
Abstract
Purpose
Type 2 diabetes mellitus (type 2 DM) and maturity-onset diabetes of the young present some similar clinical and biochemical characteristics that make them difficult to differentiate. Currently, the polymorphism T130I (rs1800961) in the HNF4A (hepatocyte nuclear factor 4A) gene has been described as a risk factor to type 2 DM and shows an autosomal dominant inheritance pattern associated to β-cell function decrease. The aim of the present work was to characterize the phenotypic profile of the T130I carrier and noncarrier relatives included in 3 unrelated families.
Methods
We studied GCK, HNF1A, and HNF4A genes by polymerase chain reaction and sequencing in 3 unrelated subjects from Valladolid, Spain, in which maturity-onset diabetes of the young was suspected. We collected genetic, clinical, and biochemical data from these subjects and their relatives in order to check the presence of the T130I polymorphism.
Results
The heterozygous T130I mutation was the unique functional gene variation that could explain diabetes phenotype. We observed significant differences in glucose metabolism, lipid profile, and Homeostasis Model Assessment index when we compared T130I mutation carriers and noncarriers. Diabetes diagnosed in T130I mutation carriers was related to stressful situations in an earlier age and tightly associated with gestational diabetes. Fasting plasma glucose and HbA1c levels increased with age in all carriers (r = 0.69 and r = 0.66, P < 0.01), respectively.
Conclusions
Our study supports the T130I variant in HNF4A as a major susceptibility genotype associated with early-onset type 2 DM. Healthy carriers of this mutation require a stricter control in the population of central Spain.
Type 2 diabetes mellitus (type 2 DM) is a complex metabolic condition led by a hyperglycemic status. 1 Although obesity and insulin resistance are frequently associated to this disease, it is sometimes difficult to discriminate it from other types of diabetes. 2 Type 2 DM is usually diagnosed in subjects older than 25 years and can be associated to an unexplained familiar predisposition similar in some extent to that reported in maturity-onset diabetes of the young (MODY).
Multiple studies have tried to clarify the genetic variants implicated in the increased risk of type 2 DM. Genome-wide association studies have indentified at least 40 loci associated with type 2 DM. Chromosomes 1q, 2q, and 20q seemed to be more closely related with the disease.3–6 More accurate linkage studies have been focused in the hepatocyte nuclear factor 4α (HNF-4α) as a possible candidate because of its localization in chromosome 20q and the reporting evidence on the implication of its P1 and P2 promoters in the development of type 2 DM.7–11
Maturity-onset diabetes of the young is a hereditary subtype of non–insulin-dependent diabetes that represents about 1% to 2% of all diabetes cases and is associated to β-cell dysfunction. 12 There are at least 6 MODY types, 13 being the most frequent the MODY1, MODY2, and MODY3 caused by pathogenic mutations in HNF4A,14,15 GCK,16–18 and HNF1A19,20 genes, respectively. MODY1 seems to be much less prevalent than the other subtypes and is characterized by a slightly higher age at diagnosis. 21
HNF-4α is a transcription factor, member of the steroid hormone receptor superfamily, coded by the HNF4A gene that is expressed in the liver, pancreatic islets, kidneys, and small intestine. HNF-4α acts as a homodimer that regulates the expression of genes involved in glucose and lipid metabolism.22,23
Recently, some studies in different populations have reported that the T130I mutation in the HNF4A gene (rs1800961) is associated with an early onset of type 2 DM,24–26 and a genome-wide association study meta-analysis has reported its relationship with high-density lipoprotein cholesterol (HDL-C) levels. 27
In this study, we performed genetic analysis in 3 unrelated subjects from Valladolid (Castilla y León, Spain) we suspected had MODY. Once confirmed that the T130I mutation in the HNF4A gene was the only molecular abnormality detected, we studied the relationship between the T130I HNF4A polymorphism and the glucose/lipidic metabolism abnormalities in T130I carriers and a control group comparable in sex, age, and body mass index (BMI).
