
Abstract
Background
Recent studies suggest an important role for leptin in respiratory immune responses and pathogenesis of inflammatory respiratory diseases. There has been an interest to explore whether leptin plays any role in the pathogenesis of chronic obstructive pulmonary disease (COPD).
Objective
We conducted a population-based study to evaluate the relationship between serum leptin and COPD in the third US National Health and Nutrition Examination Survey participants.
Participants and Design
Our study group was constituted by 6415 adults who had fasting serum leptin and underwent spirometry measurement.
Main Outcome Measures
Serum leptin levels were compared (1) between subjects with normal lung function and those with COPD and (2) among COPD subjects with different severities.
Results
Among male participants, 2257 were controls, and 680 had COPD. Compared with controls, COPD subjects were older (62 vs 43 years) and had higher prevalence of smokers (78% vs 58%), lower body mass index (BMI) (26.3 vs 26.9), and higher serum leptin levels (6.6 vs 5.9). For female participants, 2918 were controls, and 560 had COPD. Those with COPD were older (60 vs 43 years) and had lower BMI (26.9 vs 27.7). No differences in serum leptin levels were observed. The independent predictors of COPD in both sexes were age, BMI, and smoking, but not serum leptin. There were no differences in serum leptin among COPD subjects with different severities.
Conclusions
We did not find any significant difference in the levels of serum leptin in subjects with COPD. Our data provide indirect evidence against a major role for serum leptin in the pathogenesis of COPD in humans.
Keywords
Chronic obstructive pulmonary disease (COPD) is characterized by airflow obstruction that is not fully reversible and is associated with an abnormal inflammatory response of the lungs to noxious particles or gases, notably cigarette smoke. 1 The COPD is one of the major causes of morbidity and mortality and will represent the third leading cause of death worldwide by the next decade. 2 Recent studies suggested that COPD is not only the pulmonary disease, but in fact, it might be the consequences of systemic inflammatory process. 3 The COPD is associated with inflammatory reactions primarily in the terminal portions of the airways, as reflected by increase in neutrophils, macrophages, and lymphocytes in the airway lumens and parenchyma. 4
Leptin is an adipocyte-derived hormone and is now known to have pleiotropic functions. Leptin is a primarily proinflammatory adipokine that affects both innate and adaptive immune responses. It is expressed by the human lung, including bronchial epithelial cells and alveolar type II pneumocytes and macrophages. 5 A study in rodent suggested that leptin differentially affects airway innate and adaptive immune responses in mice after cigarette smoke exposure 6 and that leptin receptor activation is important in regulating the cigarette smoke-induced inflammatory response in the lung. 7 Several investigators have explored the association between serum leptin and COPD in humans, but these have yielded mixed results.8–10 In this study, we conducted the population-based study using the data from the Third National Health and Nutrition Examination Survey (NHANES III) to explore the relationship between serum leptin and COPD.
Methods
The NHANES III was conducted in the United States from 1988 through 1994 by the National Center for Health Statistics of the Centers for Disease Control and Prevention. This survey was designed to collect information about the health and diet of people in the United States. The NHANES III used complex, multistage, stratified, clustered samples of civilian, noninstitutionalized populations 2 months and older. A detailed description of the survey and its sampling procedures are available at http://www.cdc.gov/nchs/nhanes/nh3data.htm#1.
Study Cohort and Definitions
As part of the survey, 6415 participants older than 20 years were randomly assigned for survey and examination in the morning after an overnight fast. Serum leptin levels were measured in all of these participants. They also underwent spirometry measurement at the mobile examination center as part of the physical examination.
Subjects were considered to be hypertensive if they were taking antihypertensive medications or if their systolic pressure is 130 mm Hg or greater or diastolic pressure is 85 mm Hg or greater. 11 Personal cigarette smoking was determined using standard questions during the survey. In this report, previous smoking was defined as a positive answer to the question, “Have you smoked at least 100 cigarettes during your entire life?”.
