
Abstract
Background
Hemoglobin/hematocrit decreases in hospitalized patients without evidence of obvious gastrointestinal (GI) bleeding are common and often attributed to GI lesions. We hypothesized that inpatients with hematocrit declines without clinically overt GI bleeding have distinct clinical features and hence aimed to evaluate this clinical syndrome.
Methods
We evaluated consecutive GI consults for patients with a decrease (drop) in hematocrit. Patients with documented prior GI bleeding, melena, hematochezia, hematemesis, and melenemesis were excluded. Hematocrit drops were calculated from preconsult zenith and nadir values and identified as acute (within 7 days), intermediate (7–30 days), or remote (beyond 30 days) on the basis of the shortest time to a hematocrit drop of at least 6%.
Results
We identified 101 patients having hematocrit drops without clinical evidence of GI bleeding. Seventy-six patients (75%) had an acute drop in hematocrit with a mean decline of 9.5%, whereas the 25 patients with an intermediate or remote drop in hematocrit had a mean decline of 12.5%. Endoscopic evaluation was performed in 55 patients. Five patients (5%) had a lesion consistent with GI bleeding; identified lesions included ischemic colitis, duodenal ulcer, esophageal varices, and postsphincterotomy ulcer. In the remaining 96 patients, a clinical explanation for the hematocrit drop was identified in 56 patients (58%), most commonly attributed to sepsis/shock, volume shifts, and postprocedure bleeding.
Conclusions
Hematocrit drops without visible GI bleeding were uncommonly caused by bleeding intestinal lesions, contrary to current dogma. Non-GI explanations for hematocrit drops were often identified, although the cause of hematocrit drop remained unexplained in many patients.
Drops in hemoglobin/hematocrit are common among inpatients and are a concern for a wide variety of clinicians. 1 Such changes are attributable to an array of pathological, laboratory, and iatrogenic processes, among which include gastrointestinal (GI) tract bleeding.1–6 In situations in which declines are neither readily explained nor manifest as visibly passed blood from the GI tract, gastroenterology consultants are frequently asked to evaluate for the presence of intestinal lesions that would explain the hematocrit change.
The prognostic significance of a decrease in hematocrit in the absence of sentinel GI bleeding is incompletely understood. The importance of hematocrit drop (or its equivalent in transfusion of red blood cells) on GI-related outcomes such as mortality and rebleeding has been demonstrated only with clinically overt bleeding (hematemesis, melena, hematochezia).7,8 When no overt signs of intestinal bleeding exist, attributing hematocrit changes to GI bleeding is confounded by the complexity of intestinal blood degradation. For example, it is well known that blood is a cathartic inducing gut peristalsis, and therefore, any GI bleed should be visibly apparent in stool. 9 In contrast, smaller amounts of blood can be digested by intestinal enzymes or bacteria and may not become readily evident to clinicians or patients.9–12 Hence, although melena, hematemesis, and hematochezia are specific for GI bleeding, they are insensitive indicators for bleeding of less than 100 mL/d. Whether such nonvisualized GI bleeding can be associated with clinically meaningful declines in hematocrit remains unknown.
In this study, we hypothesized that a drop in hematocrit without clinically overt GI bleeding would be uncommonly associated with the discovery of any meaningful GI tract pathology. Moreover, we postulated that the change in hematocrit should be explainable by other concomitant clinical factors in most instances; hence, this patient cohort would likely have unique clinical features. Our aim was to determine how often a “decline in hematocrit” resulted in a diagnosed bleeding GI lesion and, if no GI bleed was determined, what caused the hematocrit drop. Secondarily, we aimed to determine how many encounters led to endoscopy and the clinical factors associated with endoscopic evaluation.
