
Abstract
Background and Aim
The data related to the association between hepatitis virus infections and diabetes mellitus (DM) are conflicting. The aim of this study was to investigate the seroprevalence of hepatitis B virus (HBV) and hepatitis C virus (HCV) and to determine the risk factors affecting the prevalence in Turkish patients with type 1 DM and type 2 DM.
Methods
The study consisted of 736 diabetic and 505 nondiabetic patients. Serological investigation for the hepatitis B surface antigen (HBsAg) and the HCV antibody (anti-HCV) was performed with a third-generation commercial chemiluminescence assay. The presence of HBsAg was considered as indicator of HBV infection. The HCV infection in the patients with positive anti-HCV was confirmed by a real-time polymerase chain reaction assay. The patients were divided according to their HBV and HCV infection status, and their demographic features, diabetes properties, general risk factors, and aminotransferase levels were analyzed.
Results
There was no significant difference in the seropositivity rate for the HBsAg (3.8% vs 3.0%, P > 0.43; odds ratio, 1.292; 95% confidence interval, 0.683–2.444). However, anti-HCV seropositivity was significantly increased in the DM group (3.3% vs 1.8%, P < 0.03; odds ratio, 2.398; 95% confidence interval, 1.025–5.609). Increased aminotransferase levels and a history of blood transfusions were positively correlated with both HBV and HCV infection. Moreover, a history of surgical procedures and high glycated hemoglobin A1c levels were positively associated with HBsAg antigen seropositivity.
Conclusions
Although no significant difference in the seropositivity of the HBsAg was determined, a high prevalence of HCV infection was detected in the DM patients compared to healthy controls.
Diabetes mellitus is a metabolic disease, characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. 3 The prevalence of DM is approximately 2.0% to 9.4% worldwide 4 and 13.7% in Turkey. 5 Worldwide, more than 382 million are experiencing type 2 DM (T2DM), which is associated with long-term cellular damage, dysfunction, and failure of various organs.3,4 Additionally, diabetic patients are more prone to have abnormal liver function tests, hepatomegaly, hepatic steatosis, and steatohepatitis. 6
The link between liver disease and DM has long been recognized. It has been reported that DM increases the risk of the development of chronic liver disease, including nonalcoholic fatty liver disease and hepatocellular carcinoma.6,7 The association between HCV infection and T2DM was first reported by Allison et al. 8 Following the paper on the increased prevalence of T2DM in HCV cirrhosis of Allison et al., interest concerning the relationship between HCV and T2DM escalated. It has been hypothesized that during the course of the disease, diabetic patients are more prone to acquire hepatitis virus (in particular HCV) infections because they are subjected to more frequent medical interventions.9-11 Thus, studies have stressed the necessity of investigating transaminase levels, a marker of hepatitis, in diabetic patients.10,11
Although mounting evidence suggests an association between HCV infection and DM, not all studies have found an association between T2DM and HCV infection.12,13 Recent studies reported that patients referred for DM did not have an excess prevalence of HCV infection.10,14,15 Furthermore, the theory that hospital practices are associated with an increased risk of HCV transmission was not confirmed in a French study, 16 but it remains uncertain whether this consequence applies in developing countries, such as Turkey.
Most of the previous studies that investigated the association between DM and viral hepatitis focused on the prevalence of HCV in diabetic patients17-31 rather than on the prevalence of HBV infection in the disease.10,17
The aim of this study was to evaluate the prevalence of both HBV and HCV infection in diabetic patients attending an outpatient endocrinology clinic in comparison with nondiabetic healthy persons. In addition, we investigated the influence of various diabetic, nondiabetic, and clinical risk factors on HBV and HCV infections in patients with DM.
Materials and Methods
Study Participants
A total of 736 consecutive diabetic patients attending the outpatient endocrinology clinic of Selcuk University, Medical Faculty and Konya Education and Research Hospital during May 2011 and March 2012 were recruited for the study. The control group consisted of 505 healthy individuals admitted to a checkup unit. Acute hepatitis and all causes of chronic hepatitis other than viral infections were ruled out in the diabetic patients. Pregnant women were excluded. Both groups were matched for age, sex, previous blood transfusion, surgical history, and intravenous drug abuse. Informed consent was obtained from each participant. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, and it was approved by the local ethics committee.
