
Abstract
Background
We aimed to quantify the potential health benefits of increased use of lipid-lowering treatment (LLT), according to current guidelines, for the Dutch diabetes population.
Design
Simulation study.
Methods
We compared the long-term health outcomes for a scenario in which all diabetes patients received LLT to those in a ‘current practice’ scenario, in which 28% received LLT. The model reflected the Dutch diabetes population 40–80 years of age, in 2003. Sensitivity analyses were performed, using more conservative assumptions.
Results
Over the lifetime, LLT for all diabetes patients reduced the expected cumulative incidences of coronary heart disease (CHD) and stroke by, respectively, 6 and 9%. Average life expectancy of Dutch diabetes patients would increase by 0.33 years, ranging from 0.14 years for patients aged 70–79 years, to 0.84 years for patients aged 40–49 years at the start of the simulation. Life-long treatment for patients aged 50–59 contributed most to the life years gained (55 000 out of 146 000). With reduced effectiveness of LLT and fewer patients starting LLT, the cumulative incidences of both CHD and stroke would decrease by approximately 2%. The number needed to treat to prevent one incident case of cardiovascular disease over lifetime was 20 for CHD and 44 for stroke.
Conclusion
This simulation study shows that increased use of LLT can substantially reduce the expected future burden of CHD and stroke in the Dutch diabetes population.
Keywords
Introduction
What would the health impact be for a population if lipid-lowering treatment (LLT) was actually prescribed to all diabetes patients? This is an interesting question as most of the recent guidelines recommend LLT for virtually all persons with diabetes [1,2], whereas prescription rates in daily practice are still far below that target.
There is a wealth of evidence that persons with diabetes are at increased risk for cardiovascular disease (CVD), whereas excess mortality in diabetes patients is mainly due to CVD [3,4]. Consequently, cardiovascular prevention should be undertaken more rigorously in diabetes patients than in the general population. Several studies have shown that LLT can substantially reduce the occurrence of major cardiovascular events in persons with diabetes [5–9]. The proportional reductions in CVD incidence due to LLT are almost similar for persons with and without diabetes, with or without coronary disease, and independent of the baseline level of cholesterol [5,6,9]. Furthermore, in persons with diabetes, relative treatment benefits seem to be independent of diabetes duration and glycaemic control [9].
However, the long-term health benefits that could be gained on a population level when all diabetes patients would be treated according to recent guidelines, are unknown. So far, all reports of observed health outcomes are from clinical trials, conducted in selected populations with a follow-up duration of at most 5 years [5]. Earlier modeling studies were confined to newly diagnosed patients and patients with dyslipidemia [10,11].
In this study we assess the potential long-term health benefits of lipid-lowering treatment, for the Dutch diabetes population.
Methods
The chronic diseases model
The chronic diseases model (CDM) is a Markov type state transition model [12,13]. In this study, the CDM simulation starts with a cohort resembling the Dutch diabetes population. The states specified in the CDM are risk factor classes, presence or absence of chronic diseases and vital status. The current state determines the probability to change to another state in the next 1-year time step. The risk factors included in the simulations in this study are total cholesterol (TC), body mass index, systolic blood pressure, and glycaemic control (HbA1c). The cardiovascular complications of diabetes modeled are coronary heart disease (CHD) and stroke.
With every time step, patients have a risk to change risk factor class, disease state or to die. The probability to develop CHD or stroke depends on age, sex, and risk factor class. For example, the risk for stroke is higher for higher levels of systolic blood pressure. Subsequently, the probability to die is higher for patients with CHD or stroke than for patients without cardiovascular complications. In addition, stroke increases the risk for CHD independently from all risk factors.
We used a closed cohort approach, meaning that persons leave the cohort due to mortality, but there are no new persons entering the cohort. With every time step the simulated cohort becomes smaller, until finally all persons have died.
The CDM has been used previously to evaluate cost effectiveness of diabetes prevention and smoking cessation [12,14], to explore the impact of lifestyle risk factors on healthy life expectancy [15] and lifetime healthcare costs [16], and to estimate the future burden of stroke and obstructive pulmonary disease [17,18].
