge Centro de Biopatologia, Lisboa, Portugal; 2Instituto Nacional de Saude Dr. Ricardo Jorge Cardiovascular Research Unit, Lisboa, Portugal; 3MRC-Clinical Science Centre, Hammersmith Hosp Lipoprotein Group, London, United Kingdom
Introduction: Mutations in the LDLR gene are the major cause of Familial Hypercholesterolemia, resulting in defective catabolism of LDL and premature atherosclerosis and coronary heart disease. The aim of this study is the functional characterization of novel missense and putative splice site mutations in LDLR.
Methods: Different LDLR mutants were generated by site-directed mutagenesis and expressed in CHO-ldlA7 cells lacking endogenous expression of LDLR. To determine the effects of mutations on LDLR function, saturable binding plus uptake and degradation of 125I-labelled LDL was measured at 37†C. Cell-surface expression of wild-type and mutant LDLR proteins was also investigated. The putative splicing mutations were analysed by RNA extraction from patient lymphocytes and RT-PCR.
Results: Cells expressing constructs W469R and V408L were severely impaired in their ability to mediate uptake and degradation of 125I-LDL (C, c.2389G>T (V776L), c.1060+1 G>A, c.2547+1 G>A caused exon skipping, and one caused retention of an intron c.1359-5C>G. Variants c.1061-8T>C and c.2140+5G>A had no effect on splicing.
Conclusion: Our findings emphasize that functional assays are necessary to prove mutation pathogenicity and to understand the functional effect of each mutation on which therapeutic treatment can be based. Care must be taken before reporting the presence or absence of a mutation in the LDLR gene for diagnostic purposes to avoid genetic misdiagnosis of FH patients.
541 The origin and differentiation potential of smooth muscle cells in coronary atherosclerosis
I Vukovic1; A Aleksic2; NN Arsenijevic1; AA Aleksic2
1Faculty of Medicine Institute of Histology and Embryology, Kragujevac, Serbia; 2KBC Zemun Cardiology, Belgrade, Serbia
The purpose of this work was determination of morphological state of endothelium, origin of foam cells, phenotip state of smooth muscle cells as well as investigation of continuity of inner elastic membrane during the evolution of atherosclerotic lesion.
Twenty one sample of atheroscleroticaly changed right coronary artheries divided in 6 stages, were analysed. The tissues were fixed in formalin and embedded in paraffin. Sections of 5 m thickness were stained by Weigert van Gieson-s, Grossman Mallory-s, Azzan Heidenhein-s, orcein, PAS and alcian blue-PAS reaction. Immunocytochemical staining were performed using an LSAB+/HRP kit (Dako), for identification of vimentin, -smooth muscle actin (−SMA), S-100 protein, CD31, CD34, CD68 and Proliferating Cell Nuclear Antigen (PCNA).
Results: Of this study have shown at first functional and then morphological damage of endothel, in the late stages of atherosclerosis. On the stage of preatheroma, revealed the presence of intimal dedifferentiation of smooth muscle cells with expression of vimentin and α-SMA and lack of expression of desmin. Described changes progressed going to the later stages of atherosclerosis. Along with these changes a huge number of foam cells of variant origin can be noticed. Some of them are developing from monocite-macrophages lineade (CD68-immunoreactive) and the others origin of smooth muscle cells (vimentin and S-100 immunoreactive). In late stages during state of atheroma includes intimal changes with forming a lipid core (S-100 immunoreactive cells and cell necrosis) while fibrosis in the lipid core and accumulation of colagen fibres with extreme hypocellularity are characteristics of stage of fibroatheroma.
542 Defining an optimal LDL threshold indicating a high likelihood of normal apolipoprotein B levels in patients with coronary artery disease
JA Stone1; SA Aggarwal1; B Brown1; A Dottridge1; R Ross Arena2
1Cardiac Wellness Institute, Calgary, Canada; 2VCU Physical Therapy, Richmond, United States of America
Purpose: Serum LDL level is a well-accepted measure with respect to defining risk for future adverse vascular events. Recent investigations have suggested that serum levels of apolipoprotein B (apo B), the primary LDL apolipoprotein, may reflect the presence of small dense LDL (sd-LDL) particles. These sd-LDL particles may be more readily incorporated into arterial endothelium, thereby accelerating the atherosclerotic process and potentially increasing the frequency of cardiovascular events. Thus, apo B levels may be a better marker of vascular risk than LDL levels alone. The purpose of the present study is to determine an LDL threshold that optimally indicates a high likelihood apo B is normal.
