
Abstract
Background
Design
Methods
Results
Conclusion
Introduction
Chronic kidney disease (CKD) is a well-known risk factor for coronary atherosclerosis and is associated with a high incidence of cardiovascular death [1–3]. Typically, renal function is assessed through serum creatinine (SCr) which, nevertheless, is limited by dependency on age, sex and body mass. Creatinine clearance quantifies CKD more accurately, but requires a carefully collected urine sample over 24 h, thus conditioning its use in routine clinical practice. For this reason, various formulas have been developed to estimate glomerular filtration rate (GFR). The Modification of Diet in Renal Disease (MDRD) formula [4], for example, has been identified recently in an American Heart Association Advisory [5] as a means to screen for CKD in patients with cardiovascular disease. The same committee, however, acknowledged that the role of the MDRD formula has not been verified in this particular setting. The aim of our study, therefore, was to examine the impact on prognosis of CKD defined by the simplified MDRD formula in comparison with GFR calculated with the Cockcroft-Gault (CG) formula [6] in a large population of patients with ischaemic heart disease (IHD) and long-term follow-up.
Methods
Patient population
The population under study consisted of 1705 consecutive Italian, Caucasian patients who had been admitted to our Institute for IHD from 1983 to 1993. During initial hospitalization, all patients underwent coronary angiography. Each examination was reviewed by an expert interventional cardiologist and significant coronary atherosclerosis (SCA) was defined, by visual assessment, as a greater than 50% stenosis in at least one major vessel, including the left main coronary artery. After discharge, patients were asked to participate in a follow-up programme and received annually, for at least 10 years, a brief questionnaire on symptoms, cardiovascular events and intervening hospitalizations. Date and cause of death were obtained through certificates provided by local health authorities.
Renal function
SCr was measured prior to coronary angiography with the Jaffé method and is expressed in milligrams per decilitre. GFR was calculated according to the simplified MDRD formula as 186 × SCr−1.154 × age−0.203. Further multiplication by 0.742 was necessary in female patients. GFR was also estimated using the CG formula (140-age) × weight in kg/(72 × SCr). In women, the value was multiplied by 0.85. As CG GFR is expressed in millilitres per minute, and not in ml/min/1.73 m2 contrary to the MDRD formula, a corrective factor of (1.73/body surface area in m2) was employed with body surface area calculated according to the DuBois formula (0.007184 × weight in kg0.425 × height in cm0.725). The limit between normal and pathological SCr corresponded to the 75th percentile of SCr distribution (1.10 mg/dl), whereas GFR was considered abnormal if less than 60 ml/min/1.73 m2, in accordance with the aforementioned American Heart Association Scientific Advisory [5].
Statistical analysis
Continuous and categorical variables are expressed as means ± standard deviation and percentages, respectively. The 75th percentile of the age distribution (62 years) was used as a cut-off value to define advanced age, and patients were considered overweight if body mass index was greater than 25 kg/m2. Comparisons between groups were made with Student's t-test for independent samples and the χ2 test to identify clinical variables associated with renal dysfunction. Kaplan-Meier survival curves were constructed to examine the effect of abnormal SCr and reduced GFR on mortality. Subsequently, multivariate Cox regression analysis, using three different models so as to assess each renal parameter (SCr, MDRD GFR, CG GFR) separately, was performed adjusting for the following variables: age, sex, traditional coronary risk factors (family history of IHD, past or current smoker, arterial hypertension, hypercholesterolaemia, diabetes mellitus, overweight), SCA, history of myocardial infarction, atrial fibrillation, left bundle branch block, left ventricular hypertrophy, peripheral arterial disease, history of cerebrovascular events, proteinuria, history of myocardial revascularization and year of enrolment. Statistical analyses were performed using SPSS v12 (SPSS, Chicago, Illinois, USA) and a P value < 0.05 was considered significant.
