
Abstract
For the reduction of microvascular complications in type 2 diabetes, glycemic control has been shown to be an important and effective intervention. However, considering the findings from several recent, large, randomized controlled trials, the utility of very tight glycemic control in all those with type 2 diabetes, for the reduction of cardiovascular disease remains controversial. The decision to aim for very tight glycemic control must be individualized and the potential benefit of reduced risk of nephropathy must be weighed against the increased risk for hypoglycemia. The results of the 10-year posttrial monitoring of the United Kingdom Prospective Diabetes Study (UKPDS) demonstrated macrovascular benefits of glycemic control in newly diagnosed type 2 diabetes but lengthy follow-up was required to demonstrate the effect. This raises the possibility that benefits of glucose lowering to reduce cardiovascular risk is more evident in those with a shorter duration of diabetes and requires many years to manifest. For the time being, there remains good evidence for targeting A1c [ 7% for microvascular protection but attempts to lower A1c beyond this must be considered on an individual basis. Eur J Cardiovasc Prev Rehabil 17 (Suppl 1):S25-S31 ©2010 The European Society of Cardiology
Introduction
The impact of diabetes mellitus, and in particular type 2 diabetes, on the affected individuals, their families, society as a whole and the healthcare system is significant and growing rapidly. It is projected that the prevalence of diabetes in the United States will rise from 23.7 million in 2009 to a staggering 44.1 million by 2034 with an associated annual cost increase of $113-$336 billion [1]. Worldwide, the prevalence is expected to grow from 284.6 million in 2010 to 438.4 million by 2030 [2]. The microvascular complications of diabetes are well recognized and glucose control has been shown to effectively reduce the risk of these complications. However, the effectiveness of glucose control in reducing the risk of cardiovascular (CV) (macrovascular) complications is less well established. Before 2008, epidemiologic studies showed an association between glycemia and CV risk [3–5]. In addition, the United Kingdom Prospective Diabetes Study (UKPDS) showed significant reductions in microvascular complication risk but nonstatistically significant reductions in macrovascular disease [6,7]. Nonetheless, until recently we had no prospective randomized trials to definitively show whether glucose control reduced macrovascular disease. In 2008, the results of several large randomized controlled trials [Action to Control Cardiovascular Risk in Diabetes (ACCORD), Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE), Veterans Affairs Diabetes Trial (VADT), United Kingdom Prospective Diabetes Study: 10-year Post-trial Monitoring (UKPDS-PTM)] [8–11] were published. These studies will be reviewed along with recent meta-analyses and their clinical implications.
Action to Control Cardiovascular Risk in Diabetes study (ACCORD)
The ACCORD trial is a large, National Health Institute sponsored, randomized controlled prospective study of 10 251 individuals with type 2 diabetes designed to determine if three separate strategies can reduce CV events [12]. The three strategies under investigation are (i) intensive therapy to target normal A1c levels ([6.0%) compared with standard therapy to target an A1c of 7-7.9%; (ii) therapy to target systolic blood pressure less than 120mmHg versus less than 140 mmHg; (iii) addition of fenofibrate versus placebo in patients with low-density lipoprotein cholesterol levels as target on statin therapy. The results of the blood pressure and lipid-lowering studies will be published in early 2010. However, the glycemic control study was stopped prematurely in February 2008 because of increased mortality among the intensively treated group after a mean follow-up of 3.5 years [8]. At baseline the ACCORD individuals had a mean age of 62.2 years, median duration of diabetes of 10 years, and a mean A1c of 8.3%. Approximately 35% had CV events earlier and 35% were already on insulin. The primary outcome was a composite of nonfatal myocardial infarction (MI), nonfatal stroke, or death from CV causes. The choice of glucose-lowering therapies to achieve the target A1c was at the discretion of the investigators. After 1 year, a median A1c of 6.4 and 7.5% was achieved by the intensive and standard groups, respectively. In fact, the intensive group achieved a drop of 1.4% in median A1c within just 4 months after randomization. To achieve that level of control, individuals were on multiple glucose-lowering medications with insulin use required by 77% of the intensive group compared with only 55% of the standard group. Among those using insulin, 62% of the intensive group were also on three or more oral medications compared with only 17% of the standard group. Hypoglycemia was also significantly higher in the intensive group. Hypoglycemia requiring any assistance occurred in 16.2% of the intensive-therapy group compared with only 5.1% of the standard-therapy group. Weight gain was also significantly higher in the intensive-therapy group with a greater than 10 kg weight gain occurring in 27.8% of the intensive-therapy group compared with only 14.1% of the standard-therapy group.
