
Abstract
Background Statin therapy has been found to substantially and significantly reduce coronary events in carriers of the KIF6 719Arg variant (rs20455) but not in noncarriers. We investigated whether, among the elderly, statin therapy also significantly reduced coronary events in carriers but not in noncarriers.
Design and methods Among 5752 patients of the PROspective Study of Pravastatin in the Elderly at Risk (PROSPER) study, we assessed the effect of pravastatin, compared with placebo, on coronary events according to 719Arg carrier status using proportional hazards models.
Results Since benefit from statin therapy in elderly patients has been primarily shown among those with prior vascular disease, we performed analyses in PROSPER patients with prior disease and found that pravastatin therapy significantly reduced events in 719Arg carriers [hazards ratio (HR): 0.66, 95% confidence interval (CI): 0.52–0.86] but not in noncarriers (HR: 0.94, 95% CI: 0.69–1.28), P= 0.09 for interaction between treatment and carrier status. Among those without prior disease, no significant benefit was observed in either carriers or noncarriers. Among those with prior vascular disease in the placebo arm, Trp719Arg heterozygotes were at significantly greater risk, compared with noncarriers (HR: 1.36, 95% CI: 1.03–1.81, P = 0.03); the HR of 719Arg carriers, compared with noncarriers, was 1.28 (95% CI: 0.98–1.69, P =0.07).
Conclusion Elderly carriers of the KIF6 719Arg variant with prior vascular disease received significant benefit from pravastatin therapy; no benefit was observed in noncarriers with prior disease or in those without prior disease (carriers or noncarriers).
Introduction
Randomized clinical studies of statins in elderly populations have shown substantial reductions of mortality and nonfatal coronary events, particularly in those with prior vascular disease [1–3]. Thus, biomarkers that may influence response to therapy should be investigated in elderly populations [4].
One biomarker associated with both risk for coronary events and reduced events from statin therapy is the 719Arg variant of kinesin-like protein 6 (encoded by the KIF6 gene). Carriers of the 719Arg variant, compared with noncarriers, were at up to 50% greater risk for coronary events in the placebo group of both the West of Scotland Coronary Prevention (WOSCOPS) and the Cholesterol and Recurrent Events (CARE) studies [5] and in three large population-based prospective cohorts: the Atherosclerosis Risk in Communities study (ARIC) [6], the Women's Health Study (WHS) [7], and the Cardiovascular Health Study (CHS) [8].
Carriers of the KIF6 719Arg risk variant (B60% of the patients), but not noncarriers, also received substantial and significant reduction of coronary events from pravastatin therapy in the CARE and WOSCOPS studies [5] and from high-dose atorvastatin therapy, compared with standarddose pravastatin therapy, in the Pravastatin and Atorvastatin Evaluation and Infection Therapy-Thrombosis in Myocardial Infarction 22 (PROVE IT–TIMI 22 study) [9].
Although carriers of the KIF6 719Arg variant, but not noncarriers, received a significant reduction of coronary events from statin therapy in the predominantly middleaged patients of WOSCOPS, CARE, and PROVE IT-TIMI 22, it was not known whether this would also be true in the elderly. Therefore, in a genetic study of the PROspective Study of Pravastatin in the Elderly at Risk trial (PROSPER), we investigated whether statin therapy significantly reduced coronary events in carriers but not in noncarriers among the elderly with and without prior vascular disease.
Methods
Study population
The study population was derived from PROSPER, a randomized, double-blind, placebo-controlled trial designed to assess the effect of pravastatin in the prevention of major cardiovascular events among participants aged at least 70 years at enrollment who were at risk for cardiovascular events because of preexisting vascular disease, smoking, hypertension, or diabetes [1]. Five thousand eight hundred and four patients (2804 men, 3000 women) were randomized to treatment with 40 mg pravastatin per day or placebo in three centers (Cork, Ireland; Glasgow, Scotland; and Leiden, The Netherlands) and followed for an average of 3.2 years; 44.2% of the enrolled patients had a history of prior vascular disease (myocardial infarction, stable angina, intermittent claudication, stroke, transient ischemic attacks, arterial surgery, or amputation for vascular disease more than 6 months before study entry). All participants provided written informed consent and the study protocol was approved by the institutional ethics review boards.
