
Abstract

Introduction
This article is based on the current European Guidelines on Cardiovascular Disease Prevention in Clinical Practice [1] with the addition of some new information. The encouragement of ‘total risk estimation’ as a crucial tool to guide patient management has been a cornerstone of the guidelines since the first (1994) edition [2]. This is because, in many people, cardiovascular risk reflects the combined effects of several risk factors that may interact, sometimes multiplicatively. That said, certain individuals declare themselves to be at high risk and deserve the most intensive risk factor advice. These are:
Patients with established atherosclerotic cardiovascular disease (CVD), whether of the coronary, peripheral, cerebral vessels, or the aorta, even if asymptomatic.
Asymptomatic individuals who are at high risk of symptomatic CVD because of:
Diabetes type 2 and diabetes type 1 with microalbuminuria.
Markedly raised levels of single risk factors, especially if associated with end-organ damage.
The presence of multiple risk factors.
For the latter, the use of a risk estimation system is recommended such as the Systematic Coronary Risk Estimation (SCORE) system described below.
Total risk estimation
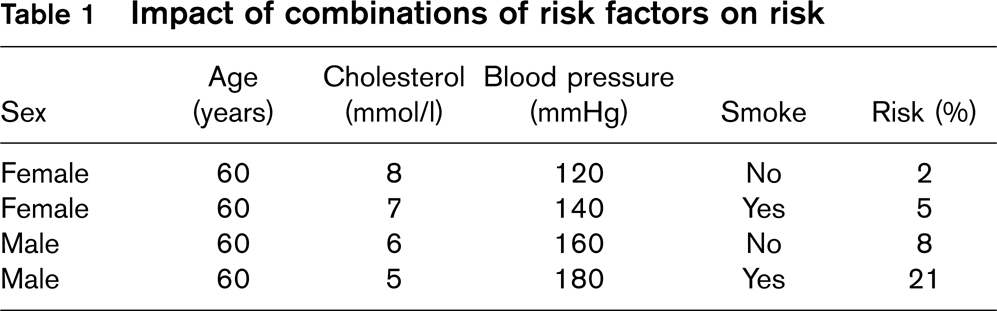
Cardiovascular risk in the context of the Joint European Guidelines means the likelihood of a person developing an atherosclerotic cardiovascular event over a defined period of time. ‘Total risk’ implies an estimate of risk that is made by considering the effect of the major factors such as age, sex, smoking, blood pressure, and lipid levels. Although the term has become widely used, it is acknowledged that is not comprehensive, in that the effects of other risk factors are not considered except as qualifying statements. The importance of total risk estimation before management decisions are made is illustrated in Table 1 and Fig. 1. Fig. 1 illustrates that the effect of lipid levels on risk is modest in women who are at otherwise low risk, and that the risk advantage of being female is lost by the combination of smoking and mild hypertension. Table 1 shows that a person with a cholesterol of 8 mmol/l can be at 10 times ‘lower’ risk than someone with a cholesterol of 5 mmol/l if the latter is a male hypertensive smoker. Randomized controlled drug trials of single risk factors do not give sufficient data to fully address these issues. Although audits such as European Action on Secondary And Primary Prevention by Intervention to Reduce Events (EUROASPIRE) [3] suggest inadequate risk factor management in very high-risk patients, it is also likely that, in the context of low-risk patients who have not had a vascular event, there is potential for substantial overuse of drugs by inappropriate extrapolation of the results of trials conducted mostly on high-risk men to low-risk individuals. In general, women and old and young participants have been underrepresented in the classic drug trials that have informed guidelines to date. For these considerations to have an impact on clinical practice, it is essential for the clinician to be able to assess risk rapidly and with sufficient accuracy to allow logical management decisions. This realization led to the development of the risk chart used in the 1994 and 1998 Guidelines [2] This chart used American data from the Framingham study and methods pioneered by Anderson and the applicability of the chart to all European populations was uncertain. Other systems are available, including the UK QRISK system [4], Prospective Cardiovascular Münster (PROCAM) in Germany [5], and ASSIGN in Scotland [6]. The 2003 Guidelines [7] used a new system for risk estimation called the Systematic Coronary Risk Estimation project (SCORE) [8], based on data from 12 European cohort studies and includes 205 178 patients examined at baseline between 1970 and 1988 with 2.7 million years of follow-up and 7934 cardiovascular deaths. The SCORE risk function has been externally validated using different datasets [9]. Risk charts such as SCORE are intended to facilitate risk estimation in ostensibly healthy persons. As noted in the introduction, patients who have had a clinical event such as an acute coronary syndrome or stroke have already declared themselves to be at high risk of a further event and automatically qualify for intensive risk factor evaluation and management.