Mean alcohol consumption was calculated based on the responses to 2 survey questions that queried about the number of days of drinking during the past 12 months and the number of drinks per day on a given drinking day. For this study purpose, the participants with reported mean daily alcohol consumption of greater than 1 drink in women and greater than 2 drinks in men were considered to have significant alcohol consumption. 12
On the basis of the spirometry results, we used the Global Initiative for Chronic Obstructive Lung Disease classification to create the following categories: severe COPD (FEV1/FVC < 0.70 and FEV1 < 50% predicted), moderate COPD (FEV1/FVC < 0.70 and FEV1 of 50% to <80% predicted), mild COPD (FEV1/FVC < 0.70 and FEV1 ≥ 80% predicted), and normal lung function or controls (FEV1/FVC ≥ 0.70). 13 We used the spirometric reference values as described by Hankinson et al. 14 to calculate %predicted FEV1 for each subject.
Laboratory Measurements
The laboratory procedures followed in the NHANES III are described in detail elsewhere. 15 All venous blood samples were immediately centrifuged and shipped weekly at −20°C to a central laboratory. Serum leptin levels were measured by a radioimmunoassay with a polyclonal antibody raised in rabbits against highly purified recombinant human leptin (Linco Research, Inc, St Louis, MO). The minimum detectable concentration for this assay was 0.5 ng/mL.
Statistical Analysis
All statistical analyses were performed using SAS software for Windows version 9.3 (SAS Institute, Cary, NC). Basic descriptive statistics, including means, SDs, ranges, and percentages, were used to characterize the study patients. Comparisons between groups were made using Student t test or analysis of variance for the continuous variables