End point and laboratory values
The end point of this genetic study was time from enrollment to the first incident coronary event, a composite of coronary heart disease death, nonfatal myocardial infarction, percutaneous transluminal coronary angioplasty, or coronary artery bypass graft. The methods of follow-up and end point validation have been described prior [1]. KIF6 Trp719Arg genotypes were determined using an allele–specific real-time PCR genotyping assay [10] in a core facility. The accuracy of the KIF6 Trp719Arg genotypes are expected to be greater than 99% on the basis of a comparison with KIF6 Trp719Arg genotypes determined using a different technology (oligonucleotide ligation) [5]. Of the 5776 patients from whom DNA samples of adequate quantity and quality were available, KIF6 Trp719Arg genotypes were determined for 5757. After excluding five patients for whom covariate data were missing, 5752 remained in this genetic study of PROSPER.
Statistical analyses
Reported P values are two-sided. Deviation from Hardy-Weinberg equilibrium was evaluated using an exact test [11]. Differences in baseline characteristics between groups defined by KIF6 Trp719Arg were assessed by analysis of variance (genotypes) or the t-test (719Arg carrier status) for continuous variables and by the X2 test for discrete variables. Cox proportional hazards models and the Wald test were used to assess the effect of pravastatin, compared with placebo, on coronary events and to assess the association between coronary events and genotype or 719Arg carrier status. Interaction between KIF6 719Arg carrier status and statin treatment was assessed by the likelihood ratio test. Potential interactions between 719Arg carrier status and each covariate was tested in a separate Cox model that included the interaction (cross-product) term between the covariate and carrier status as well as the main effect terms for 719Arg carrier status and the covariates used in the adjusted model. The method of Kaplan and Meier was used to estimate the cumulative incidence of coronary events at 3 years of follow-up; differences were assessed with the log-rank test. Differences between the mean on-therapy lipid levels in 719Arg carriers and noncarriers were assessed by t-test. SAS version 9 was used, except that power was assessed by QUANTO version 1.2.4, May 2009, (http://hydra.usc.edu/gxe/).
