
Abstract
Objectives
We sought to assess whether serum salusin-β levels are correlated with the presence and severity of coronary artery disease (CAD).
Methods
We measured serum salusin-β levels in 278 consecutive patients undergoing coronary angiography (CAG) for the evaluation of CAD and in 126 healthy controls. Serum salusin-β levels were measured by enzyme-linked immunosorbent assay. The severity of CAD was assessed by angiographic coronary atherosclerosis index score system.
Results
Serum salusin-β levels were significantly higher in patients undergoing CAG (n = 278) than those in healthy controls (n = 126) (3.81 ± 0.99 vs 4.34 ± 1.40 nmol/L, P < 0.01). In patients undergoing CAG, patients with CAD (n = 160) had significantly higher serum salusin-β levels compared to patients without CAD (n = 118) (4.65 ± 1.44 vs 3.94 ± 1.23 nmol/L, P < 0.01). Multivariate logistic regression analysis revealed that serum salusin-β levels were independently associated with the presence of CAD (odds ratio, 1.439; 95% confidence interval, 1.176–1.760; P < 0.01). Serum salusin-β levels were positively correlated with the coronary atherosclerosis index score (r = 0.316, P < 0.001).
Conclusions
Serum salusin-β levels were associated with the presence and severity of CAD. Salusin-β in serum might serve as a potential biomarker for reflecting the development and progression of CAD. Therapeutic treatment by inhibiting salusin-β interaction to prevent CAD warrants further investigation.
A limited number of biomarkers, such as cardiac troponin I and T, B-type natriuretic peptide, and C-reactive protein (CRP), have demonstrated significant diagnostic and/or therapeutic value in the field of cardiovascular medicine. Additional reliable biomarkers would allow a better understanding of the etiology and pathogenesis underlying the disease and thus facilitate therapeutic decision-making. 2
Salusins are recently identified endogenous bioactive peptides discovered by bioinformatics analyses of a full-length cDNA library. 3 Salusin-α and salusin-β are the 2 highly homologous isoforms of salusins. 3 Experimental studies revealed that the 2 salusin isoforms have opposite effects on the pathophysiologic processes of atherosclerosis. 4 Salusin-β exerts systemic proatherogenic activity, whereas salusin-α has a contrasting antiatherogenic effect. 4 More recently, Du et al. 5 demonstrated that serum salusin-α levels were inversely correlated with the presence and severity of CAD. However, little information has been obtained about salusin-β levels in CAD patients. Therefore, we aimed to detect serum salusin-β levels in CAD patients and to investigate their correlation with the presence and severity of the disease.
Materials and Methods
Subjects
From August 2013 to August 2014, 278 consecutive patients undergoing coronary angiography (CAG) for the diagnosis and interventional treatment of CAD at Tangdu hospital, were consecutively recruited to take part in the study. The patients were classified into 2 groups according to the presence (CAD group, n = 160) or absence (non-CAD group, n = 118) of CAD. One hundred twenty-six age- and sex-matched healthy volunteers undergoing routine physical examination in our hospital were recruited as controls during the same period. Coronary artery disease was defined as angiographic evidence of stenosis 50% or greater in at least 1 major coronary artery. Patients with recent acute coronary syndromes (<3 months), peripheral artery disease, diabetes mellitus, autoimmune diseases, malignancies, chronic or acute inflammatory disease, severe renal or hepatic dysfunction, and asthma were excluded. The study was approved by the ethics committee of Tangdu Hospital, and informed consent was obtained from each patient. The study was carried out in accordance with the regulations and recommendations of the Declaration of Helsinki.
CAG Analysis
Coronary angiography was carried out in the catheterization of our hospital according to standard protocols. Angiograms were analyzed by 2 experienced interventional cardiologists blinded to risk factors and biochemical analyses. The severity of CAD was estimated by coronary atherosclerosis index (CAI), 6 which was defined as the sum of the following scores by assigning points to each lesion as follows: no significant stenosis of the luminal diameter, 0; stenosis of less than 25%, 1; 25% to 49% stenosis, 2; 50% to 74%, 3; 75% to 100%,4.