Materials and Methods
Patients
Two unrelated men (subjects 1.1 and 3.1) and 1 woman (subject 2.1) were treated in the Diabetes Unit of the University Clinical Hospital of Valladolid (Spain) on different dates because of a presumptive diagnosis of MODY. The patients had an early-onset type 2 DM (average age, 40 years), normal BMI (<25 kg/m2), and familiar diabetes with a consistent pattern of autosomal dominant inheritance. Clinical records included fasting analysis for insulin, C-peptide, glucose, HbA1c, lipid profile, and an oral glucose tolerance test (OGTT). Moreover, glutamic acid decarboxylase antibody was measured in all affected individuals, and the increased risk for diabetes (prediabetes) or normoglycemia categories were established according to the criteria of the American Diabetes Association 2012. 28 In addition, a possible diabetes neuropathy, retinopathy, or nephropathy was ruled out by physical examination, by eye fundus exploration, and by microalbuminuria test (data not shown).
Control Subjects
The nondiabetic control group was selected through mutation-negative relatives (4 subjects) and 23 unrelated subjects consecutively selected in outpatient clinical practice. The control group was selected to be comparable in age, sex, and BMI to the patients. None of them possessed the mutation being studied.
Biochemical Variables
Plasma concentration of glucose was analyzed by an automated glucose hexoquinase method (Roche Diagnostics, Geneva, Switzerland). Insulin and C-peptide in serum were measured by electrochemiluminescence immunoassay (Roche Diagnostics), and HbA1c was measured by turbidimetric inhibition immunoassay standardized to NGSP quality criteria. Values are reported in percentages (NGSP/DCCT [Diabetes Control and Complications Trial] units) and mmol/mol (SI).
Dna Extraction
All the blood samples were extracted by a venipuncture standard technique and were sent to the Molecular Medicine Unit of Salamanca (Faculty of Medicine, University of Salamanca-IBSAL). There, high-molecular-weight DNA was obtained from peripheral leukocytes carrying out an isolation procedure and cell lysis using the Fornace buffer (0.25 M sucrose, 50 mM Tris-HCl pH 7.5, 25 mM KCl, 5 mM MgCl2), the chelating EDTA (0.5 M, pH 8), proteinase K 20 mg/mL (AppliChem, Darmstadt, Germany), and sodium dodecyl sulfate (1%). The mixture was incubated at 55°C for 16 hours; we then proceeded to the extraction and purification of the DNA by treating it with phenol-chloroform (AppliChem), chloroform (Panreac Quimica S.L.U., Barcelona, Spain), absolute ethanol, and 70% ethanol. Finally, the DNA was resuspended in sterile ddH2O. The extracted DNA was stored at −80°C until analyzed.
Mutation Detection
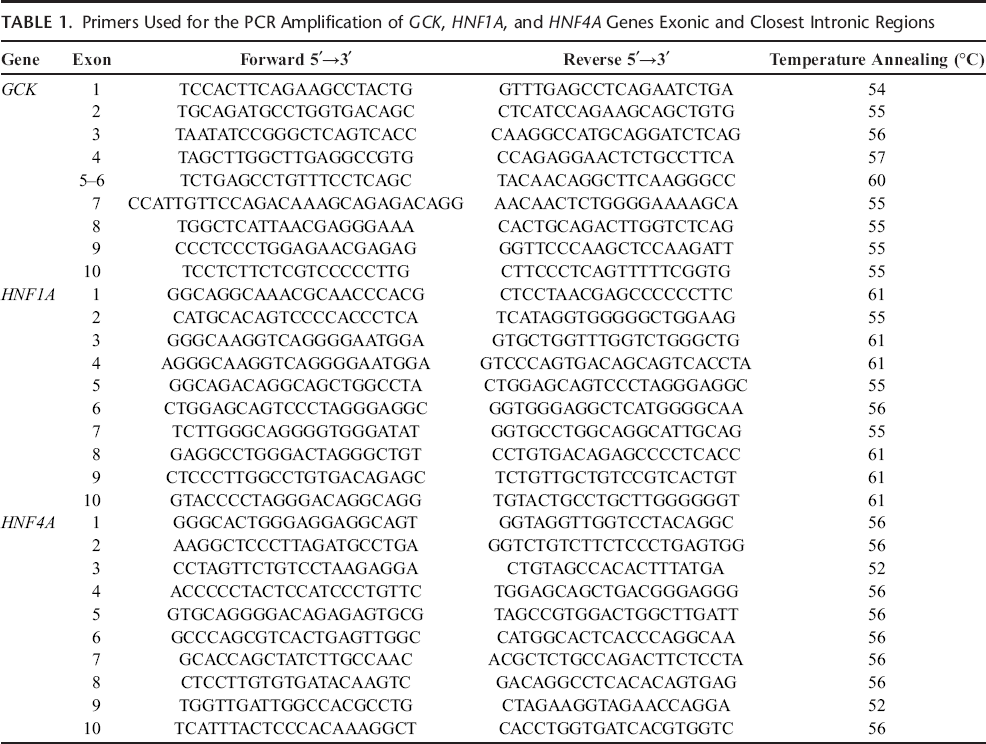
Bearing in mind the patients did not have a clear profile of a concrete type of MODY, we decided to analyze the 3 most frequently mutated genes GCK, HNF1A, and HNF4A. For this, we studied all the exons and the closest intronic regions by using the polymerase chain reaction (PCR). The program used for the amplification consisted of 35 cycles of denaturation at 95°C for 30 seconds, annealing of primers for 30 seconds, and primer extension at 72°C for 30 seconds. All amplification reactions were performed in an automatic thermocycler (Life Technologies-Invitrogen, Carlsbad, CA) (Table 1).