Methods: One hundred and fifty-six subjects (133 male/23 female, mean age: 60.9 ± 10.4 years) diagnosed with coronary artery disease and referred to cardiac rehabilitation (CR) participated in this analysis. Ninety-six percent of the subjects were on a lipid-lowering medication. Lipid analysis was performed at program entry to determine LDL (mmol/L) and apo B (g/L). An apo B value >0.90 g/L was considered normal.
Results: Twenty-one subjects (13.5%) presented with an apo B value 0.90 g/L. Receiver operating characteristic curve analysis revealed the LDL classification scheme was highly effective in identifying individuals with an abnormal apo B value (Area under the curve: 0.89, 95% confidence intervals: 0.81-0.98, p>0.001). The optimal LDL threshold for identifying patients with a normal apo B value was >1.8111 mmol/L (sensitivity: 67%, specificity: 90%). Only two of 93 subjects (2.2%) with an LDL >1.8111 mmol/L presented with an apo B >0.90 g/L. Using an LDL threshold of >2.5999 mmol/L, sensitivity improved (99%) while specificity was reduced (48%). Ten of 52 patients (19.2%) with an LDL between 1.81 and 2.5999 mmol/L presented with an apo B >0.90 g/L. Lastly, nine of 11 patients (81.8%) with an LDL >2.5999 mmol/L had an apo B >0.90 g/L.
Conclusion: Research supporting the clinical implementation of apo B assessment continues to mount. If an apo B value is not available, an LDL >1.8111 mmol/L may indicate a high likelihood that this important marker of cardiovascular risk is within normal limits. However, a substantial percentage of individuals with an LDL >2.5999 mmol/L (a widely accepted goal for patients with coronary artery disease) but >1.8111 mmol/L, may have apo B values >0.90 g/L. Lastly, in this population of CR patients, the likelihood of an elevated apo B value appears to be extremely high when the LDL >2.5999 mmol/L.
543 Plasma total cysteine is independently associated with cardiovascular risk burden in healthy subjects
V Sedda1; R De Maria1; M Parolini1; M Bianchi1; J Campolo1; G Pizzi2; O Disoteo2; C Dellanoce1; G Cighetti3; O Parodi1
1CNR Clinical Physiology Institute Cardiovascular Department, Niguarda Hospital, Milan, Italy; 2Diabetologic-Metabolic Unit, Niguarda Hospital, Milan, Italy; 3Department Preclinic Sciences LITA Vialba, University of Milan, Milan, Italy
Purpose: Cardiovascular risk factors (RF) are responsible for atherosclerosis development and oxidative stress is involved. Aim of this study was to assess whether redox analysis may provide sensitive markers of oxidative processes associated to an increasing RF burden, independently of RF type.
Methods: We classified 304 healthy subjects [169 males, 53 (43, 63) years] into 4 groups according to number of RF (smoking, hypertension, hypercholesterolemia, hyperhomocysteinemia, diabetes and obesity), irrespective of type (group 0, 1, 2, and 3 if = 3 RF). Eighty-one (27%), 95 (31%), 80 (26%), and 48 (16%) subjects belonged to group 0, 1, 2 and 3, respectively. Oxidative stress was evaluated by measuring plasma total and reduced aminothiols [homocysteine (HCy), cysteine (Cys), glutathione (GSH), cysteinylglycine (CG)], blood reduced glutathione and malondialdehyde (MDA).
Results: Plasma total thiol levels (micromol/L) were HCy 9.5 (7.4, 14.1) Cys 250 (210, 291), GSH 5.5 (4.1, 7.3), CG 31 (24, 42); MDA was 0.76 (0.47, 1.34). Cys increased with a greater RF burden (Figure). By multivariable ordinal regression analysis adjusted for age and gender, plasma total Cys was the only redox variable associated to a higher number of RF (OR=1.006 per unit change, 95% CI 1.003 to 1.010; p=0.002).
Conclusion: The total RF burden is associated with raised extracellular total Cys levels. A pro-oxidant pattern of increasing severity characterizes subjects with RF. This finding underscores the role of redox imbalance as possible mediator of global cardiovascular risk.
