
Abstract
Objective
The aim of this study was to determine if differences in coronary endothelial function are observed between asymptomatic women with type 2 diabetes mellitus (DM) and control subjects using coronary phase contrast flow velocity magnetic resonance imaging in response to cold pressor stress, an established endothelium-dependent vasodilatory stress.
Methods
Phase contrast flow velocity imaging of the right coronary artery was performed in 7 asymptomatic premenopausal women with DM and 8 healthy female participants in response to the cold pressor test at 3 T.
Results
There was no significant difference in percent increase in coronary flow velocity from rest to peak flow velocity between DM and control subjects (32% ± 22% vs 46% ± 17%; P = 0.11). However, percent increase in coronary flow velocity was lower in DM than in control subjects (−3% ± 14% vs 31% ± 30%; P = 0.01) during the second minute of cold pressor stress, when endothelial-mediated vasodilation should occur.
Conclusions
Asymptomatic women with DM demonstrate reduced coronary flow velocity during the second minute of cold pressor stress, indicating coronary endothelial dysfunction.
Type 2 diabetes mellitus (DM) substantially increases the risk of cardiovascular (CV) events, particularly in women. 1 Cardiovascular risk in asymptomatic patients with DM is equivalent to that of patients without DM who have had a prior CV event.2–4 Specifically for premenopausal women, the diagnosis of DM heralds a dramatic change in CV risk, essentially eliminating the favorable sex differences observed before menopause. Of greater concern, women with DM are more likely to die following their first CV event than women or men without DM. 5 Although there is a significant need to identify women with asymptomatic CV disease prior to the first event, most noninvasive screening tests focus on plaque-based disease, such as measurements of coronary calcium, computed tomography angiography, and exercise or pharmacologic stress tests. Coronary endothelial dysfunction has been characterized in women with angina prior to the development of significant obstructive plaque, and the presence of coronary endothelial dysfunction increases the risk of CV events. 6 However, these studies diagnosed coronary endothelial dysfunction during coronary angiography, a technique that would be inappropriate for screening asymptomatic women.
Noninvasive imaging techniques for measuring coronary vascular reactivity include ultrasound and cardiac magnetic resonance (CMR) strategies. Transthoracic Doppler echocardiography has been used to measure coronary flow velocity reserve in the left anterior descending artery with good correlation to intracoronary Doppler flow. 7 Prior studies using transthoracic Doppler have demonstrated reduced coronary flow velocity reserve in asymptomatic patients with DM 8 and in patients with syndrome X. 9 However, feasibility of transthoracic Doppler is limited in patients with large body habitus and poor acoustic window. More recently, coronary vascular reactivity has been measured using quantitative myocardial perfusion CMR in response to cold pressor stress.10,11 However, this technique requires intravenous gadolinium contrast, which limits repeat measurements and is unsuitable for patients with decreased renal function.
Pharmacologically induced changes in coronary flow velocity have been measured noninvasively using phase contrast CMR at 1.5 T12–17 and validated with intracoronary Doppler. 14 Phase contrast coronary CMR is technically challenging as both high spatial and temporal resolution are required for accurate flow measurement.13,18 More recent studies have reported feasibility of coronary phase contrast CMR at 3 T, which affords higher signal-to-noise ratio that can be leveraged for increased spatial resolution.19,20 To further improve spatial and temporal resolution, k-space sampling techniques can also be utilized with less sensitivity to motion than Cartesian methods. 21 We tested a protocol using coronary phase contrast flow velocity CMR at 3 T with spiral k-space sampling to determine (1) if changes in coronary flow velocity can be measured in response to cold pressor stress, a well-established endothelium-dependent vasodilatory stress, 22 and (2) if the technique could detect significant differences in coronary flow velocity between asymptomatic women with DM and control subjects.
Methods
Study Participants
This study was approved by the University of Texas Southwestern Institutional Review Board, and all participants provided written informed consent. Seven asymptomatic premenopausal women with DM and 8 premenopausal overweight but otherwise healthy female participants were recruited. Women with DM were required to have a hemoglobin A1c below 10 within 3 months of the study. Participants were excluded if they had chest pain, a history of coronary artery disease, heart failure, hypertension, stroke, lung disease, smoking or cocaine use. Participants were excluded if they were taking oral contraceptives or any medications that would affect vascular function or if they had a contraindication to magnetic resonance imaging (MRI).
