
Abstract
Purpose
To investigate the nutrition-related care needs of older patients in hospitals.
Methods
A qualitative multimethod study was performed. By purposive sampling, older patients were included for observations of the nutrition process and interviews from a perioperative unit, an internal Medicine unit, and one acute geriatric care ward of an acute care hospital. Preliminary findings were discussed, validated, and further explored in two focus group discussions with interprofessional nutritional healthcare experts.
Findings
Seventeen women and five men with a mean age of 86 years participated in patient observations and interviews. Eight experts with at least 10 years of professional experience who were employed in this setting for 3 years or more participated in interviews. Three themes of nutrition-related care needs were elaborated: The need to assess and address older patients’ attitudes toward life, the need for nutrition-related education, and the need for food intake support. These care needs added to the development and validation of a new nursing diagnosis “risk for inadequate protein energy nutrition” and in consequence to develop a complex nursing intervention to optimize the nutrition of older patients.
Conclusions
It is crucial to assess and understand the patients’ attitudes toward life, which affect purposes of treatment, diet, and menu choices.
Implications for nursing practice
Implementation of assessing nutrition-related care needs of older inpatients is needed. Addressing these care needs within the Advanced Nursing Process can lead to appropriate nursing diagnoses, nursing outcomes, and interventions, which enhance person-centered care, patients’ self-care abilities, and consequently patients’ nutritional status.
Ziel
Untersuchung der ernährungsbezogenen Pflegebedürfnisse älterer Patient*innen im Krankenhaus.
Methode
Es wurde eine qualitative Multimethodenstudie durchgeführt. Mittels zielgerichteter Rekrutierung wurden ältere Patient*innen aus den Abteilungen allgemeine Chirurgie, innere Medizin und universitäre Klinik für Akutgeriatrie eines Krankenhauses für Beobachtungen des Ernährungsprozesses und Interviews einbezogen. Die vorläufigen Ergebnisse wurden in zwei Fokusgruppengesprächen mit Expert*innen aus verschiedenen Berufsgruppen diskutiert, validiert und weiter analysiert.
Ergebnisse
Siebzehn Frauen und fünf Männer mit einem Durchschnittsalter von 86 Jahren nahmen an Patient*innenbeobachtungen und -interviews teil. Es wurden drei Themen ernährungsbezogener Pflegebedürfnisse herausgearbeitet: Das Bedürfnis, die Lebenseinstellung älterer Patient*innen zu erfassen; das Bedürfnis, ernährungsbezogene Informationen zu erhalten und das Bedürfnis nach Unterstützung bei der Nahrungsaufnahme. Diese Pflegebedürfnisse unterstützten die Entwicklung und Validierung einer neuen Pflegediagnose “Risiko für inadequate Protein-Energie-Ernährung” und infolgedessen einer komplexen pflegerischen Intervention zur Optimierung der Ernährung älterer Patient*innen.
Schlussfolgerung
Es ist von entscheidender Bedeutung, die Lebenseinstellung der Patient*innen einzuschätzen und zu verstehen, da sich diese auf die Behandlungsziele, die Ernährung und die Menüwahl auswirkt.
Auswirkungen auf die Pflegepraxis
Die Erfassung der ernährungsbezogenen Pflegebedürfnisse älterer stationärer Patient*innen muss implementiert werden. Die Berücksichtigung dieser Pflegebedürfnisse im Rahmen des Advanced Nursing Process kann zu angemessenen Pflegediagnosen, Pflegeergebnissen und Interventionen führen, welche die personenzentrierte Versorgung, Selbstpflegefähigkeiten der Patient*innen und damit deren Ernährungszustand verbessern.
INTRODUCTION
The prevalence of risk of malnutrition in European older patients is around 8.5–28% of the population, with the highest rates being in the context of hospitals (Leij-Halfwerk et al., 2019). In a study including 330 hospitalized older patients, only 1% reached the recommended protein and energy intake (Rosenberger et al., 2019). The present research focuses on older patients according to the definition of the European Union of Medical Specialists (2021): This group of patients is considered to have a high degree of frailty and active multiple pathologies, requiring a holistic approach. Diseases may present differently in old age, are often difficult to diagnose, the response to treatment is often delayed, and there is frequently a need for social support. (European Union of Medical Specialists, 2021)
Specialists of geriatric Medicine further state about older people's medical needs, demands, and supply—which are high in this advanced stage of life: “The ‘needs’ are the individual's problems that will benefit from health care measures, like prevention, diagnostic procedures, treatment regimes and terminal care. The ‘demands’ are what older people request […]” (Duursma et al., 2004: 190). Older patients’ insufficient protein and energy intake have severe consequences, such as a higher risk of falls, wound infection, delirium, and a higher mortality rate (Correia et al., 2014; Volkert et al., 2019).
