
Abstract
Background
Myeloproliferative disorders are characterized by proliferation of 1 or more lineage of hematologic cells. Rapid proliferation of cells may lead to depletion of vitamin B12, which may be falsely elevated by conventional assays in these disorders. We evaluated vitamin B12 status with conventional vitamin B12 assay and levels of serum methylmalonic acid (MMA), serum holotranscobalamin (holoTC), and plasma homocysteine in myeloproliferative disorders.
Methods
In 58 patients who had myeloproliferative disorders and normal serum creatinine levels, we measured levels of vitamin B12, MMA, holoTC, and homocysteine. Correlations were evaluated between these tests, with MMA as the reference standard for vitamin B12 deficiency.
Results
Prevalence of vitamin B12 deficiency was 69%, despite high serum vitamin B12 levels. Levels of holoTC of 40.6 pmol/L or less and homocysteine of greater than 14 mol/L were the best cutoff levels with sensitivity values of 75% and 70%, specificity values of 80% and 68%, and positive predictive values of 88% and 80%. Logistic regression showed that cutoff values of holoTC of 40.6 pmol/L or less and homocysteine of greater than 14 mol/L resulted in odds ratio 15.5 for low versus high holoTC, and odds ratio 5.4 for high versus low homocysteine, to confirm vitamin B12 deficiency.
Conclusions
Patients who had myeloproliferative disorders had a high prevalence of vitamin B12 deficiency, despite high serum vitamin B12 levels. Therefore, vitamin B12 status should be evaluated in patients with myeloproliferative disorders. Holotranscobalamin level may be the best initial test and may replace vitamin B12 assay to accompany MMA and homocysteine levels.
Vitamin B12 deficiency is associated with various diseases including megaloblastic anemia and neuropsychiatric disorders. 4 Reversible bone marrow failure and demyelinating neurologic disease necessitate early diagnosis and treatment.5,6 However, clinical recognition of vitamin B12 deficiency and confirmation of the diagnosis by laboratory tests may be difficult. 7 Results may be controversial when lower cutoff values of serum vitamin B12 levels are used in diagnosing vitamin B12 deficiency, especially when there are no clinical manifestations. Serum vitamin B12 assay (with a cutoff <148 pmol/L) has 95% to 97% sensitivity for the detection of clinical vitamin B12 deficiency, and sensitivity decreases to 38% to 39% in subclinical vitamin B12 deficiency. 8 The specificity of serum vitamin B12 measurement is unknown but may be less than 80% for clinical vitamin B12 deficiency. 9 Methylmalonic acid (MMA), homocysteine, and holotranscobalamin (holoTC) have better sensitivity values than serum vitamin B12 but may be less sensitive for subclinical vitamin B12 deficiency, and the specificity of all these tests is not well defined. 8
Serum vitamin B12 levels are falsely elevated in myeloproliferative disorders, and a reverse algorithm has been suggested for the use of elevated serum vitamin B12 levels as a nonspecific marker of malignancy.10,11 However, elevated serum vitamin B12 levels may occur in patients who have myeloproliferative disorders and vitamin B12 deficiency. In addition to high cell proliferation that causes vitamin B12 depletion, myeloproliferative disorders frequently occur in the elderly, and the prevalence of vitamin B12 deficiency in the elderly is 11% to 90%. 12
The purpose of this study was to determine the prevalence of vitamin B12 deficiency by measuring serum MMA in patients who had myeloproliferative disorders and to evaluate the usefulness of serum vitamin B12, holoTC, and homocysteine levels in detecting vitamin B12 deficiency in these patients.
