
Abstract
Background
Primary aldosteronism (PA) is one of the major etiologies for secondary hypertension featuring more prominent left ventricular hypertrophy. The purpose of the study was to investigate the predictive factors of left ventricular mass index (LVMI) regression in patients with PA after adrenalectomy.
Methods
We prospectively analyzed 30 patients with aldosterone-producing adenoma (APA) who received adrenalectomy from October 2006 to September 2008. Echocardiography was performed preoperation and 1 year after operation.
Results
Thirty patients with aldosterone-producing adenoma undergoing adrenalectomy were enrolled. In a 1-year follow-up, LVMI decreased significantly by an average of 18.6%. Net LVMI decrease (ΔLVMI) was associated with preoperative LVMI, preoperative serum potassium level, baseline systolic blood pressure (SBP), baseline diastolic blood pressure, net SBP decrease (ΔSBP), net diastolic blood pressure decrease, preoperative/postoperative change of log-transformed plasma aldosterone concentration, preoperative/postoperative change of log-transformed plasma renin activity, and preoperative/postoperative change of serum potassium level (Δserum potassium level). In a multiple regression analysis, preoperative LVMI (β = −0.287, P = 0.049), ΔSBP (β = 0.518, P = 0.01), and Δserum potassium level (β = −20.471, P = 0.014) were significantly correlated with ΔLVMI.
Conclusions
The LVMI in patients with PA regressed significantly after adrenalectomy. Preoperative LVMI, ΔSBP, and Δserum potassium levels are independent factors associated with the degree of LVMI regression.
Primary aldosteronism (PA) is characterized by the inappropriate production of aldosterone and is currently considered as the most prevalent cause of secondary hypertension.1–3 The incidence of PA is around 5% to 13% of hypertensive patients. 4 Despite the hemodynamic effects derived from high blood pressure (BP), excessive aldosterone directly influences the cardiovascular system, causing larger left ventricular (LV) mass, increased myocardial fibrosis, and increased vascular stiffness in patients with PA.5–10 Therefore, patients with PA suffer more cardiovascular events and atrial fibrillation, which are independent of BP effects, than patients with essential hypertension. Treatment of PA, either by surgical or medical management, results in regression of LV hypertrophy as well as improvement of myocardial fibrosis and vascular stiffness.10–12
Hypokalemia, a major characteristic of PA, plays an important role in various cardiovascular diseases and affects both cardiac structure and function. 13 Potassium deficiency not only leads to change in cardiac structure and increased cardiac fibrosis14,15 but also influences myocardial contractile and relaxation responses.16,17 Hypokalemia is also associated with damage in the cardiovascular system in patients with PA. First, patients with hypokalemic PA have been observed to have a higher cardiovascular morbidity than patients with normokalemic PA. 18 Second, in our previous study, serum potassium level was significantly associated with LV mass in patients with PA. 19 Furthermore, in one of our more recent studies, patients with hypokalemic PA had a greater increase in vascular stiffness compared with patients with normokalemic PA. 20 This implies that hypokalemia may therefore play a role in the damage of the cardiovascular system in patients with PA.
Although there are many studies demonstrating the effect of adrenalectomy on LV mass regression, the predictive factors still require elucidation. In a retrospective study from our group, preoperative LV mass index (LVMI) and differences between preoperation/postoperation systolic BP (SBP) were associated with the degree of LVMI decrease. 21 However, that study was limited by its retrospective setting and irregular follow-up duration. Furthermore, it is also interesting to study whether serum potassium or its change after adrenalectomy influences the degree of LVMI regression after adrenalectomy. For these reasons, we conducted this prospective study to investigate the predictive factors of LVMI regression in patients with PA after adrenalectomy.
Materials and Methods
Patients
This prospective study enrolled 30 patients with aldosterone-producing adenoma (APA) who were scheduled to receive adrenalectomy and registered in the Taiwan Primary Aldosteronism Investigation (TAIPAI) database from October 2006 to September 2009. The database was constructed for quality assurance by 2 medical centers (National Taiwan University Hospital [NTUH], Taipei; Taipei Medical University Hospital, Taipei), 3 metropolitan hospitals (Cardinal Tien Hospital, New Taipei City; Taipei Tzu Chi Hospital, New Taipei City; Yun-Lin Branch of NTUH, Douliou City), and 2 local hospitals (Hsin-Chu Branch of NTUH, Hsin-Chu City; Zhongxing Branch of Taipei City Hospital, Taipei). 22 The serum potassium levels were measured during the first evaluation of these patients and 1 year after adrenalectomy. Plasma renin activity (PRA) was measured as the generation of angiotensin I in vitro using a commercially available radioimmune assay kit (Cisbio, Bedford, MA), and plasma aldosterone concentration (PAC) was measured by radioimmune assay with commercial kits (Aldosterone Maia Kit; Adaltis Italia, Bologna, Italy). Medical histories, including demographics and medication, were carefully recorded. This study was approved by the institutional review board of National Taiwan University Hospital, Taipei, Taiwan, and all patients signed informed consent.