Impact of combinations of risk factors on risk
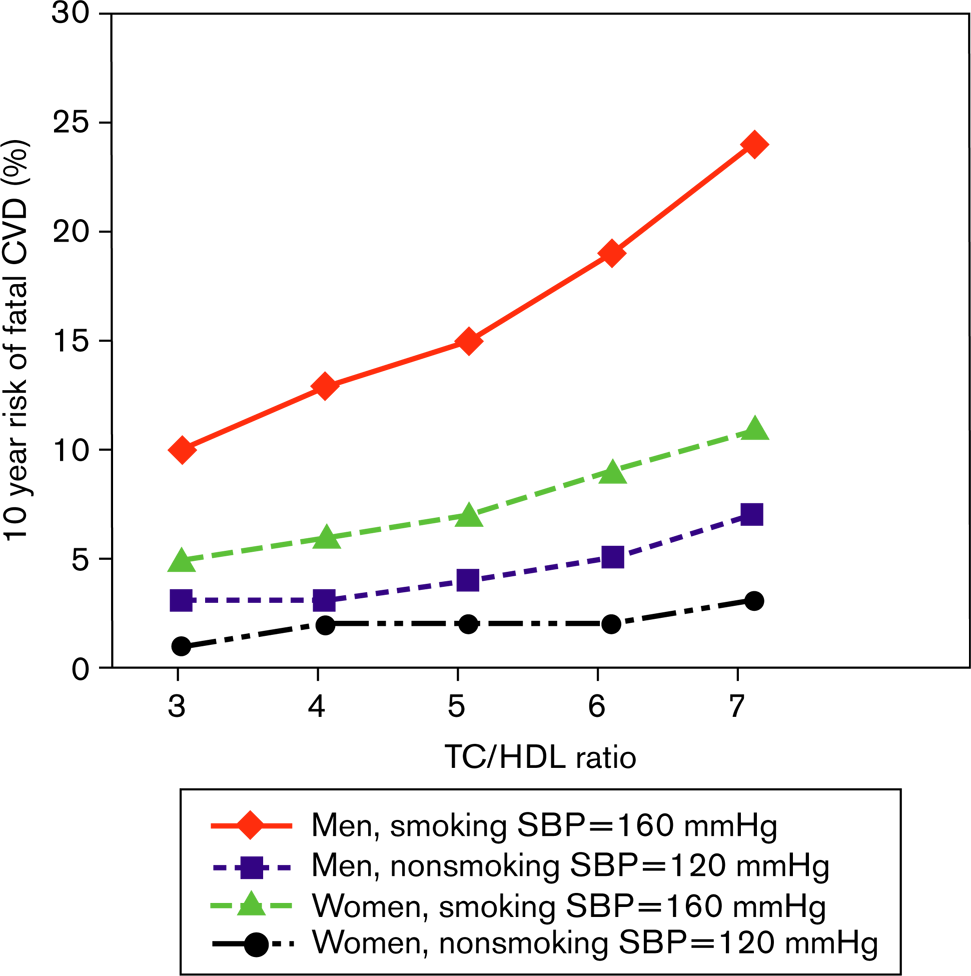
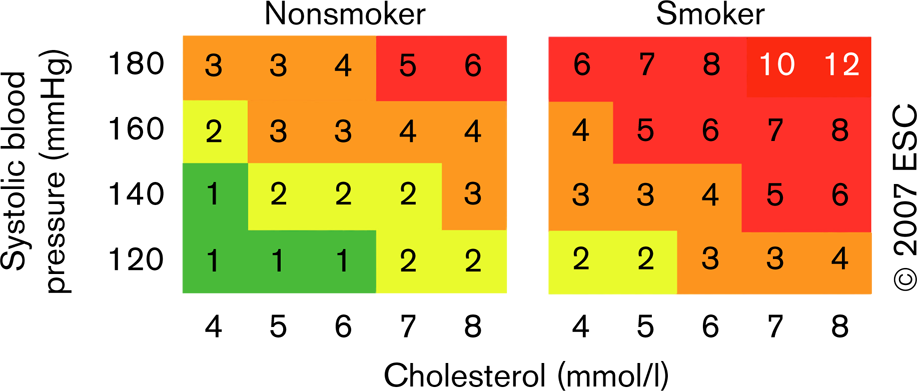
The relationship of total cholesterol (TC)/high-density lipoprotein (HDL) cholesterol ratio to 10-year fatal cardiovascular disease (CVD) events in men and women aged 60 years with and without risk factors, based on a risk function derived from the Systematic Coronary Risk Estimation (SCORE) project. SBP, systolic blood pressure.
When to assess total CVD risk?
Upon the patient's request.
If during a consultation:
There is obesity, especially abdominal.
One or more risk factors such as raised blood pressure, lipids, or glucose.
The person is a middle-age smoker.
There is family history of previous diseases, premature CVD, or major risk factors such as hyperlipidaemia, smoking, exercise, and dietary habits.
Symptoms suggestive of CVD.
How to assess total CVD risk?
The SCORE risk charts are shown in Figs 2–6, including a chart of relative risks. Instructions on their use and qualifiers are as follows:
This relative risk chart is useful in explaining to a younger person that, even if his/her absolute risk is low, it may still be 10–12 times higher than that of a person of a similar age with low risk factors.
How to use the risk estimation charts?
The low-risk charts should be recommended for use in Belgium, France, Greece, Italy, Luxembourg, Spain, Switzerland and Portugal and also in countries, which have recently experienced a substantial lowering of the CV mortality rates. The high-risk charts should be recommended in all other countries of Europe. Note that several countries have undertaken national recalibrations to allow for time trends in mortality and risk factor distributions. Such charts are likely to better represent current risk levels.
To estimate a person's 10-year risk of CVD death, find the table for their sex, smoking status, and age. Within the table find the cell nearest to the person's blood pressure and total cholesterol or cholesterol: HDL cholesterol ratio. Risk estimates will need to be adjusted upwards as the person approaches the next age category.
Low-risk persons should be offered advice to maintain their low-risk status. Although no threshold is universally applicable, the intensity of advice should increase with increasing risk. In general, those with a risk of CVD death of 5% or more qualify for intensive advice, and may benefit from drug treatment. At risk levels over 10%, drug treatment is more frequently required. In persons above 60 years of age, these thresholds should be interpreted more leniently, because their age-specific risk is normally around these levels, even when other CV risk factor levels are ‘normal’. In particular, uncritical initiation of drug treatments of all elderly with risks beyond 10% threshold should be discouraged.
Relative risks may be unexpectedly high in young persons, even if absolute risk levels are low. The relative risk chart may be helpful in identifying and counselling such persons.
The charts may be used to give some indication of the effects of reducing risk factors, given that there will be a time lag before risk reduces and that the results of randomized controlled trials in general give better estimates of benefits. Those who stop smoking in general halve their risk.