After a mean follow-up of only 3.5 years, the study was prematurely terminated, upon recommendation by the Data Safety Monitoring Board, based on the finding of increased mortality in the intensive group. At that time, intensive glucose lowering was associated with a nonsignificant 10% reduction for the primary outcome [hazard ratio (HR): 0.90; 95% confidence interval (CI): 0.78-1.04; P = 0.16]. There were 257 deaths in the intensive group compared with 203 deaths in the standard group [HR: 1.22 (95% CI: 1.01-1.46; P = 0.04)]. After multiple analyses, no definitive explanation has yet been identified to explain this surprising mortality finding. Achieving a lower A1c was not associated with increased mortality. In fact, the mortality was higher in those patients in the intensive group who did not achieve a lower A1c. Similarly, the mortality was higher in those patients in the intensive group whose A1c did not come down quickly in the first 12 months postrandomization. As would be expected, there were more frequent episodes of severe hypoglycemia in the intensively treated group. Furthermore, although a history of at least one severe hypoglycemic event was associated with increased mortality, there was no evidence that hypoglycemia accounted for the higher mortality in the intensive group. These newer data suggest that although perhaps glycemic control is worthwhile for reducing CV risk, the avoidance of hypoglycemia is also critical and suggests that one should loosen the glycemic targets in the person in whom achieving tighter glycemic targets proves to be difficult and/or is limited by hypoglycemia.
ADVANCE trial
The ADVANCE trial [9] was a factorial randomized controlled international trial of 11 140 patients with type 2 diabetes, investigating the effects of two interventions (targeting an A1c of 6.5% or less and/or lowering blood pressure with perindopril and indapamide) on major vascular outcomes. For the glucose component, individuals were randomized to receive either a strategy of intensive blood glucose lowering (gliclazide modified release based) to target an A1c of 6.5% or less, or a strategy of standard glucose lowering (target A1c based on local guidelines). The primary outcome was a composite of macrovascular (CV death, nonfatal MI, or stroke) and microvascular (retinopathy or nephropathy) events. At baseline, the mean age of the participants was 66 years, duration of diabetes was 8 years, and mean A1c was 7.5%. Approximately 32% of participants had a history of macrovascular disease and 10% had microvascular disease.
After a mean follow-up period of 5 years, the mean A1c was 6.5% in the intensive group and 7.3% in the standard group. The primary outcome was lower in the intensively treated group (18.1%) compared with the standard group (20%) with a HR of 0.90 (95% CI: 0.82-0.98; P = 0.01). However, this difference was driven by the reduction in microvascular events (HR: 0.86; 95% CI: 0.77-0.97; P = 0.01) and not the incidence of major macrovascular events, which was reduced to 6% nonsignificantly (HR: 0.94; 95% CI: 0.85-1.06; P = 032). The reduction in microvascular events was primarily because of the reduction in renal events, specifically, the development of macroalbuminuria. Once again, hypoglycemia occurred more frequently in the intensively treated group with severe hypoglycemia occurring in 2.7% of patients compared with only 1.5% of the standard group. Given the surprising finding in the ACCORD trial, it is important to note that there was no increase (or decrease) in mortality among the intensively treated group in ADVANCE. Although there was no mortality difference between the groups in the trial, recently presented analyses suggest a 25% relative reduction in CV mortality and 22% relative reduction in all-cause mortality for every 1% reduction in A1c. Therefore, the ADVANCE trial showed that lowering A1c to 6.5% or lower reduces renal events (development of macroalbuminuria) but does not reduce macrovascular events over 5 years, but also does not increase mortality - which is reassuring. Although the benefits of blood pressure lowering and intensive glucose control on renal outcomes were independent of each other, the combination of both strategies resulted in additive benefits with significant reductions in renal outcomes, and importantly, a significant 18% relative risk reduction in all-cause death (1-32%; P = 0.04) [13].
