
Abstract
Purpose
To present a case study with Epidermolysis bullosa (EB) in Cyprus and to determine the nursing care plan, explaining the nursing interventions and showing the importance of nursing care of patients with EB.
Methods
Literature review on EB and semi-structured interviews commenced through a direct discussion with open-ended questions to the research subject as well as to a close relative describing his feelings, experiences, and concerns about the disease.
Findings
Thematic analysis approach was used to identify and analyze patterns in the data. Then, data were synthesized using the standardized nursing terminology of NANDA-I and the Nursing Interventions Classification. The accuracy of the diagnoses and the appropriateness of the nursing interventions were supported by the positive health outcomes of the patient.
Conclusions
Nurses should apply evidence-based practice interventions for EB wound care, pain management, nutrition, psychological and social support to these patients.
Implications for nursing practice
Although EB is classified in the category of rare diseases, the presentation of a case study in Cyprus and the nursing care plan contribute further bibliographically to the holistic and at the same time individualized nursing practice.
INTRODUCTION
Epidermolysis bullosa (EB), also called “Butterfly Skin,” is a hereditary group of rare skin diseases, transmitted in an autosomal dominant or recessive way of low prevalence, belonging to the group of genodermatoses (skin diseases of genetic origin). The main features are the fragility of the skin and the formation of blisters on it (blistering epidermolysis) after minor mechanical injury as well as varying degrees of damage to the mucous membranes of the internal organs (Jackson et al., 2017). The first description and use of the term disease was in 1886 by Köbner. Regarding the terminology of blistering epidermolysis, modern science attributes to the disease the term “skin-onion,” which includes its histological description and the specific mutations found in patients. This disease, regardless of sex and ethnicity, is chronic and currently incurable (Has et al., 2020).
It is estimated that one in 227 has a defective gene that could cause EB. In addition, one newborn in 17,000 live births is born with some form of blistering epidermolysis. It is estimated that the total individuals suffering from this rare disease in Europe amounts to 30,000, while worldwide to 500,000 (Debra International, 2020).
EB shows great clinical heterogeneity and different ways of heredity. The spectrum of EB extends to more than 30 clinical subtypes with pathogenic mutations in at least 18 different genes (McGrath, 2015; Reimer et al., 2018). EB is classified into four main categories: (a) simple EB (simplex EB–EBS), (b) junctional EB–JEB, (c) dystrophic EB–DEB, which includes the recessive dystrophic EB–RDEB, and (d) mixed EB. EB is characterized by blisters, skin erosions, affected mucosa, and mechanical fragility where after a minimal injury painful open wounds are formed, the epithelial lining of the organs is affected in more severe cases (Abercrombie et al., 2008; Fine, 2010), and complications include secondary infection and extensive scarring (Lynne et al., 2018).
In the case of recessive dystrophic EB (RDEB), which we will study in the present study, less than 100 cases have been reported to date, as it is probably underreported (Pfendner & Lucky, 2018). The onset of action usually occurs at or shortly after birth with the signs and symptoms of RDEB varying widely among patients. In mild cases, blistering may primarily affect the hands, feet, knees, and elbows, but in severe cases of this condition widespread blistering can lead to hearing loss, corneal erosions, anemia, esophageal stricture, and squamous cell carcinomas, with cumulative risk reaching 23% by age 50 (Gannon, 2004; Pfendner & Lucky, 2018). The most important problems of patients with EB is pain, pruritus, difficulty of participation in various activities, the lack of perception by others, feeling different from others, and their lack of autonomy (Bodán, 2020; Brun et al., 2017; Lynne et al., 2018; Papanikolaou et al., 2021; Schräder et al., 2018). For the patients who have been affected by a more serious form, wound care is often a long, endless, and painful process (Bodán, 2016).
It is very important to note that for EB patients, in addition to the predictable mechanisms of injury, even simple daily procedures can cause pain and injury. These functions include eating (e.g., painful mouth blisters), bathing, walking (e.g., EB-related neuropathic pain of the feet skin erosions), time spent with friends and family (e.g., being held improperly can cause significant skin erosions, emotional impact of not being able to keep up with peers), and sleeping (e.g., wounds adhering to clothing or sheets, pain to open the eyes) (Bodán, 2020; Grocott et al., 2013). Moreover, the consequences of chronic injuries, pain, and discomfort could lead to various consequences such as symptoms of anxiety and depression, behavioral changes, difficulties with self-regulation, attention and academic difficulties, nightmares, sleeping and eating difficulty, as well as drug and alcohol use (Kearney et al., 2020; Williams et al., 2011).
