
Abstract
Background
Aminopeptidase N (APN; EC 3.4.11.2) is a membrane dimeric metallopeptidase involved in differentiation, development, and proliferative processes of several tissues. Recent studies have demonstrated the increased expression and activity of this enzyme in several cancers. However, there are no available data about the impact of this peptidase in the biological aggressiveness and the survival of colorectal cancer (CRC) patients.
Methods
The activity and mRNA expression of APN in tumor tissue (n = 81) and plasma (n = 40) of patients with CRC of low and high grades and stages were prospectively analyzed by fluorimetric and quantitative reverse transcriptase–polymerase chain reaction methods. Data obtained in adenoma and CRC were compared with those from the surrounding normal mucosa. Classic clinical and pathological parameters were stratified following APN data and analyzed for 5-year survival.
Results
mRNA levels of APN (ANPEP) were lower in colorectal adenomas and adenocarcinomas than in the surrounding uninvolved mucosa (Kruskal-Wallis, P < 0.001). Aminopeptidase N activity in CRC tissue was higher in patients with better overall survival (log-rank P < 0.05, Cox analysis P < 0.05). By contrast, higher plasmatic APN activity correlated with worse overall survival (log-rank P < 0.01, Cox analysis P < 0.05).
Conclusions
Aminopeptidase N activity in tissue and plasma from CRC patients is an independent prognostic factor of 5-year survival. The determination of APN activity levels in the plasma may be a safe, minimally invasive, and inexpensive way to define the aggressiveness of CRC in daily practice.
Colorectal cancer (CRC) is the third commonest malignancy in the United States. In 2014, an estimated 71,830 men and 65,000 women will be diagnosed with CRC and 26,270 men, and 24,040 women will die of the disease. 1 Europe and other developed regions show similar rates of incidence and mortality. 2 This pathology is a health problem of major concern because of its increasing frequency in the last decades, perhaps as a result of worsening dietary habits. 3 Huge resources are being invested in prevention and early diagnosis of this disease. Population-based screening campaigns try to discover as much early tumors and precursor lesions as possible, aiming to decrease the incidence of the disease, to simplify the clinical management of patients once the lesion develops, and to improve survival. In consequence, mortality rates are decreasing in the last decades. 4
The recent molecular classification of CRC proposed by Jass 5 in 2007 has been of much help in the understanding of the diverse etiopathogenetic mechanisms of this disease. Adenomatous lesions in the large bowel are fully accepted precursors of CRC, 6 and the adenoma-carcinoma sequence still provides a solid model for research on carcinogenesis.
Aminopeptidases catalyze the cleavage of the N-terminal residues from peptide or protein substrates. 7 These enzymes play a key role in carcinogenesis in several ways, for instance, regulating bioactive peptides that are crucial in neoplastic growth, degrading the extracellular matrix, acting as adhesion molecules, or participating in intracellular signaling. 8 Besides, some studies have demonstrated that the activity and expression of these enzymes vary in different tumors depending on the several clinicopathologic parameters such as histological grade, stage, and patient survival.8-17 For all these reasons, peptidases may be useful tools in the development of clinical strategies for treatment and follow-up of cancer patients.
Aminopeptidase N (APN; EC 3.4.11.2) (APN), also known as CD13, is a member of M1 peptidase family present in several human tissues and particularly in absorptive epitheliums, such as the intestine. 18 It is a type II integral membrane protein located on the plasma membrane as an ectoenzyme 19 and in soluble form in different body fluids.20-22 Although its better known role is the hydrolysis of bioactive peptides, APN has been described as a “moonlighting enzyme” because of its involvement in multiple biological functions that are dependent and independent from its catalytic activity. 19
Aminopeptidase N is one of the most studied peptidase with regard to carcinogenetic processes.8,19 It has been associated with proliferation, invasion, metastasis, apoptosis, and angiogenesis, and for this reason, it has become an important target for designing anticancer agents.19,23,24 Moreover, this peptidase has been also proposed as a diagnostic/prognostic target in cancer because the expressions of its membrane-bound and soluble forms are significantly changed in several tumor tissues and plasma from cancer patients.8,10-14 In this sense, it was described that APN protein expression is correlated with histological grade, stage, and survival rates of pancreatic, gastric, and CRCs.10,25,26
Recently, we have demonstrated that the activity of APN is also altered in several solid tumors and that it is an independent prognostic factor in the survival of renal cancer patients.14-17 In this context, we also studied the activity of other peptidases in tissue and plasma from CRC patients and showed that this activity changes throughout the adenoma-carcinoma sequence 15 and that it is independently correlated with 5-year survival.27,28 As far as we know, there are no previous reports on the involvement of APN activity in CRC prognosis and survival. Therefore, the aim of the present study was to analyze in a prospective way the metabolic and expression profiles of APN in patients with CRC, analyzing tumor tissue and plasma samples, and to correlate the obtained results with classic histopathologic parameters for tumor prognosis and survival.