Results
Baseline characteristics and KIF6 Trp719Arg genotype frequencies
The baseline characteristics according to KIF6 719Arg carrier status are presented in Table 1. The prevalence of traditional risk factors used in multivariate analyses did not differ between carriers of the 719Arg variant and noncarriers with the exception of diabetes, which was more common among noncarriers; thus, the prevalence of diabetes does not seem to explain the association of 719Arg carriers with increased risk of coronary events. The prevalence of these risk factors did not differ between treatment groups in the PROSPER genetic cohort (P>0.14, not presented). Carriers of the 719Arg variant were 58.8% of this PROSPER cohort: the genotype frequencies were 12.6% for ArgArg, 46.2% for ArgTrp, and 41.2% for TrpTrp, a distribution that did not deviate from Hardy-Weinberg equilibrium expectations (P = 0.58).
Baseline characteristics of the patients according to KIF6 Trp719Arg genotype and 719Arg carrier status
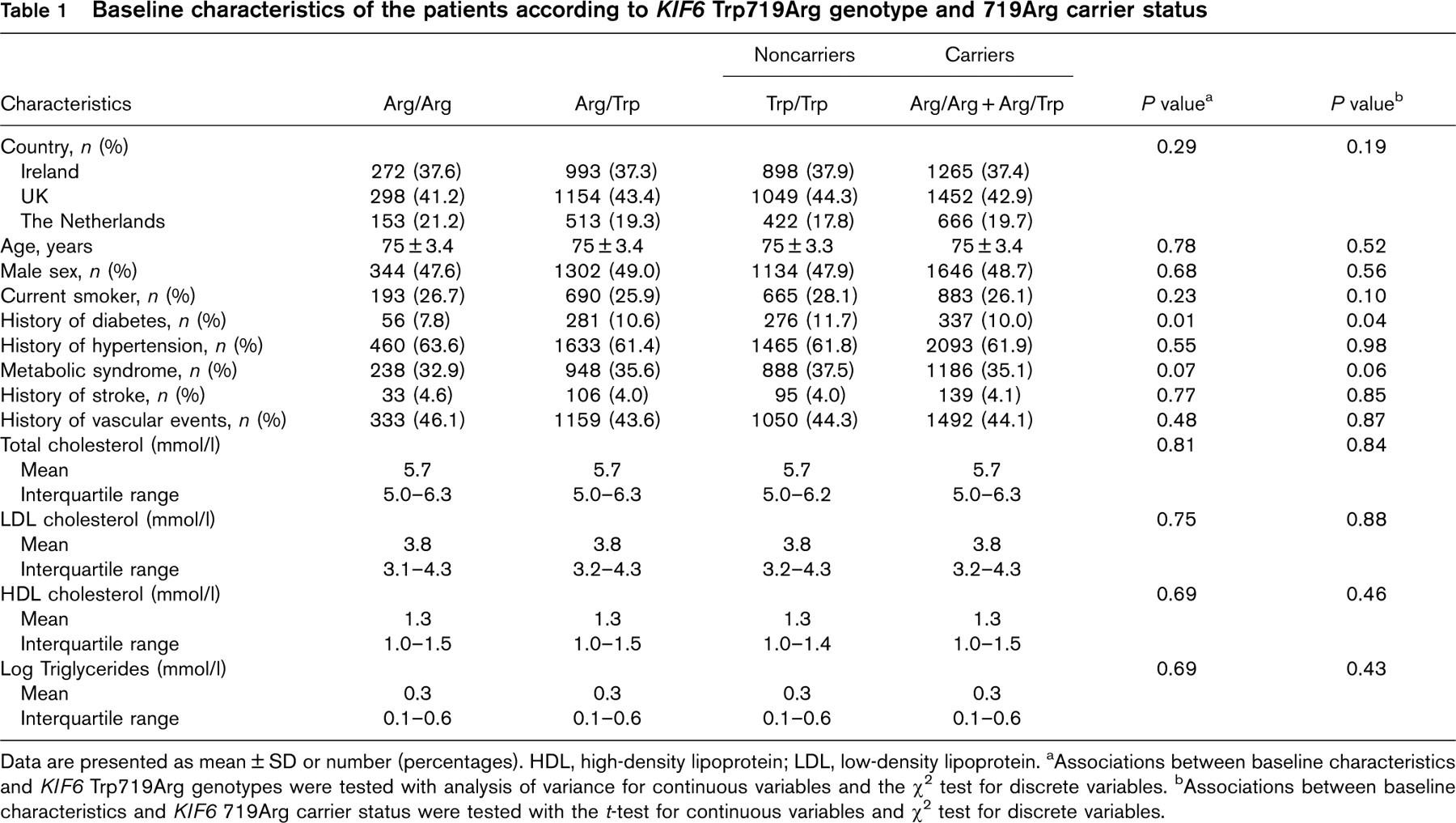
Data are presented as mean ± SD or number (percentages). HDL, high-density lipoprotein; LDL, low-density lipoprotein. aAssociations between baseline characteristics and KIF6 Trp719Arg genotypes were tested with analysis of variance for continuous variables and the X2 test for discrete variables. bAssociations between baseline characteristics and KIF6 719Arg carrier status were tested with the t-test for continuous variables and X2 test for discrete variables.
Effect of pravastatin on coronary events by KIF6 Trp719Arg among patients with prior vascular disease
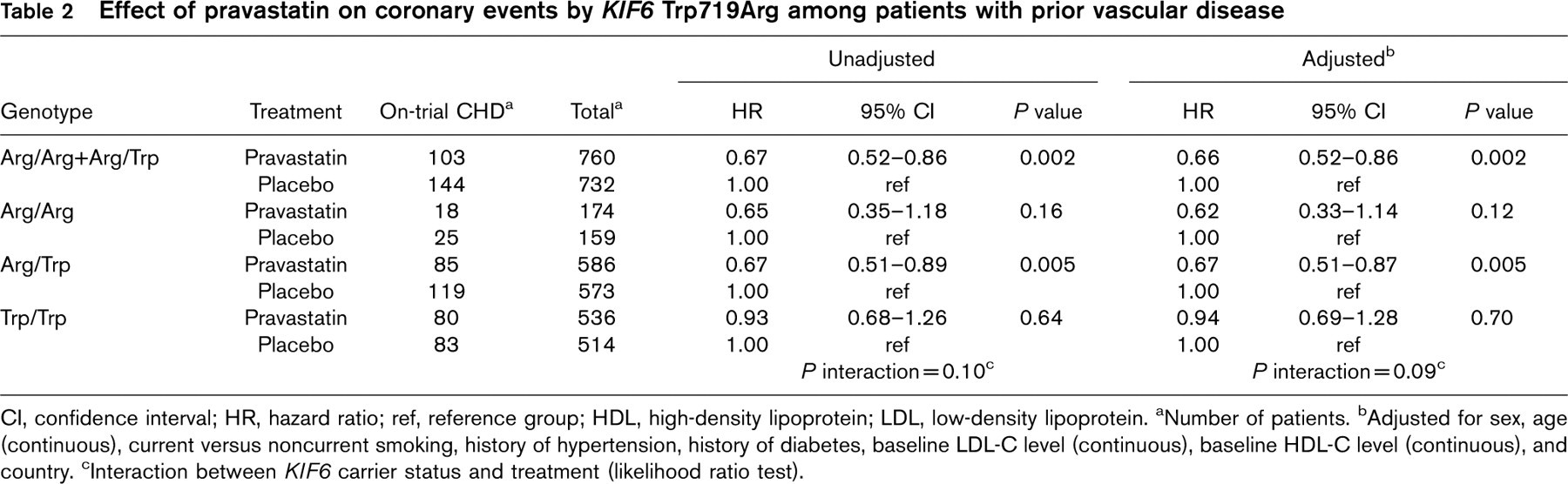
CI, confidence interval; HR, hazard ratio; ref, reference group; HDL, high-density lipoprotein; LDL, low-density lipoprotein. aNumber of patients. bAdjusted for sex, age (continuous), current versus noncurrent smoking, history of hypertension, history of diabetes, baseline LDL-C level (continuous), baseline HDL-C level (continuous), and country. cInteraction between KIF6 carrier status and treatment (likelihood ratio test).