Primers Used for the PCR Amplification of GCK, HNF1A, and HNF4A Genes Exonic and Closest Intronic Regions
The amplified fragments were separated by horizontal electrophoresis through a 2% agarose gel (Gel Company Inc, San Francisco, CA) prepared with TBE buffer (Tris 0.044M, 0.044M boric acid, 1.0 mM EDTA, pH 8.3) and stained with SYBR Safe DNA Gel Stain (1:10,000; Life Technologies-Invitrogen). Finally, PCRs were purified with the PureLink PCR Purification Kit (Life Technologies-Invitrogen) and sequenced at the DNA Sequencing Service of the University of Salamanca (Technelysium, South Brisbane, Australia). Sequences were analyzed with the Chromas Lite 2.1 program and compared with the genomic sequences published in the databases.
Data Analysis
The categorical data were described using frequencies and percentages.
Bivariate analysis of the main variables was performed in order to determine differences between patients with and without the mutation. Furthermore, we carried out 2 × 2 contingency tables using the Fisher exact or the χ2 tests to evaluate significant differences in frequencies for categorical variables. The parametric t test was used to compare quantitative data. Those quantitative variables with a nonparametric distribution were analyzed with the Mann-Whitney U test. The Spearman correlation method was used to study a possible linear relation between the age and the HbA1c and basal glucose. Multivariate analysis (multiple linear regression) was also conducted to control for sex, age, and BMI.
All analysis were carried out using the Statistical Package for Social Sciences version 20.0 (SPSS, Chicago, IL) and Stata 11.0 (College Station, TX). P < 0.05 was considered statistically significant.
Ethical Principles and Data Collection
A standardized questionnaire was used to collect the clinical and laboratory data. Clinical features were recorded after the patients’ visit to the hospital.
This study adheres to the principles that govern biomedical research involving human subjects. Prior informed consent was obtained from the participants or from their parents. The private and confidential collection of data was ensured.
Results
Subject 1.1 (family A) was diagnosed at 48 years old after a myocardial infarction that required temporary insulin treatment. At present, he is undergoing treatment with metformin 850 mg/8 h (HbA1c 6.9%). Subject 2.1 (family B), at 40 years of age, was referred to the Diabetes Unit after diabetes decompensation secondary to corticoid therapy. She is currently undergoing treatment with metformin 850 mg/8 h and glicazide 120 mg/24 h (HbA1c 8%). Subject 3.1 (family C) was diagnosed at 40 years of age. He is being treated with metformin 850 mg/8 h and glicazide 60 mg/24 h (HbA1c 6.8%). He was referred to the Diabetes Unit from the primary care physician because of his young age at diagnosis and BMI of less than 25 kg/m2.
