
Abstract
Background
Accumulating evidence shows that gradual loss of white matter integrity plays an important role in the development of Alzheimer disease (AD).
Objective
The aim of this research was to study the microstructural integrity of white matter in AD in vivo.
Methods
Global fractional anisotropy, global axial diffusivity (AxD), and global radial diffusivity (RD) were analyzed in subjects with normal controls (NC), mild cognitive impairment (MCI), and AD using Alzheimer's Disease Neuroimaging Initiative data (total N = 210). We further compared specific white matter tracts among the 3 groups.
Results
Compared with the NC group, the MCI group had significantly increased global AxD and global RD. Compared with the NC and MCI groups, the AD group had significantly decreased global fractional anisotropy, increased global AxD, and increased global RD. With regard to specific white matter tracts, in the MCI group, we found increased AxD and increased RD in the external capsule, part of the lateral cholinergic pathway, in addition to the tracts connecting the limbic regions, predominantly in the left hemisphere. In the AD group, white matter abnormalities were widespread, including in the external capsule (cholinergic pathway) and limbic region tracts as well as tracts connecting anterior to posterior regions bilaterally.
Conclusions
The radiographic manifestation of damaged white matter microstructural integrity in the cholinergic pathway in MCI patients may provide a rational basis for the use of cholinesterase inhibitor drugs in the MCI stage of AD.
Keywords
Accumulating evidence shows that the gradual loss of morphological and functional integrity of both gray and white matters is evident in brain imaging in the development of Alzheimer disease (AD).1,2 To dissect the pathophysiological process of AD in vivo, it is necessary to investigate the evolution of anatomic microstructural changes in the brains of AD patients via neuroimaging techniques.
Gray matter atrophy, particularly in vivo hippocampal atrophy, has been extensively characterized in AD patients via magnetic resonance imaging (MRI). In addition, few studies report a significant volume reduction in the cholinergic nuclei of the basal forebrain in the mild cognitive impairment (MCI) and AD patients.3,4 These gray matter changes are closely associated with the clinical presentation of AD dementia.5,6 However, in vivo white matter changes in these brain region tracts have been less extensively characterized.6,7
There is increasing evidence that white matter pathology plays an important role in the development of AD dementia.8–10 Because gray matter atrophy and white matter changes are typically found together radiographically in AD dementia, it has been suggested that white matter damage may secondarily result from neuronal loss. 11 In addition, white matter lesions are found independently from atrophic gray matter regions in patients with MCI and AD. This indicates that neurodegeneration may begin in axons and dendrites.11–14 Given these findings, it is important to explore the role of white matter lesions in the pathogenesis of AD.
Diffusion tensor imaging (DTI) has proven to be a powerful tool to investigate the microstructural integrity of white matter. 15 Fractional anisotropy (FA) and mean diffusivity (MD) are 2 measures of DTI that detect summative directional and random diffusion of water molecules in brain tissue. Component analysis of the diffusion tensor parallel to (axial diffusivity, AxD) and perpendicular to (radial diffusivity, RD) the principal diffusion direction provides more detailed information about white matter tract microstructure. 16 Decreased FA, increased AxD, and increased RD have been reported in selected brain regions in patients with MCI and AD.6,16–19 However, global microstructural changes of white matter are still under investigation in these patients. 20 Studying the process of white matter disruption in MCI and probable mild AD due to AD pathophysiology will increase our understanding of the mechanisms underlying patients’ clinical symptoms as they progress from MCI to AD dementia.
In this study, we investigated how whole-brain white matter microstructural integrity differs among normal controls (NCs) and MCI and AD patients by comparing global FA, AxD, and RD measurements reported in the Alzheimer's Disease Neuroimaging Initiative (ADNI) database. We compared the regional FA, AxD, and RD of 52 tracts of NCs with those of the MCI group and with those of the AD group. On the basis of these comparative analyses, we formulated conclusions about the radiographic manifestation of clinical progression from MCI to mild AD dementia, as a probable evolution of DTI findings from decreased regional microstructural integrity in specific white matter tracts to globally reduced microstructural integrity.
To our knowledge, this study is the largest sample size to date of DTI investigations of MCI and AD dementia. Our study confirms previously described anatomic locations of cerebral white matter abnormalities in MCI and AD dementia. Furthermore, our study extends previous in vivo findings of cholinergic tract abnormalities in MCI and mild AD dementia by demonstrating DTI abnormalities of the external capsule, through which the lateral cholinergic pathway travels. Accumulating evidence of disrupted cholinergic pathway white matter tracts in MCI may provide a rational basis for the use of cholinesterase inhibitor therapy in the MCI stage of AD.