Outcome of therapy and KIF6 Trp719Arg
In the original PROSPER study, significant benefit from pravastatin therapy was observed among only the 44.2% of the patients with prior vascular disease and not among those without prior vascular disease [1,2], and substantial benefit from statin therapy among the elderly with prior vascular disease has been reported in a meta-analysis of nine trials [2]. Therefore, we investigated the effect of pravastatin therapy according to KIF6 719Arg carrier status separately in PROSPER patients with and without prior vascular disease. We found that in patients with prior vascular disease, pravastatin therapy, compared with placebo, resulted in a 33.6% reduction of coronary events among 719Arg carriers; in contrast, among noncarriers with prior vascular disease the reduction of coronary events was not significant (Table 2). Among patients without prior vascular disease, no significant reduction of coronary events was observed in either carriers or noncarriers (Fig. 1).
In carriers of the KIF6 719Arg variant with prior vascular disease, the cumulative incidence of fatal or nonfatal coronary events at 3 years was 18.8% in the placebo group and 12.5% in the pravastatin group (log rank P = 0.002, Fig. 1a), an absolute risk reduction of 6.3% [95% confidence interval (CI): 2.5–10.0%], favoring pravastatin therapy. However, in noncarriers with prior vascular disease, the cumulative incidence events were essentially the same in the two treatment groups: 14.0% in the placebo group and 12.8% in the pravastatin group (Fig. 1b), an absolute risk reduction of 1.2% (95% CI: − 3.0 to 5.4%).
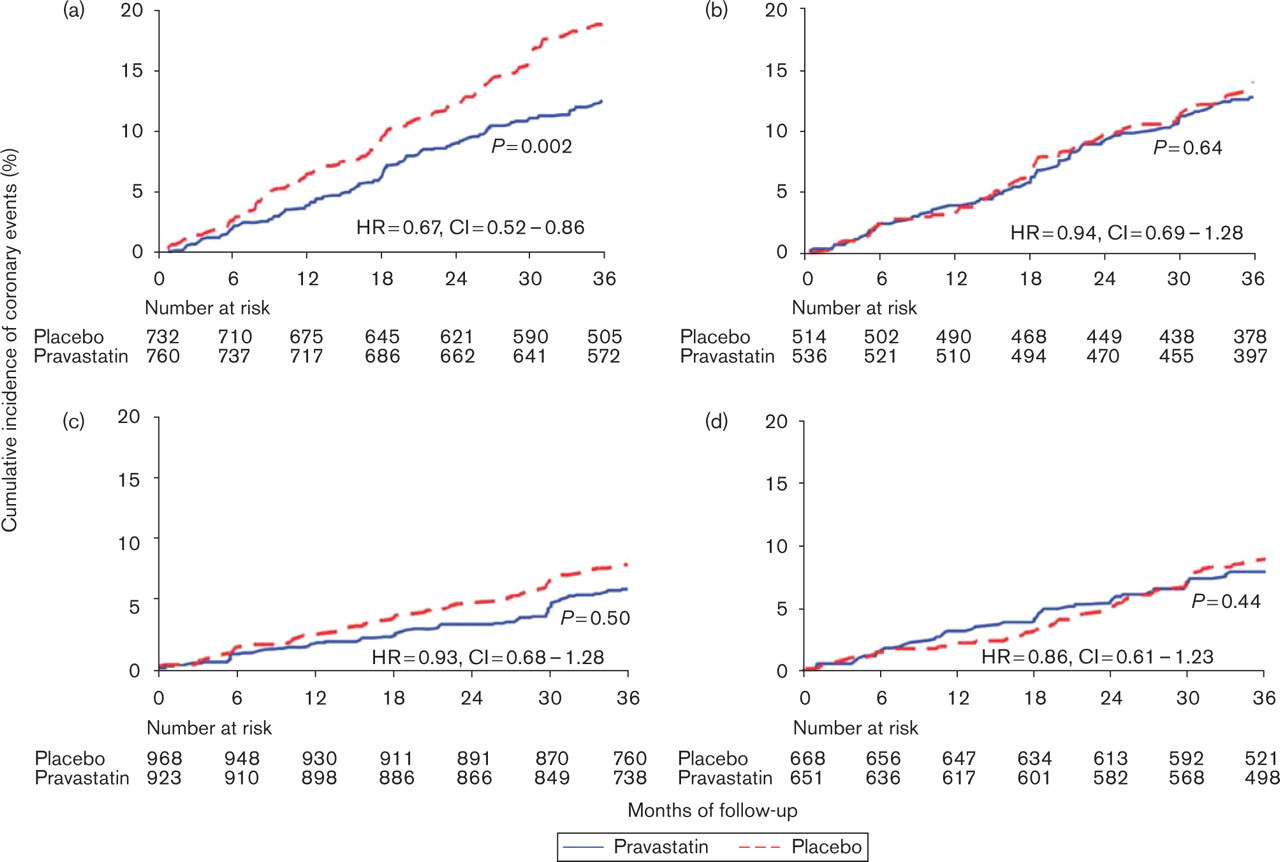
On-trial coronary events according to treatment and KIF6 719Arg carrier status. Kaplan-Meier estimates of the cumulative incidence of coronary heart disease death, nonfatal myocardial infarction, percutaneous transluminal coronary angioplasty, or coronary artery bypass graft in pravastatin and placebo-treated patients: (a) among carriers of the KIF6 719Arg variant with prior vascular disease, (b) among noncarriers with prior vascular disease, (c) among carriers of the KIF6 719Arg variant without prior vascular disease, (d) among noncarriers without prior vascular disease. The logrank P values are based on 3 years of follow-up.