Patients and Methods
The authors declare that all the experiments carried out in this study comply with current Spanish laws and conform to the principles outlined in the Declaration of Helsinki. Samples and data from patients included in this study were provided by the Basque Biobank for Research-OEHUN (www.biobancovasco.org). All patients were informed about the potential use for research of their surgically resected tissues and accepted this eventuality by signing a specific document approved by the Ethical and Scientific Committees of the Basque Country Public Health System (Osakidetza) (CEIC 11/51) and the University of the Basque Country (UPV/EHU) (CEISH/158R/2012, CEIAB/123/2012).
Patients
A total of 81 patients with CRC were prospectively included in the study. Males predominated in the series (51 male patients/30 female patients), the average age being 71 years for males and 67 years for females. Mean follow-up was 50.2 months (range, 3–80 months). Follow-up was closed by December 31, 2012. At that time, 25 patients had died of disease. All patients received partial colectomies. In 16 of these patients, both adenomatous and adenocarcinomatous polyps were diagnosed. These cases were used to analyze the APN activity and mRNA levels throughout the normal mucosa–adenoma–adenocarcinoma sequence.
Preoperatively collected plasma was also analyzed in 40 of these patients (26 male patients/14 female patients; average age, 72 and 67 years, respectively). As control sample, plasma from 30 healthy volunteers with no clinical history of neoplastic diseases was used.
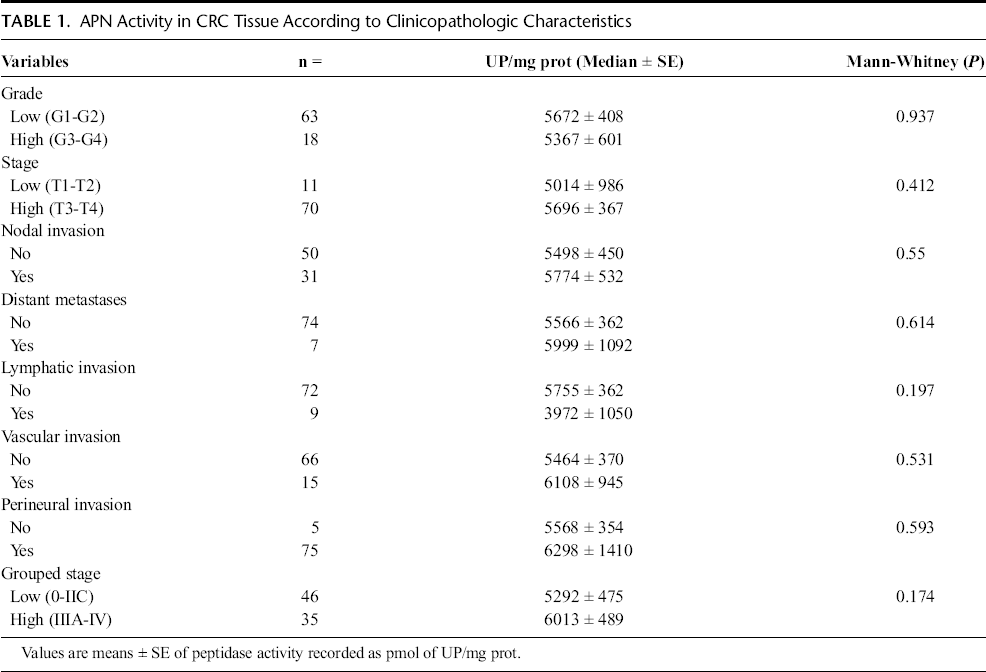
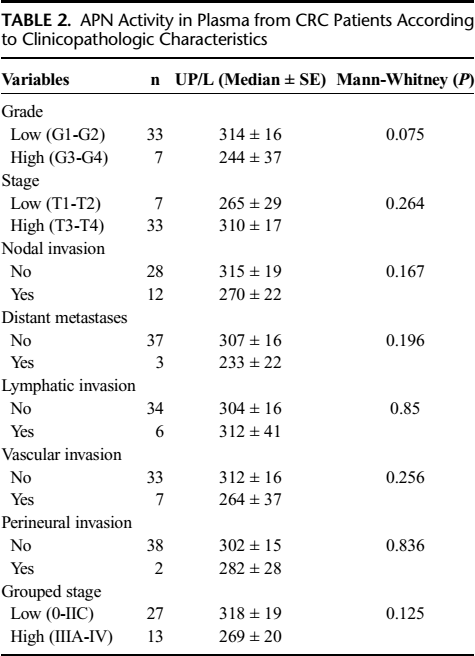
Stage and grade were assigned applying the AJCC system. 29 Tables 1 and 2 show, among other results, the clinical data included in the study, which were retrieved from the patient clinical records.