Materials and Methods
Patients
Patients followed up in our hematology department with a diagnosis of myeloproliferative disorders were recruited for this study. Exclusion criteria were gastrointestinal disorders such as Crohn disease, prior gastric or ileal resection, concurrent metformin use, a purely vegetarian diet, or serum creatinine levels greater than 1.1 mg/dL for women and greater than 1.3 mg/dL for men. There were 58 patients included in the study (29 male and 29 female patients; mean age, 61 ± 15 years). Informed consent was obtained from all patients for inclusion in the study. The study was approved by Sakarya University School of Medicine Ethical Committee for Clinical Research (no. 16214662.050.01.04/39; October 2, 2013).
Evaluation
Fasting blood samples were obtained from participating patients and stored at −80°C. Vitamin B12 status was assessed by serum MMA analysis that was performed using liquid chromatography–tandem mass spectrometry (HPLC 1200 binary pump and 1200 Autosampler; Agilent, Santa Clara, CA) and a detector (API 5500; ABSciex, Framingham, MA). The lower limit of quantitation was 40 nmol/L, linearity was tested up to 10 000 nmol/L, and coefficient of variation was less than 5.2%. The insert from the manufacturer suggested that MMA concentration greater than 0.27 nmol/mL was elevated; in this study, we used the age and sex cutoffs for MMA defined by the US Centers for Disease Control and Prevention: age, 20 to 39 years: greater than 0.27 nmol/mL; 40 to 59 years: greater than 0.30 nmol/mL; and older than 60 years: greater than 0.45 nmol/mL. 13
The holoTC levels were measured using an automated commercial immunoassay (Architect i2000SR, Active B12; Abbott Laboratories, Abbott Park, IL). The holoTC cutoff was greater than 35 pmol/L according to information from the manufacturer.
Serum vitamin B12 and folate levels were analyzed using an electrochemiluminescence assay (Architect i2000SR). Cutoff value for serum vitamin B12 was 148 pmol/L, and folate was 3.1 ng/mL according to information from the manufacturer. Levels of aspartate aminotransferase and alanine aminotransferase, kidney function tests (Cobas 8000 modular analyzer; Roche Diagnostics, Indianapolis, IN), and complete blood count with differential (Coulter-Celldyne 3700; Abbott Laboratories) were determined for each patient. Normal serum creatinine was less than 1.1 mg/dL for women and less than 1.3 mg/dL for men. Total plasma homocysteine was determined (Immulite 2000; Siemens Healthcare Diagnostics, Deerfield, IL); according to the manufacturer, plasma homocysteine of greater than 13 mol/L was considered elevated. Anemia was defined as hemoglobin of 12.2 g/dL or less for women and 13.6 g/dL or less for men.
Statistical Analysis
Data analysis was performed with statistical software (SPSS, version 10.0 [SPSS Inc, Chicago, IL]; MedCalc 14.10.2 evaluation version [MedCalc Software, Ostend, Belgium]). Normally distributed data were compared with 1-way analysis of variance, and non–normally distributed data were compared with Mann-Whitney U test. Multiple linear regression and correlation were used to evaluate associations between continuous data. Categorical associations were evaluated using χ2 test and multiple logistic regression. Goodness of fit was determined with Nagelkerke R2 and Hosmer-Lemeshow goodness-of-fit test. Performance of holoTC and homocysteine was assessed using receiver operating characteristic (ROC) curve analysis and calculation of area under the curve (AUC) of the ROC curves. Statistical significance was defined by P ≤ 0.05.
Results
The vitamin B12, folate, homocysteine, holoTC, and MMA levels were similar between men and women, but hemoglobin levels were lower in women than in men (women, 12.2 ± 1.6 g/dL; men, 13.2 ± 2.4 g/dL; P ≤ 0.04). Prevalence of anemia was 56.9% and was similar for men and women.
Most patients had essential thrombocytosis (Table 1). Median duration from diagnosis of a myeloproliferative disorder was 6 years (range, 2 months to 18 years), and median duration of follow-up at our clinic was 24 months (range, 3–24 months). All patients received a stable dose of hydroxyurea during the study, but this was changed to interferon α after several weeks in 1 patient. There were 56 patients (97%) who received antiplatelet therapy and 52 patients (90%) who received allopurinol. Steroids were used only in the short term in 1 patient, and no patients used androgens.