Since low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol, and triglyceride levels have been used as surrogate markers for the benefit of statin therapy [12], we investigated whether the ontherapy levels of LDL-C, high-density lipoprotein cholesterol, and triglyceride differed between carriers and noncarriers of the KIF6 719Arg variant. We found no significant differences in mean levels when comparing carriers with noncarriers at baseline or at any scheduled visit during the study (P>0.18, Fig. 2) with the exception of a difference in mean LDL-C levels in the pravastatin group at 6 months of follow-up, where ontherapy LDL-C levels were greater in carriers than in noncarriers (P = 0.021).
Association of KIF6 719Arg with coronary events
In the placebo group of PROSPER, carriers of the KIF6 719Arg variant were not at increased risk for fatal or nonfatal coronary events, compared with noncarriers: adjusted hazards ratio 1.06 (95% CI: 0.86–1.30), P = 0.59. However, we observed an interaction between KIF6 Trp719Arg carrier status and history of vascular disease (P = 0.03), indicating that the risk of coronary events for carriers, compared with noncarriers, differed significantly between those with and without prior vascular disease. In patients with prior vascular disease, carriers of the KIF6 719Arg risk variant were at 28% greater risk of coronary events, compared with noncarriers; in contrast, carriers without prior vascular disease were not at increased risk (Table 3).
Discussion
In this genetic study of PROSPER, we found that carriers of KIF6 719Arg with prior vascular disease received substantial and significant reduction of coronary events from statin therapy: absolute risk reduction was 6.3% in carriers versus 1.2% in noncarriers. Thus, 16 carriers needed to be treated with pravastatin to prevent one event whereas the number needed to treat for noncarriers was 83. Among those without prior vascular disease, event reduction was not significant in either KIF6 719Arg carriers or noncarriers.
