
Abstract
Background
Cirrhosis is diagnosed in patients of all ages and is the end result of many different diseases. The aim of this study was to characterize clinical and ethnic features of adult patients who were admitted to the hospital at different (young/old) ages and examine associations between age and ethnicity within these groups.
Methods
In this retrospective analysis of a diverse cohort of 2017 patients with a clinical diagnosis of cirrhosis between January 2001 and December 2011, we focused on age, ethnicity, and outcome of patients with cirrhosis.
Results
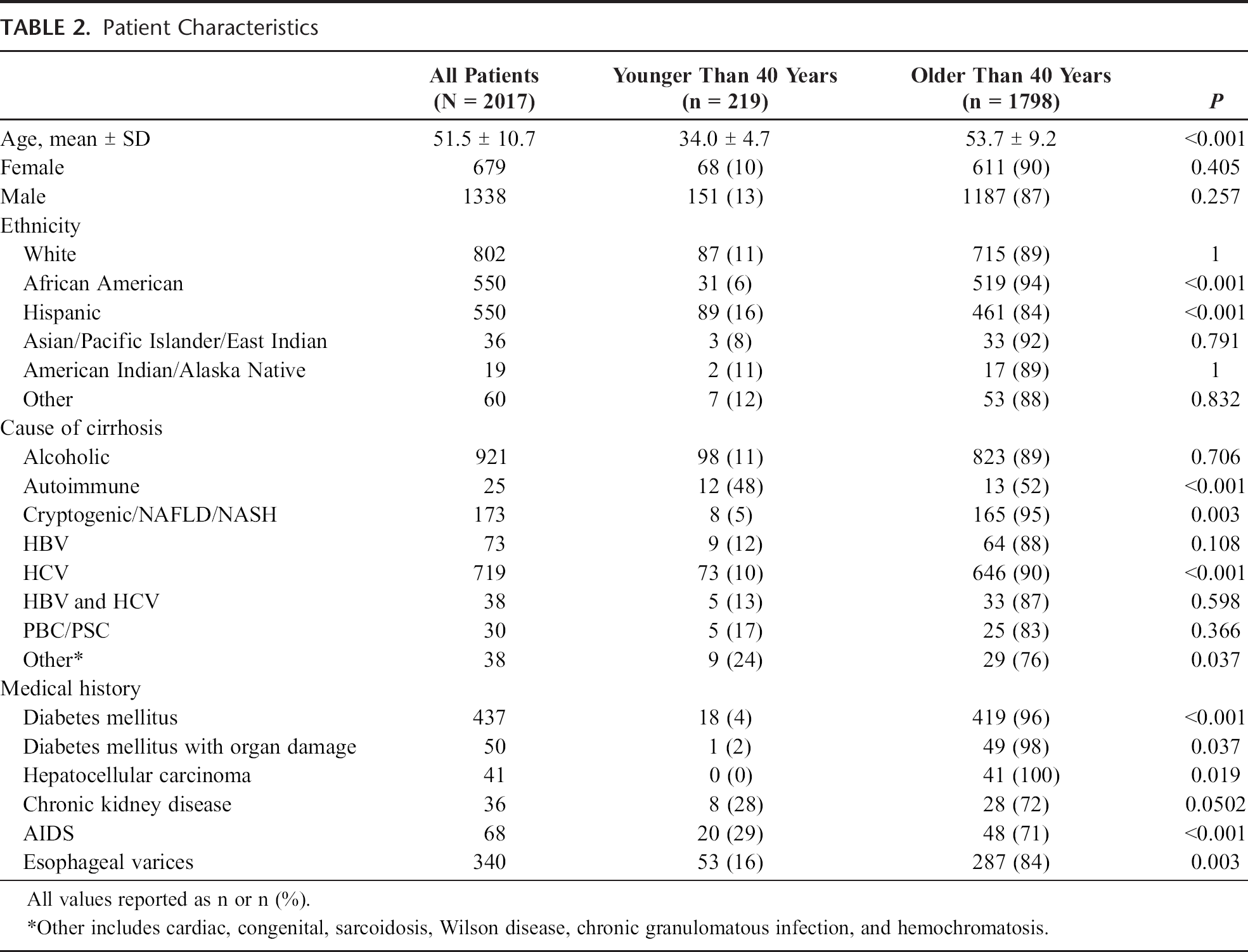
We identified 219 patients younger than the age of 40 years, including 87 (11%) of 802 white, 31 (6%) of 550 African American, and 89 (16%) of 550 Hispanic patients (P < 0.001). Ethnicity and causes of cirrhosis were found to have a significant correlation with age. Overall, Hispanic and white patients together were more than twice as likely to be diagnosed with cirrhosis at an age younger than 40 years compared with African American patients (P < 0.001). Autoimmune hepatitis caused cirrhosis at a younger age regardless of ethnicity (P < 0.001), whereas cryptogenic/nonalcoholic fatty liver disease/nonalcoholic steatohepatitis was more likely identified at an older age (P = 0.008). African American patients with cirrhosis due to either alcohol or hepatitis C virus were older than Hispanic (P < 0.001 and P = 0.003, respectively) and white patients (P < 0.001 and P < 0.001, respectively) at presentation. Finally, younger patients admitted with cirrhosis had a higher in-hospital mortality rate (P < 0.001).