Veterans Affairs Diabetes Trial (VADT)
This multicenter trial investigated the effects of intensive glycemic control (target A1c of 6% or less) compared with standard control (A1c 8-9%) on CV outcomes among 1791 participants with type 2 diabetes [10]. The choice of treatments to achieve necessary glucose targets was at the discretion of the investigator. Blood pressure and lipids were treated equally and aggressively in both groups. The primary outcome of interest was a composite of major CV events (CV death, MI, stroke, congestive heart failure, severe inoperable coronary artery disease), amputation for ischemia, coronary or peripheral revascularization. At baseline, the mean age was 60 years, mean duration of diabetes was 11.5 years, and mean A1c was 9.4%. Approximately 40% of patients had a macrovascular event history.
After a mean follow-up of 5 years, the intensive group achieved a median A1c of 6.9% and the standard group achieved a median A1c of 8.4%. There was no difference in the primary outcome between the groups (25.9% intensive vs. 29.3% standard; HR: 0.87; P = 0.12) and importantly, no difference in mortality. No difference was found in any of the various CV secondary outcomes. In addition, no significant difference occurred in microvascular outcomes, with the exception of the development of new microalbuminuria and the progression of albuminuria [14].
Predictors of the primary outcome were vascular event (HR: 3.0), age (HR: 1.3), and hypoglycemia (HR: 2.06) earlier. Although the impact was smaller, duration of diabetes (HR: 1.02) and A1c (HR: 1.1) also predicted the primary outcome and high-density lipoprotein cholesterol level was inversely predictive (HR: 0.62). Therefore, the VADT, such as the ACCORD and ADVANCE trials, also showed that over a follow-up of 3.5-5 years strategies to target lower A1c levels in individuals with long standing type 2 diabetes do not reduce CV events among those at high risk of CV disease.
United Kingdom Prospective Diabetes Study: 10-Year Post-trial Monitoring (UKPDS-PTM)
In the original UKPDS trial, the median follow-up for the glucose intervention was 10 years (range 6-20 years) [6,7]. Individuals with newly diagnosed type 2 diabetes (n = 4209) were randomized to intensive glycemic control (sulfonylurea or insulin) or conventional control (diet) and a smaller overweight subset was randomized to intensive control with metformin. At the end of the original trial, the A1c achieved in the intensive group was 7%, compared with 7.9% in the conventional group. Significant reduction in microvascular complications was noted in the intensively treated group but no reduction was noted in macrovascular complications, with the exception of the metformin group that showed benefit [6,7]. After the conclusion of the original trial, surviving individuals (n =3277) were observed for an additional 10 years from 1997 to 2007 through clinic visits and then questionnaires [11]. The median follow-up by the end of the observation period was 17 years (range: 16-30 years).
After 1 year, there was no A1c difference between the two groups. By the end of the observation period, the mean A1c was around 7.8% in both groups. Overall mortality was 44%. When comparing intensive (sulfonylurea/ insulin) and conventional groups, microvascular complication risk reduction persisted with a HR of 0.76 (P = 0.001). Although the difference in macrovascular complications between the two groups did not achieve statistical significance in the original UKPDS trial, the difference became more apparent over the longer followup period. MI risk reduction became significant with a HR of 0.85 (P = 0.14) and a number needed to treat (NNT) of 36. All-cause mortality risk reduction also became significant with a HR of 0.87 (P = 0.007) and a NNT of 29. When comparing intensive (metformin) and conventional glucose-lowering treatments, the reduction in MI risk persisted (HR: 0.67; P = 0.005; NNT 14), as did the reduction in all-cause mortality (0.73; P = 0.002; NNT 14). Therefore, the results of the 10-year posttrial monitoring have shown significant microvascular and macrovascular risk reductions with early intensive glycemic control in newly diagnosed type 2 diabetes. There seems to be a ‘legacy effect’ in that early risk reductions persist over time and, in the case of macrovascular risk reduction, may take many years to manifest. Interestingly, this legacy effect was not observed for the UKPDS blood pressure intervention [15].
