
Abstract
Background Little data exists on the prognostic role of inspiratory muscle strength (PImax) in chronic heart failure (CHF). Training studies, however, frequently use it as a therapeutic target and surrogate marker for prognosis. The prognostic value of changes of PImax that allow this extrapolation is unknown.
Design Patients with stable CHF were prospectively included and 1-year and all-time event rates recorded for endpoint analysis.
Methods In 158 patients (85% men; New York Heart Association functional class: 2.4 ± 0.6), PImax was measured along with clinical evaluations at two visits, the initial visit and the second visit, 6.4 ± 1.4 months apart. The mean follow-up was 59 ± 34 months.
Results Overall, 59 patients (37%) reached the primary endpoint of death or hospitalization (endpoint positive), and overall mortality rate (secondary endpoint) was 26% (42 patients). PImax did not differ between endpoint-negative and endpoint-positive patients, both at the initial and at the second visit (8.3 ± 5.6 vs. 7.3 ± 3.4 kPa and 8.8 ± 6.0 vs. 7.9 ± 3.6 kPa, respectively; P = NS), and both groups showed increased PImax (0.6 ± 2.6 vs. 0.6 ± 2.8 kPa; P = NS). Cox analyses found neither the absolute nor the relative change of PImax to be significant predictors for the primary and secondary endpoints (P = NS for both), both for the 1 -year and for the all-time event rates. Endpoint rates did not differ between patients showing increasing or decreasing PImax (P = NS; relative risk (RR): 0.77; 95% confidence interval: 0.47–1.27).
Conclusion Trials focusing on inspiratory muscle function should use the actual levels of PImax as a surrogate marker to represent prognostic information, rather than relative or absolute changes. This is the first study to investigate the prognostic information of the changes of PImax over time, regarding both short-term and long-term morbidity and mortality in patients with stable CHF.
Keywords
Introduction
Evaluation of markers for risk prediction in chronic heart failure (CHF) is commonly carried out at a defined point of time during its clinical course (static markers); interventional studies mostly evaluate the time course of such markers (dynamic markers) [1]. Only very few studies, nevertheless, have addressed the link between dynamic measurement and prognostic information. Although some [2–4] reported a benefit from serial analyses, others [5] were not able to confirm this.
Dysfunction of skeletal and respiratory muscle has been described as a comorbid status, reflecting the systemic impact of heart failure [6–9]. Inspiratory muscle strength representing respiratory muscle function is estimated through maximum inspiratory mouth occlusion pressure (PImax). It is reduced early in CHF [10], and a reduction is associated with a poor outcome [9]. PImax is an established surrogate marker and a therapeutic target for interventions in many trials [11,12]. If, however, changes of PImax resulting from interventions are to be interpreted correctly, the link between these changes and their possible prognostic information needs to be established. So far, only two studies [9,13] with a total of 389 patients have addressed the prognostic value of PImax, demonstrating its independence from earlier established prognostic markers [13]; however, the prognostic value of serial estimates of PImax has never been addressed before.
Analysis of parameter changes during a certain follow-up period requires a homogeneous state of patients. Therefore, this study prospectively evaluated the prognostic significance of PImax and the potential additional value of PImax changes during a 6-month period in a large cohort of stable CHF patients.
Methods
We prospectively included 168 patients (85% men) with stable CHF. At inclusion (initial visit, V1), PImax was determined, and a baseline clinical evaluation performed. A second evaluation (second visit, V2) including the determination of PImax was performed after 6 months (mean: 6.4 ± 1.4 months). For V2, this study design mirrors the common outpatient setting, in which the clinician judges the individual course of a patient in the light of previous data.
All patients were followed up for at least 12 months after V2, the mean follow-up period being 59 ± 34 months. Patients had to be on stable medication for more than 4 weeks prior to inclusion. Patients with an endpoint between V1 and V2 were excluded from the final analysis because they no longer fulfilled the entry criterion of stability of CHF.
Exclusion criteria were a positive history for primary pulmonary disease, uncorrected valvular defects, cardiac decompensation requiring inotropic support within the last 3 months prior to study inclusion, and conditions that could possibly affect respiratory muscle function (e.g. thyroid dysfunction and electrolyte disturbance). The study conformed to the principles outlined in the Declaration of Helsinki and was approved by the local Ethics Committee. All patients gave their written informed consent.