Cmr Technique
Cardiac magnetic resonance imaging was performed using a 3-T MRI scanner (Achieva; Philips, Amsterdam, The Netherlands) equipped with a maximum gradient strength of 40 mT/m and slew rate of 200 mT/m per millisecond. Images were acquired with a 6-element cardiac receiver coil with the subject in the supine position. Retrospective electrocardiographic gating was utilized. Initial scout images were acquired in 3 orthogonal planes using a balanced turbo field echo sequence. Axial balanced turbo field echo images of the heart were obtained through the proximal right coronary artery (RCA). An imaging plane was selected perpendicular to the proximal RCA at a distance 2 to 3 cm from the ostium for phase contrast imaging.
Velocity-encoded phase contrast imaging of the coronary arteries has previously been described.13,14,16 In our study, phase contrast flow velocity imaging of the proximal RCA was performed using a vectorcardiogram-triggered end-expiratory breath-hold (11–15 seconds) and spiral k-space sampling. Additional parameters included echo time of 3.5 milliseconds, repetition time of 34 milliseconds, flip angle of 20 degrees, field of view of 256 × 256 mm2, matrix size of 312 × 312, spatial resolution of 0.8 × 0.8 × 7 mm3, temporal resolution of 44 milliseconds, spiral interleaves of 11, velocity encode of 35 cm/s, and readout time of less than 40 milliseconds. In each flow imaging series, at least 14 phases of data were acquired and reconstructed into velocity maps with corresponding magnitude images.
Study Protocol and Cold Pressor Test
Three series of baseline RCA flow were obtained for each subject. Next, the cold pressor test was performed, with the subject remaining supine in the MRI scanner by immersing the subject's left hand in a magnet-compatible ice-water bath (50% ice, 50% water) for 3 minutes. 23 During the cold pressor test, 2 additional series of RCA flow were initiated after the first and second minute of cold stress. The ice-water bath was removed after 3 minutes of cold stress, and 2 additional series of recovery flow were acquired at 1 and 10 minutes poststress (Fig. 1). Peripheral blood pressure and heart rate were continuously monitored throughout the experiment at 30-second intervals using an automated brachial blood pressure cuff rated MRI compatible at 3 T. Repeated flow measurements were obtained in 12 participants to evaluate reproducibility of peak RCA flow velocity.
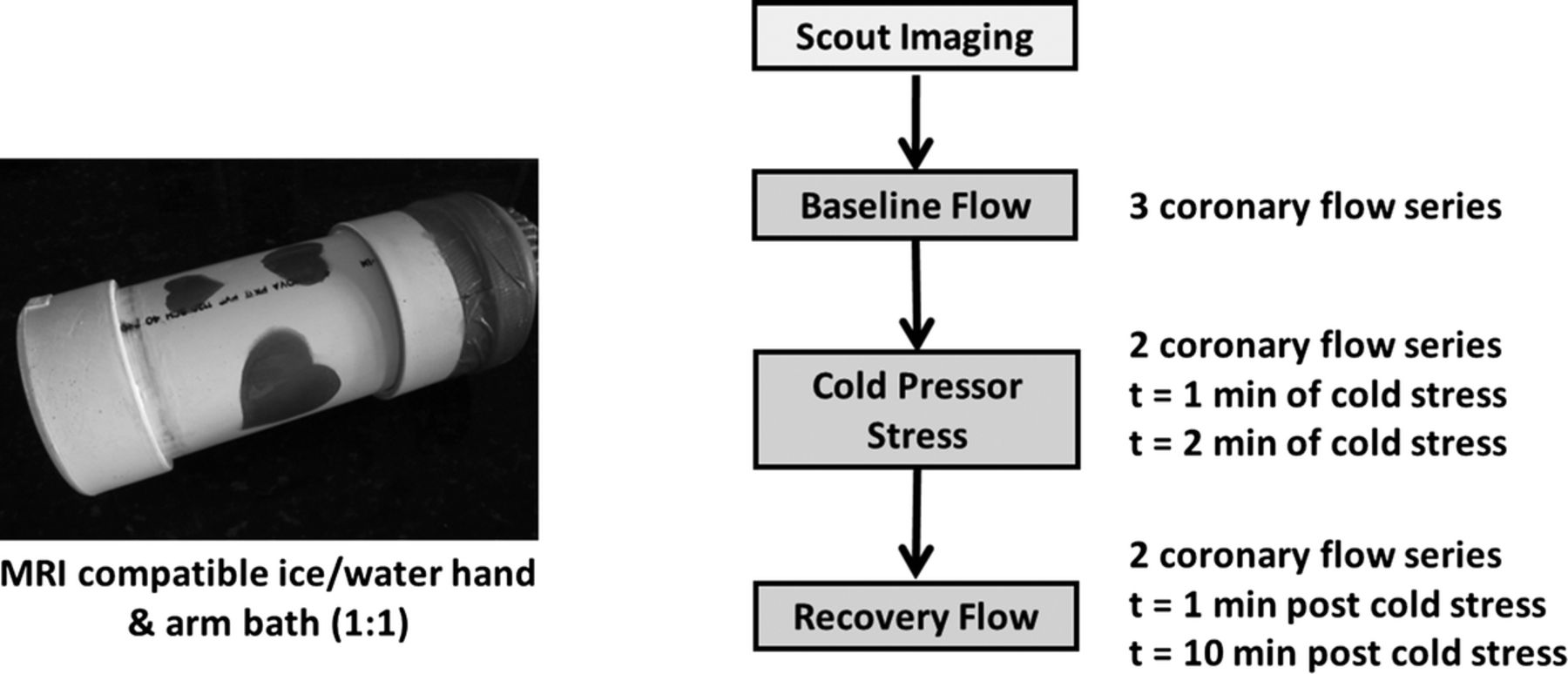
Study protocol for measurement of coronary flow velocity in response to cold pressor stress.
Image Analysis
