
Abstract
Background
Clostridium difficile infection (CDI) has recently markedly increased, incurring greater health care–associated costs and hospitalizations especially in vitamin D deficient patients. Accordingly, the aim of this study was to evaluate the relationship between low vitamin D levels and the severity and recurrence of CDI.
Methods
A retrospective case-control study evaluated patients hospitalized between 2007 and 2013 with CDI and a positive C. difficile toxin assay. Severe complicated CDI was defined based on (1) laboratory or radiological criteria correlated clinically and (2) sepsis requiring intensive care unit admission. Recurrent CDI (RCDI) was defined as a new episode of diarrhea occurring within 90 days of resolution of the initial episode for at least 10 days after discontinuing therapy and confirmed by positive stool C. difficile toxin assay or polymerase chain reaction. Patients were divided into 4 groups based on vitamin D level (ng/mL): severely deficient (<10), insufficient (10-19.9), predeficient (20-29.9), and control group (≥30).
Results
Two hundred seventy-one patients were diagnosed with CDI, of which 48 had RCDI distributed as 5 (12.5%), 15 (16.1%), 10 (15.6%), and 13 (17.5%) patients in each of the aforementioned groups, respectively (P= 0.55). Severe complicated CDI was identified in 7 (17.5%), 17 (18.2%), 9 (14%), and 3 (4%) patients, respectively (P = 0.04). Thirty-day mortality was 1 of 40, 1 of 93, 2 of 64, and 2 of 74 patients, respectively (P = 0.43).
Conclusions
Normal vitamin D level has a protective effect against severe CDI, and low vitamin D is associated with greater severity of CDI but not with an increased risk of RCDI or 30-day mortality.
Keywords
Attenuated immune responses seem to play a crucial role in the development and propagation of CDI. 5 Recently, the role of vitamin D in regulating key elements of the immune system has become an area of active scientific investigation. Vitamin D deficiency has been associated with autoimmune diseases. 2 Furthermore, there is increasing evidence of the antimicrobial efficacy of vitamin D and that vitamin D can boost innate immunity and regulate T-cells and B-cells. 6 This has lead investigators to hypothesize that vitamin D deficiency may play a role in the pathogenesis of various nosocomial infections,7–10 hospital-acquired bloodstream infections, 11 and sepsis.12–14 Moreover, vitamin D deficiency has also been associated with a higher risk of all-cause mortality in hospitalized patients. 15 Recent studies suggest a correlation between vitamin D levels and the risk of developing hospital-acquired CDI.5,16 Vitamin D status is usually determined by accounting for calcidiol, 25(OH) D3, ergodiol, and 25(OH) D2; most 25(OH) D in humans is composed of calcidiol.
Youssef et al. 2 reported that patients with low vitamin D levels had 5-fold greater health care–associated costs and longer hospital stay compared with non–vitamin D deficient patients. Furthermore, an observational study showed that every 1-ng/mL increase in 25(OH) D3 was associated with an 8% decrease in the risk of CDI severity. 5 Wang et al. 16 suggested that low vitamin D level and age older than 70 years were associated with an increase in the likelihood of recurrence. Vitamin D status before hospital admission has been shown to be inversely associated with the risk of hospital-acquired CDI. 17 Recurrent CDI is a challenging disease that often develops due to the persistence of strains responsible for the initial episode of infection.18,19 The recurrence risk rises from approximately 20% after the initial episode to 40% after a first recurrence to over 60% with 2 or more recurrences. 20 Therefore, the aim of the present study was to elucidate whether low vitamin D level is an independent risk factor for predicting severity of CDI or RCDI.
Materials and Methods
A retrospective case-control study was performed that included patients hospitalized at a single institution (Akron General Medical Center, Akron, OH) from January 2007 to December 2013 with CDI code (008.45). Akron General is a 532-bed tertiary academic medical center. After obtaining institutional review board approval, a total of 3020 patients with CDI were identified. Clostridium difficile infection was defined as more than 3 episodes of unformed stools within 24 hours with a positive C. difficile stool toxin assay A/B and/or polymerase chain reaction (PCR) and not attributed to any other cause. In addition, we ascertained confirmatory findings from computed tomography scan such as pancolitis, colonic wall thickening, megacolon, and ileus.
