
Abstract
Background
Low vitality, characterized by fatigue and lack of energy, is common among survivors of acute myocardial infarction (AMI) and has been shown to be associated with increased risk of primary and secondary cardiac events. The goal of this study was to determine whether an association between vitality and recurrent cardiac events (nonfatal MI, cardiac death) among acute MI survivors persists after controlling for possible physiological and psychological confounders.
Design and methods
Incident AMI survivors (n = 1328) from Erie and Niagara (New York) county hospitals were enrolled and followed up to 9 years. Vitality was measured by the Short Form-36 on a 0–100 scale approximately 4 months post-AMI. Cox proportional hazards models were developed to assess the vitality-recurrent event association controlling for traditional cardiovascular disease risk factors, index MI severity, and psychological correlates of vitality.
Results
Low-vitality individuals at baseline were more likely females, of higher BMI, smoking, diabetic, less physically active, and to have worse depression scores. Vitality was not strongly associated with MI severity markers. Lower vitality scores were associated with increased risk of recurrent cardiac events: adjusted hazard ratios (95% CI) for vitality scores 51–79, 21–50, and ≤ 20 (compared with ≥ 80) were 1.2 (0.8, 1.8), 1.4 (0.9, 2.2), and 2.9 (1.5, 5.4), respectively (P trend = 0.005).
Conclusion
Low vitality was associated with increased risk of recurrent cardiac events among AMI survivors after controlling for physiological and psychological confounders. Mechanistic links with vitality should be sought as interventional targets.
Introduction
Low vitality, often characterized subjectively by fatigue and lack of energy, is a common ailment among survivors of acute myocardial infarction (AMI), especially in women [1–3]. Furthermore, low vitality has been shown in several studies to be associated with increased risk of fatal and nonfatal cardiac events among individuals with and without known coronary artery disease [1, 4–11]. Identification of the underlying element of vitality imparting increased risk of cardiac events remains elusive, but has substantial implications for the appropriate targeting of potential risk-reducing interventions. In the realm of heart disease, vitality is characterized as having physiological and psychological attributes, both of which have known ramifications with respect to cardiac event risk. Physiologically, vitality has been hypothesized to be an indicator of reduced peripheral perfusion consequent to heart failure, left ventricular systolic dysfunction, myocardial ischemia, and/or damaged myocardium after AMI, though empirical findings have not revealed strong associations between vitality and these measures [3, 5, 8, 12–16]. Psychologically, vitality is strongly associated with symptoms of depression, hopelessness, and anxiety, common psychological disorders after AMI, with mixed findings on the association between vitality and cardiac outcomes when controlling for these conditions [17, 18].
Despite these presumed contrasting components to vitality, previous studies have not been able to simultaneously account for both domains adequately when assessing the association between vitality and subsequent cardiac outcomes, inhibiting the ability to completely control for possible mediating and/or confounding effects. Most of these studies have been conducted in either general populations or patients undergoing revascularization procedures, while to the authors’ knowledge only one study examining the association between vitality and future risk of cardiac events has been done in survivors of a first MI [1, 4–11, 13, 15]. This study was limited to a small cohort of women (n = 110) with few recurrent events [15]. Further research on the implications of low vitality on cardiac event risk is warranted, especially among AMI survivors given the high prevalence of the condition among this group. As such, the current report based on the Western New York AMI (WNYAMI) study describes the association between vitality and recurrent cardiac events in a population-based AMI cohort followed prospectively up to 8.8 years after a first MI. The WNYAMI study measured both physiological and psychological hypothesized correlates of vitality in addition to traditional risk factors to allow more thorough control of potential mediating and/or confounding effects. The main goal of this study was to determine whether an association between vitality and recurrent cardiac events persisted among survivors of a first AMI after accounting for an extensive collection of traditional cardiac risk, physiological, and psychological factors.