Velocity and magnitude images were transferred to a remote workstation and analyzed using QFLOW (version 4.1.6; Medis, Leesburg, VA). Cross-sectional contours of the RCA lumen were manually traced on each magnitude image during diastole by 2 trained observers (C.D.M. and A.Y.C.) masked to study group. Identical tracings were automatically applied to the corresponding velocity maps so that peak RCA flow velocity (in centimeters per second) during diastole could be measured. 14 Images acquired during systole were not evaluated because of excessive coronary motion. 24
Calculated Variables
Mean arterial pressure (MAP) was estimated using the following formula:

Rate-pressure product was defined as the product of heart rate and MAP. Coronary flow velocity was defined as the peak RCA flow velocity measured by phase contrast imaging during diastole. The change in coronary flow velocity after cold pressor stress was calculated as percent increase in coronary flow velocity from baseline to peak coronary flow during the 2 minutes after stress 14 and by percent increase in coronary flow velocity from baseline to the first minute, and baseline to the second minute after cold pressor stress. Coronary vascular resistance was estimated by dividing MAP by peak diastolic RCA flow velocity.
Statistical Analysis
Data are expressed as mean ± SD. Measurement differences between baseline and cold stress were analyzed by means of a t test for paired data (baseline and cold stress) or independent t test between groups for the first and second minute of the cold stress. Coefficients of variability were calculated to evaluate interobserver and intraobserver reproducibility of coronary flow velocity measurements. P < 0.05 was considered to indicate statistical significance.
Results
The baseline characteristics of our study participants are presented in Table 1. Compared with control subjects, women with DM had higher body mass index (P = 0.03), greater waist circumference (P = 0.02), and greater systolic and diastolic blood pressures at rest (P = 0.02 and P = 0.03, respectively). Only 1 DM patient was on insulin, whereas the others were on oral medications. All 15 participants successfully tolerated the cold pressor test. Diastolic RCA phase contrast flow images were successfully acquired in 100% of participants at baseline and during cold stress (Fig. 2). Recovery flow images were not obtained in 1 subject because of early termination of the MRI study related to claustrophobia. Coefficients of variability for measures of peak coronary flow velocity were 5.0% for interobserver variability and 2.0% for intraobserver variability.