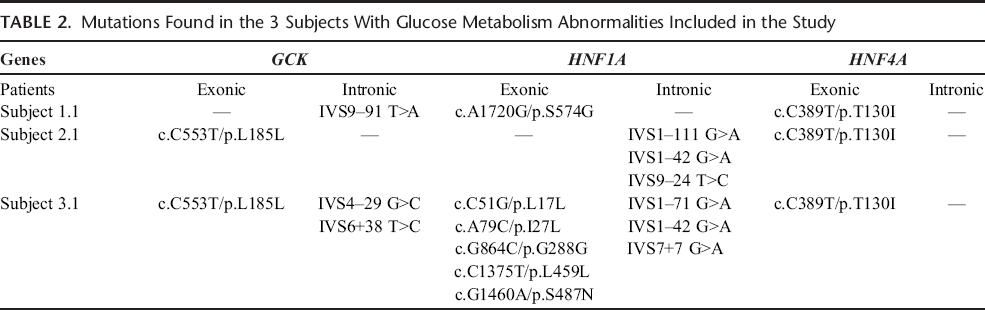
After performing the analysis of GCK, HNF1A, and HNF4A genes, we observed that the 3 patients were carriers of the HNF4A T130I mutation in heterozygosis, the only MODY mutation associated to the diabetes phenotype. Thus, other MODY pathogenic mutations were ruled out (Table 2). Therefore, we recruited and studied all closest relatives, whenever possible, studying the glucose metabolism parameters (fasting insulin, C-peptide, glucose, HbA1c, and OGTT), the lipid profile (total cholesterol, low-density lipoprotein cholesterol [LDL-C], HDL-C, ApoA, ApoB), and the clinical features that could be related to the T130I mutation in the HNF4A gene (Fig. 1, A–C).
Mutations Found in the 3 Subjects With Glucose Metabolism Abnormalities Included in the Study
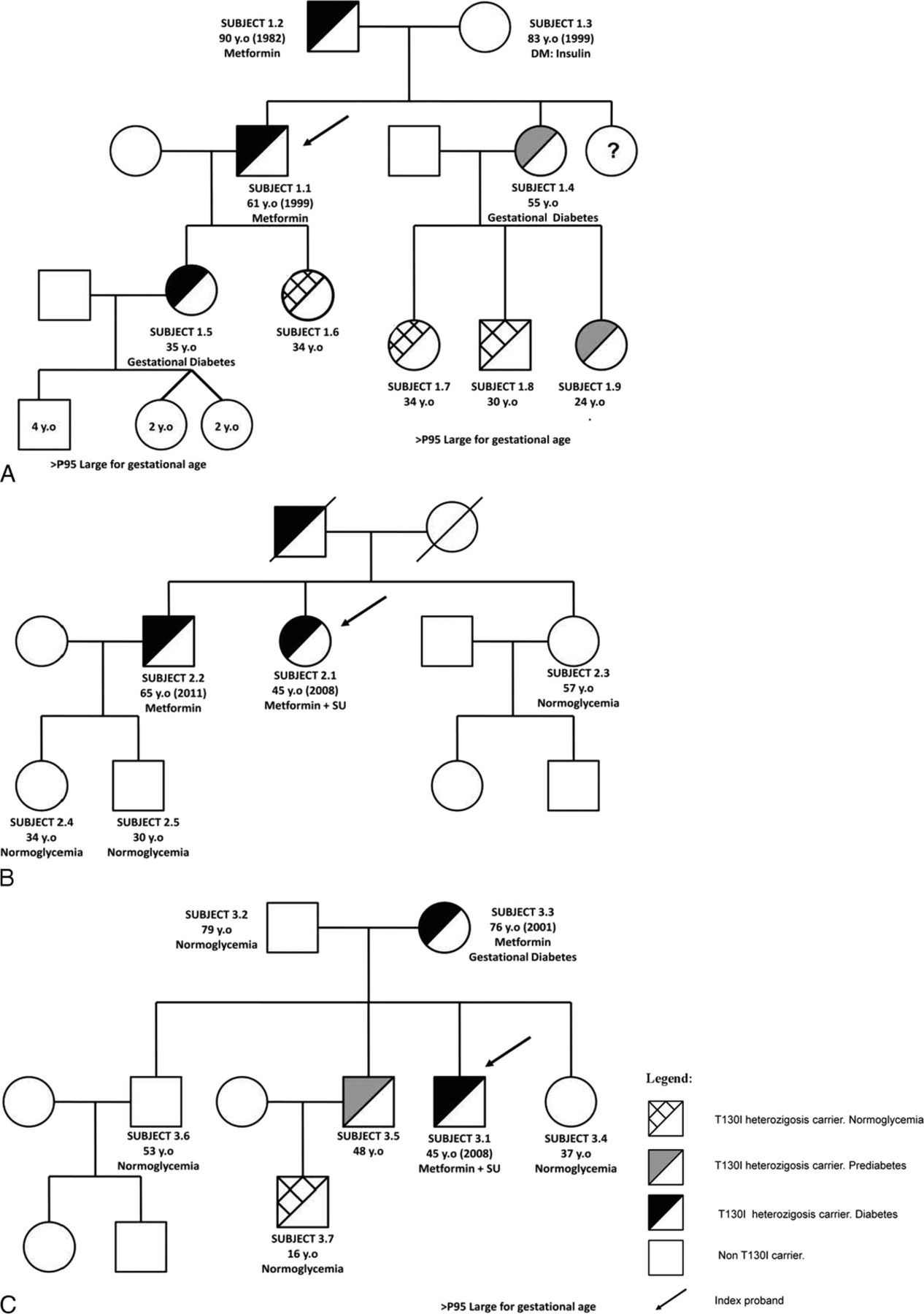
Family pedigrees. Subjects 1.1, 2.1, and 3.1: index probands. A, Subject 1.1's family. B, Subject 2.1's family. C, Subject 3.1's family.
Fourteen (74%) of the 19 relatives were classified as T130I carriers. Diabetes was diagnosed in 50% of carriers, prediabetes in 21%, and normoglycemia in 29%. All T130I carriers older than 35 years and 33% of the carriers younger than 35 years were diagnosed with a degree of glucose metabolism abnormality (diabetes or prediabetes). No microvascular complications were diagnosed in any carrier. The mean referred age at diabetes/prediabetes diagnosis was 51 (SD, 14) years in family members. However, most of the T130I carriers showed mild hyperglycemia in fortuitous or routine checkups that were not informed as pathological. Those with earlier diagnosis were in the context of gestational diabetes or intercurrent illness.
Of note was that 3 mothers of family A (subjects 1.4 and 1.5) and family C (subject 3.3) were diagnosed as carriers of the mutation. In all 3 cases, gestational diabetes was diagnosed, and insulin treatments were prescribed, and newborns were large for gestational age at delivery because of complications from gestational diabetes. However, all those first-degree relatives without the T130I mutation showed normal glucose metabolism rates after fasting and OGTT, except subject 1.3 (an 83-year-old woman diagnosed with type 2 DM in 1999 under treatment with insulin, BMI of 31 kg/m2).
T130I carriers were compared with a control group formed by nondiabetic and non–T130I carriers selected from mutation-negative relatives and unrelated consecutive selected subjects from an outpatient clinic in our Diabetes Unit. The control group and T130I carriers were comparable in age, weight, and BMI (Table 3). However, the T130I carriers showed significantly higher levels of fasting (P < 0.01), 60 and 120 minutes after OGTT plasma glucose and HbA1c (P < 0.05). On the other hand, serum concentration of C-peptide and Homeostasis Model Assessment–Insulin Resistance (HOMA-IR) calculation was significantly higher in the T130I group. Homeostasis Model Assessment β-Cell Function (HOMA-B) was lower in T130I carriers when compared with the control group, although it was not statistically significant.