Demographic and Laboratory Parameters of Patients Who Had Myeloproliferative Disorders*
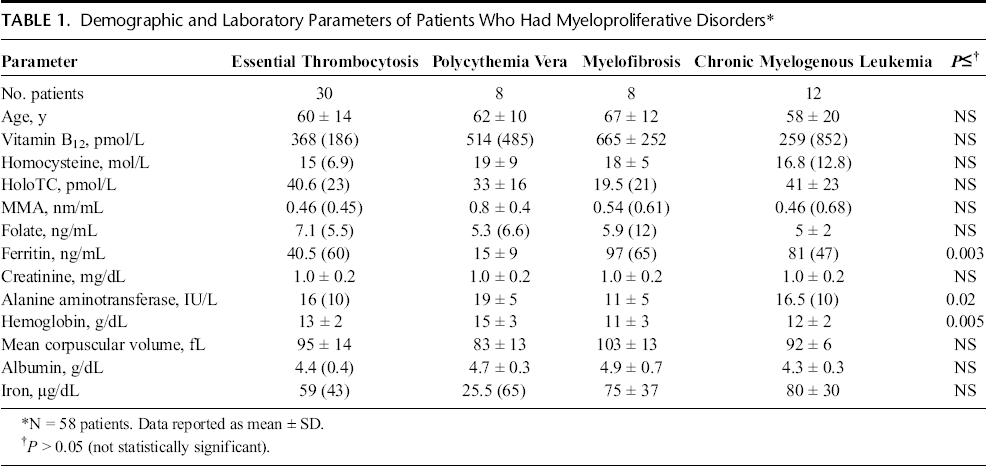
Laboratory parameters did not differ between patients who had different diagnoses, except that ferritin level was lower and alanine aminotransferase and hemoglobin levels were higher in patients who had polycythemia vera than other diagnoses (Table 1). Vitamin B12 levels were increased in all except 1 patient. Anemia was present in 32 patients (55%), including 23 patients who had vitamin B12 deficiency based on elevated MMA. In patients who had vitamin B12 deficiency, 8 patients had coexisting iron deficiency, and 3 other patients had mild folate deficiency (folate, 2.7–3.0 ng/mL).
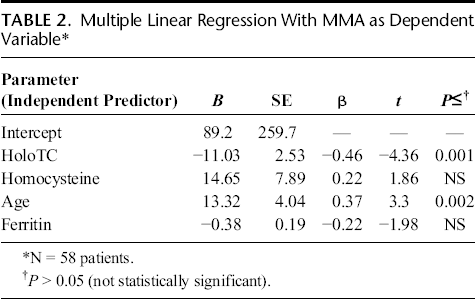
The MMA level was positively correlated with homocysteine (r = 0.263; P ≤ 0.004) and negatively correlated with holoTC (r = −0.456; P ≤ 0.001). Age was positively correlated with MMA (r = 0.332; P ≤ 0.001). Serum creatinine was not correlated with MMA (r = 0.085; not significant). Multiple regression analysis for continuous variables (MMA as the dependent variable) showed that the best model included holoTC, homocysteine, age, and ferritin as independent predictors (Table 2); assumptions of multiple linear regression were met. The model explained 42.5% variation in MMA level, and inclusion of other parameters such as creatinine level did not improve the model.
Multiple Linear Regression With MMA as Dependent Variable*
The prevalence of vitamin B12 deficiency according to MMA level was 69%. In patients who had elevated MMA level, 12 patients had macrocytosis, and 8 patients had neutrophil hypersegmentation, both of which were not associated with elevated MMA (not significant). The MMA level was not associated with sex (not significant).