Baseline Characteristics of the Study Participants
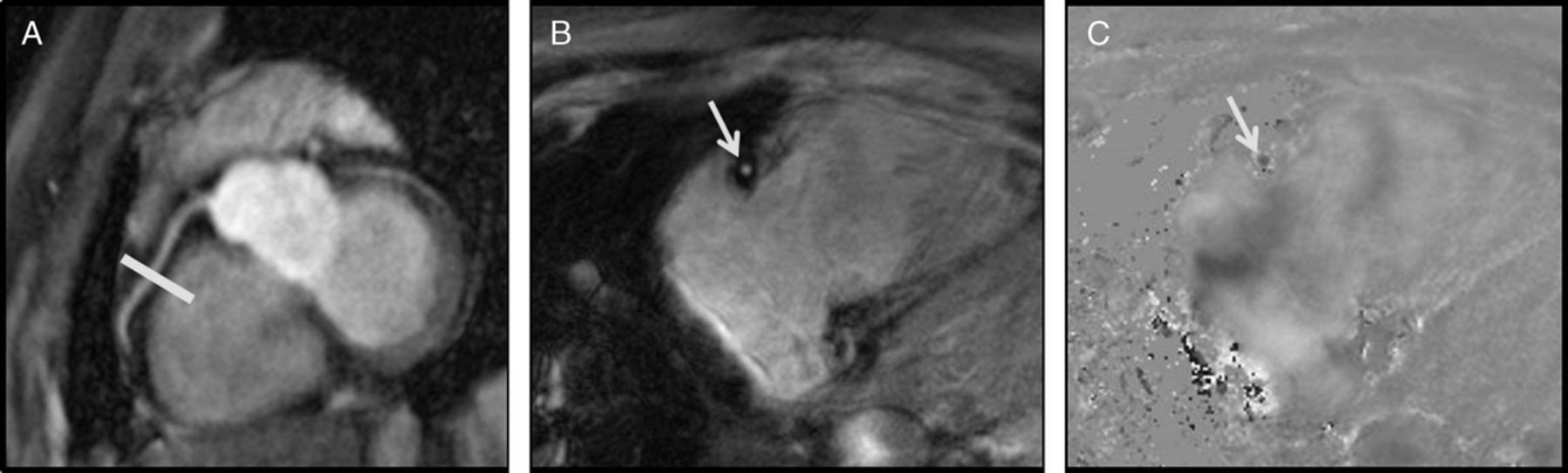
Localization and phase contrast images of the proximal RCA. Noncontrast balanced turbo field image (A) of the proximal RCA (white arrows) with selection of the imaging plane for phase contrast imaging (yellow line). Representative magnitude (B) and velocity (C) phase contrast images through the RCA at middiastole.
Changes in coronary flow velocity for women with DM and control subjects in response to cold pressor stress are also depicted in Figure 3. A significant and similar hemodynamic response to the cold pressor test was observed in both women with DM and control subjects, as represented by changes in the rate-pressure product from baseline: at 1 minute of cold pressor stress, 40% ± 26% and 46% ± 25% (P = 0.76), and at 2 minutes of cold pressor stress, 28% ± 1% and 23% ± 16% (P = 0.41). There was no difference in baseline coronary flow velocity between women with DM and control subjects (DM, 18.5 ± 6.6 cm/s, vs control subjects, 16.9 ± 6.4 cm/s; P = 0.65) or in peak percent increase in coronary flow velocity (DM, 32% ± 22%, vs control subjects, 46% ± 17%; P = 0.11). However, when comparing changes in coronary flow velocity specifically during the second minute of cold stress, a significant difference was observed between women with DM and control subjects (−3% ± 14% vs 31% ± 30%; P = 0.01) (Fig. 4). Upon further review, differences in coronary flow velocity at the second minute of cold stress correlated with changes in coronary vascular resistance between women with DM and control subjects (18% ± 25% vs −9% ± 16%; P = 0.02), not MAP (Fig. 4).
