
Abstract
Background Earlier studies show that medical factors and disease severity predict early readmission to hospital after coronary artery bypass graft surgery (CABGS). Few studies have investigated psychosocial predictors. This study investigated medical, sociodemographic and psychosocial predictors of 30-day hospital readmission.
Methods A consecutive sample of 181 patients wait-listed for CABGS completed self-report questionnaires before surgery, and at 2 and 6 months after surgery.
Results Twenty-six (14.4%) patients were readmitted within 30 days of hospital discharge. Readmitted patients were older (t = 2.12, df = 179, P = 0.035), and more likely to be unmarried (χ2 = 5.80, df = 1, P = 0.016), live alone (χ2 = 8.33, df = 1, P = 0.004), have a history of hypertension (χ2 = 2.731, df = 1, P = 0.098) and have higher anxiety before surgery (t = 1.67, df = 175, P = 0.097). When these variables were entered into a backward stepwise logistic regression, the only significant unique predictor of 30-day readmission was living alone (Wald = 7.08, odds ratio = 3.42, P = 0.008). Patients living alone were over three times more likely than those living with others to be readmitted to hospital. Disease severity and other medical factors were not associated with readmission.
Conclusion Living alone was identified as the single most important risk factor for early readmission after CABGS. Patients who live alone may benefit from additional support during early convalescence. Intervention studies could explore support options for these patients.
Keywords
Introduction
With the current emphasis on the delivery of quality patient care and reduced hospital costs [1], early readmission to hospital after coronary artery bypass graft surgery (CABGS) has gained considerable attention in the research literature [2–5]. Early readmissions after cardiac surgery are costly and are associated with increased risks for patients [6]. As such, in addition to morbidity and mortality rates, readmission to hospital within 30 days of discharge is now regarded as an important outcome measure in CABGS studies [4].
Although the majority of patients experience improved health and quality of life after CABGS [7], a significant minority are readmitted to hospital within 30 days of hospital discharge. In their large study of readmissions after CABGS, Hannan and colleagues [4] observed that 12.9% patients were readmitted within 30 days, although higher rates in the order of 14.5% have also been reported [5]. The most common reasons given for early readmission to hospital after CABGS are cardiac problems, pulmonary complications, gastrointestinal complications, infection and wound healing difficulties [2–5,8,9].
Certain patient groups are at increased risk of early readmission after CABGS and other cardiac procedures. Female cardiac patients [3–5,10] and those who are older [4,11] consistently show higher readmission rates. Patients who are obese [5,8] or diabetic [2,3,10], have had a previous myocardial infarction (MI) [4,11] or have more severe disease [2,5,11] are also at increased risk. Despite concerns that ‘fast track’ surgery might increase the likelihood of readmission [12], patients who are discharged early (within 5 days of surgery) are less likely to be readmitted to hospital during early convalescence [2,4,12].
Most earlier studies investigating hospital readmission after cardiac procedures have involved relatively large samples of consecutively admitted patients. Patient samples have ranged from around 1000 to 16000 patients in the study by Hannan and colleagues [4]. In these studies, most of which have been undertaken in the last decade, details of patient characteristics have generally been obtained from hospital medical records or databases. This approach has enabled identification of sociodemographic and medical factors that predispose patients to readmission.
Relatively few studies have, however, investigated psychosocial predictors of early readmission. The few exceptions include an early study by Berkman and colleagues [13,14], which involved a postal questionnaire survey of 628 CABGS patients, enabling investigation of some psychosocial variables based on patients' self-reports. In that study, being unmarried, having poorer self-reported mental health, and higher self-reported stress following hospital discharge predisposed patients to early readmission. As medical determinants of readmission were not investigated, however, the relative importance of the psychosocial predictors could not be ascertained. The Israeli CABGS study also included a follow-up of patients, with living alone being identified as a significant determinant of readmissions within 100 days of hospital discharge [9]. Other psychosocial variables such as anxiety and depression, however, were not investigated.
The aim of this study was to identify significant unique predictors of 30-day readmission to hospital after CABGS. The limitations of previous investigations were addressed in this study by consideration of psychosocial as well as sociodemographic and medical factors.