Materials and Methods
Adni Study
Data used in this study were obtained from the ADNI database (adni.loni.usc.edu). The ADNI was launched in 2003 by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, the Food and Drug Administration, private pharmaceutical companies, and nonprofit organizations. The primary goal of ADNI has been to test whether serial MRI, positron emission tomography, other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of MCI and early AD. The principal investigator of this initiative is Michael W. Weiner, MD. 21 The ADNI is the result of efforts of many co-investigators from a broad range of academic institutions and private corporations, and subjects have been recruited from more than 50 sites across the United States and Canada. To date, more than 1500 adults, aged 55 to 90 years, have been recruited, consisting of cognitively healthy older individuals, people with early or late MCI, and people with early AD (for up-to-date information, see www.adni-info.org). In our study, every subject with an initial analysis of DTI data including FA, AxD, and RD was included in this study. Institutional review board approval is obtained at each ADNI site, and informed consent is obtained from each participant or authorized representative. Demographic information was extracted from the ADNI database. There were 60 NCs, 106 MCI subjects, and 44 mild AD subjects.
Image Process and Analysis
The DTI acquisition and analysis were described by Nir et al. 22 All subjects underwent whole-brain MRI scanning on 3-Tesla GE Medical Systems scanner at 14 acquisition sites across North America. Anatomical T1-weighted sequences and diffusion weighted images were collected. According to the described preprocessing protocol, head motion and eddy current distortions were corrected. All extracerebral tissues were removed from the T1-weighted anatomical scans. Anatomical scans subsequently underwent intensity inhomogeneity normalization. More details of the preprocessing steps are described by Nir et al. 22
The FA images from the Johns Hopkins University DTI atlas were registered for each subject based on an elastic registration algorithm. 23 The FA, a measure of the degree of diffusion anisotropy, was calculated from the standard formula. The AxD was defined as the primary (largest) eigenvalue (AxD = λ1) and captures the longitudinal diffusivity or the diffusivity parallel to axonal fibers. The RD, which captures the mean diffusivity perpendicular to axonal fibers, was calculated as the mean of the 2 smaller eigenvalues. Tract-based spatial statistics were performed according to the Functional Magnetic Resonance Imaging of the Brain Software Library software package and protocols outlined by the ENIGMA-DTI group.22,24
Statistics
Repeated measures analysis of variance (ANOVA) was performed to compare the global differences across the 3 groups, with follow-up post hoc analyses performed as needed to explain the main effects and interactions. A general linear model with multivariate ANOVA (MANOVA) with post hoc test Bonferroni correction was performed to compare the FA, AxD, and RD of each tract between the groups. P ≤ 0.05 is considered to indicate a statistically significant difference between groups. SPSS (version 20; SPSS Inc., Cary, NC) was used for this statistical analysis.
Results
Demographic Information of Study Population
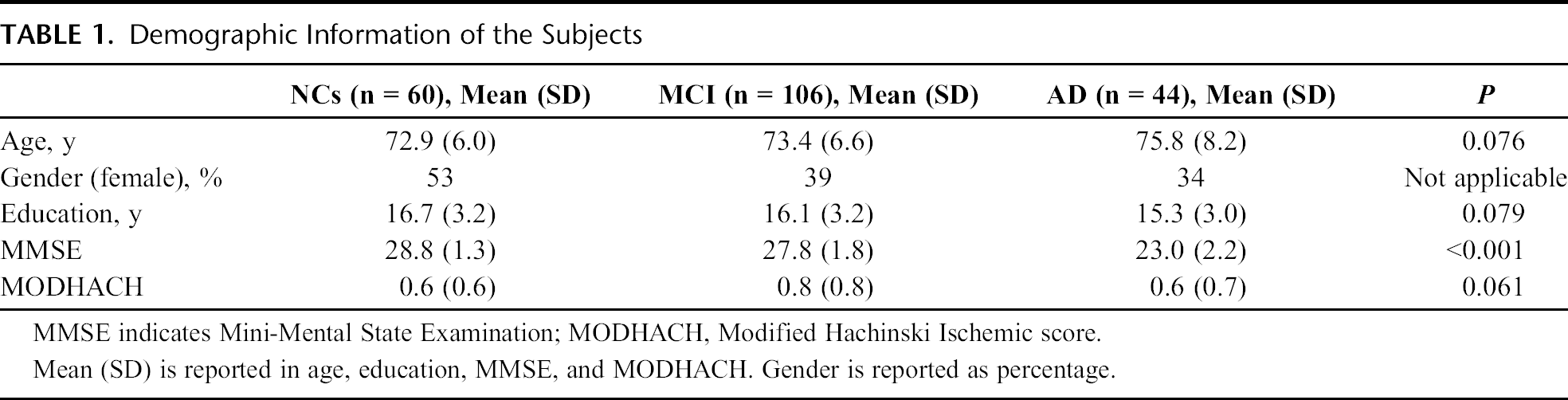
Table 1 shows the demographic information of the subjects. There were no significant differences in age, Modified Hachinski score, and education across the 3 groups. As expected, there was a significant difference in Mini-Mental Status Examination (MMSE) scores across the 3 groups, F(2,207) = 150.07, P < 0.001, η2 = 0.769. The mean MMSE score in the patients with AD was 23, consistent with mild AD dementia.