Methods
Incident cases of AMI were recruited from 12 of the 15 hospitals in Erie and Niagara Counties in Western New York between 1996 and 2004 as part of multiple epidemiologic studies conducted at the Center for Preventive Medicine at the University at Buffalo. Individuals discharged from any of these hospitals with an AMI diagnosis between ages 35–69 and without a history of prior AMI, coronary artery bypass graft, percutaneous transluminal coronary angioplasty (PTCA), symptomatic angina pectoris, or diagnosis of other cardiovascular diseases were contacted for possible study participation. Hospital medical records were abstracted to allow diagnostic confirmation of AMI according to World Health Organization criteria [19]. Clinical information related to the index MI (cardiac enzymes, ejection fraction) was collected when available. Informed consent for study participation was sought from all confirmed first AMI cases after permission to contact was granted by the patient's primary physician. Among eligible cases, 59% agreed to participate. All study protocols were approved by the Institutional Review Board at the University at Buffalo.
Approximately 4 months after the index MI, enrolled cases completed a series of questionnaires and underwent a comprehensive interview and physical examination as part of study protocols. Data collected included sociodemographic characteristics, anthropometrics, family and personal medical history, lifestyle and behavioral factors, measures of depression [Center for Epidemiologic Studies Depression Scale (CES-D)], and quality of life indices [Short Form-36 (SF-36)]. The SF-36 attempts to measure eight quality of life domains: physical functioning, role limitations because of physical problems, social functioning, bodily pain, general mental health, role limitations because of emotional problems, general health perceptions, and vitality, the focus of the current study [20].
After the study interview, nonfatal cardiac events were tracked prospectively through mailed surveys to study participants who identified the occurrence of all hospitalizations lasting 24 h or more, emergency room visits, and outpatient procedural visits. Participants not responding to mailed surveys were contacted by telephone and asked to return the survey by mail or complete the survey at the telephone contact. At least one survey was provided by 93.5% of enrolled study participants. All events reported by study participants were adjudicated through review of medical records by an experienced research nurse. Deaths and the underlying cause of death were determined through the query of the National Death Index with follow-up through 31 December 2004.
The primary independent variable is the vitality domain from the SF-36, composed of four, six-response questions inquiring whether patients, during the past 4 weeks, (i) ‘feel full of life’, (ii) ‘have a lot of energy’, (iii) ‘feel worn out’, and (iv) ‘feel tired’ [20]. Responses to these questions were transformed into a 0–100 vitality score with low values indicative of low vitality and high values indicative of high vitality. Very low and very high vitality groups were defined a priori as vitality scores less than or equal to 20, and vitality scores greater than or equal to 80, respectively. Four vitality score groups were used in the analysis: ≤ 20, 21–50, 51–79, and ≥ 80. Descriptive statistics for all the study variables are reported across vitality groups. Continuous variables are reported as medians and interquartile ranges; categorical variables are reported as percentages. Differences across vitality groups were assessed by Kruskal–Wallis and χ2 tests for continuous and categorical variables, respectively. Correlations between continuous variables were estimated by Spearman correlation coefficients.
The primary endpoint is time-to-first-event defined as the number of days from the baseline interview to either recurrent MI or death owing to a cardiac cause. Participants not identified as having an event were censored on 31 December 2004, the truncation date for which mortality information could be identified through the National Death Index. Cox proportional hazards models were developed to estimate the association between vitality and recurrent MI/cardiac death. Hazard ratios (HR) were estimated with vitality score ≥ 80 (highest vitality) serving as the reference group in unadjusted (model 1) and adjusted models, respectively. Adjusted models added to model 1, traditional cardiac risk factors (model 2), index MI severity measures (model 3), and psychological variables (model 4) iteratively to determine the respective effects of each set of variables on the vitality-outcome HRs. Traditional cardiac risk factors added in model 2 included age, sex, body mass index, diabetes, smoking status, history of hypercholesterolemia, history of hypertension, physical activity level measured as hours of moderate to intense physical activity in the 7 days before the interview, and medications at the baseline interview (aspirin, lipid-lowering, blood pressure-lowering). For model 3, relative peak creatine kinase (CK) (relative to upper limit of normal), an indicator of severity of the index MI, was added to model 2. Relative peak CK was modeled as tertile groups plus a fourth ‘unknown’ group to account for missing values (2% of cohort). Model 4 added the SF-36 general mental health domain and CES-D scores. Additional Cox models examined the short-term and long-term associations between vitality and outcome by stratifying on follow-up time (≤ 2, > 2 years). Tests for trend were facilitated by including an ordinal integer variable for the four vitality groups (1, 2, 3, 4) as a continuous variable in the respective models.