Inspiratory muscle-function testing
Measurements of PImax were performed by a technician blinded to the status of the patient and unaware of the other variables in the study. PImax was determined through a flanged mouthpiece in deep inspiration from functional residual capacity against a shutter with a minor air leak to prevent undesirable glottis closure (Master-LabPro 4.2; Erich Jaeger, Wuerzburg, Germany) [14]. Out of three measurements with [ 5% variability, the highest pressure was used for analysis. A short rest was allowed between manoeuvres when necessary. PImax is expressed in kPa as positive values, although they are negative pressures with respect to atmosphere.
Follow-up and endpoint
Patient follow-up was performed by either regular outpatient visits or telephone calls to patients' homes or to their respective physicians. The combined endpoint of death or hospitalization due to cardiac reasons within 1 year was defined as the primary endpoint, and 1-year mortality was defined as the secondary endpoint. Analyses were further extended to overall follow-up for both endpoints. Patients were classified as endpoint positive (EPP) if they had an event after V2; otherwise they were classified as endpoint negative (EPN). No patient underwent coronary artery bypass grafting or implantation of a left-ventricular assist device during follow-up. Patients receiving orthotopic heart transplantation were censored at the date of transplantation.
Statistics
Statistical tools such as the χ2 analysis, the t-test and the two-sample Wilcoxon test were used wherever appropriate. All tests are two-tailed, and a P value of less than 5% was regarded as being statistically significant. Differences in event-free survival were detected by the Cox proportional-hazard model and depicted by the Kaplan–Meier product-limit method. The data are presented as mean ± SD, except when specified otherwise. Calculations were performed with SAS version 6.12 (SAS Institute Inc., Cary, North Carolina, USA).
Results
Of the 168 patients included, 10 patients reached a predefined endpoint between V1 and V2. According to the study protocol, they were excluded from the analysis because they no longer fulfilled the criterion of stable CHF. Therefore, 158 patients were retained for the final analysis and followed up for a mean period of 59 ± 34 months. Of this final study population, 19 patients (12%) reached the primary endpoint of death or hospitalization within 1 year, and the 1-year mortality rate was 8% (12 patients). The profiles of the patients included at V1 and V2 for the study population analysed are shown in Table 1.
Patient profile
Both at V1 and V2, PImax was higher in EPN than in EPP, the difference not reaching statistical significance. At V1, EPN differed from EPP only in mean age and in the left-ventricular ejection fraction (LVEF). At V2, the difference for LVEF was no longer significant, but the mean result for the 6-min walk test had become significant. No other difference between EPN and EPP was noted for other clinical characteristics. For complete results, see Table 2.