Demographic Information of the Subjects
Global Decreased FA, Increased AxD, and Increased RD in MCI and AD Patients Compared with Controls
Figure 1A shows the comparison of global FA among the NCs, MCI patients, and AD patients. There was a significant difference in global FA across the 3 groups, F(2,207) = 10.67, P < 0.001, η2 = 0.093. Post hoc analysis showed that global FA was significantly decreased in the AD group compared with the NCs and the MCI group (P < 0.001 and P = 0.002). There was no significant difference in global FA between the controls and the MCI patients (P = 0.162).
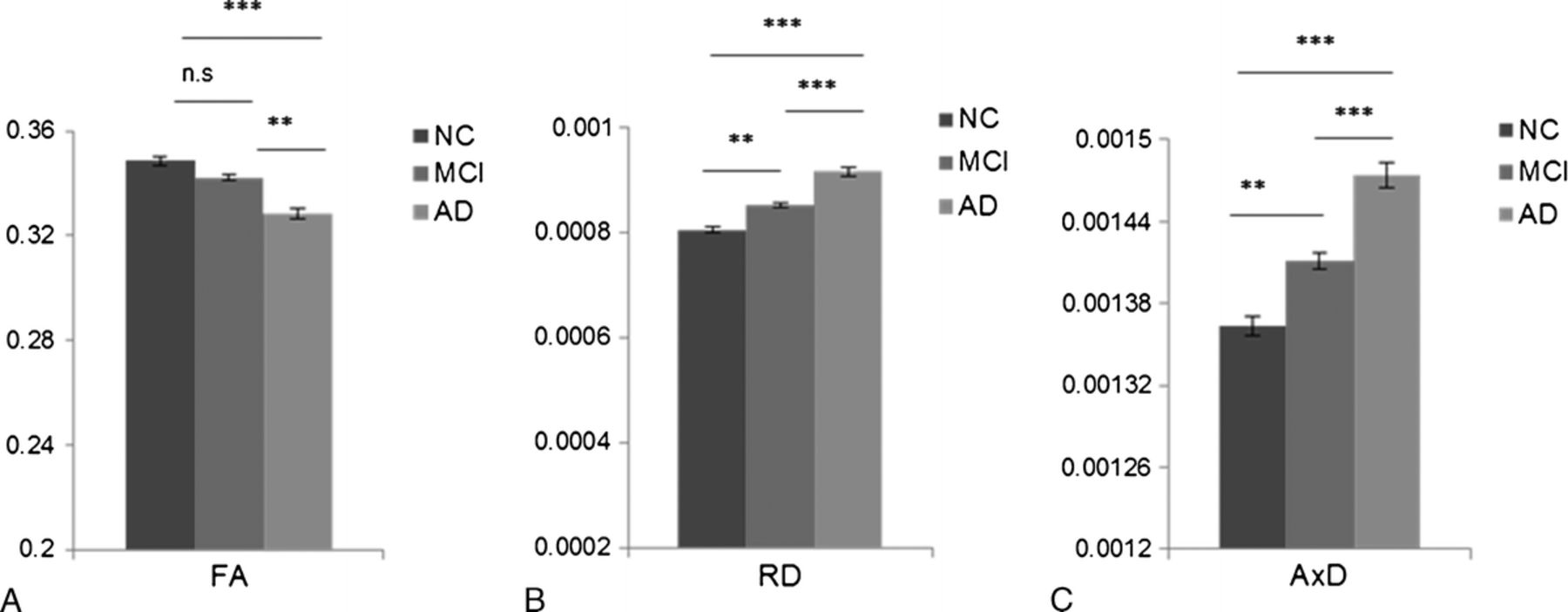
Significantly decreased global FA, increased global RD, and global AxD in the MCI and AD patients compared with the NCs. Comparison of global FA, RD, and AxD among the 3 groups. A, Global FA is significantly reduced in the AD group compared with the NC and MCI groups. No significant difference of FA between the NC and MCI groups is observed. B, Global RD is significantly increased in the AD and MCI groups compared with the NC group. C, The global AxD is significantly increased in the AD and MCI groups compared with the NC group. Error bar represents mean (SEM).