Among 1496 AMI cases initially enrolled in the WNYAMI study, 1328 (89%) with sufficient data were available for the analysis. Cases missing data on the SF-36 vitality domain (n = 54) and those never returning a follow-up survey despite being alive at least 2 years after the study interview (n = 114) were excluded from the current analysis. Excluded participants were significantly younger than those included (mean age 52 vs. 55 years, P < 0.01), though there were no important differences between the groups for sex, lifetime pack-years smoking, or body mass index (all P values > 0.40). Mean (standard deviation) follow-up time among individuals not experiencing any recurrent event was 5.2 (2.5) years (maximum 8.8 years). During follow-up a total of 240 first recurrent events were recorded, 207 recurrent MIs and 33 cardiac deaths.
Results
Baseline demographics, risk factors, post-MI treatments, and index MI characteristics are presented across vitality groups in Table 1. Individuals with low vitality scores were more likely to be younger, female, of higher body mass index, diabetic, currently smoking, and less physically active than individuals with higher vitality scores. Among study participants with available data, measures of MI severity were not strongly associated with vitality scores, though the association between vitality score and relative peak CK-MB was statistically significant; the Spearman correlation coefficients were very low between vitality score and peak CK (r = –0.04), relative peak CK (r = –0.05), peak CK-MB (r = –0.01), relative peak CK-MB (r = 0.04), and ejection fraction (r = 0.02). The vitality score was strongly and significantly positively associated with all other SF-36 scales (all Spearman correlation coefficients between 0.45 and 0.62) and negatively associated with CES-D scores (r = – 0.60).
Baseline patient and index MI characteristics across vitality groups
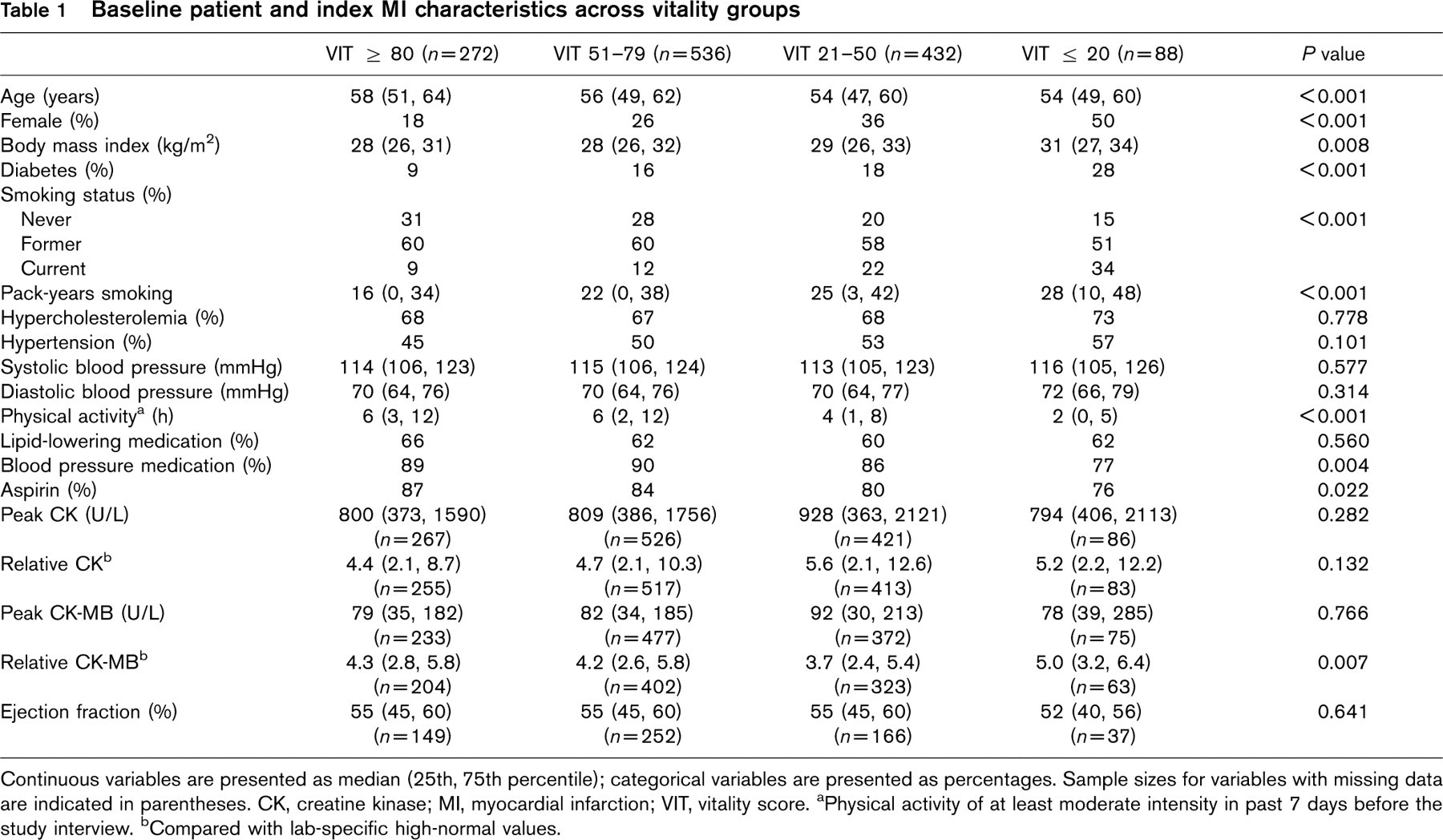
Continuous variables are presented as median (25th, 75th percentile); categorical variables are presented as percentages. Sample sizes for variables with missing data are indicated in parentheses. CK, creatine kinase; MI, myocardial infarction; VIT, vitality score. aPhysical activity of at least moderate intensity in past 7 days before the study interview. bCompared with lab-specific high-normal values.
Cox proportional hazards models are presented in Table 2. The unadjusted analysis showed a strong monotonic association between vitality score and recurrent MI/death from cardiac causes (model 1). Adjusting for the traditional cardiovascular disease risk factors (model 2) attenuated the HRs, though a strong significant trend was still observed. The results were relatively unchanged by adding relative peak CK to the model (model 3). Results of model 3 were similar when replacing relative peak CK with other enzyme indices or ejection fraction. Adding the SF-36 general mental health domain and CES-D scores (model 4) accentuated the HRs. Interactions between vitality and sex were assessed but were not statistically significant in any adjusted model (all P values > 0.80).
