
Abstract
Introduction
Although there has been a reduction in coronary heart disease (CHD), it remains a major cause of morbidity and mortality in Ireland. 1 There is strong trial evidence for the benefit of secondary preventive therapeutic measures in patients after acute myocardial infarction (MI), percutaneous coronary intervention or coronary artery bypass graft surgery. 2,3 Changes in lifestyle and risk factors also have a positive influence. 4,5
The Heartwatch programme 6 of secondary prevention for CHD was implemented in 2003 under the auspices of the Irish College of General Practitioners. The first 2 years of follow-up of this programme has been published earlier (11542 patients). 7 Significant changes in systolic blood pressure (SBP), diastolic blood pressure (DBP), total and low-density lipoprotein (LDL) cholesterol and smoking status at 1 and 2 years were observed.
There was no improvement in exercise, body mass index (BMI) or waist circumference. Increased prescription of preventive medications was observed. We now present further evaluation of this programme on a total of 12 358 patients, with up to 3.5 years of follow-up.
Methods
Patients recruited to Heartwatch have significant proven CHD, that is, a history of MI, percutaneous coronary intervention or coronary artery bypass graft surgery. The programme involved 20% of general practices [480 general practitioners (GP)]. Participating patients were invited to attend on a quarterly basis, with continuing care being implemented according to clinical protocols, which initially followed the recommendations of the second European Joint Task Force on Coronary Prevention and subsequently those of the third. 8,9 All GPs were provided with written materials and study training on risk factor interventions, including general measures, lifestyle advice, pharmacological therapies and referral pathways to specialist services should patients require specialist care. Heartwatch participants were offered lifestyle-related advice about smoking cessation and other CHD risk factors. GPs prescribed medication as clinically indicated, including nicotine replacement therapy. Practices could refer patients to community services, including smoking cessation, physical activity and dietary advice. Nurse facilitators were available to address the needs of practice nurses. The total additional cost of the programme over the first 2 years was h4169 023, including the cost of visits, medications and administration. 10
Data recorded by GPs in the centrally held Heartwatch database on the major risk factors (through clinical examination, blood test, patient self report) and prescribed medications enabled monitoring of each patient's response to the Heartwatch programme over a 3.5-year follow-up period.
Analysis was performed for patients at 1, 2, 3 and 3.5 years after recruitment (study visits). The visit date closest to 1, 2, 3 and 3.5 years was determined for each patient and assigned to the relevant follow-up as long as the actual visit was within 60 days of the nominal study visit date. To be included in follow-up at a given year, patients had to have valid data for that and all earlier study visits; for example, patients included in the 3-year follow-up had to have attended the 1 and 2-year study visits. As patients were recruited to Heartwatch on a continuous basis, follow-up of 3.5 years is limited to the smaller numbers who have been in the programme for a sufficient length of time.
Statistical analysis
Means at baseline and the four follow-up study visits were calculated for SBP, DBP, total cholesterol, LDL cholesterol, BMI, waist circumference, fasting glucose (for patients without diabetes mellitus) and haemoblobin A1c (for patients with diabetes mellitus). The percentage smoking was calculated based on an individual having one or more of the following recorded — smoker of one or more cigarettes per day, cigar or pipe. Absolute changes in risk factors between baseline and follow-up were calculated.
Proportions within the target for risk factors and relative changes in proportions between baseline and follow-up study visits were calculated. The targets were those recommended by the Third Joint Task Force of European Society of Cardiology: 9 total cholesterol less than 5 mmol/l, LDL cholesterol less than 3 mmol/l, nonsmoker, SBP less than 140 mmHg, DBP less than 90 mmHg, fasting blood glucose less than 6 mmol/l, exercise ≥210 min/week.