Conclusions
The data suggest an association between ethnicity and age of cirrhosis diagnosis, both overall and in patients with certain cirrhosis etiologies. This work raises the possibility of an ethnic and/or genetic basis for cirrhosis.
Cirrhosis is the result of persistent hepatic injury from chronic liver disease (CLD). It is a wound healing process during which fibrosis and scar tissue is deposited in the space of Disse and in other portions of the liver.1,2 This has a number of important functional consequences, including alteration of normal portal blood flow. The end result of the fibrosing process is cirrhosis, which results in a number of systemic complications, including ascites and portal hypertension, which are associated with poor quality of life and approximately 30,000 deaths per year in the United States. 3
Extensive investigation has demonstrated that the fibrotic process is due largely in part to the activation of effector cells, including fibroblasts, fibrocytes, and hepatic stellate cells, which proliferate, release proinflammatory, profibrogenic, and promitogenic cytokines and produce extracellular matrix. This process is complex and is dependent on a variety of control pathways, growth factors, cytokines, vasoactive mediators, transcriptional regulators, epigenetic regulators, and immune system regulators, which modulate cellular fibrogenesis. 1
Because cirrhosis is the end result of a variety of diseases affecting the liver, it follows that mechanisms underlying the fibrogenic process are likely to be common across these different disease states. Furthermore, a variety of exogenous factors, such as obesity, alcohol abuse, and viral coinfection, contribute to the progression of fibrosis.4,5 However, even after controlling for these factors, a large variation still exists in the propensity of developing cirrhosis between individuals.6,7 For example, 1 study revealed a difference in cirrhosis mortality rates among various ethnicities. 8 This suggests that there are genetic and possibly inherited ethnic factors associated with the development of hepatic fibrosis and cirrhosis. Thus, we have hypothesized that individuals who develop cirrhosis at a young age may share common demographic and/or clinical features. We therefore aimed to better clinically characterize patients who develop cirrhosis younger than the age of 40 years, and here, we describe several key associations with age and ethnicity.
Methods
We performed a retrospective cross-sectional study of 2048 patients admitted to Parkland Memorial Hospital with a documented clinical diagnosis of cirrhosis from 2001 to 2011. Patients were identified by an International Classification of Diseases, Ninth Revision, Clinical Modification search for causes of cirrhosis, which included the following codes: 571 (CLD and cirrhosis), 571.2 (alcoholic cirrhosis), 571.5 (cirrhosis of liver without alcohol), 571.6 (biliary cirrhosis), 572.2 (hepatic encephalopathy), 572.3 (portal hypertension), 456.0 (esophageal varices with bleeding), and 456.1 (esophageal varices without documented bleeding). The electronic medical record (EMR) (EPIC Systems Corporation, Verona, WI) was manually reviewed in all patients to confirm the diagnosis of cirrhosis, defined as consistent histology or imaging showing a cirrhotic-appearing liver with any associated signs of portal hypertension (ascites, encephalopathy, varices, or splenomegaly; see also below under definitions). 9 Ethnicity was self-reported. The study was approved by the institutional review board at the University of Texas Southwestern Medical Center, St Paul University Hospital, and the Parkland Health and Hospital System and met all criteria for good clinical research.
A Microsoft Access database was created that included demographic, clinical, and historical data for all patients. This included cause of cirrhosis, medical comorbidities, complications of cirrhosis, and laboratory values. Clinical and laboratory variables reported were recorded at the time of hospital admission. The age at index hospitalization was taken to be the age at diagnosis of cirrhosis.
Patients for whom ethnicity or a cause of cirrhosis could not be identified were excluded from the final analysis. We separated all remaining patients (n = 2017) into 2 groups: those younger than the age of 40 years (n = 219) and those older than the age of 40 years (n = 1798). Deceased patients were identified by searching for the last documented encounter in the hospital system's EMR after their index admission.
Definitions
Cirrhosis was defined based on clinical features, including a history consistent with CLD as well as a documented complication of CLD (ie, ascites, varices, hepatic encephalopathy) 10 and/or imaging consistent with cirrhosis and/or liver histology consistent with cirrhosis. 11 The cause of cirrhosis was determined according to the following criteria: (1) hepatitis C cirrhosis was defined by the presence of cirrhosis in a person with hepatitis C virus (HCV) RNA; (2) hepatitis B cirrhosis was defined by the presence of cirrhosis in patients with hepatitis B virus (HBV) surface Ag; (3) alcoholic cirrhosis was determined by chart review in the presence of a history of prolonged alcohol consumption with abuse or dependence in the absence of other potential causes of liver disease; (4) nonalcoholic fatty liver disease (NAFLD) or nonalcoholic steatohepatitis (NASH) cirrhosis was defined by biopsy proven or the presence of the metabolic syndrome without any other potential cause of liver disease; (5) patients without any known cause of primary liver disease were considered to have cryptogenic cirrhosis; and (6) other causes of cirrhosis were determined using standard diagnostic criteria (ie, serologies, histology, iron studies). Cryptogenic cirrhosis was combined with NAFLD and NASH, consistent with previous studies showing that cryptogenic may be related to NAFLD/NASH,12,13 and current best practice. Finally, mortality was defined as death occurring during the hospital admission at Parkland Memorial Hospital and was determined for all patients.
