
Abstract
Background
Chronic obstructive pulmonary disease (COPD) results from an abnormal inflammatory response of the lungs to noxious particles or gases. Serum soluble urokinase-type plasminogen activator receptor (suPAR) is a glycoprotein secreted during infections and inflammation. The main goal of this study was to evaluate the serum suPAR level in stable COPD patients compared with a control group.
Methods
Forty-six stable COPD patients and 41 control subjects were included in the study. Blood samples were collected from 46 stable COPD patients (40 men, 6 women; mean [SD] age, 55.92 [7.91] years; the forced expiratory volume in 1 second, 45.32% [19.1%] of predicted). Forty-one healthy subjects were selected as control subjects and were matched to COPD patients with respect to age and body mass index. Serum suPAR and plasma fibrinogen levels were measured in stable COPD patients and control subjects.
Results
Serum suPAR levels of the COPD patients were significantly higher than those of the control subjects (4.94 [2.79] and 2.40 [2.01] ng/mL, respectively; P < 0.001). Plasma fibrinogen levels of the COPD patients were significantly higher than those of the control subjects (406.77 [172.6] and 336.53 [96.1] g/L, respectively; P < 0.05).
Conclusions
Our study indicated that serum suPAR may play an important role in the inflammatory process of COPD, and this increase may be particularly large for patients in Global Initiative for Chronic Obstructive Lung Disease stages III and IV. Serum suPAR and plasma fibrinogen level measurements may be useful for the evaluation of stable COPD.
Keywords
Chronic obstructive pulmonary disease (COPD) is usually characterized by a progressive airflow limitation that is not fully reversible and is associated with an abnormal inflammatory response of the lungs to noxious particles or gases, such as cigarette smoke. Disease processes include chronic bronchitis, emphysema, and small airway diseases (chronic inflammation and remodeling of the small airways and particularly of the terminal bronchioles).1–4 The COPD not only causes pulmonary inflammation and airway remodeling but also includes systemic manifestations such as systemic inflammation, cardiovascular events, osteoporosis, and anemia. 5 Disease severity and progression are classified by forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC), which are measured by spirometry. The percentage of FEV1 determines which Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage patients are classified into I to IV.2,6
The COPD is a complex disorder caused by multiple mediators and pathways (including innate and acquired immunity, tissue destruction and repair, oxidative stress, inflammation, protease/antiprotease imbalance, and apoptosis of structural cells).1,4,7,8 The chronic inflammation of COPD is characterized by an accumulation of polymorphonuclear neutrophils (PMNs), macrophages, CD8+ T cells, B lymphocytes, and dendritic cells.7,9 Neutrophils and activated macrophages release oxygen radicals, cytokines, proteinases, and chemokines.1,7,9,10 Emphysema is a disease component that contributes to COPD, which results from alveolar airspace enlargement, loss of lung elasticity, and protease-mediated degradation of the extracellular matrix.4,7,11 Proteinases consist of 4 groups (serine, metallo-, cysteine, and aspartic proteinases). Serine proteinases are classified as PMN-derived serine proteinases, urokinase-type plasminogen activator (uPA), granzymes, and plasmin. The uPA is secreted by PMN and macrophages; afterward, uPA binds to membrane uPA receptor (uPAR) on cell surfaces (including macrophages, PMN, vascular endothelial cells, lymphocytes, epithelial cells, and dendritic cells).7,12,13 The uPAR expression in these cells is increased by a variety of activating factors, including many inflammatory cytokines (eg, IL-1 and tumor necrosis factor-α) and bacterial products (eg, endotoxins and lipopolysaccharides).13,14 The uPAR-bound uPA can convert plasminogen to plasmin (another serine proteinase), which degrades fibrin, activates matrix metalloproteases, and mediates proteolysis of extracellular matrix proteins during cellular invasion.15,16 Soluble uPAR (suPAR) is formed by proteases or cleaved from the glycosylphosphatidylinositol anchor by phospholipases and released from cell membrane-bound uPAR.17,18 Both membrane-bound uPAR and suPAR bind to and modulate the functions of integrins (including activating intracellular signals and pathways, PMN/monocyte chemotaxis, cell adhesion and proliferation). Circulating suPAR activates podocyte β3 integrin and grafted kidneys, causing foot process effacement, proteinuria, and focal segmental glomerulosclerosis-like glomerulopathy.14,17,19,20 The suPAR contributes to plasminogen activation, cell adhesion, migration, proliferation, inflammation, chemotaxis, proteolysis, immune system activation, tissue remodeling, and signal transduction.17,21 The suPAR is expressed in various cell types, such as macrophages, monocytes, endothelial cells, fibroblasts, neutrophils, and activated T lymphocytes. 22 Plasma levels of suPAR have been shown to potentially cause or modulate disease in patients with cancer, various infectious, and inflammatory diseases (including infections with human immunodeficiency virus, tuberculosis, arthritis, liver fibrosis, and inflammatory bowel disease). 17
Several studies have indicated that suPAR level is a risk indicator in patients with various infectious diseases, and it reflects the disease severity and is associated with a poorer outcome in a range of noninfectious and infectious diseases.15,21 Fibrinogen is an acute phase soluble plasma glycoprotein. The IL-6 increases synthesis of fibrin in the liver during acute phase stimulation and inflammation. Thrombin converts fibrinogen into fibrin. 6
In the literature, there are few studies of the relationship between suPAR and lung disease, and only 1 study investigates the levels of serum suPAR in COPD. 23 Portelli et al. 23 reported that elevated serum suPAR levels were identified in asthma and COPD cohorts when compared with control subjects. We hypothesized that suPAR has a diagnostic value in COPD. The suPAR and fibrinogen levels were also evaluated in patient and control groups to define the level of pulmonary inflammation and its correlation with the GOLD stages (II–IV).