Between-visit differences were assessed using paired t-tests for continuous variables and McNemar's test for categorical variables. At each study visit, data on patients included in the trend analysis (i.e. patients who attended all four study visits) was similar to that of all patients. Significance of trends in medication use over the period of follow-up was determined using Cochran's test. Logistic regression was used to examine the relationship of age and sex to being within the target for risk factors at 3.5 years. SAS statistical software was used (SAS Version 9: Cary, North Carolina, USA).
Results
There were 12,358 patients in the dataset; 75.8% male, 65.6% in the age range of 55-74 years, 14.8% under 55 years and 19.7% above 74 years.
For the 1-year cohort, patients with no valid data at 1 year (4049) were excluded to give 8309 patients. The 2, 3 and 3.5-year cohorts consisted of 5431, 3470 and 2078 patients, respectively.
2-year follow-up
Risk factor data at baseline, 1 and 2 years in the 2-year follow-up cohort
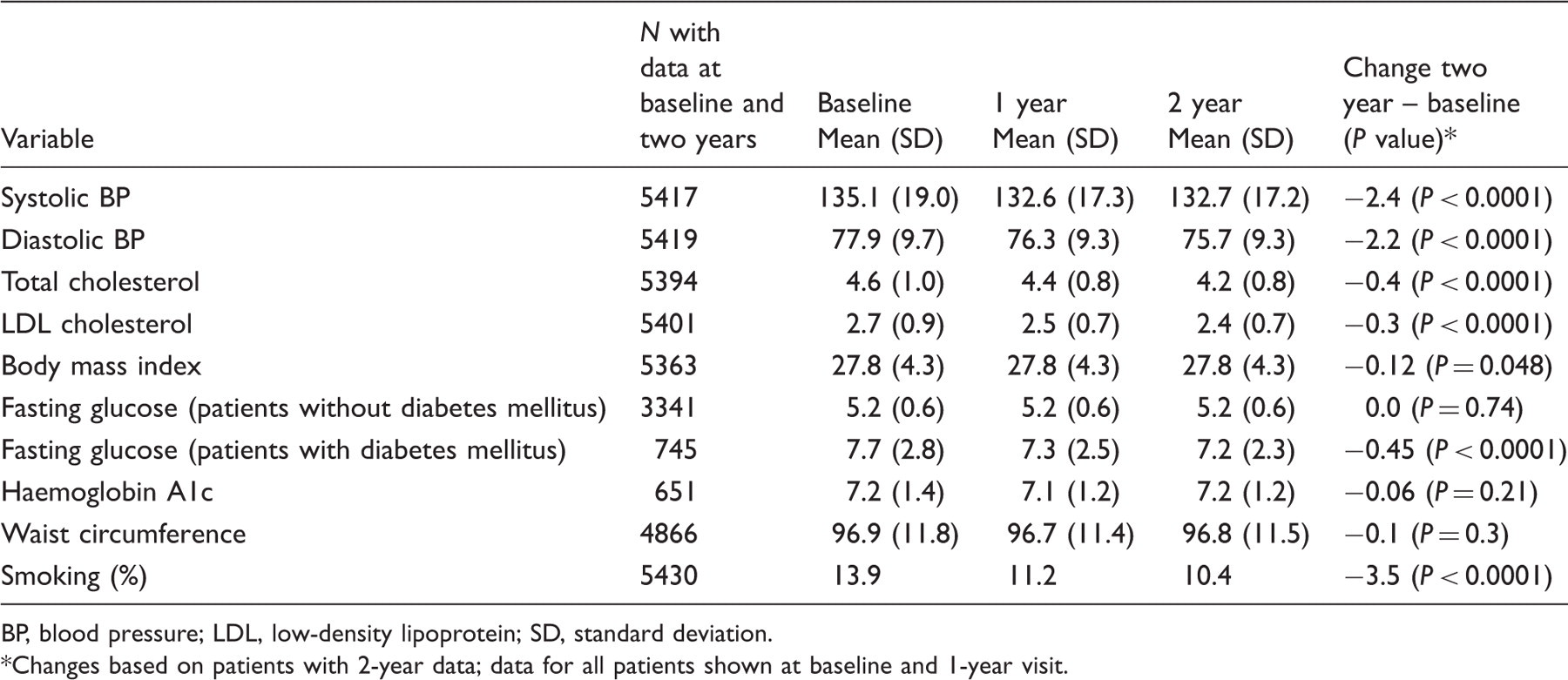
BP, blood pressure; LDL, low-density lipoprotein; SD, standard deviation.
