
Abstract
Background
Little is known about the relative cost-effectiveness of different secondary prevention cardiac rehabilitation (CR) program designs or how cost-effectiveness is influenced by patient clinical and demographic characteristics. The purpose of the study was (i) to evaluate the incremental cost-effectiveness of a standard 3-month CR program (SCR) versus a program distributed over 12 months (distributed CR, DCR); and (ii) to determine the effect of patient demographic characteristics (cardiac risk, cardiac diagnosis, sex) on incremental cost-effectiveness.
Methods
A two group cost-effectiveness analysis was conducted alongside a randomized controlled trial. Patients with coronary artery disease (mean age = 58 years, SD ± 10) were randomized to either SCR (n = 196) or DCR (n = 196) and followed for 24 months. Program delivery costs, cardiac healthcare use, morbidity, mortality, and quality-adjusted life years were assessed. Cost-effectiveness was evaluated with incremental cost-utility analysis.
Results
In the pooled analysis, we found the probability of SCR being more cost-effective than DCR was 63–67%. The subanalysis found SCR to be the more cost-effective intervention for patients at high risk, patients with previous coronary artery bypass graft and for male patients. The DCR program was more cost-effective for patients with lower risk of disease progression and for female patients.
Conclusion
Differences were noted in the cost-effectiveness of CR models based on cardiac risk level, reason for referral, and demographic characteristics. Our results suggest improved cost-effectiveness may be gained by triaging patients to different CR intervention models, however, further investigation is required.
Background
An aging population and continuing constraints on healthcare resources accentuates the need to develop and deliver cost-effective interventions for the secondary prevention and management of cardiovascular disease. Secondary prevention cardiac rehabilitation (CR) has been recommended for all eligible patients with coronary artery disease (CAD) [1–3]. The dose response model, however, including frequency and duration, that is required to produce optimum gains in patient health-related quality of life (HRQL), clinical status, and cost-effectiveness is unknown.
The standard CR (SCR) intervention typically consists of medical evaluation, behavioral change, cardiac risk factor modification, education, counseling, and supervised exercise training on 2–3 days per week over 12 weeks [1–3]. Participation in a 12-week SCR program has been shown to result in positive changes in cardiac risk factors, mortality, and HRQL in patients with CAD [4]. There is evidence in some [5], but not all [6] studies that patients may gain additional benefit from extending the SCR program length beyond the standard 12 weeks to ensure long-term behavior change and optimal risk factor control is observed. In this study, the SCR program content was extended over a 52-week period and we defined this as distributed CR (DCR).
Economic analyses are an important tool for the evaluation of competing healthcare interventions. To date, three trials have offered prospective randomized controlled trial evidence of the cost-utility of CR versus standard care [7–9] but none have compared alternative CR program delivery models. Little is known about the relative cost-effectiveness of different CR program designs and whether program cost-effectiveness is influenced by a patient's clinical and demographic characteristics [10]. Previous researchers [10,11] have suggested that patient characteristics may influence the cost-effectiveness derived from CR interventions. Developing an understanding about which patient populations derive the greatest benefits from available intervention models may assist with optimizing the use of scarce healthcare resources.
Therefore, the aim of this study was to compare the cost-effectiveness of a SCR versus a DCR program model using incremental cost-utility at the end of a 24-month follow-up, and to evaluate the effect of patient demographic characteristics (cardiac risk, reason for referral, sex) on the incremental cost-utility.
Methods
This economic evaluation was conducted alongside a two-group randomized control trial evaluating the efficacy of SCR and DCR on clinical outcomes [6]. Eligibility was based upon documentation of CAD, English proficiency, and geographic availability for intervention and follow-up. The primary outcome measure was the incremental cost-utility ratio (ICUR) determined as the cost (2004US$) per quality-adjusted life year (QALY) gained evaluated from the perspective of the healthcare system focusing on costs related to CAD over a 2-year follow-up period. Follow-up data collection occurred at 3, 6, 12, 15, and 24 months.
Intervention comparators
Two models of CR service delivery were compared: SCR versus DCR. The SCR intervention consisted of 33 program contacts delivered twice weekly over a 3-month period. The DCR intervention delivered the 33 program contacts over a 12-month period with contacts tapered over time. The DCR intervention was designed in accordance with behavior change theories which suggest patients may require up to 12-months or more to establish new lifestyle patterns and improvement in HRQL with contacts concentrated early in the behavior change process and tapered over time [12], and which have been experimentally tested in CR [5,6].