Results
Baseline characteristics
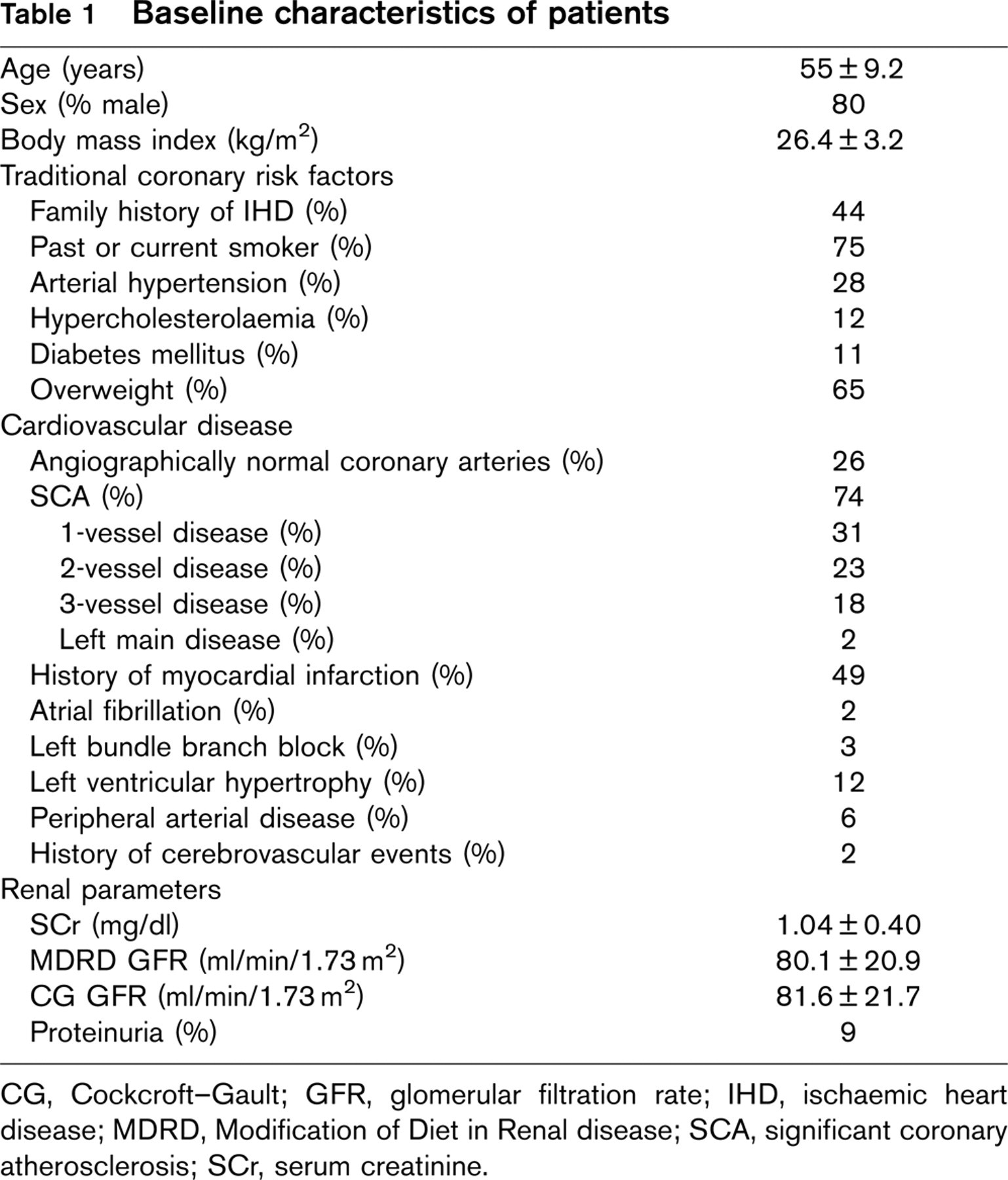
Characteristics of the population on enrolment are shown in Table 1. The mean age was 55 ± 9.2 years and 80% of the patients were male. Ten-year risk for fatal cardiovascular disease was estimated according to the SCORE system [7] and varied from 1% (in female nonsmokers) to 3% (in male smokers). One in four patients presented normal coronary arteries at angiography and roughly half the population had a history of myocardial infarction. Among patients with at least one critical (i.e. greater than 70%) stenosis, angina, either exertional or at rest, was frequent (79%). In this subgroup, myocardial ischaemia at stress testing was also a common finding (74%), although 16% were symptomatic in the absence of any objective evidence of ischaemia.