Our definition of severe complicated CDI was a combination of (1) a laboratory finding of white blood cell (WBC) count greater than 15,000 cells/μL + serum creatinine level greater than or equal to 1.5 times premorbid level or radiological finding of severe CDI (ileus and megacolon with correlated clinical examination findings [abdominal tenderness]) and (2) significant systemic toxic effects meeting sepsis criteria and resulting in intensive care unit (ICU) admission. The primary outcome of the study was RCDI, defined as a new episode of diarrhea within 90 days and confirmed by a positive stool C. difficile toxin assay or PCR, after resolution of the initial CDI episode for at least 10 days and after discontinuation of the CDI therapy. The secondary outcome was severity of CDI and 30-day mortality in relation to vitamin D level.
Vitamin D deficiency was defined as total 25(OH) D (D3 + D2) levels less than 20 ng/mL of vitamin D. We categorized total 25(OH) D levels into 4 groups: severe vitamin D deficient group, vitamin D less than 10 ng/mL; vitamin D insufficient group, 10 to 19.9 ng/mL; pre–vitamin D deficient group, 20 to 29.9 ng/mL; and control group, greater than or equal to 30 ng/mL. We collected the following data through review of electronic medical records: (1) demographic data: age, race, and sex; (2) residence state before admission (nursing facility or home); (3) ICU admission for patients meeting the sepsis criteria; (4) antibiotic therapy within 2 months of the current admission, proton pump inhibitor (PPI) use, and vitamin D supplementation (type and dose in international units) and treatment used; (5) physical examination findings, including the presence of abdominal pain or distention, diffuse abdominal tenderness, severity of diarrhea, and peritoneal signs; (6) physiologic parameters, including complete blood count with differential, complete metabolic profile, serum protein, and albumin levels; (7) abdominal computed tomography scan findings; (8) modified Charlson-Deyo Comorbidity Index (CCI); and (9) length of hospital stay and 30-day mortality. Exclusion criteria included (1) patients treated as outpatients or in the emergency department and not admitted to the hospital; (2) patients with diarrhea suspected to have CDI but without a positive C. difficile toxin A/B or PCR assay; (3) patients lost to follow-up; and (4) patients without recorded vitamin D levels within 2 months of the hospital admission.
Continuous variables in the comparison groups were described using means and SDs. Categorical variables in the comparison groups were described as percentages. Point biserial correlation analyses were performed to determine the association between recurrence of C. difficile and the continuous variables, which included age, WBC count, creatinine, serum glucose, and vitamin D levels. Spearman ρ correlation analyses were performed to determine the association between recurrence of C. difficile and the categorical variables, which included sex, albumin less than 3.4 mg/dL, end-stage renal disease, diabetes mellitus, CCI, PPI use, antidepressant use, antibiotic use before diagnosis, steroid use, and the antibiotic treatment regimen. Hierarchical linear regression analysis was conducted to determine the predictive model for recurrence of C. difficile. Sex and age were entered as control variables in the first block of the model. Variables that were found to correlate to the recurrence of C. difficile during univariate analysis at P ≤ 0.10 were entered in the second block. Vitamin D was added in the third block. A nonsignificant value (P > 0.10) for the Hosmer and Lemeshow test was indicative of a good model fit. A P < 0.05 was indicative of overall ability for the model to predict recurrence of C. difficile.