Determination of Diabetes
According to the American Diabetes Association criteria, patients were diagnosed as having DM if they were using oral hypoglycemic medication or insulin or if they had a fasting glucose level above 126 mg/dL on 2 occasions or a random glucose level above 200 mg/dL 2 hours after an oral glucose tolerance test, which was performed in patients with impaired fasting glucose levels (fasting glucose concentration ≥100 and <126 mg/dL). 3 The diabetic patients were also grouped as type 1 DM (T1DM) and T2DM. 3
Investigated Parameters
After explanation of the aim of the study, the diabetic patients were asked to complete a questionnaire containing sociodemographic variables (age, sex, smoking, and alcohol consumption) and clinical characteristics (duration of diabetes, mode of therapy, diabetic complications, history of blood transfusion and surgical procedures, intravenous drug abuse, hospital admission, tattooing, and hemodialysis). Fasting plasma glucose, glycated hemoglobin A1c (HbA1c), alanine aminotransferase (ALT), and aspartate aminotransferase (AST) levels, and body mass index (BMI) were determined.
Determination of BMI
The BMI was calculated using the formula: BMI = weight (kg)/height2 (m2). According to the criteria of the World Health Organization for BMI, normal was defined as less than 25 kg/m2, overweight was defined as between 25 and 29.9 kg/m2, and obese was defined as greater than or equal to 30 kg/m2.
Assay Methods Used in Detection of Laboratory Parameters
Levels of HbA1c were measured by latex immune-agglutination using an HbA1c 2000 apparatus (Ramsey, MN). Levels of HbA1c more than 7% were accepted as poor diabetic control. Levels of ALT and AST were determined with a fully automated clinical chemistry autoanalyzer (Abbott ARCHITECT c8000, Abbott Park, IL) and original reactives. Aminotransferase levels greater than or equal to 60 U/L were considered as enhancement.
The diagnosis of HBV infection was made by positive serology for the hepatitis B surface antigen (HBsAg) that lasted for more than 6 months. The diagnosis of HCV infection was based on the presence of an affirmative HCV RNA real-time polymerase chain reaction in the patients and the healthy controls with positive HCV antibody (anti-HCV) serology. Third-generation chemiluminescence assay reactives were used for both the HBsAg and anti-HCV assays (Siemens Healthcare Diagnostics Inc, Tarrytown, NY) and carried out using a whole automated immunoassay device (ADVIA Centaur XP; Siemens Healthcare Diagnostics Inc). Determination of the viral load of HCV RNA was made with an automated real-time polymerase chain reaction system (Cobas AmpliPrep/COBAS TaqMan 48 System; Roche Diagnostics Ltd, Rotkreuz, Switzerland).