Statistical Analysis
This study was a cross-sectional analysis of cirrhotic patients younger than the age of 40 years compared with cirrhotic patients older than 40 years. Patient characteristics and clinical laboratory data were summarized using descriptive statistics. Categorical and continuous variables were compared using the χ2 test, Student t test, and Fisher exact test; P ≤ 0.05 using a 2-sided t test was considered statistically significant. A multiple regression analysis was performed with age as the dependent variable and ethnicity (African American, Hispanic, and white), causes of cirrhosis (alcohol, HCV, cryptogenic/NASH/NAFLD, and all others listed previously), comorbid diabetes mellitus with and without end-organ damage, acquired immunodeficiency syndrome (AIDS), and a history of esophageal varices (hepatocellular carcinoma and chronic kidney disease were not studied due to the small number of patients with these comorbidities) as independent variables; P ≤ 0.05 was considered statistically significant.
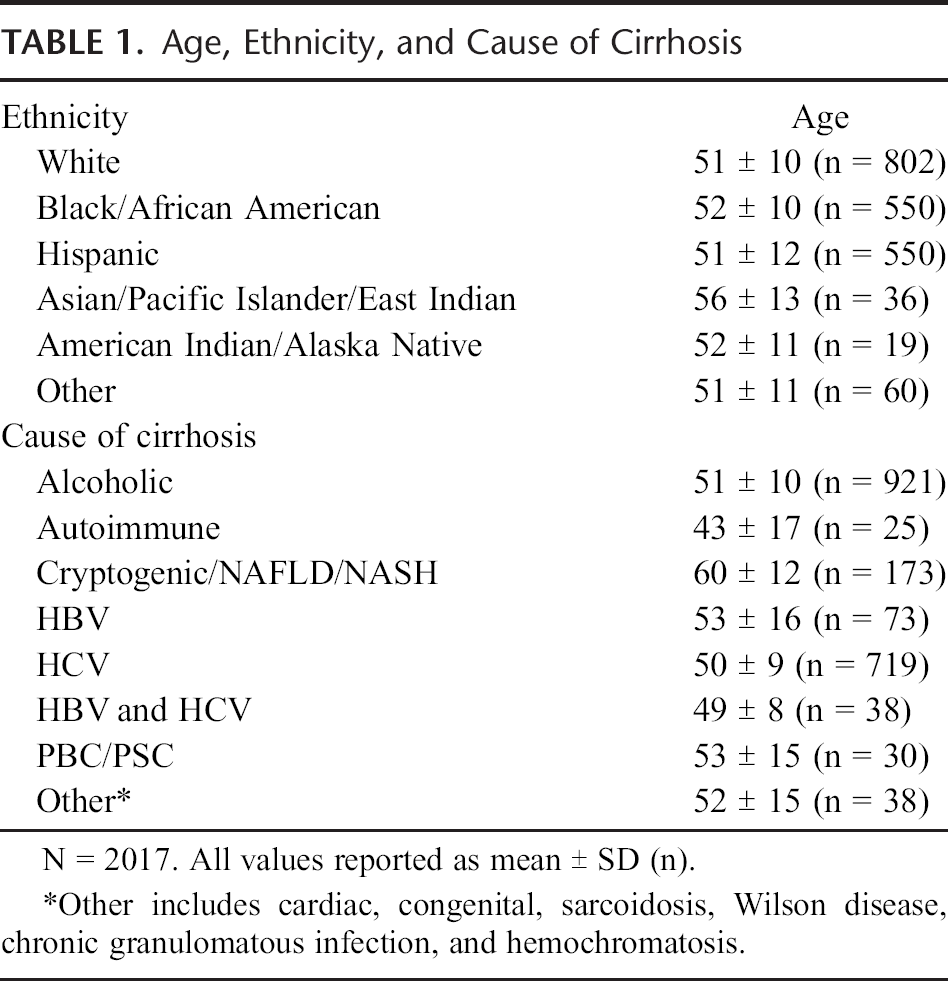
Results
A total of 2048 unique cirrhotic patients were identified. Thirty-one patients lacked data specifically as to ethnicity and/or a cause of cirrhosis and were excluded. The final analysis was therefore performed on 2017 cirrhotic patients, in which 219 were younger than the age of 40 years and 1798 were older than the age of 40 years. The average age of all patients was 52 ± 11; however, patients with cryptogenic/NAFLD/NASH cirrhosis were older (age 60 years), and those with autoimmune cirrhosis were younger (age 43 years) (Table 1, Fig. 1A). The mean model for end-stage liver disease (MELD) score for patients younger than 40 years (17.0 ± 8.0; range, 6–45; n = 213) was greater than that for patients older than 40 years (15.8 ± 7.2; range, 6–52; n = 1224) (P = 0.0275; 95% CI, 0.132–2.268).