Diagnosis Criteria for APA
The confirmation of PA and its subtype-differentiating protocol of the TAIPAI group were described previously.23–25 Briefly, APA is diagnosed on the basis on the following 4 conditions: (1) autonomous excess aldosterone production evidenced with an aldosterone-to-renin activity (ARR) of greater than 35, a TAIPAI score higher than 60%, 26 and postsaline-loading PAC of greater than 10 ng/dL; (2) adenoma evidenced with a computed tomography scan for preoperative evaluation; (3) lateralization of aldosterone secretion at adrenal venous sampling or during dexamethasone suppression NP-59SPECT/CT 27 ; and (4) pathologically proven adenoma after an adrenalectomy for those with operations and subsequent emergence of either a cure pattern of hypertension without antihypertensive agents or improvement in hypertension, potassium, PAC, and PRA.23,24 In this study, all patients received adrenalectomy, and all at least fulfilled conditions 1, 2, and 4.
Echocardiography
A Hewlett-Packard 5500 ultrasound system with an S3 transducer (1.0–3.0 MHz) was used in this study. Transthoracic echocardiographic images were acquired in the fundamental imaging mode. Two-dimensional, M-mode Doppler and tissue Doppler ultrasonography were performed on each patient. Chamber dimensions, wall thickness, and the LV ejection fraction (M-mode) were measured via the parasternal long-axis view. The LVMI was calculated according to the method by Devereux and Reichek. 28 The ΔLVMI was defined as the difference of LVMI after operation (postoperative LVMI minus preoperative LVMI).
Statistics
Data were expressed as mean (SD). Pearson correlation test was used to analyze the association between LVMI (or ΔLVMI) and their determinants. Data of PAC, PRA, and ARR were log transformed because of non-normality and was tested by the Kolmogorov-Smirnov test. Significant determinants derived from Pearson correlation test (P < 0.05) were then tested by a multivariate linear regression test with stepwise subset selection to identify independent factors predicting ΔLVMI. Statistical analyses were performed with SPSS for Mac version 21 (SPSS Inc, Chicago, IL). A P value of <0.05 was considered to indicate statistical significance.
Results
Patient Characteristics and Clinical Outcome after Surgical Treatment
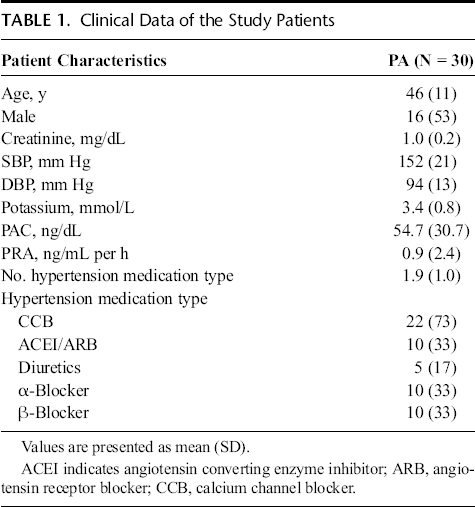
Thirty patients (male, 16) were enrolled in this study with a mean age of 46 years. The average baseline SBP was 152 mm Hg, diastolic BP (DBP) was 94 mm Hg, and serum potassium level was 3.4 mmol/L. The detailed demographic data are listed in Table 1.
Clinical Data of the Study Patients
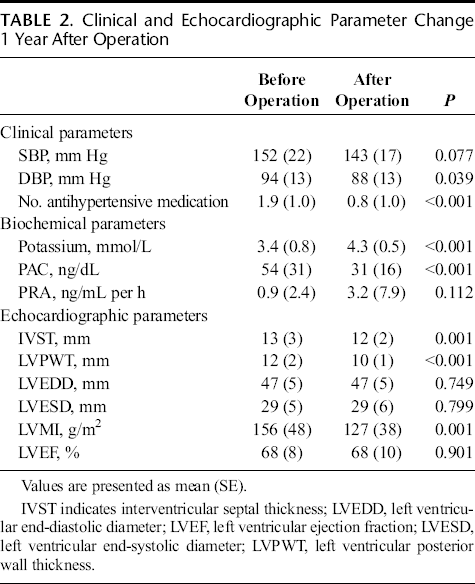
One year after adrenalectomy, the usage of the antihypertensive agents and DBP was significantly reduced. The potassium levels increased and the serum aldosterone levels decreased significantly. The interventricular septum thickness, posterior wall thickness, and LVMI also reduced significantly. These findings are listed in Table 2.
