
Abstract
Background
High weight status is associated with increased forearm fracture risk but its relationship to severity of fracture has not been evaluated. We compared the epidemiology of children's forearm fractures treated with fracture reduction to those not treated with reduction, hypothesizing that high weight status would be significantly associated with need for reduction.
Methods
This is a case-control study including Washington, DC children, ages 2 to 17 years, treated for isolated forearm fractures in an urban, tertiary care pediatric emergency department from 2003 to 2006. Descriptive statistics and logistic regression were conducted to compare patients with forearm fracture reductions to nonintervention controls.
Results
Of 888 forearm fractures, 330 (37.2%) required reduction (cases) whereas 558 (64.8%) did not (controls). Cases were more likely than controls to be male [adjusted odds ratio, 1.67 (95% confidence interval, 1.11–2.50)] and to have experienced a more severe mechanism of trauma [adjusted odds ratio, 2.11 (95% confidence interval, 1.14–3.90)]. The groups did not differ in weight status, age, or race/ethnicity.
Conclusions
The need for reduction among children with forearm fractures is significantly associated with male sex and major mechanisms of trauma but not with high weight status. Strategies to reduce severe forearm fractures should focus on preventing major mechanisms of trauma.
The prevalence of pediatric overweight and obesity is also rising 6 and may contribute to risk for forearm fracture in childhood. The relationship between pediatric overweight and overall injury risk has been well described. For instance, overweight children have 15% to 48% increase in odds of sustaining an injury compared to their normal weight peers. 7 More specifically, high weight status is associated with increased forearm fracture risk, particularly for fractures incurred from minor trauma mechanisms.8,9 Studies of lower extremity orthopedic injuries have shown that overweight children have increased severity of injuries (ankle sprain), 10 longer-lasting effects from those injuries (ankle sprain), 10 and increased postoperative complications (femur fracture) 11 in the treatment of injuries compared to nonoverweight children. The relationship between high weight status and severity of forearm fractures has not been evaluated.
The objective of this study was therefore to compare the epidemiology of pediatric forearm fractures that did and did not require intervention (defined as open or closed reduction). Because overweight children fall with a greater force than normal weight children, 12 our primary hypothesis was that fractures requiring intervention would be significantly associated with high weight status (weight for age/sex percentile ≥95th).
Materials and Methods
This study reflects an analysis of 888 pediatric emergency department (ED) visits for isolated forearm fractures utilizing a case-control design. We have previously described the methods used to identify the children with forearm fractures. 13
In brief, eligible study participants included children 2 to 17 years of age who were evaluated for an isolated forearm fracture in a large, urban academic pediatric ED in Washington, DC, from January 1, 2003, to December 31, 2006. The mean annual census of this ED exceeded 70,000 visits during this study period, and the patient racial/ethnic composition was 80% African American, 15% Hispanic, 3% non-Hispanic white, and 2% other. This database was limited to patients who resided in a Washington, DC census block group with both an estimated greater than 85% catchment at this ED 14 and a minimum total population of 250 persons. Patients with known bone mineralization disorders or follow-up visits to the ED for reevaluation of the same fracture event were excluded.
Detailed medical record review was completed to obtain the following data elements: age, sex, race/ethnicity, weight, date of injury, details of mechanism of injury, forearm bone(s) involved, need for open or closed reduction, and patient disposition (discharge vs. admission). Weight for age/sex percentiles were calculated using Centers for Disease Control growth chart values 15 and were used as a proxy for high weight status given the inability to determine body mass index (BMI) consistently from the ED chart.
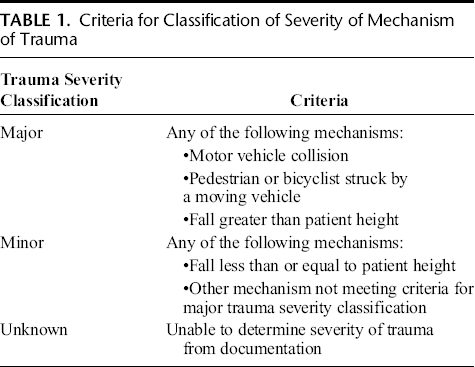
Severity of injury mechanism was classified as major, minor or unknown after independent review by two of the study investigators (LMR and JMC); disagreement was resolved by consensus discussion. Criteria for each category of mechanism severity were defined a priori as detailed in Table 1. The estimated height of the fall for cases in which standardized measures were available (eg, stairs) was used if height of the fall was not documented in the medical record. Centers of Disease Control growth chart values 15 were used to estimate each patient's height as the 50th percentile of height for age/sex to determine if the height of the fall exceeded the patient's height. As previously described, 13 there was an initial agreement by the 2 study investigators in 80% of severity classifications and final agreement in 100% of the classifications.
Criteria for Classification of Severity of Mechanism of Trauma
Cases were defined as patients with forearm fractures that underwent fracture reduction. Controls were defined as patients with forearm fractures that did not undergo fracture reduction. In this ED, forearm fracture reduction is typically performed by pediatric orthopedic surgeons.