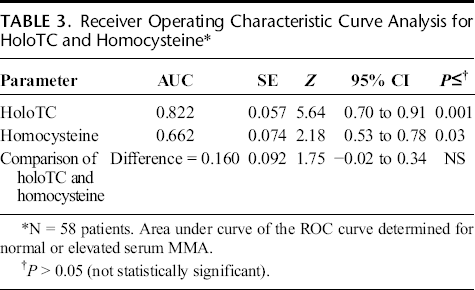
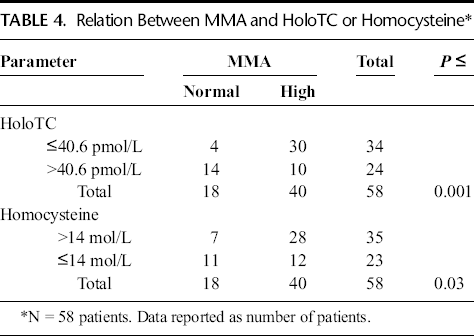
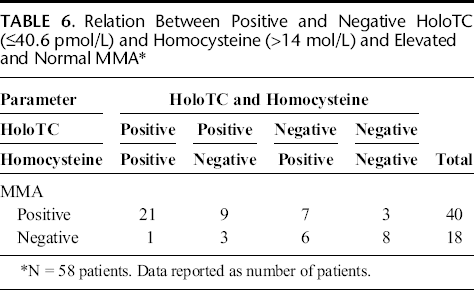
The ROC curve analysis for holoTC and homocysteine, with MMA as the B12 status variable, showed statistically significant AUC values (Table 3). The AUC was similar for holoTC and homocysteine (Table 3 and Fig. 1). There were significant associations between high MMA level and low holoTC or high homocysteine levels (Table 4). The sensitivity, specificity, positive likelihood ratio, positive predictive value, and negative predictive value were greater for holoTC than for homocysteine (Table 5). Holotranscobalamin and homocysteine agreed with MMA in most cases (Table 6 and Fig. 2).