and χ2 test for the categorical variables. Univariate logistic regression was performed, and those variables with P < 0.05 were entered in the multivariate logistic regression models to identify independent predictors of COPD. Strength of association is reported as adjusted odds ratio (OR) with 95% confidence interval and P value. P < 0.05 was considered statistically significant.
Results
Comparison between Patients with Normal Lung Function and COPD in Male Participants
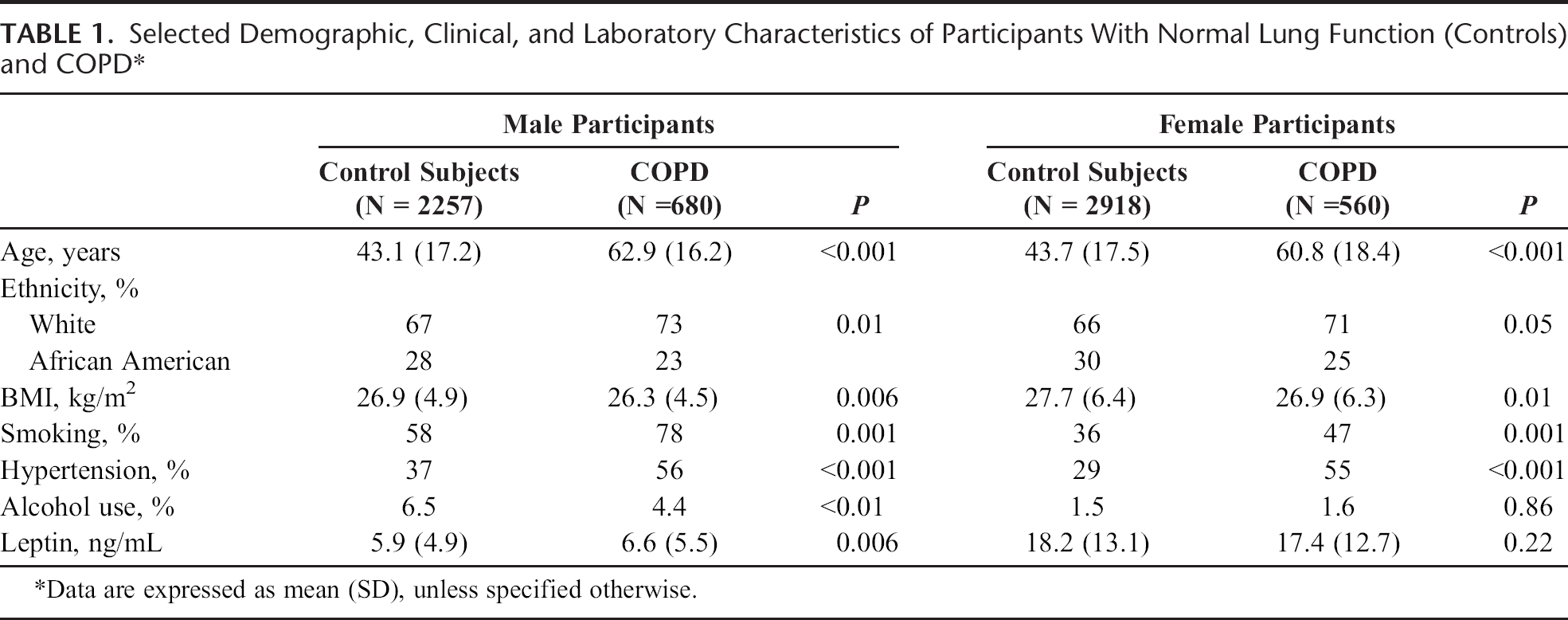
This analysis consisted of 2937 subjects. Of these, 2257 were controls, and 680 had COPD. Selected demographic and laboratory data were shown in Table 1. Compared with controls, as expected, individuals with COPD were older (62.9 vs 43.1 years, P < 0.001), had significantly higher prevalence of smoking (78% vs 58%, P = 0.001), and had hypertension (56% vs 37%, P < 0.001). However, we observed that male subjects with COPD had lower body mass index (BMI) (26.3 vs 26.9, P = 0.006) and lower prevalence of alcohol drinking (4.4 vs 6.5, P < 0.01). Serum leptin in male COPD subjects was significantly higher than in controls (6.6 vs 5.9 ng/mL, P = 0.006).
Selected Demographic, Clinical, and Laboratory Characteristics of Participants With Normal Lung Function (Controls) and COPD*
Comparison between Patients with Normal Lung Function and COPD in Female Participants
This analysis consisted of 3478 subjects. Of these, 2918 were controls, and 560 had COPD. Selected demographic and laboratory data were shown in Table 1. Compared with controls, female subjects with COPD were older (60.8 vs 43.7 years, P < 0.001) and had significantly higher prevalence of hypertension (55% vs 29%, P < 0.001), higher prevalence of smoking (47% vs 36%, P = 0.001), and lower BMI (26.9 vs 27.7, P = 0.01). There was no difference in the prevalence of alcohol use (1.6% vs 1.5%, P = 0.86) and serum leptin levels (17.4 vs 18.2 ng/mL, P = 0.22) between these 2 groups.