Figure
544 Hyperuricaemia, a Forgotten Risk Factor? Is it important in the Setting of Acute Coronary Syndrome (ACS)?
S Pernencar1; M Peres2; J Aranha2; I Monteiro2; A Francisco2; V Martins2; M Pitta2; M Leal2; J Loureiro2; G Silva2
1Leiria, Portugal; 2Santarem, Portugal
Purpose: Hyperuricaemia is been considered a cardiovascular risk factor for a long time, though there are few data reporting the prevalence of hyperuricaemia in the setting of ACS and its prognostic value. The aim of this study is to determine the prevalence and the prognostic value of hyperuricaemia.
Methods: We retrospectively analysed data from 530 consecutive and randomised patients (pts) who were hospitalized at our center with ACS, during 2004 through 2006. Patients were divided in two groups: in Group A included those who had serum Uric Acid (UA) level >77 mg/dl and/or in treatment with Allopurinol (n=130); and Group B, those who had normal UA level (n=400).
The primary endpoint of the study was the incidence of any of the following major events (MACE): death, myocardial infarction and stroke.
Results: Female gender was more prevalent in group A (36.9% vs 27.5%, p=0.041). There were also differences comparing both Group A and Group B, in regard of cardiovascular risk factors: patients in Group A had a higher risk profile, with increased prevalence of hypertension (51% vs 27%, p>0.001), hypercholesterolemia (57% vs 42%, p=0.004), smoker (71% vs 52%, p>0.001) and previous MI (48% vs 32%, p=0.002). There ware no differences on the type of ACS, medical treatment and percutaneous angioplasty.
Patients in group A had a worse in-hospital outcome: left ventricular dysfunction (38% vs 10%, p>0.001), sustained ventricular arrhythmia (9% vs 2.5%, p=0.001), stroke (9% vs 0.5%, p>0.001), recurrence of MI (6% vs 0.3%, p>0.001) and death rate (15% vs 1%, p>0.001).
Conclusion: In “real world” practice, patients with hyperuricaemia had a higher risk profile and worse prognosis due to higher rates of repeat ACS, stroke and death.
545 Circulating endothelial progenitor cells and low-dose-aspirin-insensitive thromboxane biosynthesis in polycythemia rubra vera
B Rocca; F Santilli; A Recchiuti; A Dragani; A Falco; F Fioritoni; G Lessiani; S Lattanzio; D Mattoscio; G Davi
University of Chieti, Chieti, Italy
Purpose: Polycythemia vera (PV) is a myeloproliferative disorder associated with high morbidity and mortality for thrombosis. We hypothesized that in PV reduced sensitivity to aspirin may be related to impairment of endothelial repair mechanisms as well as of the nitric oxide (NO) system.
Methods: In 37 PV patients on chronic low-dose aspirin, we evaluated thromboxane (TX)A2 biosynthesis, in parallel with endothelial colony-forming cells (ECFCs) and plasma levels of dimethylarginine (ADMA), an endogenous NO inhibitor.
Results: Compared to non-aspirinated healthy subjects, PV patients showed significantly higher median urinary 11-dehydro-TXB2 (TXM) and plasma ADMA levels (P>0.0001), whereas they displayed a reduced number of ECFCs (P>0.0001). Multiple regression analysis showed that lower ECFCs quartiles (Beta=-0.61; SE=0.13; P=0.001, R2=0.375) were the only independent predictors of higher TXM quartiles.
Conclusion: These results indicate that PV patients have a profound perturbation of ECFC/NO axis, which may contribute to aspirin-insensitive TXM formation. Thus, additional antithrombotic strategies may be required in PV.
546 Atorvastatin reduces C-Reactive Protein and Vascular Cell Adhesion molecule levels independently of low density Lipoprotein in hypercholesterolemic individuals
TSF Leong1; D Ward1; A Fitzgerald2; P Gaffney1; J Fogarty1; G Boran1; I Graham1
Background: The benefits of statins in reducing cardiovascular risk may extend beyond that of cholesterol lowering. This so-called pleotrophic effect of statins has been attributed to an unmeasured effect on novel risk factors associated with cardiovascular disease. Previous experiments have suggested that statins may reduce inflammation and cell adhesion. The present study examined whether atorvastatin reduces CD40 ligand (CD40L), Vascular Cell Adhesion molecule (VCAM) and C-Reactive Protein (C RP) levels in hypercholesterolemic individuals independently of cholesterol.