Changes based on patients with 2-year data; data for all patients shown at baseline and 1-year visit.
3.5 year follow-up
Risk factor data at baseline, 1, 2, 3 and 3.5 years in the 3.5-year follow-up cohort
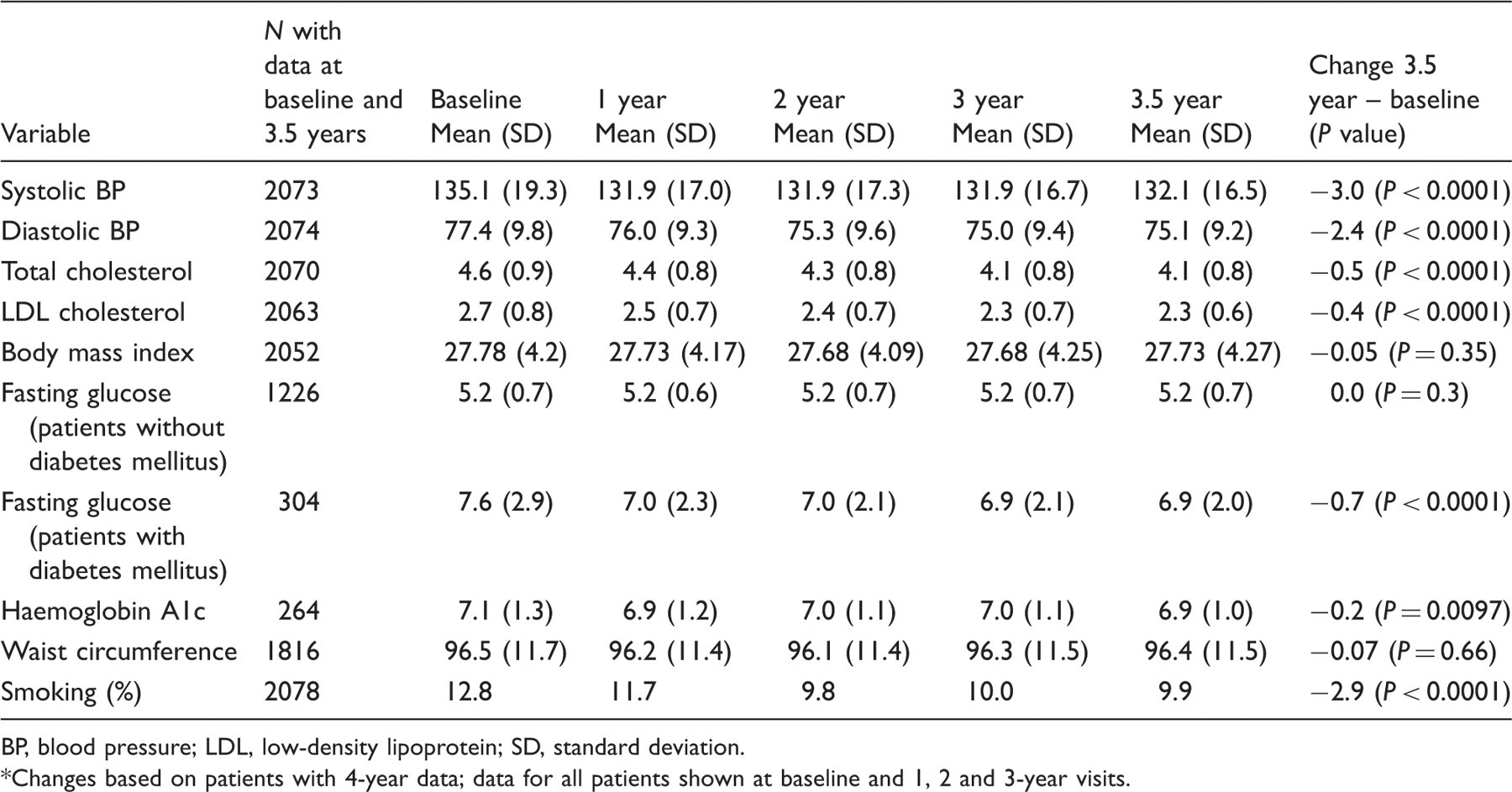
BP, blood pressure; LDL, low-density lipoprotein; SD, standard deviation. *Changes based on patients with 4-year data; data for all patients shown at baseline and 1, 2 and 3-year visits.