Materials and Methods
Participants
The study protocol was approved by the ethics committee of the Meram Medical School, University of Selcuk, Konya, Turkey. The ethics number was 2012/69. All of the patients were informed of the details of the study, and written consent was received from each patient. Patients with stable COPD (stages II-IV) who were admitted to the outpatient clinic of a university hospital in Konya, Turkey (Meram Medical School, University of Necmettin Erbakan) between September 2012 and June 2013 were included in the study.
A total of 46 patients with stable COPD were recruited from the hospital. Patients were matched with respect to age, sex and body mass index (BMI) to 41 healthy control subjects. The 41 healthy control subjects were volunteers recruited from the hospital staff. The subjects selected for the control group consisted of current or ex-smokers with at least 10 pack-years, healthy men and women between 30 and 70 years old (matched with the patient group), and individuals with normal spirometry and without any infectious or inflammatory diseases. Before inclusion in the study, the healthy controls were fully examined by a chest physician for lung impairment, cardiovascular disease, diabetes, or other diseases.
A stable condition was defined as a stable disease for 2 months, without any reported exacerbations and both no changes in respiratory medication (on a standard treatment regimen consisting of inhaled corticosteroids and β-adrenergic agonists) and the absence of an infection before inclusion in the study. We enrolled a cohort of the stable COPD outpatients who were diagnosed according to GOLD criteria. 24 Postbronchodilator spirometry was performed according to American Thoracic Society criteria. The FEV1 and the FEV1/FVC ratio were expressed as “% Pred.” The inclusion criteria for cases included (1) a diagnosis of COPD with an FEV1/FVC ratio of less than 70%, (2) a negative history of acute exacerbations in the previous 2 months, and (3) stable COPD patients between the ages of 30 and 70 years who were either current smokers or ex-smokers with at least 10 pack-years.
The exclusion criteria for cases included (1) bronchiectasis, pulmonary thromboembolism, pneumothorax, asthma, interstitial pulmonary fibrosis, granulomatous lung disease, or tuberculosis; (2) COPD exacerbations within the last 2 months (increase in cough, sputum production, worsening dyspnea, or sputum purulence); (3) cardiovascular disease and hypertension; (4) systemic diseases, such as rheumatoid arthritis, malignancies, diabetes mellitus, metabolic or endocrine diseases, chronic gastrointestinal diseases, chronic liver diseases, and chronic kidney diseases; or (5) pateints who were treated with oral corticosteroids or any medication apart from COPD maintenance therapy or immunosuppressors, for any reason. This study was performed on 46 (40 men, 6 women) COPD patients aged 30 to 70 years (mean [SD], 55.92 [7.91] years), of whom 17 were classified as GOLD stage II, 15 were classified as GOLD stage III, and 14 were classified as GOLD stage IV COPD, and 41 (30 men, 11 women) healthy control subjects aged 30 to 70 years (mean [SD], 52.41 [9.51] years) from the general population. The BMI was calculated as weight divided by height (kg/m2).