Equally important as mentioned above is that EB does not only affect the patient, but it also has an impact on families on a psychological, social, economic, and physical level. The family plays an important role in providing care for children, not just in terms of daily basis activities, but also in psychological support (Fine et al., 2005). The more serious the disease and the more the blisters spread on the body of children, the greater the burden on the family. In addition, the family is even more burdened when the members who take care of the patient are more emotionally involved (Wu et al., 2020).
The main aim of this study was to present a case study of RDEB in Cyprus and to determine the nursing care plan of the patient with EB, explaining the nursing interventions and showing the importance of nursing care of patients with EB.
METHODS
The current research is a case study. Using NANDA-I classification and the Nursing Interventions Classification, we selected nursing diagnoses and evidence based nursing interventions for a clinical case with RDEB in Cyprus. (Brito-Brito et al., 2016; Pena et al., 2013)
Sampling: Participant profile
The selection of the target sample was done by deliberate sampling. The sample consist of a patient from Cyprus, as he is one of the four alive adult patients with EB in Cyprus.
Ethics
Participant gave informed written and verbal consent prior to participating in the interview. During the process, the researcher took notes, photos, and at the same time recorded the interview after obtaining the consent of the participant. The researcher had informed him that he could stop at any time. He was also informed that the anonymity and protection of his personal data would be ensured.
Data collection
Five meetings of 1 h each were held at the patient's house in an appropriate and intimate environment, without disturbances for the discussion. Semi-structured interviews commenced through a direct discussion with open-ended questions to the research subject as well as to a close relative describing the subject's feelings, experiences, and concerns with the disease. Interviews were audio-recorded to ensure the accuracy of the verbal response while capturing the emotional impact of patient responses. Demographic information and a genealogical tree were also collected.
Data analysis
Thematic analysis approach was used to identify and analyze patterns in the data, often utilized in qualitative research and used when little is known about the subject. This approach enables the development of knowledge to be guided by the participants’ data rather than any predetermined constructs (Kearney et al., 2020). In the current study, data analysis was the basis for nursing assessment and detection of the patient's nursing needs following the nursing process. A nursing care plan (NCP) is the process that correctly identifies existing needs and recognizes potential needs or risks. Care plans provide communication among nurses, their patients, and other healthcare providers to achieve health care outcomes (Herdman & Kamitsuru, 2017; NANDA-I, 2014). With the nursing care planning process, the quality and consistency of patient care is ensured, from holistic and individual care plan to standardized care plans for patients with EB.
RESULTS
To the best of our knowledge, the present clinical case was the first recorded incident of EB in Cyprus. Doctors were not able, due to lack of appropriate laboratories test and specialization on the subject, to make a diagnosis (Verroiou et al., 2018). There were indications that the child's illness was potentially fatal. From his birth, which took place as a normal birth in the 39th week of pregnancy, the mother had noticed that the baby had something in his neck. The newborn developed jaundice, so he remained in the incubator for phototherapy. In the first week, one night she saw him crying, with the diaper open and full of blisters all over his body, except for the genitals, buttocks, and head. The pediatricians informed her that he probably had a disease called “pemphigus” and that babies rarely survive. After some years and in order to confirm the diagnosis, a skin biopsy and a mutation analysis were performed resulting in the diagnosis of RDEB. However, there are no other cases in the family, according to the patient's genealogical tree, which is presented in Figure 1.