Materials and Methods
This cohort study focused on hematocrit levels in inpatients whom the gastroenterology consult service was asked to evaluate for possible GI bleeding, typically to perform endoscopy in search of a bleeding lesion. The cohort was identified from 5510 total consultative encounters at Parkland Memorial Hospital between August 1, 2006, and July 31, 2009. The primary diagnosis leading to the consult was collected; additionally, for all patients with any form of GI bleeding, an extensive data set was prospectively collected; data pertaining to the hospital admission were abstracted and entered into a GI bleeding registry database (Microsoft Access; Microsoft Corporation, Redmond, WA). Captured registry data include multiple clinical and historical features, American Society of Anesthesiologists physical status score (1–3, normal to severe; 4–5, life threatening to moribund), medications, as well as laboratory and endoscopic data (endoscopic diagnosis, stigmata of recent or active hemorrhage, and therapies). By design, a bleeding intestinal lesion or a lesion with stigmata of recent bleeding in any given case is designated as the primary diagnosis. Any concomitant lesions/diagnoses were deemed secondary problems that were not the cause of hemorrhage. The attending physician and one of the study authors (ie, by visualization of endoscopic images) verified the presence of a primary bleeding lesion. Data entry into the database was double key entered.
Hematocrit change at the time of consult was calculated for each encounter and categorized according to the acuity of the drop. Hematocrit values in this study are expressed as standard liters per liter percentage, and all changes in hematocrit are reported as absolute differences. Raw maximum hematocrit changes were calculated for each period of within a week, within a month, and beyond 1 month. The raw differences were derived from the zenith hematocrit within each period and the lowest subsequent preconsult hematocrit. Hematocrit drops for each encounter were then classified as acute (<1 week), intermediate (between 1 week and 1 month), or remote (beyond 1 month) on the basis of the shortest period within which hematocrit changed at least 6% (the minimum arbitrary amount of expected hematocrit change with 2 U of packed red blood cells) or else the shortest time encompassing the entire hematocrit change if the maximum difference was less than 6%. 13 An algorithm identified study encounters through non–case-sensitive key words found within consult descriptions detailing hematocrit declines in the absence of GI bleeding (decline, drop, HCT, hematocrit, crit, hemoglobin, anemia).
Patients with any active GI bleeding or with encounters referencing prior GI bleeding were excluded (melena, hematochezia, bright red blood per rectum, hematemesis, melenemesis, upper GI bleeding, lower GI bleeding, “coffee ground” emesis). Consult encounters and complete inpatient medical records were reviewed for outcomes of GI intervention, attributable pathological GI lesions causing hematocrit changes, and otherwise explainable reasons for hematocrit drops. Patients were also excluded if hospital encounters were unverifiable because of incorrect identification of information and in situations in which 2 or more of the following key clinical information sets were missing or incomplete on chart review: clear documentation of the absence of visible GI bleeding and/or a statement about an isolated hematocrit drop, medical comorbidities, medications present on admission, and incomplete GI consultation/endoscopy records for the encounter.
Intestinal lesions were determined to be bleeding sufficiently enough to cause hematocrit drops based on the final impression of the attending endoscopist during the consult encounter and secondarily by the GI consult attending in cases in which endoscopy was not performed. Endoscopic lesions consistent with bleeding were lesions actively bleeding at the time of endoscopy and lesions with stigmata of bleeding (protuberant vessel, red wale signs, etc). Comorbid diseases recorded for all encounters include type 1 and type 2 diabetes mellitus, coronary artery disease, presence of prior myocardial infarctions, systolic and diastolic congestive heart failure (CHF), atrial fibrillation/flutter, peripheral vascular disease, hypertension, emphysema, asthma, prior strokes (hemorrhagic and ischemic), chronic kidney disease, (including end-stage renal failure), gastroesophageal reflux disease, peptic ulcer disease, cirrhosis, varices (esophageal and gastric), prior intraperitoneal surgeries, nondermatologic neoplasms, as well as human immunodeficiency virus seropositivity.
Fecal occult blood tests (FOBTs) were all guaiac-based tests, performed with Hemoccult II SENSA (Beckman Coulter, Brea, CA).
Statistical Analysis
Microsoft Excel was used to determine descriptive statistics, and Windows Kwikstat SDA 7 (Texasoft) was used for 2-tailed t test analysis. Results of hematocrit drops were presented as mean (SD). A 2-tailed t test was used to compare the mean hematocrit drop between the patients with identified bleeding GI lesions and those who had no GI bleeding. A P value of less than 0.05 was considered statistically significant.