While most recent studies and guidelines focus on physiological and nutritional needs, such as protein, energy, or vitamins (Volkert et al., 2019), the perception of older patients in hospitals about their achieved food intake and nutritional status has rarely been assessed (Haldemann-Jenni et al., 2016; Huber, 2009). Furthermore, the severe consequences of the risk of malnutrition indicate its international relevance, while current research on this topic is heterogeneous and of low methodological quality (Gomes et al., 2019; Richards et al., 2018). In addition, there is scarce research about the specific care needs of older hospitalized patients according to their perceptions independent of their medical diagnosis or cognitive status.
BACKGROUND
A needs assessment is part of the Advanced Nursing Process, the theory guiding the present study. Its definition is: “The Advanced Nursing Process consists of defined, validated concepts. It includes assessment, nursing diagnoses, nursing interventions, and nursing outcomes that are rooted in scientifically based nursing classifications” (Müller Staub et al., 2015, p. 13). This evidence-based process in which professional nurses apply the concepts of “nursing assessment,”, “knowing the person,” and “clinical reasoning” responds to patients’ needs (Leoni-Scheiber et al., 2019).
The purpose of the Advanced Nursing Process is “an application of scientific knowledge being appropriate to the clinical patient situation” (Müller Staub et al., 2015, p. 13). The term patients’ needs might be synonymous with patients’ experiences or responses to their situation on a health-illness continuum (Herdman et al., 2021; Oter-Quintana et al., 2021).
As a major research gap, dieticians hypothesized that older patients with acute diseases might not reach the required protein and energy intake according to nutritional guidelines (Grob et al., 2018). Research was needed to explore further care needs of nutrition in older patients in hospitals.
Aim
Thus, the present study aimed to seek a deeper understanding of inpatients’ nutrition and food intake care needs by including the nutrition process within the hospital context and perspectives of older patients. This comprehensive needs analysis was performed to provide the basis to develop and validate a nursing diagnosis, deepen the understanding of the nutrition-related process, and—in consequence—develop a complex nursing intervention to optimize the nutrition of older patients.
Research question
What are the nutrition-related care needs of older patients in hospital?
METHOD
Design
A qualitative multimethod approach with inductive content analysis was applied based on social constructivism's philosophical stance, as described by Guba and Lincoln (Mayer, 2019). The care needs analysis presented here included a qualitative exploration of the nutrition processes in the context of an acute care hospital to elaborate on implicitly observed and explicitly expressed care needs. This broad problem identification was reached with various data collection and analysis types, including data triangulation from observations on hospital wards, patient interviews, and two focus group discussions. Triangulation was defined as combining two or more methods or data sources to describe one phenomenon from different perspectives (Mayer, 2019). In addition, an effective way to validate interviews and observation findings and reach broader insights from patients’ and researchers’ perceptions was achieved through focus group discussions, as stated by experts (Krueger & Casey, 2015; Mayer, 2019).
Setting and recruitment
Observations and interviews were conducted at one perioperative, internal medicine, and one acute geriatric ward of a 200-bed Swiss hospital. Food was prepared freshly in the hospital kitchen and warmed up on the ward to serve warm dishes. The hospital of the investigation was selected because of gaps suspected by a registered dietician. Three wards (one per clinic) were selected. Wards for premium insured patients were excluded because they had catering services and different nurse-to-patient ratios. Older patients were screened for eligibility and asked to participate through oral and written information from the project leader 1 day before data collection (purposive sampling). Included were patients aged 80 and over, staying in the hospital for at least 5 days, and capable of following a German-language dialogue. Excluded were patients who were terminally ill, tube-fed, or getting parenteral nutrition. As the setting was a small hospital, some patients knew the project leader in advance, while some did not. In most cases, the interviewer, a research team member, started and ended a professional relationship on the day of data collection. According to the medical diagnoses or nursing reports, patients’ relatives were asked to participate in the interview if patients were cognitively impaired. The research team consisted of a registered dietician, three Nursing Masterclass students, and three Advanced Practice Nurses. Every member of the research team signed a confidentiality agreement. Data from seven to nine patients per ward were pursued to be included to gain a rich description. Inclusion meant taking part in observations and interviews concerning the whole nutrition process—from food orders, delivery, and service to feeding support during mealtimes. Observations also included mealtime ambience and staff communication on nutrition-related care needs.