Pulmonary Function Testing
The FEV1, FVC, and FEV1/FVC were measured according to American Thoracic Society criteria. The COPD stages were classified according to the GOLD Criteria 2012. 24
The stages of COPD were determined by using the GOLD criteria:
GOLD II (moderate): FEV1/FVC of less than 70% and FEV1 of less than 80% and of 50% or greater
GOLD III (severe): FEV1/FVC of less than 70% and FEV1 of less than 50% and of 30% or greater
GOLD IV (very severe): FEV1/FVC of less than 70% and FEV1 less than 30%
The FEV1 was also measured 15 minutes after 4 inhalations of salbutamol (400 μg) from a metered-dose inhaler.
Spirometry was performed using a Sensor Medics VMax 22 respiratory analyzer.
Laboratory Methods
After a 12-hour fast, a venous blood sample was collected from each subject in empty vacuum tubes and in tubes containing Na-citrate of 3.2%. Serum and plasma (Na-citrate, 3.2%) samples were obtained after suitable centrifugation, and samples were stored frozen at −80°C until measurement. Blood samples were obtained from the stable-phase COPD patients and from the healthy control group. Plasma fibrinogen was analyzed immediately by the hospital pathology service using commercial autoanalyzers.
Arterial blood samples were gently drawn from the brachial artery using a dedicated preheparinized blood sampler. Arterial oxygen and carbon dioxide tensions (pO2 and pCO2) were analyzed using a Radiometer Copenhagen ABL 700 series blood gas analyzer.
Biochemical Analyses
Fibrinogen levels were measured by routine methods using commercially available kits on a Siemens BCS System. Analysis of suPAR was detected in serum samples using the AssayMax Human Urokinase Receptor (uPAR) ELISA Kit (Assaypro, St Charles, MO), in accordance with the manufacturer's guidelines. All samples (serum) were diluted 1:4 in the supplied buffer and measured in duplicate. Absorbance was measured at 450 nm on an ELx800 Absorbance Microplate Reader (Biotek, Winooski, VT). This assay used a quantitative sandwich enzyme immunoassay technique to measure suPAR. The mean value of the duplicate readings for each standard and sample was calculated and then multiplied by the dilution factor. The unknown sample concentration was determined from the standard curve. Concentration values were reported in ng/mL.
Statistical Analyses