When comparing patients with, versus those without, reduced GFR, the following variables were linked to renal dysfunction: advanced age, arterial hypertension, diabetes mellitus, presence and extent of SCA, history of myocardial infarction, atrial fibrillation, left bundle branch block, left ventricular hypertrophy, peripheral arterial disease and history of cerebrovascular events (P < 0.05 for each). Angina and silent myocardial ischaemia, on the other hand, were not associated with renal dysfunction.
Baseline characteristics of patients
CG, Cockcroft-Gault; GFR, glomerular filtration rate; IHD, ischaemic heart disease; MDRD, Modification of Diet in Renal disease; SCA, significant coronary atherosclerosis; SCr, serum creatinine.
Follow-up data
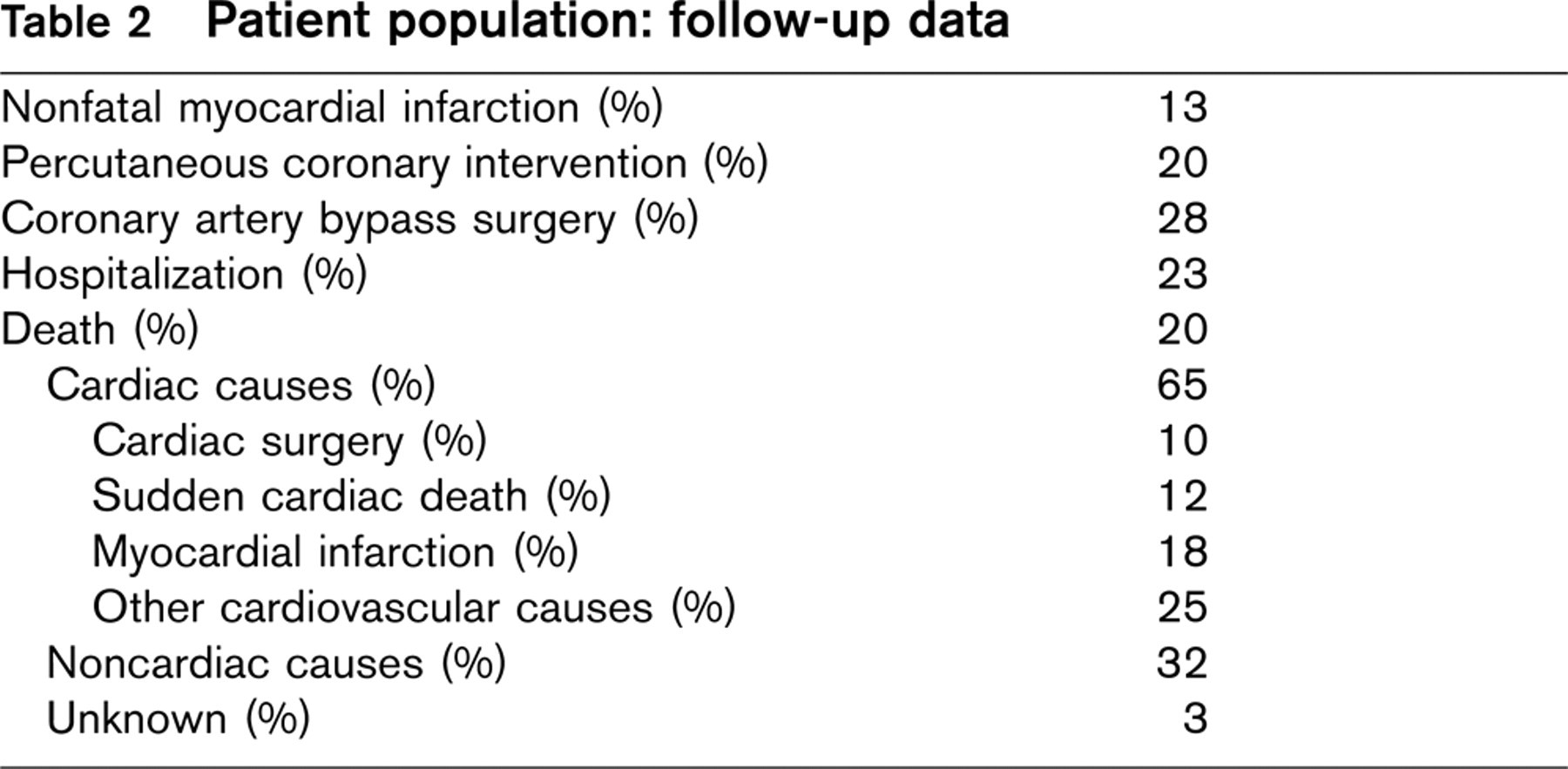
No patients were lost to follow-up, and 10-year mortality was 20% (Table 2), two-thirds of which was attributable to cardiovascular disease. Renal function was more compromised among patients who had died compared with those alive at the end of the follow-up period (SCr 1.14 ± 0.65 vs. 1.01 ± 0.29 mg/dl; MDRD GFR 75.8 ± 25.7 vs. 81.2 ± 19.4 ml/min/1.73 m2; CG GFR 74.3 ± 23.4 vs. 83.4 ± 20.8 ml/min/1.73 m2; P < 0.001 for each). After discharge, 13% of patients experienced nonfatal myocardial infarction, 43% underwent myocardial revascularization and 23% were hospitalized.
Kaplan-Meier survival curves, stratified by renal function, are shown in Fig. 1. CG and MDRD GFR less than 60 ml/min/m2, as well as abnormal SCr, were associated with an increase in 10-year mortality. After excluding patients with normal SCr, only reduced CG GFR, but not MDRD GFR, continued to be a significant predictor of survival (log-rank 9.35, P = 0.037).
Cox regression (Table 3) revealed that SCA was the strongest predictor of increased mortality, followed by reduced CG GFR, left bundle branch block and diabetes mellitus. An additional analysis was performed including only cases of cardiac death, but results did not change significantly and the rank order was maintained with SCA [hazard ratio (HR) 5.91, 95% (confidence interval) CI 3.37-10.35], reduced CG GFR (HR 2.85, 95% CI 2.12-3.84), left bundle branch block (HR 2.49, 95% CI 1.37-4.50) and diabetes mellitus (HR 2.28, 95% CI 1.65-3.14). When the cohort was subsequently divided into four subgroups of CG GFR (Fig. 2) an increase in the risk of all-cause death, adjusted for the same variables used in the Cox regression, was observed along with declining renal function.
Discussion
The study demonstrates that estimated GFR is an important predictor in IHD. It is superior to both traditional coronary risk factors, including diabetes mellitus and markers of cardiovascular disease, such as left ventricular hypertrophy, atrial fibrillation and proteinuria. Only SCA was a stronger predictor of mortality in the patient cohort. Although the relationship existing between renal dysfunction and cardiovascular disease had already been examined previously, our findings remain significant in light of the size of the population under study amounting to almost 2000 patients with a follow-up of 10 years.