APN Activity in CRC Tissue According to Clinicopathologic Characteristics
APN Activity in Plasma from CRC Patients According to Clinicopathologic Characteristics
Tissue Specimens
Surgical resections were submitted fresh to the pathology laboratory within a period of 30 minutes after removal. Handling of specimens was performed following conventional protocols for the management of surgical resections of colon and rectum. 30 Tumor characteristics were recognized on gross examination, and selected fragments of tumor and nontumor tissues were frozen in isopentane and stored at −80 °C. Routine procedures in the pathology laboratory included formalin fixation of the surgical specimen and paraffin embedding of the tissue fragments selected for histopathologic examination. Histological slides were stained with hematoxylin-eosin. Immunohistochemistry was performed when needed. Pathological data included in the study are summarized in Table 1. Besides, peripheral venous blood samples (from patients and controls) were centrifuged at 1500 revolutions/min during 15 minutes. The obtained plasma was also stored at −80 °C.
Sample Preparation
Explanted tumor samples were homogenized in 10 mM Tris-HCl buffer at pH 7.4, for 30 seconds at 800 revolutions/min using a Heidolph PZR 50 Selecta homogenizer (Heidolph PZR 50 Selecta: Heidolph Instruments GmbH & Co. KG, Schwabach, Germany), and ultracentrifuged in a Centrikon T-2070 Kontron Instruments apparatus (Kontron Instruments, Milan, Italy) at 100,000 g for 35 minutes. The resulting supernatants were used to measure APN activity. Previously collected plasma samples were also used to determine plasmatic APN activity. All the previously described steps were carried out at 4 °C.
Neutral Aminopeptidase Activity Assays
Aminopeptidase N activity was fluorimetrically measured using a modified version of the method described by Olivo et al., 31 using Ala-β-naphthylamide (0.125 mM) as substrate. The assay is based on the fluorescence of β-naphthylamine (β-NA) generated from the substrate by APN. The components of the assay mixture (total volume 2 mL) included the following: 50 mM of sodium phosphate buffer (pH 7.4), 1.2 mM of dl-dithiothreitol, 0.15 mg/mL of bovine serum albumin, and 40 μM of puromycin, which inhibits puromycin-sensitive aminopeptidase, an enzyme that also hydrolyzes the substrate Ala-β-naphthylamide.
The reaction was initiated by adding 50 μL of tissue extract or plasma sample to 1 mL of the assay mixture. This was incubated at 37 °C for 30 minutes, and the reaction was stopped by addition of 1 mL of 0.1 M sodium acetate buffer (pH 4.2). The excitation and emission wavelengths were 345 and 412 nm, respectively. Blanks were used to determine background fluorescence. Relative fluorescence was converted into picomoles of product using a standard curve constructed with increasing concentrations of β-NA.
We also performed inhibition assays in CRC tissue and plasma with a specific inhibitor of APN (leuhistin, 50 μM) to verify that, after using puromycin, the formation of β-NA was due to the action of APN. The releasing of β-NA was mainly inhibited in tumor tissues (92%) and in plasma samples (91%).
Total Protein Determination
Protein concentration was measured in triplicate by the Bradford method, 32 using bovine serum albumin (1 mg/mL) as the calibrator. Results from the CRC tissues and from plasma samples were recorded as units of peptidase per milligram of protein (UP/mg prot) and per liter of plasma (UP/L), respectively. One unit of peptidase activity (UP) is the amount of enzyme required to release 1 pmol of β-NA per minute. Fluorogenic assays were linear with respect to hydrolysis time and protein content.