Receiver Operating Characteristic Curve Analysis for HoloTC and Homocysteine*
Relation Between MMA and HoloTC or Homocysteine*
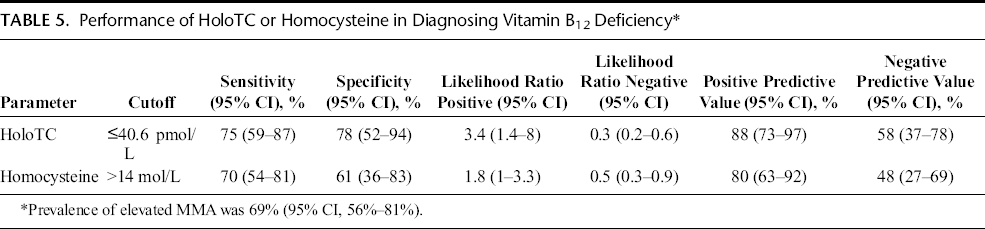
Performance of HoloTC or Homocysteine in Diagnosing Vitamin B12 Deficiency*
Relation Between Positive and Negative HoloTC (≤40.6 pmol/L) and Homocysteine (>14 mol/L) and Elevated and Normal MMA*
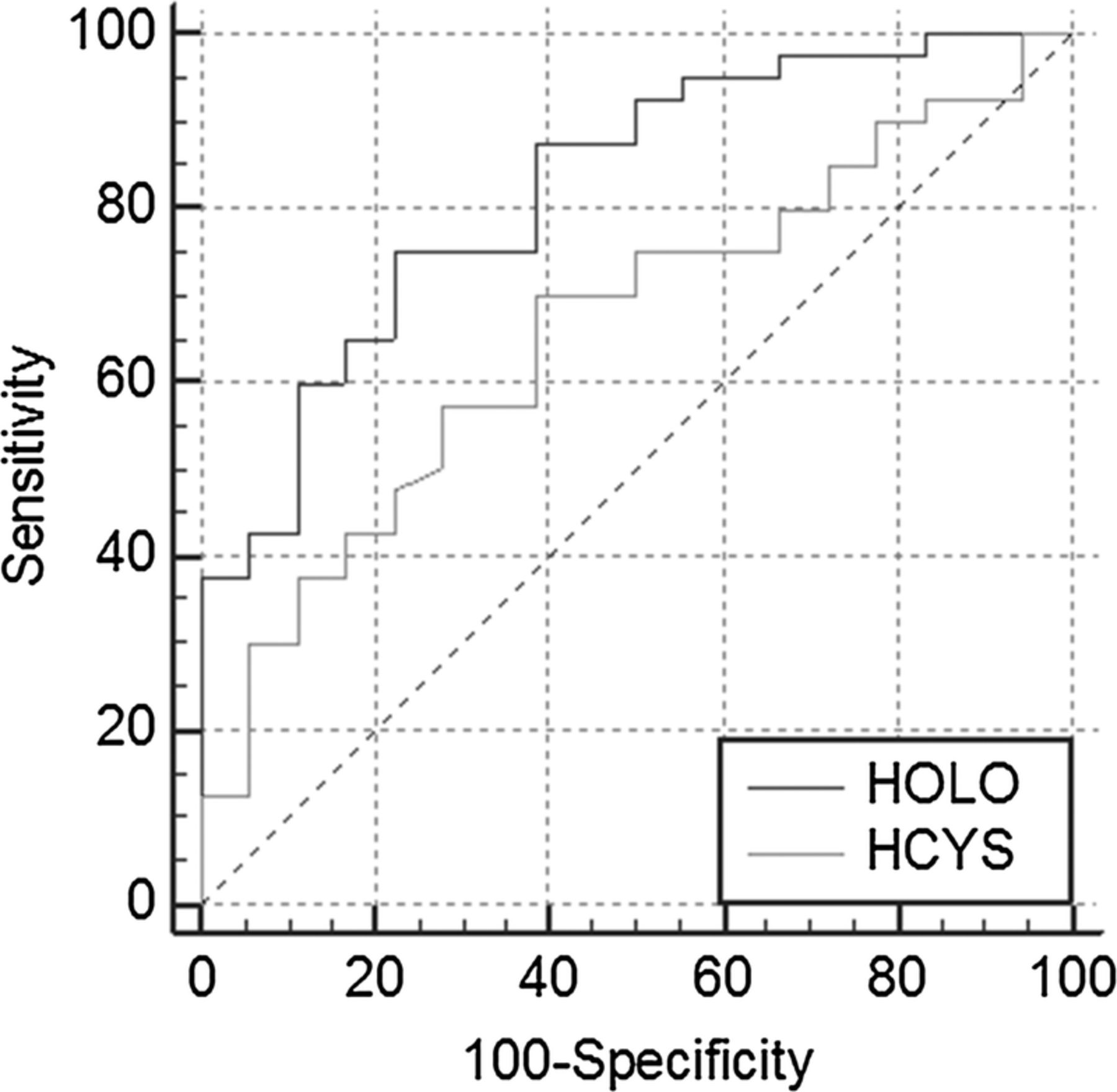
Receiver operating characteristic curve for holoTC and homocysteine. Methylmalonic acid level according to age and sex was categorized for B12 status.