The association between vitality and recurrent events persisted across both short-term (≤ 2 year) and long-term (> 2 years) follow-up intervals in unadjusted models (Table 3). Though higher HRs were observed over the longer-term follow-up, the proportional hazards assumption was not significantly violated. Adjustment for variables from model 2 led to the trend being nonsignificant for short-term follow-up, though an increased risk of more than 90% in the lowest versus highest vitality groups remained. A significant trend persisted over long-term follow-up after adjustment. The associations remained strong when analyzing cardiac death and recurrent MI individually in separate models (data not shown).
Cox proportional hazards models for recurrent cardiac events (recurrent myocardial infarction, cardiac death) across vitality groups
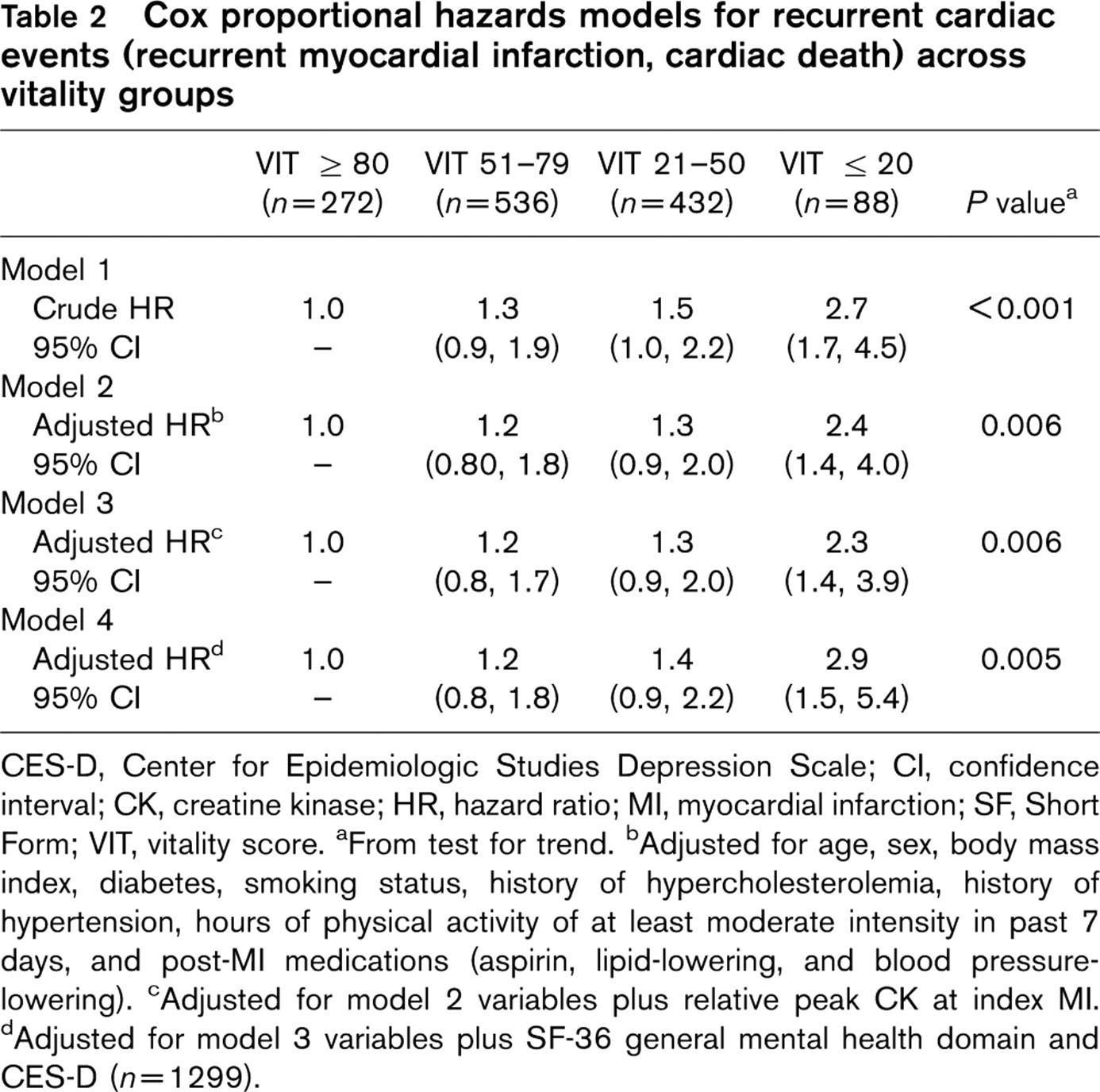
CES-D, Center for Epidemiologic Studies Depression Scale; CI, confidence interval; CK, creatine kinase; HR, hazard ratio; MI, myocardial infarction; SF, Short Form; VIT, vitality score. aFrom test for trend. bAdjusted for age, sex, body mass index, diabetes, smoking status, history of hypercholesterolemia, history of hypertension, hours of physical activity of at least moderate intensity in past 7 days, and post-MI medications (aspirin, lipid-lowering, and blood pressure-lowering). cAdjusted for model 2 variables plus relative peak CK at index MI. dAdjusted for model 3 variables plus SF-36 general mental health domain and CES-D (n = 1299).