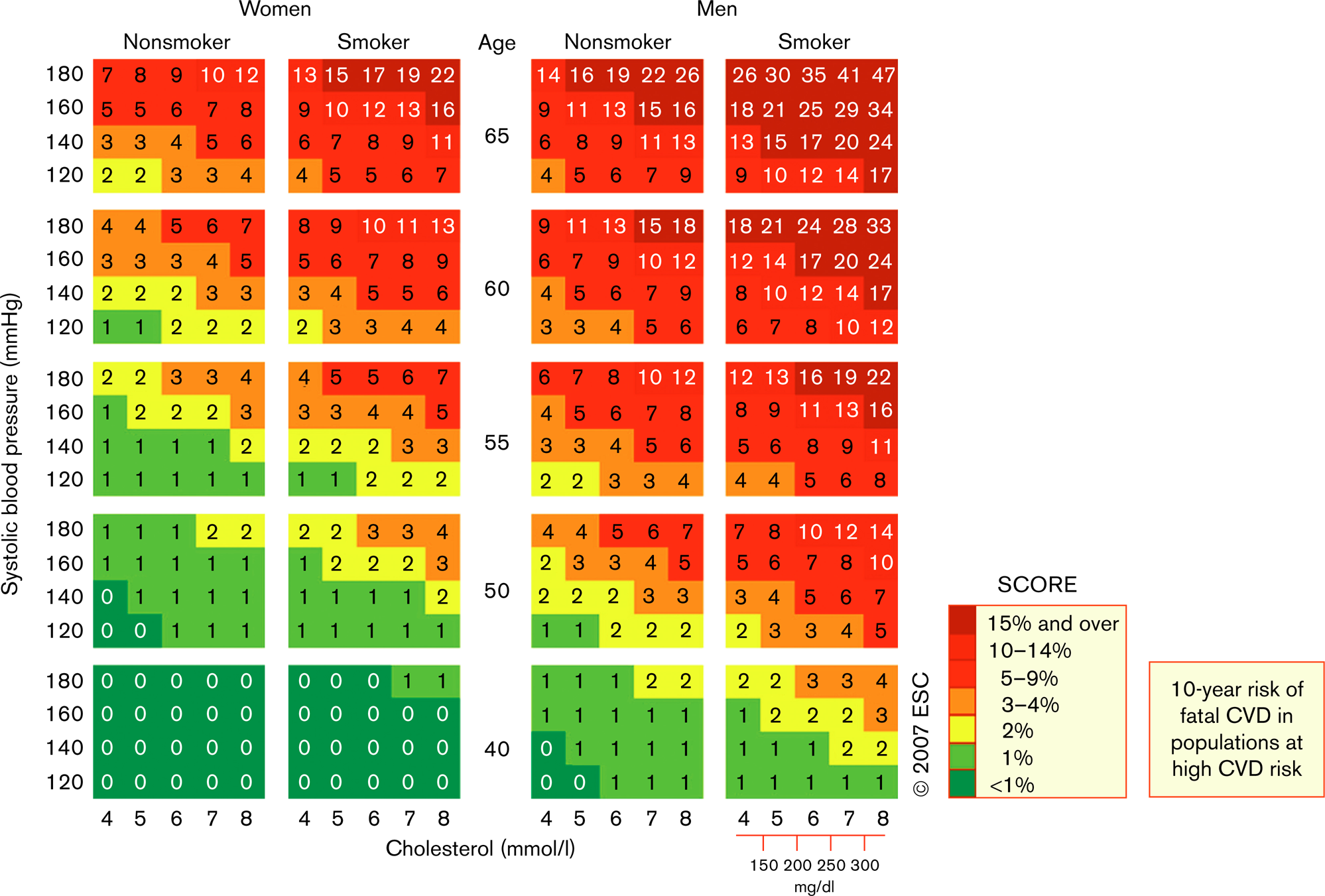
Systematic Coronary Risk Estimation (SCORE) chart: 10-year risk of fatal cardiovascular disease (CVD) in populations at high CVD risk based on the following risk factors: age, sex, smoking, systolic blood pressure, total cholesterol.
Qualifiers
The charts can assist in risk assessment and management but must be interpreted in the light of the clinician's knowledge and experience, especially with regard to local conditions.
Risk will be overestimated in countries with a falling CVD mortality, and underestimated in countries in which mortality is increasing.