Statistical Analysis
The Student t test was used to compare continuous variables between the groups, and a χ2 test and Fisher exact test were used for the categorical variables. The Mann-Whitney U test was used to compare 2 independent groups without a normal distribution. Pearson correlation test was carried out among the diabetic population variables. The variables that were found to be significant in the Pearson correlation test were included in the multivariate logistic regression model to determine the independent effects of the various factors that were potentially associated with the risk of hepatitis. The software package used for the statistical analysis was the Statistical Package of Social Science, version 13.0 (SPSS Inc, Chicago, IL). Data were presented as the mean (SD) or the number and percentage. A P value less than 0.05 was considered statistically significant.
Results
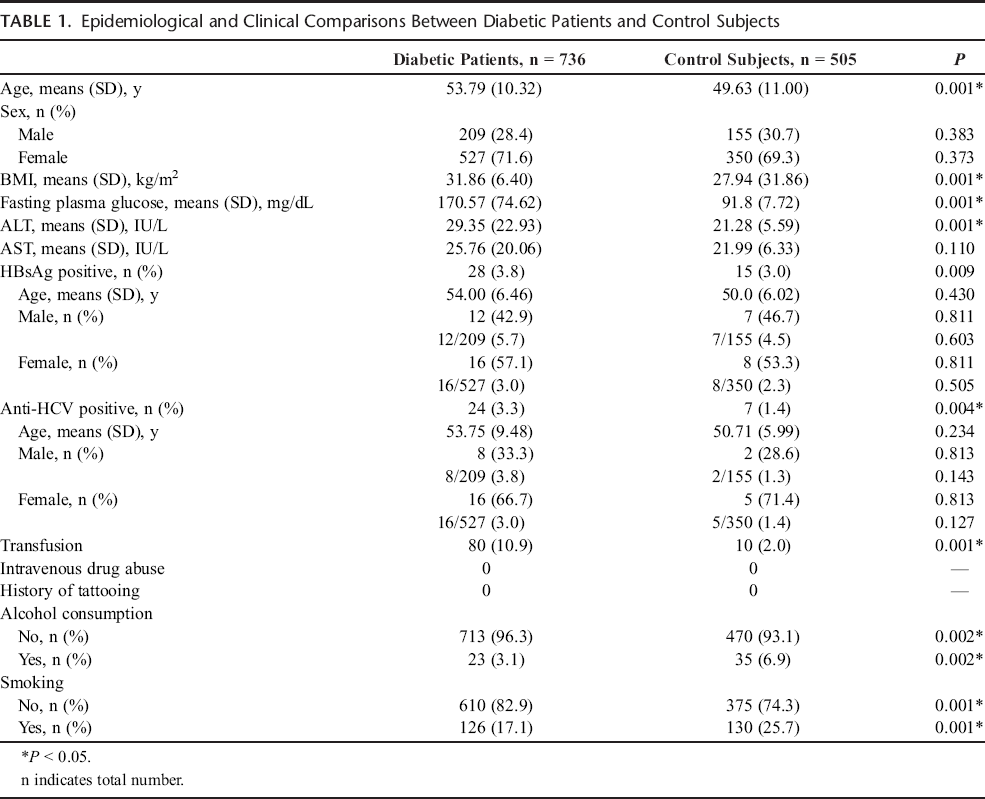
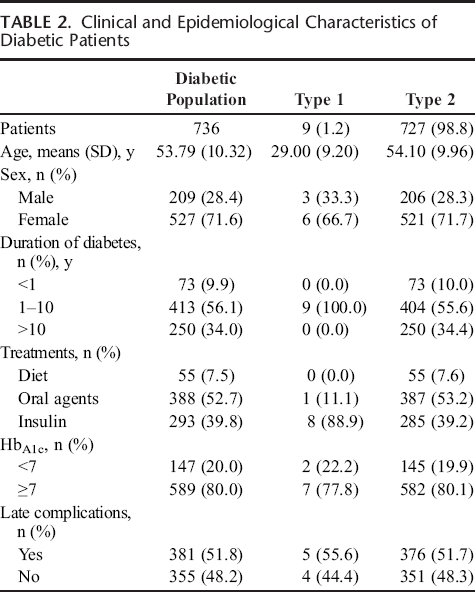
Seven hundred thirty-six consecutive diabetic patients [527% (71.6%) females, 209% (28.4%) males; mean age, 53.79 (10.32) years] and 505 healthy controls [350% (69.3%) females, 155% (30.7%) males; mean age, 49.63 (11.0) years] were included in the study. The epidemiological and clinical comparison of the diabetes and control groups is shown in Table 1. The BMI, glucose, ALT levels, and previous blood transfusion rate were significantly higher and the smoking and alcohol consumption rate were significantly lower in the diabetic patients than in the controls (P < 0.05). The epidemiological and clinical characteristics of the diabetic patients are shown in Table 2.
Epidemiological and Clinical Comparisons Between Diabetic Patients and Control Subjects
Clinical and Epidemiological Characteristics of Diabetic Patients
The seropositivity for HBsAg and anti-HCV was 3.8% and 3.3%, respectively, among the diabetic patients and 3.0% and 1.4%, respectively, among the healthy subjects. Although there was no significant difference in the seropositivity rate of the HBsAg (odds ratio, 1.292; 95% confidence interval, 0.683–2.444; P = 0.430), the anti-HCV seropositivity was significantly increased in the diabetic patients (odds ratio, 2.398; 95% confidence interval, 1.025-5.609; P = 0.038).