According to the definition of experts in specific social and health science research (Quatrini Carvalho Passos Guimarães et al., 2016), experts were requested to participate in focus group discussions. The purposive recruitment of experts for focus group discussions aimed to recruit individuals who dealt with patient nutrition in different ways to obtain the broadest possible view and a deeper understanding of the nutrition process in the investigated hospital. These experts knew about menu creations, services, feeding support, gastrointestinal treatments, and malnutrition treatments. Organizational recruitment took place via the hospital management, who legitimated inviting employees for focus group discussions. The project leader sent e-mail requests for participation to group leaders who participated by themselves or delegated someone from their team (e.g., gastroenterologist, dietician, and nurse). Participation was voluntary and without any consequences in case of refusal. The group's common sense was that they all cared for the older patients’ nutrition.
Data collection
According to a pilot study and based on pre-existing hospital service standards, the research team elaborated and pilot-tested observation and interview guides with three Advanced Practice Nurses and a study supervisor as suggested for interview and observation guides (Mayer, 2019). The research team conducted observations and interviews with 22 older patients from September to November 2018. Guided observations aimed to get insight into nutrition-related care needs according to nursing researchers’ viewpoints, including reading the electronic health record (nurses’ documentation) and the nutrition process in an acute care hospital. These observations occurred at patients’ bedside, on the ward aisle, and in the nurses’ report room. Observation days started at 07:30 am, entailed all three main meals, and ended after dinner (6:30 pm). This comprehensive observation allowed observing the food delivery and service process, whether patients could wash their hands before meals, whether and how feeding support took place, and whether doctors discussed nutrition topics with nurses and patients during the ward rounds. Moreover, the researchers observed the food service staff's tasks. In addition, observations included nutrition-related patients’ electronic health records to detect further patients’ needs in concordance or contradiction to patient interviews’ statements.
Patient interviews were conducted with open-ended questions to explore perceptions, experiences, and directly and indirectly expressed nutrition-related care needs. The older patients were interviewed about their appetite, perception of nutritional status, and whether their eating and drinking preferences were considered in the whole nutrition process. Interviews were voice recorded and transcribed verbatim by the interviewers.
Afterward, focus group discussions were held to deepen the understanding of patient nutrition-related care needs and achieve credibility. In spring 2019, the focus group discussions were held. Preliminary findings, such as observation statements, interview quotes, and extreme examples from observations and interviews, were presented and discussed in the focus groups as a means of validation through peer review (Creswell & Poth, 2018). Questions were asked about older patients’ needs, responsibility for older patients’ nutrition, and nutrition-related information flow. Supporting and deviating findings were specifically questioned and discussed in the focus groups to minimize the risk of bias in the data analysis process.
Analysis
The applied inductive content analysis procedure was rule-governed based on simple text comprehension's psychological and linguistic theory (Mayring, 2015) and thus intersubjective verifiable. In addition, during the entire research project, contextual information was collected through observations and memos. These were considered when paraphrasing, building codes, and summarizing data into categories and themes during the content analysis (Mayring, 2015).