Patient population: follow-up data
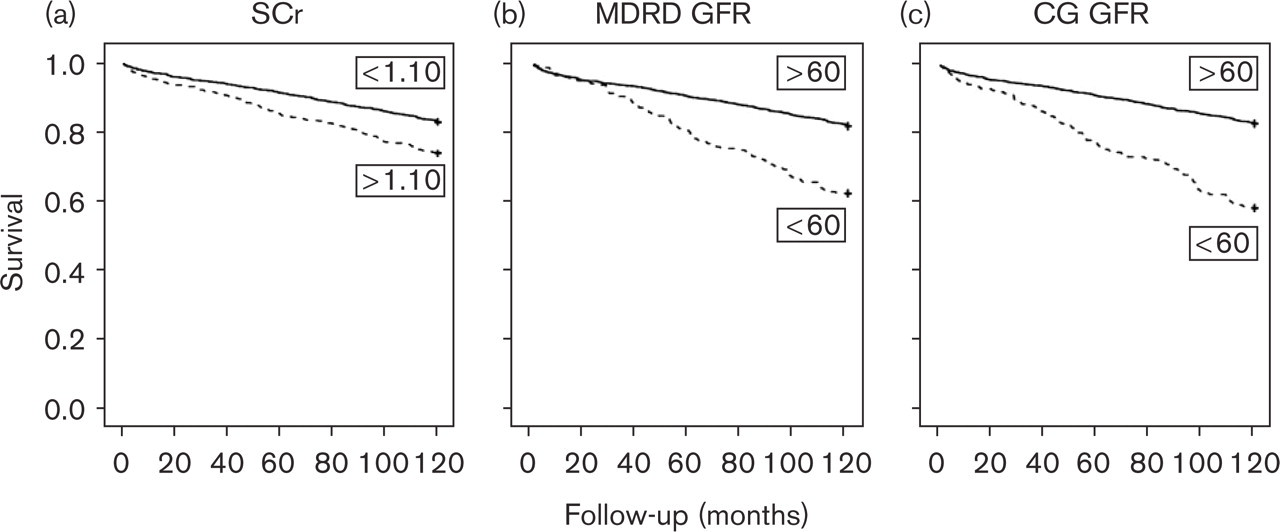
Kaplan-Meier survival curves stratified by (a) SCr in milligrams per decilitre (log-rank 21.0, P < 0.0001), (b) MDRD GFR in ml/min/1.73 m2 (log-rank 46.7, P < 0.0001), and (c) CG GFR in ml/min/1.73 m2 (log-rank 80.3, P < 0.0001). CG, Cockcroft-Gault; GFR, glomerular filtration rate; MDRD, Modification of Diet in Renal Disease; SCr, serum creatinine.
The observation of a better performance of the CG formula, corrected for body surface area, over the simplified MDRD formula is of interest. Although the reliability of this finding should not be overemphasized given the retrospective nature of the study, one may hypothesize that the simplified MDRD formula, taking into account only age, sex, and race, lacks accuracy in patients with IHD. The extended version of the MDRD formula, on the other hand, is difficult to apply to routine clinical practice owing to its dependency on serum albumin and blood urea nitrogen. The CG formula corrected for body surface area, therefore, presents itself as an attractive choice for estimating GFR in IHD.