At any given age, risk estimates are lower for women than men. This may be misleading because, eventually, at least as many women as men die of CVD. Inspection of the charts indicates that risk is merely deferred in women, with a 60-year-old woman resembling a 50-year-old man in terms of risk.
Risk will also be higher than indicated in the charts in
Sedentary patients and those with central obesity; these characteristics determine many of the other aspects of risk listed below.
Socially deprived individuals.
Individuals with diabetes: re-analysis of the SCORE database indicates that those with known diabetes are at greatly increased risk; five times higher in women and three times higher in men. Risk rises with increasing blood sugar before overt diabetes occurs.
Individuals with low HDL cholesterol, increased triglycerides, fibrinogen, apolipoprotein B and lipoprotein (a) levels, and perhaps increased high-sensitivity C-reactive protein and homocysteine levels.
Asymptomatic individuals with preclinical evidence of atherosclerosis, for example ultrasonography.
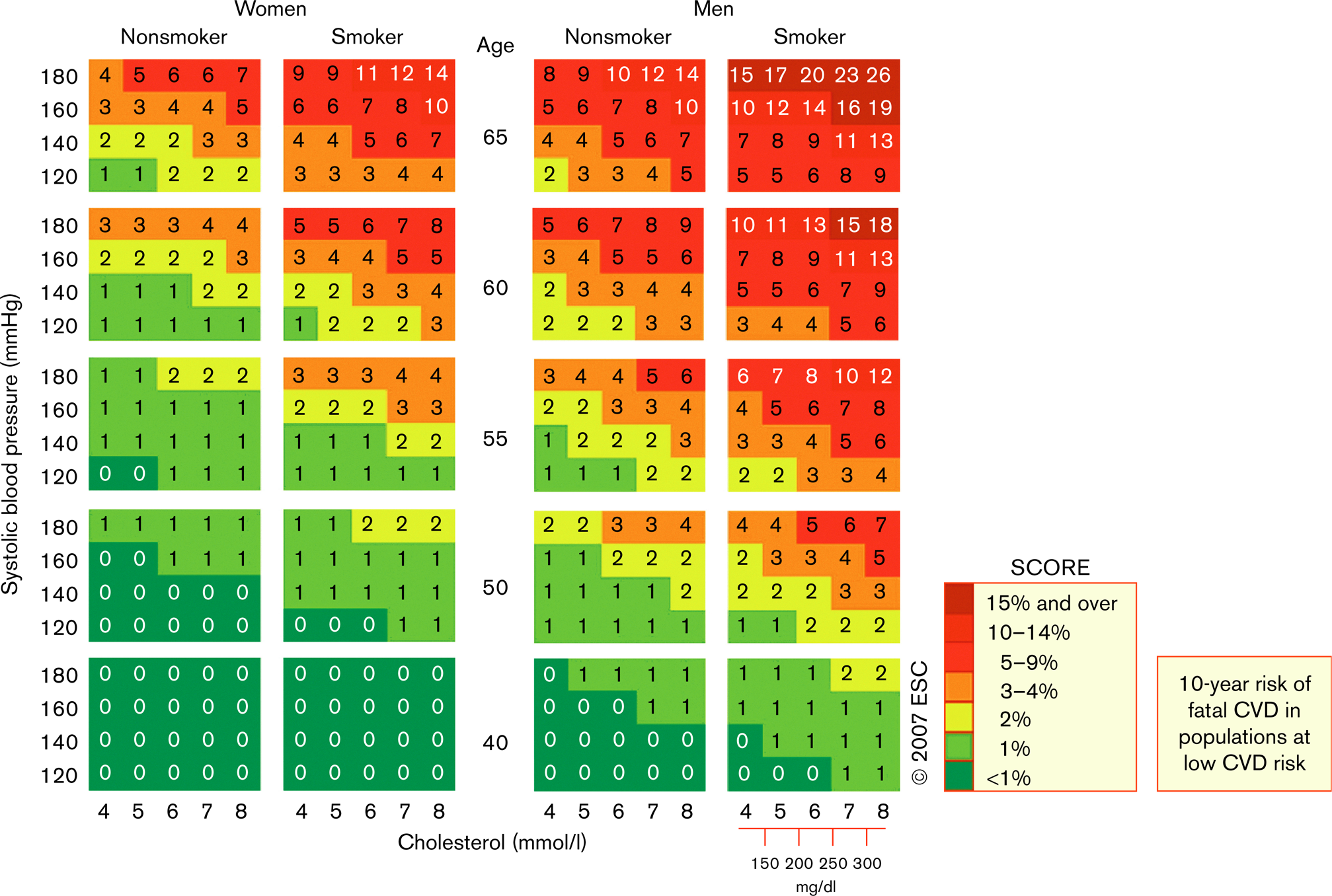
Systematic Coronary Risk Estimation (SCORE) chart: 10-year risk of fatal cardiovascular disease (CVD) in populations at low CVD risk based on the following risk factors: age, sex, smoking, systolic blood pressure, total cholesterol.