According to the interpretative-reductive method, observation notes were summarized by rewriting and summarizing texts (observation memos and observation notes) into a concise description (Mayer, 2019). Finally, according to rules for “annotated transcripts,” interviews were transcribed verbatim (Mayer, 2019). Afterward, observation data and patients’ interview transcripts were encoded using the qualitative data analysis software MAXQDA (Rädiker & Kuckartz, 2019). The cyclic process of data analysis followed the steps displayed in Figure 1. Finally, intercoder agreement about the level of abstraction was sought and reached through discussion within the research team as suggested by Mayring (2015).
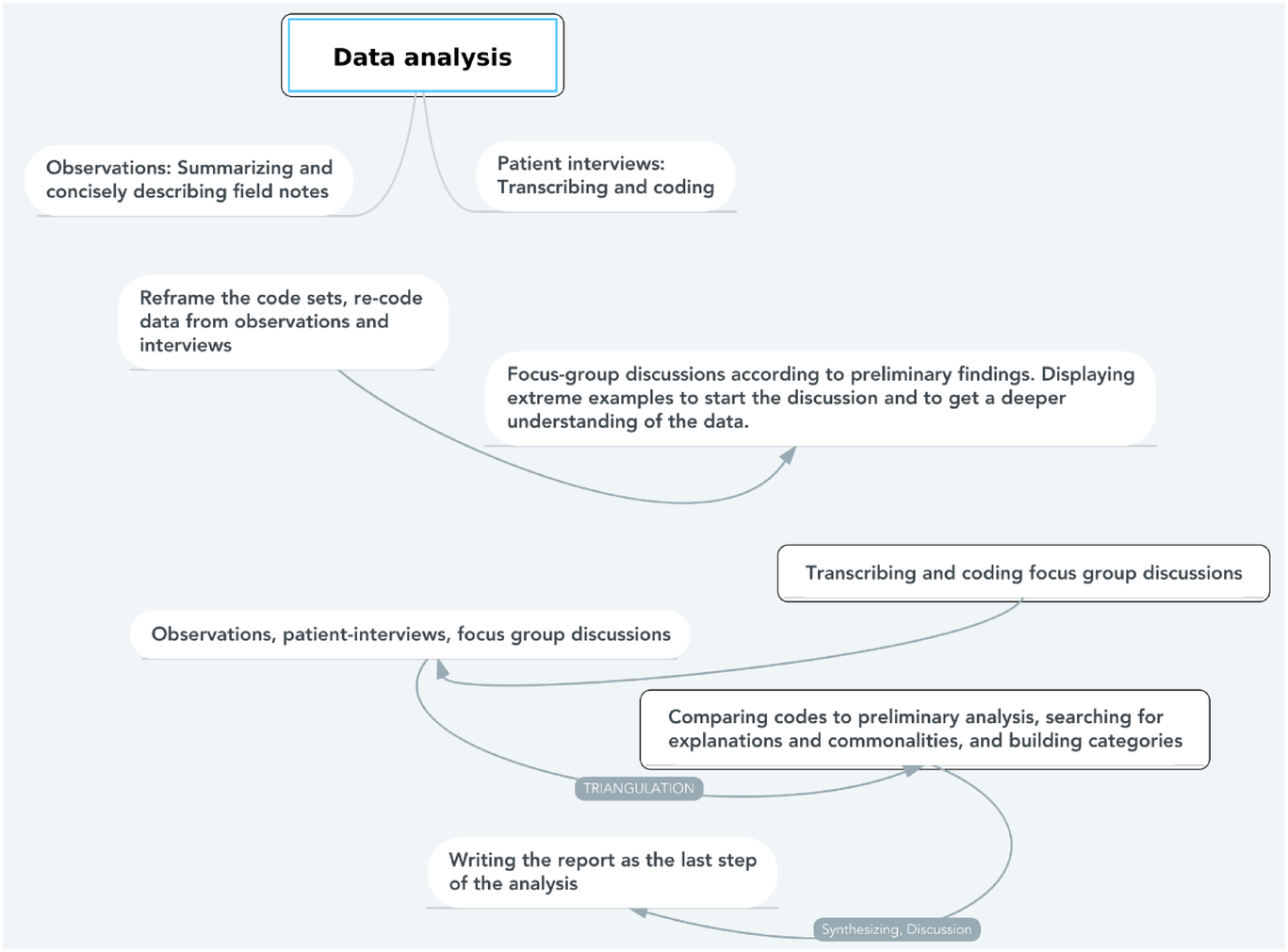
Data analysis of patient interviews, observations, and focus group discussions
Triangulation
Triangulation was performed during data analysis and interpretation. After coding observation data and interview transcripts, the complete data corpus was recoded and summarizing codes were defined from observations and interviews. Subsequently, focus group discussions were transcribed and coded within the same dataset. Codes were adjusted, summarized, and reframed into themes through discussion within the research team to distinguish themes from each other.
Ethical considerations
Qualitative validity was sought through data collection and analysis applying principles of trustworthiness. The latter included dependability, comprehensibility, and credibility of collected and analyzed data (Creswell & Plano Clark, 2018). Dependability in this project meant ensuring a traceable research process so that findings might be repeated (Cohen & Crabtree, 2006; Nowell et al., 2017).
The procedure of developing the data collection guides with experts in nursing and research, and the discussion of preliminary findings within a focus group enhanced dependability in the form of peer review (Creswell & Poth, 2018; Lincoln & Guba, 1985). In addition, a supervised trial run of every research team member took place to achieve intersubjective comprehensibility and credibility during interviews and observations, as depicted by Flick et al. (2019).
Additionally, dependability was sought through a transparent description of the methodology, accurate data integration, and applying it to the Consolidated criteria for reporting qualitative studies (COREQ, see Table A1) (Tong et al., 2007). Furthermore, several feedback rounds by the research team aimed to enhance the credibility of the triangulated data (Lamnek & Krell, 2016). In addition, trustworthiness was facilitated since the first author was in the role of the investigator. Thus, this researcher knew the data in their context well, which supported the credibility in data analyses, which was subsequently checked and proofed by the study supervisor. Finally, credibility was sought by a detailed description of the methods and context, and triangulating various data sources, such as patient interviews, observations, and focus group discussions that may complement, strengthen, support, and validate the synthesis (Creswell & Plano Clark, 2018; Mertens et al., 2016).
One day before signing a consent form, participants or their legal representatives received oral and written information about the study aims and their right to quit participation at any time point. They were assured that participation or denial did not influence current care or medical treatment. Each participant was given a pseudonym when data were entered into a data collection file.
FINDINGS
Patient characteristics
Twenty-two of the 37 hospitalized older patients who met the inclusion criteria in the investigation period participated. Reasons for denial were: too ill (3), perceived themselves as disabled to contribute (3), declined to participate (8), or discharged unexpectedly (1).