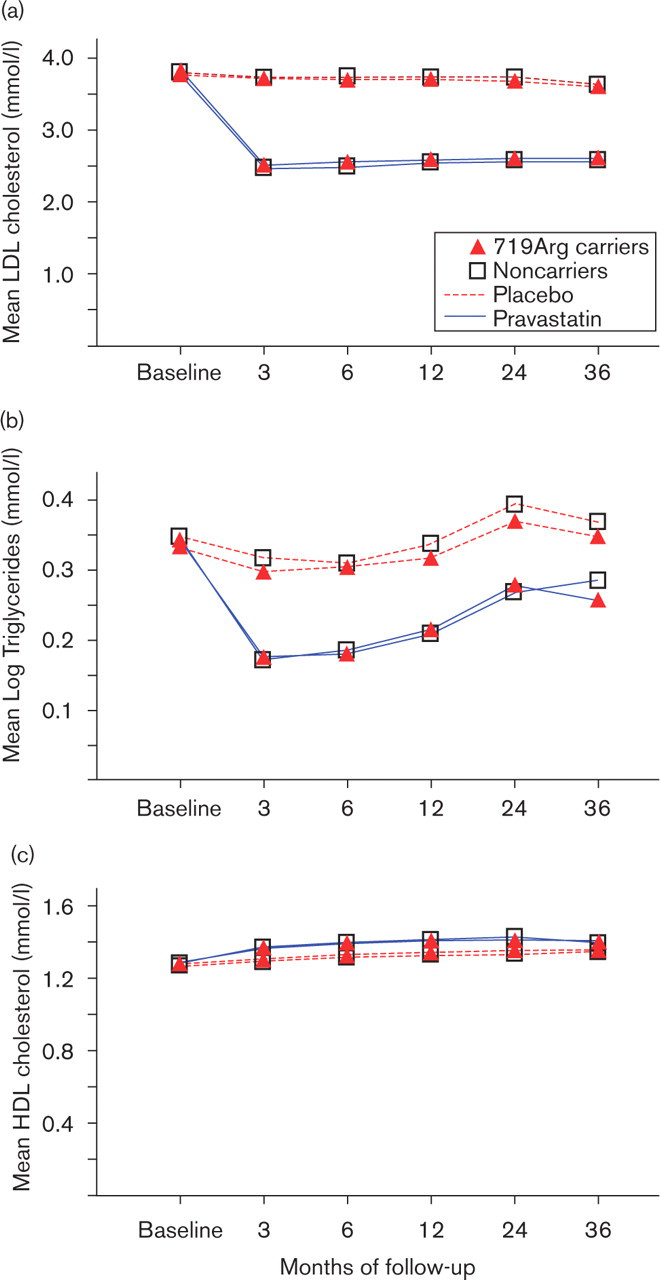
Mean lipid levels according to treatment and KIF6 719Arg carrier status. Mean lipid levels according to KIF6 carrier status: (a) low-density lipoprotein (LDL) cholesterol levels, (b) triglyceride levels, and (c) high-density lipoprotein (HDL) cholesterol levels.
Among PROSPER patients with prior vascular disease, risk reduction was significant in KIF6 719Arg carriers (34%) but not in noncarriers (6%), although the interaction between carrier status and treatment did not reach significance (P = 0.09), possibly because of a lack of statistical power. For example, given the relative risk reduction of 34% in carriers and 6% in noncarriers, 1244 events would have been required for the test of interaction to have 80% power, but this PROSPER analysis had only 410 events. Nevertheless, the significant event reduction from statin therapy in carriers but not in noncarriers is consistent with that observed in genetic studies of CARE [5] and PROVE IT-TIMI 22 [9], two secondary prevention studies and also in WOSCOPS [5], a primary prevention study (Fig. 3).
The differential reduction of coronary events between KIF6 719Arg carriers and noncarriers in PROSPER patients with prior vascular disease was observed despite similar on-therapy lipid levels in carriers and noncarriers. This observation is consistent with the results of a genetic study of PROVE IT-TIMI 22, where event reduction from high-dose atorvastatin therapy, compared with standard-dose pravastatin therapy, was significant in 719Arg carriers, but not in noncarriers, while median ontherapy lipid levels did not differ between carriers and noncarriers [9]. Thus, the event reduction in carriers during statin therapy may be related to a pleiotropic or plaque stabilizing effect of statins.