Input data
Age-specific prevalence rates for diabetes derive from Dutch general practitioners’ registrations [13]. The risks for CHD and stroke in the diabetes group are calculated from two different input parameters: (i) age-specific CHD and stroke incidence rates in the general population (from general practitioners registrations) and (ii) relative risks for CHD and stroke for persons with diabetes compared with persons without diabetes. A similar approach is used to calculate age-specific mortality rates for persons with diabetes. Distributions of cholesterol levels derive from Dutch health monitoring studies conducted between 1998 and 2001 [19–21]. The strengths of the associations (relative risks) between risk factors and diseases (CHD and stroke) are based on international observational studies, and we assume that these associations are similar in persons with and without diabetes. All data in the CDM are age and sex specific.
Treatment effect
In the CDM, TC is modeled in four classes, with cutoff points at 5.0, 6.5, and 8.0 mmol/l. In the model, these classes are linked to CHD through relative risks of disease incidence [13]. The level of TC has no effect on the incidence of stroke [22]. To simulate the effect of LLT, each cholesterol class is stratified by treatment status (treated or untreated). Estimates for cardiovascular risk reductions for treated patients as compared with untreated patients derived from a meta-analysis of statin treatment [6]. We used the following estimates, independent from the pretreatment level of TC: a 26% risk reduction for CHD incidence in persons younger than 65 years, and a 19% risk reduction for persons above 65 years. For stroke, a 17% risk reduction for all ages. These estimates correspond to treatment effects obtained with an average LDL reduction of 1.0 mmol/l [6].
Current practice scenario
At the start of the simulation (2003), the cohort comprised 445 200 diabetes patients aged 40–80 years, with a mean age of 65 years. The prevalence of known CHD was 24% and that of stroke 5%. In this cohort, 86% had TC levels > 5.0 mmol/l and 28% (123600 patients) were treated with lipid-lowering medication. We assumed that treated patients continued treatment for the rest of their lives. Similarly, we assumed that untreated patients remained untreated, whereas TC levels stayed stable (no transitions between cholesterol classes).
Guideline scenario
In this scenario we assumed treatment for all patients, whereas keeping all other risk factors unchanged. This means that we assumed lifetime treatment for an additional 321 600 patients.
Sensitivity analysis
The effect of LLT may be lower in daily practice than in well-controlled trials. Furthermore, some patients may refuse treatment or discontinue within a few years. Therefore, we defined and run the following alternative scenarios (AS):
AS 1. The relative risk reductions for CHD and stroke, due to LLT, were set equal to the lower boundaries of the confidence intervals as reported by Baigent et al. [6]: 21% for persons under 65 years and 12% for persons above 65 years for CHD; 12% for stroke.
AS 2. Reduced effect (AS 1) + the assumption that additional treatment is confined to 50% of currently untreated patients.
AS 3. Reduced effect (AS 1) + additional treatment is confined to 50% of currently untreated patients with TC > 5.0 mmol/l
AS 4. Reduced effect (AS 1) + additional treatment is confined to 50% of currently untreated patients with TC > 5.0 mmol/l and age ≤ 70 years.
Results
Coronary heart disease and stroke incidence
Cumulative CHD and stroke incidence were consistently lower in the guideline scenario than in the current practice scenario, although the proportional reductions declined with increased treatment duration (Table 1). With lifelong treatment, cumulative numbers of incident cases of CHD and stroke were 16 100 (5.6%) and 7300 (8.8%), respectively, lower in the guideline scenario. Lifelong treatment started at age 50–59 years contributed most to the reduction in CHD (5247 cases, Table 2) and treatment started at age 60–69 years contributed most to the reduction in strokes (2304 cases).
Life years and life expectancy
The guideline scenario resulted in 146200 life years gained, meaning that average life expectancy (LE) increased by 0.33 years (146 200/445 200) in the total diabetes cohort and by 0.45 years (146 200/321 600) in additionally treated patients (Table 1). The largest contribution to the life years gained derived from lifelong treatment for all patients aged 50–59 years at the start of the simulation. Increase in average LE ranged from 0.14 years in patients aged 70–79 years to 0.84 years in patients aged 40–49 years (Table 2).