Methods: We measured baseline CD40L, VCAM and CRP levels in 34 volunteers from a hospital staff screening initiative who were identified as being hypercholesterolemic where statin therapy is indicated. After 16 weeks of treatment with atorvastatin 100 mg, the subjects were reexamined.
Results: Correlations at baseline with LDL cholesterol were: CD40L (r=0.22, p=0.22), VCAM (r=-0.25, p=0.16), CRP (r=0.03, p=0.84). Table 1 compares the median values after 16 weeks of treatment with atorvastation. In generalized linear models also adjusting for age and sex, the reduction in LDL cholesterol was not significantly associated with the reduction in VCAM and CRP.
Conclusion: Atorvastatin reduces CRP and VCAM but not CD40 ligand levels in individuals with hypercholesterolemia. This effect on inflammation and cell adhesion appears to be independent of LDL cholesterol lowering.
Before treatment
After treatment
P value
Cholesterol (mmol/L)
6.1
4.2
>0.0001
LDL Cholesterol (mmol/L)
3.9
2.3
>0.0001
CD40 ligand (pg/L)
156
161
0.57
VCAM (ng/mL)
588
532
0.0002
CRP (mg/L)
2.20
2.05
0.0006
547 Up-regulation of platelet gp 91phox in patients with hypercholesterolemia relationship with urinary isoprostanes
P Pignatelli1; R Carnevale1; L Loffredo1; V Sanguigni2; S Di Santo1; F Martino1; F Violi1
1University of Rome La Sapienza Experimental Medicine & Phatology Department, Rome, Italy; 2University of Rome Tor Vergata, Rome, Italy
Background: Enhanced formation of reactive oxidant species (ROS) has been observed in hypercholesterolemic patients but the underlying mechanism is still unclear.
Methods and Results: Urinary excretion of isoprostanes, a marker of oxidative stress, platelet expression of gp91phox, the catalytic unit of NADPH oxidase, and platelet production of O2- were measured in 50 children and 50 adults with normal or high serum cholesterol. The above reported variables were also measured in 4 patients with hereditary deficiency of gp91phox. Hypercholesterolemic adults had higher platelet gp91phox expression and O2− formation compared to controls. Similar findings were obtained in hypercholesterolemic children compared to controls. Patients with hereditary deficiency of gp91phox expressed a significantly lower gp91phox on platelet surface and lower production of platelet O2− compared to healthy subjects. Adults with hypercholesterolemia had significantly higher urinary excretion of isoprostanes compared to controls. Similar findings were obtained in hypercholesterolemic children compared to controls. Patients with hereditary deficiency of gp91phox showed a significantly lower excretion of urinary isoprostanes compared to healthy subjects. Platelet expression of gp91phox significantly correlated with platelet production of O2− and urinary excretion of isoprostanes in adults and children.
Conclusion: The study provides the first evidence that in hypercholesterolemia platelet gp91phox, a useful new marker of oxidative stress, is up-regulated and may be responsible for enhanced production of isoprostanes.
correlation
548 (WITHDRAWN) Association of differing measures of body fat and body fat distribution with prevalent inflammation - the Heartsake Study
A Schmidt-Trucksaess1; K Winkler2; T Schuster1; L Klatt3; K Boettcher1; E Bitzer4; M Halle3; H-H Dickhuth4; M Sandrock5
Purpose: The purpose of this study was to evaluate the association between elevated levels of high sensitive C-reactive protein (hs-CRP), different body fat measurements and body fat distribution in a large female population-based sample from Eastern Germany.
Methods: Using data from the Heartsake Study, we investigated how different measures of obesity (such as body mass index (BMI), waist circumference (WC), subscapular (SC) and biceps skinfold (BC)) related to elevated hs-CRP (>33 mg/l), a marker of inflammation.