Predictors of 10-year mortality at multivariate analysis
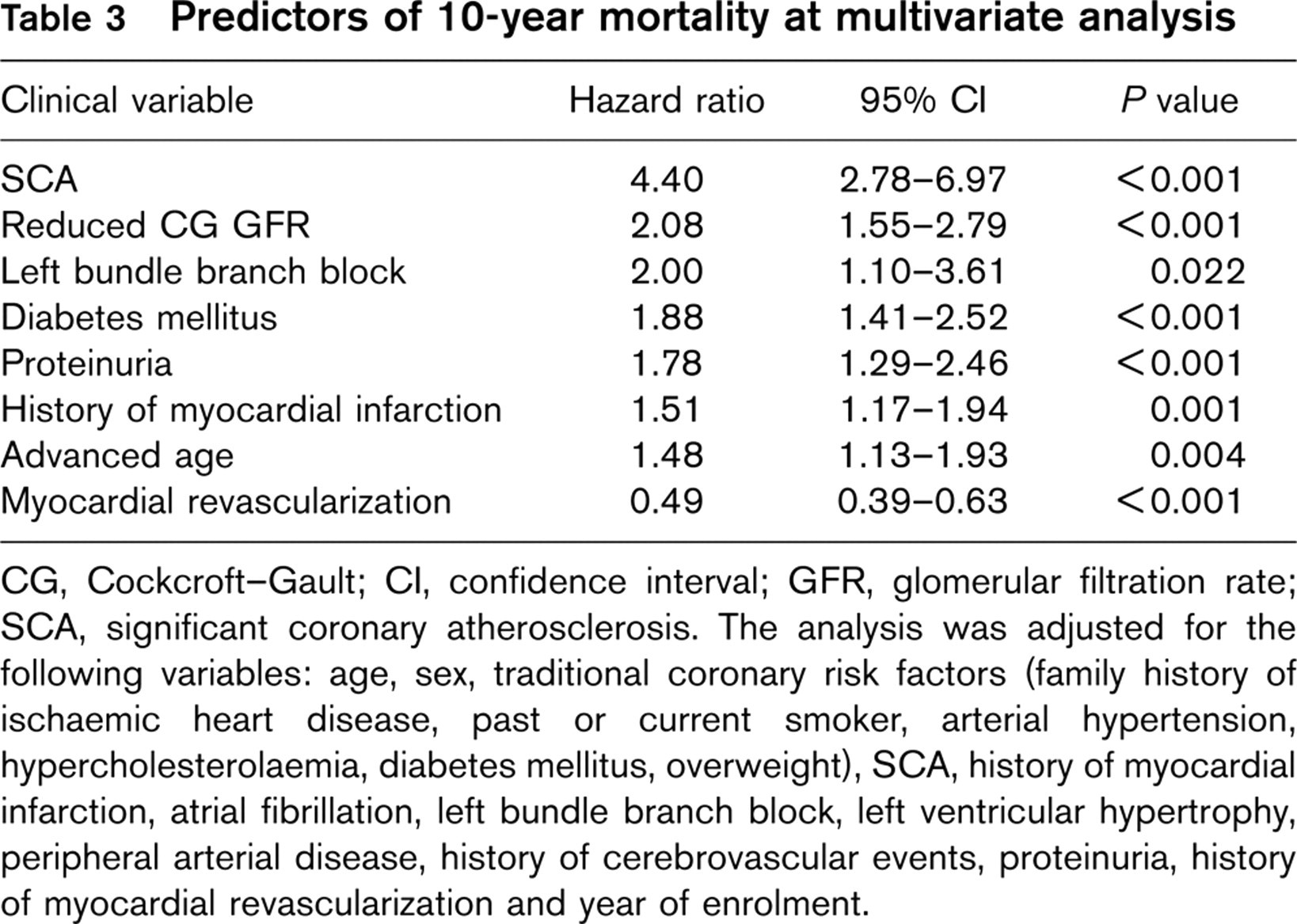
CG, Cockcroft-Gault; CI, confidence interval; GFR, glomerular filtration rate; SCA, significant coronary atherosclerosis. The analysis was adjusted for the following variables: age, sex, traditional coronary risk factors (family history of ischaemic heart disease, past or current smoker, arterial hypertension, hypercholesterolemia, diabetes mellitus, overweight), SCA, history of myocardial infarction, atrial fibrillation, left bundle branch block, left ventricular hypertrophy, peripheral arterial disease, history of cerebrovascular events, proteinuria, history of myocardial revascularization and year of enrolment.