Figure 1B shows the comparison of global RD among the 3 groups. There was a significant difference in global RD across the 3 groups, F(2,207) = 16.25, P < 0.001, η2 = 0.136. Post hoc analysis showed that global RD was significantly increased in the AD group compared with the NCs and the MCI group (P < 0.001 and P = 0.001). There was a significant difference in global RD between the controls and the MCI patients (P = 0.012).
Figure 1C shows the comparison of global AxD among the 3 groups. There was a significant difference in global AxD across the 3 groups, F(2,207) = 16.85, P < 0.001, η2 = 0.140. Post hoc analysis showed that global AxD was significantly increased in the AD group compared with the NCs and the MCI group (P < 0.001 and P = 0.001). There was a significant difference in global AxD between the controls and the MCI patients (P = 0.009).
Gradual Loss of White Matter Microstructural Integrity in the MCI and AD Patients Compared with Controls
Next, a linear model of MANOVA was conducted to compare differences in the regional FA, RD, and AxD of 52 specific axonal tracts across the 3 groups.
Decreased FA in the MCI and AD Patients
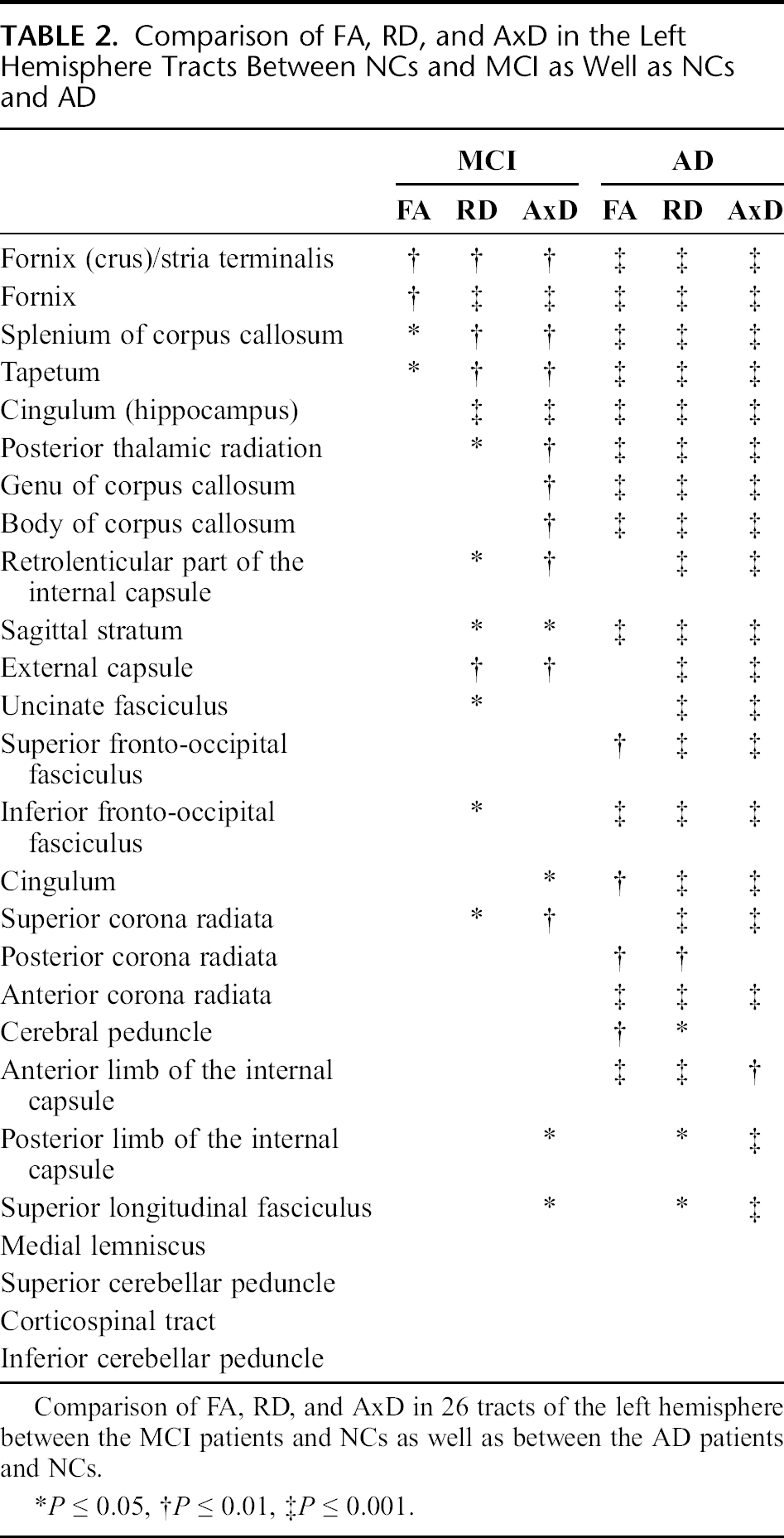
A MANOVA revealed a significant multivariate main effect in FA for the diagnosis (normal vs MCI vs AD), Pillai trace = 0.67, F(104, 314) = 1.525, P = 0.003, η2 = 0.336. The post hoc tests were performed to compare the regional FA of each specific axonal tract between NCs and MCI patients as well as between the NC and AD groups (Tables 2 and 3).
Comparison of FA, RD, and AxD in the Left Hemisphere Tracts Between NCs and MCI as Well as NCs and AD
Comparison of FA, RD, and AxD in the Right Hemisphere Tracts Between NCs and MCI as Well as NCs and AD
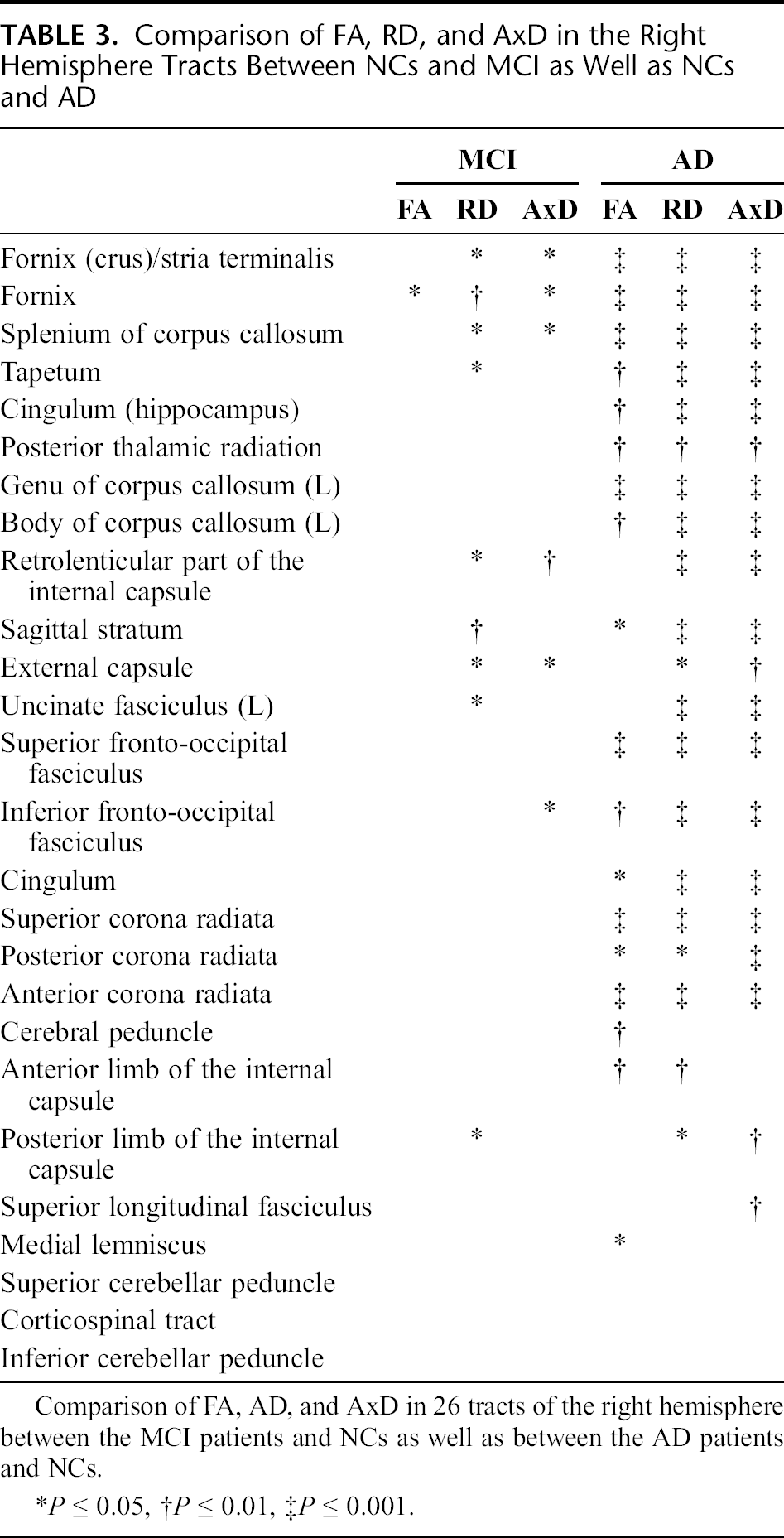