Results
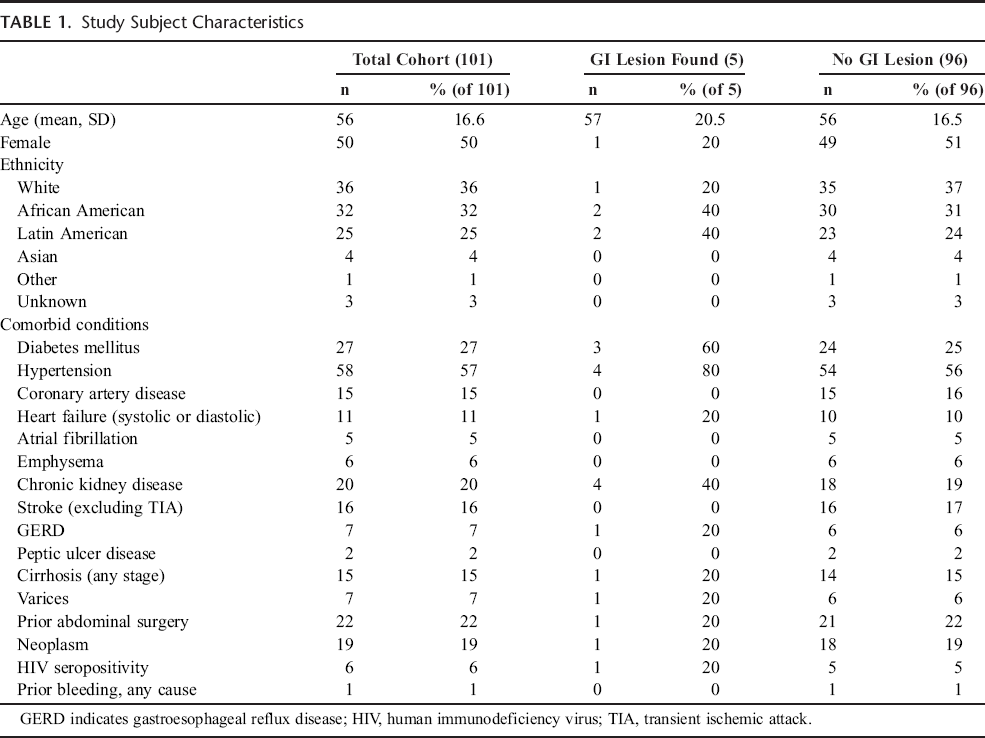
We identified 101 patients with a drop in hematocrit whom the gastroenterology service was asked to evaluate (Fig. 1). Demographic characteristics of the study cohort were typical of inpatients at Parkland Memorial Hospital (Table 1), including equivalent numbers of men and women and a high proportion of Hispanic and African American patients. Comorbid conditions were prominent among the patients in the study population (Table 1), as 27% of the patients in the study had diabetes mellitus and more than half of the cohort had hypertension. Cirrhosis was present in 15% of the patients; and chronic kidney disease, in 20%. Prior intra-abdominal surgical procedures including bowel procedures, cholecystectomy, appendectomy, and trauma-related repair were common.