In this genetic study, significant risk reduction from pravastatin therapy occurred only among those carriers of KIF6 719Arg variant with prior vascular disease. Similarly, in the original PROSPER analysis where the results were not stratified by genotype, only those patients with prior disease received significant benefit from pravastatin [1]. Interestingly, we observed a significant interaction between KIF6 719Arg carrier status and prior vascular disease status and found that only among PROSPER patients with prior vascular disease were carriers of 719Arg at increased risk for coronary events although this risk did not reach significance (P = 0.07). In these separate analyses by prior vascular disease history, the power to detect an association between carrier status and coronary events (assuming the true hazards ratio was 1.3) was 41% among those with prior vascular disease and 32% for those without prior disease.
KIF6 encodes a kinesin motor protein, a member of a large family of proteins that play key roles in the intracellular transport of proteins, lipids, and nucleic acids [13]. The variable 719 residue of KIF6 is located in the tail domain, a domain shown to bind cargo molecules and to regulate motor activity and microtubule binding in other kinesins [14]. The role of the KIF6 kinesin in cardiovascular disease is not known; however, KIF6 is expressed in coronary arteries (see data [15] deposited by King et al. [16]).
Association of KIF6 Trp719Arg with coronary events in the placebo group
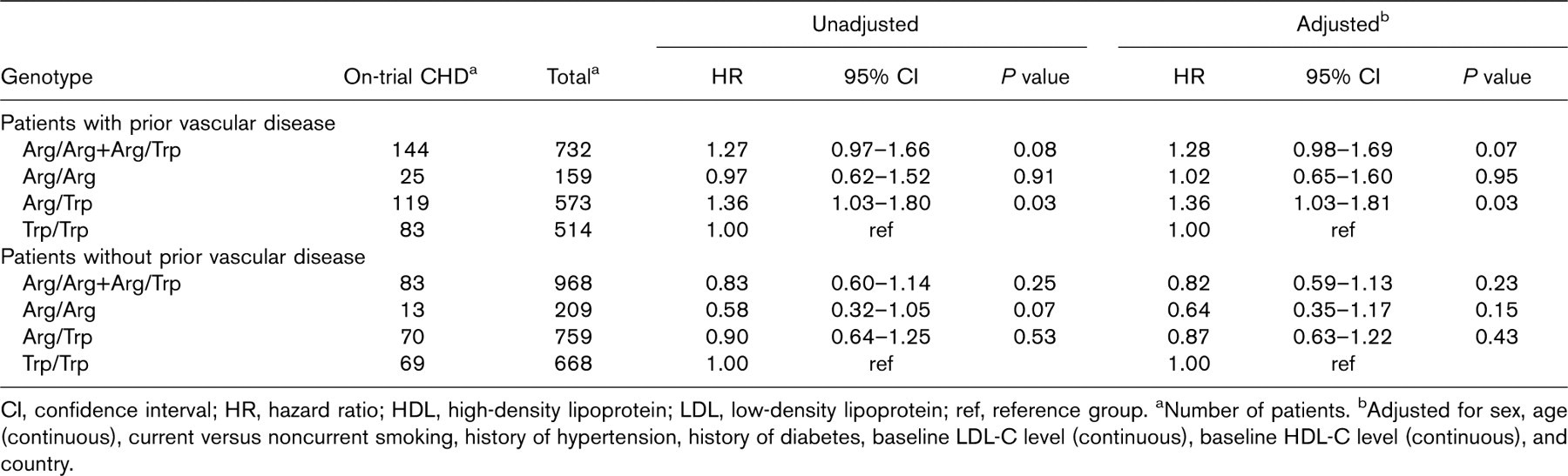
CI, confidence interval; HR, hazard ratio; HDL, high-density lipoprotein; LDL, low-density lipoprotein; ref, reference group. aNumber of patients. bAdjusted for sex, age (continuous), current versus noncurrent smoking, history of hypertension, history of diabetes, baseline LDL-C level (continuous), baseline HDL-C level (continuous), and country.