Predictors of COPD in Male Participants
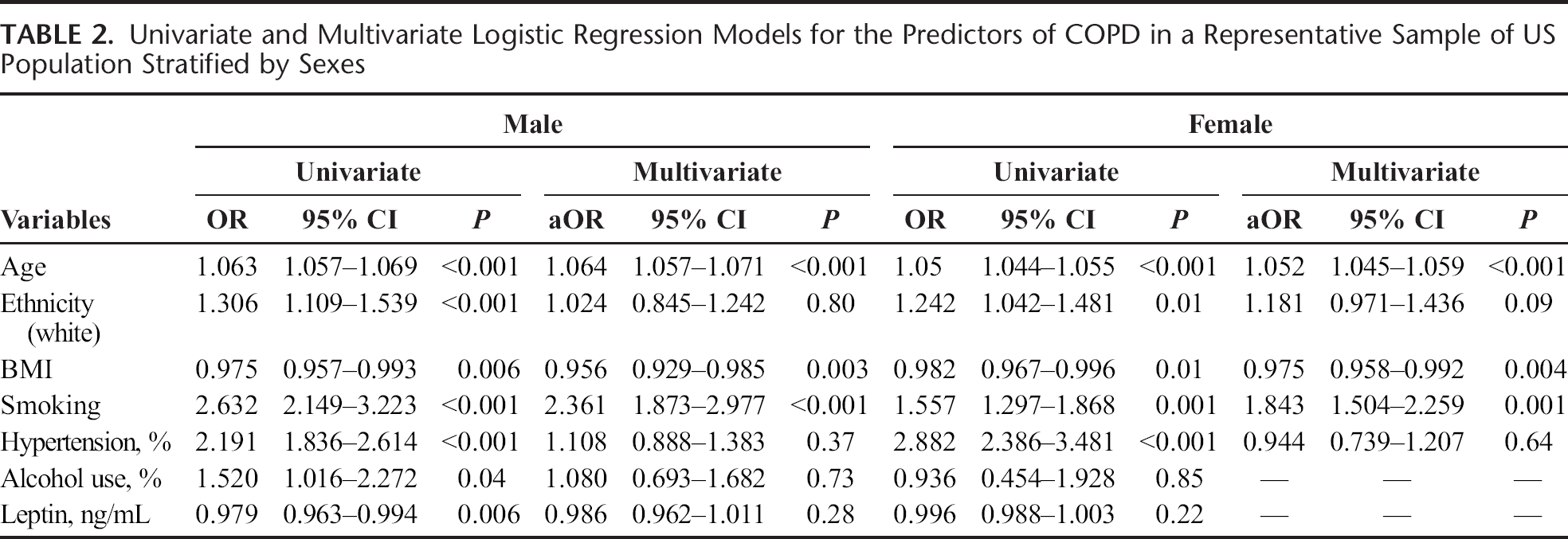
We performed the logistic regression analysis to evaluate the independent predictors of COPD. The results of univariate and multivariate analyses are shown in Table 2. In the univariate analysis, age (OR, 1.063; 95% confidence interval [CI], 1.057–1.069), being white (OR, 1.306; 95% CI, 1.109–1.539), BMI (OR, 0.975; 95% CI, 0.957–0.993), smoking (OR, 2.632; 95% CI, 2.149–3.223), hypertension (OR, 2.191; 95% CI, 1.836–2.614), alcohol use (OR, 1.520; 95% CI, 1.016–2.272), and serum leptin (OR, 1.022; 95% CI, 1.006–1.038) were associated with COPD. However, after adjusting for covariates in the multivariate analysis, only age (adjusted OR [aOR], 1.06; 95% CI, 1.057–1.071), BMI (aOR, 0.956; 95% CI, 0.929–0.985), and smoking (aOR, 2.361; 95% CI, 1.873–2.977) were independent predictors of COPD in male participants.
Univariate and Multivariate Logistic Regression Models for the Predictors of COPD in a Representative Sample of US Population Stratified by Sexes
Predictors of COPD in Female Participants
For female participants, age (OR, 1.05; 95% CI, 1.044–1.055), being white (OR, 1.242; 95% CI, 1.042–1.481), BMI (OR, 0.982; 95% CI, 0.967–0.996), smoking (OR 1.557; 95% CI, 1.297–1.868), and hypertension (OR, 2.882; 95% CI, 2.386–3.481) were associated with COPD in the univariate analysis. However, after controlling for covariates, age (aOR, 1.052; 95% CI, 1.045–1.059), BMI (aOR, 0.975; 95% CI, 0.958–0.992), and smoking (aOR, 1.843; 95% CI, 1.504–2.259) were independent predictors of COPD in female participants.