Four types of contacts were provided to each group and are described in detail elsewhere [6]: case manager contacts to support behavior modification (n = 3), physician consult for medical management of risk factors (n = 1), group educational workshops (n = 2), and supervised exercise classes (n = 27). Both intervention groups received 27 supervised exercise sessions with participants in the SCR program receiving twice weekly exercise sessions over 3 months and those in the DCR receiving exercise sessions that were tapered from weekly to monthly over 12 months. Referral to specialized services was made as required to meet individual patient rehabilitation needs.
Economic evaluation
Cost-utility analysis (CUA) is a special case of cost-effectiveness analysis in which the health effect is measured in terms of QALYs gained and which is recommended in both US and Canadian guidelines for health economic analyses as the gold standard methodology in the economic evaluation of healthcare interventions [13,14]. The ICUR is the basis of the CUA and calculated as ICUR = (Cost a–Cost b)/(QALY a–QALY b). Four possible findings can result when comparing the ICUR between two treatments: (i) experimental therapy is less expensive and more effective than existing therapy ('dominant'); (ii) existing therapy is less expensive and more effective than experimental therapy ('dominant'); (iii) experimental therapy is more expensive but also more effective; and (iv) experimental therapy is less expensive but also less effective.
Cost determination
The principal resource items of interest were the costs associated with CR program delivery and the use of cardiac specific healthcare resources. The use of cardiac specific healthcare resources was estimated by a 10-item questionnaire delivered to patients at each of the follow-up time points. Clinical events, including death, myocardial infarction (MI), and repeat revascularizations, were tracked from the date of randomization until the 2-year follow-up.
Cost valuation
The cost of sessions for the CR programs was measured using a bottom-up costing methodology with institutional cost data used to calculate professional staff wages, equipment, and overhead. The cost of cardiac procedures and diagnostic tests was obtained from published costing analyses [15,16]. Costs are presented in 2004 US dollars (2004US$) using the 2004 exchange rate for Canadian dollars (ÏS$ = $1.30CDN$) and the 2004 US consumer price index for medical care [17].
Quality-adjusted life years
The mean incremental change in QALYs was used as the measure of effectiveness in the present analysis. The time trade-off preference-based utility scores (measured on an interval scale ranging from 0.0 representing death to 1.0 representing full health) are used to estimate mean gain in QALYs [18].
Statistical analysis
Costs (program delivery plus healthcare utilization) were summed over the entire 2-year period for each participant and total costs were compared between groups using a t-test. QALYs gained were calculated for the 2-year study period using the area under the curve methodology [19] and the ICUR calculated. Bootstrapping was used to describe the underlying variation in the study sample [20]. The bootstrapped pairs (n = 10000) are represented graphically on a cost-effectiveness plane as well as on a cost-effectiveness acceptability curve (CEAC). The CEAC is a widely adopted method to quantify and graphically represent the uncertainty in estimates of cost-effectiveness [21]. Differences in cost-utility between patient groups were explored using stratified analyses. Stratification variables were selected a priori to reflect those factors identified by previous researchers [10,11] as potentially important variables in predicting cost-effectiveness of CR programs. Stratification variables were: Canadian Association of Cardiac Rehabilitation (CACR) (i) acute risk and (ii) risk of disease progression (low, moderate, high), (iii) reason for referral [i.e. MI, percutaneous coronary intervention (PCI), coronary artery bypass graft (CABG)], and (iv) sex [1]. The reason for referral was obtained from the cardiac diagnosis identified on the CR referral form. A minimum of 40 individuals per patient group was required for subgroup analysis. The ICUR (cost per QALY) was generated for each stratification group. The robustness of the results was reported as the probability that DCR is more cost-effective than SCR at a threshold of $50000/QALY [22].
Results
Participant flow and follow-up
Six hundred and five patients with CAD referred to CR between September 1999 and March 2001 were asked to participate in the study and 396 (66%) agreed to do so. Four participants were excluded from the study when additional testing established that they were free of CAD. Compared with those who refused participation, study participants were younger (58 vs. 60 years; P = 0.02) and less likely to be current smokers (7 vs. 13%; P = 0.03). Participants and nonparticipants were similar on sex, education, BMI, and clinical diagnosis. In total, 392 participants (196 to SCR and 196 to DCR) were randomly allocated to treatment.