Clinical and Echocardiographic Parameter Change 1 Year After Operation
The Determinants of Baseline Lvmi and Ιlvmi
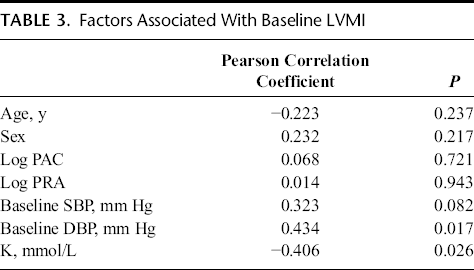
Baseline LVMI was significantly negatively associated with serum potassium level and positively associated with baseline DBP (Table 3).
Factors Associated With Baseline LVMI
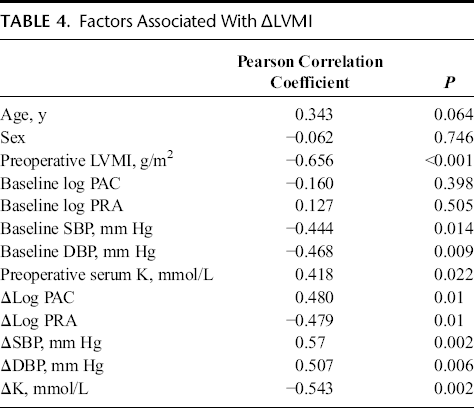
As for the regression of LVMI (ΔLVMI), the change of serum potassium level (postoperative minus preoperative serum potassium level, ΔK) had a strong negative correlation (P = 0.002). Other significant factors associated with LVMI regression included baseline LVMI, SBP, DBP, serum potassium level, the differences between preoperation/postoperation SBP (postoperative minus preoperative DBP, ΔSBP), DBP (postoperative minus preoperative DBP, ΔDBP), log PAC (postoperative minus preoperative log-transformed PAC, Δlog PAC), and log PRA (postoperative minus preoperative log-transformed PRA, Δlog PRA; Table 4).
Factors Associated With ΔLVMI
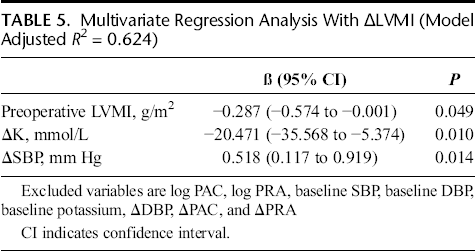
We put the significant factors (P < 0.05 in correlation study) into a multi-regression analysis, and only baseline LVMI (β = −0.287, P = 0.049), ΔK (β = −20.471, P = 0.01), and ΔSBP (β = 0.518, P = 0.014) were independent factors predicting ΔLVMI (Table 5).
Multivariate Regression Analysis With ΔLVMI (Model Adjusted R2 = 0.624)
Discussion
The major findings of our study are the following: (1) adrenalectomy decreased LVMI significantly in patients with APA; (2) baseline LVMI was significantly negatively associated with serum potassium level; and most importantly, (3) ΔLVMI was significantly associated with ΔK, baseline LVMI, and ΔSBP.
Aldosterone is the hormone produced from the renin-angiotensin-aldosterone axis responsible for body fluid homeostasis. However, long-term exposure to excess plasma aldosterone develops progressive LV geometric changes, diastolic dysfunction, myocardial fibrosis, and cardiovascular damage.29,30
In comparison with patients with essential hypertension or other types of secondary hypertension, patients with PA tend to have higher LVMI. 7 Aldosterone has been suggested to possibly directly stimulate myocardial hypertrophy through activating protein kinase C, ERK1/2, and JNK. 31 However, despite the direct involvement in the pathogenesis, clinical studies found that PAC, PRA and ARR were only weakly correlated with LVMI in patients with PA.19,32 The same condition was also observed in the present study. One explanation is that plasma aldosterone level is influenced by many factors such as sodium intake, medication, 33 or circadian rhythm. 34 Therefore, a single time-point plasma level might not represent a good correlation with the chronic exposure of myocardium to aldosterone for a long period, and for this reason, other parameters should be incorporated to evaluate the true severity of aldosteronism. Another reason for the poor correlation of LVMI with PAC could be the variable duration of disease before diagnosis, which is usually impossible to determine. In our previous study, the 24-hour urinary aldosterone level was significantly correlated with LVMI, but the plasma PAC was not. 35 In contrast, serum potassium level seems to be a valuable parameter associated with LVMI. Patients with PA and lower plasma potassium levels tend to have higher aldosterone level and higher LVMI. 6 After multivariable regression analysis, this study in combination with our previous study reveals that the serum potassium level is an independent predictive factor to LVMI, 19 indicating an important correlation between serum potassium levels and LVMI in patients with PA. The current study further demonstrates the association between ΔK and ΔLVMI, thus implying that ΔK may be a parameter for better recovery from previous hyperaldosteronism after treatment.