Meta-analyses
Several meta-analyses of these major trials have been recently conducted [16–18]. The meta-analysis by Turnbull et al. [16] incorporated the four major trials above (ACCORD, ADVANCE, VADT, UKPDS) and showed significant reductions in major CV events (HR: 0.91; 95% CI: 0.76-0.94) and MIs (odds ratio: 0.85; 95% CI: 0.75-0.93) (Fig. 1). There was no overall increase or decrease in all-cause mortality (HR: 1.04; CI: 0.90-1.20). There were significantly more major hypoglycemic episodes (HR: 2.48; 95% CI: 1.91-3.21). Significant heterogeneity for CV events was observed based on the history of macrovascular disease. A significant 16% reduction was observed in those in whom it was absent (HR: 0.84; CI: 0.75-0.94), whereas no effect (HR: 1.00; CI: 0.89-1.13) was observed in whom it was present. Other subgroups including age, baseline A1c, and duration of diabetes did not show any heterogeneity.
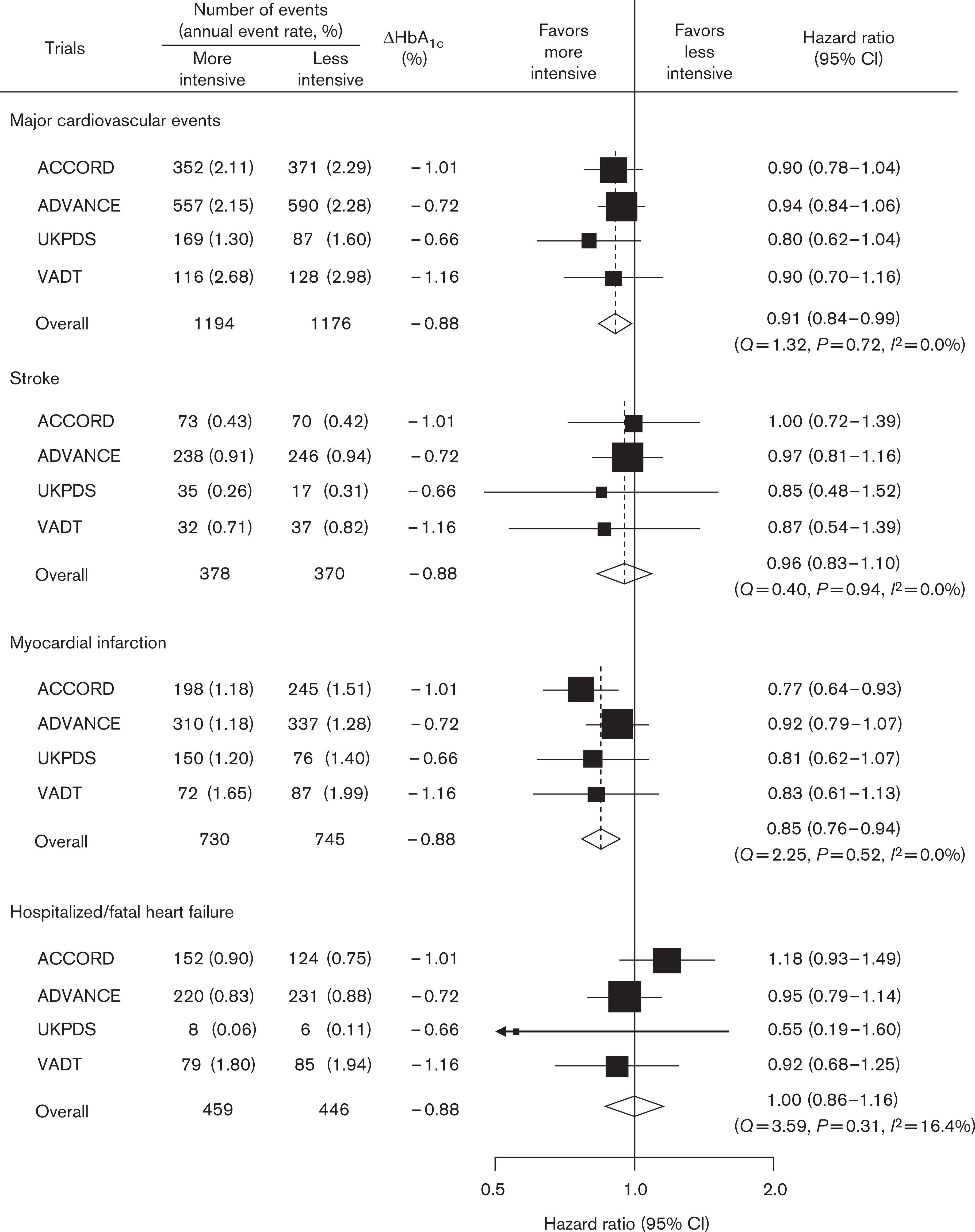
Effects of more-intensive glycemic control versus less-intensive glycemic control on major cardiovascular events (cardiovascular death or nonfatal stroke, or nonfatal myocardial infarction), stroke (fatal or nonfatal), myocardial infarction (fatal or nonfatal), and heart failure resulting in hospitalization or death. The diamond incorporates the point estimate, represented by the vertical dashed line, and the 95% confidence interval (CI) of the overall effect for each outcome. The HRs are given for more-intensive glucose