In the MCI patients, we found significantly decreased regional FA in a few specific tracts: bilateral fornices, left tapetum, left fornix (crus)/stria terminalis, and left splenium of corpus callosum. In contrast, in the AD patients, we found widespread destruction of white matter microstructural integrity in multiple specific tracts. Compared with the NCs, FA is significantly decreased in the AD patients in the following bilateral tracts: tapetum, fornix (crus)/stria terminalis, fornix, splenium of corpus callosum, genu of corpus callosum, body of corpus callosum, cingulum (hippocampus), cingulum, anterior corona radiata, posterior thalamic radiation, superior fronto-occipital fasciculus, inferior fronto-occipital fasciculus, cerebral peduncle, sagittal striatum, and anterior limb of the internal capsule. The FA was also significantly decreased in the AD in the right medial lemniscus.
Increased RD in the MCI and AD Patients
A MANOVA revealed a significant multivariate main effect for the diagnosis (normal vs MCI vs AD) in RD, Pillai trace = 0.67, F(104, 314) = 1.529, P = 0.003, η2 = 0.336. The post hoc tests were performed to compare the regional RD of each specific axonal tract between NCs and MCI patients as well as between the NC and AD groups (Tables 2 and 3).
In the MCI patients, we found significantly increased regional RD in the following specific tracts: bilateral tapetum, bilateral fornix (crus)/stria terminalis, bilateral fornices, bilateral splenium of corpus callosum, bilateral retrolenticular part of the internal capsule, bilateral external capsule (Fig. 2), bilateral uncinate fasciculus, the left cingulum (hippocampus), left sagittal stratum, left posterior thalamic radiation, the left inferior fronto-occipital fasciculus, left superior corona radiata, and right posterior limb of the internal capsule.