Methods
Study population and procedure
Eligible patients were 444 adults on the waiting list for elective CABGS at The Royal Melbourne Hospital (RMH), Australia, between July 2001 and April 2004. The RMH is a large teaching hospital which serves patients from the western and northern metropolitan area, and therefore from a range of cultural backgrounds. Approval for the study was obtained from The RMH Human Research Ethics Committee. Names and addresses of the patients were taken from the list of patients waiting for surgery at RMH. Patients were mailed the questionnaire package, which included a cover letter, signed by the Head of the Cardiothoracic Surgery Unit, outlining the study and requesting patient consent to participate. The questionnaire order was varied to avoid systematic bias of missing data. Questionnaires were completed before surgery and returned by reply-paid post. Medical records were consulted to obtain medical data and to determine whether patients had had a procedure other than, or additional to, CABGS.
Of the consecutive sample of 444 patients mailed a questionnaire package, 220 patients (50%) completed and returned the questionnaires. The mean interval between completion of the baseline questionnaire and surgery was 32 days (SD = 34 days; median = 24 days). Of the 220 patients who returned their questionnaires, 37 were excluded because it was ascertained that they had not undergone either CABGS or had had a procedure other than CABGS (33 had surgery deferred or cancelled, two had percutaneous coronary intervention, one had valve replacement and one had aortic root repair), leaving 183 included patients. The remaining 224 patients did not return their questionnaire. To ascertain reasons for noncompletion or nonreturn of questionnaires, a random sample of one in three nonresponding patients (n = 78) was contacted by telephone. Reasons for noncompletion of the questionnaire were language difficulties (42%), refusal (38%), death (12%) or disability (8%). Relatives provided information concerning the 12% of patients who had died. The 261 patients who were either excluded or did not return the questionnaire were compared with the 183 included patients on all medical variables, sex and age. Nonparticipants were less likely to have high cholesterol (χ2 = 10.6, df = 1, P = 0.001) and more likely to have a positive family history of cardiovascular disease (CVD) (χ2 = 4.6, df = 1, P = 0.033). No significant differences in all other medical variables, sex or age were observed.
Readmission status was determined using a 3-step method. First, a list of 30-day readmissions to RMH was supplied to the research team by the Medical Records Unit of the hospital. Second, all patients not listed as being readmitted to RMH within 30 days of hospital discharge were contacted by telephone by either the first author (B.M.) or a research assistant to determine whether they had been readmitted to a hospital other than RMH. Patients unable to be contacted by telephone were contacted by post and asked to return a brief form indicating hospital readmissions. Finally, individual patient's hospital medical records from RMH were consulted to (a) verify patient reports of hospital readmissions elsewhere; and (b) determine readmissions to hospitals other than RMH.
Of the 183 patients included at baseline, one patient died during the 30-day follow-up period and the readmission status of another patient could not be determined. Thus, the final study sample comprised 181 patients who completed baseline questionnaires before surgery and for whom readmission data were collected. Exclusions and inclusions are depicted in Fig. 1.
Admission sociodemographic, medical and psychosocial (anxiety, depression and living arrangements) data were collected. Sociodemographic information included age, sex, marital status, country of birth, living arrangements, school leaving age, and current or last occupation. Wherever possible, sociodemographic variables were dichotomized. Marital status was reclassified as married (married or defacto)/unmarried (widowed, divorced or never married). Country of birth was reclassified as English speaking/non-English speaking. Occupations were classified into manual/nonmanual using categories devised by the Australian Institute of Health and Welfare [15]. Medical data included reported high cholesterol (yes/no), hypertension (yes/no), smoking status (current smoker/nonsmoker), body mass index (BMI), positive family history of CVD (yes/no), diabetes mellitus (yes/no), previous MI (yes/no), length of time on waiting list (days) and length of hospital stay (days). New York Heart Association (NYHA) classification of dyspnoea (I, II, III or IV) was included as a measure of disease severity, as in several earlier studies [2,5,11]. Psychosocial data included living arrangements (living alone/with others), and anxiety and depression, assessed using the Hospital Anxiety and Depression Scale (HADS) [16]. The HADS has been found to have good internal consistency, test-retest reliability and construct validity when used with cardiac patients [17,18].