Clinical characteristics of the patients included and of the actual study population retained at the initial and follow-up visits
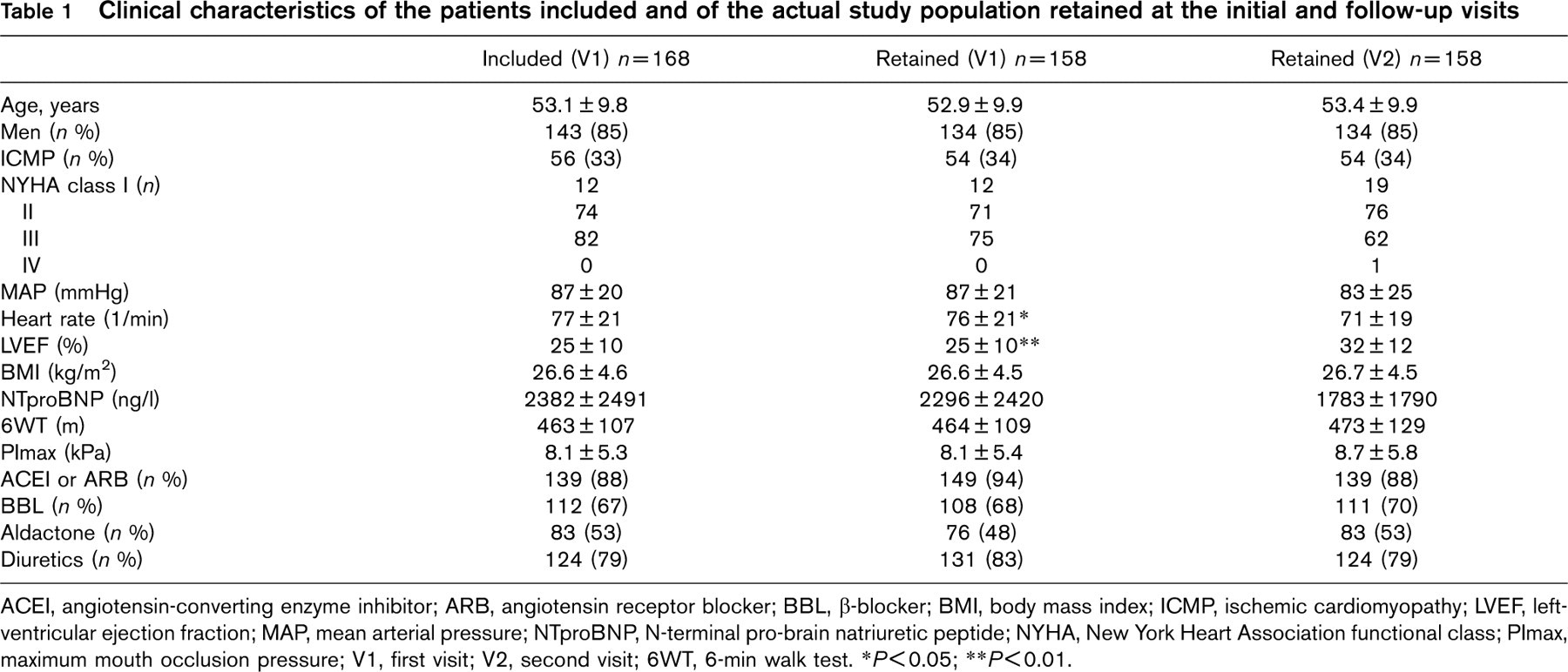
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BBL, β-blocker; BMI, body mass index; ICMP, ischemic cardiomyopathy; LVEF, left-ventricular ejection fraction; MAP, mean arterial pressure; NTproBNP, N-terminal pro-brain natriuretic peptide; NYHA, New York Heart Association functional class; PImax, maximum mouth occlusion pressure; V1, first visit; V2, second visit; 6WT, 6-min walk test.
∗ P [ 0.05;
∗∗ P [ 0.01.
Endpoint-positive and endpoint-negative patients for 1-year follow-up, at the initial visit and the follow-up visit after 6.4 ± 1.4 months
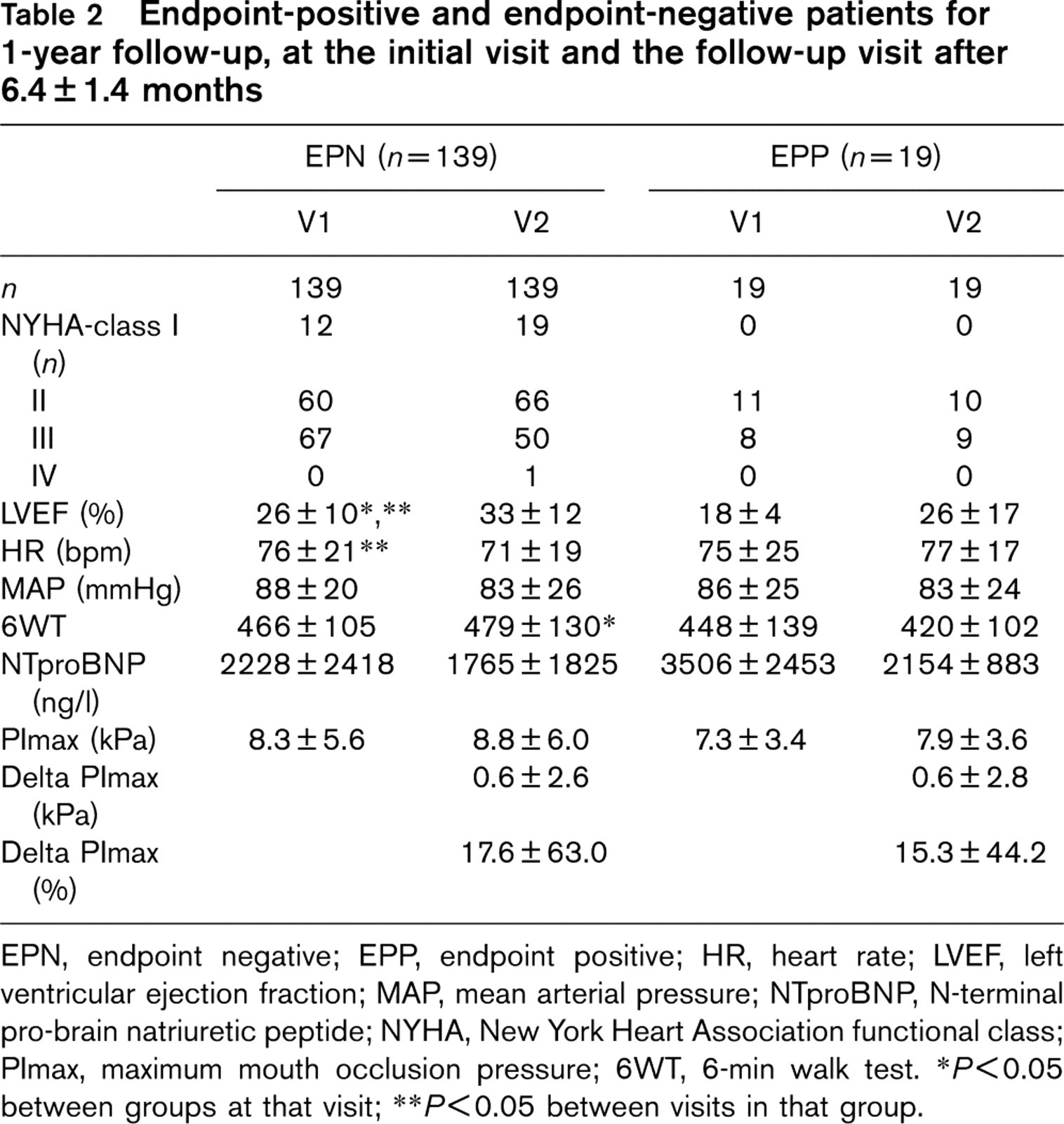
EPN, endpoint negative; EPP, endpoint positive; HR, heart rate; LVEF, left ventricular ejection fraction; MAP, mean arterial pressure; NTproBNP, N-terminal pro-brain natriuretic peptide; NYHA, New York Heart Association functional class; PImax, maximum mouth occlusion pressure; 6WT, 6-min walk test.
∗ P [ 0.05 between groups at that visit;
∗∗ P [ 0.05 between visits in that group.
Changes over time
Both EPN and EPP increased the mean PImax between visits. This increase, however, was not significant for either of the groups. Furthermore, no significant difference was noted when comparing the mean change of PImax between groups, both as absolute values and as percentages of the initial value (Fig. 1). EPN significantly increased