control compared with less-intensive glucose control. DHbA1c = mean HbA1c of more-intensive group minus mean HbA1c of less-intensive group. UKPDS follow-up truncated at 5 years from the time of randomization. ACCORD, Action to Control Cardiovascular Risk in Diabetes; ADVANCE, Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation; HR, hazard ratio; UKPDS, United Kingdom Prospective Diabetes Study; UKPDS-PTM, UKPDS: 10-year posttrial monitoring; VADT, Veterans Affairs Diabetes Trial. Reproduced with permission from [16].
BARI 2D trial
Another question that has been raised is whether the specific method of glucose lowering has an impact on CV risk. Is there a difference, for example, between an insulin sensitizing (IS) or an insulin providing (IP) strategy? The bypass angioplasty revascularization investigation 2 diabetes trial [19] enrolled 2368 patients with angiographically proven coronary artery disease who were candidates for elective revascularization with either coronary bypass artery grafting or percutaneous coronary intervention. These patients were randomized to receive either an IS strategy (metformin±thiazolidinedione) or an IP strategy (sulfonylurea±insulin). After an average follow-up of 5.3 years, there were no differences between the IS and the IP groups in either of the two primary outcomes [overall survival and freedom from major CV events (death, MI, or stroke)], although the IP group experienced more hypoglycemia and more weight gain.