No Differences in the Levels of Serum Leptin in COPD Subjects with Different Severities
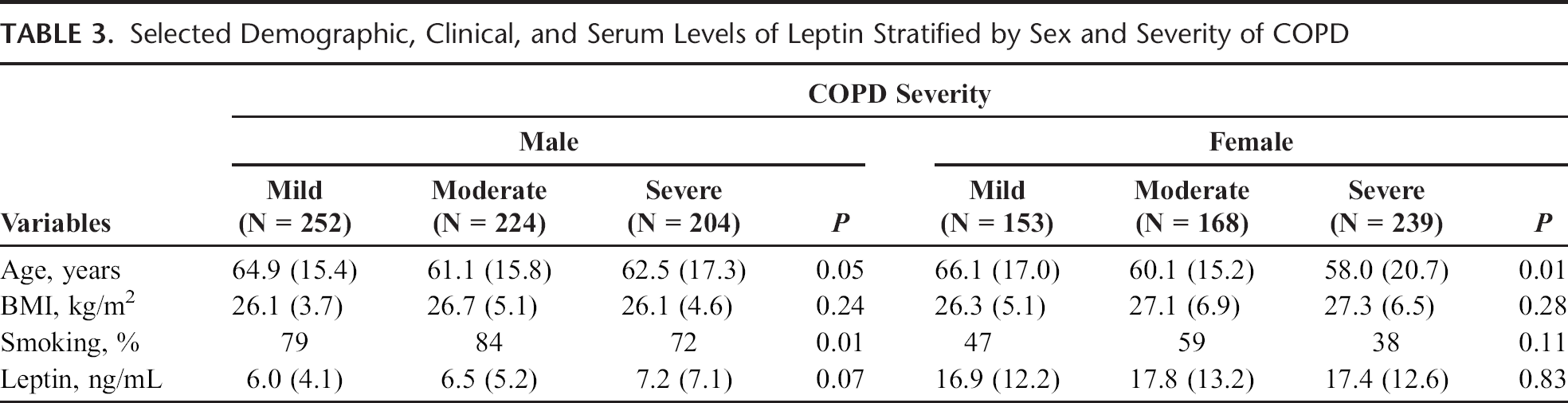
As shown in Table 3, there were no differences in the level of serum leptin among COPD subjects with different severities in both sexes.
Selected Demographic, Clinical, and Serum Levels of Leptin Stratified by Sex and Severity of COPD
Discussion
In this large, national, population-based study, we failed to demonstrate a relationship between serum leptin and COPD.
Leptin is an adipocyte-derived hormone, recognized as a critical mediator of the balance between food intake and energy expenditure by signaling through its functional receptor (Ob-Rb) in the hypothalamus. 16 Leptin is now known to have pleiotropic functions in both innate and adaptive immunity. 6 The presence of the functional leptin receptor in the lung, together with evidence of increased airspace leptin levels arising during pulmonary inflammation, suggests an important role for leptin in respiratory immune responses and, eventually, pathogenesis of inflammatory respiratory diseases, such as COPD. 16 Currently, the human data regarding the independent association between serum leptin and COPD remain inconclusive. 7 Breyer et al. 9 studied the differences in serum leptin in 91 COPD patients compared with 35 healthy controls. They found the higher serum leptin concentrations only in women with COPD when compared with BMI-matched controls. In another study from Korea, there were no differences in the levels of leptin among men participants with and without COPD. 10 The differences in these results, including ours, are likely due to the study design and the study population.
Consistent with previous studies, 17 we found that age is an independent predictor for COPD for both sexes. In a study using the Bayesian network model to predict COPD from the electronic medical records, age is the strongest single variable predictor for COPD. This variable alone predicts COPD with an area under the receiver operating characteristic curve of 0.81. 17 In fact, the relationship between age and COPD is well known as COPD is a chronic disease that worsens over time and is mainly present in older adults. 17 In our study, subjects with COPD were approximately 20 years older than controls. We also found the inverse relationship between the BMI and COPD. Our findings are similar to others when low BMI is associated with COPD and that low BMI is a determinant of poor survival of COPD patients.18–20 Smoking is a known risk factor for COPD. 3 In our study, it is not surprising that we found smoking as the independent predictor for COPD in both sexes.
The strength of our study is that NHANES III used uniform methods to collect data on serum leptin and spirometry measurement and that the study design allows the results to be extrapolated to the entire US population. Despite its strength, our study has several shortcomings. The cross-sectional design of the NHANES III prohibits us to examine the causative nature or temporal association between serum leptin and COPD. It is also plausible that there might be some participants who were classified as having COPD but in fact had reversible airway obstruction, such as asthma. To look at this issue more carefully, we found that, among male and female participants in NHANES III who underwent spirometry measurement, 5.9% and 7.7%, respectively, were told by physicians that they had asthma. When we excluded these subjects from the analyses, we still did not find any association between serum leptin and the presence of COPD. Finally, the information on the level of FEV1 after administration of short-acting β2-agonist to determine the reversibility of the obstructive airway was not available in the NHANES III database.
Conclusion
In summary, in this population-based study, we did not find any significant difference in the level of serum leptin in subjects with COPD. Our data provide indirect evidence against a major role for serum leptin in the pathogenesis of COPD in humans.