Numbers needed to treat
The numbers needed to treat (NNT) to prevent one incident case of CHD or stroke declined with increased treatment duration (Table 1). The NNT for CHD declined from 36 to prevent one event in 5 years to 20 to prevent one event over the lifetime. The corresponding NNT for stroke were 99 and 44, respectively.
Expected health outcomes for the ‘current practice’ and ‘guideline’ scenario, for the total diabetes cohort
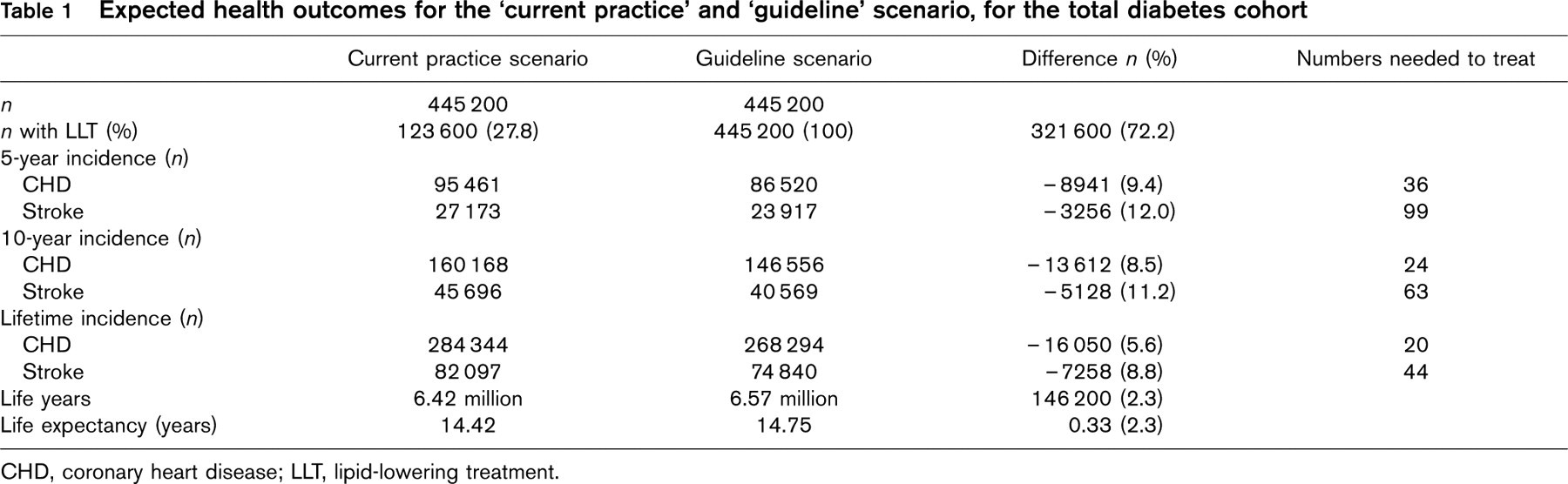
CHD, coronary heart disease; LLT, lipid-lowering treatment.