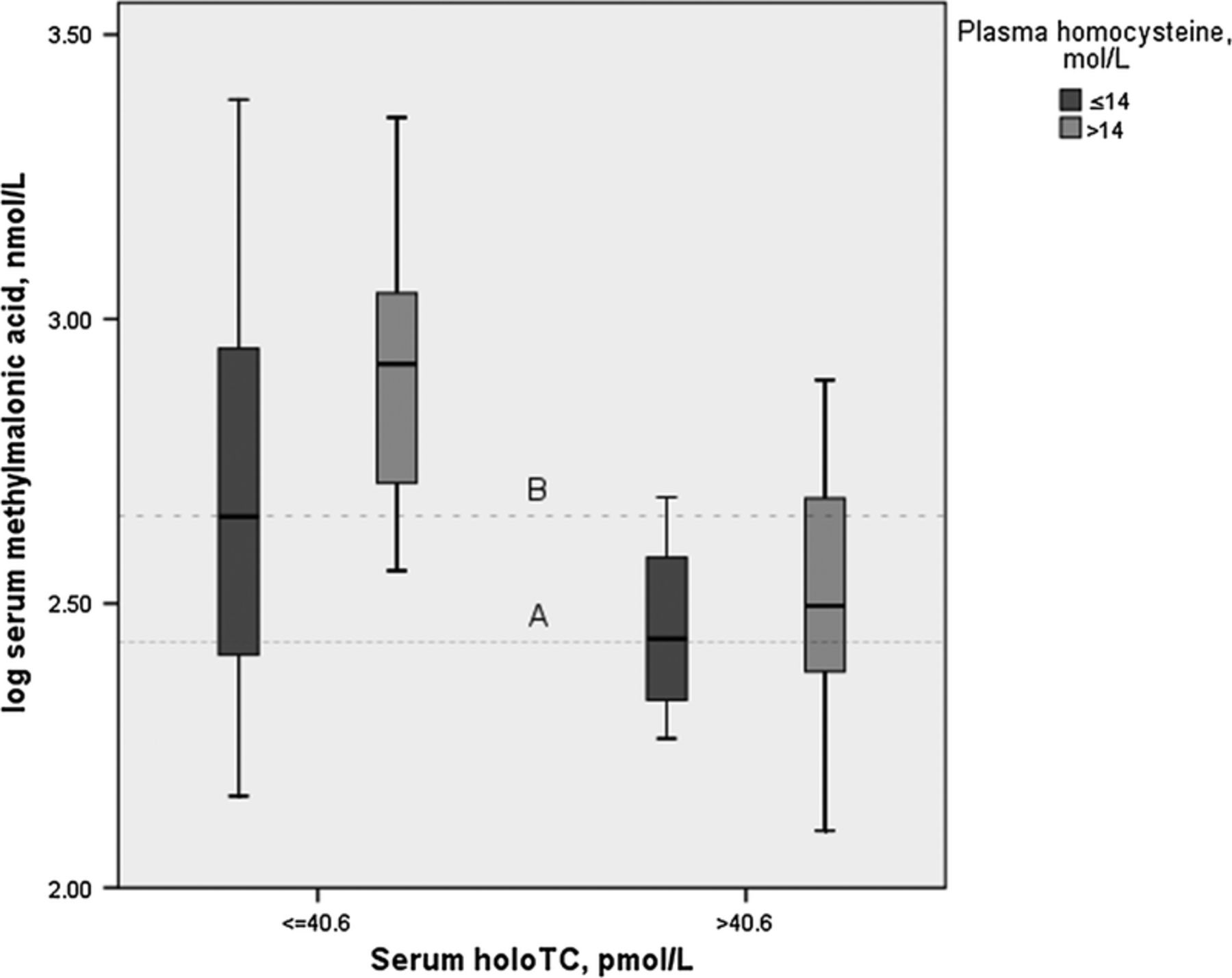
Relation between MMA, holoTC, and homocysteine levels in patients who had chronic myeloproliferative disorders. Reference lines represent MMA cutoff values (line A, 0.27 nmol/mL; line B, 0.45 nmol/mL).
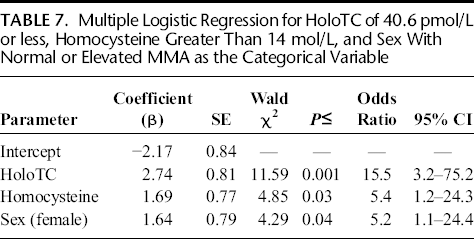
When multivariate logistic regression analysis was performed with vitamin B12 status as the state variable, the best model included holoTC of 40.6 pmol/L or less, homocysteine of greater than 14 mol/L, and sex as categorical variables for predicting elevated MMA levels (Table 7). Assumptions of logistic regression were met. Nagelkerke R2 was 47.7%, and Hosmer-Lemeshow goodness-of-fit test was not significant.