LVEF and decreased heart rate, whereas the decrease in New York Heart Association functional class, mean arterial pressure and serum N-terminal pro-brain natriuretic peptide, as well as the increase in the 6-minute walk test were not statistically significant. No significant changes were noted for EPP between visits (Table 2).
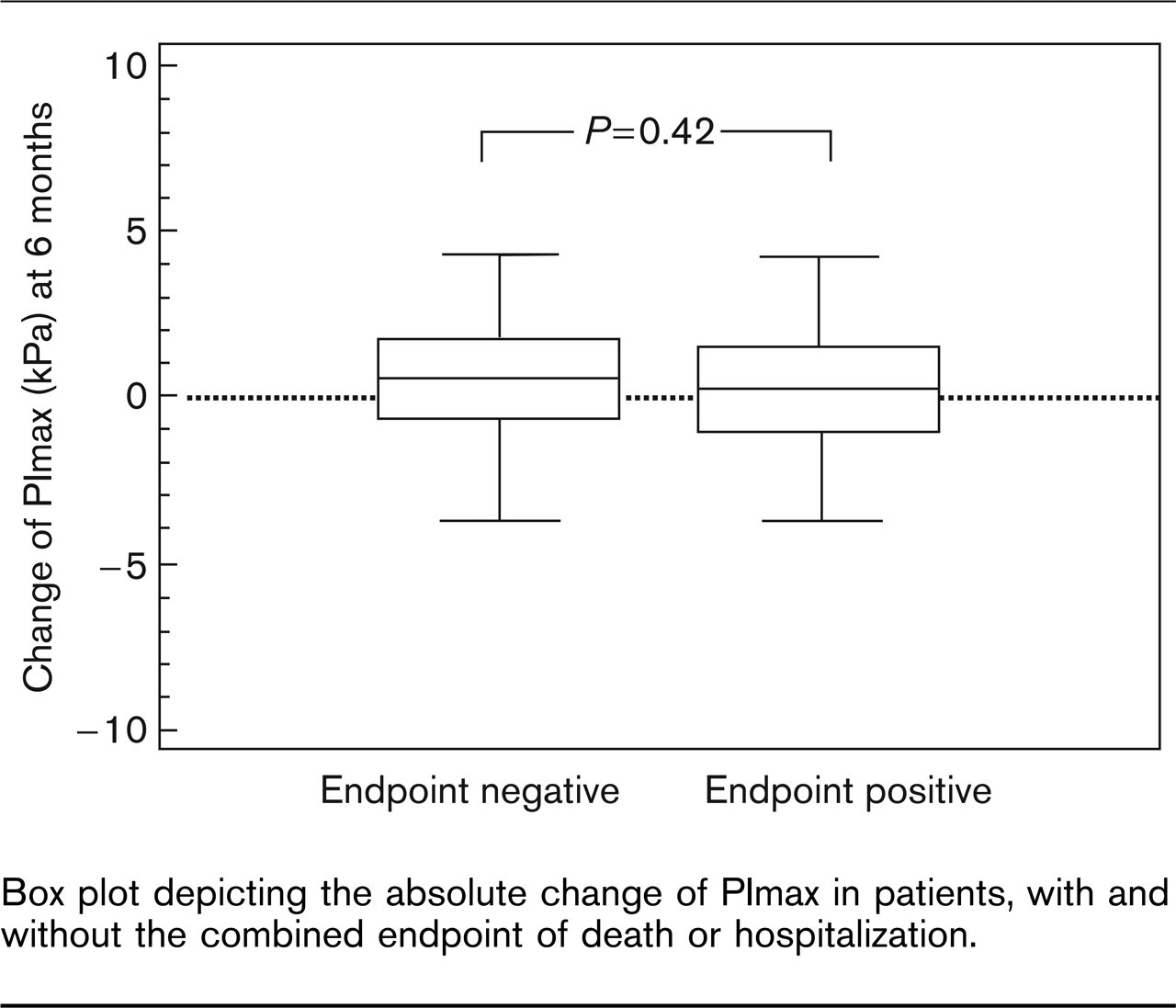
Box plot depicting the absolute change of PImax in patients, with and without the combined endpoint of death or hospitalization.
Change of PImax, resultant event rates and Cox analyses
During the 1-year follow-up, patients with increasing PImax between visits had a primary endpoint rate of 11% (10 patients) for death or hospitalization in contrast to 14% (nine patients) for patients with decreasing PImax [P = NS; RR: 0.77; 95% confidence interval (CI): 0.47–1.27]. During the entire follow-up period, 32% (30 patients) of patients with increasing PImax and 45% (29 patients) of patients with decreasing PImax reached the combined endpoint (P = NS; RR: 0.79; 95% CI: 0.59–1.05) during follow-up. Patients with increasing PImax had a 1-year mortality rate of 6% (six patients). In contrast, patients with decreasing PImax had a 1-year mortality rate of 9% (six patients; P = NS; RR: 0.83; 95% CI: 0.46–1.48). The overall morality rate was 22% (21 patients) for patients with increasing PImax and 33% (21 patients) for patients with decreasing PImax (P = NS; RR: 0.79; 95% CI: 0.57–1.11) (Figs 2 and 3).
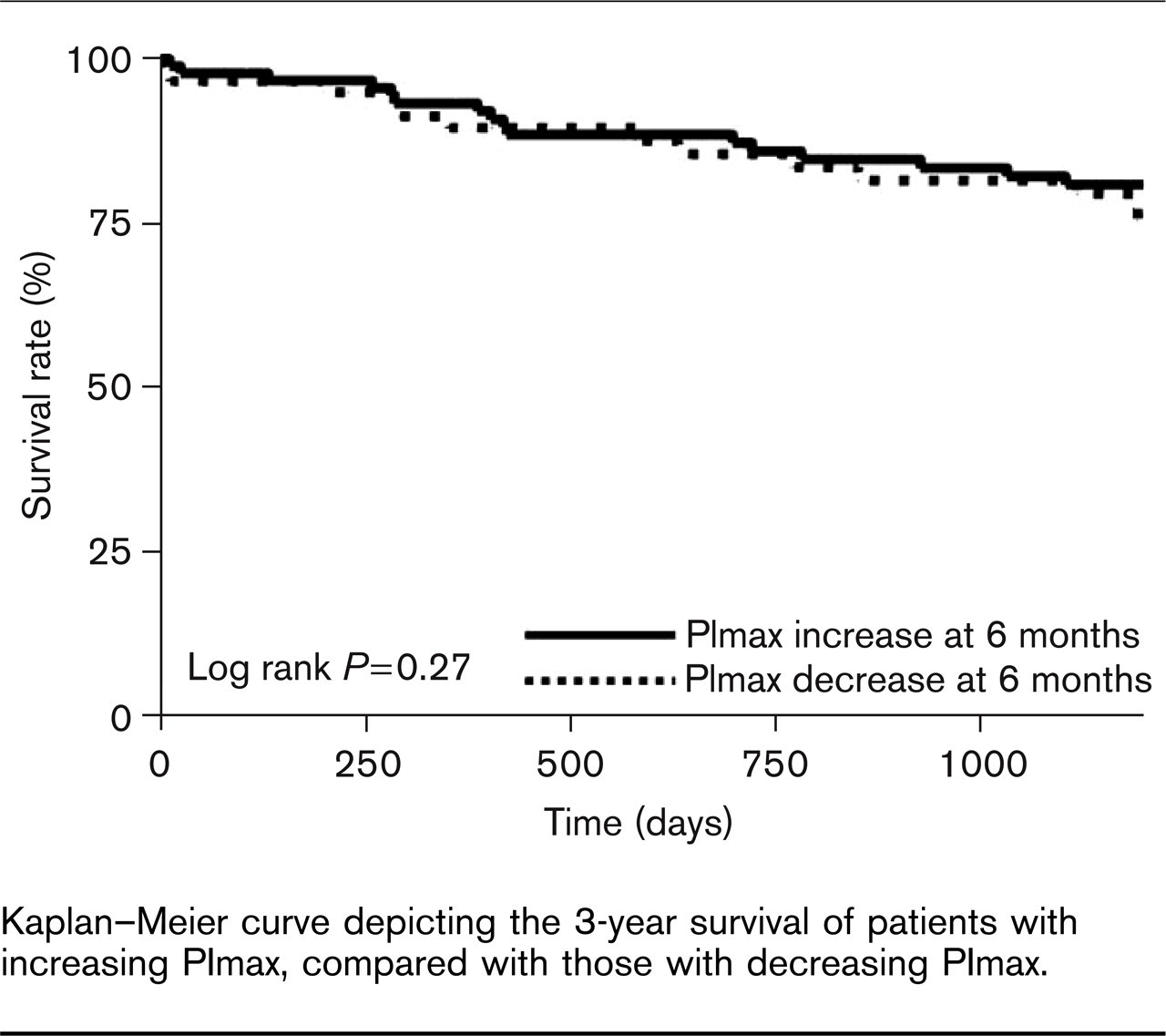