Results: Of the 3.872 female subjects taking part in the study, 976 (25.2%) were found to have an elevated hs-CRP. A J-shaped relationship between hs-CRP and all measures of body fat distribution was observed using a univariable linear regression analysis. The odds were greater for each quintile above the third quintile for BMI and WC compared with SC and BC. After adjustment for age and diabetes (HbA1C>6%), hs-CRP was significantly increased in all quintiles of BMI [OR second quintile 1.62, 95% confidence interval (CI) 1.15 to 2.27, OR fifth quintile 3.90, 95% (CI) 2.49 to 6.09] and in the fourth [OR 1.50, 95% (CI) 1.15 to 2.08] and the fifth quintile of BC [OR 2.30, 95% (CI) 1.68 to 3.16] and the fifth quintile of WC [OR 1.70, 95% (CI) 1.17 to 2.59]. Hs-CRP was not significantly increased in any quintile of SC.
Conclusions: The data presented in this cross-sectional study provide support to the association found between subcutaneous and visceral adipose tissue and inflammation in a large female population sample. The data suggest that extra- and intra-abdominal fat compartments contribute to inflammation and thus should be measured in risk assessment of cardiovascular diseases.
549 Plasmatic levels of apolipoprotein in young subjects without cardiovascular disease: influence of age, gender and body mass index
DA Siniawski; WM Masson; P Sorroche; W Scordo; L Casanas; J Krauss; AM Cagide; Hospital Italiano Cardiology, Buenos Aires, Argentina
Background: Cardiovascular risk scores have low sensibility to stratify young people. Plasmatic levels of Apolipoproteins (AL) could increase this sensibility. The distribution of AL levels is unknown in subjects less than 50 years old in our region.
Objetive: Establish the distribution of AL levels according to age, gender and body weight in a healthy population >50 years old.
Methods: The apolipoprotein A1 (A) and apolipoprotein B (B)levels were determinated by kinetic nephelometry in samples obtained of blood givers less than 50 years old. The distribution according to sex, age (groups >30, 30-40,>40 years old) and body mass index (BMI) was analyzed.
Results: 338 patients were recruited. Mean age±SD: 33±9 years, 70% men(M). Mean BMI±SD: 25,53±4,4. 52% of the population had BMI >25 (mean±SD 22,3±2) and 48% BMI >25 (mean±SD 28,9±3,6). The levels in the population (mean±SD) were: A 147±32 mg/dL, B 91 ± 26 mg/dL, B/A ratio 0,64±0,22. The levels of A were higher in women (W) than in M in the global analysis (164±38 mg/dL vs. 141±26 mg/dL, p>0.0001) and in the younger groups (>30 years: 166±40 mg/dL vs. 138±26 mg/dL, p>0.005; 30-40 years: 168±36 mg/dL vs. 140±25 mg/dL, p>0.0001). The group>40 years showed a not statistically significant tendency (156±37 mg/dL vs. 147±26 mg/dL, p=0.1). The levels of B were lower in W than in M in the global analysis (80±21 mg/dL vs. 95±26 mg/dL, p>0.0001) and in the older groups (30-40 years: 80±23 mg/dL vs. 102±25mg/dL, p>0,005;>40 years: 85±19 mg/dL vs. 109±25 mg/dL, p>0.005). The group >30 years showed a not statistically significant tendency (76±21 mg/dL vs. 80±23 mg/dL, p=0.3). The B/A ratio was higher in M than in W (0,69±0.21 vs. 0,50±0.14, p>0,0001). The subjects with BMI >25 had higher A levels (153±36 vs. 142±26 mg/dL, p>0.01) and lower B levels (83±25 vs. 99±25 mg/dL, p>0.0001) than patients with a BMI>25. When we analyze these data according to sex, we find the following results: W(A 167±41 vs. 151±20, p=0.07; B 79±21 vs. 85±23, p=0.17), M (A 141±25 vs. 140±26, p=ns; B 86±27 vs. 101±25, p>0.0001).
Conclusion: In this population, W had lower levels of B, lesser B/A ratio, and higher concentrations of A levels than M. BMI and age affected the levels of apolipoproteins. These results could be used to improve the risk stratification in young people.
550 Association of low-grade inflammation and platelet activation in hypertensive patients with microalbuminuria
G Davi1; F Santilli1; P Ferroni2; MT Guagnano2; MR Manigrasso2; N Michetti2; F Guadagni1; S Basili3
1University of Chieti, Chieti, Italy; 2IRCCS San Raffaele, Rome, Rome, Italy; 3University of Rome, Rome, Italy
Purpose: Increased levels of soluble CD40 ligand (sCD40L) have been associated with enhanced in vivo platelet activation, and may represent a molecular link between inflammation and prothrombotic state. We aimed at analyzing the relationship among platelet activation, endothelial dysfunction low-grade inflammation and sCD40L in hypertensive patients with or without microalbuminuria (MA).