Real-Time Quantitative Reverse Transcriptase–Polymerase Chain Reaction Analysis
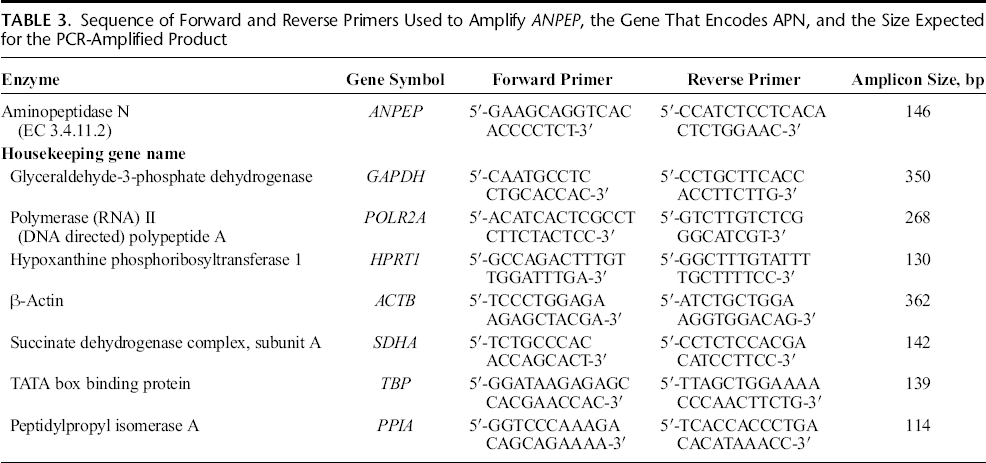
The expression of ANPEP, the gene that encodes APN, was analyzed in 16 paired samples of CRC and adjacent, apparently normal, control tissue. To avoid degradation, tissue sections were immersed in RNAlater immediately after surgery and stored at −80 °C until processed. Total RNA was extracted from 20 mg of tissue using TriReagent (Sigma, St Louis, MO). The RNA samples were then incubated with RNase-free DNase I and RNasin (Promega, Madison, WI) to remove residual genomic DNA. First-strand cDNA was synthesized from 5 μg of total RNA of each human sample using first-strand cDNA synthesis kit (Roche, Mannheim, Germany). The resulting cDNA samples were amplified by polymerase chain reaction (PCR) with specific oligonucleotide primer pairs designed with the analysis software primer 3 and synthesized by Sigma-Genosys (Cambridge, UK). Based on previous experiments on human renal cell carcinoma33,34 and other human samples, 35 we chose glyceraldehyde-3-phosphate dehydrogenase (GAPDH), polymerase (RNA) II (DNA-directed) polypeptide A (POLR2A), hypoxanthine phosphoribosyltransferase 1 (HPRT1), β-actin (ACTB), succinate dehydrogenase complex, subunit A (SDHA), TATA box binding protein (TBP), and peptidylprolyl isomerase A (PPIA) as endogenous reference genes. The sequences of the primers used to amplify ANPEP and the 7 housekeeping genes are shown in Table 3.
Sequence of Forward and Reverse Primers Used to Amplify ANPEP, the Gene That Encodes APN, and the Size Expected for the PCR-Amplified Product
The expression of ANPEP and the housekeeping genes was quantified in all cDNAs by real-time PCR using the iCycler iQ real-time detection apparatus (Bio-Rad Laboratories, Hercules, CA). Experiments were carried out essentially as described previously.27,35 Dilutions of the cDNA template were prepared from each tissue and amplified in triplicate using SensiFAST SYBR Mix (Bioline Ltd, London, UK). Three negative controls (with no template, no reverse transcriptase, and no RNA in the reverse transcriptase reaction) were also included in each plate to detect any possible contamination. After a hot start (10 minutes at 94 °C), the parameters used for PCR amplification were as follows: 10 seconds at 94 °C, 20 seconds at 60 °C, and 30 seconds at 72 °C, for 50 cycles.
Real-time PCR data were expressed as the fold change of the target gene expression relative to the geometric mean (g.m.) mRNA expression of the housekeeping genes in each sample, as described by Vandesompele et al. 36 The fold change in gene expression was calculated by the formula:

where CT is the threshold cycle, calculated by the iCycler software, [INCREMENT]CT = (CTtarget gene − CTg.m.reference genes) and [INCREMENT][INCREMENT]CT = ([INCREMENT]CTtest sample − [INCREMENT]CTcontrol sample).