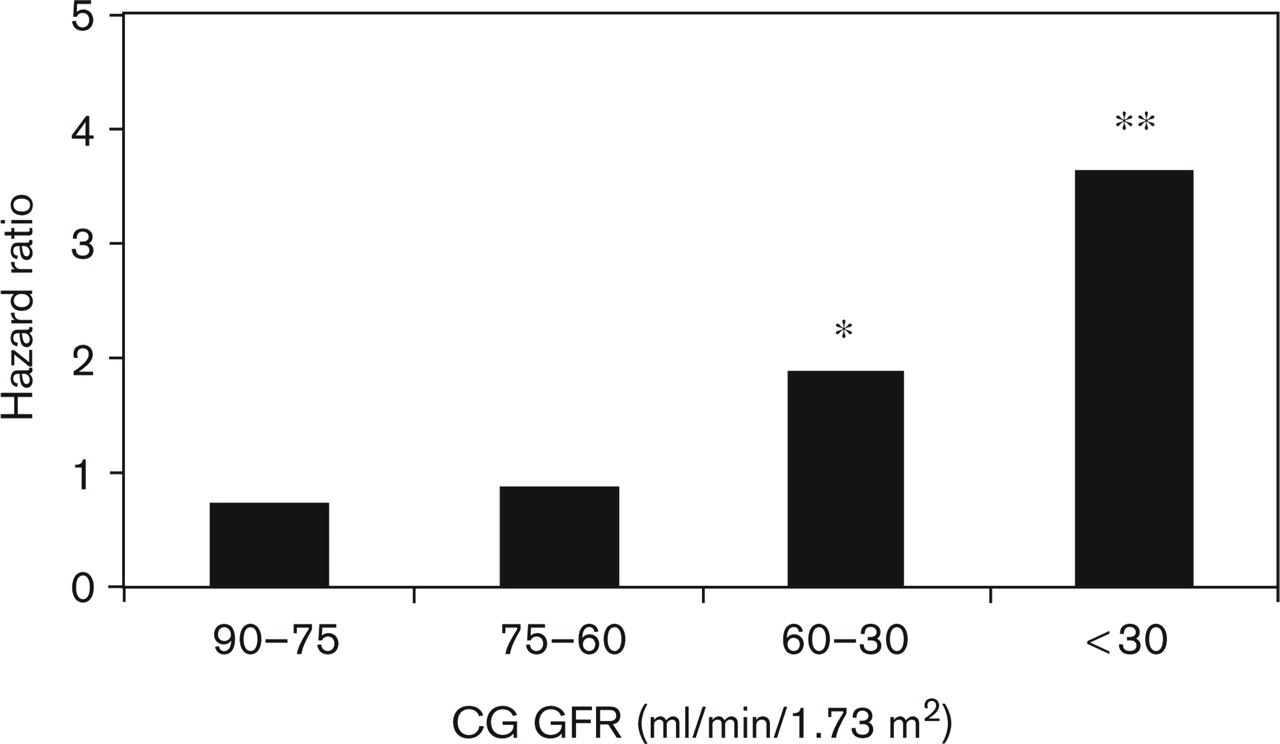
Hazard ratio for 10-year mortality, after multivariate adjustment, according to different levels of CG GFR. Statistical significance was observed in two subgroups, that is, GFR between 60 and 30 ml/min/1.73m2 (∗P<0.001) and GFR less than 30 ml/min/1.73 m2 (∗∗P = 0.003). The analysis was adjusted for the following variables: age, sex, traditional coronary risk factors (family history of ischaemic heart disease, past or current smoker, arterial hypertension, hypercholesterolemia, diabetes mellitus, overweight), significant coronary atherosclerosis, history of myocardial infarction, atrial fibrillation, left bundle branch block, left ventricular hypertrophy, peripheral arterial disease, history of cerebrovascular events, proteinuria, history of myocardial revascularization and year of enrolment. CG, Cockcroft-Gault; GFR, glomerular filtration rate.