All data values are expressed as mean (SD). Statistical analyses were performed using Statistical Package for the Social Sciences v. 16.0 (SPSS Inc, IL). To compare the ratio of categorical variables, we used the χ2 test (sex [female/male], smoking status). The normality of the variables was evaluated using the 1-sample Kolmogorov-Smirnov test.
Normal distributions of variables were examined using the independent-samples t test. Groups of data were compared by analysis of variance followed by Tukey multiple comparison tests. Correlations between variables were determined using Pearson correlation test. A probability level of P < 0.05 indicated a significant difference between groups.
Results
All patients in the study were clinically and spirometrically diagnosed with COPD. All healthy subjects exhibited normal lung function. The clinical and demographic characteristics of the subjects are presented in Table 1.
Clinical and Demographic Characteristics of the Patients and Controls
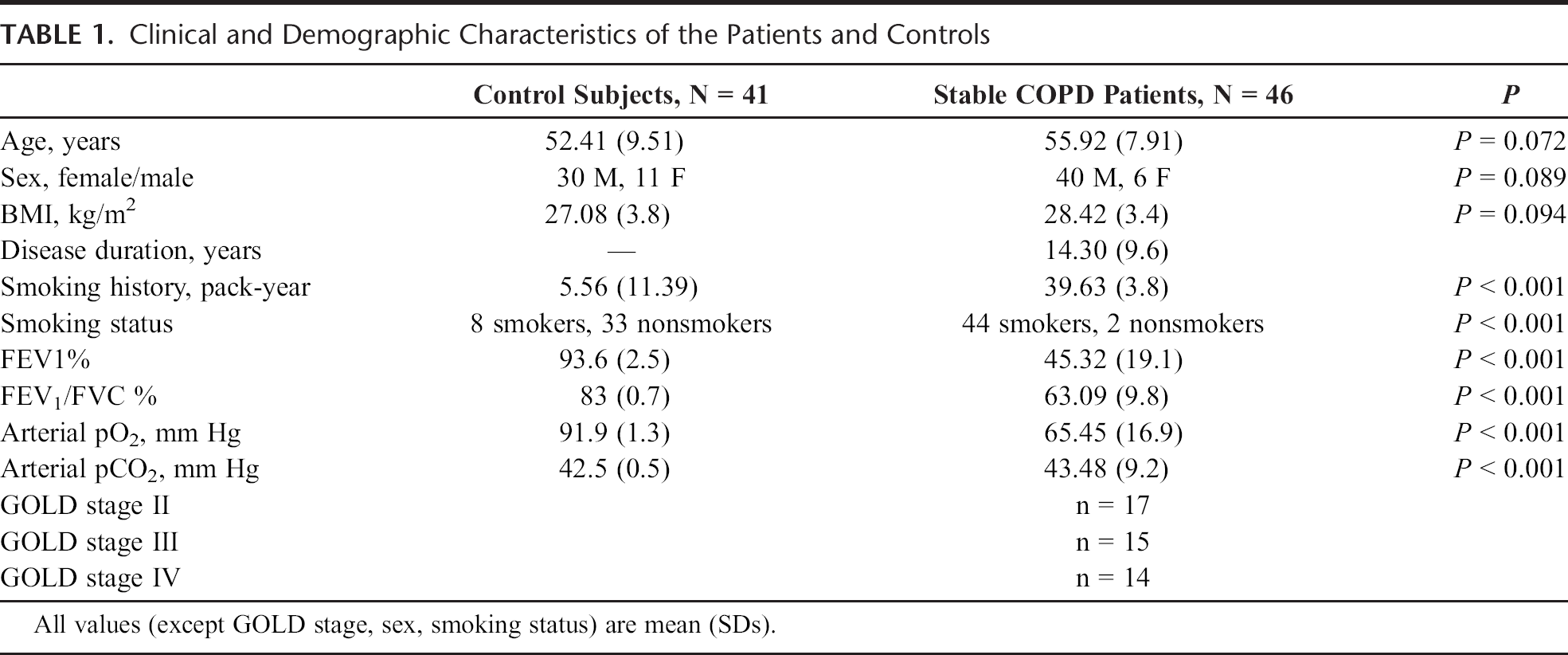
The age, sex, and BMI of the 2 groups were not significantly different. However, smoking history and the smoking status of the COPD patients were significantly higher compared with the control subjects (P < 0.001).
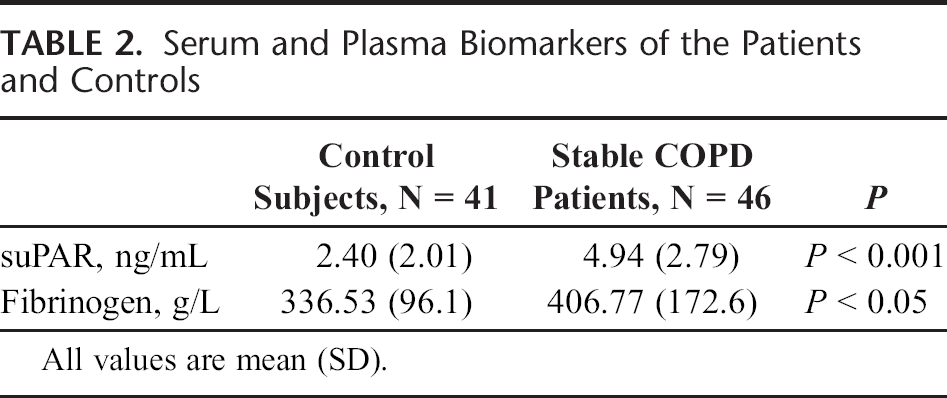
Circulating biomarker levels in the COPD patients and control subjects are shown in Table 2. Serum suPAR levels and plasma fibrinogen levels of the COPD patients were significantly higher than those of the control subjects (Ps < 0.001 and 0.05, respectively).
Serum and Plasma Biomarkers of the Patients and Controls
Serum and plasma biomarkers in the various GOLD stages of the patients and controls are shown in Table 3. There were no significant differences between plasma fibrinogen levels in patients in GOLD stages II, III, and IV and control subjects (P = 0.059). There were significant differences between serum suPAR levels in patients in GOLD stages II, III, and IV and control subjects (P < 0.001).
Serum and Plasma Biomarkers in GOLD Stages of the Patients and Controls

Serum and plasma biomarkers in the various GOLD stages of the patients are shown in Table 4. There were no significant differences between serum suPAR and plasma fibrinogen levels in patients in GOLD stages II, III, and IV (Ps = 0.288 and 0.244, respectively).