Paired malignant (tumor) and uninvolved surrounding samples (normal) from the same patient were always measured in the same analytical run to exclude between-run variations. The PCR data obtained in 1 of the normal CRC samples were arbitrarily chosen as control, and this sample was included in all PCR experiments to correct for possible interassay variations. As indicated in previous works, expression measured in these systems may not always be normally distributed. 34 Thus, we performed a D'Agostino and Pearson omnibus normality test. Because expression data fitted to a Gaussian distribution, the unpaired t test was applied for all significance calculations. P < 0.05 was considered significant.
Statistical Analysis
Kolmogorov-Smirnov and Shapiro-Wilk tests were applied to data obtained from tissue and plasma samples, respectively, to know if the numbers followed or not a normal distribution. Based on this information (P < 0.05), APN activity in tissue and plasma was analyzed with nonparametric probes: Mann-Whitney U test and Kruskal-Wallis tests were used to detect differences between 2 or 3 groups, respectively. Spearman correlation test was performed to evaluate the correlation between tissue and plasmatic APN activity, tumor size, and patient age and sex.
Finally, Kaplan-Meier curves and log-rank test were performed to evaluate the association between APN activity and 5-year survival, comparing groups created by cutoff points based on median APN activity values. A Cox regression model was used to test the independent effects of clinical and pathological variables and APN activity on survival. SPSS 21.0 software (SPSS Inc, Chicago, IL) was used for the statistical analysis.
Results
Apn in Tissue Samples
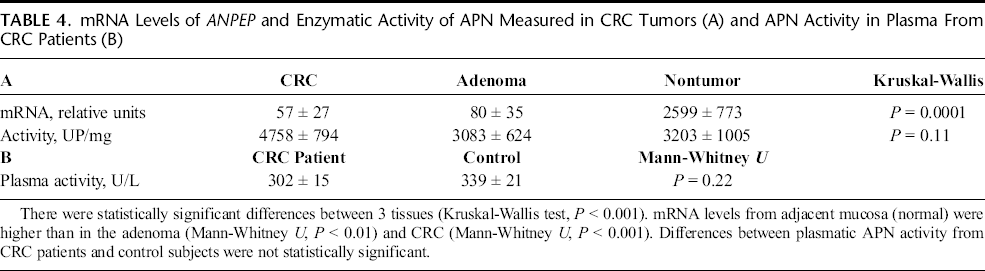
ANPEP (APN) mRNA levels were significantly lower in CRC and adenomatous polyps than in the adjacent nonneoplastic intestinal mucosa (Kruskal Wallis, P = 0.0001) (Table 4A). Inversely, APN activity was higher in CRC tissue than in both adenomatous and normal tissues; however, this trend did not reach statistical significance (Kruskal Wallis, P = 0.11) (Table 4B).
mRNA Levels of ANPEP and Enzymatic Activity of APN Measured in CRC Tumors (A) and APN Activity in Plasma From CRC Patients (B)
After stratification according to pathological variables shown in Table 1, APN activity did not show any significant change. However, 5-year overall survival (OS) of patients with CRC was better when tissue APN activity was higher than 3000 UP/mg prot (log-rank test, P = 0.014) (Fig. 1A). Multivariate analysis demonstrated that APN activity was an independent prognostic factor for OS (Cox regression model, P = 0.02) (Fig. 1B).