Cox proportional hazards models for recurrent cardiac events (recurrent myocardial infarction, cardiac death) across vitality groups, split by follow-up time (≤ 2, > 2 years)
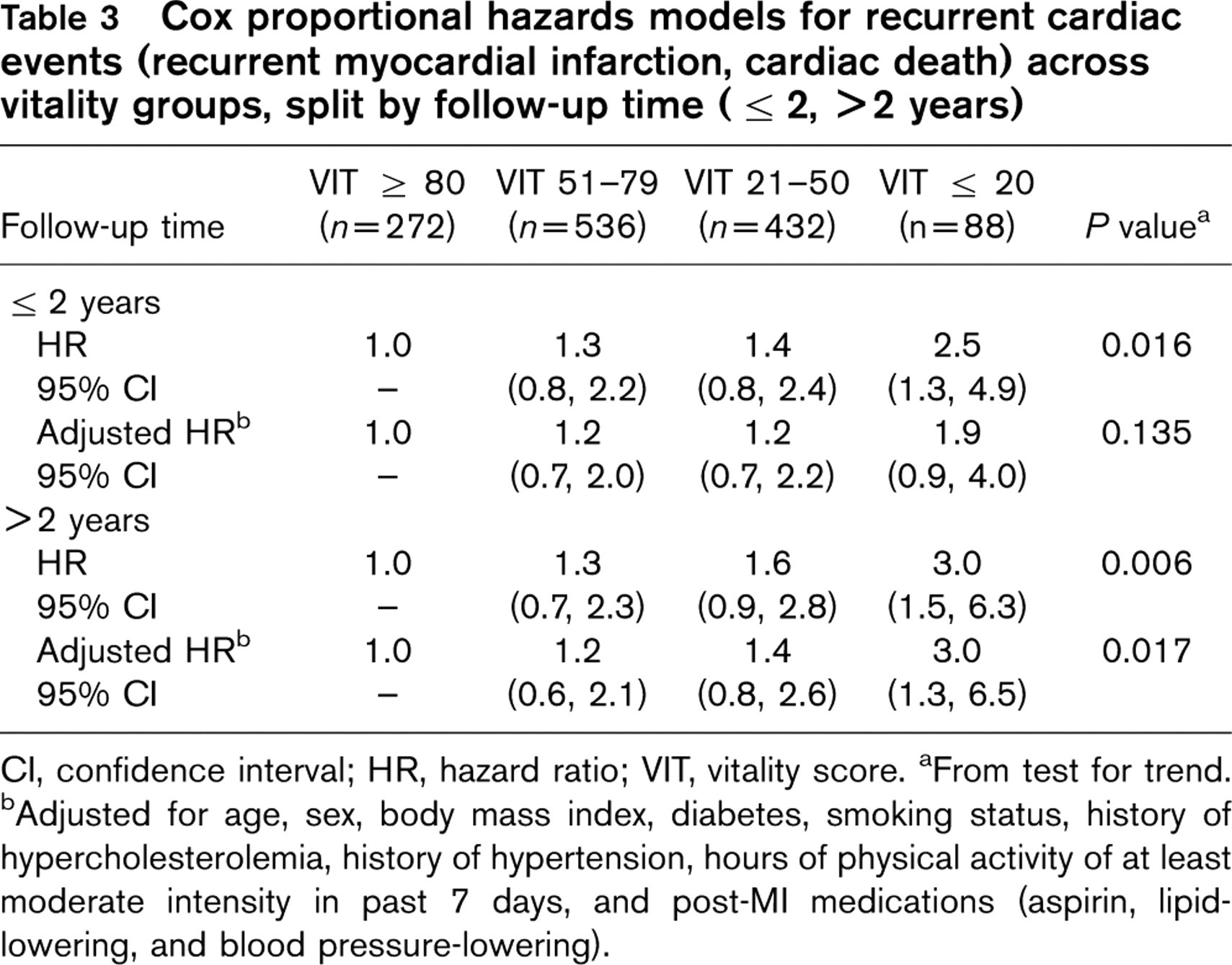
CI, confidence interval; HR, hazard ratio; VIT, vitality score. aFrom test for trend. bAdjusted for age, sex, body mass index, diabetes, smoking status, history of hypercholesterolemia, history of hypertension, hours of physical activity of at least moderate intensity in past 7 days, and post-MI medications (aspirin, lipid-lowering, and blood pressure-lowering).
Discussion
The major finding in this population-based prospective study is the increased likelihood of recurrent MI and cardiac death among MI survivors reporting low vitality. This association remained strong after controlling for traditional cardiovascular disease risk factors, severity of the index MI as measured by cardiac enzymes and ejection fraction, and mental correlates of vitality including depression. The association persisted beyond 2 years of follow-up, suggesting that the vitality measure was not merely a marker of ‘acute’ illness and concomitant event risk. Though residual physiological and/or psychological effects driving the observed association remain a viable hypothesis not disproved in this study, our data suggests that these mechanisms may be acting in both an acute and chronic manner. This persistent association over long-term follow-up has been observed by some authors but contradicted by others [1, 8, 10, 11, 18, 21], with one prospective study showing a complete lack of association between vitality and cardiac events by the fourth year of follow-up [10].