Expected health outcomes for the ‘current practice’ and ‘guideline’ scenario, specified by age
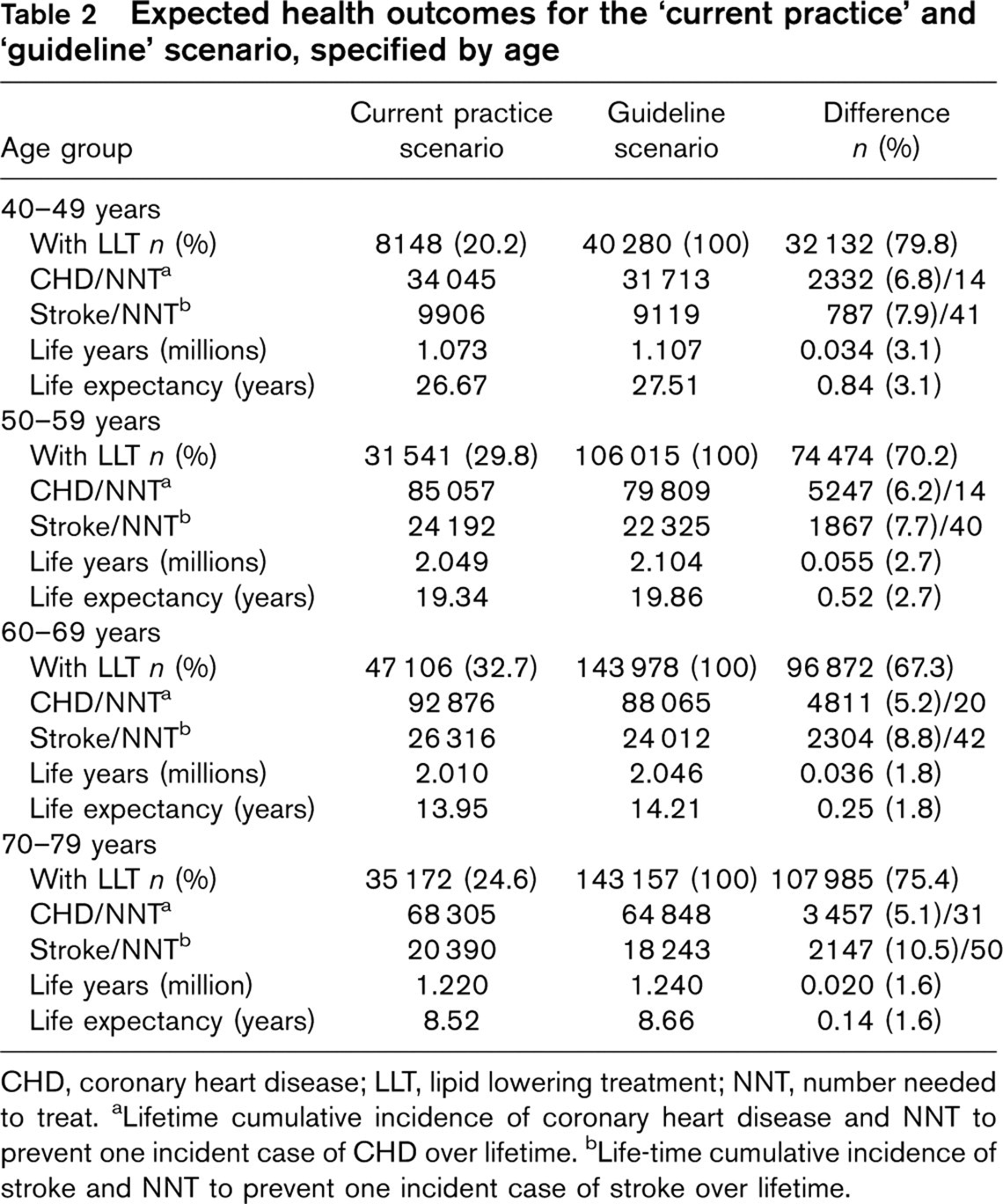
CHD, coronary heart disease; LLT, lipid lowering treatment; NNT, number needed to treat. aLifetime cumulative incidence of coronary heart disease and NNT to prevent one incident case of CHD over lifetime. bLife-time cumulative incidence of stroke and NNT to prevent one incident case of stroke over lifetime.