Interactive risk estimation – HeartScore®
HeartScore® is the electronic version of SCORE and is the interactive tool for estimating and managing the risk of heart attack and stroke in Europe. The following are certain advantages of the tool:
Intuitive and easy to use.
Allows instant risk estimation and targets to be adjusted to suit physician preference.
Can accommodate extra variables more easily than the paper charts.
Interacts with the pocket guidelines to produce appropriate guidance for the physician.
Produces both a graphic illustrating the person's risk and simple risk management advice in lay language.
Includes patient data history and allows progress monitoring.
Is available online in a web-based format, as a Windows-based program and as a quick calculator.
Two European versions (high and low risk) and 11 national versions translated into 15 local languages are available online. More information can be obtained through www.HeartScore.org.
What is new in risk estimation?
Since the present Guidelines on CVD Prevention in Clinical Practice were published, several developments have occurred:
Secular changes in mortality means that the designation of ‘high’ and ‘low’ risk countries will have to be revised. This can also be dealt with by recalibration, which adjusts for mortality and risk factor changes over time, and has been done for nine countries (Belgium, Czech Republic, Germany, Greece, The Netherlands, Poland, Slovakia, Spain, and Sweden) to date.
Further analyses of the SCORE data indicate that the importance of HDL cholesterol in risk estimation has been underestimated. The cholesterol: HDL cholesterol ratio charts look remarkably similar to the total cholesterol charts. This is a little misleading as, at any given level of cholesterol, a higher or lower ratio will result in adjustment of the risk up or down, respectively, and this may be sufficient to alter management decisions. Recent work based on the SCORE dataset indicates that HDL cholesterol modifies risk at all levels of baseline risk and in both sexes and new risk charts based on HDL cholesterol have been produced [10, 11].
Current, as yet unpublished research suggests that body weight, expressed as body mass index, has the potential to allow a simplified risk estimation system using easily measured, nonlaboratory variables.
Ways of expressing risk in younger and older individuals are being explored.
The title of this article raises the possibility of making risk assessment directly accessible to lay people, so that they can evaluate their own risk and participate more directly in its management. This is currently being actively developed with simpler risk charts, as in the three above, and in a pharmacy-based system in Sweden.