Serum and Plasma Biomarkers in Various GOLD Stages of the Patients

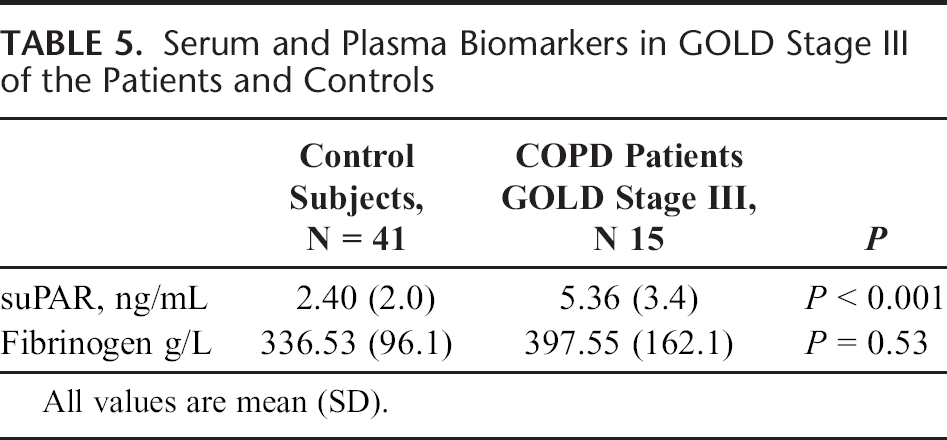
Serum and plasma biomarkers of the patients in the GOLD stage III and controls are shown in Table 5. Patients in GOLD stage III had significantly higher serum suPAR levels than those of the control subjects (P < 0.001). Hovever, no significant difference was observed between plasma fibrinogen levels in patients in GOLD stage III and the control subjects (P = 0.53).
Serum and Plasma Biomarkers in GOLD Stage III of the Patients and Controls
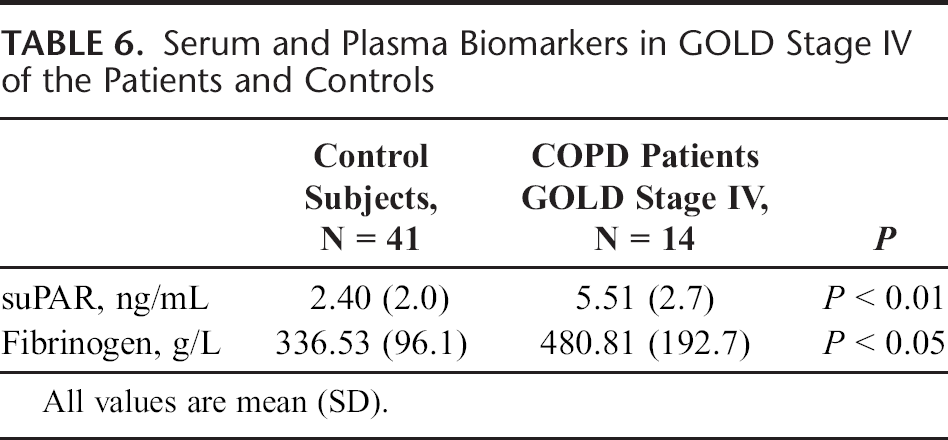
Serum and plasma biomarkers of the patients in GOLD stage IV and control subjects are shown in Table 6. Patients in GOLD stage IV had significantly higher serum suPAR and plasma fibrinogen levels than those of the control subjects (Ps < 0.01 and 0.05, respectively).
Serum and Plasma Biomarkers in GOLD Stage IV of the Patients and Controls
Simple correlation analysis was performed to investigate the associations among serum suPAR, plasma fibrinogen, age, smoking history, disease duration, BMI, FEV1 %, FEV1/FVC %, pO2, and pCO2. The disease duration was positively correlated with age (r = 0.426, P < 0.01), whereas pCO2 was negatively correlated with pO2 (r = −0.338, P < 0.05). The pCO2 was negatively correlated with FEV1% (r = −0.406, P < 0.01) in COPD patients. Moreover, fibrinogen was negatively correlated with BMI (r = −0.334, P < 0.05) and FEV1/FVC % (r = −0.387, P < 0.05).