Methods: A cross-sectional comparison of sCD40L levels was performed in 25 patients with essential hypertension and MA (MH) pair-matched for gender and age with 25 patients with essential hypertension (EH) and 25 healthy normotensive subjects (HS). Circulating C-reactive protein (CRP, marker of inflammation), sP-selectin (marker of in vivo platelet activation), asymmetric dimethylarginine (ADMA) and von Willebrand Factor (vWF) (markers of endothelial dysfunction) levels were analyzed in each subject.
Results: sCD40L levels were increased in MH patients compared to either EH (p>0.001) or HS (p>0.0001). A highly significant correlation between plasma sCD40L and sP-selectin (p>0.0001), vWF (p>0.001) or CRP levels (p>0.05) was observed in MH patients. Multivariate regression analysis showed that sP-selectin was the strongest independent predictor of sCD40L levels (p>0.0001) in MH patients. Hypertensive patients with both vWF and CRP levels above the median had the highest sCD40L levels (p>0.0001). Factorial ANOVA analysis of all hypertensive subjects confirmed that only MH patients with low-grade inflammation had elevated levels of sCD40L.
Conclusion: sCD40L levels appear to discriminate a subset of patients characterized by microalbuminuria and low-grade inflammation, suggesting that inhibition of the CD40/CD40L system may represent a potential therapeutic target in hypertensive subjects at high risk for cardiovascular events.
551 Relations of vitamin D concentrations with left ventricular geometry and function
E Ingelsson1; P Bergea Af Geijerstam1; J Sundstrom1; TJ Wang2; J Arnlov2; L Lind2
1Uppsala University Department of Public Health and Caring Sciences, Uppsala, Sweden; 2Massachusetts General Hospital, Boston, United States of America
Purpose: Circulating vitamin D concentrations have been related to cardiovascular risk factors and overt cardiovascular disease (CVD) in humans, but data regarding associations with subclinical CVD are scarce. Further, animal studies support a role for vitamin D in the development of left ventricular (LV) hypertrophy and dysfunction. Thus, we examined relations of serum 25-dihydroxyvitamin-D (25-OH D) concentrations to echocardiographic measures of LV geometry and function in a community-based sample of elderly.
Methods: We measured 25-OH D concentrations and performed routine echocardiography in 870 70-year-old participants of the Prospective Study of the Vasculature in Uppsala Seniors (PIVUS) study (52% women), free of heart failure, valvular disease and prior myocardial infarction. Multivariable regression analyses were performed to examine relations of 25-OH D to LV mass, wall thickness, end-diastolic diameter, left atrial diameter, fractional shortening, LV isovolumic relaxation time, and E/A-ratio.
Results: Adjusting for sex, examination date, and height, serum 25-OH D was negatively associated with LV mass, end-diastolic diameter, and left atrial diameter, and positively associated with fractional shortening and E/A-ratio. In fully adjusted models (adjusting for sex, examination date, height, weight, smoking, diabetes, total cholesterol, high-density lipoprotein cholesterol, creatinine, systolic blood pressure, anti-hypertensive treatment, and history of stroke, angina pectoris or interventional treatment of the coronary arteries), 25-OH D concentrations were significantly associated with fractional shortening (β 0.7% per 1-standard deviation increase in 25-OH D; P=0.010). Fractional shortening increased in a linear fashion over sex-specific quartiles of 25-OH D (Q1: 66.4%; Q2: 66.9%; Q3: 67.7%; Q4: 68.0%; P for trend, 0.028 in fully adjusted models). There were no sex differences with regard to relations between 25-OH D and echocardiographical measures (P>0.1 for all interaction terms).
Conclusion: In our community-based sample of elderly, higher serum 25-OH D was related to higher fractional shortening, a measure of LV systolic function, even after adjustment for potential confounders. This could indicate that vitamin D deficiency may increase the risk for overt CVD through influence on LV function; however, this hypothesis needs to be evaluated in further studies utilizing longitudinal data.