Clinical Features of the Patients Carrying Heterozygous T130I HNF4A Mutation and the Control Group
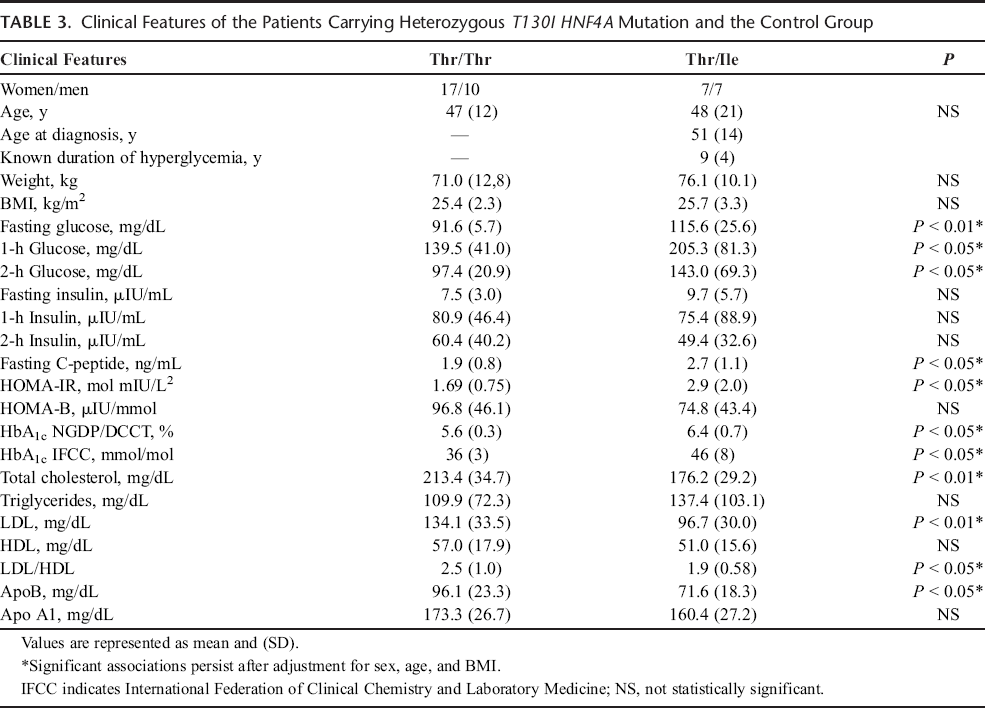
T130I carriers showed significantly lower levels of total cholesterol, LDL-C, and ApoB, and no one showed significantly higher level of triglycerides and lower levels of HDL-C when compared with noncarriers.
The associations between T130I variation carriers and HbA1c, fasting, and OGTT plasma glucose, C-peptide, HOMA-IR, LDL-C, and ApoB remained significant after adjusting for sex, age, and BMI.
Finally, we analyzed the influence of age in HbA1c, fasting glucose, and C-peptide in T130I carriers by Spearman correlation. Strong positive correlations between age and fasting plasma glucose, HbA1c, and C-peptide were found (r = 0.69, P < 0.01; r = 0.66, P < 0.01; r = 0.59, P < 0.05), respectively (Fig. 2).