Multiple Logistic Regression for HoloTC of 40.6 pmol/L or less, Homocysteine Greater Than 14 mol/L, and Sex With Normal or Elevated MMA as the Categorical Variable
Discussion
In this study, prevalence of vitamin B12 deficiency in patients with myeloproliferative disorders was 69% based on MMA levels. Serum holoTC, homocysteine, and ferritin accounted for 42.5% variation in serum MMA. Although the AUCs were similar for holoTC and homocysteine, the holoTC cutoff that was defined by ROC curve analysis in diagnosing vitamin B12 deficiency was better than the cutoff for homocysteine, with higher sensitivity, specificity, and positive predictive value for holoTC than homocysteine (Table 5). Logistic regression showed that patients with serum holoTC of 40.6 pmol/L or less were 15.5-fold more likely to have vitamin B12 deficiency than patients with serum holoTC greater than 40.6 pmol/L, and patients with homocysteine of greater than 14 mol/L were 5.4-fold more likely to have vitamin B12 deficiency than patients with homocysteine of 14 mol/L or less (Table 7). Serum vitamin B12 levels did not assist in the diagnosis because they were elevated in all except 1 patient. Furthermore, macrocytosis and neutrophil hypersegmentation were not significantly associated with elevated MMA.
Diagnosis of subclinical vitamin B12 deficiency with the available markers is difficult. The MMA and homocysteine levels, but not holoTC levels, are affected by small changes in renal function and increase with increased age. 14 In the present study, serum MMA was correlated with age (Table 2); therefore, we used age-specific cutoffs for MMA defined by the US Centers for Disease Control and Prevention to overcome the effect of age. 13 For sex effect, despite the absence of an association between MMA and sex, we used upper limits of 95% confidence interval (CI) for age groups 20 to 59 years and mean for age of older than 60 years, which were about the same for both sexes to obtain a categorical variable of MMA level. We preferred the available report from 2008 because 95% CIs were available, study populations were large, and general population data were preferred over ethnic classifications.
The holoTC, which is the active form of vitamin B12, may be an optimal marker for vitamin B12 deficiency, even better than serum vitamin B12 level in population-based assessment studies. 15 Although not affected by small changes in renal function or sex (except in 1 study 16 ), a more rational approach is needed. 8 In a multicenter evaluation of laboratory performance noting cutoffs of holoTC from 11 to 41 pmol/L, higher values were more representative of normal vitamin B12 status. 17 In agreement with this suggestion and other studies, 18 we observed that holoTC performed best as a marker of vitamin B12 deficiency at a holoTC cutoff of 40.6 pmol/L or less. In a large cohort of elderly people, a cutoff of holoTC = 44 pmol/L performed best for absolute vitamin B12 deficiency (defined by MMA >0.75 nmol/mL) in patients with normal renal function. 19 The slightly lower cutoff for holoTC in the present study may have occurred because we had younger patients (45% patients aged <60 years), and we studied patients who had myeloproliferative disorders and not healthy subjects. In the present study, the best performing cutoff for plasma homocysteine was greater than 14 mol/L, consistent with a cutoff greater than 15 mol/L defined in 937 otherwise healthy subjects who had elevated MMA levels. 20 Population characteristics might explain the small difference in cutoff values between studies.