Discussion
The suPAR is a relatively new disease marker, and few studies have investigated suPAR in COPD patients. In the present study, we found serum suPAR levels and plasma fibrinogen levels of stable COPD patients to be significantly higher than those of control subjects. Patients in GOLD stages III and IV had significantly higher suPAR levels than those of control subjects, and patients in GOLD stage IV had significantly higher plasma fibrinogen levels than those of control subjects. These findings show that suPAR and fibrinogen are nonspecific markers of inflammation in COPD (especially for patients in GOLD stage IV). Our findings were in agreement with previous studies. Portelli et al. 23 reported that elevated serum suPAR levels were identified in asthma and COPD cohorts compared with control. Backes et al. 25 reported that pulmonary levels of suPAR were increased in burn patients with inhalation trauma and were correlated with pulmonary inflammation and coagulation. Stewart et al. 26 found that uPAR expression was significantly increased in the bronchial epithelium of patients with asthma compared with controls. In our study, we found that patients in GOLD stages III and IV had significantly higher suPAR levels than those of control subjects, but there were no significant differences between patients in GOLD stages II, III, and IV.
The COPD is characterized by a chronic inflammation of the lower airway and the lung parenchyma and includes inflammatory cell accumulation; proteinase production; and proteinase release from inflammatory, immune, and structural cells. Proteinases cause airspace enlargement by degrading the extracellular matrix and promoting the death of structural cells in the alveolar walls. Proteinases also increase lung inflammation, mucus hypersecretion, and small airway fibrosis. 7 Plasmin, a serine protease, plays a central part in fibrinolysis and extracellular matrix degradation, which is an essential part of tissue remodeling. Plasminogen activation is increased by inflammation; specifically, the proinflammatory cytokines IL-1 and tumor necrosis factor-α induce an upregulation of uPA. 27 The suPAR is closely correlated with inflammation and renal and hepatic dysfunctions, which are central pathophysiological and therapeutic targets of the disease. The suPAR is highly stable in serum samples and undergoes limited circadian changes in plasma concentrations. 28
According to our hypothesis, suPAR may play an important role in the pathogenesis of COPD and may specifically increase in patients in GOLD stages III and IV. Wang et al. 29 found that uPAR expression was significantly increased in the small airway epithelium of patients with COPD compared with controls. Koch et al. 28 reported that serum suPAR concentrations upon admission to the intensive care unit are elevated in critically ill patients when compared with healthy controls and are higher in sepsis than nonsepsis patients. Yeh et al. 30 found that the levels of plasma uPA and soluble suPAR were significantly increased in pelvic inflammatory disease patients when compared with normal controls. Barton et al. 31 reported that plasma urokinase plasminogen activator receptor (PLAUR) single-nucleotide polymorphisms are associated with PLAUR levels and influence the rate of decline of FEV1 in asthma, supporting the hypothesis that PLAUR is involved in chronic changes in the airways. The PLAUR is a novel therapeutic target for the treatment of asthma.
In summary, we found that serum suPAR levels were elevated in stable COPD, and no significant difference in theses levels was found between patients in GOLD stages II, III, and IV. Our findings were in agreement with the study by Mardining Raras and Noor, 32 which showed that mobilization of macrophages into the bronchi increased suPAR levels. Adherence and migration of monocytes were associated with a functional interaction between uPAR and integrins. In this study, the suPAR level among patients with far advanced lesions, moderately advanced lesions, and minimal lesions did not differ significantly.
Fibrinogen is an acute phase soluble plasma glycoprotein that is converted thrombin into fibrin by thrombin. The IL-6 regulates fibrinogen production in the liver. Fibrinogen increases blood viscosity, platelet aggregation, and thrombosis. It is an important risk factor for the development of a prethrombotic state, progressive airway inflammation, and lung tissue injury.6,33 Fibrinogen is a useful biomarker in COPD. We found that plasma fibrinogen was elevated in stable COPD. Patients in GOLD stage IV had significantly higher plasma fibrinogen levels than those of the control subjects. However, there was no significant difference between patients in GOLD stages II, III, and IV. In previous studies, Gan et al. 34 showed that patients with stable COPD had higher fibrinogen levels than the control subjects. Dahl and Nordestgaard 35 showed that increased levels of plasma fibrinogen were associated with reduced lung function and increased risk for COPD. Valvi et al. 36 showed that subjects with more advanced COPD (stage III or IV) had a greater elevation in fibrinogen levels than patients in GOLD stage II or I.
Biomarkers of COPD are required to aid diagnosis, define clinical phenotypes, and monitor the response to existing and new therapeutic strategies. Fibrinogen and suPAR are markers of inflammation in COPD. In conclusion, our findings showed significant associations between serum suPAR levels, plasma fibrinogen levels, and stable COPD. Our findings suggest that suPAR may play an important role in the pathogenesis of COPD and suPAR specifically increases in patients in GOLD stages III and IV. Further studies with larger sample sizes are necessary to explain the relationship between serum suPAR levels and plasma fibrinogen levels in stable COPD.