Making sense of it
Despite the methodologic differences between ACCORD, ADVANCE, and VADT, the results are fairly similar (Table 1). All three individually did not show any CV benefit to intensive glycemic control, and in fact, ACCORD showed potential harm with a small increase in mortality. However, it is important to note that the follow-up in these three trials were between 3.5 and 5 years. In addition, the individuals in these three trials were much further along in the disease process, having had diabetes for 8-11 years at the start of the trials. Although the results of ACCORD, ADVANCE, and VADT would suggest that the role of glycemic control, in and of itself, is not effective in reducing macrovascular events, the results of the 10-year posttrial monitoring of the UKPDS raises the question of timing. In the UKPDS, intensive glycemic control was instituted in individuals with newly diagnosed type 2 diabetes - early in the course of disease. In ACCORD, ADVANCE, and VADT, the individuals had a significantly greater duration of diabetes at enrollment. In addition, the follow-up time required to show the macrovascular benefit was a median of 17.8 years in the UKPDS. This raises the possibility that glycemic control does play a role in reducing CV complications, but it needs to be instituted early in the disease course and the benefit may take many years to manifest. In addition, the recent meta-analyses suggest that there may even be benefit to more intensive glycemic control among those later in their disease, but this must be tempered against the increased risk of potentially harmful episodes of hypoglycemia. Therefore, glycemic control remains an important intervention in the prevention of complications among those with diabetes. Of course, one must also consider the benefits of the reduced risk of microvascular complications. The results of ACCORD, ADVANCE, and VADT should not detract from the importance of glycemic control or alter existing guidelines that recommend targeting an A1c of 7% or less [20]. The decision as to whether one should aim for even lower A1c levels must be individualized. The ADVANCE trial showed a reduced risk for nephropathy associated with a mean achieved A1c of 6.5%. Finally, the absolute event rates in ACCORD, ADVANCE, and VADT, in both the intensive and standard treatment groups were lower than expected (6.9-10.6%), especially when compared with the event rates seen in the UKPDS of approximately 20%. This overall reduction in events is likely a result of the multiple risk factor modification strategies that have come into place over the past decade. Blood pressure control, lipid control, use of vascular protection medications, smoking cessation, and lifestyle modifications have become more widely applied in the overall