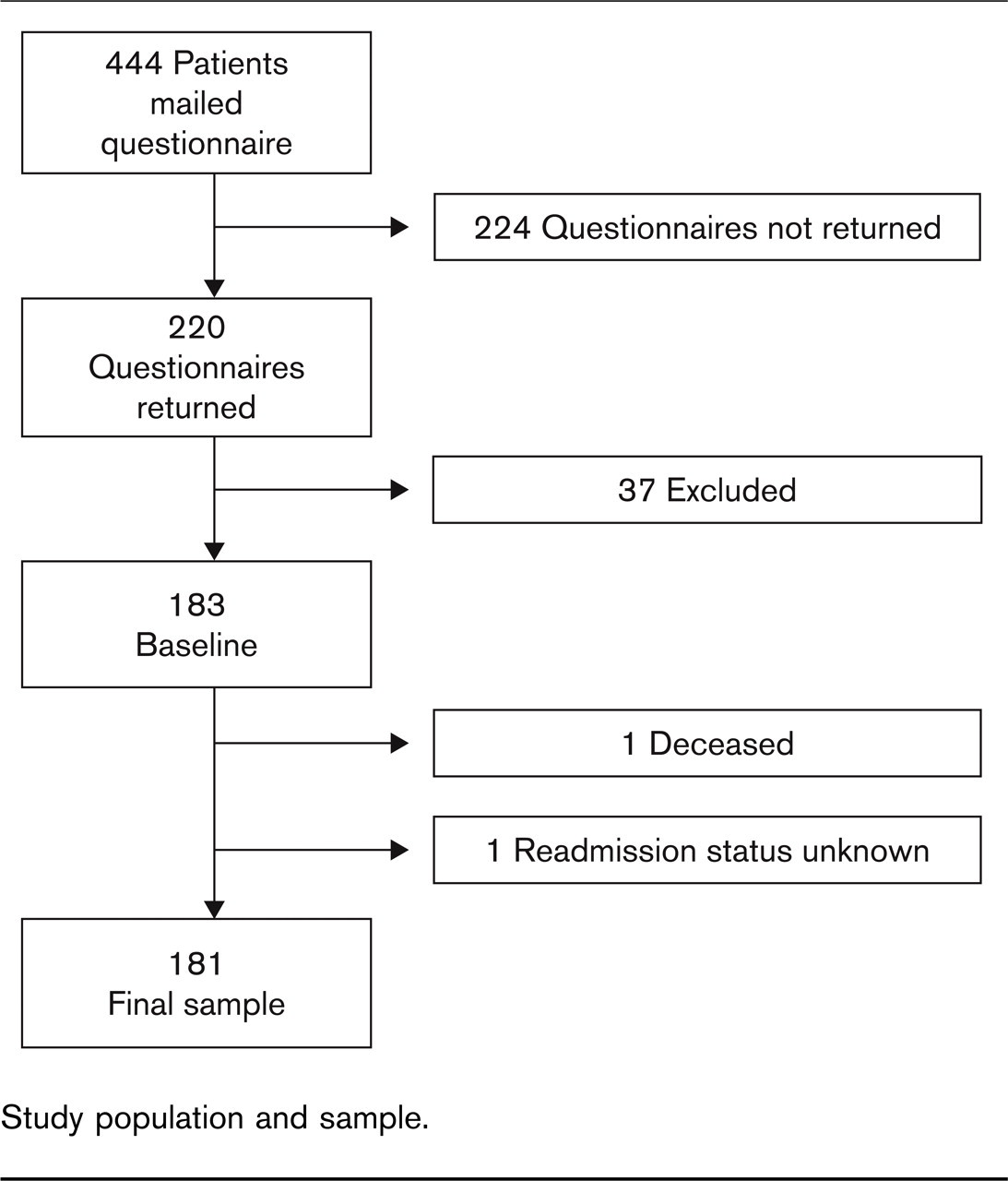
Study population and sample.
Data analysis
Chi-squared and t-tests were used to identify factors associated with 30-day readmission. Variables associated with readmission at P [ 0.1 were entered into a backward stepwise logistic regression to identify the significant predictors of readmission. The significance level was set at P [ 0.1 to reduce the likelihood of type 2 error.
Results
Characteristics of the sample
Patients' ages ranged from 41 to 82 years, with a mean (SD) of 64.0 (9.28) years. Length of hospital stay ranged from 4 to 66 days, with a mean (SD) stay of 7.1 (5.21) days. Only six (3%) patients had a length of stay ≥ 14 days. Other patient characteristics are shown in Table 1. Most patients were male, about three quarters were married and most of them had high cholesterol and/or a history of hypertension.