Kaplan–Meier curve depicting the 3-year survival of patients with increasing PImax, compared with those with decreasing PImax.
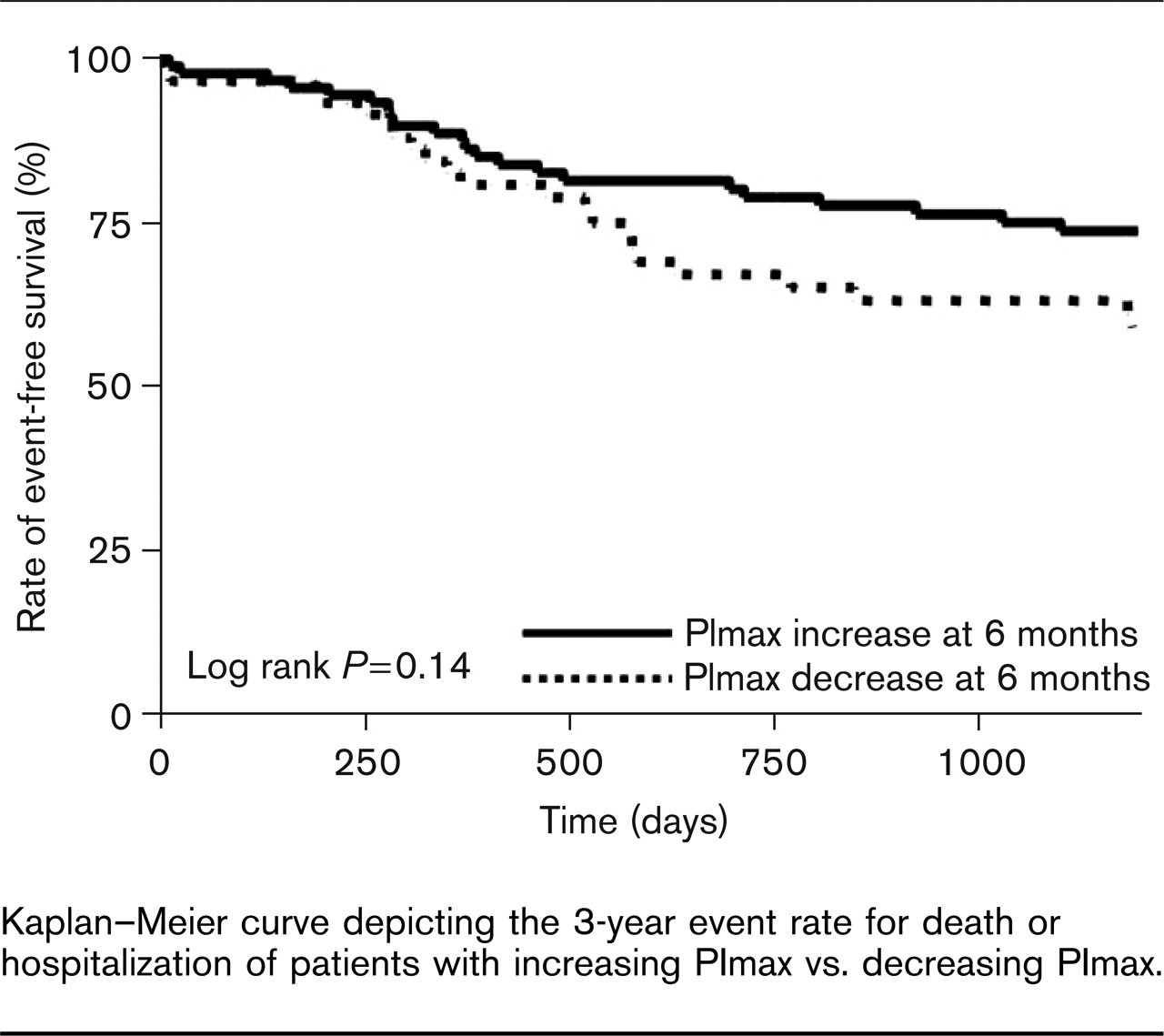
Kaplan–Meier curve depicting the 3-year event rate for death or hospitalization of patients with increasing PImax vs. decreasing PImax.
Cox analysis showed that neither the absolute (d_PImax) nor the relative change of PImax (d_PImax%) were significant predictors for the primary and secondary endpoints (P = NS for both). Furthermore, the predictive accuracies of d_PImax and d_PImax% (as judged by the area under the curve of the receiver-operating curve) were not superior to PImax, both for the prediction of the primary and the secondary endpoints. The same results were obtained for overall mortality or the all-time combined endpoint. In contrast, PImax was a significant predictor for death or hospitalization both at V1 and V2 (χ2: 7.83, P [ 0.01; χ2: 9.73, P [ 0.01; respectively) as well as for death both at V1 and V2 (χ2: 8.13, P [ 0.01; χ2: 5.37, P [ 0.05; respectively).
Discussion
Although PImax is frequently used as a surrogate marker and therapeutic target for interventions in many trials of CHF, the prognostic value of serial determinations of PImax has not been addressed before. This, however, seems to be crucial if one wants to correctly interpret the changes of PImax resulting from intervention, or to use them as a surrogate for prognosis. We sought to provide this link in a prospective setting without intervention between visits, to differentiate the prognostic information relating to the level of change of PImax from that relating to the intervention performed. The main findings of our study are as follows:
Without any intervention targeting inspiratory muscles, neither the absolute nor the relative changes of PImax predict the 1-year or overall mortality in stable CHF.
Without any intervention targeting inspiratory muscles, neither the absolute nor the relative changes of PImax predict the 1-year or overall event rate for the combined endpoint of death and hospitalization for cardiac reasons in stable CHF.
Neither the absolute nor the relative changes of PImax were found to be additional significant predictors with respect to PImax.
We were able to confirm previous reports [9,13] regarding the prognostic value of PImax. Even though no information is available with regard to the prognostic value of serial measurements of PImax, the issue of change over time of other predictive variables in CHF has been addressed before. Although Gullestad et al. [5] were not able to demonstrate any additional benefit from serial determination of echocardiography parameters or pVO2, Florea et al. [3] found that the change of exercise parameters and LVEF significantly added to the prognostic value of single measurements. Grigioni et al. [2] extended these findings to ECG parameters, but changes in these failed to gain significance in their study. Recently, Corra et al. [4] reported that a combination of single and time-related functional variables would enhance the prognostication process.