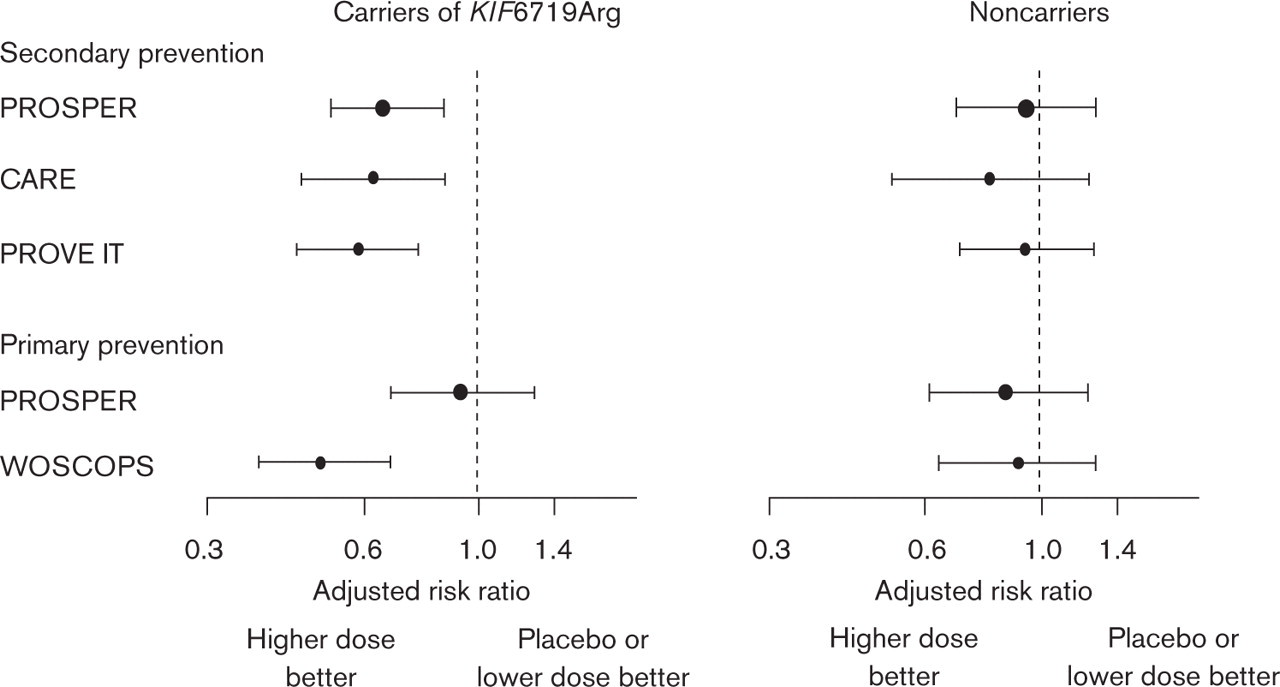
Effect of statin therapy on secondary (patients with prior vascular disease) and primary (patients without prior vascular disease) prevention of coronary events according to KIF6 719Arg carrier status in four randomized prospective studies. CARE, Cholesterol and Recurrent Events; PROSPER, PROspective Study of Pravastatin in the Elderly at Risk; PROVE IT, Pravastatin and Atorvastatin Evaluation and Infection Therapy; WOSCOPS, West of Scotland Coronary Prevention.
Conclusion
In PROSPER, those carriers of the KIF6 719Arg variant with prior vascular disease received substantial and significant reduction of coronary events from statin therapy whereas no benefit was observed in those without prior disease or in noncarriers with prior disease. This preferential benefit from statin therapy in elderly carriers with prior vascular disease could lead to a better-tailored management of coronary heart disease in this rapidly growing population.
Footnotes
Acknowledgements
The authors would like to express their gratitude to Dr Thomas White, Dr John Sninsky, Dr Koustubh Ranade, Dr Katy Simonsen, Dr Lynn Ploughman and Dr Todd Kirchgessner for helpful comments on this study. Funding: The PROSPER trial was supported by research grants from Bristol-Myers Squibb (to PROSPER investigators); genotyping was funded by Celera. Data analyses were done independently of funding source.
Conflicts of interest: O.A.I., C.M.R., C.H.T., J.J.C., and J.J.D. have employment and ownership interest in Celera; J.S. is a consultant for AstraZeneca, Pfizer, and GSK and is on the speaker's bureau for AstraZeneca, Pfizer, and Sankyo; I.F., M.R., J.W.J., G.J.B., and M.B.M. have no disclosures.