Confirmation of MMA status by a second test was limited to holoTC and homocysteine in our study. In patients who had elevated MMA level, there were 3 patients in whom both holoTC and homocysteine tests were negative, possibly because of false-positive MMA results (Table 6). In contrast, there was 1 patient with positive holoTC and homocysteine tests in whom serum MMA was not elevated, possibly representing a false-negative result in our study. Therefore, prevalence of vitamin B12 deficiency may be 65.5%; when holoTC is included as the second test (accepting 10 possible false-negative results as true), prevalence may be 51.7%, which still would be considered high. Although macrocytosis may have low specificity for vitamin B12 deficiency without megaloblastic changes such as neutrophil hypersegmentation, 8 these findings were not associated with MMA status in our study, possibly because of confounders such as hydroxyurea-associated hypersegmentation and coexisting folate and iron deficiency in our patients.
The prevalence of vitamin B12 deficiency in our study was higher than previously reported in patients who had myeloproliferative disorders. 3 As in our study, serum vitamin B12 levels measured by electrochemiluminescence assay were normal to high in all patients who had myeloproliferative disorders. The previous study used laboratory-provided cutoffs (>0.318 and >0.376 nmol/mL) for serum MMA to diagnose vitamin B12 deficiency. There were differences between the previous and present study including confounding factors such as age, sex, and renal function; lack of a second test such as holoTC; and a smaller sample size in the previous study. 3 These factors were taken into account with the present larger sample, suggesting that the present results may more closely represent vitamin B12 status in patients who have myeloproliferative disorders.
In typical vitamin B12 assays, total serum vitamin B12 is measured, which includes both bound and free forms. 21 Most (70%–90%) vitamin B12 is bound to haptocorrin, and less (10%–30%) vitamin B12 is bound to transcobalamin as the metabolically active form. Elevated vitamin B12 levels in patients who have myeloproliferative disorders have been explained by increased haptocorrin synthesis, which likely was the primary mechanism in our study. 22 Immune complex forms of circulating vitamin B12 also may cause falsely elevated vitamin B12 levels.23,24 Although this mechanism may account for 8% elevated vitamin B12 levels in blood samples received during routine vitamin B12 evaluation, our unpublished preliminary work suggests that immune complexes may account for a larger percentage of elevated vitamin B12 levels in patients who have myeloproliferative disorders than normal subjects (data not shown).
Limitations of the present study included the limited focus of studying patients who had a rare condition and the need to exclude patients who had elevated serum creatinine level. Larger studies are necessary to determine disease-specific cutoff assessment in patients who have myeloproliferative disorders. In addition, serum homocysteine remained correlated with serum creatinine. Although mild, there was folate deficiency in 4 patients (6.9%). Therefore, serum homocysteine levels probably did not depend solely on vitamin B12 status in our patients.
Strengths of the present study included the evaluation of vitamin B12 deficiency using MMA, holoTC, and homocysteine levels. The effects of renal function were minimized by studying only patients who had normal serum creatinine. The MMA was not correlated with serum creatinine. The effects of age and sex were taken into account when assessing MMA status. Potentially false test results were minimal. Cutoff values for holoTC and homocysteine were defined for patients who had myeloproliferative disorders. The present study may be unique in comprehensively evaluating vitamin B12 status and holoTC and homocysteine levels in patients who had myeloproliferative disorders.
In summary, the present study showed a high prevalence of vitamin B12 deficiency in patients who had myeloproliferative disorders, despite normal to high serum vitamin B12 levels. We identified novel performance characteristics for holoTC and homocysteine levels in these patients. Patients with serum holoTC of 40.6 pmol/L or less were 15.5-fold more likely and patients with homocysteine of greater than 14 mol/L were 5.4-fold more likely, to have vitamin B12 deficiency than patients with holoTC greater than 40.6 pmol/L and homocysteine of 14 mol/L or less. Early diagnosis and treatment of vitamin B12 deficiency in patients who have myeloproliferative disorders necessitate prompt assessment of vitamin B12 status, to prevent reversible bone marrow failure and demyelinating neurologic disease. The holoTC level may replace conventional vitamin B12 level as the optimal initial test for this patient group and may replace vitamin B12 level as a second direct test for metabolic indicators.