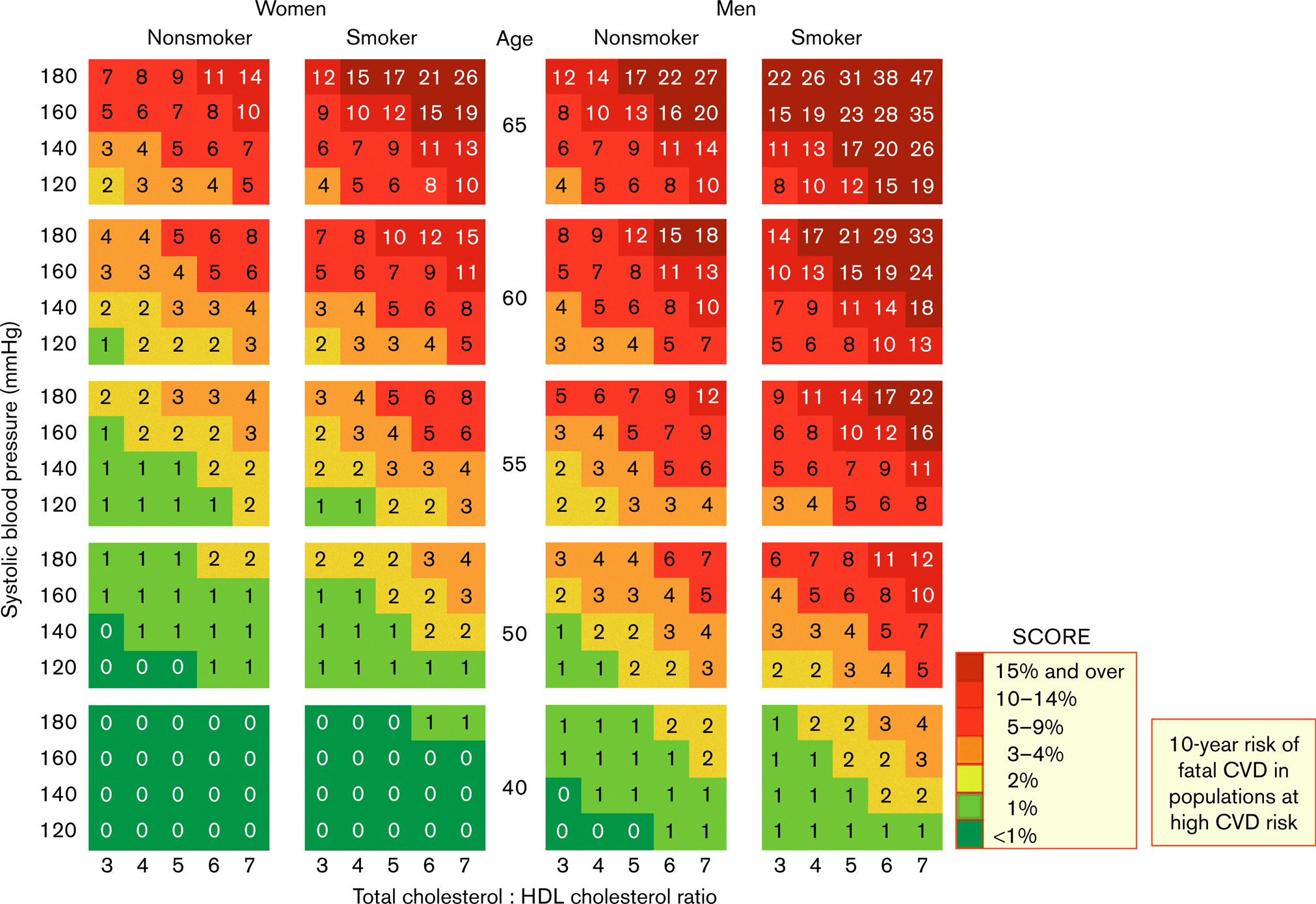
Systematic Coronary Risk Estimation (SCORE) chart: 10-year risk of fatal cardiovascular disease (CVD) in populations at high CVD risk based on the following risk factors: age, sex, smoking, systolic blood pressure, total cholesterol: HDL cholesterol ratio.
Summary
Those with established vascular disease, diabetes, and very high levels of single risk factors have declared themselves to be at high risk and deserve intensive risk factor management. For all others, estimation of ‘total risk’ using SCORE or Heart-Score remains a crucial part of the present guidelines. Information on relative as well as absolute risk is added to facilitate the counselling of younger persons whose low absolute risk may conceal a substantial and modifiable age-related risk. The total risk approach also allows flexibility in risk management – if perfect control of one risk factor is not possible, total risk can still be reduced by trying more actively with others.