management of a patient with type 2 diabetes and this seems to be working to reduce overall events. The landmark Steno-2 study of a comprehensive multifactorial intervention (glycemic, blood pressure, lipid control, smoking cessation, aspirin, angiotensin-converting enzyme inhibitor, and lifestyle), clearly showed both microvascular and macrovascular reductions including impressive reductions in morbidity and mortality [21]. A 5-year passive followup of the original 8-year study cohorts showed that the benefits of intensive multifactorial management continued to provide significant benefits, despite similar glucose, blood pressure, and lipid levels by the end of the observation period [22]. In fact, the NNT to prevent one death over the 13 years of follow-up was a remarkable 5. Therefore, although glycemic control should remain an important part of the management of type 2 diabetes, as it is one of many components, one must not neglect the other interventions, including blood pressure and lipid-lowering treatments that have clearly shown macrovascular benefits.
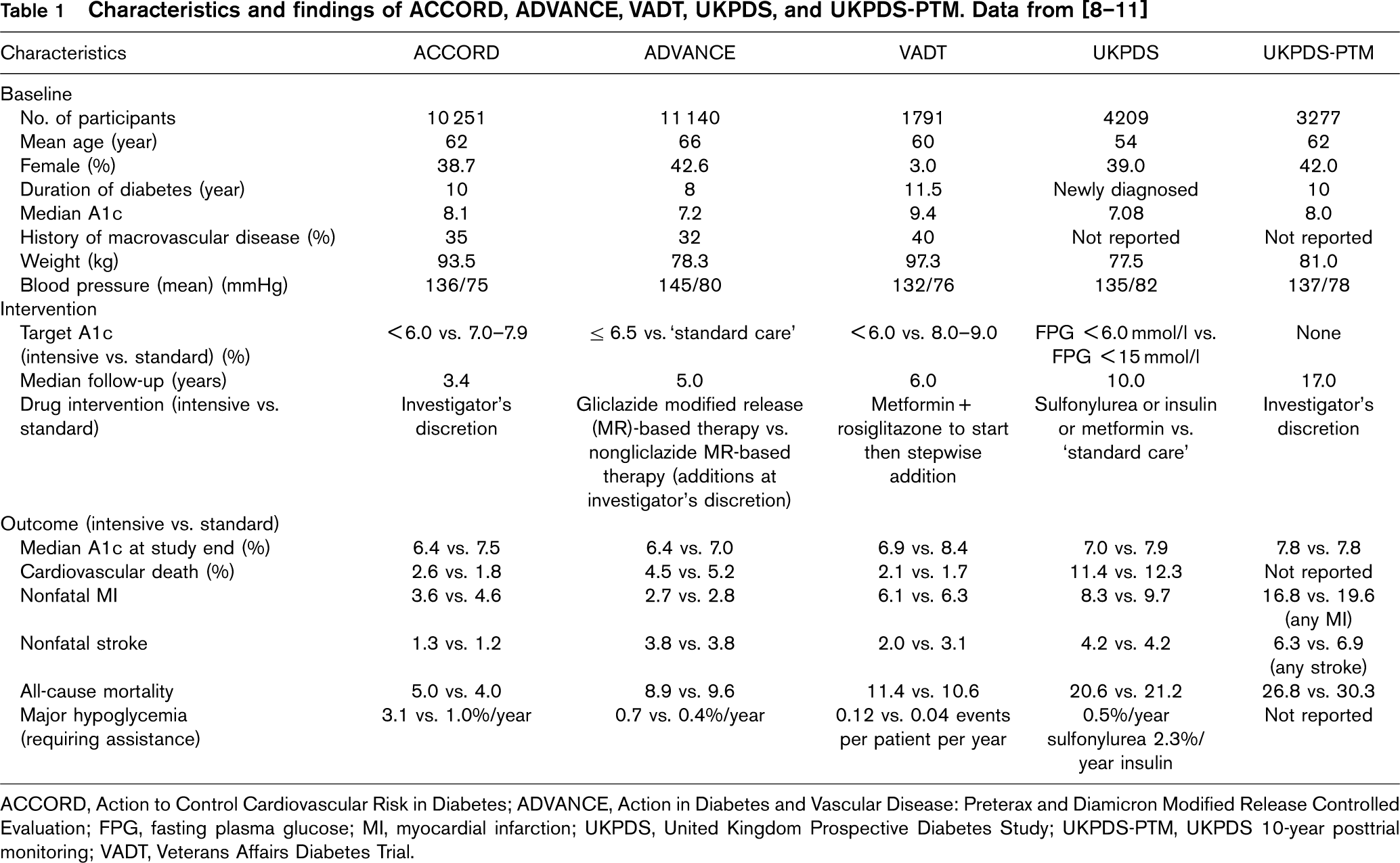
ACCORD, Action to Control Cardiovascular Risk in Diabetes; ADVANCE, Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation; FPG, fasting plasma glucose; MI, myocardial infarction; UKPDS, United Kingdom Prospective Diabetes Study; UKPDS-PTM, UKPDS 10-year posttrial monitoring; VADT, Veterans Affairs Diabetes Trial.
Conclusion
Glycemic control remains an important intervention in the treatment of type 2 diabetes - particularly for the reduction of microvascular complications. The decision to aim for very tight glycemic control must be individualized and the potential benefit of reduced risk of nephropathy must be weighed against the increased risk for hypoglycemia. The results of the 10-year posttrial monitoring of the UKPDS showed macrovascular benefits of glycemic control in newly diagnosed type 2 diabetes; however, lengthy follow-up was required to show the effect. This raises the possibility that benefits of glucose lowering to reduce CV risk are more evident in those with a shorter duration of diabetes and requires many years to manifest. For the time being, good evidence exists for targeting A1c less than 7% for microvascular protection, but attempts to lower A1c beyond this must be considered on an individual basis.
Footnotes
Acknowledgements
Alice Cheng has received honoraria for CME from, and/ or has acted as a consultant to AstraZeneca, BMS, Eli Lilly, GlaxoSmithKline, Merck-Frosst, Novo Nordisk, sanofi-aventis. Lawrence Leiter has received research funding from, has provided CME on behalf of, and/or has acted as a consultant to AstraZeneca, BI, BMS, Eli Lilly, GlaxoSmithKline, Merck, Novo Nordisk, Novartis, Roche, sanofi-aventis, and Servier.