Age, Ethnicity, and Cause of Cirrhosis
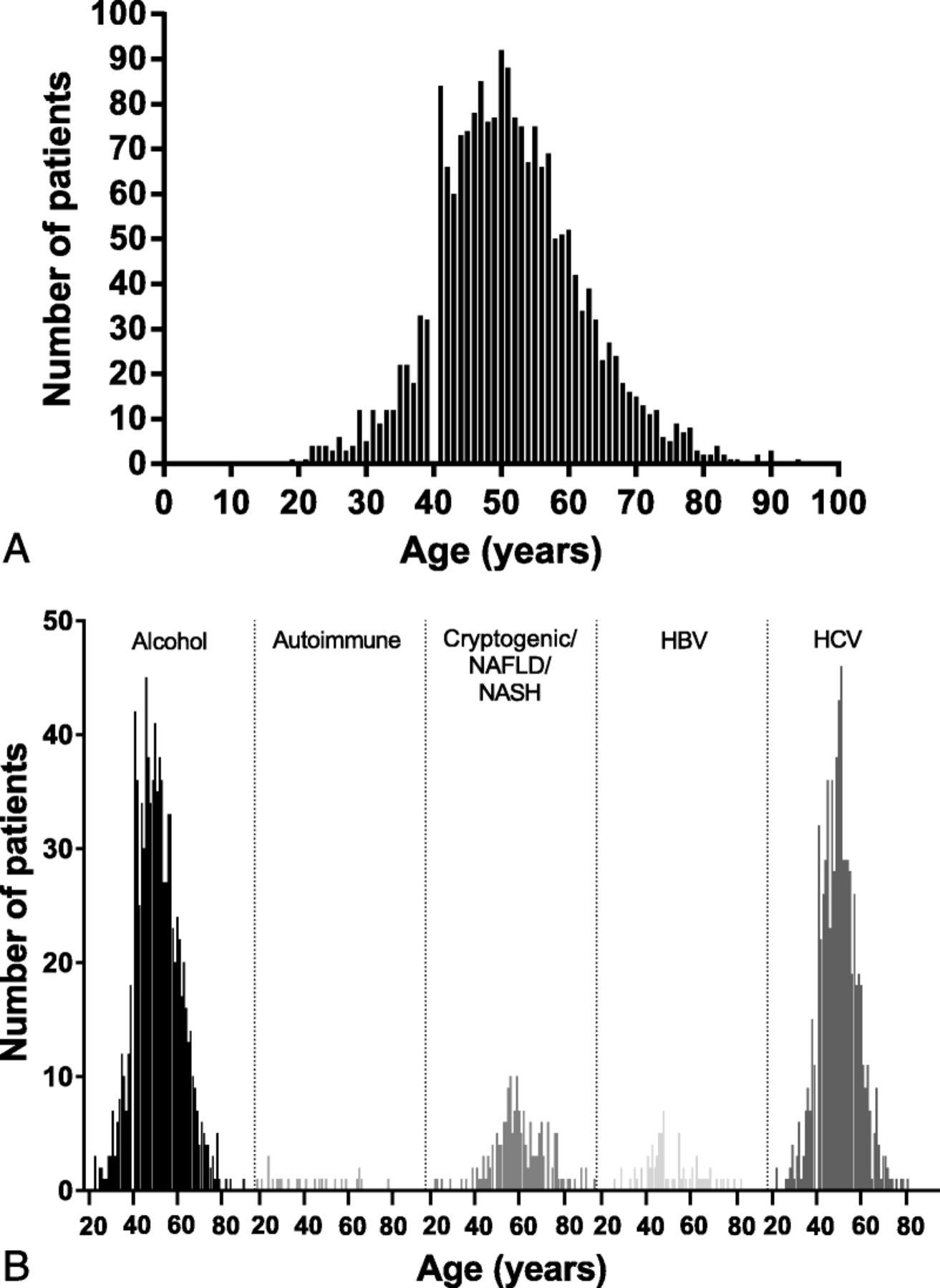
Differences in cirrhosis ages. A, All patients are shown grouped by age. Ages ranged from 19 to 94 with a mean of 51.5 ± 10.7. B, All patients with cirrhosis due to alcohol, autoimmune causes, cryptogenic or NAFLD/NASH, HBV, or HCV are shown grouped by age. Ages ranged from 23 to 90 for alcohol (n = 921), 19 to 78 for autoimmune (n = 25), 22 to 94 for cryptogenic/NAFLD/NASH (n = 173), 26 to 83 for HBV (n = 73), and 22 to 81 for HCV (n = 719).
The major causes of cirrhosis were due to HCV and alcohol (Table 1, 2; Fig. 1B, 2). Other prominent causes of cirrhosis included the following disorders: cryptogenic/NAFLD/NASH liver disease, HBV, autoimmune hepatitis, primary biliary cirrhosis (PBC), and primary sclerosing cholangitis (PSC) (Table 1, 2; Fig. 1B, 2). The average age at presentation of cirrhosis due to alcoholic liver disease was 51 ± 10 years, significantly greater than that for HCV (P < 0.001) and less than that for cryptogenic/NAFLD/NASH (P < 0.001), and nearly 90% of these patients (n = 823/921) were older than 40 years. Similarly, the average age at presentation of cirrhosis due to HCV was 50 ± 9, and again most of these patients (n = 646/719) were older than 40 years. The average age for presentation of cirrhosis due to cryptogenic/NAFLD/NASH causes was 60 ± 12, significantly greater than that for HCV (P < 0.001).