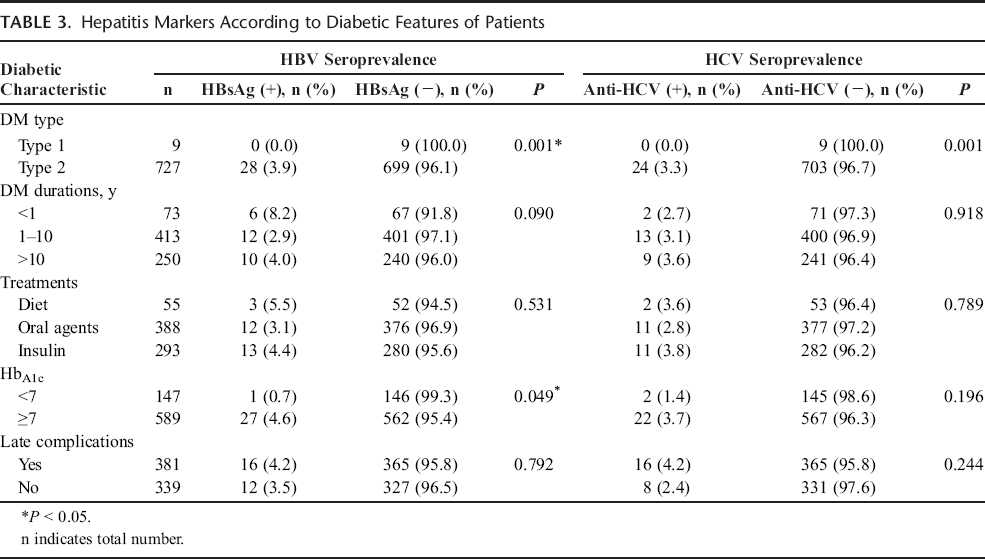
When the HBsAg status and the anti-HCV status of the patients were analyzed according to their diabetic features (Table 3), a weak correlation was found between the positivity of HBsAg and the levels of HbA1c (P = 0.049). However, no correlation was observed between anti-HCV seropositivity and diabetic factors.
Hepatitis Markers According to Diabetic Features of Patients
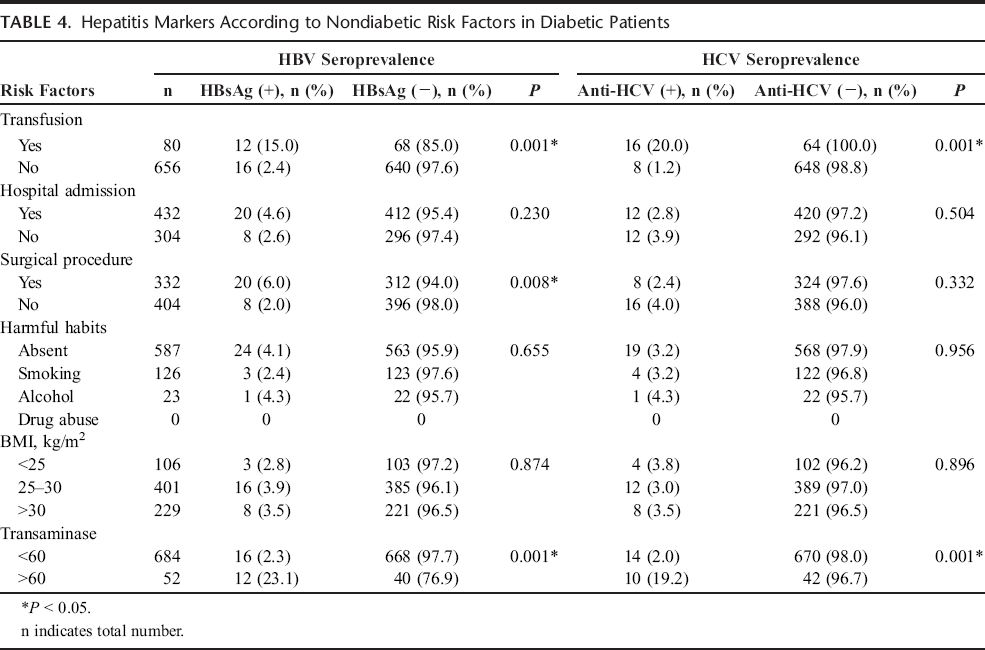
When the HBsAg status and the anti-HCV status of the patients were evaluated according to general risk factors (history of transfusions, hospital admission, and surgical procedures), unhealthy behavior (alcohol consumption and smoking), the BMI, and the presence of elevated transaminase levels (Table 4), a history of transfusions (P = 0.001) and surgical procedures (P = 0.008) were associated with seropositivity of HBsAg. Only a history of transfusions (P = 0.001) was associated with anti-HCV seropositivity. The seropositivity rates of both HBsAg and anti-HCV were higher in the patients with increased aminotransferase levels than in those without an increase in aminotransferase levels (P = 0.001).
Hepatitis Markers According to Nondiabetic Risk Factors in Diabetic Patients
The risk factors affecting the prevalence of HBV and HCV were evaluated by logistic regression analysis. The risk factors for HBV were the presence of increased aminotransferase levels (P < 0.001), a history of transfusions (P = 0.001), a history of surgical procedures (P = 0.007), and high levels of HbA1c (P = 0.028). The risk factors for HCV were a history of blood transfusions (P = 0.001), the presence of increased aminotransferase levels (P = 0.012), and a history of surgical procedures (P = 0.019).