Sociodemographic and medical characteristics of the study sample at baseline (N = 181)
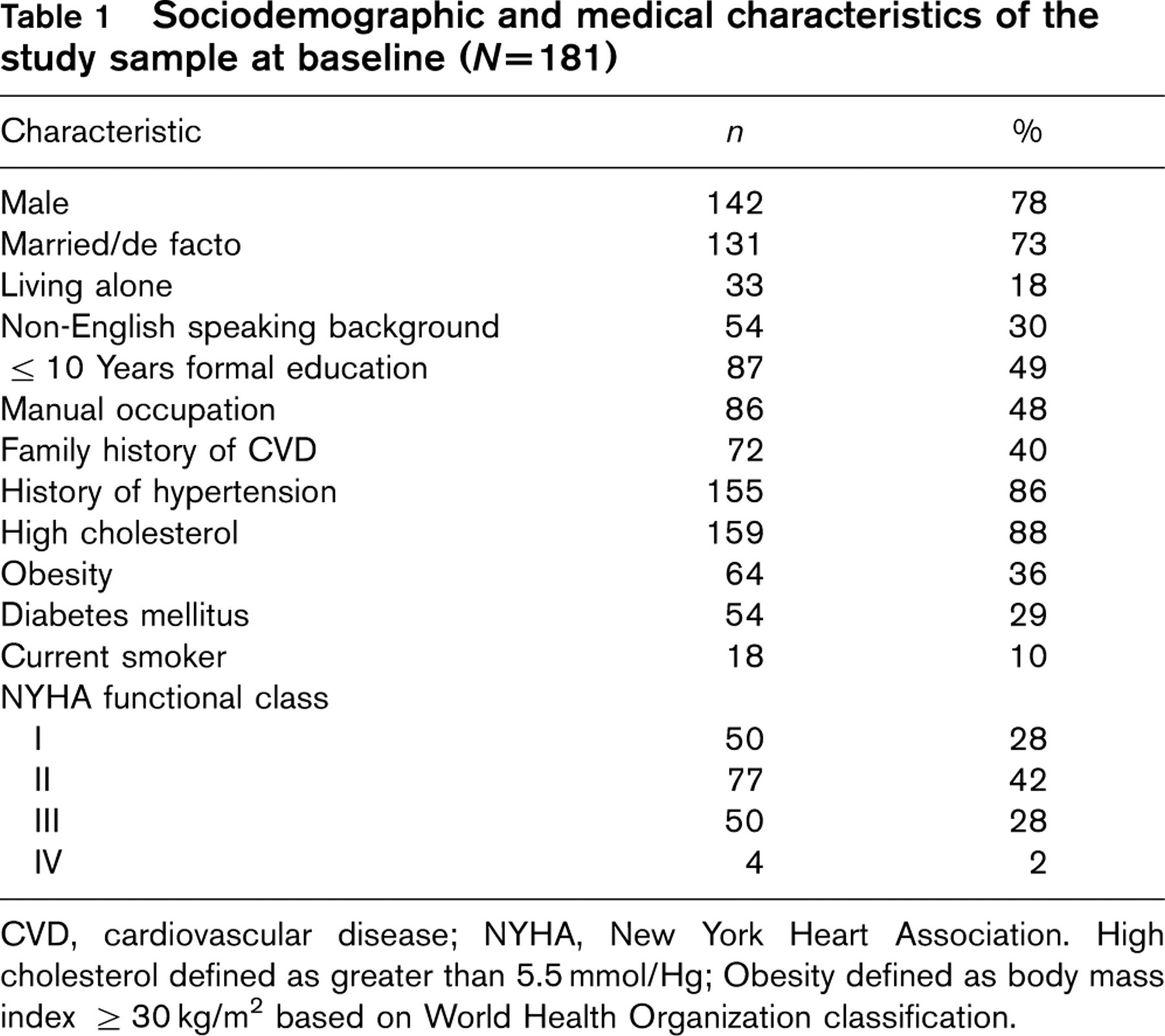
CVD, cardiovascular disease; NYHA, New York Heart Association. High cholesterol defined as greater than 5.5 mmol/Hg; Obesity defined as body mass index > 30 kg/m2 based on World Health Organization classification.