An alternative, and more thought-provoking, hypothesis is that the value of GFR estimating formulas varies according to clinical context, which is not implausible considering that these formulas have been validated primarily in young populations or with chronic renal disease. Maaravi et al. [8], for example, observed that among 70-year-old patients in a community-based setting reduced CG GFR, but not MDRD GFR, was associated with 12-year mortality at multivariate analysis. A different finding was reported by Smilde et al. [9] in a population with chronic heart failure of ischaemic and nonischaemic origin. In fact, after 12 months of follow-up, both the simplified and extended versions of the MDRD formula, compared with the CG formula corrected for body surface area, predicted more accurately a combined endpoint of death, heart transplantation or hospitalization for heart failure. The superiority of MDRD GFR over CG GFR was also described by Ruilope et al. [10] in a study conducted in high-risk hypertensive patients in which several endpoints — myocardial infarction, stroke, heart failure — were taken into consideration.
Clinical implications
The American Heart Association has recently recommended the use of the MDRD formula to screen for CKD in patients with cardiovascular disease [5]. In the same document, however, it is recognized that the accuracy of the MDRD formula in IHD has not been assessed. For this reason, and in light of our findings, we believe that further research is required to determine which GFR estimating formula — CG corrected for body surface area, simplified MDRD, or extended MDRD — should be used in patients with IHD.
The study demonstrates that estimated GFR has a stronger predictive value than SCr. Nevertheless, GFR is not calculated routinely in the risk stratification of IHD. For example, not only the EuroSCORE system [11], being routinely employed before cardiac surgery, but also the clinical guidelines for the preoperative evaluation of patients with cardiovascular disease undergoing noncardiac surgery [12] limit their analysis of renal function to SCr. Furthermore, the SCORE system [7], which predicts 10-year incidence of cardiovascular death in healthy individuals, takes into account age, sex, smoking habit, serum cholesterol levels and arterial blood pressure, but not renal function. Even risk stratification in acute coronary syndromes [13] does not consider GFR, despite the numerous studies [14, 15] pointing to increased mortality among patients with CKD.
Limitations
Besides the limitations inherent in an observational and retrospective study, other drawbacks need be recognized. The entire cohort consisted of a distinct Caucasian group which had been hospitalized for IHD. Some caution should, therefore, be used in extending results to other populations as well as to the community setting where risk factors may not be managed as effectively. In addition, many patients were enroled in the 1980s and information regarding medical therapy was not available. In contrast, all patients were discharged from the same Institute and significant differences in therapy are unlikely. The cohort did not have a measure of left ventricular systolic function, such as echocardiographically derived ejection fraction. Each patient discharged from our Institution is, however, characterized according to a multiparameter system, one of which defines the presence of cardiac dysfunction on the basis of the results of instrumental examinations. Thirteen percent of the population had cardiac dysfunction and when this term was inserted into the Cox regression model, it did not emerge as a significant predictor of survival. It should also be kept in mind that the 10-year mortality was low and, therefore, a high prevalence of systolic dysfunction may be reasonably excluded. Renal function was not assessed with a ‘gold standard’ reference technique, such as the clearance of iothalamate, as such a test is time consuming and expensive. Moreover, the objective of this study was to examine the prognostic impact and not the diagnostic accuracy of estimated GFR. Finally, SCr was measured only once during initial hospitalization and we were not able to account for possible variations in renal function over time.
Conclusion
Reduced GFR is an important prognostic determinant in hospitalized patients with IHD. The predictive value of GFR, in particular when calculated with the CG formula corrected for body surface area, is superior to other measures of renal function, traditional coronary risk factors and markers of cardiovascular disease. Calculation of GFR should be included in the management of IHD to identify those patients at higher risk. In this way, therapeutic strategies would more accurately be tailored to the individual with the attendant expectation of improved survival.
Footnotes
Acknowledgements
The authors would like to thank Patrizia Landi and Claudio Michelassi for their assistance with data collection and subsequent analysis.
Conflicts of interest: none.