Patient Characteristics
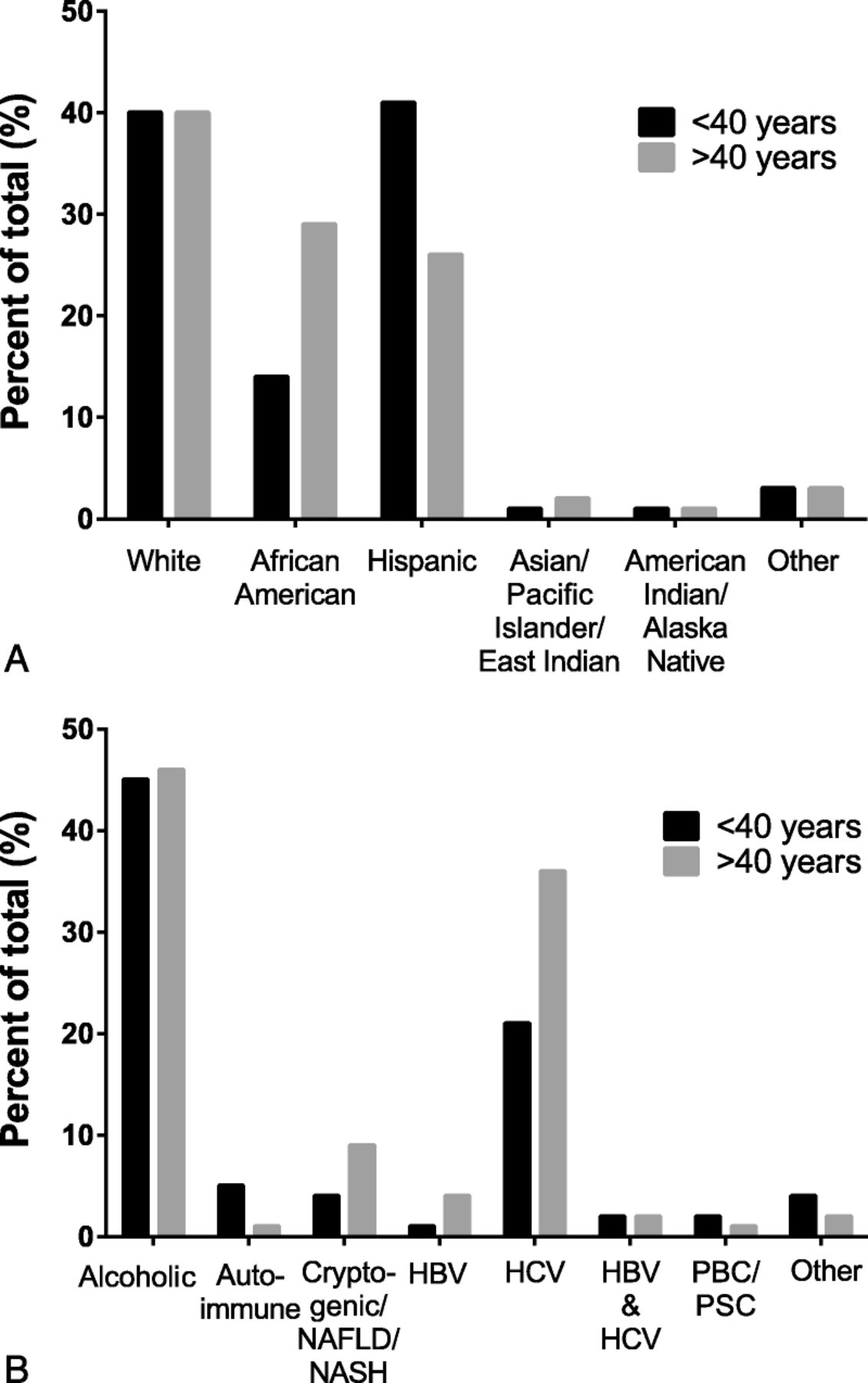
Differences in cirrhosis by age group according to ethnicity and etiology of cirrhosis. A, The frequencies with which patients in different ethnic groups were identified is shown. African Americans were more likely to present with cirrhosis at age older than 40 years (P < 0.001), whereas Hispanics were more likely to present with cirrhosis at age younger than 40 years (P < 0.001). B, the frequency of patients with different etiologies in each age group is shown. Percent is out of the total for ages younger than 40 years (n = 219) or older than 40 years (n = 1798). Autoimmune liver disease was identified more often at age younger than 40 years than those who are older than 40 years (P < 0.001). Cirrhosis due to cryptogenic/NAFLD/NASH was identified more often at age older than 40 years (P = 0.008).
African Americans were significantly more likely to be older, with 94% older than the age of 40 years (P < 0.001, Table 2), whereas Hispanic patients were less likely to be older (P < 0.001, Table 2). The average age of all African American patients was significantly greater than that of Hispanic (P < 0.001) and white (P = 0.031) patients. There was no difference in average age between Hispanic and white patients (P = 0.181). The mean MELD score for African American patients older than 40 years (15.2 ± 8.0; range, 6–52; n = 318) was no different from that of other patients older than 40 years (P = 0.215). The mean MELD score for Hispanic patients younger than 40 years (13.5 ± 7.5; range, 6–33; n = 88) was significantly less than that of other patients younger than 40 years (P < 0.001). Hispanic (89/550) and white (87/802) patients together (176/1352, 13%) were more than twice as likely to be diagnosed with cirrhosis at an age younger than 40 years as African American patients (31/550, 6%) (P < 0.001). When considering all patients specifically younger or older than the age of 40 years (Fig. 2), the proportion of African American patients older than the age of 40 years (519/1798, 29%) was much greater than the proportion younger than the age of 40 years (31/219, 14%) (P < 0.001). In contrast, Hispanic patients were comparatively younger at diagnosis; 461 (26%) of 1798 of patients were older than 40 years, whereas 89 (41%) of 219 were younger than 40 years (P < 0.001). White patients had equal proportions of cirrhotic patients in the younger and older (40% for each) age groups.