To our knowledge the current report is the first population-based study to describe the association between a vitality measure and recurrent events in a large MI cohort of both men and women, while simultaneously adjusting for traditional, physiological, and psychological confounders and/or mediators of the vitality-cardiac event relationship. Our results extend the findings from previous studies reporting associations between measures of vitality and various cardiac events among general populations, among individuals undergoing revascularization procedures, and in the single study focusing on AMI survivors [1, 4–11, 13, 15]. None of these studies measured vitality with the SF-36 vitality domain, however, precluding direct comparison of the effect estimates with this study.
The subjectiveness of the vitality construct makes interpreting study findings challenging. The current study uses the vitality domain from the well-validated and well-studied SF-36, where Ware and Sherbourne [20] described the vitality domain as a measure of ‘energy level and fatigue’. Another commonly used label among researchers in this field is ‘vital exhaustion’, which adds irritability and a sense of demoralization to the previous definition. Appels et al. [22] have shown vital exhaustion to be a common premonitory symptom of AMI, and accordingly developed the Maastricht Questionnaire (MQ) to enable quantification of the vital exhaustion construct in subsequent research. Several studies from general populations have shown increased risk of cardiac events with low vitality as measured by the MQ [6–7, 9–11, 21, 22]. For instance, in a case–control study reported by Appels et al. [7], low vitality as identified by the MQ was associated with an increased likelihood of a first MI among women after controlling for traditional cardiovascular disease risk factors (odds ratio = 2.8 for MQ score above vs. below median; i.e. low vs. high vitality). Furthermore, in a prospective cohort study of general practice patients with or without cardiovascular disease, MQ scores in the top third of the range were associated with an almost three-fold increased risk of nonfatal MI and cardiac death after adjusting for traditional risk factors [6]. None of these studies controlled for physiological measures of cardiovascular disease or psychological factors which may have explained the observed associations.
Many of the aforementioned studies conducted in general populations noted unmeasured underlying cardiac disease as a possible mechanistic link between low vitality and increased cardiac event risk. Studies conducted among individuals undergoing revascularization procedures attempted to address this concern by including a measure of cardiac disease severity. For instance, in a study of 127 men undergoing PTCA, Kop et al. [13] found that post-PTCA vital exhaustion was associated with a composite endpoint (cardiac death, MI, coronary artery bypass graft, repeat PTCA, new coronary lesion, recurrent angina) after 1.5 years of follow-up, adjusted for presence of multivessel disease and hypercholesterolemia (odds ratio = 2.3 for MQ scores above vs. below upper tertile). Subsequently published studies extending this same study population reported similar findings [4, 5]. Appels et al. [5] showed vital exhaustion was modestly yet significantly associated with the number of diseased vessels, but the association between vital exhaustion and cardiac events remained strong after controlling for this measure of disease severity.
In a study of 110 female AMI survivors, Koertge et al. [15] found vital exhaustion to portend an increased risk of recurrent MI, cardiac death, and need for revascularization procedures (HR = 2.2 for MQ scores above vs. below median) after adjusting for chest pain severity and any significantly stenotic coronary artery (≥ 50% luminal obstruction) over a mean follow-up period of 4.7 years. The number of events available for multivariable analysis was small (35 events), with over half of these events identified as ‘softer’ revascularization procedures. Psychological correlates of vitality were not evaluated in this particular study, though another relevant study among 671 AMI survivors with or without previous MI found an association between fatigue and sudden cardiac death after adjusting for depression [23].
The precise physiological and/or psychological mechanism(s) whereby vitality serves as a marker for increased risk of recurrent cardiac events in survivors of AMI remains unclear. Strong associations between vitality and physiologic measures of MI severity/cardiac dysfunction were not observed in our study. In particular, our results did not show strong associations between vitality and post-MI ejection fraction, peak CK, or peak CK-MB. As such, controlling for these variables had little effect on the association between vitality and outcome despite observing slightly increased risk of events with high cardiac enzymes and low ejection fraction in our data (data not shown). The lack of correlation between these markers and vitality has been observed in previous studies, yet other studies have observed associations between vitality and another measure of disease severity – the number of diseased vessels as determined by angiography – though the amount of variation in vitality scores explained by the number of diseased vessels was noted as small at less than 10% [3, 5, 13, 16, 24]. Interestingly, vitality scores have been shown to improve 2 weeks after angioplasty of significantly stenosed vessels, and 6–15 weeks after pharmacotherapy, angioplasty, or bypass surgery among individuals undergoing angiography [5, 24, 25]. With these interventions myocardial perfusion is assumed to be improved compared with pretreatment levels, however these studies did not directly evaluate whether myocardial perfusion served as an important link between vitality and subsequent cardiac outcomes. In summary, the combination of findings reported to-date suggests at most a weak association between vitality and physiologic measures of cardiovascular disease, though future studies incorporating more relevant measures of subclinical cardiovascular disease such as myocardial perfusion and novel biomarkers of heart failure may provide clarifying information.