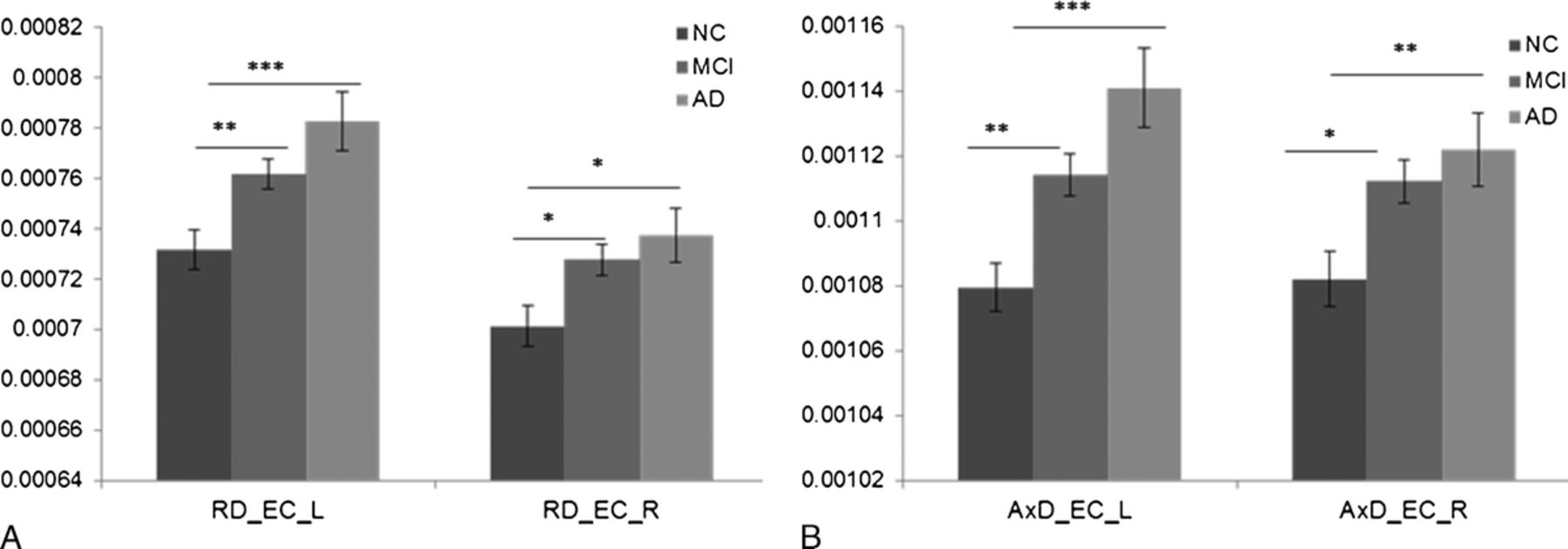
Increased RD and AxD of the external capsule (EC) in the MCI and AD patients compared with the NCs. A, Comparison of RD of the left and right external capsule between the MCI patients and NCs as well as between the AD patients and NCs. B, Comparison of AxD of the left and right EC between the MCI patients and NCs as well as between the AD patients and NCs. Error bar represents mean (SEM).
In the AD patients, compared with the NCs, RD was significantly increased in the following bilateral tracts: tapetum, fornix (crus)/stria terminalis, fornix, splenium of corpus callosum, genu of corpus callosum, body of corpus callosum, cingulum (hippocampus), cingulum, anterior corona radiata, superior fronto-occipital fasciculus, inferior fronto-occipital fasciculus, superior corona radiata posterior corona radiata, posterior thalamic radiation, sagittal striatum, anterior limb of the internal capsule, bilateral external capsule (Fig. 2), and posterior limb of the internal capsule. The RD was also significantly increased in the AD patients in the following unilateral tracts: left cerebral peduncle and left superior longitudinal fasciculus.
Increased AxD in the MCI and AD Patients
A MANOVA revealed a significant multivariate main effect in AxD for the diagnosis (MCI vs AD), Pillai trace = 0.62, F(104, 314) = 1.377, P = 0.019, η2 = 0.313. The post hoc tests were performed to compare the regional AxD of each specific axonal tract between NCs and MCI patients as well as between the NC and AD dementia groups (Tables 2 and 3).