Twenty-two percent of the 392 patients were lost to follow-up, with a larger proportion of women than men lost to follow-up (P = 0.03). No difference between the SCR and DCR groups were observed in lost to follow-up rates (40 in SCR vs. 45 in DCR, P = 0.52), age, education, or clinical diagnosis. Data analysis was, therefore, based on the 307 participants for whom data were available at the end of the 2-year follow-up period.
Patient characteristics
A summary of patient characteristics is provided in Table 1. Groups were balanced with respect to age, education (years), and reason for referral.
Morbidity and mortality
In the 24-month period following baseline assessment, there were six deaths (SCR = 2; DCR = 4); four of which were cardiac-related (SCR, n = 1; DCR, n = 3) and two cancer-related (SCR, n = 1; DCR, n = 1). The total number of participants with a primary adverse cardiac event (i.e. cardiac death, or hospitalization for nonfatal MI, PCI, or CABG) over the 2 years was the same (n = 22) in both the SCR and DCR groups.
Incremental cost-utility
The mean direct costs of the SCR and DCR interventions are provided in Table 2. The incremental costs, the mean QALYs gained, the ICURs, and their interpretation for the entire sample and the subgroup analyses are provided in Table 3. The SCR intervention was found to cost $103 (95% confidence interval: –$355 to $479.00) less than the DCR intervention (not