Predictors of 30-day hospital readmission
Of 181 patients, 26 (14.4%) were readmitted to hospital within 30 days of hospital discharge: 24 were readmitted to RMH and two to a nonmetropolitan hospital. In bivariate analyses, the factors found to be associated at P [ 0.1 with readmission were older age (t = 2.12, df = 179, P = 0.035), being unmarried (χ2 = 5.80, df = 1, P = 0.016), living alone (χ2 = 8.33, df = 1, P = 0.004), having a history of hypertension (χ2 = 2.731, df = 1, P = 0.098) and higher HADS anxiety scores at admission (t = 1.67, df = 175, P = 0.097). The remaining socio-demographic and medical variables were not associated with readmission. These were patient sex (P = 0.216), country of birth (P = 0.356), school leaving age (P = 0.888), manual occupation (P = 0.108), high cholesterol (P = 0.917), smoking status (P = 0.261), BMI (P = 0.286), family history of CVD (P = 0.113), diabetes mellitus (P = 0.751), previous MI (P = 0.447), length of time on waiting list (P = 0.377), length of hospital stay (P = 0.746), NYHA class (P = 0.969) and HADS depression score (P = 0.147).
Table 2 shows readmission rates based on the significant (P [ 0.1) patient characteristics. Patients' age and HADS anxiety scores were dichotomized to calculate the readmission rates. HADS anxiety scores ≥8 were classified as indicating clinical levels of anxiety [16]. Readmission rates increased substantially for patients with these key characteristics, most notably increasing from 11% readmission among those living with others to 30% among those living alone.
When the five variables that were associated with readmission in the bivariate analyses (P [ 0.1) were entered into a backward stepwise logistic regression, living alone emerged as the only unique predictor of 30-day hospital readmission after CABGS (Wald = 7.08, odds ratio = 3.42, P = 0.008). Living alone explained approximately 10% of the variance in readmission (Nagelkerke R 2 = 0.096). Results of the logistic regression are shown in Table 3.
Readmission rates based on significant patient characteristics (N = 181)
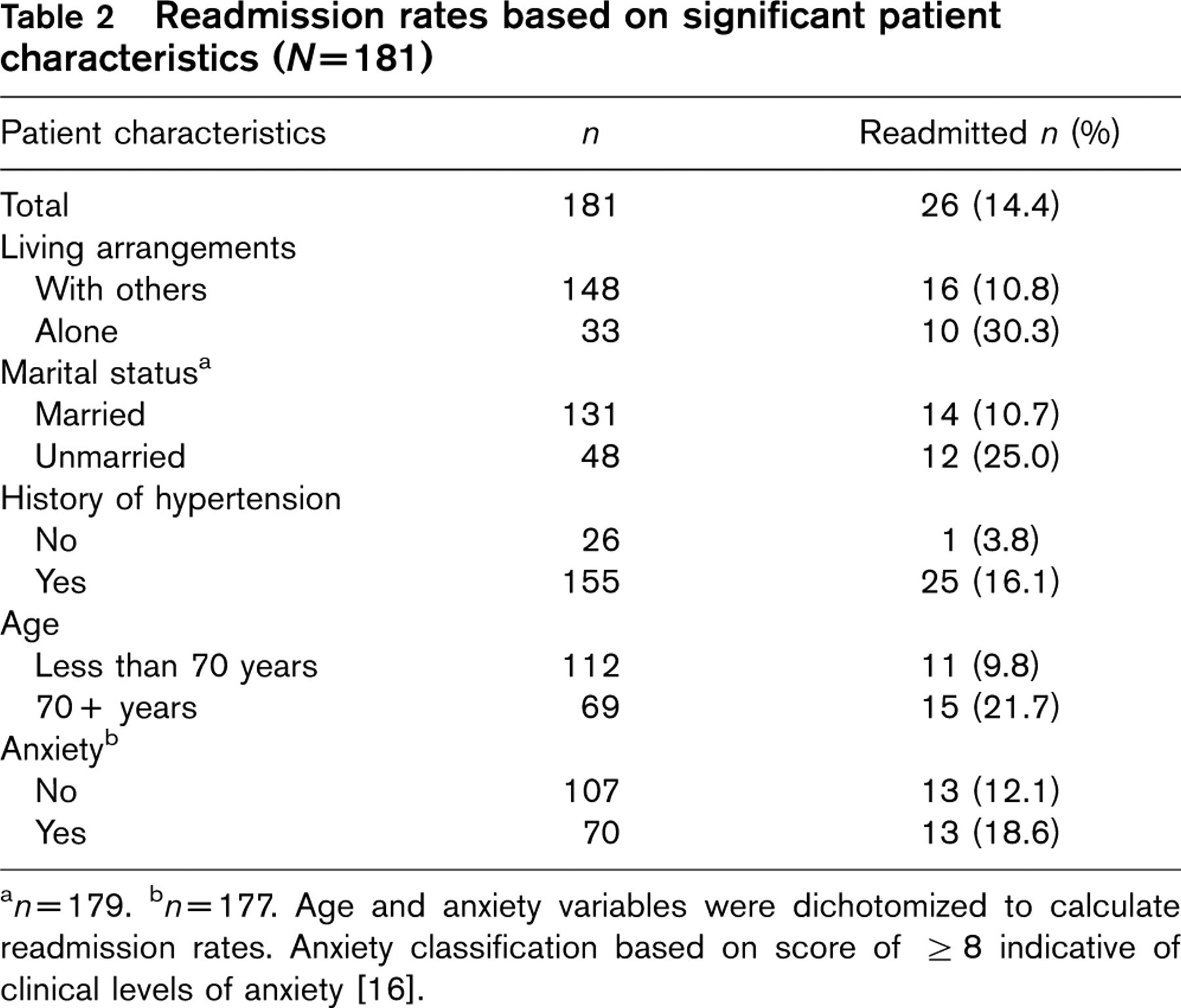
a n = 179.