In the MCI patients, we found significantly increased regional AxD in these tracts: bilateral fornix (crus)/stria terminalis, bilateral fornices, bilateral splenium of corpus callosum, bilateral retrolenticular part of the internal capsule, bilateral external capsule (Fig. 2), bilateral sagittal stratum, left tapetum, left cingulum (hippocampus), left superior longitudinal fasciculus, left posterior thalamic radiation, left body of corpus callosum, left genu of corpus callosum, left tapetum, left superior corona radiata, left posterior limb of the internal capsule, and right inferior fronto-occipital fasciculus.
In the AD patients, compared with the NCs, AxD was significantly increased in these bilateral tracts: tapetum, fornix (crus)/stria terminalis, fornices, splenium of corpus callosum, genu of corpus callosum, body of corpus callosum, cingulum (hippocampus), cingulum, anterior corona radiata, superior corona radiata, posterior corona radiata, superior fronto-occipital fasciculus, inferior fronto-occipital fasciculus, posterior thalamic radiation, sagittal striatum, posterior limb of the internal capsule, retrolenticular part of the internal capsule, bilateral external capsule (Fig. 2), and uncinate fasciculus. The AxD was also significantly increased in the AD patients in the left posterior limb of the internal capsule.
Discussion
Although postmortem studies of white matter changes in AD have been reported for decades,25–28 investigation of white matter microstructure in vivo only became possible after the development of DTI. 19 Many studies using DTI have focused on changes in white matter in selected brain regions rather than on the global microstructural integrity of cerebral white matter.29–32 Studying white matter disruption in MCI and AD dementia may advance our understanding of the mechanisms underlying patients’ clinical symptoms as a subset progresses from MCI to AD.