significant). A mean QALY gain was found in the SCR of 0.062 QALYs compared 0.053 QALYs in the DCR resulting in an incremental gain of 0.009 (95% confidence interval: 0.004–0.013) QALYs in favor of SCR (not significant). The base case point estimate for the ICUR of the entire sample showed SCR to be dominant although the between-groups differences are minimal. The cost-effectiveness plane scatter plot of the individual bootstrap cost-effect points (Fig. 1) demonstrates significant variability in the cost-effectiveness of the intervention models within the study sample. A CEAC was used to summarize the probability of a positive benefit (number of times the bootstrap ICUR replications fall below the threshold monetary values plotted on the cost-effectiveness plane) for specific incremental cost-effectiveness thresholds (Fig. 2). The observed probability of a benefit for SCR ranged between 0.63 and 0.67 indicating the probability of SCR being cost-effective ranges between 63 and 67%, depending on the cost per QALY threshold chosen which in this case ranged from $0 to $100000.
Participant sociodemographic and clinical characteristics
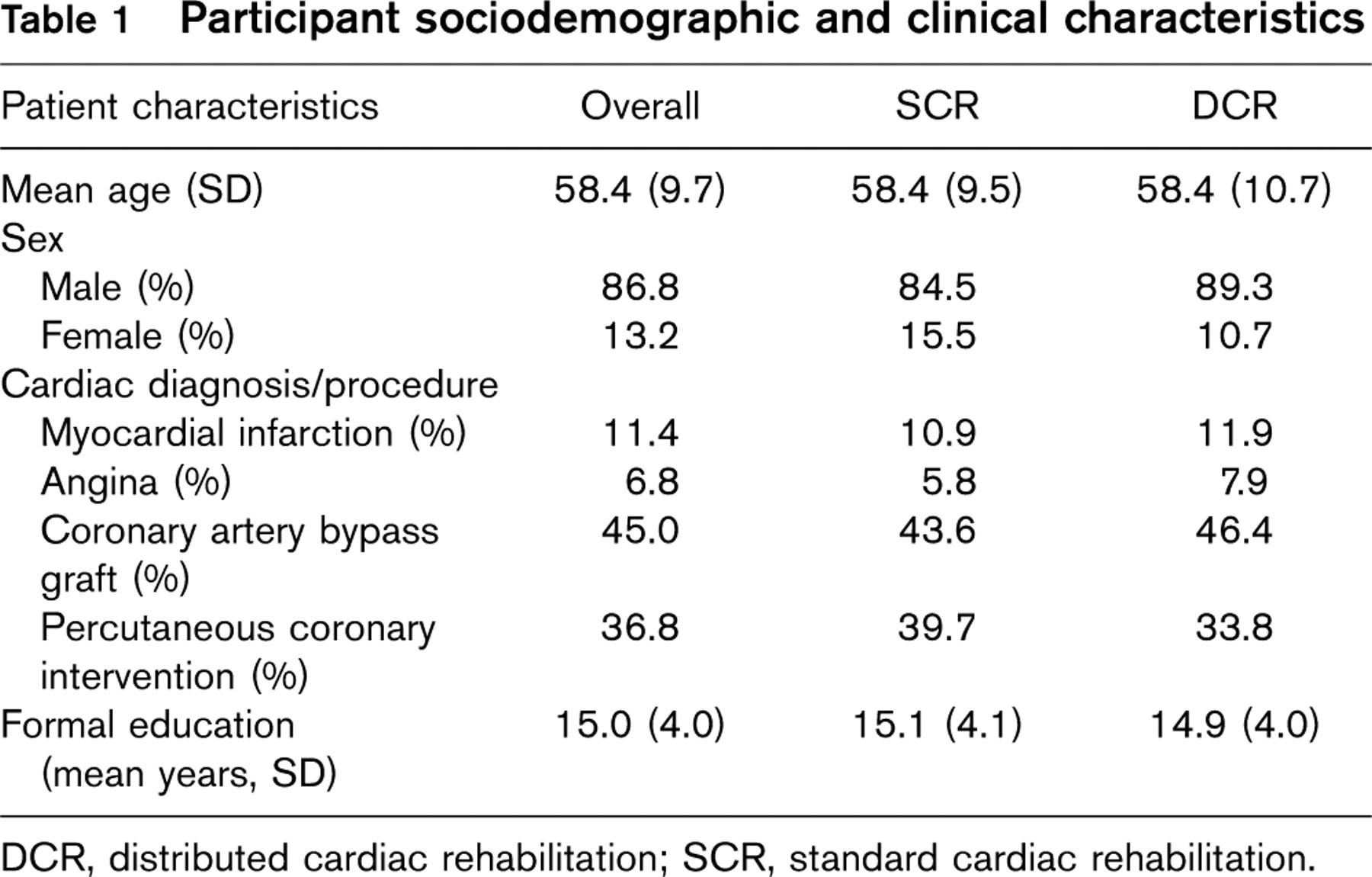
DCR, distributed cardiac rehabilitation; SCR, standard cardiac rehabilitation.
Mean direct costs per patient for SCR and DCR
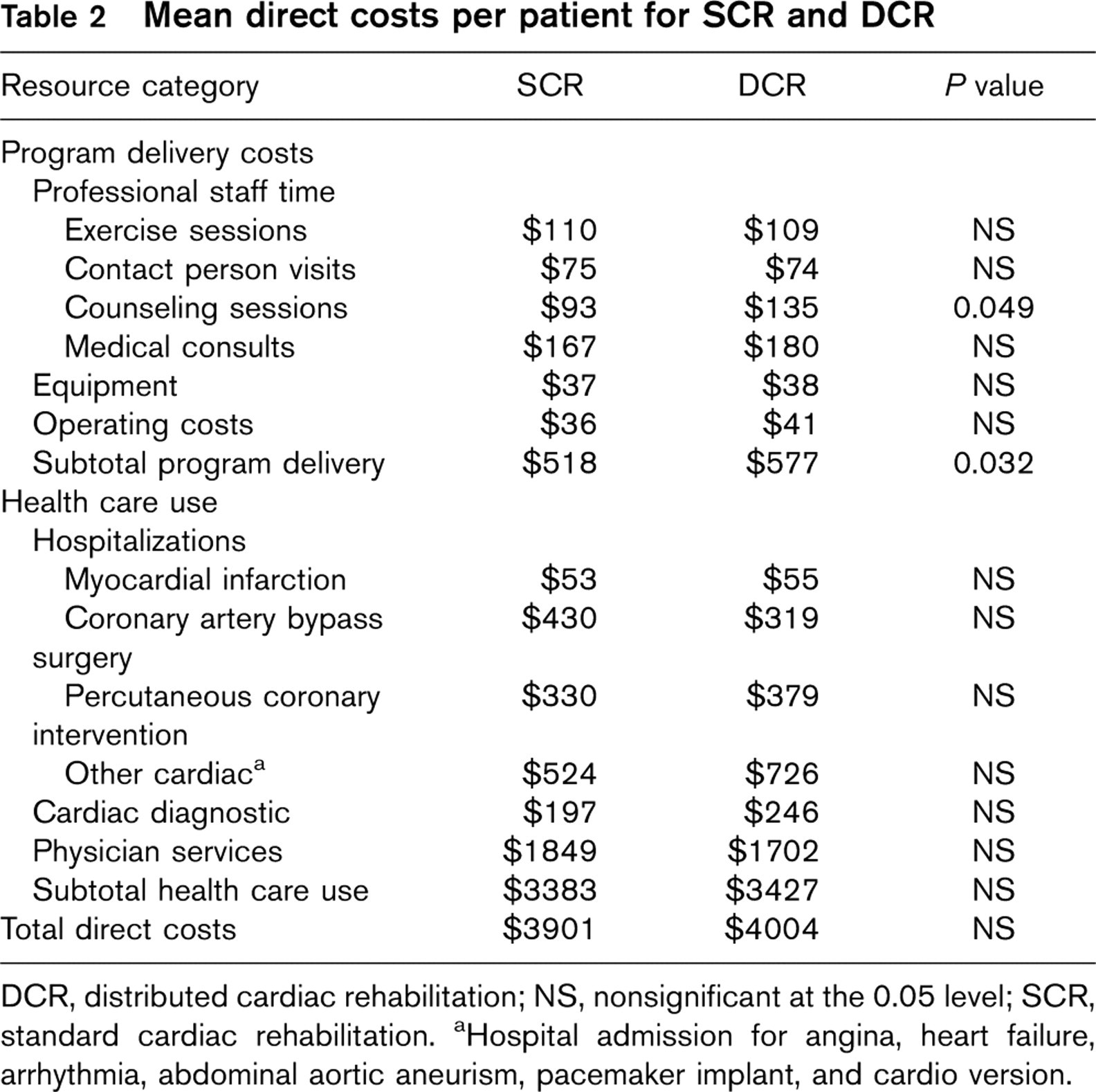