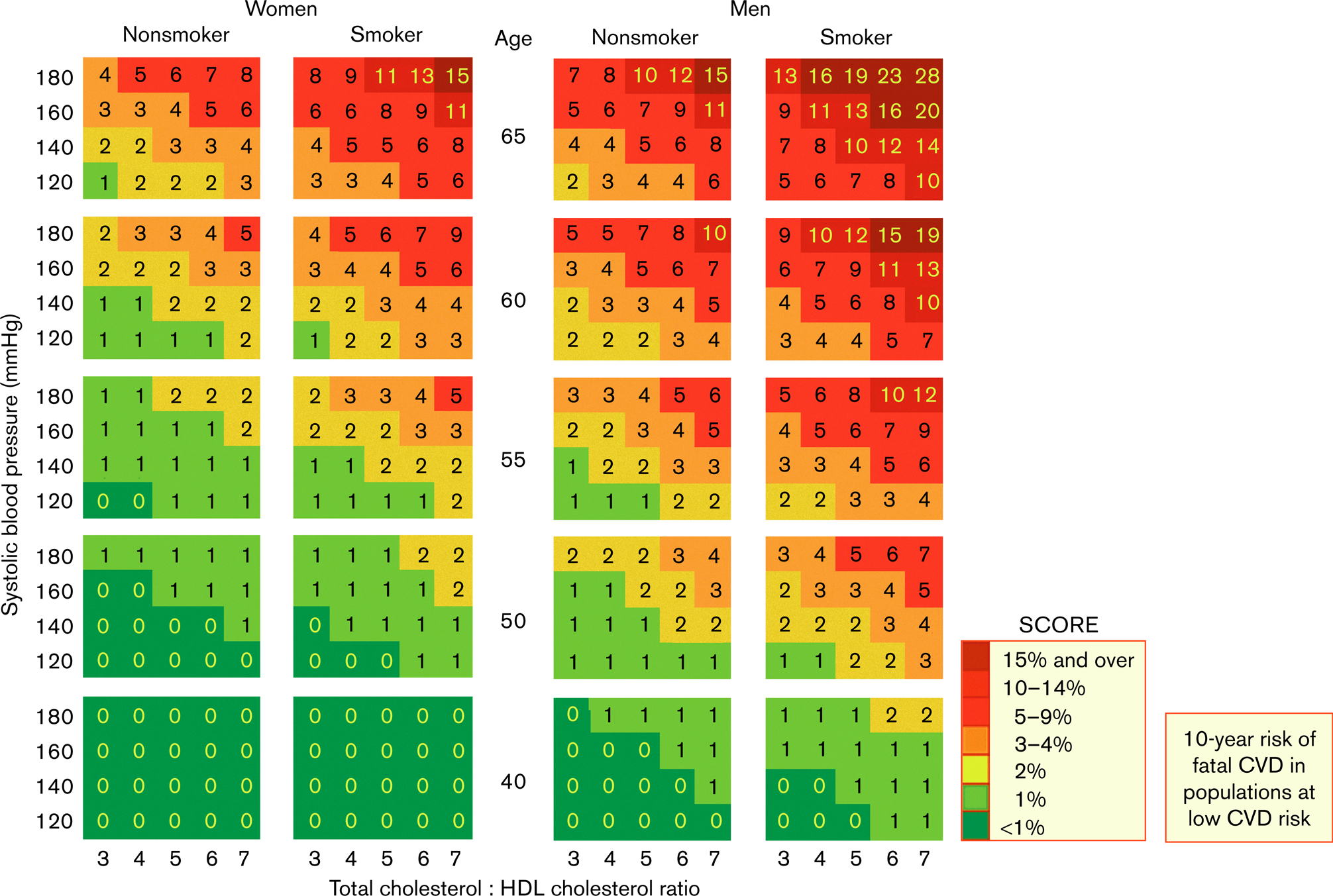
Systematic Coronary Risk Estimation (SCORE) chart: 10-year risk of fatal cardiovascular disease (CVD) in populations at low CVD risk based on the following risk factors: age, sex, smoking, systolic blood pressure, total cholesterol: HDL cholesterol ratio.
Relative risk chart.