Participants were hospitalized in the perioperative unit (7), internal Medicine unit (8), and in an acute geriatric care ward (7). Medical diagnoses were in the domain of frailty or fracture (6), cardiovascular diseases (6), infectious diseases or inflammation (4), metabolic disorders (3), impaired urinary elimination (2), and chronic pain (1). Twelve participants had no cognitive disorder, while seven had mild cognitive impairment, two were diagnosed with delirium, and one participant had a diagnosis of dementia. The mean participant age was 86.1 years (range = 80–94 years), and they lived on their own (18) or in a long-term care institution (4). The total observation time was 198 h (mean: 9 h per patient). Interviews lasted between 20 and 60 min. Nutrition-related nursing diagnoses would have been necessary but not recorded for four patients.
Focus group participants’ characteristics
The following 8 out of 13 invited practitioners participated in the two focus group discussions: three Advanced Practice Nurses, a food preparation leader, a registered dietician, a gastroenterologist, one member of the acute geriatric nursing ward, and a member of the service team. Five practitioners denied participation due to a lack of time and other priorities. Both focus group discussions lasted for 85 min. All participants had at least 10 years of professional experience and were employed in this setting for 3 years or more.
Nutrition-related care needs of older patients
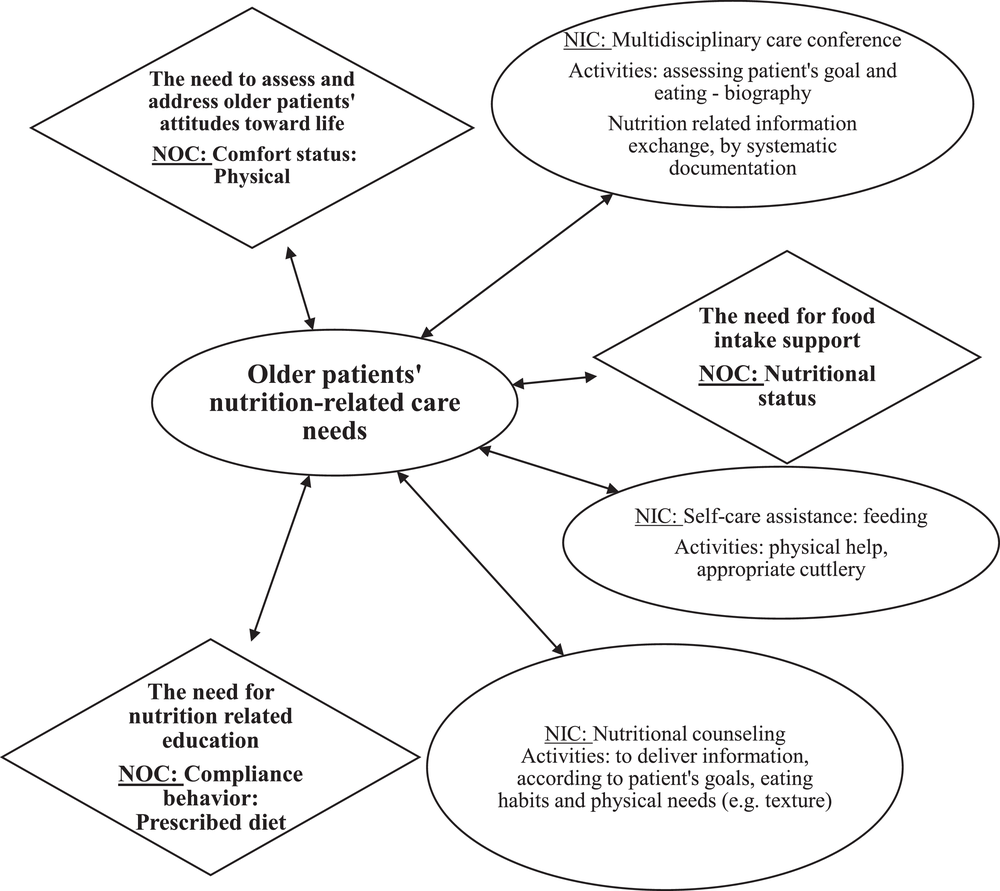
The analysis of this multimethod research revealed three themes of nutrition-related care needs of older hospitalized patients: The need to assess and address older patients’ attitudes toward life, the need for nutrition-related education, and the need for food intake support. These care needs are characterized in the text below, while Table 1 displays a more detailed example of the theme the need to assess and address older patients’ attitudes toward life. Figure 2 gives an overview of the care needs and their linkages to the conceptual framework of the Advanced Nursing Process, including Nursing Outcome Classification (NOC) (Moorhead et al., 2018) and Nursing Intervention Classification (NIC) (Butcher et al., 2018).