A multiple regression analysis was performed to examine the relationship between several different variables and age as in Methods. A significant correlation was identified with ethnicity (African American, Hispanic, and white) (P < 0.001), all causes of cirrhosis (P < 0.001), comorbid diabetes mellitus without end-organ damage (P < 0.001), and comorbid AIDS (P < 0.001) on admission.
The age of presentation in patients with certain causes of cirrhosis differed among the different ethnic groups. African American patients with alcoholic cirrhosis had an older average age (54 ± 10) than both Hispanics (50 ± 11, P < 0.001) and whites (51 ± 9, P = <0.001) (Fig. 3A). A greater proportion of patients with alcoholic cirrhosis were Hispanic (291/921, 32%, P < 0.001) or white (374/921, 41%, P < 0.001) than African American (218/921, 24%) (Fig. 3A); this was the case for both the young and old age groups. Among patients older than 40 years, Hispanic patients (78/1798, 4%) were more likely than white patients (52/1798, 3%, P < 0.001) and white patients were more likely than African American patients (23/1798, 1%, P < 0.001) to present with cirrhosis due to cryptogenic/NAFLD/NASH (Fig. 3B). African American patients were significantly older (52 ± 8) when presenting with cirrhosis due to HCV than either Hispanic patients (49 ± 10, P = 0.003) or white patients (49 ± 8, P < 0.001) (Fig. 3C). Among patients older than 40 years, African American patients (235/1798, 13%, P < 0.001) and white patients (258/1798, 14%, P < 0.001) were more likely than Hispanic patients (122/1798, 7%) to present with cirrhosis due to HCV (Fig. 3C). Among patients younger than 40 years, Hispanic (23/219, 11%, P = 0.048) and white (34/219, 16%, P < 0.001) patients were more likely than African American patients (11/219, 5%) to present with cirrhosis due to HCV (Fig. 3C). African American patients composed a larger percentage of patients with cirrhosis due to autoimmune disease younger than 40 years than Hispanic patients (P = 0.012). Cirrhosis due to HBV in patients older than 40 years was more common in African American and white patients than in Hispanic patients (P < 0.001).
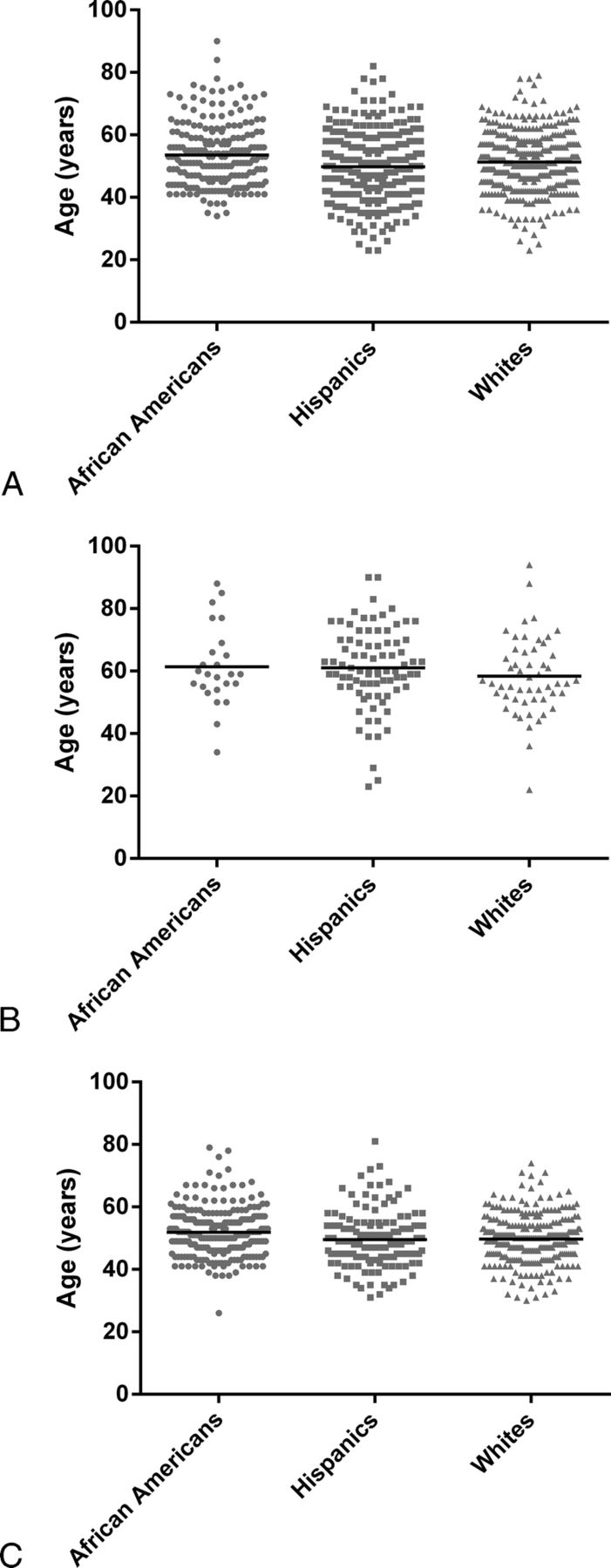
Cirrhosis in African Americans, Hispanics, and whites. Individual patients as a function of their age and ethnicity are shown. The black line indicates average age. A, In patients with alcoholic cirrhosis, it was 53.5 ± 10.0 for African Americans (n = 218), 49.8 ± 10.7 for Hispanics (n = 291), and 51.3 ± 9.3 for whites (n = 374) (there were differences in age between African Americans and either Hispanics [P < 0.001] or whites [P = 0.001]). B, in patients with NASH, NAFLD, or cryptogenic cirrhosis, average age was 61.4 ± 13.0 for African Americans (n = 24), 61.1 ± 13.0 for Hispanics (n = 83), 58.4 ± 12.2 for whites (n = 54). C, in patients with HCV cirrhosis, average age was 51.5 ± 8.1 for African Americans (n = 246), 48.7 ± 9.5 for Hispanics (n = 145), and 49.1 ± 8.0 for whites (n = 292) (there were differences in age between African Americans compared with Hispanics [P = 0.003] or whites [P < 0.001]).