Study Subject Characteristics
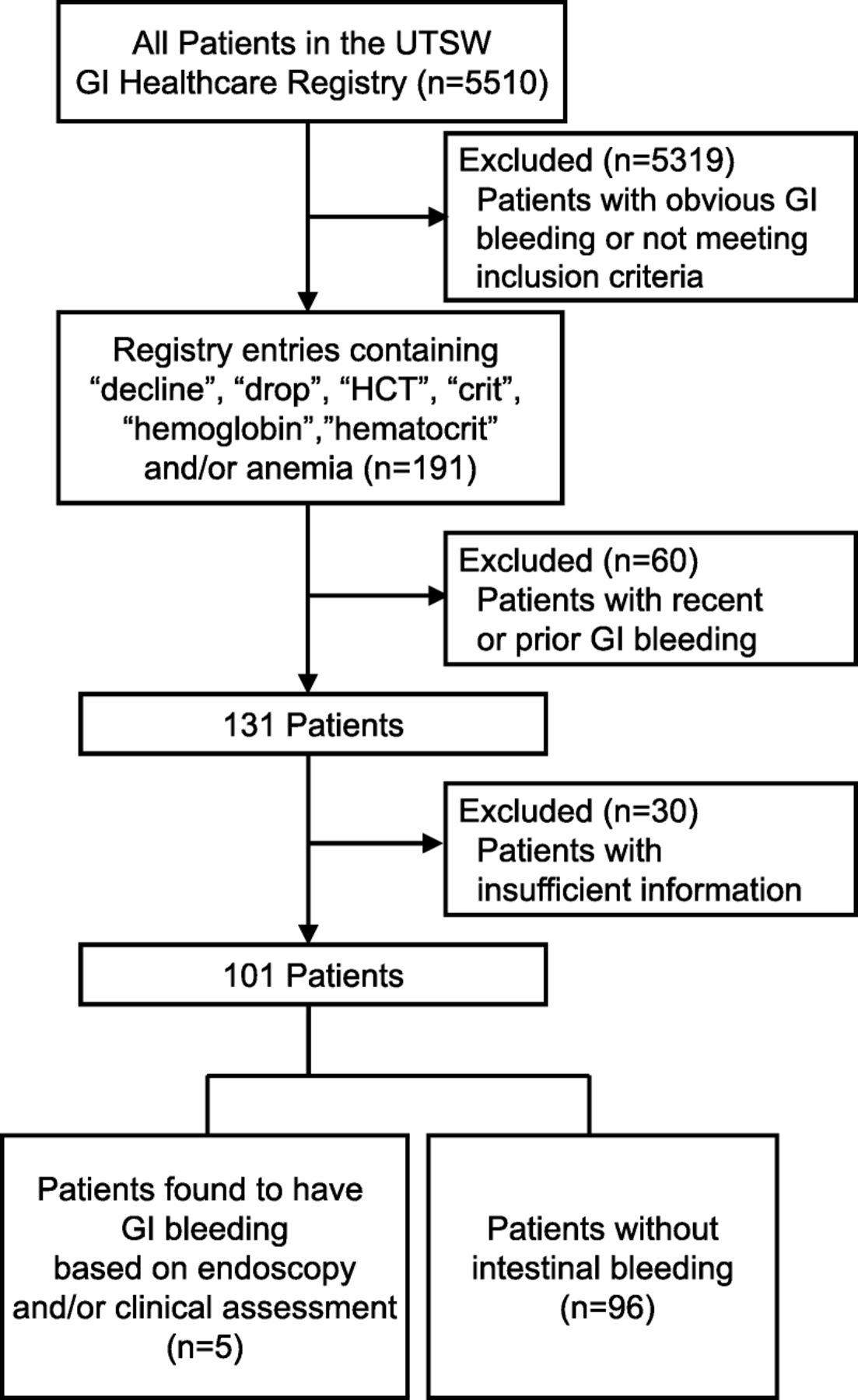
Patient cohort. The flow of patients included in the study is shown.
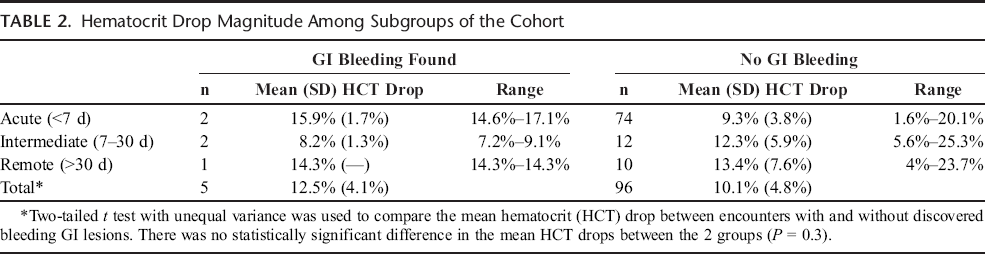
Most of the patients in the cohort had an acute drop in hematocrit (Table 2), with a mean change of 9.5%. Anemia, defined as a hematocrit of less than 36%, was present at the time of consult for all but 1 patient, who had a hematocrit of 42.6%. Among the 5 patients with identified GI bleeding pathology, 2 had an acute hematocrit drop, with a mean change of 15.9% (Table 2). Hematocrit drops among the patients with intermediate or remote changes tended to be slightly larger overall (12.5%), particularly for those with hematocrit drops occurring beyond 30 days (13.5%).