Results for the sensitivity analysis: proportional reductions in lifetime cumulative Incidence of coronary heart disease and stroke and total life years gained
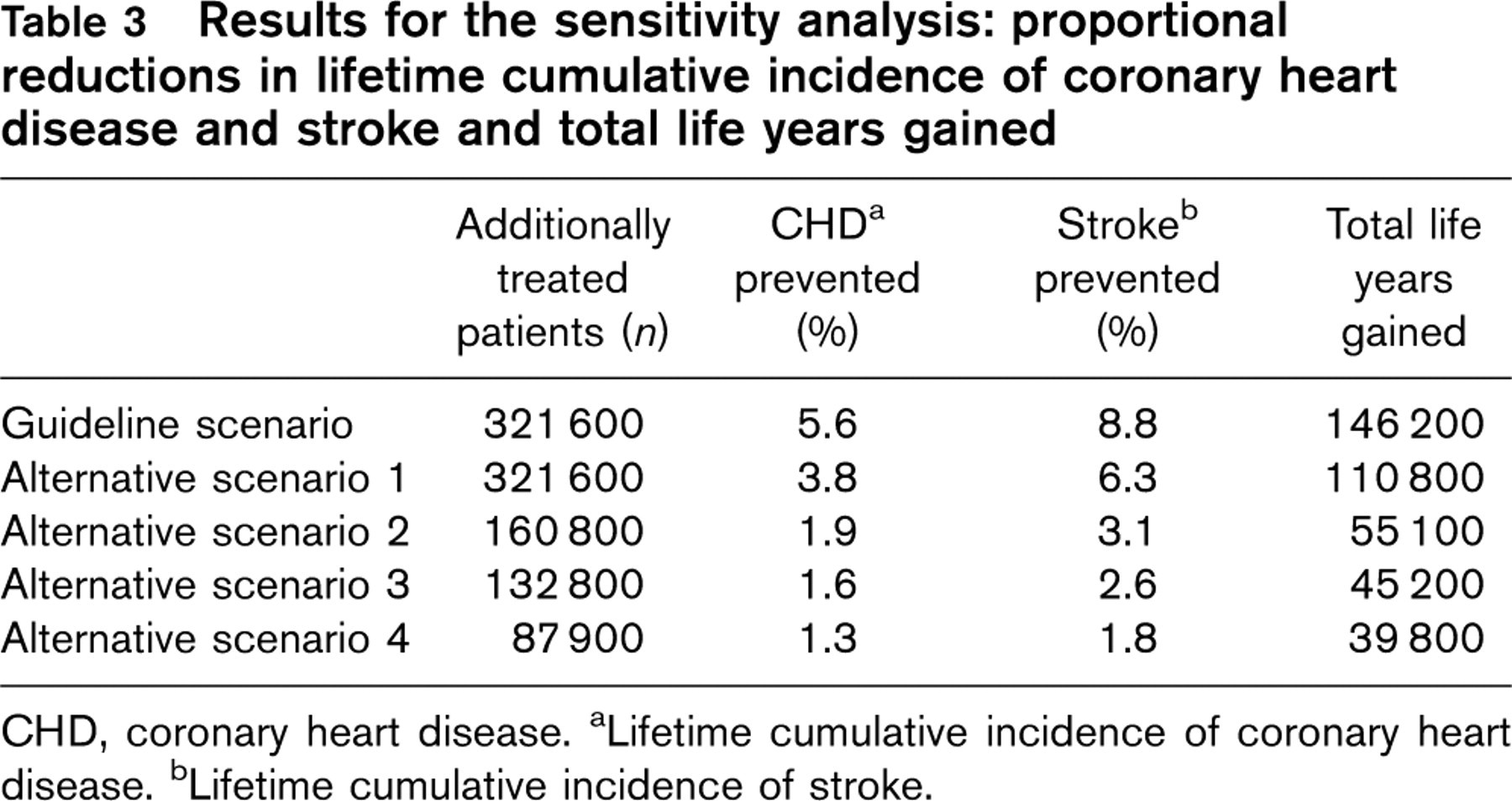
CHD, coronary heart disease. aLifetime cumulative incidence of coronary heart disease. bLifetime cumulative incidence of stroke.
Sensitivity analysis
With more conservative estimates for treatment effect and additional treatment confined to 50% of untreated patients with TC > 5.0 mmol/l (AS 3), the proportional reductions in CHD and stroke incidence declined to 1.6 and 2.6%, respectively. Life years gained declined from 146 200 to 45 200 (Table 3).
Discussion
Our simulation study showed that 6, respectively, 9% of the expected cumulative CHD and stroke incidence in the Dutch diabetes population could be prevented if all patients (instead of 28% in current practice) would use lifelong lipid-lowering medication. Average LE of the diabetes population would increase by 0.33 years. The NNT to prevent CVD over lifetime was 20 for CHD and 44 for stroke.