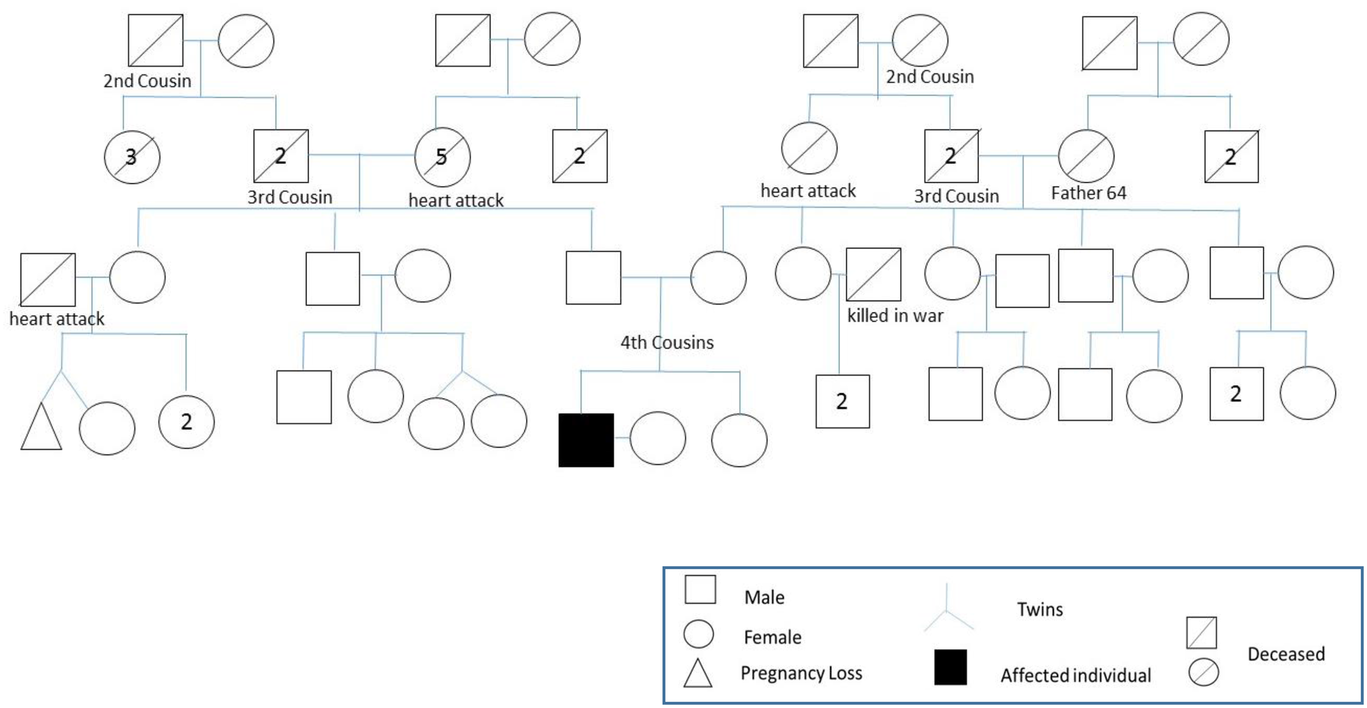
Epidermolysis bullosa patient's genealogical tree
Around middle-aged now our patient presents physical, psychological, and social needs and therefore his approach must be interdisciplinary and individualized. Nursing assessment is the first stage of the nursing process and is based on subjective, objective data, but also on what the patient says and is the way to detect the patient's needs. It determines the nursing diagnoses and the nursing care plan and sets the priorities to nursing interventions for an optimized personalized patient care (Flanagan, 2021).