The effects of hypokalemia in cardiovascular system are complex. Not only related to the arrhythmia, hypokalemia leads to change in cardiac structure change, increase in cardiac fibrosis, and influences on cardiac contractility and relaxation.14–17 Several explanations have been proposed trying to unveil the underlying mechanism of how the serum potassium affects the myocardium physiology. In vitro and in animal models, hypokalemia may cause a hypertrophic response.36,37 Reductions in extracellular potassium concentration produce a rapid and sustained increase of cytosolic calcium levels as well as a hypertrophic response of the myocytes in a dose-dependent manner. The alternation of Na/K-ATPase activity may also be involved. 36
The physiological role of potassium is especially complex in patients with PA. Because the renal effect of aldosterone has the tendency to excrete potassium, hypokalemia is a specific character in PA. Approximately, half of patients with PA have hypokalemia in their medical history or biochemical tests.18,23 In a study from the German Conn registry, patients with hypokalemic PA have a higher cardiovascular morbidity than patients with normokalemic PA. 18 Further, patients with hypokalemia have a higher degree of LV hypertrophy and vascular stiffness than patients with normokalemic PA.19,20 Hypokalemia seems to be a specific characteristic and is detrimental to the cardiovascular system in patients with PA. Despite the effect of hypokalemia itself, which was mentioned previously, 1 possibility is that hypokalemia is a characteristic of a more severe degree of hyperaldosteronism. For example, the APA subtype in patients with PA was correlated with a higher LV mass and lower serum potassium levels in a previous study, 38 thus implying that the APA subtype has more severe degree of hyperaldosteronism. Regarding the same condition among patients with APA, patients with hypokalemia may have more severe hyperaldosteronism than patients with normokalemia.
This study is the first ever to demonstrate that the change of serum potassium level (ΔK) is an independent predictive factor for the degree of LVMI regression (ΔLVMI). In a univariate analysis of ΔLVMI, both Δlog PAC and Δlog PRA were significantly associated with ΔLVMI. However, both Δlog PAC and Δlog PRA were excluded in the final multiple regression model. In the present study, ΔK was significantly correlated with Δlog PRA (data not shown). Therefore, ΔK may represent the improvement of hyperaldosteronism and ΔK may be a better predictor than other clinical parameters.
In a previous study by Catena et al., 39 ΔLVMI was correlated with BP changes and pretreatment PAC but not with pretreatment plasma potassium and active renin. In that study, ΔK was not evaluated as a predictor for LV mass regression, but it should be noted that the study by Catena et al. 39 differed from ours in 3 important aspects. First, only half of patients with PA in Catena's study were patients with APA, whereas we included only patients with APA. A second difference is that Catena et al. 39 included both medical and surgical treatments, whereas our patients with APA only received adrenalectomy. Finally, the follow-up periods were different in both studies.
There are a number of limitations of the present study. First, our study only enrolled patients with APA undergoing surgical treatment. Whether the association would be repeated in bilateral adrenal hyperplasia patients treated by aldosterone antagonist is uncertain. Second, we did not check for KCNJ5 mutation, which is a significant factor that was recently found to be associated with LVMI. 40 Third, the patient number was relatively small and the follow-up period was short. A bigger prospective study with a longer follow-up period study is needed for confirmation of the results.
In conclusion, the LVMI regressed significantly after adrenalectomy in patients with APA. Change of serum potassium after adrenalectomy was an independent factor associated with the degree of LVMI regression.
Footnotes
Appendix
Taiwan Primary Aldosteronism Investigation (TAIPAI) Study Group: Vin-Cent Wu, MD, Yen-Hung Lin, MD, Yi-Luwn Ho, MD, PhD, Hung-Wei Chang, MD, PhD, Lian-Yu Lin, Fu-Chang Hu, MS, ScD, Kao-Lang Liu, MD, Shuo-Meng Wang, MD, Kuo-How Huang, MD, Yung-Ming Chen, MD, Chin-Chi Kuo, MD, Shih-Chieh Chueh, MD, PhD, Ching-Chu Lu, MD, Fang-Chi Chang, MD, Shih-Cheng Liao, MD, Ruoh-Fang Yen, MD, PhD, Wei-Chou Lin, MD, PhD, Bor-Sen Hsieh, MD, PhD, and Kwan-Dun Wu, MD, PhD.