Change in proportions within target
Figure 1a shows the proportions within the target for pharmacologically modifiable risk factors and Figure 1b the proportions within target for lifestyle-related risk factors at each year of follow-up. Although proportions of patients within the target for all risk factors except waist circumference showed significant change over the follow-up period, the greatest increase was observed in cholesterol and BP control (Figure 1a), with smaller but significant changes also observed in smoking (Figure 1a) and exercise (Figure 1b). For risk factors where significant change was observed, the greatest annual change occurred in the first year of the programme.
(a) Percentage within the target by pharmocogically modifiable risk factors over 3.5-year follow-up (significance relates to test for trend). (b) Percentage within the target by lifestyle-related risk factors over 3.5-year follow-up (significance relates to test for trend). BMI, body mass index; BP, blood pressure.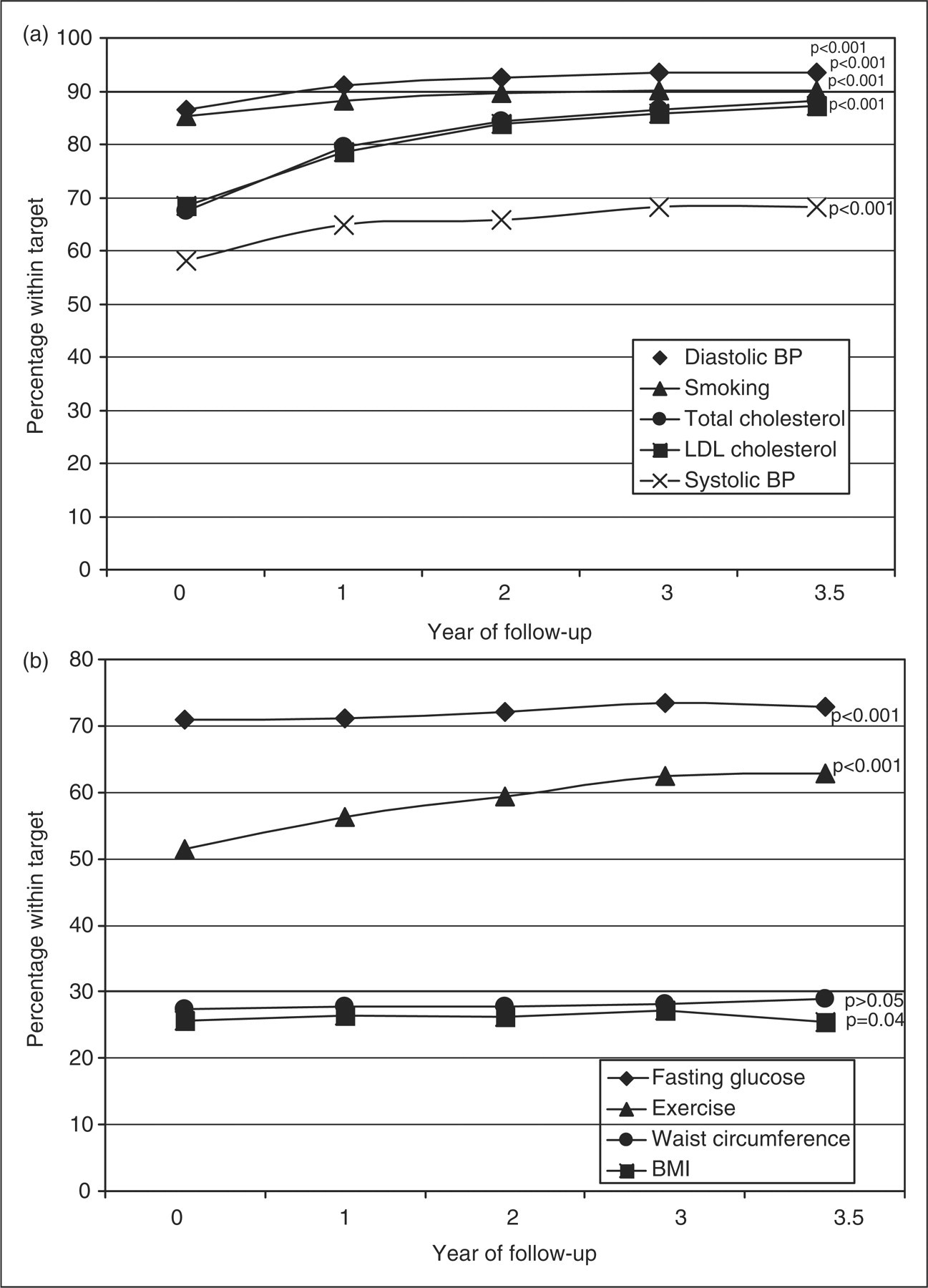