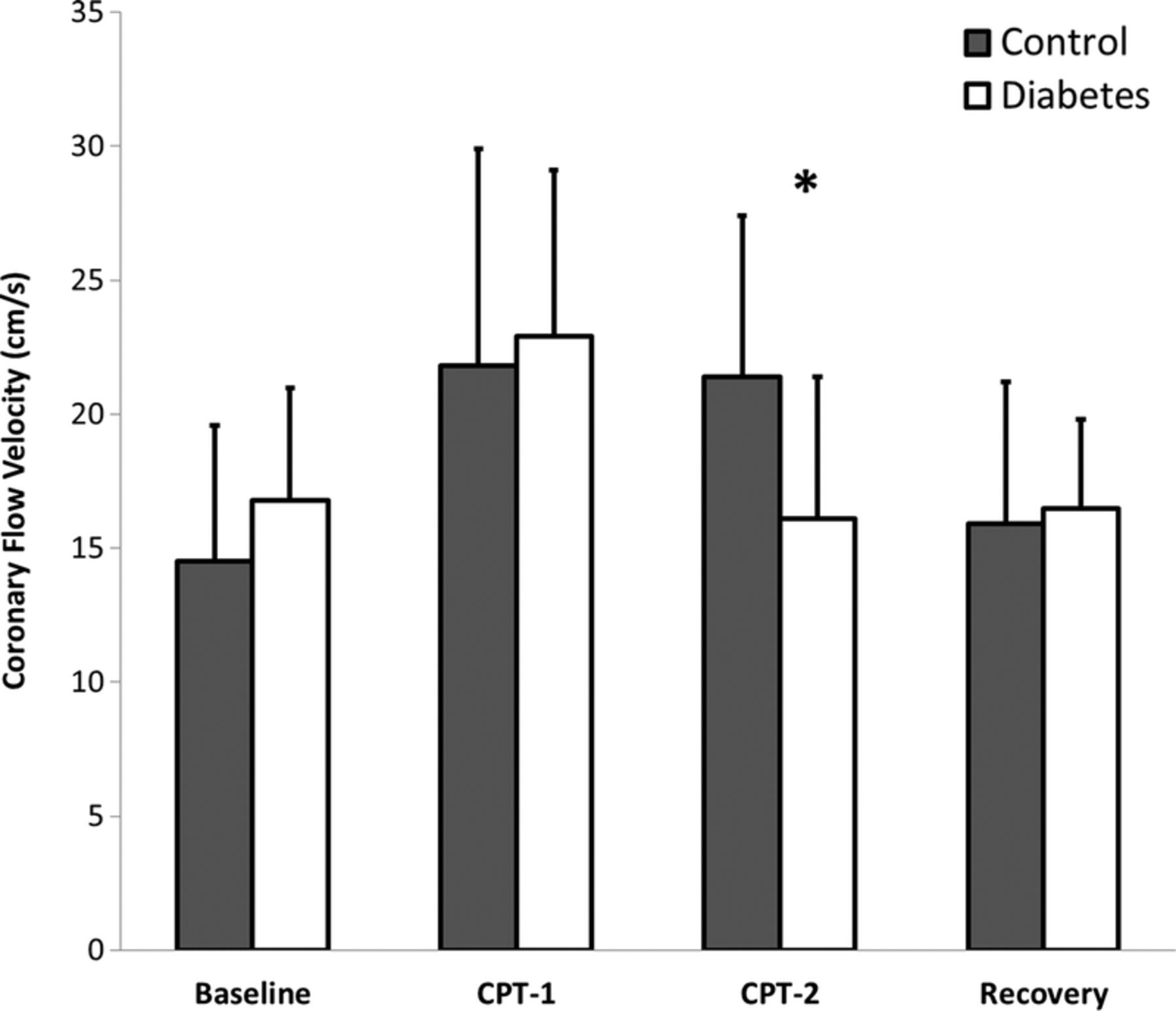
Changes in peak coronary flow velocity in response to the cold pressor test. *P < 0.05. Error bars indicate the 95% confidence interval. CPT-1 indicates first minute of cold pressor stress; CPT-2, second minute of cold pressor stress.