After comprehensive nursing assessment, the needs of the patient with EB were grouped into four basic Nursing diagnoses identified by Nursing researchers: (1) deterioration of skin integrity, (2) acute pain, (3) imbalanced nutrition: less than body requirements, and (4) disturbed body image (Herdman & Kamitsuru, 2017; NANDA-I, 2014)
Nursing diagnosis 1: (Domain 11. Security/protection. Class 2. Injury physical)
Deterioration of skin integrity, related to external factors (humidity, pressure, mechanical factors, etc.) and internal factors (alteration in hydration, in the flexibility of the skin, etc.) as evidenced by alteration of the skin surface. His current condition is reflected in the following indicative figures (Figures 2, 3, 4) and in the patient's words about the condition of the wounds:

Patient's hands with Epidermolysis bullosa
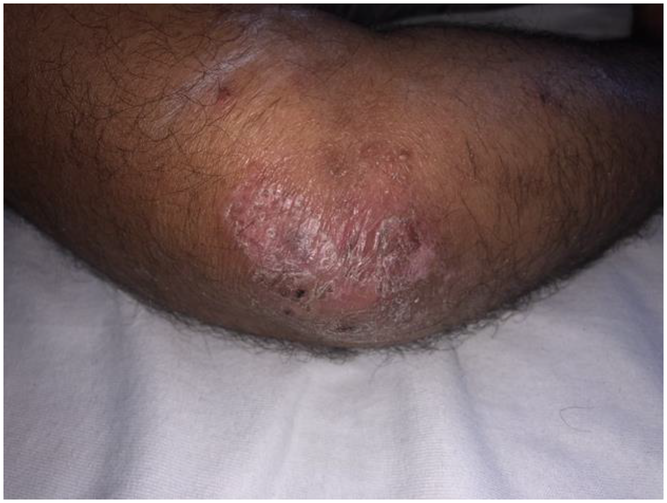
Patient's elbow with Epidermolysis bullosa

Patient's knees with Epidermolysis bullosa
Depending on the part of the body, there is the corresponding wound. For example, on the knees, ankles, wrists, ankles the skin is very thin and fragile, so it is easier for blisters to form, while in other parts of the body it must be preceded by rubbing or hitting to create them, as the skin has better appearance and composition (patient). I feel discomfort and pain when I hit a part of my body, or when there is pressure from a hard object (such as shoes), or when I press a part of my body on a hard surface (patient) Depending on the point and the size, there is a corresponding healing time. “About 1–2 weeks” (patient). Baths in the sea is a relief as the sea helps to heal wounds faster, relieve itching, and harden the skin. (patient)
Also, his mother recalls the situation she experienced with the patient when he was child: “The skin was so sensitive, since after the bath, when the child was placed on the towel, his skin came off.” (patient's mother)
Nursing diagnosis 2: (Domain 12. Comfort. Class 1. Physical comfort)
Acute pain related to skin shedding, injuries, destruction of skin/tissues as evidenced by facial expressions of pain, narrowed focus, alteration in muscle tone, and reports of pain: “There is pain in the wounds, bleeding or bloody fluid, many times there is itching and after itching, wounds form.” “I learned to live with pain.” (patient)
Nursing diagnosis 3: (Domain 2. Nutrition. Class 1. Ingestion)
Imbalanced nutrition: Less than body requirements related to hypermetabolic state (can be as much as 50%–60% higher than normal proportional to the severity of injury), protein catabolism, anorexia, and restricted oral intake as evidenced by decrease in total body weight, loss of muscle mass/subcutaneous fat. The disease affected the child's development, and he lost his height, since at the age of four, he was as tall as two years old. (patient's mother)
Nursing diagnosis 4: (Domain 6. Self-perception. Class 3. Image bodily).
Body image disorder related to skin lesions, disfigurement and pain as evidenced by negative feelings about his body/self, fear of rejection/reaction by others, reduced social interaction, reduced ability to take on a role and memories by himself and his mother: ‘I remember there were people who did not want to come in contact with me because there was a fear that it was a contagious disease. (patient) When he became an adult and had to accomplish his military service, he was rejected due to incompetence, something that stigmatized him. (patient's mother) Another unpleasant memory was when he was planning to get engaged to a woman at the age of twenty-five and her parents not only objected, but were also clear that the cause was his disease and that he could inherit to their grandchildren. (patient's mother)
After many years, the patient had the courage to dream and make the decision to get married. However, he is totally pessimistic about having children. In his opinion, he has gone through a difficult life and his mother even more, to want to get into this process. In the past, I felt comfortable talking only to doctors and very close friends. After my wife's long-term support and encouragement, I am more open to talking to strangers. (patient)
DISCUSSION
The role of nursing in a chronic, unstable condition, such as EB, requires focus on the prevention of deterioration. Nursing goals should be realistic and desired as both clinically and personally significant by the people affected. The nursing approach to EB plays a fundamental role, not only in wound care but also in providing all the information that these families need about the care that patients require (Grocott et al., 2013). The patient participates in the design of the nursing care plan and the goals, and the time frame of their implementation are determined according to the nursing process (Abercrombie et al., 2008). Moreover, according to synergy model concept, it is also important to match the needs of the patient with a specific nurse who could provide comprehensive care helping the patient and the family to establish trust and decrease their level of anxiety (Packard, 2011). Therefore, it is appropriate to have a care plan regarding the most frequent diagnoses and complications in these patients.