DCR, distributed cardiac rehabilitation; NS, nonsignificant at the 0.05 level; SCR, standard cardiac rehabilitation. aHospital admission for angina, heart failure, arrhythmia, abdominal aortic aneurism, pacemaker implant, and cardio version.
Incremental costs (DCR minus SCR costs in 2004US$), QALYs gained, and ICUR by the entire sample analysis (SCR vs. DCR) and by the subgroup analyses (acute cardiac risk strata, risk of disease progression, referring diagnosis, and sex by SCR vs. DCR)
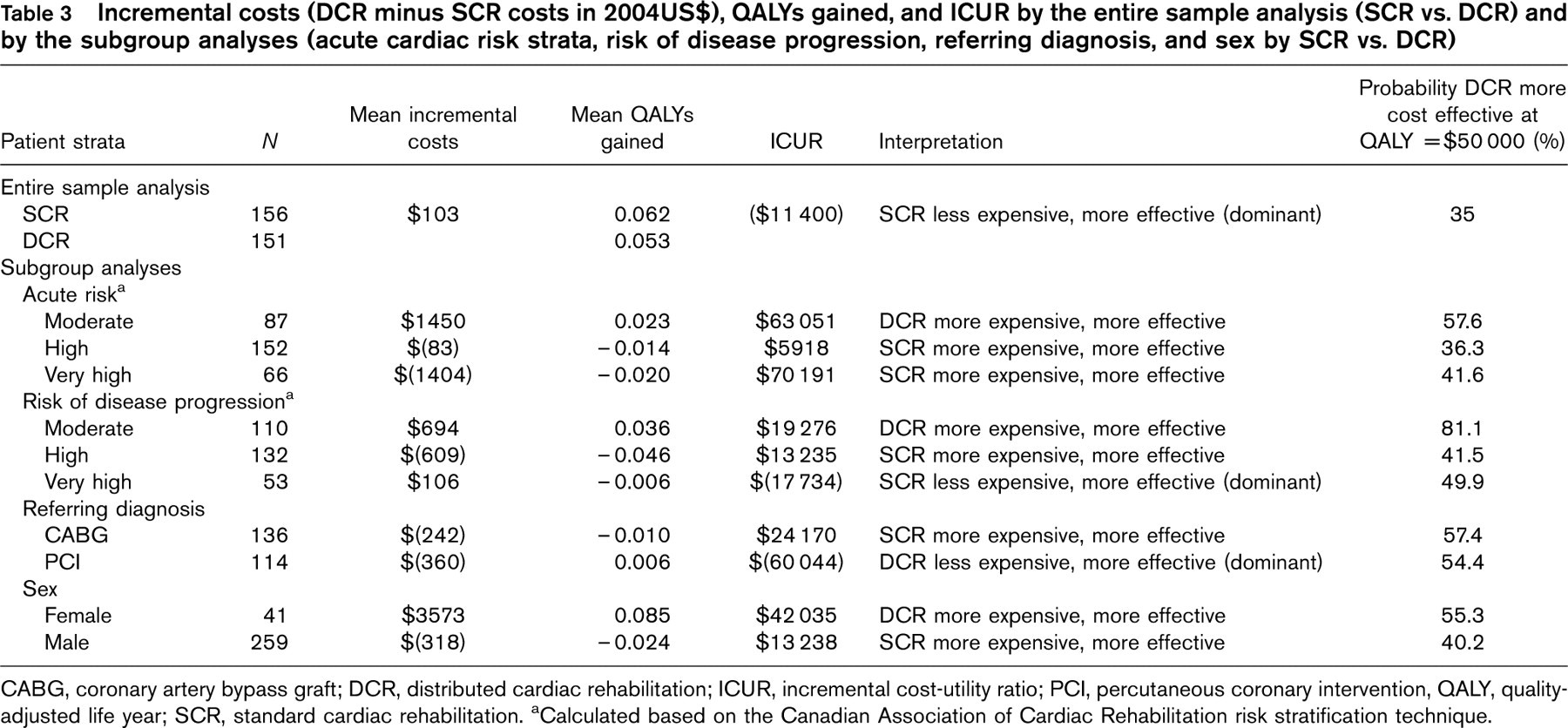
CABG, coronary artery bypass graft; DCR, distributed cardiac rehabilitation; ICUR, incremental cost-utility ratio; PCI, percutaneous coronary intervention, QALY, quality-adjusted life year; SCR, standard cardiac rehabilitation. aCalculated based on the Canadian Association of Cardiac Rehabilitation risk stratification technique.
Cost-utility of distributed cardiac rehabilitation and standard cardiac rehabilitation by patient subgroup
Table 3 presents the results of the subgroup analyses; as there were fewer than 40 patients with angina and MI as the reason for referral, angina and MI were not considered as predictor variables. Differences were observed in both the mean QALYs gained and mean healthcare costs across patient subgroups. The ICUR in patients with a very high CACR risk of disease progression demonstrates that SCR is dominant over DCR. The ICUR in patients with PCI demonstrates that DCR is dominant over SCR. The ICURs in patients with a high and a very high CACR acute risk, and high CACR risk for disease progression, with CABG and male sex demonstrate that SCR is more expensive but more effective than DCR. The ICURs associated with a moderate CACR acute risk, a moderate CACR risk of disease progression and female sex demonstrate that DCR is more expensive but more effective than SCR.
Discussion
When analyzed across the entire study sample, the incremental costs were $103 and the incremental QALYs gained were 0.009, both in favor of the SCR program delivery mode, meaning that SCR was dominant when compared with the DCR program delivery mode. To date, CUAs have been limited to the evaluation of CR against standard care and this study is, to our knowledge, the only CUA to have compared two alternative CR program delivery models. In a 1993 CUA of CR services, an 8-week CR intervention, Oldridge and colleagues [7] compared CR against a standard care control group in MI patients and reported a mean incremental gain of 0.052 QALYs with an ICUR of $16118/QALY gained when compared with a standard care control group. A second CUA was published which reported savings of $668 per QALY gained for supervised CR versus standard care in a 2-year follow-up of patients with MI and PCI in Hong Kong [8]. Most recently, Briffa [9] reported an ICUR of $42535/QALY saved for comprehensive CR relative to standard care, with large variations observed in their sensitivity analysis.