Overall at 3.5-years, 62.8% of patients were within the target for exercise, a relative increase of 17% from baseline (P < 0.0001). There was a 25.2% relative increase in numbers within the target for SBP (to 68.3%, P < 0.0001), 48.4% relative increase for DBP (to 93.5%, P < 0.0001) and 64.8% (to 88.2%, P < 0.0001) and 61.7% (to 87.2%, P < 0.0001) for total and LDL cholesterol, respectively. There was a relative increase of 22.7% in proportion of nonsmokers from baseline (to 90.1%, P < 0.0001). There was no significant reduction for BMI or waist circumference.
Logistic regression showed that males were more likely than females to be within target for SBP [adjusted odds ratio (OR): 1.4, 95% confidence interval (CI): 1.13-1.74], total cholesterol (OR: 2.39, 95% CI: 1.79-3.19), waist circumference (OR: 1.87, 95% CI: 1.46-2.40) and exercise (OR: 1.76, 95% CI: 1.43-2.17) at 3.5 years, but less likely to be within target for BMI (OR: 0.63, 95% CI: 0.50-0.79). Increasing age was positively associated with being within target for total (OR: 1.24, 95% CI: 1.08-1.43) and LDL cholesterol (OR: 1.17, 95% CI: 1.02-1.34), BMI (OR: 1.59, 95% CI: 1.41-1.79) and waist circumference (OR: 1.16, 95% CI: 1.04-1.28), but negatively associated with being within target for SBP (OR: 0.79, 95% CI: 0.72-0.88) and exercise (OR: 0.77, 95% CI: 0.69-0.85).