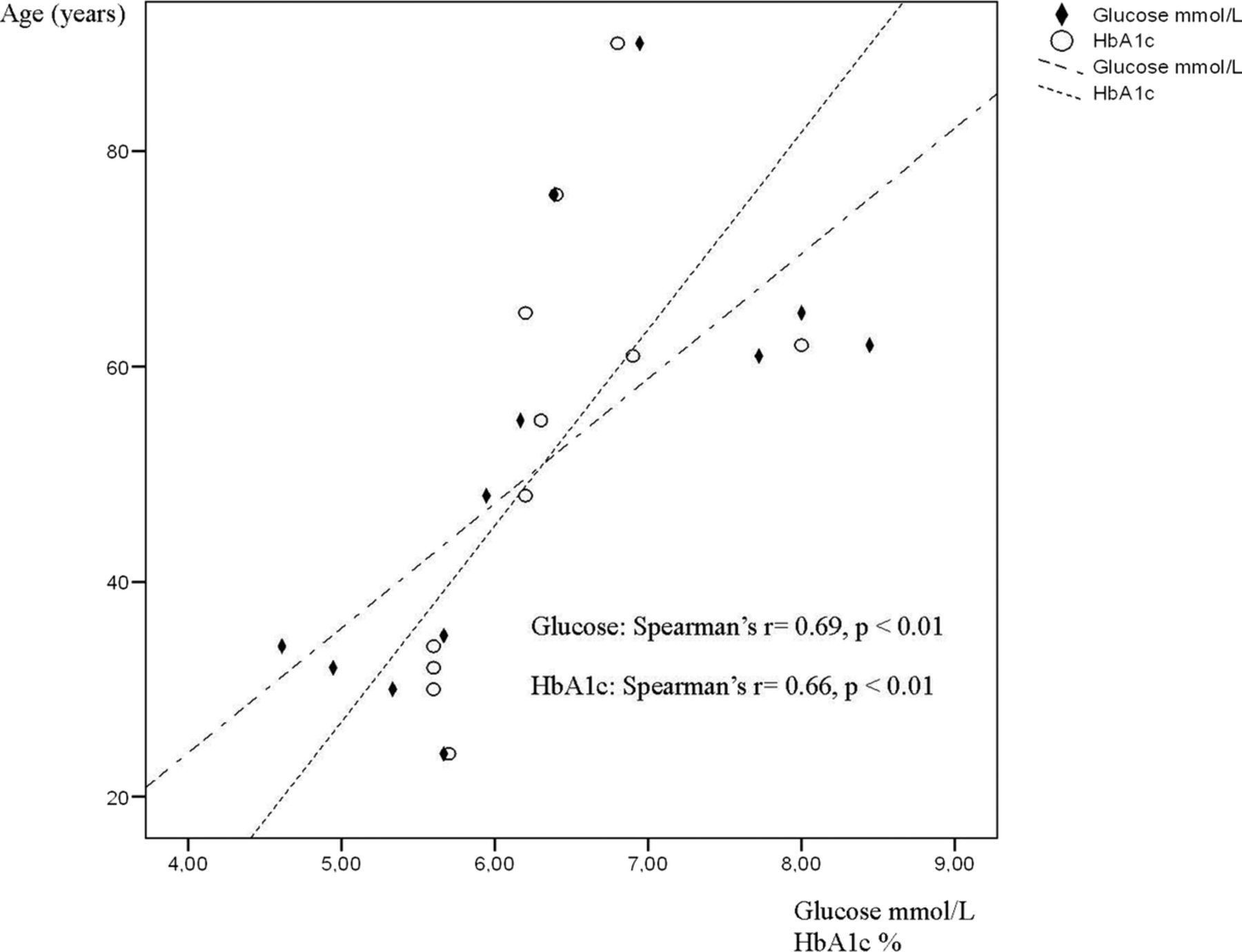
Positive correlation between age and fasting plasma glucose and HbA1c in T130I carriers.
Discussion
Hepatocyte nuclear factor 4α is a nuclear transcription factor codified by the HNF4A gene. It is mainly expressed in the liver and the pancreatic β cells, depending on 2 promoters P1 and P2, respectively.29–31 This protein plays a vital role in normal glucose metabolism in pancreatic β cells and in insulin gene expression and secretion, as well as in liver gluconeogenesis.
HNF4A is located in 20q13 and consists of 10 exons. Its protein has several functional domains, highlighting the N-terminal activation function, 2 zinc fingers involved in DNA binding, and the C-terminal domain involved in homodimerization. 32 Different studies have found that the T130I polymorphism, located in the DNA binding domain, reduces the transactivation function of the HNF-4α protein and decreases pancreatic β-cell function.24,25 A significant association between T130I polymorphism and late-onset and early-onset type 2 DM has been reported.33,34 Nevertheless, other studies did not find any significant relation.35,36
As we have shown in the pedigrees (Fig. 1, A–C), the T130I functional variant acts as a major susceptibility genotype for the development of early-onset type 2 DM in the families included in our series. All carriers older than 35 included in our series have a certain degree of dysglycemia (prediabetes or diabetes) according to the American Diabetes Association criteria. 28 We also have shown a high family penetrance of the T130I mutation, although the younger affected relatives (<35 years old) show mild glycemia metabolism alterations (prediabetes). Glucose metabolism abnormalities progressively increase and are strongly correlated with age (Fig. 2).