Wound care in EB
Adult patients with RDEB usually have both chronic and acute wounds and often self-manage, whether they cover their own wounds or are supported by a caregiver who leaves the decisions to them. In order to make a concordance with the patient, it is essential to discuss with him the current wound management, and carefully explain the rationale of any proposed new therapy (Abercrombie et al., 2008).The Nursing Interventions for surveillance of the skin and wound care according to NANDA-I Nursing Interventions Classification (NIC) (Herdman & Kamitsuru, 2017), include: Local wound evaluation: In order to properly evaluate the wound, it is necessary to implement special wound care programs which include the evaluation of the size of the affected area, the exudate, its appearance, undermining, and its reassessment. These data are important for monitoring the skin response to a particular treatment (Pope et al., 2012). Wet the skin with saline solution or water, minimizing pain and the appearance of new lesions. Water dries the skin that could become more irritated and itchy. The use of bath emollients and moisturizers on intact skin may help (Abercrombie et al., 2008). It is important to explain to the patient and their caregivers that bathing should preferably be done by immersion and avoiding friction when washing and drying. According to Shayegan et al (2020) the most common method of skin cleansing is bathing and the most frequently topical products are antimicrobial products, such as Mupirocin. Some patients choose to dress all their wounds on a daily basis, while others may find this a very time consuming and painful. These patients may prefer to bandage only one or two wounds each day. The decision to change the dressings will also be affected by the type of bandage used, the stage of wound healing, and whether there is an infection or pain. Wounds are treated as “clean wounds” unless they are surgical, in which case a sterile dressing procedure is required (Abercrombie et al., 2008). As long as there is no infection, clean the wounds in this order: the area of the back and buttocks, followed by the head, thorax and abdomen until finishing with the extremities minimizing the painful dressing removal (Denyer, 2011) Aspiration of blisters with a hypodermic needle parallel to the skin is mandatory when they appear and always clean the wound with saline solution, avoiding friction, and if signs of infection are observed, apply topical antibiotic cream, as prescribed. After covering the injury with the dressing that best suits patients’ needs, moisture is needed for the rest of the skin, to minimize discomfort and provide greater flexibility. At the end, perform the cure in a place with a suitable temperature and lighting and with the highest possible aseptic conditions. Regarding topical therapeutic approaches, gentamicin administration to the skin has been shown to increase collagen VII synthesis (Woodley et al., 2017). An oral anti-inflammatory treatment showed better effect on the severity of the itching and the fragility of the skin rather than the antimicrobial mechanism of erythromycin (Chiaverini et al., 2015). The protein thymosin b4 peptide (Goldstein & Kleinman, 2015) and Vitamin D3 Supplement (Guttmann-Gruber et al., 2018) have been used successfully to facilitate tissue repair and chronic inflammation respectively.
Pain management in EB
Pain management is a multifactorial issue, as dealing with it can improve many other parameters, such as stress, fear, sleep, self-perception, and quality of life. The primary factor is the timely and correct assessment of the pain intensity and then the appropriate medication administration. Multiple research on the management of pain in patients with EB and guidelines have been developed for the management of acute and chronic pain, as well as for pain during bathing and changes in dressings depending on the age and EB subtype of the patient (Brun et al., 2017; Fine et al., 2004).
Pain in EB comprises of both neuropathic and nonneuropathic qualities (Schräder et al., 2018) and may come from the wound (fear of the dressing change, infection, type of dressing used, and the dressing technique) or from other symptoms such as oral ulcerations and erosions, esophageal blistering, osteoporosis, and corneal erosions and ulceration (DEBRA International, 2020; Denyer, 2011). This pain is described usually as “burning,” “pricking,” “electric shocks,” “tingling,” “numbness,” and “itching” and most of the patients declare waking at night because of the pain (Brun et al., 2017; Papanikolaou et al., 2021).