Discussion
Diabetes is an independent cofactor of fibrosis in chronic hepatitis. In patients with cirrhosis, the survival rate is reduced in the presence of diabetes. 33 Therefore, screening programs to increase the awareness of the community and health practitioners of the dangers of hepatitis viruses and diabetes comorbidity are very important. In Turkey, the prevalence of HBV is approximately 2% to 7%, and HCV is 0.3% to 1.8%. 34 In this study, we determined that the seropositivity prevalence of anti-HCV was significantly higher in the diabetic patients than in the control group, but there was no difference for HBsAg seropositivity. Studies performed to establish the association between DM and hepatitis virus infections have been conducted from the following 2 perspectives: investigating the prevalence of hepatitis in diabetic patients or investigating the prevalence of DM in patients with viral hepatitis. Most of these studies, which have been performed in various countries, have focused on the prevalence of HCV infection.12,13 In general, they have reported a higher prevalence of hepatitis C in diabetic patients than in nondiabetic patients. The results of these studies are presented in Table 5. The seropositivity prevalence for anti-HCV in our study is in agreement with the rate reported in these studies. Our findings are also in agreement with those of other studies performed in different areas of Turkey,21,23 except the study of Gulcan et al. 10 They reported that although the rates of anti-HCV seropositivity in Turkish diabetic patients were higher than control group, they did not reach statistically significance. We determined the presence of T2DM as a risk factor for HCV infection in this region.
Published Results of Hepatitis C and B Virus Prevalence in Type 2 Diabetes in Comparison With Controls
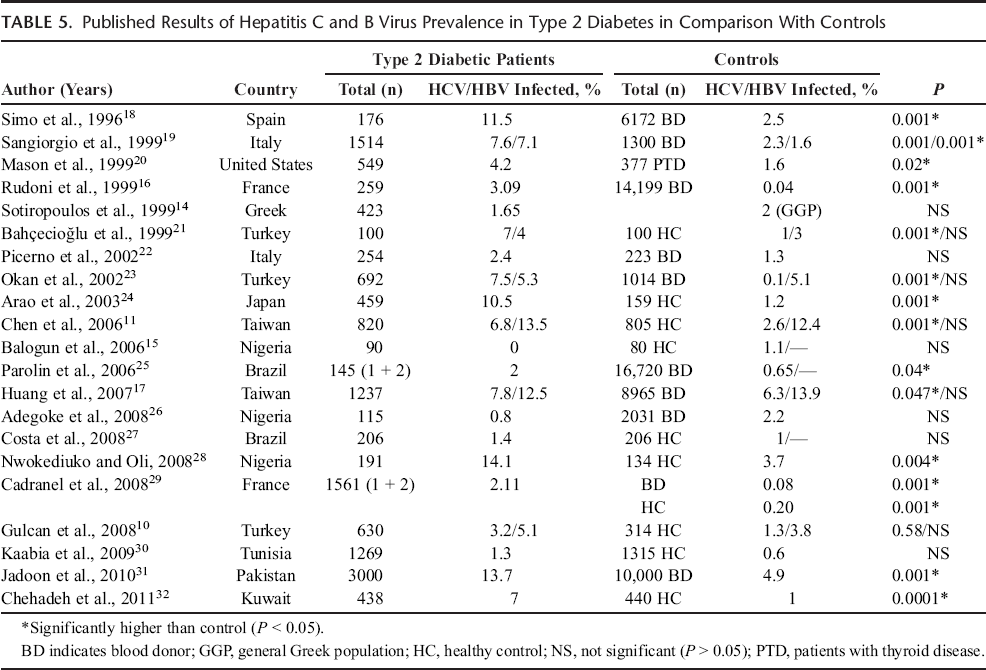
Few studies have been reported concerning the prevalence of HBV infection in diabetic patients. In studies performed by Sangiorgio et al. 19 and Li-Ng et al., 35 the prevalence of HBV infection was higher in the diabetic group than in the control group. However, similar to our study, other studies10,11,17,21,23,36,37 found no significant difference between diabetic and control groups.
Most of the studies mentioned in Table 5 selected blood donors as the control group. In our study, the control group consisted of nondiabetic individuals who attended the same hospital for a medical checkup. As patients whose HBsAg and/or anti-HCV serology was previously determined as positive are prohibited from donating blood, we suggest that the prevalence rates of both markers in blood obtained from blood centers are considerably lower than those of the general population, and thus they do not reflect true rates.