b n = 177. Age and anxiety variables were dichotomized to calculate readmission rates. Anxiety classification based on score of ≥8 indicative of clinical levels of anxiety [16].
Results of backward stepwise logistic regression to predict 30-day readmission
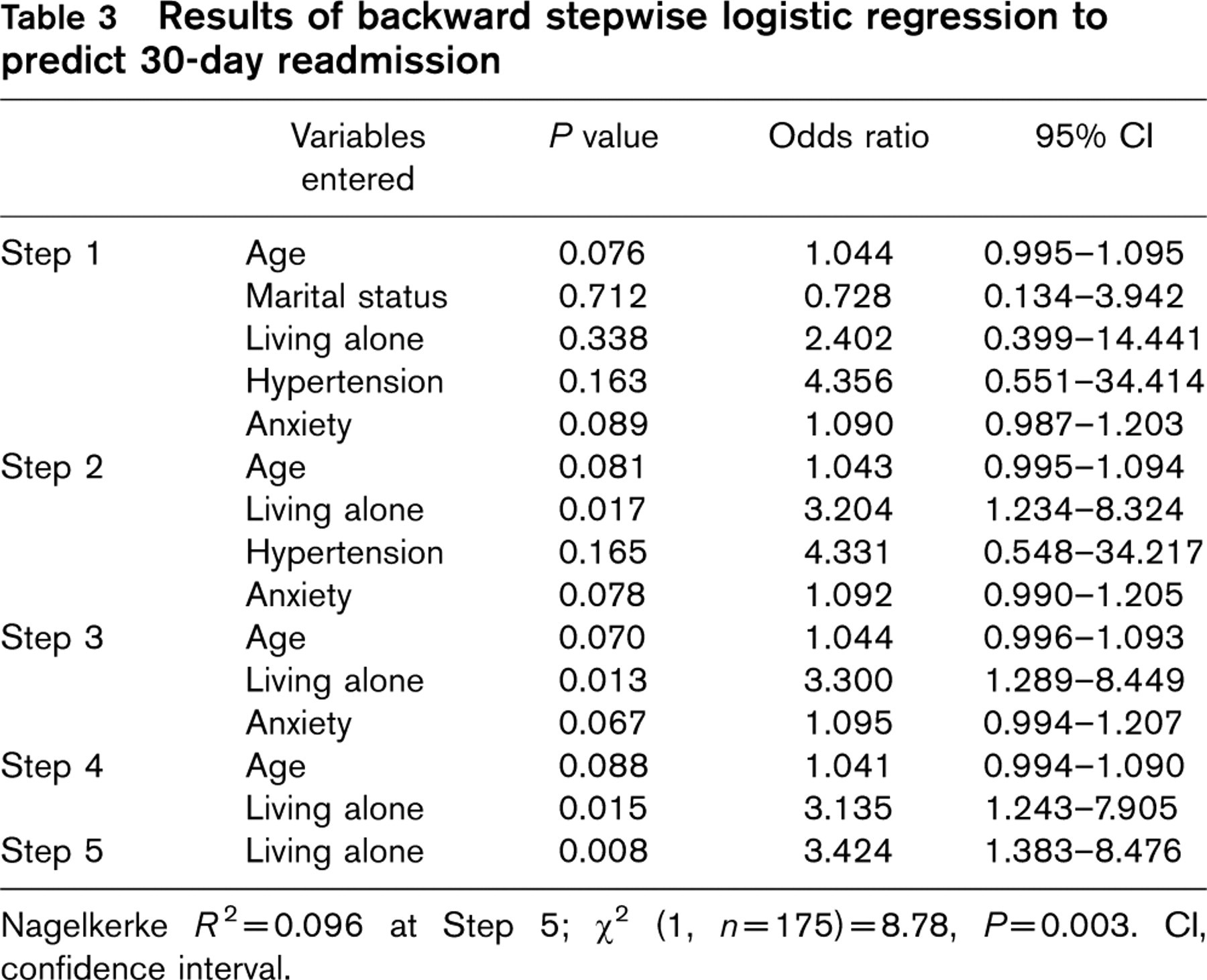
Nagelkerke R 2 = 0.096 at Step 5; χ2 (1, n = 175) = 8.78, P = 0.003. CI, confidence interval.
Discussion
The readmission rate of 14.4% reported here is almost identical to that reported in other larger studies of CABGS patients [4,5]. Patients who lived alone had over three times the risk of early readmission, with the readmission rate increasing from 11% among patients who lived with others to 30% among those who lived alone. One earlier study in this area has identified living alone as a risk factor for 100-day hospital readmission [9]. No other studies have explored the relative importance of psychosocial, medical and sociodemographic factors in predisposing patients to hospital readmission.
A number of reasons for why living alone might increase the risk of readmission have been obtained. Patients who are socially isolated are more likely to smoke and drink alcohol heavily [19,20], present with a second or subsequent MI [19], delay in seeking treatment [21] and demonstrate nonadherence to medical regimens [22]; these are the factors associated with poorer health outcomes. Indeed, at least one earlier study has identified living alone as a predictor of death in patients hospitalized for acute coronary syndrome [23]. In our study though, patients who lived alone were no more likely than others either to smoke (P = 0.271), or to have diabetes (P = 0.711), high cholesterol (P = 0.613), hypertension (P = 0.905), previous MI (P = 0.945), higher BMI (P = 0.607), more severe disease (P = 0.355), or to be older (P = 0.223). Moreover, apart from hypertension, medical factors including disease severity, indicated by NYHA class and previous MI, were themselves unrelated to early hospital readmission.
Alternatively, it could be hypothesized that living alone is associated with socioeconomic disadvantage and low education, both of which have been linked with poorer health outcomes following a cardiac event [24,25]. In our study, however, neither living alone nor readmission was related to markers of low socioeconomic status, including level of education and occupation.