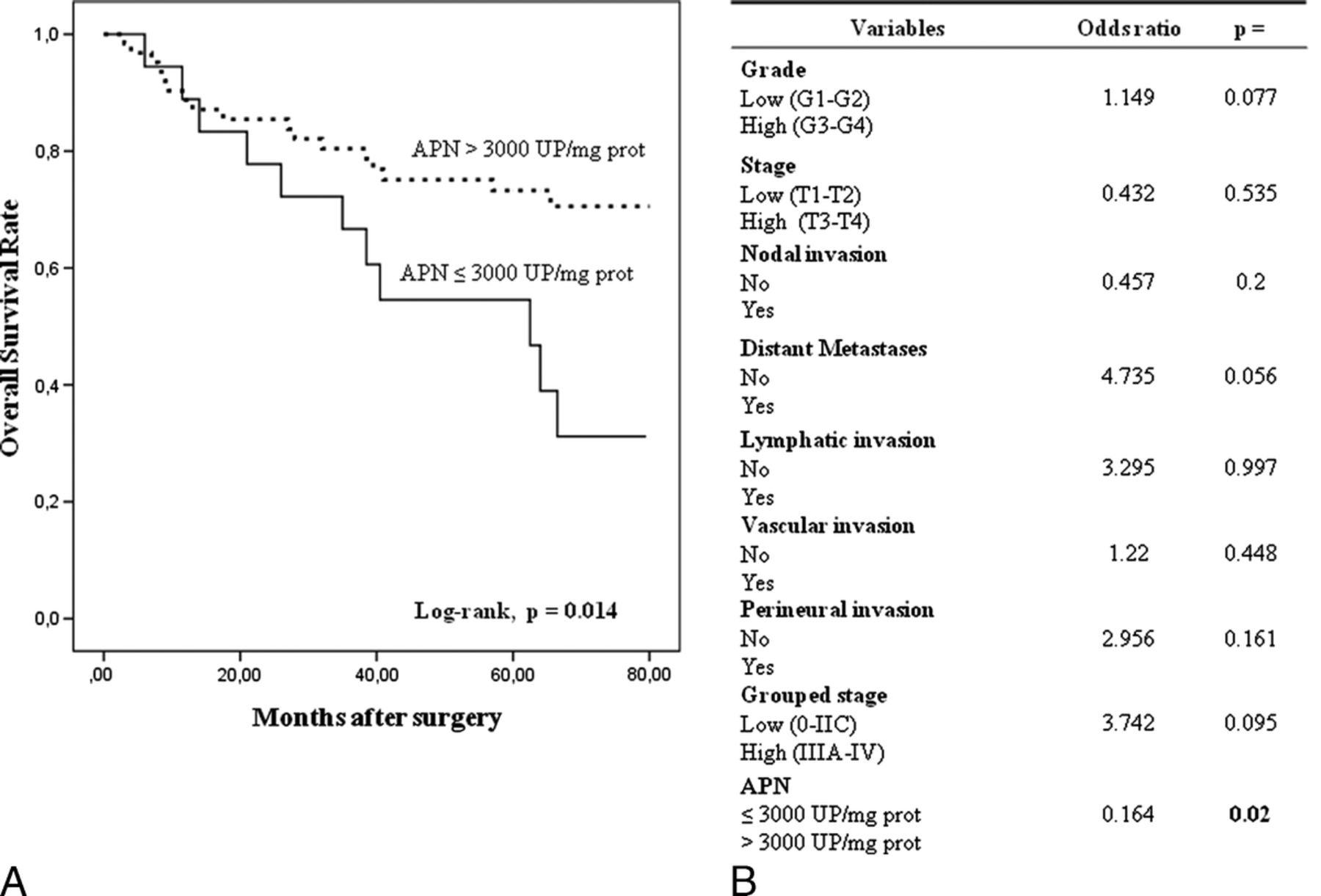
Kaplan-Meier curves and multivariate analysis (Cox regression model) with APN activity in CRC tissues. Overall survival (A) of 81 CRC patients according to their tumor APN activity pattern. Multivariate analysis of clinicopathologic variables and tumor APN activity in predicting OS (B) of patients with CRC.
Apn in Plasma Samples
Aminopeptidase N activity in plasma samples of CRC patients was similar to healthy individuals (Table 4B), and the stratification of data according to clinicopathologic variables did not throw any significant result (Table 3).
With regard to patient 5-year survival, the analysis of APN activity in plasma samples displayed opposite results to those obtained in tissue. Thus, when plasmatic APN activity was higher than 275 UP/L, the OS of CRC patients was significantly worse (log-rank test, P = 0.006) (Fig. 2A). The Cox regression model showed that APN activity was an independent factor influencing patient OS (P = 0.017) (Figs. 2B).