Medication prescription
Medication usage at baseline (by cohort) and 1, 2, 3 and 3.5 years
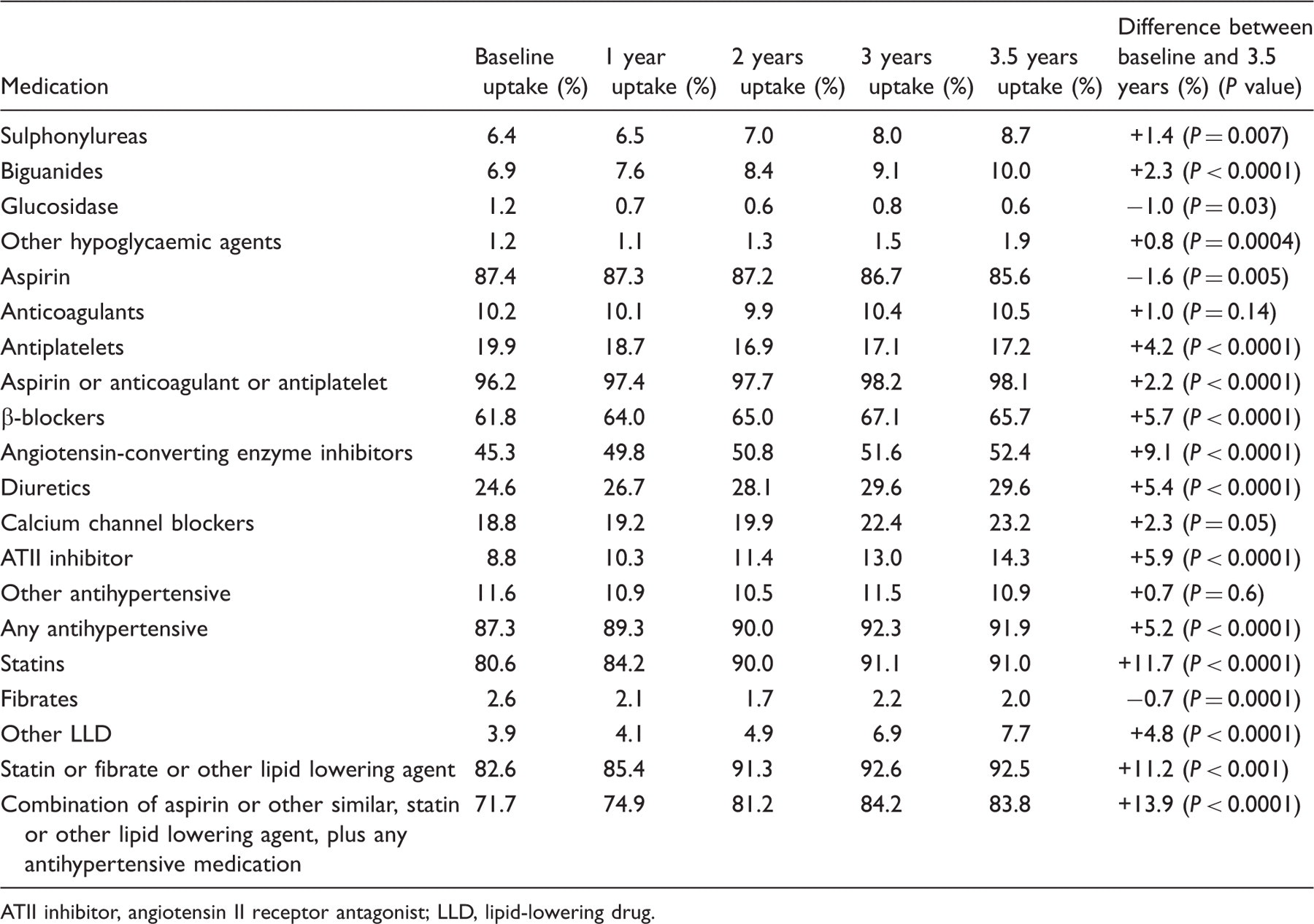
ATII inhibitor, angiotensin II receptor antagonist; LLD, lipid-lowering drug.