Results
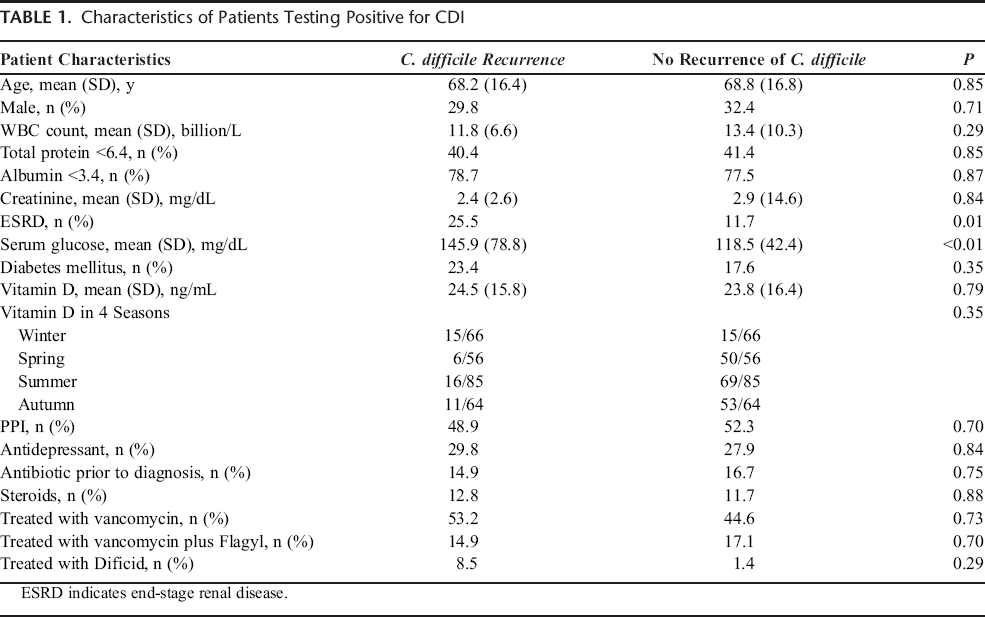
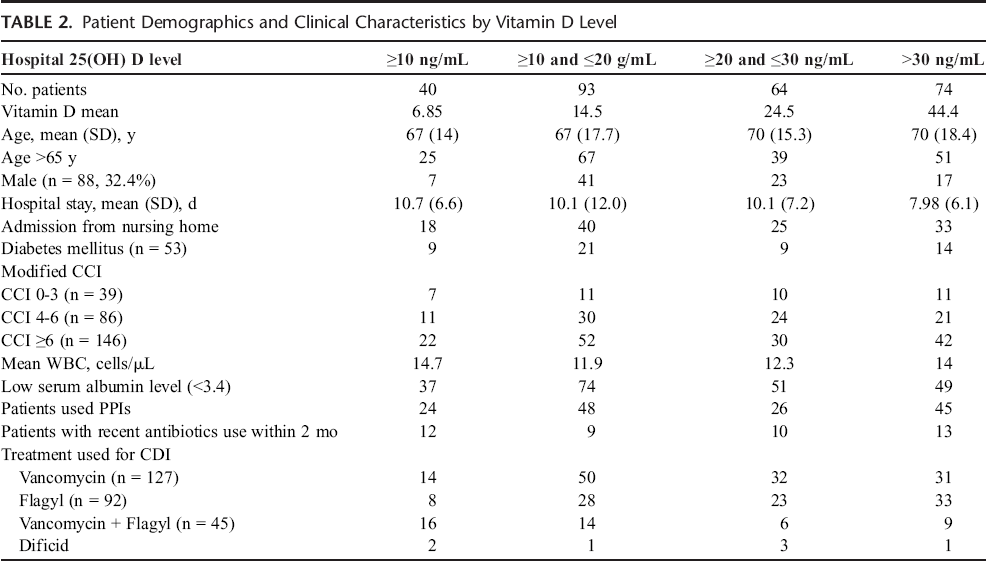
There were a total of 271 patients who met the stated inclusion criteria of recorded vitamin D levels within their hospital stay and tested positive for CDI between the dates of January 2007 and December 2013. One hundred eighty-three of 271 patients were female (67.5%). The mean (SD) age was 68.7 (16.7) years. The average length of hospital stay was 9.6 days. Sixty-nine patients were admitted from nursing homes. Fifty of 271 patients were admitted to the ICU during their hospitalization. The mean CCI in the study population was 7.9 (range, 1–18).The mean vitamin D level was 23.8 ng/mL. Of the patients included in the study, 81.5% had new onset CDI (221 of 271), whereas 16.9% had recurrent disease (46 of 271) (Tables 1, 2).