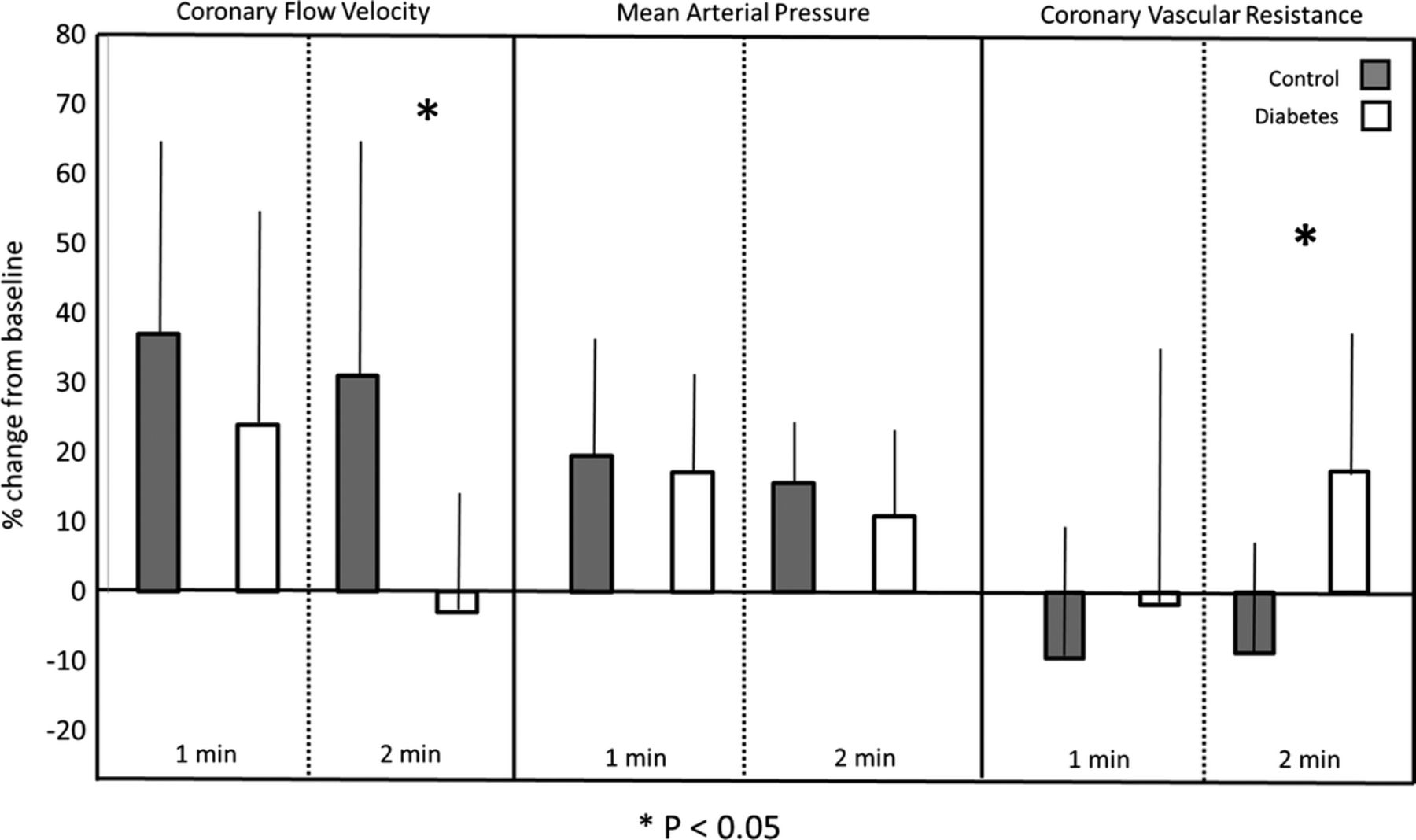
Impaired coronary flow velocity in women with DM after cold stress corresponds with increased coronary vascular resistance. *P < 0.05. Error bars indicate the 95% confidence interval.
Discussion
To our knowledge, this is the first study demonstrating the feasibility of coronary phase contrast flow velocity CMR at 3 T for measuring changes in coronary flow velocity during the cold pressor test. Cold pressor stress induced similar peak increases in coronary flow velocity in women with DM and control subjects. However, women with DM demonstrated reduced flow velocity during the second minute of the cold pressor stress when endothelial-mediated vasodilation should occur. Thus, asymptomatic women with DM have evidence of coronary endothelial dysfunction measurable using a noninvasive CMR technique without the use of intravenous contrast or pharmacologic stress.
Previous studies have shown evidence for impaired myocardial flow reserve and coronary flow velocity reserve in DM. For example, Yokoyama et al. 25 used 13N-ammonia positron emission tomography (PET) to demonstrate reduced myocardial flow reserve in response to pharmacologic stress among 25 asymptomatic, normotensive patients with DM compared with 12 control subjects. QuPrior et al. 26 also used 13N-ammonia PET to show reduced myocardial flow reserve in response to endothelium-dependent cold pressor stress among patients with insulin resistance and DM compared with insulin-sensitive control subjects. These data are concordant with our observation of attenuated endothelium-dependent coronary flow velocity in asymptomatic women with DM at the second minute of cold stress, which corresponds to the interval of maximum stimulated sympathetic nerve activity and endothelial-dependent pressor response. 27 While PET is considered the criterion standard for quantification of absolute myocardial blood flow, this technique is limited by the injection of radiopharmaceuticals and exposure to ionizing radiation, making it a less suitable technique for screening asymptomatic patients. Using transthoracic Doppler echocardiography, Kawata et al. 8 further demonstrated reduced coronary flow velocity reserve in response to adenosine stress among a cohort of asymptomatic patients with DM compared with control subjects. Although the phase-contrast CMR technique has been validated against intracoronary Doppler flow with good correlation, 7 the feasibility of transthoracic coronary Doppler flow is limited in some patients with large body habitus and poor acoustic windows. However, both the interobserver variability and intraobserver variability of transthoracic coronary Doppler flow are similar to those reported in our study using phase contrast coronary CMR.