Clinical Characteristic Collection and Biochemical Analyses
Subjects complicated questionnaires about present conditions, medical histories, cardiovascular risk factors and complications. Body mass index was calculated as weight divided by height squared (kg/m2). Systolic blood pressure and diastolic blood pressure were measured after 15 minutes rest with a sphygmomanometer in sitting position. Venous blood samples were collected from all subjects after an overnight fast. As salusin is a peptide hormone and can be broken down by proteases, aprotinin (500 Kallikrein units per mL) was added to plain biochemistry tubes before the collection of blood samples from the participants to prevent proteolysis. 7 After clotting, serum samples were immediately centrifuged and stored at −80°C until analysis. Serum fasting blood glucose, total cholesterol, triglyceride (TG), low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol were detected by standard laboratory techniques on a Hitachi 7600 Automatic Biochemical Analyzer (Hitachi Co., Tokyo, Japan). High-sensitivity CRP (hs-CRP) levels were measured in an Abbott ci8200 Automatic Biochemical Analyzer System (Abbott Diagnostics, Chicago, IL). Serum salusin-β levels were determined using a commercially available enzyme-linked immunosorbent assay kit with high-sensitivity specificity for detection of human salusin-β (USCN Life Science Inc, Houston, TX). Preliminary data obtained in our laboratory showed that the coefficient of variation was less than 8%.All the samples were routinely analyzed by enzyme-linked immunosorbent assay in duplicate, and the results were averaged.
Statistical Analyses
Continuous variables with normal distributions were expressed as mean ± SD and compared by unpaired t test. Continuous variables with skewed distributions were summarized as median and quartile ranges and compared using Mann-Whitney U test. The χ2 test was used to test categorical variables. Multivariate logistic regression analysis was used to analyze correlations between clinical variables and CAD. Correlations between clinical variables and CAI scores were analyzed by Spearman correlation analysis. Multivariate linear regression analysis was performed to assess the independent predictors of log (CAI scores). SPSS 17.0 software was used for statistical analysis. The value of P less than 0.05 was considered to be statistically significant.
Results
Baseline Clinical and Laboratory Characteristics
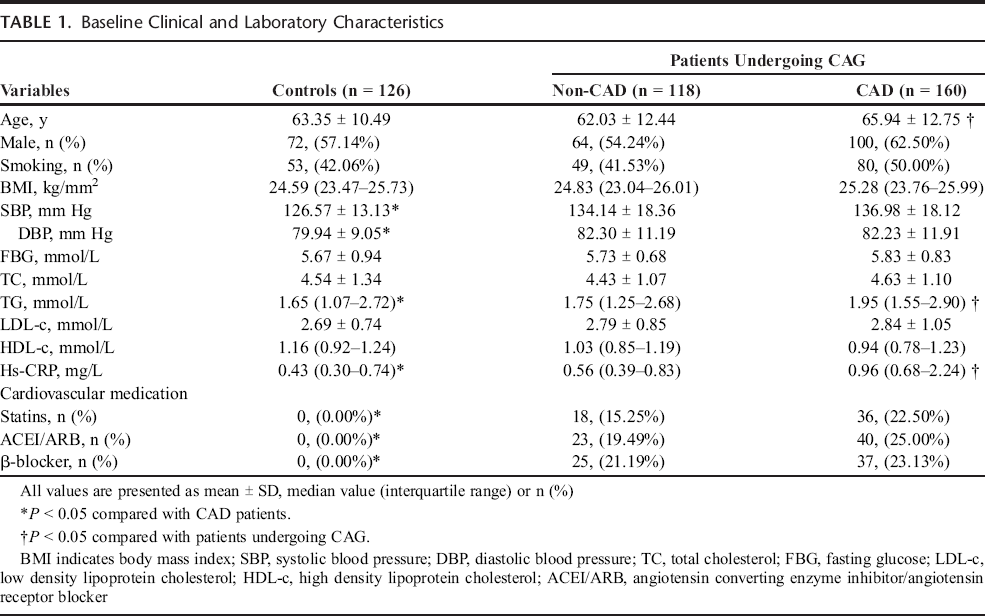
The baseline clinical and laboratory characteristics of the subjects were shown in Table 1. Compared with patients undergoing coronary angiography, controls had significantly lower systolic blood pressure, diastolic blood pressure, TG, and hs-CRP levels. Moreover, statins, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker, and β-blocker medication were more prevalent in patients undergoing CAG. In patients undergoing CAG, the patients with CAD were older and had significantly higher TG and hs-CRP levels compared to patients without CAD.
Baseline Clinical and Laboratory Characteristics
Serum Salusin-β Levels
We revealed that serum salusin-β levels in controls were significantly lower compared with those in patients undergoing CAG (3.81 ± 0.99 vs 4.34 ± 1.40 nmol/L, P < 0.01; Fig. 1A). In patients undergoing CAG, patients with CAD had significantly higher serum salusin-β levels compared to patients without CAD (4.65 ± 1.44 vs 3.94 ± 1.23 nmol/L, P < 0.01; Fig. 1B).