Our data analysis included descriptive statistics for cases and controls. Multivariable logistic regression was performed to test for the association of weight status with requirement for reduction while controlling for potential confounders of sex (proportion male), age (continuous variable), race/ethnicity (proportion African American), and severity of injury mechanism (proportion major vs minor). These measures were included in the analysis because sex, age, race/ethnicity and severity of injury mechanism have been associated with fracture risk and/or fracture severity.16–22 Logistic regression was performed in distinct groups: the overall study sample, the sample stratified into the 2 age groups with the highest rates of forearm fracture (5–9 years and 10–14 years), 1 and the portion of the sample with fracture from minor trauma (given the known association between risk for forearm fracture from minor trauma and obesity in children8,9). Adjusted odds ratios (adjORs) are reported together with 95% confidence intervals (95% CIs).
This study was approved by the Institutional Review Board at Children's National Medical Center. Data analysis was conducted using SPSS Statistics 17.0 (SPSS Inc., Chicago, IL).
Results
Of the 888 children with isolated forearm fractures present in the database, there were 330 cases (37.2%) whose fractures required reduction and 558 controls (62.8%) whose fractures did not. The cases included 327 patients treated with closed reduction and 3 patients treated with open reduction. Demographic and clinical characteristics of the overall forearm fracture group and the group stratified by intervention status for children ages 2 to 17 years are presented in Table 2. The overall forearm fracture cohort was 64% men, 81% African American, and had a mean age of 8.8 (±3.6) years. Cases were more likely to be male and to have experienced a major mechanism of trauma but did not differ from controls with respect to age or race/ethnicity.
Demographic and Clinical Characteristics of Cases (Forearm Fractures Requiring Reduction) and Controls (Forearm Fractures not Requiring Reduction), Ages 2 to 17 Years, With Adjusted* OR and 95% CIs
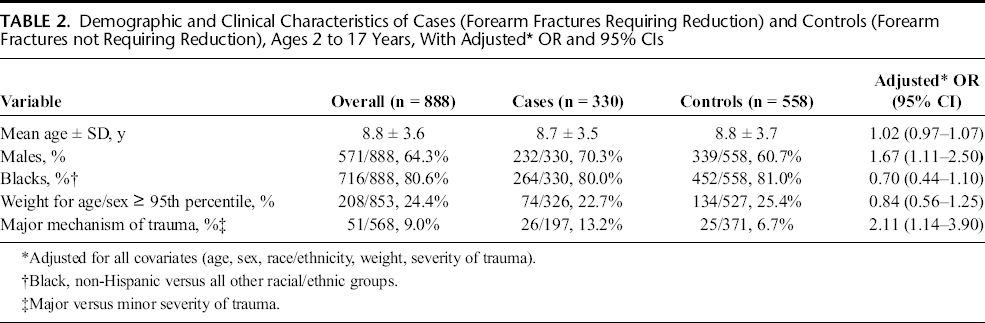
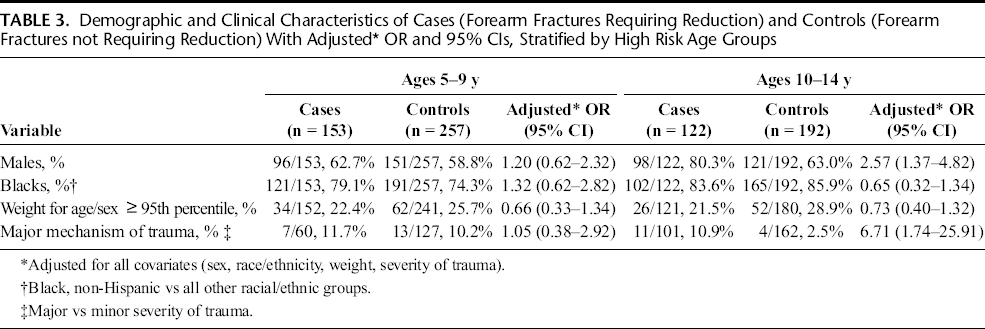
A weight was recorded in the medical record for 326 of 330 cases (98.8%) and 527 of 558 controls (94.4%). The proportion of patients with a weight for age/sex of 95th percentile or greater was not significantly different for cases when compared to controls (22.7% vs 25.4%; adjOR, 0.84; 95% CI, 0.56–1.25). When stratified into the age groups with the highest rates of forearm fracture (5-9 years and 10-14 years), there remained no significant associations between intervention status and weight for age/gender ≥95th percentile in either the 5- to 9-year age group (adjOR, 0.66; 95% CI, 0.33–1.34) or the 10- to 14-year age group (adjOR, 0.73; 95% CI, 0.40–1.32) (Table 3).