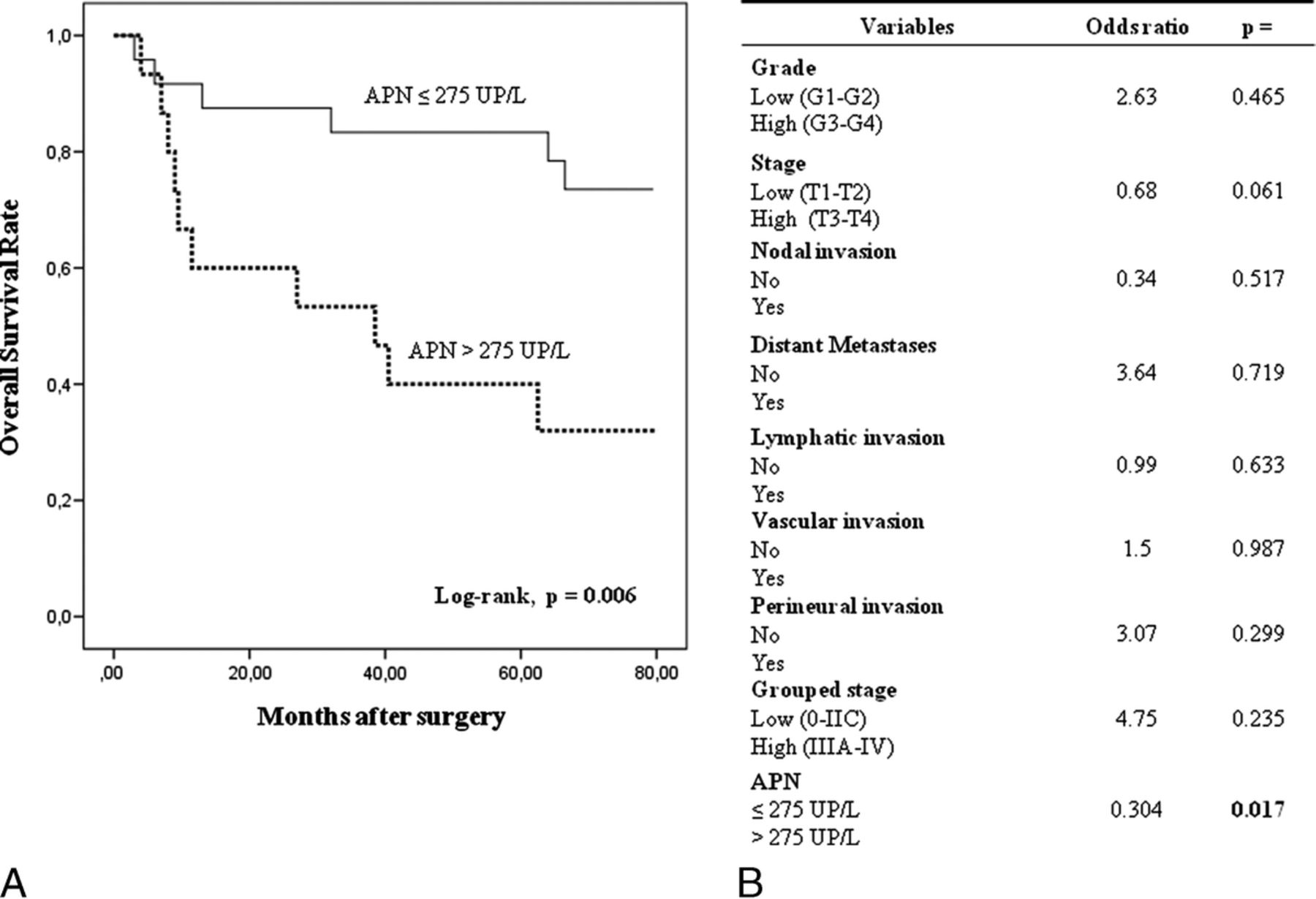
Kaplan-Meier curves and multivariate analysis (Cox regression model) with APN activity in plasma from CRC patients. Overall survival (A) of 40 CRC patients according to their plasmatic APN activity pattern. Multivariate analysis of clinicopathologic variables and plasmatic APN activity in predicting OS (B) of patients with CRC.
To better understand these opposite results, we analyzed if there is any correlation between plasmatic and tissue APN activity; however, we did not find any significant result (Spearman ρ test, r = 0.09; P =0.58). We also observed that these activities were not correlated with tumor size (r = 0.084; P = 0.61) and patient age (r = −0.161; P = 0.32) and sex (r = −0.078; P = 0.63).
Discussion
Since its initial description as the 13th “cluster of differentiation” (CD13), APN has been associated with several neoplastic processes and appeared as a therapeutic, diagnostic, and prognostic target in several hematopoietic and solid cancers.10-19,37 Previous studies showed the immunohistochemical expression of this protein in colorectal benign and malignant neoplasms and suggested that this expression is correlated with tumor aggressiveness.10,18,38 In the present work, we show the enzyme activity and mRNA expression profiles of APN in colorectal tumors and in the plasma from CRC patients.
The first relevant result was obtained in the colorectal adenoma-adenocarcinoma sequence. This term describes that the gradual progression from normal to dysplastic epithelium, and hence to carcinoma, is the result of the successive accumulation of genetic imbalances. 6 ANPEP, the gene that encodes APN, was described as a down-regulated gene in CRCs when compared with the normal surrounding mucosa. 39 Our study shows that ANPEP mRNA levels are significantly down-regulated not only in CRCs but also in their precursors, the adenomatous polyps, which indicates that these genomic imbalances occur in the first stages of neoplastic transformation of the colorectal mucosa.