A variety of medical disorders, including diabetes mellitus with and without end-organ damage, hepatocellular carcinoma, chronic kidney disease, and AIDS, were also noted (Table 2). Diabetes mellitus with and without end-organ damage and hepatocellular carcinoma were identified more commonly in patients older than 40 years (P = 0.037, P < 0.001, and P = 0.019, respectively). AIDS was more prevalent in cirrhotic patients younger than 40 years (P < 0.001). Varices were more prevalent in patients older than 40 years (P = 0.003). As explained previously, diabetes mellitus and AIDS had a significant correlation with age.
Mortality among patients was 32% (70/219) in the younger than 40 years age group (34 with alcoholic, 24 with HCV, 3 with autoimmune, 2 with cryptogenic/NAFLD/NASH, and 7 with other causes of cirrhosis), significantly greater than 11% (202/1798) in the older than 40 years age group (141 with alcoholic, 36 with HCV, 16 with cryptogenic/NAFLD/NASH, and 9 with other causes of cirrhosis) (P < 0.001). Of deceased patients younger than 40 years, 33 (38%) of 87 were white, 12 (39%) of 31 were African American, and 22 (25%) of 89 were Hispanic (P = 0.07 and P = 0.17 compared with white and African American patients, respectively). Of those older than 40 years, 89 (12%) of 715 were white, 61 (12%) of 519 were African American, and 46 (10%) of 461 were Hispanic.
Discussion
Here, we have studied a uniquely diverse cohort of patients with cirrhosis and identified associations between the age at which cirrhosis develops and ethnicity. We found that Hispanic patients were more likely to be younger when presenting with cirrhosis, whereas African American patients were more likely to be older when presenting with cirrhosis. Another novel finding was that alcoholic cirrhosis presented later in life in African American patients compared with Hispanics and whites.
Various correlations between ethnicity and causes of cirrhosis in young and old patients were apparent in our large and diverse patient sample, consistent with several epidemiological associations reported by smaller studies.14,15 Although the data raise the speculative possibility that there may be inherent genetic factors that could predispose to more rapid fibrosis progression in certain groups of patients, it is important to emphasize that hepatic fibrosis and cirrhosis are complex and that there are multiple potential levels of intrinsic cell and molecular interactions. Furthermore, environmental factors almost certainly play a critical role in the development of the cirrhosis phenotype and likely exhibit critical interplay with host factors. For example, Hispanic and white patients were more likely to have cirrhosis due to alcohol than African American patients. Bearing in mind environmental factors, it has been reported that among college students, Hispanic students were more than twice as likely as African American students to report episodic heavy drinking, 16 which in theory could lead to earlier development of cirrhosis. In addition, African American patients constituted most of the autoimmune cases of cirrhosis in younger patients. Previous studies have reported that African American patients have a poorer outcome and higher mortality due to autoimmune hepatitis compared with other ethnicities. 14
Among older patients, cryptogenic causes of cirrhosis were greatest in Hispanic patients, followed by white patients and then African American patients, consistent with previous studies. 15 The prevalence of type 2 diabetes and average body mass index is similar in Hispanic patients and African American patients, but the former have the greatest annual increase in body mass index of all ethnicities in the United States, and Hispanic patients also have greater hepatic steatosis. 17 Thus, genetic factors are likely to play a role in making Hispanic patients more susceptible and/or African American patients less susceptible to NAFLD, and consequently cryptogenic/NAFLD/NASH cirrhosis.18,19
The prevalence of HCV seems to be the greatest in African American patients, compared with all other ethnic groups in the United States, 20 yet in our study, cirrhosis caused by HCV presented at an older age in African American patients than in either Hispanic or white patients. It is possible that environmental factors may explain this finding, such as differential age at exposure to HCV, but epidemiologic data supporting this possibility are lacking. Rather, while previous data have demonstrated that African American patients have decreased viral clearance and decreased response to antiviral therapy, previous data also suggest slower progression to cirrhosis.20,21 On the other hand, Hispanic patients presenting with cirrhosis due to HCV at a younger age may be due to more aggressive and faster disease progression in this ethnic group. 22
In addition, the presence of medical comorbidities varied with age. For example, it was remarkable that patients with AIDS were more likely to have cirrhosis at a young age (Table 1). This may be related to the biology of fibrogenesis in these patients, in which it has been demonstrated that patients coinfected with a hepatitis virus have a more accelerated fibrosing process. 23 Diabetes mellitus both with and without end-organ damage, as well as hepatocellular carcinoma, was more often identified in older cirrhotic patients; the finding of hepatocellular carcinoma at an older age would be expected because hepatocellular carcinoma takes time to develop.