Characteristics of Patients Testing Positive for CDI
Patient Demographics and Clinical Characteristics by Vitamin D Level
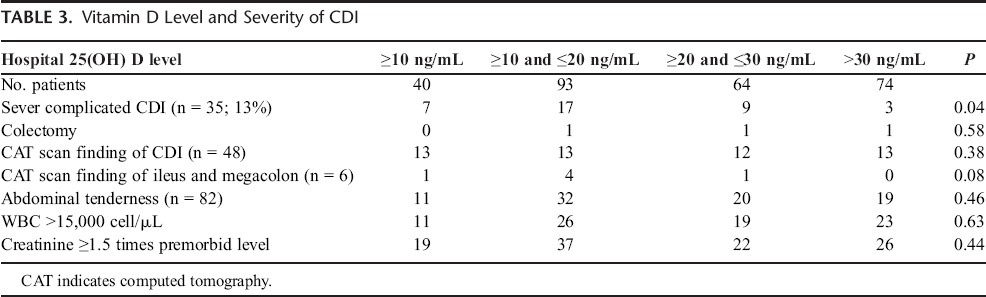
A diagnosis of severe complicated CDI was identified for 13.2% (36 of 271) of the patients. Vitamin D deficient patients tended to have more severe CDI. Severe complicated CDI was identified in 7 patients (17.5%) in the severe vitamin D deficient group, 17 patients (18.2%) in the vitamin D insufficient group, 9 patients (14%) in the pre–vitamin D deficient group, and 3 patients (4%) in control group (P = 0.04) (Table 3).
Vitamin D Level and Severity of CDI
Thirty-day mortality was identified in 1 of 40 patients in the severe vitamin D deficient group, 1 of 93 patients in the vitamin D insufficient group, 2 of 64 in the pre–vitamin D deficiency group, and 2 of 74 in the control group (P = 0.43). Recurrence occurred in 5 patients (12.5%) in the severe vitamin D deficient group, 15 patients (16.1%) in the vitamin D insufficient group, 10 patients (15.6%) in the pre–vitamin D deficiency group, and 13 patients (17.5%) in the control group (P = 0.55). Low vitamin D was not associated with an increase in RCDI. The results of the hierarchical logistic regression are detailed in Table 2. Demographic variables of age and sex were not predictive of RCDI in the study population (χ2 [2] = 0.204, P = 0.66). After controlling for age, sex, and CCI, vitamin D was not a significant predictor of CDI recurrence (χ2 [1] = 0.402, P = 0.50).
Discussion
Recurrent CDI is a challenging clinical dilemma. Several studies have reported low vitamin D levels to be a risk factor for the incidence and severity of acquisition of C. difficile (Tables 4, 5).2,5,17 However, risk factors for RCDI differ notably from risk factors for acquisition of C. difficile and development of the initial episode. 19 In all previous studies that investigated vitamin D deficiency as a risk factor for CDI, it was not clear whether the infections were initial or recurrent. In designing the present study, we hypothesized that vitamin D deficiency would be associated with an increased severity of CDI and that low vitamin D would increase the risk of RCDI after the initial episode. The results of this study show that vitamin D deficiency is associated with more severe CDI but is not associated with increased 30-day mortality or RCDI. Furthermore, when we compared the rate of recurrence in the mild, moderate, and severely vitamin D deficient groups, no significant difference was observed.
Vitamin D Level and 30-Day Mortality

List of Comorbidities According to the Modified CCI

This study is one of the largest retrospective investigations of the relationship between vitamin D deficiency and severity and recurrence of CDI. However, it does have several limitations. First, the retrospective design means it is possible that some data could be missing or incomplete. Second, the population sample size was relatively small. Third, unmeasured confounding variables may not have been identified. However, we tried to eliminate confounding by employing multivariate analyses and calculating the modified CCI. Fourth, in some patients, follow-up vitamin D levels after replacement therapy were initiated but were not available. Finally, the timing of the blood samples drawn for vitamin D levels and CDI diagnoses may not have been standardized for all patients. In our study as in prior ones,2,5,16,17 the association between 25(OH) D2 levels and CDI as a 1-point assessment of 25-hydroxyvitamin D after acute stress may provide a false assessment of vitamin D status. Some have suggested that interpretations of vitamin D status based on 25(OH) D2 measurement without controlling for low serum albumin or vitamin D–binding protein (DBP) as potential confounders in acute stress (eg, sepsis) can lead to inaccurate data. Because more than 99% of 25(OH) D2 is bound to DBP and albumins; loss of these binding proteins can cause a disproportionately low vitamin D status. Loss of albumin and DBP in critically ill patients is thought to occur by acute hemodilution, interstitial extravasation, or decreased synthesis. 21
In conclusion, this study showed a significant relationship between vitamin D and severity of CDI that did not translate into increase risk of RCDI or 30-day mortality. Future prospective studies that include larger sample sizes and investigate the role of vitamin D deficiency in CDI before and after replacement are warranted.