In the present study, we demonstrated that both HBV and HCV infection rates in diabetic patients were not correlated with demographic features, such as age and sex, or with anthropometric measures, such as obesity and BMI. Neither our study nor other studies10,11,20 observed an effect of obesity on the prevalence of HBV and HCV infection in diabetic patients.
Increased transaminase levels seen in diabetic patients are generally attributed to hepatosteatosis. In our study, the presence of increased aminotransferases, regardless of BMI levels, was strongly related with the prevalence of HBV and HCV infection. Several studies have shown that the prevalence of HBV and/or HCV infections is increased in diabetic patients with increased aminotransferase levels compared to diabetic patients with normal aminotransferase levels.10,11,19,23
In our study, the incidence of increased aminotransferases was 7.6%, and the prevalence of HBV and HCV in the patients with increased and normal aminotransferase levels was 23.1% versus 2.3% (P < 0.001) for HBV and 19.2% versus 2.0% (P < 0.001) for HCV. These cases may remain undiagnosed for a long time, as elevated liver enzymes may be clinically disregarded and considered features of nonalcoholic steatohepatitis, not signs of a possible underlying viral infection. Therefore, we suggest that increased aminotransferase levels may constitute an indication for investigation of both hepatitis viruses.
We evaluated the correlation of clinical characteristics of DM, such as the duration of diabetes, treatment regimen, and HbA1c, with hepatitis markers, only the patients whose HbA1c level values of 7.0% or greater had a higher prevalence of HBV infection than the matched control group. We found no relation between the prevalence of HCV infection and the clinical characteristics of the diabetic patients. Similarly, Chen et al. 11 and Gulcan et al. 10 reported that they did not find any relation between the prevalence of HCV infection and the clinical characteristics of DM.
In previous studies that investigated the association between HCV infection and general risk factors unrelated with DM, such as hospital admission, blood transfusion, and surgical procedures, similar to our study, Simo et al., 18 and Sotiropoulos et al. 14 found an association only with a history of blood transfusions among these 3 risk factors. Our study showed a significant association between HBV infection and a history of blood transfusions and surgical procedures. Gulcan et al. 10 and Chen et al. 11 have not determined these relations for HBV infection, except hospital admission. These findings indicate that medical procedures, such as blood transfusions and surgical interventions, in diabetic patients may increase the risk of acquiring the hepatitis virus, especially in developing countries. Therefore, we suggest that consideration of these factors may be beneficial when evaluating the seropositivity of hepatitis markers in diabetic patients.
Therefore, the major question is: Is DM a risk factor for HCV infection or is HCV a risk factor for T2DM? Several studies have shown that HCV increases the risk of T2DM development12,13 and concluded that HCV may have a direct role in the development of diabetes. Others concluded that routine testing for HCV infection in diabetic patients should be mandatory.12,13 Although the link between HCV infection and DM is not clearly understood yet, several studies have postulated that DM might be an extrahepatic manifestation of HCV12,38 that might result in metabolic changes secondary to hepatic steatosis,38,39 exert direct effects of HCV on pancreatic cells resulting in insulin secretion defects 8 or affect autoimmune processes.12,14 The HCV infection promotes insulin resistance, mainly through increased tumor necrosis factor production, combined with the enhancement of suppressor cytokines. 40 Hepatic steatosis in chronic hepatitis C is attributed to cytopathic effects of HCV. 41 Steatosis also influences liver fibrosis progression and worsens insulin resistance. 41 However, although the prevalence of HCV worldwide is markedly high (60%-90%) among intravenous drug users, according to one study, the incidence of T2DM was found to be similar to that of the normal population. 42
As in other studies of the prevalence of hepatitis in the literature,17-31 the data we obtained in the present study did not allow us to evaluate whether the risk factors mentioned above were present before the development of DM. Another limitation of our study is the lack of data on hepatitis markers among family members of the participants. Moreover, in the majority of the participants, it was not possible to determine the timing of the onset of the diabetes or viral hepatitis.
In conclusion, in our study, the prevalence of HCV infection was significantly higher in the T2DM patients than in the controls, but the prevalence of HBV was not. For HBV, the presence of increased aminotransferase levels, a history of blood transfusions and surgical procedures, and high levels of HbA1c (HbA1c levels values of ≥7.0%) were the major factors associated with seropositivity. For HCV, the major factors associated with seropositivity were the presence of increased aminotransferase levels and a history of blood transfusions. We concluded that a prospective large cohort study is required to ascertain the chronological sequence of acquiring HCV infection and the development of T2DM.