Our study is not the first to model diabetes treatment. Palmer et al. [23] evaluated the impact of theoretical 10% improvements in several cardiovascular risk factors. Life expectancy values for a typical US diabetes cohort increased by 1.0 due to improved glycaemic control (HbA1c), 0.7 due to improved blood pressure control and 0.3 with improvements in cholesterol, from which the authors concluded that reducing HbAlc has the greatest impact on long-term health. However, although a 10% reduction in HbA1c seems feasible [24], mean improvements in blood pressure are generally smaller [24,25]. In contrast, average reductions in cholesterol due to lipid-lowering treatment are generally much larger, in the range 15–20% [5]. Consequently, Palmer et al. underestimated the potential impact of LLT by assuming equal reductions in all cardiovascular risk factors.
Other simulation studies that examined the long-term health impact of LLT in diabetes patients reported increases in life expectancy ranging from 0.2 years for patients with CHD to 5.4 years in young patients with dyslipidemia [10], showing the large variation in outcome depending on population characteristics and methods used [11]. In addition, the CDC study [10] showed that lifelong treatment reduced lifetime cumulative incidence for CHD but not for stroke, probably because the CDC model did not include an effect of statin treatment on stroke. However, despite the absence of an independent positive association of cholesterol with stroke mortality as found in observational studies, there is conclusive evidence from randomized trials that statins substantially reduce stroke rates [22].
We found that in our diabetes cohort, in which the majority had no vascular disease, the NNT to prevent one case of CHD over a 5-year period was 36. This is consistent with previous findings. Costa et al. [5] showed that the NNT to prevent a coronary event was 37 in persons (with or without diabetes) without CVD, for an average follow-up of 5 years. A recent meta-analysis [26] confined to persons with diabetes reported 36 fewer people with major vascular events after 5 years, per 1000 patients without vascular disease at baseline, corresponding with a NNTof 28. This is very close to the NNTof 26 to prevent one cardiovascular event over 5 years in our study, which can be calculated by adding the coronary and stroke events prevented as displayed in Table 1.
Several limitations are found with respect to the input data and assumptions used in our model. First, the input parameters in our model derived from well-designed and controlled intervention studies, whereas, for example, treatment dose and adherence are probably lower in day-to-day realistic conditions. Although a Dutch study [27] showed that less than half of the patients were still taking their medication 2 years after initiating statin treatment, compliance might be better in persons with diabetes [28]. Our sensitivity analysis showed the impact of assuming lower treatment effect and compliance. Second, our estimates for treatment effect were based on a metaanalysis of trials including both persons with and without diabetes. Results of a recently published meta-analysis [26] confirmed that our model estimates are valid for persons with diabetes, because the impact of statin treatment on the incidence of major coronary events and strokes appeared similar for persons with and without diabetes. Finally, we assumed that untreated patients remained untreated, although treatment rates seem to increases with advancing age (Table 2). If increased use of LLT in current practice would have been taken into account, the calculated health gains in our study would have been lower. In contrast, we assumed that cholesterol levels did not increase with advancing age. If deterioration of cholesterol levels in untreated patients in the current practice scenario would have been included, the calculated health gains would have been larger.
Although our study provides meaningful insight into the possible long-term effects of LLT, our study did not address potential drug-induced adverse events [6,29], or the impact of drug use on quality of life [30]. In contrast, our model ignores potential beneficial effects of statin treatment on microvascular complications [29].
In conclusion, better adherence to current guidelines for LLT would substantially reduce the occurrence of cardiovascular complications in the Dutch diabetes population. With respect to future improvements, more efforts should be devoted to maximizing the potential for decreasing cardiovascular risk in diabetes patients. Strategies should be developed to increase adherence to guidelines by healthcare providers, and to increase patient compliance to pharmacological treatment as well as lifestyle recommendations.
Footnotes
Acknowledgements
This project was funded by the Dutch Ministry of Health, Welfare and Sports. The authors thank Hendriek Boshuizen and Talitha Feenstra for their valuable contribution to this manuscript.
Conflicts of interest: none.