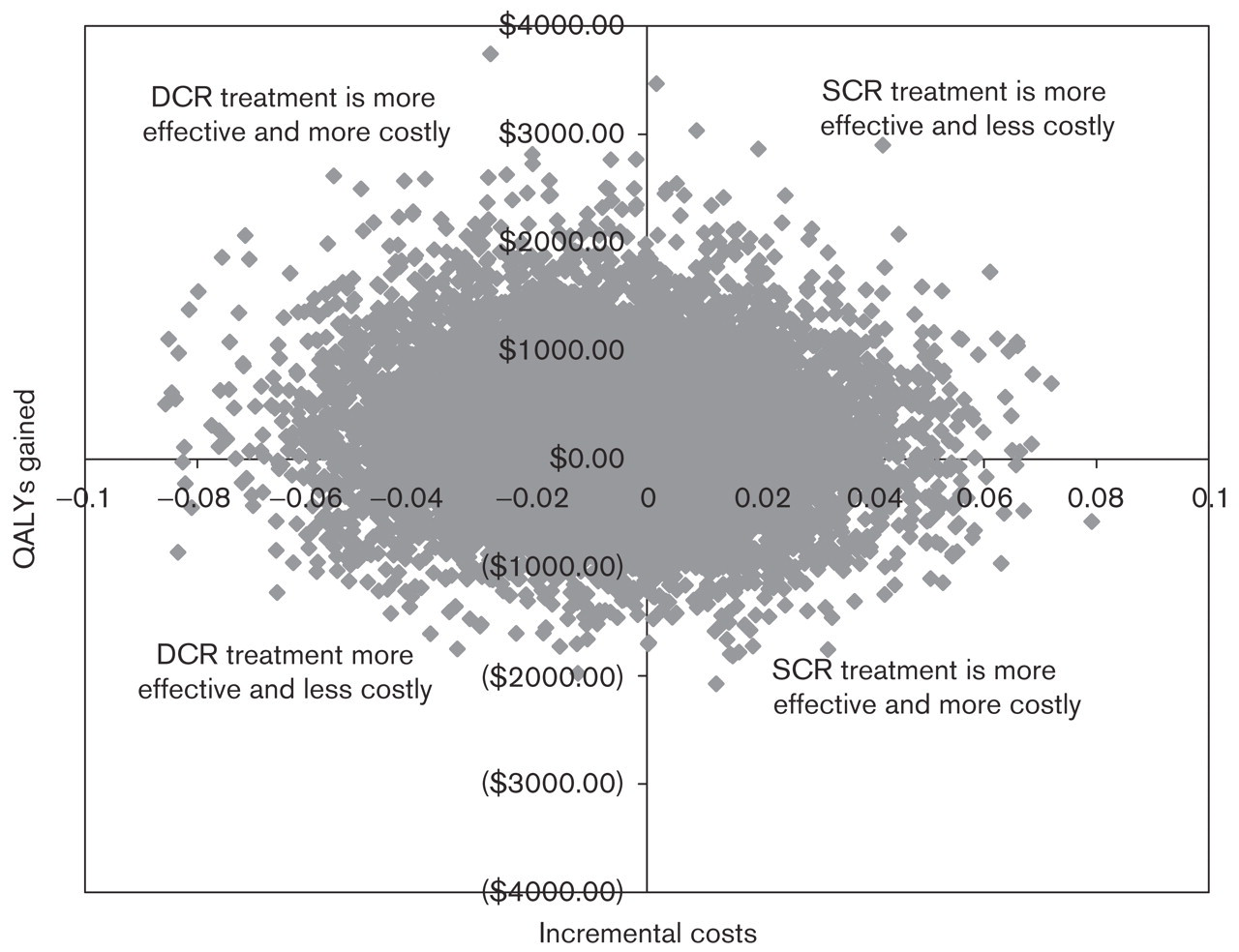
Cost-effectiveness plane scatter plot of the incremental cost and incremental quality-adjusted life years (QALY) gained generated from bootstrap replications (B = 10000).
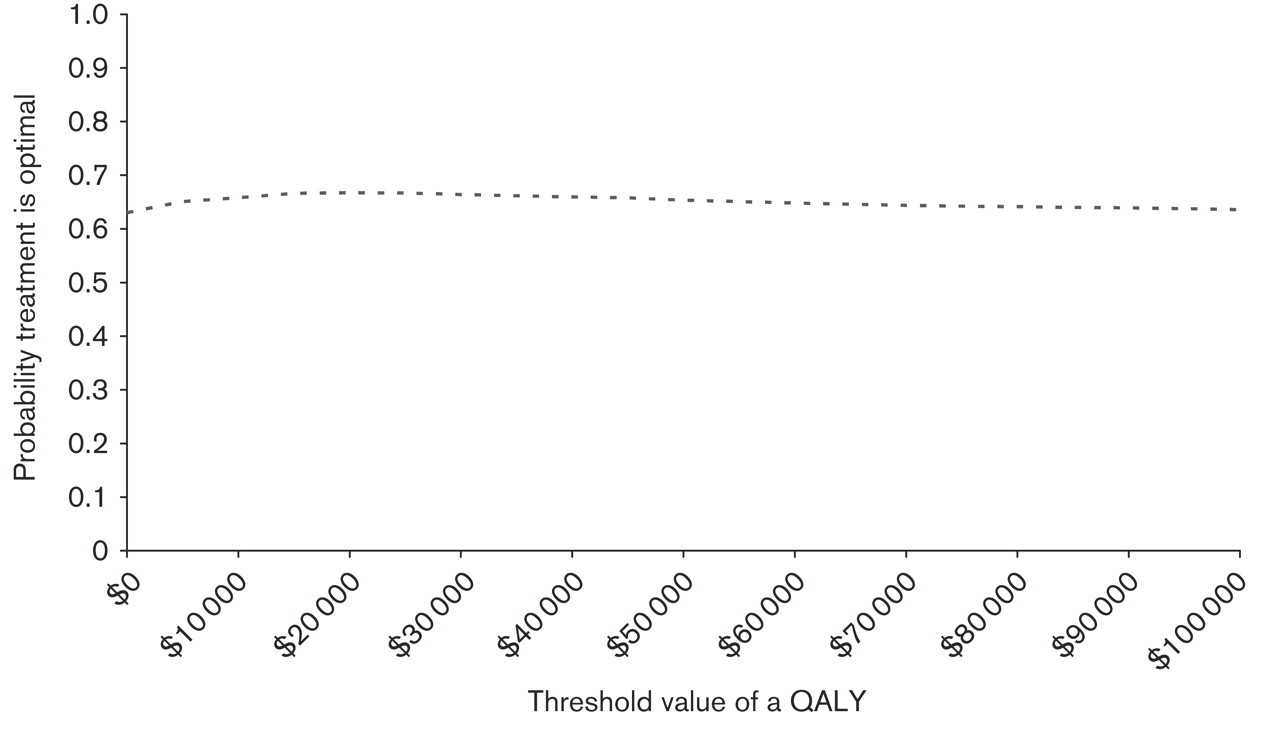
Cost-effectiveness acceptability curve illustrating the probability that standard cardiac rehabilitation is optimal at each of the monetary threshold values. QALY, quality-adjusted life years.
Our analysis across the entire study sample, however, found significant variability in the bootstrap individual cost-effect points which cross all four quadrants of the cost-utility plane (see Fig. 1). This finding suggests the possible presence of subgroup differences in cost-utility of intervention models. Differences were noted in the cost-effectiveness of the two CR models based on cardiac risk level, reason for referral, and demographic characteristics. We found SCR to be more cost-effective than DCR for men, for CABG patients, and for patients at high risk of disease progression while, in contrast, DCR provided greater cost-effectiveness in women and patients at lower risk of disease progression. Our results serve to validate earlier hypotheses regarding differential economic benefits of CR among patients of varying clinical risk and reason for referral [10] and work by Lowensteyn et al. [11], which suggested the cost-effectiveness of CR was more favorable for men than for women. The certainty associated with the subgroup analysis, however, varies across patient clinical and demographic groups suggesting future research is required to validate the trends observed in this study.