Example of one of the three themes of nutrition-related needs: the need to assess and address attitudes toward life
Source: Data extracted from the data analysis process supported by MAXQDA.
Older people's nutrition-related needs
The need to assess and address older patients’ attitudes toward life
A remarkable finding was that older people still felt forced to eat in some moments and tried hard to keep up their autonomy with different strategies. They explained that they enjoyed it if the ambience was easy and friendly, and they did not eat if they felt forced. This noneating behavior was also observed in a way that one patient occupied himself with other things when the meal was served. Ms R. explained in the interview: “I eat when I feel hungry, not when I ‘must’ eat or feel forced.”
This theme entails understanding the older patients and knowing if it is their goal to become independent again or to face the end of their lives as exemplary quotes have shown in triangulated data in Table 1. In addition to the data in Table 1, the field observation of Mr S. revealed that Mr S. was lying in bed for the majority of the time. No impulse to eat or drink could be observed on the day of data collection.
The attitude toward life also affects the goal of treatment and the choice of diet and menu design. This need consists of timely information exchange within and between the healthcare teams, service team, dietician, and cooking personnel with relevant implications for medical treatment. Still, nutrition-related information exchange was observed only when nutritional status was a topic in the doctor's ward rounds.
In line with data triangulation, there is a need to include older patients and their relatives to assess expectations and the persons’ overall situation. Ms N. from the perioperative care ward explained her attitude and stance toward food in the hospital clearly: “Here, in hospital, not at home, but here, I need the soup. In this kitchen, it's very important, for example, where there are different dishes that don't suit me so well. So, a good, well-made soup is often important.” Another finding is displayed in the attitude of Ms C., who was used to eating with her husband, as she explained: “Even in the hospital, my husband comes to eat with me for lunch.”
As reported by a focus group participant, it is as essential as challenging to figure out and differentiate whether someone was talking about dying because of physical exhaustion, fatigue, sickness, or when an older person ate less based on suicidal ideation, as displayed in the column of observations in Table 1. A similar issue of assessing care needs and attitudes has been explained in the focus group discussion: “We need to record how much was eaten from one full-size portion or half a serving (…) often nurses do not care too much, they forget about how much one ate.”
A disconfirming finding to the need to assess older patients’ attitudes was the statement of Ms B. on the acute geriatric care ward when the interviewer asked: “Do they (nurses or doctors) ask you about your appetite here in the hospital?” Ms B.’s answer is short: “No.” As another example, in the case of Ms O., it seemed as if the staff was not aware that she had liquid restrictions due to hemodialysis, as she had no liquid intake protocol and received soup at every meal during the last days (interview Ms O.).
The need for nutrition-related education
This theme was developed when it became evident that some older patients did not know what they could select for dinner. For example, during an interview, Mr D. said, “Sometimes I get what I like, sometimes I do not know what I have ordered, as the names of the menus sound unfamiliar to me.” Still, most of the interviewed patients were satisfied with the selection possibilities, as confirmed by observation and interview with Ms E.: “I can choose most of the time; usually, I find something I like.”
The observation of Ms T. revealed a large variety of possible menu selections: two menus with meat, one vegetarian menu, a soup, a cold salmon plate, pasta with tomato sauce, or “Bircher Muesli” (yoghurt with cereals and fruits). This service team member used a folder with pictures of the menus for the patient speaking a language other than German. In the case of a patient's cognitive impairment, it was much more challenging for patients to choose a menu, which was shown in the observation of Mr S., who could not say what he felt like eating. Similarly, during the observation of Mr V., the service team member did not have eye contact nor listen to the patient. Instead, she suggested different menus, looking into her notebook.
When Mr V. said: “No, please, no sausage,” she asked again whether to “order mashed potatoes, carrots and sausage…” During the research interview, Mr V. reported that the food ordering process was too fast.
The need for nutrition-related education became even more clear as patients and their relatives were often not informed about the prescribed food type or about medical barriers in swallowing or digestion, such as dysphagia due to dementia. In addition, relatives needed education on how to support their loved ones back at home. Finally, patients themselves need to know more about what a dietician comes for and why they receive nutritional counseling.
According to data triangulation, another important point was that patients needed to get information about taste and taste disorders in advanced age, including dysgeusia due to medication. This finding was reinforced by the interview with Ms F., where the need for information about why food might taste metallic came to light.
Ms E. saw herself as an expert in her nutrition, on the contrary to the need for information and education: “I just have to look for myself; I know what I'm not allowed to have.” The interviewer asked: “Did you mention your intolerance of pulses towards the hospital care team?” Ms E. replied, “No, no, it's not even an intolerance; it's just, it makes too much uric acid, and that makes gout attacks.”