Interestingly, the in-hospital mortality rate was higher among younger patients than in older patients, although mortality did not seem to differ among ethnic groups. Although this finding is surprising, it is consistent with the concept that younger patients had more advanced disease at the time of hospital admission than older patients. Furthermore, the finding that MELD scores were higher in younger patients than in older patients is consistent with this possibility. We are unable to explain this surprising finding, but we speculate that either the biology of their disease is different than that of older patients or that they come to hospital admission later in the course of their disease.
Several gene association studies in humans have uncovered genes contributing to hepatic fibrosis. 24 In studies focused on hepatitis C, the lipopolysaccharide receptor toll-like receptor (TLR) 4 was identified to be a profibrotic protein; there was no association with progression of other forms of CLD. 1 Mice with a targeted deletion of the TLR4 are largely protected from experimental fibrosis. 25 More significantly, a genome-wide screen identified 7 SNPs, termed the cirrhosis risk score, to be associated with the progression of liver disease. 26 Recently, studies have demonstrated an inverse correlation between 25(OH)-vitamin D levels and the commencement of fibrosis. 27 The 7 single nucleotide polymorphisms, representing 7 genes (AP3S2, AQP2, AZIN1, DEGS1, STXBP5L, TLR4, and TRPM5), are the best tool for genetic prediction of liver fibrosis in hepatitis C infection.28,29 Whether this score can predict fibrosis progression in non-HCV liver disease is unclear. Furthermore, 2 large-scale genome-wide association studies identified 3 novel markers showing strong association with liver fibrosis. These were the DEAD box polypeptide 5 (DDX5) and carnitine palmitoyltransferase 1A (CPT1A) proteins, involved in the development of liver fibrosis in subjects with HCV, 30 and the integrin β5 (ITGB5) protein, associated with liver fibrosis in HCV and HCV/human immunodeficiency virus patients. 31 Complement factor 5 may also be a cause for the development of liver fibrosis. 32 Clearly, there are genetic links to the development of cirrhosis in some patients.
Additional studies in mice have identified genes or gene families in which mutations are associated with the development of hepatic fibrosis. Included are a phospholipid transporter ABCB4 (MDR2/MDR3) necessary for proper bile formation, 33 an overexpressed proliferative protein of the PDGF family (Pdgf-A, Pdgf-B, Pdgf-C),34–36 TGF-B1 a promoter of ECM protein synthesis in hepatic stellate cells, 37 LIM homeobox protein LHX2, 38 the taurine transport protein TAUT, 39 and the antiapoptotic protein Bcl-xl. 40 Furthermore, a locus has been mapped to chromosome 15 for susceptibility to hepatic fibrosis. 41
Although a remarkable strength of this study was that we examined an extremely large and ethnically diverse population, we recognize several limitations of this work. First, our study was retrospective, and certain data elements could not be identified. However, patients lacking key data (ethnicity and cause of cirrhosis) were excluded from the study. In addition, as emphasized previously, we cannot exclude the possibility that certain ethnic groups had specific environmental influence(s) that may have predisposed them to liver disease at a younger age. However, with regard to ethanol consumption and the acquisition of HCV, the most common causes of liver disease in our cohort, we are not aware of definite epidemiologic factors in the United States that predispose certain groups to develop cirrhosis at a younger age.42,43
A further consideration with the current study is that we focused on patients admitted to the hospital. Although most of these patients were also followed in outpatient clinics, it is possible that inpatients had more advanced disease than outpatients. If anything, the focus on inpatients would have skewed the results toward finding patients with cirrhosis at an older age or at a more decompensated stage. It should also be emphasized that by virtue of the safety net status of the Parkland Health and Hospital System, there do not appear to be disparities to access to care among ethnic groups. Thus, we doubt that there is bias toward 1 ethnic group or another with regard to hospital admission and inclusion in our patient cohort. Finally, the study was performed in a single institution, raising the concern that our findings may not be generalizable to other health care systems. However, the wide diversity of the population studied here is a unique strength of the study, and this element raises the possibility that our study findings are likely in fact to be more generalizable to the entire US population than studies from only tertiary or other focused health care systems.
In conclusion, our data suggest that ethnicity may play an important role in the fibrogenic process leading to cirrhosis, and raises new questions regarding ethnicity and age in patients with cirrhosis. The correlations here may become crucial in identifying risk factors for cirrhosis in certain patient populations. We speculate that further studies may identify ethnic and perhaps genetic factors that are important in the fibrogenic response and development of cirrhosis.
Footnotes
Acknowledgments
The authors thank Changxing Chen from Southern Methodist University for statistical analysis assistance. The work was supported in part by the NIH (grant DK 098819 to D.C.R.).