A contrasting secondary mechanistic hypothesis implicates vitality as a surrogate for psychological attributes portending increased risk of cardiac events, such as depression. Though our results did reveal a strong association between vitality and depression as measured by the CES-D (r = –0.60) and the general mental health domain from the SF-36 (r = 0.57), inclusion of these factors in statistical models did not attenuate the association between vitality and outcome despite modest associations (P ≤ 0.20) between both of these variables and recurrent events. Depression and low vitality/fatigue are often paired and indistinguishable disorders among individuals with heart disease, creating difficulty in teasing out their independent effects [13, 17, 23, 26–29]. That the SF-36 vitality domain may be measuring depression to some extent cannot be determined from the cross-sectional association reported here. The possible synonymous interpretation of low vitality and depression is crucial in light of the volume of evidence suggesting an association between depression and future cardiac events. Two recent meta-analyses have quantified the independent effect of depression on the increased risk of cardiac events to be as much as 50–150% [30, 31]. However, notwithstanding some encouraging results with the selective serotonin reuptake inhibitor class of antidepressant pharmacotherapy, randomized intervention trials designed to target depression in MI patients for the purpose of reducing cardiac events have not revealed promising findings [32–34]. Another randomized clinical trial designed to reduce cardiac events by targeting the psychological component of exhaustion/vitality with behavioral therapy among 710 ‘exhausted’ individuals after successful percutaneous coronary intervention has also reported negative findings despite promising results from an earlier pilot study [35, 36]. In summary, data from clinical trials thus far do not support targeting psychological components of vitality for reducing events among MI survivors with low vitality.
Our results in combination with results from previous studies do not identify a clear interventional target specifically for post-MI survivors with low vitality. Although control or improvement of traditional cardiovascular disease risk factors, systolic dysfunction, and psychological disorders after AMI will remain therapeutic mainstays, our findings suggest an increased risk imparted by low vitality may persist even with control of these factors. Additional research examining more closely the vitality-outcome ‘black box’ have focused on perturbations of the hypothalamic-pituitary-adrenocortical axis, coagulation and inflammatory markers, heart rate variability, etc. as possible mediators of this relationship [28]. Further evaluation of myocardial perfusion and sensitive biomarkers of heart failure may also provide valuable information on possible mechanistic links. Of note, multiple interventions have shown the ability to improve vitality in patients with cardiovascular disease [5, 35, 37, 38]; though none have shown that cardiovascular events can be reduced by targeting vitality.
A key limitation of our study is the lack of information on post-MI adherence to both pharmacologic and nonpharmacologic therapies, especially cardiac rehabilitation. Furthermore, our study group represents a healthier segment of the AMI population, having survived the index event on average at least 4 months and being willing to undergo an extensive interview and physical examination for research purposes. The validity of findings may also be weakened by imprecise measurement of key parameters such as cardiac enzymes. Peak cardiac enzymes were recorded from medical charts and may not accurately reflect the true peak level, which can only be determined by serial enzyme measurements. Imprecise characterization of these and other variables may have led to residual confounding of the vitality-outcome relationship, though our group does not believe the observed association can be attributed solely to residual confounding.
Conclusion
Low vitality was associated with increased risk of recurrent cardiac events among first AMI survivors after controlling for traditional risk factors, markers of index MI severity, and psychological confounders. Future studies should investigate possible physiological and psychological links with vitality as possible targets of intervention after AMI.
Footnotes
Acknowledgements
This study was funded by the following grants: R01-DE012085 and R01-DE1358501A1 (National Institute of Dental and Craniofacial Research); 5 P50 AA09802 (National Institute on Alcohol Abuse and Alcoholism).
Conflicts of interest: none declared.