Instead of medical, behavioural or socioeconomic explanations, it appears that the increased risk of readmission evident among patients who live alone is simply due to lack of emotional or practical support gained through living with another person. It is possible that simply having another person in the house helps to allay the patients' fears and anxieties, particularly those experienced during the night and associated with physical symptoms such as sinus tachycardia, which is common in the early convalescent period. Without reassurance from another person when they experience such symptoms, patients who live alone might feel a greater need to return to the care environment. Thus, just as living alone increases the risk of recurrent cardiac events [26], so too it increases the risk of hospital readmission.
It is noteworthy that marital status was associated with hospital readmission, as in earlier studies [13,14], although it did not remain in the final regression model. Clearly there was a substantial overlap between marital status and living arrangements: the two variables were significantly associated with one another (χ2 = 110.42, df= 1, P [ 0.001) and shared much of the variance in predicting readmission (Table 3). Although it is highly likely that patients who live alone are unmarried, the reverse may not always be true. Indeed, a cross tabulation between the two variables confirmed that, while no married patients lived alone, 15 unmarried patients lived with others, presumably adult offspring, siblings or other relatives or friends. Despite the overlap between the two variables, we had no a priori theoretical grounds for elevating one variable over the other. Of the two earlier studies that have investigated psychosocial predictors of readmission, one identified marital status as a predictor [13] and the other identified living alone as a predictor [9]. That our statistical analysis identified living alone as a stronger predictor of readmission than marital status, underscores the importance of living with another person regardless of the relationship.