This result was not correlated with the enzyme activity, which did not vary significantly throughout the colorectal adenoma-adenocarcinoma sequence. A similar result was previously reported when the APN expression was analyzed in these tissues. 38 This discrepancy between mRNA and protein, which has been described in several tumors,34,40 suggests that the protein modification of APN could occur at a posttranscriptional level and illustrates the importance of not relying only on mRNA level the evaluation of any protein change.
We have shown in recent studies that APN activity increases in head and neck cancers, 41 decreases in renal tumors, 42 and is not altered in thyroid tumors 16 when compared with the uninvolved surrounding tissues. Even more, this activity is correlated with high-grade renal cell carcinomas and with worse survival of these patients. 14 In this study, we observed that APN activity did not change significantly in colorectal tumors compared with normal mucosa. However, 5-year OS of CRC patients was significantly better when tissue APN activity was higher, pointing to this enzyme as a protein with prognostic value in this disease. Some authors stress that APN and other peptidases may change their activities depending on the tumor type or on the phase of development where the tumor is, this way suggesting that tumor growth regulation by these enzymes occurs in a tumor-specific manner.8,19 Our accumulated experience in the study of APN and other peptidases supports this idea.
Aminopeptidase N has been widely studied as a target for anticancer therapy, and several drugs are currently under clinical investigation. 23 A classic approach in this field has been the use of APN inhibitors23,43; however, the phenomenon of tumor specificity and its multifunctional nature 19 sets forth practical difficulties when applying these inhibitors. A new trend in this topic consists in the use of APN as a peptide homing receptor in malignant environment or as an enzymatic activator of cytotoxic prodrugs enabled to be activated by APN only where this enzyme is active or highly expressed, aiming to damage the neoplastic cells without modifying the enzyme functionality. 23 Because APN is active in colorectal tumor tissues, CRC patients may be beneficed by these treatments. With this regard, it has been proposed in recent clinical trials the use tumor necrosis factor fused with the tumor homing peptide asparagine–glycine–arginine motif binding in patients with metastatic CRC.23,44
Cell-surface peptidases can be released to diverse body fluids and have become useful biomarkers for helping in screening, diagnosis, staging, prognosis, and monitoring cancer therapy.8,9,12,27,28 A fully active soluble form of APN has long been recognized in several fluids of healthy subjects and cancer patients.12,20,22 Thus, it was described that higher circulating APN levels are correlated with worse survival of non–small cell lung cancer patients. 12 Increased APN activity was also demonstrated in pleural effusion, ascites, and serum from gastrointestinal, ovarian, and breast cancer patients. 22 In our study, we did not find any significant difference in the APN activity in plasma between CRC patients and healthy individuals. However, we observed that CRC patients with poorer OS had higher plasmatic APN activity. This result was independent from the other pathological variables analyzed and therefore points to plasmatic APN as a potential candidate of prognosis in patients with CRC. Further studies with higher number of patients would be advisable to confirm the diagnostic/prognostic significance of these data.
This finding is exactly the opposite of that observed with APN activity in tumor tissue samples and is in accordance with that recently reported with other plasmatic peptidases.27,28 This result could suggest an APN release from the tumor cells to the plasma as the CRC progresses and becomes more aggressive. Indeed, some authors place the origin of circulating peptidases in tumor microenvironment among others.9,12,22 However, in our study, we did not find any correlation between tissue and plasmatic APN activities, or between tumor size and APN activity. This point needs further clarification because the source of plasmatic peptidases seems critical to validate these enzymes as reliable markers of diagnosis and prognosis in cancer patients.
In summary, the present study demonstrates that APN mRNA levels are down-regulated in adenomatous and CRC tissues when compared with the uninvolved mucosa and that tissue APN and plasmatic APN are independently associated with 5-year OS of CRC patients. The determination of APN activity in the plasma is a safe, minimally invasive, and inexpensive method. Taken into account that CRC is a health problem of major concern in developed countries, the use of this enzyme as a new diagnostic tool with prognostic impact could be of help in hospital practice.
Footnotes
Acknowledgments
The authors thank Arantza Pérez (UPV/EHU) for her technical contribution to this study and Prof Juan Bilbao (UPV/EHU) for his statistical support.