Phase contrast coronary imaging can be performed during breath hold or by using a respiratory gating technique.13,15 However, both techniques are subject to error from through-plane motion of the coronary artery throughout the cardiac cycle. While prior studies have described strategies for correcting phase contrast coronary flow velocities to account for through-plane vessel motion, 28 these strategies were not applied in our study. Rather, we selected peak coronary flow velocity measurements during end-diastole, during which time the RCA motion is minimal. This reporting method is similar to that used for intracoronary Doppler flow measurement. 29 Furthermore, a 3-dimensional spiral k-space acquisition technique was utilized in our study to improve motion sensitivity. 30 Utilizing a spiral readout technique, we were able to achieve readout times (<40 milliseconds) much shorter than the average diastolic rest period, typically around 80 to 100 milliseconds. A readout time shorter than this can be achieved only by using a spiral technique. In spiral k-space acquisitions, the center of k-space is oversampled, thereby allowing for phase correction between lines of acquired data. Bornert et al. 31 previously demonstrated that 3-T coronary magnetic resonance angiography with a spiral acquisition technique yielded higher signal-to-noise ratio and less motion when compared with Cartesian schemes. Importantly, our measurement of peak diastolic coronary flow velocity demonstrated a consistent measurable increase in response to cold pressor stress with measurement reproducibility at baseline and after stress. Although as a group, women with DM had a significantly decreased percent change in coronary flow velocity in the second minute, there is enough interindividual variability to suggest this technique may potentially differentiate those at lower and higher risks (Fig. 3).
Limitations
Although we did not independently validate our phase contrast technique against the criterion standard technique of intracoronary Doppler flow, prior studies have reported significant agreement between coronary phase contrast flow velocity imaging with intracoronary Doppler flow 14 and phantom flow models.19,20 In addition, the plane chosen for through-plane phase contrast velocity mapping of the RCA was determined using a single localization view of the RCA. Because the RCA was not interrogated in multiple planes, the velocity mapping imaging plane may not have been optimally perpendicular to flow, thus contributing to measurement variability. In future studies, the optimal location for phase contrast imaging of the RCA can be determined by empirically quantifying periods of low motion to improve measurement reproducibility. 32 Because we could not reliably detect small cross-sectional area changes of the RCA in response to cold pressor stress because of limitations in spatial resolution, we could not confirm whether changes in peak coronary flow velocity were primarily attributable to a lack of vasodilation or an increase in microvascular resistance. In future studies, coronary flow velocity imaging could be performed along with high-resolution vessel wall imaging at baseline and during peak stress to assess cross-sectional area changes. 33 Finally, in this pilot study, we did not match on body size, blood pressure, or age. These factors may impact resting coronary flow velocity and cardiac preload and thereby impact coronary flow reserve. However, the objective of this study was to prove the feasibility of detecting differences in coronary flow velocity between groups using MRI. Therefore, we tried to compare 2 groups anticipated to demonstrate a difference in coronary flow velocity to cold pressor stress. As such, larger studies with matched baseline characteristics are necessary to establish the full utility and prognostic value of coronary phase contrast flow velocity imaging among asymptomatic women with DM.
Conclusions
In conclusion, our results demonstrate the feasibility of coronary phase contrast flow velocity CMR at 3 T to detect changes in coronary flow velocity in response to the cold pressor test in control subjects and asymptomatic women with DM. Women with DM demonstrate reduced flow velocity during the second minute of cold pressor stress, the interval when maximum endothelial-mediated vasodilation should occur. Thus, asymptomatic women with DM have evidence of coronary endothelial dysfunction measurable using a noninvasive imaging technique without the use of intravenous contrast, ionizing radiation, or pharmacologic stress.
Footnotes
Acknowledgments
The authors thank Drs. Ivan Dimitrov and Andrew Kontak for assistance with design and testing of the CMR protocol.