The need for food intake support
The need for food intake support describes patients’ need for practical and physical support during mealtime. This theme also includes the need for motivation to be present, listen to and observe the patient, and offer and serve food in a friendly manner. As explained in a focus group discussion, food intake support was lacking in some situations: An older woman ordered a pureed meal instead of asking someone to cut the fish or bring her dentures. In addition, older patients need individual support, such as oral care and help to put the dental prosthesis in or to sit comfortably at the table to eat well, as explained in a focus group discussion: “It is our responsibility that the patients do not only receive food but are nourished adequately.”
A negative case in which the need for food intake support was not met, was described in the following observation of Mr D.: The patient has difficulty cutting the meat. He then manages to cut it into a bite size that is appropriate for him. The patient tells me that his right arm hurts with every movement, even when cutting meat. He drops the cutlery twice, and the research assistant gets him a new one.
DISCUSSION
This study fills the gap in nutrition-related care needs by triangulation of patients’ perspectives, nurses’ observations, and expert opinions concerning older patients in hospitals that led to the following three elaborated care needs: The need to assess and address older patients’ attitudes toward life, the need for nutrition-related education, and the need for food intake support. This care needs analysis implies that older hospitalized patients would like to be asked about their aims concerning goals in life, food and nutrition during a hospital stay, and discuss their nutrition-related objectives. Assessing food experiences, habits, and personal assumptions is fundamental, as intrinsic and extrinsic motivators for eating diminish in this advanced stage of life, as explained in focus group discussions. The urgency of an appropriate assessment as the first step of the nursing process has been declared by Ackley, Ladwig, and Makic: “Data on all dimensions of the ‘patient's story’, including biophysical, psychological, sociocultural, spiritual and environmental characteristics, are embedded in the assessment.” (Ackley et al., 2017, p. 3). In a practical booklet called “Assess Notes,” Prof. M. Gordon stated that a nursing assessment is needed to identify whether or not a potential or current problem is there that would need a nursing intervention (Gordon, 2013). Thus, a needs assessment is of utmost importance to elaborate on and select an evidence-based nursing, such as the risk for inadequate protein energy nutrition. According to nurses’ needs assessment, the diagnosis leading to evidence-based, patient-centered interventions is based on “Guided Clinical Reasoning” (Gordon, 2013; Müller Staub et al., 2015).
Several investigations showed that nurse-sensitive outcomes had improved if nurses were educated and empowered to assess, judge, and systematically document patients’ reactions in clinical information systems (Leoni-Scheiber et al., 2021). Therefore, the need to assess and address older patients’ attitudes toward life could be responded to by implementing the Advanced Nursing Process focusing on food intake- and appetite-related, standardized nursing diagnoses. Responding to older patients’ nutritional care needs could include stating nursing diagnoses from the NANDA-I classification and linking patients’ responses to standardized nursing outcome criteria and nursing interventions (Table 2). Even though there is an expert study entitled “NANDA-I, NOC, and NIC Linkages for Nutritional Problems,” there is little consistency, such as the NOC “Appetite” or “nutritional status” and NIC “Nutrition Management” or “Self-care assistance: Feeding.” The main difference is that the herein presented study aimed to explore the care needs of older people in hospital, while the formerly investigated Linkages focused on the nursing diagnosis of nutrition of infants and of obesity and overweight (Mantovani et al., 2020). Older patients’ nutritional care needs can be met when nurses are empowered to pass on the information and professionally argue for their well-being toward relatives and patients themselves. This finding is confirmed by an investigation of the Advanced Nursing Process and “Guided Clinical Reasoning” (Leoni-Scheiber et al., 2021). According to “Guided Clinical Reasoning,” the quality and coherence of the nursing assessments, diagnoses, and effective nursing interventions have improved after workshops with case evaluations (Leoni-Scheiber et al., 2021).
A newly developed risk nursing diagnosis “Risk for inadequate protein energy nutrition” with linkages to NOC outcomes and NIC interventions
Patients’ needs can be divided into patients’ subjectively expressed demands and healthcare provider-based needs according to evidence-based knowledge (Duursma et al., 2004). According to the literature for this older hospitalized population, a need could be to reach emotions and memories during the absence of appetite and “knowing that one has to eat” (Biedermann, 2013; Ellrott, 2013). Furthermore, as explored in the present study, older patients with visual impairment and taste disorders can only relate to previously enjoyed meals (Brombach, 2018). Therefore, it is vital to ask older patients in hospitals or their relatives about eating habits, what has influenced their eating behavior, and in which culture they live (Brombach, 2018). Similarly, Ellrott and Biedermann state that healthcare staff need to assess inpatients’ nutritional biography to let older people feel comfortable and enjoy mealtimes (Biedermann, 2013; Ellrott, 2013).