Discussion
This analysis of the Heartwatch programme shows sustained improvement in the main modifiable CHD risk factors and a high level of prescription of secondary preventive medications over a follow-up period of 3.5 years. This is an important finding in the context of the documented inadequacy of integration of cardiovascular disease prevention into daily clinical practice in repeated Euroaspire surveys. 11,12 The third Euroaspire survey showed an increase in antihypertensive and lipid-lowering drugs, but despite this, BP management remained unchanged and almost 50% had high lipid levels. 12
The biggest change observed were in those risk factors where prescribed medication can be used, that is, smoking, SBP and DBP, LDL and total cholesterol levels. There was little improvement in BMI and waist circumference, despite the improvement seen in reported physical activity. It is known that patients with CHD have varying levels of adherence to risk factor management. 13,14 Adherence to medication is best, but diet and weight loss interventions have poor adherence. A community-based programme such as Heartwatch gives the opportunity for monitoring of adherence over a protracted period to optimize risk factors to prevent subsequent cardiovascular events. However, despite monitoring, weight loss proved a challenge, with a modest and nonsustained reduction in weight; women had greater success than men. Evaluation of the implementation of agreed strategy in regular clinical practice is important, as issues in the design of randomized trials may lead to a dilution or magnification of treatment effect. 15 Weight management was shown to be a challenge in the GOSPEL Trial of post-MI prevention; both the study groups showed increased BMI. 16
As patients were recruited to Heartwatch some time after their initial cardiac event, it is likely they would have already had secondary prevention implemented to some extent. Therefore the amount of improvement achievable through a programme like this is likely to be additive and thus less than might be seen if it represented the first implementation of secondary prevention.
Continued prescription and self-reported adherence to medication was good. Patients who adhere to a statin post-MI have a relative risk of recurrence 80% lower than that of nonadherent patients. 17 Post-MI patients who discontinue their prescribed aspirin, statin and b-blocker are over three times more likely to die than those who adhere. Health care costs are also lower among adherent patients, which may offset some of the costs incurred in secondary prevention programmes. However, adherence rates have been found to be poor post-MI with usual care. 18 It is recognized that sustained long-term treatment usually follows a successful negotiation between patient and GP; 19 this seems to be have been achieved by most patients in Heart watch.
Males were more likely to be within the target at 3.5 years for SBP and cholesterol; this may reflect more aggressive treatment in males, which has been recognized earlier. 20 UK data suggest a systematic bias towards men compared with women in secondary prevention of CHD. 21 The Aspire studies found inequalities, with substantial gradients disadvantaging women and older patients. 11,12 Although in this study males were more likely to be within the target for waist circumference and exercise, females were more likely to be within the target for BMI. Younger patients were more likely to be within the target for SBP and exercise, but increasing age was significantly associated with being within the target for BMI, waist circumference and cholesterol. The benefits of careful management of hypertension in older patients have been clearly shown, 22 yet despite this, both in this and other studies, 23 management of hypertension remains more rigorous in younger patients.
Heartwatch was not designed as a randomized controlled trial, but as a demonstration project. The analysis is a ‘before—after’ design, capturing changes within individual patients after implementation of the programme. Heartwatch has captured health care in practice, which makes it generalizable to a wider population than a randomized controlled trial. 24 Some evidence that the structured programme achieved more than expected without the programme exists. Heartwatch GPs significantly increased prescribing of preventive therapies among all patients, beyond that expected from underlying trends. 10
In general, it is considered that risk factor control in patients with established CHD remains poor with routine care paths alone. Studies of cardiac rehabilitation without follow-up show that over time patients revert in part to previous lifestyle habits. 13,14,25 Although not achieving improvement across all risk factor profiles and weight management remaining a challenge, the Heartwatch programme goes some way to answer the need for implementation in primary care of effective actions in an organized fashion with sustained benefit.
Footnotes
Acknowledgements
The authors thank the Irish College of General Practitioners, the Independent National Data Centre and all involved with the Heartwatch Programme. This study was supported by funds received from Health Research Board and Irish Heart Foundation.