A trend for presurgical anxiety to be associated with 30-day hospital readmission was also observed. Earlier studies have demonstrated that postsurgical anxiety experienced is associated with increased rates of rehospitalization and health care consumption [27], and also increased morbidity and mortality [28,29]. With a focus on presurgical anxiety rather than postevent anxiety, our study highlights the possibility that anxiety might be a preexisting risk factor for rehospitalization after CABGS.
Unlike several earlier large-scale studies, which identified medical risk factors for admission, such as obesity, diabetes, previous MI and longer hospital stay [2–5,8], we did not find associations between these medical factors and hospital readmission. Likewise, disease severity as measured by the NYHA classification was not associated with readmission, contrary to some previous findings [2,5,11]. Perhaps with a larger sample, these medical risk factors for readmission might have been identified. Even in a study of over 4000 patients, Zitser-Gurevich and colleagues [9] did not find an association between disease severity and hospital readmission.
A history of hypertension was the only medical variable associated with increased risk of readmission. Importantly, the rate of readmission increased only marginally to 16% among those with hypertension. Those without a history of hypertension, who represent a minority of the study sample (14%), had a very low readmission rate of 4%, suggesting that having no previous history of hypertension was a protective factor for these patients.
The present findings raise concerns about patients who live alone being discharged from hospital without adequate planning for support options. Those who live alone need focussed discharge planning that mobilizes family members, other relatives and friends to provide support during the convalescent period. Ideally, patients should not be discharged home alone, and instead should stay with a friend or family member for the first several nights after discharge. Patients without family might need extra formal services to support them during this time. Patients who live alone could easily be identified before surgery so that appropriate arrangements can be made. Living alone is such an easily determinable marker of risk that it underscores the importance of the findings of this study. More comprehensive assessment of social support needs could be undertaken with patients found on admission to live alone. Presurgical screening might also be beneficial to identify other patients at risk of readmission, particularly those experiencing high levels of anxiety, and unmarried patients. Again comprehensive assessment could follow to determine existing supports and identify unmet needs for support.
It is interesting to note that earlier studies have identified living alone as a key predictor of both reevents [26] and mortality [23], in patients with acute coronary syndrome and MI, respectively. Our study extends previous findings by identifying living alone as a risk for readmission in CABGS patients. The consistency across studies in different cardiac populations and using different outcome measures highlights the importance of this simple, easily determinable marker of risk.
This study has some limitations. First, while the 50% return rate is consistent with that for previous postal surveys for this patient group [30], it reduces the external validity of the study findings. The fact that participants and nonparticipants were comparable in terms of age, sex and all but two medical risk factors lends some support to the generalizability of the findings. Moreover, the rate of 14.4% readmission reported here is almost identical to that reported in other larger studies of CABGS patients [4,5], providing further validation of our findings.
Second, we did not include a comprehensive measure of social support or assess patients' experiences of and satisfaction with their support networks. It is possible that living alone is a greater risk factor for patients without other support networks. Without additional measures of social support, we were unable to investigate this possibility.
Finally, the study relied on self-report assessment of anxiety and depression before surgery. The validity of self-report measures can be compromised by patient denial, frailty and comorbidities [17]. Despite the limitations, the HADS has been found to have good internal consistency, test-retest reliability and construct validity when used in this patient population [17,18].
Conclusion
Unlike earlier studies, in this study we explored the relative importance of psychosocial as well as medical and socio-demographic factors in predicting 30-day hospital re-admission. Living alone was identified as the single most important risk factor for early hospital readmission after CABGS. Patients who live alone might benefit from additional support during early convalescence. Intervention studies are needed to investigate the benefits of presurgical screening to identify patients at risk for early readmission, and to explore support options for patients who live alone. In the meantime, health professionals should enquire about living arrangements at the time when patients are waitlisted for surgery, so that appropriate arrangements can be made for care during convalescence.
Footnotes
Acknowledgements
Funding for this study was provided by the Percy Baxter Charitable Trust, the Eirene Lucas Foundation, and the Marian and EH Flack Trust. The authors would like to acknowledge the contributions of Ms Hema Navaratnam, Heart Research Centre, and Mrs Marlyn Reid, Department of Cardiothoracic Surgery, The Royal Melbourne Hospital.
Conflict of interest: none declared.