In this study, we report decreased global FA, increased global RD, and increased global AxD in AD dementia patients compared with MCI patients and NCs, using ADNI data. We did not find a significant decrease in global FA in MCI patients compared with NCs, consistent with previous findings. 20 With regard to diffusivity, increased global RD and global AxD were readily found in MCI patients compared with controls in our study. One possible explanation is that FA is a less sensitive method for the detection of early AD pathology, as reported by other studies.17,22 However, our results can also be interpreted as clinically meaningful. The reduced global FA of white matter in AD dementia patients may be the radiographic representation of dementia. In line with this interpretation, a significant correlation between measures of white matter abnormality and dementia severity has been reported by others. Our results, along with those of other investigators, suggest that it may be possible to use quantitative radiographic measures of white matter destruction as surrogate markers for monitoring the clinical progression of AD.33,34
In this study, we also investigated DTI measures of specific white matter tracts in AD dementia and MCI. Our study extends previous in vivo findings of cholinergic tract white matter abnormalities in MCI and AD dementia.3,4,35–38 To our knowledge, this is the first report of increased RD and AxD in the external capsule in MCI and AD dementia patients. The external capsule and uncinate fasciculus comprise the capsular division of the lateral cholinergic pathway. The capsular division of the lateral cholinergic pathway innervates frontal, parietal, and temporal neocortices. 39 The finding of damage in the lateral cholinergic pathway in MCI and AD dementia is consistent with AD pathology, given that degeneration of cholinergic neurons of the basal forebrain is a distinctive neuropathological feature of AD.
Evidence of damage to the cholinergic pathway in MCI patients is supportive of early medical intervention with cholinesterase inhibitors in the MCI stage of AD in clinical practice. In Likitjaroen and colleagues’ 40 longitudinal randomized, placebo-controlled, double-blinded study of AD patients treated with the cholinesterase inhibitor galantamine, increased FA was found in AD dementia patients after 6 months of treatment with galantamine. In contrast, the AD dementia patients who received placebo had decreased FA in the posterior part of corpus callosum at the 6-month point of the study. 41 Such findings suggest that DTI measurements such as RD and AxD could potentially be used to monitor AD patients’ response to treatment with cholinesterase inhibitors.
Congruent with previously published studies, in the MCI patients, we found decreased FA, increased RD, and increased AxD in association fibers and commissural fibers involving the corpus callosum, hippocampus, and amygdala. White matter tracts associated with the hippocampus and the amygdala form part of the Papez circuit,42,43 and damage to the Papez circuit is known to be linked to episodic memory impairment. 44 Therefore, the in vivo radiographic finding of reduced FA and increased diffusivity in specific white matter tracts associated with the Papez circuit is consistent with the clinical presentation of MCI due to the AD pathophysiologic process.
In addition, our finding of reduced FA and increased diffusivity in the splenium of the corpus callosum in MCI patients is consistent with the postulation that the pathophysiological process of AD is partially a disconnection syndrome. 45 In AD dementia patients, we found widespread reduced FA and increased diffusivity, indicating a general disruption of connectivity not seen in the MCI patients. Disconnection of neuroanatomic structures due to damaged white matter tracts may be one of the mechanisms underlying the clinical presentation of the initial stage of AD. 46
In this study, we observed the following pattern of damaged white matter tracts in AD: (1) in both the MCI and AD dementia patients, when the damage to white matter tracts is unilateral, the damaged tracts are more often in the left hemisphere than in the right. Of relevance to this finding, Thompson and colleagues 47 demonstrated that gray matter loss in AD is more prominent in the left hemisphere than in the right. (2) Damaged white matter tracts are limited primarily to the limbic region in the MCI patients, in contrast to the AD dementia patients, in whom damaged white matter tracts extend from the limbic region to the thalamic and cortical regions, consistent with the results of other published studies. 19 (3) In the MCI patients, damaged white matter tracts are found primarily in posterior brain regions, whereas in the AD dementia patients, they are also found in the anterior and lateral brain regions. (4) Regarding fiber classification, association fibers and commissural fibers are damaged in the MCI patients, whereas in the AD dementia patients, there are also abnormalities in some projection fibers. All together, this anatomic pattern of white matter changes measured by FA and directional diffusivity may represent a temporal clinical progression from predementia to dementia in AD.48,49
The limitations of our study include the following. First, because this is a cross-sectional study, we are not able to use DTI to elucidate dynamic changes in AD progression, and the role of DTI in predicting disease evolution remains unknown. Second, in this study, we do not have data showing the relationship between white matter and gray matter in cerebral regions affected in AD. Further study of the relationship between white matter and gray matter changes could provide insights into the mechanisms of neurodegeneration underlying clinical manifestations of the AD pathophysiologic process. Understanding the role of damaged white matter in the development of AD clinically and pathophysiologically may lead to the identification of new targets for treatment.