Hematocrit Drop Magnitude Among Subgroups of the Cohort
A total of 56 patients underwent endoscopy in search of GI tract lesions (Table 3). Four of the 5 patients with GI bleeding lesions underwent endoscopy during the consult encounter. Findings included bleeding from ischemic colitis, duodenal ulcer with visible vessel, postsphincterotomy bleed, and grade 2 to 3 esophageal varices with no stigmata of recent bleeding but with hematin present in the stomach. The last patient who had a bleeding GI lesion but who did not undergo endoscopy was determined by the consultation service to have likely bled from ischemic colitis on the basis of medical history and suggestive concurrent imaging. Of the group without identifiable bleeding GI lesions, 52 (54%) of 96 underwent esophagogastroduodenoscopy (EGD) and/or colonoscopy, with combined EGD and colonoscopy occurring in 25 encounters (Table 3). Small bowel endoscopy and enteral radiography were all unremarkable, although infrequently performed.
Frequency of EGD and Colonoscopy Among the Study Cohort

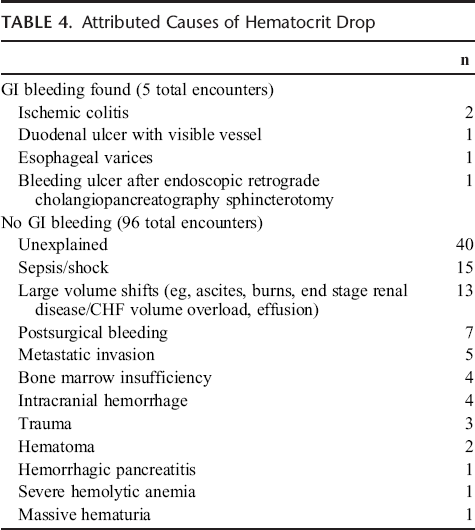
Attributed causes for the drop in hematocrit among the cohort patients are shown in Table 4. The cause of bleeding varied widely for those in whom a culpable bleeding lesion was identified (Table 4). The most common identified causes of a hematocrit drop not due to a GI tract lesion were sepsis/shock (15 patients); postsurgical bleeding (7 patients); and large volume shifts (13 patients) associated with chronic kidney disease, CHF, pleural effusions, ileus, ascites, or burns. A variety of other disorders accounted for hematocrit drops in the patients without GI tract lesions; these included bleeding from metastatic tumor invasion, bone marrow suppression/insufficiency (due to medication, radiation), and intracranial bleeding (Table 4). Two large hematomas were identified: 1 patient with a groin hematoma and another with a retroperitoneal hematoma. A total of 40 patients (42%) had no clear explanation for the change in hematocrit.
Attributed Causes of Hematocrit Drop
For 41 (79%) of 52 patients who underwent endoscopy but had no GI bleeding discovered, GI abnormalities were identified but were not believed to be the primary cause of the documented hematocrit change. Lesions found were polyps, trivial erosions or inflammation, small esophageal varices without stigmata of bleeding, small internal hemorrhoids without bleeding stigmata, and/or diverticulosis. In 26 of these patients, an alternative explanation for the hematocrit drop was present; however, in 26 others, the cause of hematocrit drop remained unexplained.
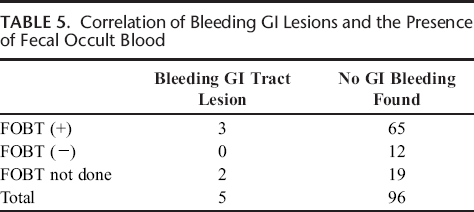
A high proportion of patients had FOBTs performed, and these were positive at a high frequency (Table 5). For example, 85% of the patients (68/80) in whom FOBTs were performed had a positive result. Of the patients who had a positive FOBT result, 40 (59%) underwent EGD and/or colonoscopy; bleeding lesions were identified in 3 patients. Of note, endoscopy was performed in 4 of 12 patients with a negative FOBT result.
Correlation of Bleeding GI Lesions and the Presence of Fecal Occult Blood
Antiplatelet agents (aspirin, nonsteroidal anti-inflammatory drugs) were concurrently taken by 2 patients with identified bleeding GI lesions. No patient with an identified bleeding GI lesion received clopidogrel or anticoagulation (lovenox, coumadin, heparin, dalteparin). Of the 96 patients who did not have a GI tract bleeding lesion clearly identified, anticoagulants were used by 16 patients (17%) and antiplatelet agents (aspirin, clopidogrel, COX-2 inhibitors, nonsteroidal anti-inflammatory drugs) were used by 25 patients (26%).