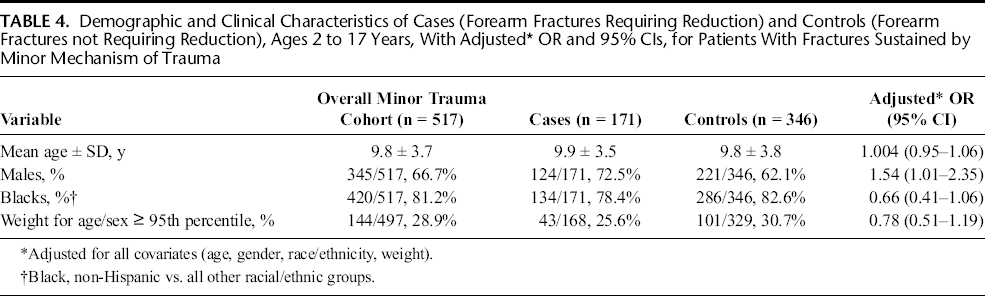
Finally, we performed a subanalysis of the 517 children with forearm fractures (58%) resulting from a minor trauma mechanism. In this group, there were 171 cases (33.1%) and 346 controls (66.9%). The proportion of minor trauma forearm fracture patients with a weight for age/sex greater than 95th percentile was not significantly different for cases and controls (25.6% vs 30.7%, respectively; adjOR, 0.78; 95% CI, 0.51–1.19) (Table 4).
Demographic and Clinical Characteristics of Cases (Forearm Fractures Requiring Reduction) and Controls (Forearm Fractures not Requiring Reduction) With Adjusted* OR and 95% CIs, Stratified by High Risk Age Groups
Demographic and Clinical Characteristics of Cases (Forearm Fractures Requiring Reduction) and Controls (Forearm Fractures not Requiring Reduction), Ages 2 to 17 Years, With Adjusted* OR and 95% CIs, for Patients With Fractures Sustained by Minor Mechanism of Trauma
Discussion
Childhood obesity is associated with increased forearm fracture risk which may relate to several factors including a relative deficiency in bone strength for patient weight,21,22 vitamin D insufficiency,23,24 and behavioral/motor characteristics 25 which may increase the risk of falling. An analysis of the association between obesity and the severity of childhood forearm fractures has not previously been reported. Our study sought to evaluate this association using the need for fracture reduction as a measure of fracture severity.
In this cohort of patients with isolated forearm fracture, a need for fracture reduction was common (37.2%). Overall, however, our analysis did not reveal a statistically significant association between fracture severity and high weight status of the patient.
When stratified into the age groups with the highest rates of childhood forearm fractures, there was also no statistically significant association between fracture severity and increased weight status. Previous studies have demonstrated an association between increased weight status and upper extremity fracture in the 5- to 9-year age group, 26 but an association, if any, on severity of fracture was not reported. Similarly, obesity has also been associated with increased forearm fracture risk specifically from minor trauma during childhood. However, our subanalysis of minor trauma-related forearm fracture injuries does not reveal a statistically significant relationship between the need for fracture reduction and the high weight status in our minor trauma cohort.
In our study population, the need for forearm fracture reduction was significantly associated with male sex. These findings are consistent with other studies which demonstrate that male sex is a risk factor for injury, and specifically severe injury. 16 Our analysis also demonstrated a significant relationship between the need for reduction and major severity of the injury mechanism. These mechanisms included motor vehicle collision, pedestrian or bicyclist struck by a moving vehicle or a fall greater than the patient height. Our data suggest that severity of forearm fracture is more strongly associated with mechanism of trauma than with patient-level factors such as weight. Although these patient-level factors may influence general forearm fracture risk, particularly due to minor trauma,8,9 they appear less likely to influence fracture displacement. As such, preventive strategies to reduce displaced forearm fractures should target these major mechanisms of trauma with primary injury prevention interventions.
This study has several limitations. First, we used weight for age/sex percentiles based on 2000 CDC growth charts to determine increased weight status because we were unable to calculate BMI, which is the standard measure of overweight and obesity in children. 27 However, analysis of National Health and Nutrition Examination Survey data has determined the predictive value of weight for age/sex percentiles to identify overweight children, and these results are reassuring. 28 A weight for age/sex of 95th percentile or greater cutoff has a sensitivity of 82%, a specificity of 96%, a positive predictive value of 80%, and a negative predictive value of 97% to identify children with a BMI of 95th percentile or greater. 28 These findings suggest that the weight for age/sex of 95th percentile or greater range has utility in the research setting to identify groups of patients likely to meet BMI criteria for obesity. 28
A second limitation is the single site design and limited racial diversity of our study population which may reduce the study's generalizability. Third, the retrospective chart review study design is further limited by incomplete or inaccurate medical record documentation. Additionally, smaller sample sizes, particularly in the subanalyses may have limited our ability to determine statistically significant associations. Finally, our outcomes reflected the decision to treat the fracture with reduction which may reflect some subjectivity in clinical practice variation. We did not measure fracture displacement or pursue objective confirmation of the clinical justification for fracture reduction.
In conclusion, a large proportion of forearm fractures in our study population required fracture reduction. The need for intervention was significantly associated with male sex and major mechanisms of trauma without a corresponding association with high weight status. Although obesity in childhood is associated with increased forearm fracture risk, our data do not suggest a relationship with an increased severity of these injuries. Primary injury prevention interventions targeting these high-risk mechanisms may be the most appropriate strategy to reduce displaced forearm fractures in childhood.