These contradictory studies possibly demonstrate some of the pitfalls that occur with serial evaluation of markers, such as the interval between visits and the range of this interval. The larger the interval, the more obvious will be the change, although clinical consequences might already have necessitated interventions. Furthermore, if the interval range is large, individual changes might no longer be comparable. In daily routine, however, it is rather difficult for the clinician to organize follow-ups in predefined periods of time outside controlled trials. Therefore, a certain range is unavoidable. In addition to these limiting factors, the value of the changes over time might be blunted if the clinical characteristics already differed at the initial visit [5]; hence, the results of the above studies might not be entirely comparable.
As far as soft endpoints such as functional capacity or quality of life are concerned, the link between change and result seems to be established for PImax. Already general training not specifically targeting the respiratory muscle alleviates dyspnoea and improves exercise performance in patients with CHF [15,16]. Training interventions and trials focusing on respiratory muscle function consistently showed improved muscle endurance and strength, resulting in enhanced exercise capacity, significantly less dyspnoea and improved functional status [12,17,18]. This, however, was not related to either the increased cardiac output or stroke volume [19]. The functional improvement resulted in less frequent periods of rest, fatigue, greater self-confidence, maintenance of independence and enhanced quality of life [11,19].
None of these trials or interventions focusing on respiratory muscle function reported any effect on survival. In contrast, a recent meta-analysis [20] confirmed the positive effect on survival of general physical training. Furthermore, skeletal muscle dysfunction and wasting responds to physical training [21]. Therefore, one would expect a positive link between the changes of PImax and survival. Given that we were unable to establish this link both for short-term and long-term mortality or morbidity, the prognostic impact of interventions and studies solely targeting respiratory muscles needs to be addressed.
It is known [20,21] that general physical training exerts positive effects on the different aspects of heart failure –ranging from cardiopulmonary, skeletal muscle and endothelial function to changes in neurohumoral activation patterns [22]. As a hypothesis, it is therefore possible for respiratory muscle function in the context of general physical training to reflect a more systemic positive modification. Inversely, respiratory muscle training alone can certainly improve respiratory function, leading to positive functional effects, without the more systemic effects of general physical training including improved survival.
To omit this possible bias regarding the kind of intervention performed, this study investigated the changes of PImax in stable patients without any intervention, thus separating the possible prognostic effect of training from the prognostic information of the measurement. Patients were followed up on a regular basis at our specialized CHF clinic, and no intervention was performed by us. Had patients been registered with any kind of training programme, the general practitioner concerned would have informed the doctor in charge. In addition, patients had been questioned accordingly during the determination of endpoints. Consequent to our results, we suggest that trials focusing on inspiratory muscle function should use the actual levels of PImax as a surrogate marker rather than the relative or the absolute changes to represent prognostic information. PImax represents a marker of severity in itself [9,13]. Therefore, the risk would be more related to the actual level of PImax, rather than to the change from earlier measurements.
Limitations
To the best of our knowledge, we included one of the largest cohorts so far regarding the serial evaluation of inspiratory muscle force. The number of patients might, nevertheless, represent a limiting factor. It might have precluded the effect of time-related changes of PImax from becoming statistically significant. A nonconservative size estimate performed, using the data on the changes of PImax derived from this study by applying a type I error (α) of 0.05 and a type II error (β) of 0.10, however, indicates that the number of patients required would be 3836. For the reasons stated above, this study investigates the relationship between the changes of PImax and prognosis without any intervention between visits. Therefore, the question as to what extent these changes of PImax might reflect the beneficial effects of general physical training cannot be fully answered. Here, we postulate the need for a randomized interventional trial. Last, the interval chosen for our study might limit the results obtained, but we chose an interval of 6 months because we consider this to be appropriate in the general clinical follow-up of patients with stable CHF.
Conclusion
Trials focusing on inspiratory muscle function should use actual levels of PImax as a surrogate marker to represent prognostic information rather than the relative or the absolute change. In this first study to address the prognostic usefulness of the changes of PImax over time regarding both short-term and long-term morbidity and mortality in patients with stable CHF change in PImax was not found to be an additional significant predictor. Furthermore, this is the first study giving a size estimate of potential randomized trials targeting a possible survival benefit of interventions on inspiratory muscles.
Footnotes
Acknowledgements
Support: This study was supported by a grant from the Carl–Baresel Foundation.
Conflict of interest: none.