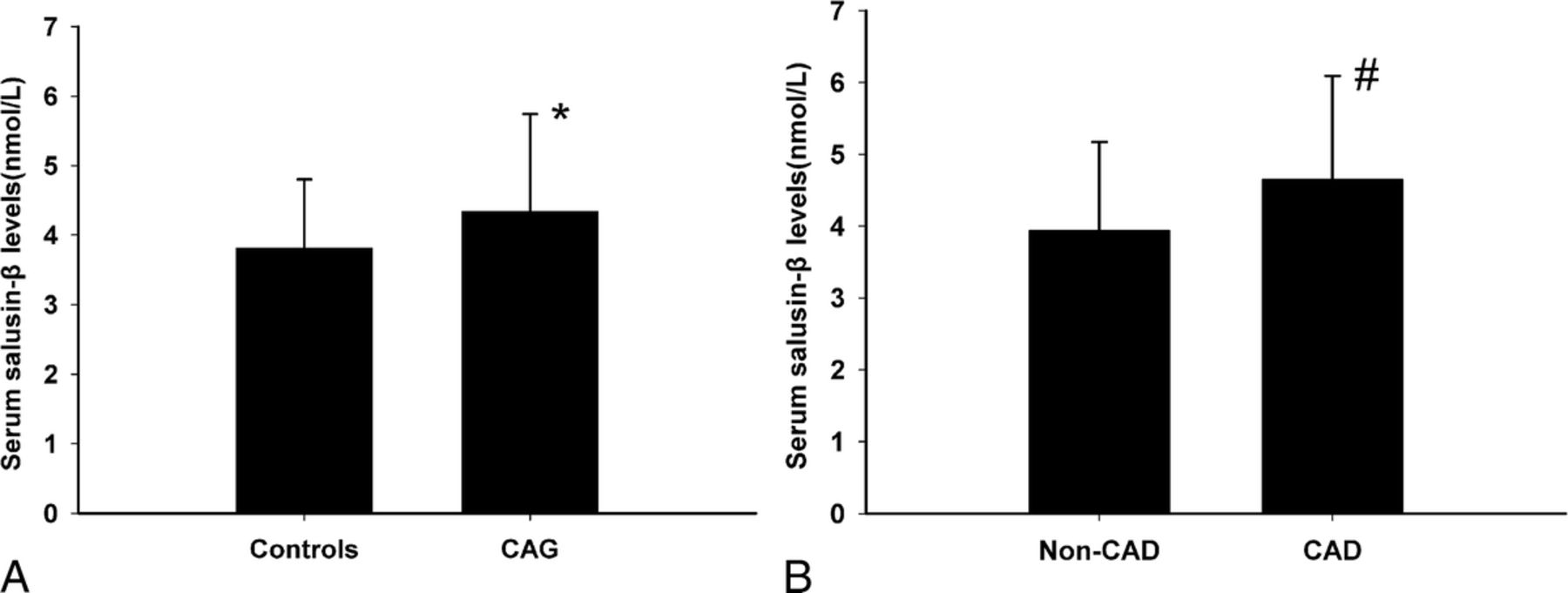
A, Serum salusin-β levels in controls (n = 126, left) and patients undergoing CAG (n = 278, right). *P < 0.01 compared with controls. B, Serum salusin-β levels in patients without (n = 118, left) and with CAD (n = 160, right). #P < 0.01 compared with CAD patients.
Multiple logistic Regression Analysis for the Presence of CAD
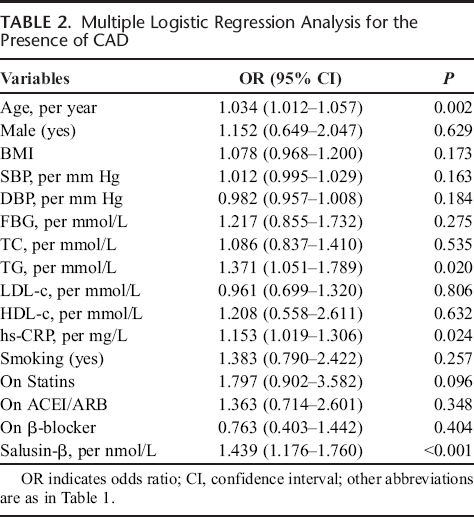
As shown in Table 2, multivariate logistic regression including all variables was run stepwise to assess their independent contribution to the presence of CAD in patients undergoing CAG. We demonstrated that serum salusin-β levels were independently correlated with the presence of angiographic CAD (odds ratio, 1.439; 95% confidence interval, 1.176–1.760; P < 0.001). Besides, age, TG, and hs-CRP levels showed a significant tendency toward positive correlation with the presence of CAD.