Nursing Interventions and some of the key recommendations for managing pain in patient with EB include: The assessment of the reports of pain, noting location, character, and intensity (0–10 scale), as well as the factors that alleviate and exacerbate it and the implementation of an objective structured clinical examination focusing on pain assessment and management in patients with EB is essential for the appropriate pain care. (Barreveld et al., 2021). A Pain Quality Assessment scale specifically for EB has been created (Schräder et al., 2018) Ensuring that the patient receives immediate pain relief before changing the dressings or other activities that induce pain. Obtaining a calm environment, informing about the type of intervention and duration, and supporting the patient's confidence about the nurse's skills are important, so as to allow the patient to control the procedure, with rest periods when needed. The room should also be warm as the body temperature drops with dressing changing something that enhances pain and discomfort, but also slows healing (Abercrombie et al., 2008). Administration of the necessary analgesia, according to medical prescription. NSAIDs and acetaminophen are often recommended for the treatment of both acute and chronic pain, although both tramadol and opioids may be used when indicated. Opioids can also be used directly on the open wound by mixing morphine sulphate with a hydrogel (Mateus et al., 2019). Gabapentin or amitriptyline is useful for neuropathic pain. Local anesthetics can be used for blood draws, intravenous access, and skin biopsies. Cannabinoids for chronic pain in people with mucosal epidermolysis are still being delineated (Schräder et al., 2021). Beyond pharmacological approaches, other nonpharmacological methods could contribute to a clinically significant analgesia such as relaxation training, biofeedback, distraction (getting the patient to watch a video, DVD, or listen to music during the dressing change), and breathing techniques. Cognitive behavioral therapy (CBT) has also proven to be very effective in managing chronic and acute pain, which helps patients manage their problems by changing the way they think and behave (Abercrombie et al., 2008; Asimakopoulou et al., 2018).
Nutrition management in EB
Unbalanced nutrition: Less than body requirements is one of the most frequent nursing diagnoses in RDEB due to chronic inflammation, secondary infection, and systemic involvement, and impacts on wound healing (Manjunath et al., 2021; Salera et al., 2020). Depending on the severity of the disease, there is a corresponding nutritional deficit, so a more serious condition is in the RDEB and JEB subtypes (Zidorio et al., 2019).
The aims of nursing interventions in nutritional support in patients with EB mainly include improving nutritional status, alleviating the stress of oral feeding, and minimizing nutritional deficiencies, thus improving growth, bowel function, immune status, and wound healing (Salera et al., 2020). Before the interventions, a comprehensive clinical assessment of patient's nutritional status is necessary including the measurement of height, weight, and BMI and the examination of the mouth for mucosal bleeding, erosions, and dental caries. The laboratory examination for anemia and vitamin deficiency is also essential. The early identification of patients with existing or those at risk of developing malnutrition with clinical indicators, plays an important role in the prognosis of the disease (Manjunath et al., 2021; Teixeira et al., 2015). Small and frequent meals prevent gastric distension or discomfort and may enhance intake. Many EB patients develop oral blistering and contracted scar tissue that makes dental hygiene difficult and often leads to decay. A soft or puree diet is often enhanced with liquid nutritional supplements. Moreover, oral hygiene before meals enhances taste and helps promote a good appetite. Educate patients to view diet as a treatment and to make high-calorie, high-protein foods as needed to maintain weight, meet metabolic needs, and promote wound healing (Teixeira et al., 2015). Socialization at meals also promotes relaxation and may enhance intake. A diet high in calories or protein with elements and vitamin supplements is recommended. Calories (3000–5000 per day), proteins, and vitamins are needed to meet increased metabolic needs, maintain weight, and encourage tissue regeneration (Zidorio et al., 2019). Dairy products are a good source of protein, calcium, and vitamin D and Vitamin C enhances collagen synthesis and promotes wound healing. Zinc, selenium, and carnitine are essential in many biochemical pathways in wound healing and cardiac physiology and iron as oral, intramuscular, or intravenous form corrects anemia with iron deficiency (Bruckner et al., 2011). Sometimes, a nasogastric tube is needed for complementary feeding and increased caloric intake (Abercrombie et al., 2008). Finally, the interdisciplinary approach to the problem requires the support of a dietitian or nutrition support team, useful in establishing individual nutritional needs (based on weight and body surface area of injury) and identifying appropriate routes (Teixeira et al., 2015).
Body image management in EB
The term “body image” refers to the individual's experience of embodiment, personal perceptions, and self-attitudes toward one's appearance. In addition, the two most central dimensions of body image are indicated by the evaluation of body image—satisfaction or dissatisfaction—and the investment in body image—the importance of its appearance in the sense of self-esteem (Asimakopoulou et al., 2019).