Developing an understanding of the influence of clinical and demographic factors on cost and benefits derived from CR may assist with improving the overall effectiveness and cost-effectiveness of CR services. Since the cardiac patient population displays significant heterogeneity, the potential to enhance the cost-effectiveness of CR may be increased by effectively matching patients to a CR program model tailored to the needs of patient subgroups. Further investigation is required to validate the added value of patient triage on the basis of reason for referral, cardiac risk, and sex. Other patient characteristics, not evaluated in the present analysis, may also impact on the cost-effectiveness of CR intervention models. Moreover, a combination of factors may be required to more precisely triage patients to the most cost-effective CR program model.
Limitations of this study include the 22% loss to follow-up over the 2 years resulted in missing data. The relative underrepresentation of women in the present trial is further amplified by the dropout rate among female participants, a trend which has been previously reported in the literature [23]. Furthermore, the DCR program model itself was selected as the comparator to the SCR program based on theoretical underpinnings, and it is possible that a different schedule or program duration may have yielded a different result.
We conclude that the main observation of this cost-effectiveness analysis was the dominance of SCR, the standard 12-week approach to CR program delivery, over DCR, program delivery distributed over 12 months. At the same time, subgroup analyses identified differences in the cost-effectiveness of the two modes of CR program delivery across cardiac risk strata, sex, and reason for referral. This suggests that it may be beneficial to consider triaging patients to different CR intervention models based on these factors. Future research is, however, required to validate both of these observations.
Footnotes
Acknowledgements
This research was supported by the Heart and Stroke Foundation of Ontario, Canada (Grant no. T-4600). Statement on potential conflicts of interests: none.