Multiple Logistic Regression Analysis for the Presence of CAD
Correlation of Serum Salusin-β Levels and CAI Scores
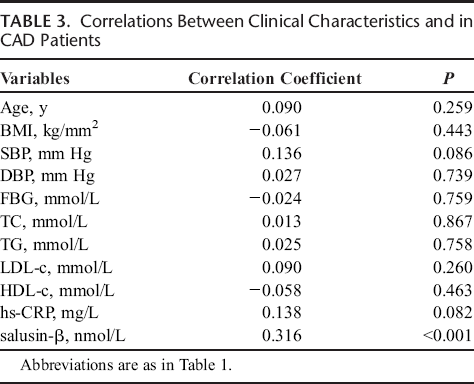
We performed Spearman correlation analysis to assess the correlation between variables and CAI scores in CAD patients. We revealed that serum salusin-β levels were positively correlated with CAI scores(r = 0.316, P < 0.001; Table 3). Multivariate linear regression was then used to adjust for the potential confounders. The analysis revealed that salusin-β level in serum was still the significant determinants of log CAI scores (t = 3.383, P = 0.001).
Correlations Between Clinical Characteristics and in CAD Patients
Discussion
In the present study, we demonstrated that CAD patients had significantly higher serum salusin-β levels compared with those without CAD and controls, and the elevated serum salusin-β level was an independent predictor of CAD. In addition, serum salusin-β levels were independently associated the severity of CAD. To our best knowledge, this is the first clinical study which focuses on the relationship between serum salusin-β levels and CAD.
Biomarkers have had an important value on diagnosis of acute or chronic diseases, risk stratification, and on monitoring of disease and therapeutic efficacy. Salusins are expressed and synthesized in the vasculature central nervous system, and kidneys.8,9 Salusins exist in human plasma in their originally predicted forms,10,11 indicating their possible role as peptide hormones and potential biomarkers. Unlike salusin-α, which has been successfully established as biomarkers of many diseases,5,12,13 the detection of salusin-β faced extreme difficulty because it can be broken down by proteases after adhering to the components of plastic tubes. 12 By using aprotinin to prevent proteolysis, we revealed in the present study that serum salusin-β levels in healthy subjects were 3.81 ± 0.99 nmol/L. This result is in accordance with previous studies and comparable with those of many other known endogenous bioactive peptides.12,14
Salusin-β, initially identified as a peptide with potent hypotensive and bradycardic effect, has been recognized to exert multifold comprehensive influences on the development of atherosclerosis. 12 Salusin-β induces the expression of cytokines such as interleukin-1β, monocyte chemoattractant protein-1, and vascular cell adhesion molecule-1 in human endothelium. 15 These cytokines provide the necessary substrate for recruitment, adhesion, and transmigration of leukocytes across an activated endothelium and subsequent induce inflammatory response and endothelial dysfunction. It is well known that inflammatory response and endothelial dysfunction are the most important early indicators of atherosclerosis. Besides, the overwhelming proatherosclerotic effect by salusin-β is its ability to induce macrophage foam cell formation by induce the expression of acyl-CoA cholesterol acyltransferase-1, 4 which stores cholesterol ester converted from free cholesterol and spontaneously increases during monocytic differentiation into macrophages. 16 We revealed in the present study that serum salusin-β levels were significantly higher in CAD patients than those in non-CAD patients. Because there were significant differences on age, TG, and hs-CRP levels between the 2 groups, we performed multivariate logistic regression to identify independent predictors for CAD. Our results suggested that higher serum salusin-β level was the independent risk factor of CAD after adjusting for potential confounders. These results concurred with those of earlier studies linking salusin-β to CAD and suggested that salusin-β might be a potential biomarker for early CAD diagnosis.
We also found that serum salusin-β levels were independently correlated with CAI scores. The CAI score is a well-established clinical system of assessing the severity of CAD. 6 Unlike SYNTAX score which had highest score in chronic total occlusion of coronary artery, CAI score could allow the investigator to better assess the coronary plaque burden. In the light of this opinion, this result indicated that salusin-β concentration in serum could also predict the progression of CAD. This result also provided preliminary evidence of salusin-β as a potential therapeutic target against atherosclerosis.
Several important limitations need to be considered. First, this study was limited by the cross-sectional nature and a relatively small sample size. Additional prospective studies with a larger cohort are needed to verify the diagnostic and/or prognostic value of salusin-β on CAD. Another limitation of our study is that we only recruited patients referred for coronary angiography to assess CAD severity. This might have resulted in increased prevalence of CAD in the study subjects than that in the general population.
In conclusion, we demonstrated that serum salusin-β levels were independently associated with the presence and severity of CAD. Salusin-β in serum might serve as a potential biomarker for reflecting the development and progression of CAD. Therapeutic treatment by inhibiting salusin-β interaction to prevent CAD warrants further investigation.