In case of suspected body image disorder, the nurse should identify the nature of the threat to the patient's body image (functional significance of the site involved, importance of physical appearance, and visibility of the site involved), the meaning the patient gives to the threat, the adequacy of the patient's coping skills, the reaction of family members and the help available to the patient and his family. As children with EB grow into adolescence, they have also another issue, to deal with other teenagers and often look for ways to become independent of their family. Many EB patients have managed to live a full life and with the right family and professional support they can go to university, travel, and live independently in their own accommodation (DEBRA International, 2020; Fine et al., 2005; Williams et al., 2011; Wu et al., 2020). The psychological well-being and a positive body image of the patient with EB should always be a part of a holistic nursing assessment and intervention. A relationship of trust and the effective communication (verbal as well as nonverbal) allows patients to verbalize feelings regarding their skin condition. Through talking, the patient can be guided to separate physical appearance from feelings of personal worth (Williams et al., 2011; Wu et al., 2020). Questions and affirmations encourage the expression of thoughts, feelings, and concerns in order to decrease the emotional response. It is recommended that the patient get involved in the care to the extent that he is competent because this enhance the patient's ability to make decisions and control his life (Packard, 2011). Moreover, the reaction of persons and family members who are important to the patient should be evaluated and all possible sources and personal strengths must be identified and strengthened (Fine et al., 2005). Nursing interventions also include the patient assistance to identify ways to enhance his appearance and encouragement to increase his recreational activities and social interactions, explaining the benefits that they could bring. At the end, nurse should refer to a psychologist, psychiatrist, and/or social assistance specialists, if required.
CONCLUSION
EB is a difficult and painful condition, thus it is very satisfying when these patients benefit from the highest standards of nursing care. Wound management of these patients is a challenge, due to the risk of infections and fluid loss. Skin intolerance and insufficient reepithelialization of wounds can lead to the development of chronic inflammation. Pain became part of everyday life as the patient said: “I learned to live with pain.” In recent years, there has been a change in the approach to pain in Nursing, from pain as a symptom to the person experiencing the pain as a whole. Nurses focus on what the patient himself defines as pain and what for him would be a relief of his pain. The multidimensional form and the individualized experience of pain has formed a multifaceted nursing role.
The training of family members and caregivers is essential for the proper care of painful blisters and sores. In addition, training is needed in the application of various techniques for simple tasks like changing clothes. The process of dressing is a painful and difficult process, as special care is needed in order for the patient to feel the least possible pain and to not bleed from the wounds or form new blisters. Therefore, trainings or special seminars could be held in the hospitals for the medical staff, but also for parents and carers, for the best possible wound and pain management of the patients with EB and the application of techniques concerning daily activities, such as bathing, changing clothes, treating painful wounds, and so on.
Furthermore, the interdisciplinary care in collaboration with different healthcare professionals for nutritional, psychological, and social support, not only for patients, but also for family members and carers is necessary . Direct and frequent contact with specialized scientific staff for psychological support, who are aware of this disease, can alleviate the emotional burden of patients and their caregivers and improve their quality of life. Holistic and at the same time individualized, compassionate nursing care and evidence-based clinical practice are essential for patients with EB daily needs, which affect not only the patients themselves, but also family members and carers.
In Cyprus, there is a nonprofit organization for Rare Disorders, in which the patient in the present study, was the first registered patient with EB. This organization provides information, support, and education to people with rare diseases. However, it would be also helpful if a single file including all patients with EB and a diagnostic management of EB could be developed. This would help healthcare professionals coming into contact with more and new cases and types of the disease and gaining more knowledge and experience both in caring and management of patients with EB.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
AUTHOR CONTRIBUTIONS
Study design: Alexandros Argyriadis, Evanthia Asimakopoulou, Athina Patelarou, and Evridiki Patelarou. Data collection: Aspasia Andreou, and Alexandros Argyriadis. Data analysis: Evanthia Asimakopoulou, Athina Patelarou, Evridiki Patelarou, and Idriz Sopjani. Manuscript writing: Aspasia Andreou, Evanthia Asimakopoulou, and Idriz Sopjani.
ETHICS STATEMENT
The protocol for the research project was approved by Research Ethics & Integrity Committee of Frederick University. Participant gave informed written and verbal consent prior to participating in the interview. Data were handled with utmost confidentiality and patient information was anonymized.