To date, few studies investigated the perspectives of older hospitalized patients. A nutrition-expert consensus described a specific need to assess patients’ nutritional status and prevent malnutrition in geriatric patients (Lems et al., 2017). The present qualitative multimethod study has strengthened these findings. The results from a literature review and expert panel (Volkert et al., 2019, p. 16) confirm the findings of this multimethod study, especially the need to address older patients’ attitudes toward life. Therefore, a comprehensive assessment of individual care needs concerning food intake support and their preferences and goals in life is required.
Strengths and limitations
Discussing the preliminary synthesis of care needs within two focus group discussions enhanced the trustworthiness of the three themes, and is a major strength of this study. However, the single-center approach might be a limitation. Data saturation was not sought nor reached. Still, collecting and triangulating data from in-depth patient observations, interviews, and focus group discussions allowed converging data to bring more profound insight into “older people's nutrition-related care needs in hospital.”
The risk of observation bias existed as open-field observators assessed nutrition-related care needs. Nevertheless, many nutrition-related care needs and gaps in practice and communication have been observed and triangulated findings supported each other. Thus, it was assumed that the healthcare team worked as usual and was not influenced by researchers.
CONCLUSIONS
Nurses can respond to older patients’ nutrition-related care needs by assessing and understanding their attitudes toward life and their biography, which affect the purposes of treatment, diet, and menu choices. Implementation of assessing nutrition-related care needs of older patients in hospitals is essential in practice and nursing education. Addressing these needs within the Advanced Nursing Process can lead to appropriate nursing diagnoses and interventions, enhancing patients’ self-care abilities. Policy strategies should consider that older patients’ specific care needs are worth being addressed. Implications for further research include developing and implementing a complex nursing intervention to optimize the nutrition of older patients in hospital. This study provides validated knowledge about nutrition-related care needs for older patients in hospital.
IMPLICATIONS FOR NURSING PRACTICE, EDUCATION AND RESEARCH
Addressing these care needs within the Advanced Nursing Process can lead to appropriate nursing diagnoses, nursing outcome criteria, and interventions, which enhance patients’ self-care abilities and, consequently, patients’ nutritional status. Thus, the herein synthesized care needs can be used to assess older patients' nutritional status in hospitals. Nutrition-related preferences and the nutritional status of older patients need to be discussed within the interprofessional team and recorded systematically.
Nurses and nursing students alike should be taught about the relevance of caring for older patients’ nutrition and their needs, leading to choosing appropriate nursing diagnoses and interventions, as displayed in Table 2 with linkages to risk factors and nursing outcome criteria. Further research is needed to develop and implement a complex nursing intervention that would take the interprofessional team and patients’ family members into account.
FUNDING
City Hospital Zurich (working hours).
CONFLICT OF INTEREST
All authors declare no conflict of interest.
AUTHOR CONTRIBUTIONS
The authors declare that they agree to be accountable for all aspects of the study entitled “Nutrition-related care needs of older inpatients: A qualitative study.” that aims to be published in the International Journal of Nursing Knowledge.
The authors ensure that questions related to any part of the work's accuracy or integrity are appropriately investigated and resolved. Each author has participated sufficiently in data collection and analysis and critically reviewed the manuscript to take public responsibility for appropriate portions of the content. Finally, they confirm to have given final approval of the version to be published.
Silvia BRUNNER, as the first author, has made substantial contributions to conception and design, including data collection, analysis, and interpretation of data. In addition, she conducted the whole writing and intern revising process.
Hanna MAYER, as a supervisor, has been involved in the conception and design, supported the draft of the manuscript, and revised it critically for important intellectual content.
Karin BLUM substantially contributed to the conception, collection, and interpretation of data and revised the manuscript.
Matthias BREIDERT substantially contributed to the interpretation of data and revised the manuscript.
Michael DIETRICH substantially contributed to the conception of the study, the interpretation of data, and revised the manuscript.
Enrico DAHL substantially contributed to the conception, collection, and interpretation of the data and revised the manuscript.
ETHICS STATEMENT
The Declaration of Helsinki (World Medical Association, 2018) was followed throughout the study. The affiliated University, the local institutional board for quality management, and the cantonal ethical committee approved the study (Req-2016-00670).
Footnotes
APPENDIX
ACKNOWLEDGMENTS
Many thanks are expressed to P. Witschi, head of the nursing department, for the working contract supporting this study. Prof. Dr M. Müller Staub and Univ.-Prof. Mag. Dr. H. Mayer are heartfully thanked for supervision and feedback during the writing process. In addition, the members of the Soundingboard discussed and developed the review question and reviewed the draft of this paper. Soundingboard members are M. Breidert, M. Dietrich, S. Frei, M. Nardi, and M. Rechsteiner.