The older relatives with clinical manifestation of early-onset type 2 DM treated with oral antidiabetic drugs had favorable outcomes. However, stressful situations such as corticoid therapy or inpatient therapy not related to diabetes induced severe dysglycemia even in the younger carriers. This situation was even more critical and well documented during pregnancy. As shown in the pedigree of families A and C, all mothers who carry the T130I variant were diagnosed with gestational diabetes and needed treatment with insulin during pregnancy. Moreover, all newborns were large for gestational age at delivery because of complications from gestational diabetes.
In our opinion, these observations reflect subclinical dysfunctions of β cells in apparent nonobese and healthy young subjects, which becomes evident through age deterioration of β-cell function and in various stressful situations.
C-peptide levels, fasting insulin, and HOMA index support this hypothesis. Homeostasis Model Assessment is a widely validated clinical and epidemiological tool for estimation of insulin resistance (HOMA-IR) and β-cell function (HOMA B). It clearly relates to type 2 DM pathogenesis when used as a predictor of future risk for type 2 DM or prediabetes in diverse populations.37,38 In our study, T130I carriers showed statistically significant higher HOMA-IR and lower, but not significant, HOMA-B values when compared with the control group. At the same time, T130I carriers had significantly higher fasting glucose and C-peptide levels. In fact, those subjects not diagnosed with dysglycemia showed a degree of dysfunction in β cells and higher insulin resistance. Thus, HOMA indexes reflect not only the classic phenotype of type 2 diabetes (characterized by insulin hypersecretion and insulin resistance in early stage), but an early insulin secretion failure as in the MODY1 mutation. 39 Therefore, our findings support the pathogenic effect of T130I polymorphism as a cause of an early onset of type 2 diabetes, probably secondary to an added defect in insulin secretion.
Lipid profile alteration in T130I carriers also has been observed. HNF4A regulates ApoB, ApoCIII, and ApoAII transcription 40 and has been related to lower levels of ApoB and HDL in MODY1 patients. We have found significantly lower levels of total cholesterol, LDL, and ApoB and a nonsignificant trend of lower levels of HDL in T130I carriers, which reinforces the clinical importance of this polymorphism. 41 Moreover, this lipidic phenotype is partially distinct from the lipid profile of type 2 diabetes, which is characterized by a high level of small and dense LDL particles, hypertriglyceridemia, and low level of HDL. Thus, this fact would support the hypothesis of a pathogenic effect of T103I polymorphism. 42
Similar associations of early-onset type 2 DM have been previously reported in the Mexican population, although familial analysis was not performed. 34 A second report with Japanese subjects found an association with the late onset of type 2 DM, but they selected patients older than 35 years with differences in diet as well as genetic background, which very well could explain these differences. 24
Our study shows differences in lipid profile, HOMA index, autosomal dominant-like pattern of transmission and an early age at diabetes onset that could not be completely explained by classic type 2 diabetes or by age, sex, or BMI β-cell deterioration. What is more, those T130I carriers without any degree of dysglycemia, alterations in lipid, and insulin secretion/resistance are already present.
Even though we cannot completely rule out other genetic alterations or environmental factors that could affect the diabetes evolution, the clinical plausibility, autosomal dominant pattern, and the lipid and insulin secretion alterations support the role of HNF1A T130I as a major determinant of early-onset type 2 diabetes in the population of central Spain.
Thus, we have described for the first time the association between HNF4A T130I polymorphism and abnormal glucose and lipid metabolism in young healthy carriers of central Spain, specifically under stressful circumstances.
Footnotes
Acknowledgments
The authors thank Ms Nieves Mateos for her technical assistance and Hanna Stilwell for the English translator assistance.