Discussion
We have attempted to describe a clinical syndrome of hematocrit drop in the absence of visible GI bleeding in a cohort of patients deemed by their primary providers to have a GI tract lesion responsible for the drop in hematocrit. This entity has been underexamined despite being pervasive among inpatients. 1 We found that, in this scenario, identification of a culprit bleeding GI lesion was uncommon (5% of 101 patients). That any bleeding GI lesion was identified in this cohort argues against our hypothesis that, without visible bleeding, a hematocrit drop would be unlikely to be associated with a culpable GI bleed. However, identification of an obvious bleeding source was uncommon.
A previous study has also examined hematocrit declines among hospitalized patients, but it differed from our study in several ways. 1 Most notably, our cohort identified patients from referrals to the gastroenterology service rather than from general medicine ward encounters. Consequently, we included a broader range of inpatient acuity and primary hospital services that would otherwise be excluded by the previous study (eg, patients encountering surgery, trauma, invasive endoscopic procedures, blood transfusions, as well as other causes of anemia such as hemolysis and chronic renal failure). 1
Importantly, the patients in our study were identified only after primary practitioners asked for consultative input subsequent to a decline in hematocrit despite an absence of overt signs of GI bleeding. Implicit in this design, there was almost certainly a bias on the part of practitioners that their patients had a GI tract bleeding lesion. We suspect that a further part of this bias stems from the fact that many of these patients were found to have fecal occult blood in their stool (Table 3). It is further important to recognize that not all instances of hematocrit decline came to the attention of the GI consultants. Thus, the group described here is highly problematic but is nonetheless representative of hospitalized patients. Perhaps the key message here is that many of these patients had clinical disorders that clearly explained their drop in hematocrit (Table 4). Thus, one of our major conclusions is that providers must assess the patient's entire clinical picture and be cognizant of clinical disorders besides GI bleeding that may account for a decline in hematocrit.
A high proportion of the patients in our cohort underwent endoscopy. Given the overall acuity of disease in this cohort, we speculate that this led to the identification of many trivial, nonbleeding GI lesions. Taken at face value, these low-risk lesions would be unlikely to have caused significant intestinal blood loss that would manifest as a significant hematocrit drop. However, it is possible that such lesions may contribute in some manner to hematocrit change but likely only to a fraction of the observed decline. Although we were able to exclude prominent bleeding lesions, we also cannot exclude the possibility that any delays in endoscopic evaluation altered the appearance of identified lesions. Finally, it should be emphasized that it is possible that bleeding lesions were missed, although if this occurred, it was likely infrequent.
The magnitude of hematocrit change among our cohort was notable, averaging approximately 13% overall. The majority of patients (75%) had a hematocrit drop within 7 days of GI consultation. There was no statistically significant difference in the mean hematocrit drops between all patients with and without identified bleeding GI lesions. The complex hemodynamic status of some of the patients in our study makes speculation inherently difficult about the true contribution of GI lesions to the observed hematocrit drop magnitudes. Our low sample size prevented us from statistically analyzing individual time-striated subgroups. Further studies using a larger population and strict fluid balance records may better expound on the association of various GI lesions and hematocrit change.
A large proportion but not all of the cohort patients underwent FOBT. Although we wish to be cautious in speculating about the reason for this finding, we wonder if FOBT results and/or the presence of anemia contributed to the concerns of the primary services for significant intestinal bleeding. Inconsistent FOBT use among cases of hematocrit drop highlights the inadequacy of guidelines for evaluating isolated hematocrit changes. Fecal occult blood tests are, by design, sensitive tests able to detect passage of intestinal blood as little as 5 to 10 mL/d.12,14 Alone, FOBTs cannot distinguish between large-volume GI bleeding and occult bleeding, making them seemingly less ideal for the identification of a significant intestinal bleed. On the basis of our study, we cannot comment on the prognostic value of FOBTs for GI bleeding among situations of isolated hematocrit drop; however, this would be an interesting area for future investigation.
In summary, we have demonstrated that, in inpatients with large drops in hematocrit without evidence of visible GI bleeding, the likelihood of finding a bleeding GI lesion is low. Nonetheless, a small proportion of patients were found to have important bleeding intestinal lesions. Further studies in other populations, including strict fluid balance records, and in which all patients undergo endoscopy, could help to better clarify our understanding of a possible causal association between large drops in hematocrit and bleeding intestinal lesions.