
Abstract
Purpose
The aim of this umbrella review was to determine the most effective nursing interventions for the prevention and management of suicidal behavior. In order to do so, the review identifies interventions from the Nursing Interventions Classifications taxonomy with evidence to this end.
Methods
A systematic search was conducted for systematic reviews included in the PubMed, CINAHL, Cochrane, Scopus, Web of Knowledge, and Joanna Briggs Institute databases between January 1, 2011 and May 1, 2020.
Findings
The review is made up of 21 systematic reviews. In order to carefully analyze the interventions described, these were coded into categories, grouping the interventions into those based on psychological therapy, interventions related to pharmacotherapy, interventions related to the professional relationship between health professional and patient, and interventions aimed at the general public.
Conclusions
Nursing interventions for suicide risk management are prevalent in the scientific literature and are shown to be effective for patients with suicidal ideation or suicide attempts. Prevention and treatment of suicidal behavior require the provision of coping tools, behavioral interventions that directly address suicidal thoughts and behaviors, and support through therapeutic partnerships, among others.
Implications for nursing practice
This paper synthesizes the most current evidence on the most effective Nursing Interventions Classifications interventions for the treatment and prevention of suicidal behavior. It provides nursing practitioners with a comprehensive review of the therapeutic interventions with the best evidence and is useful for the development of clinical guidelines and protocols, as well as for the development of health policies and plans.
INTRODUCTION
Suicidal behavior (ideation, attempt, and death by suicide) is the result of a complex interaction of factors grouped under diathesis-stress models, which are also called vulnerability-stress models. These include risk factors that can trigger suicidal behavior, such as unemployment; relationship problems; drug and alcohol abuse, and social, psychological, genetic, and educational precipitating factors, along with protective factors such as self-confidence; resilience; social integration, and lethal means restriction (Wasserman, 2001; World Health Organization, 2002). Consequently, the intervention of the nursing professional should aim to promote protective factors, reduce risk factors, and mitigate precipitating factors (Anseán, 2014; World Health Organization, 2014).
The World Health Organization – WHO (2014) has warned health authorities that suicidal behavior is a major public health problem, which is why working on its prevention and management should be a priority for public health policies worldwide. Annual figures released by the Pan American Health Organization (2020) are as high as 700,000 deaths by suicide each year worldwide, as well as more than 16 million suicide attempts (since for every suicide there are around 20 attempts). Suicide attempts are considered to be the most significant individual risk factor in the general population (World Health Organization, 2018) because these acts are repeated by up to 30% of people during the first year, with 2% subsequently committing suicide successfully in the next 5 or 10 years (Cano et al., 2009).
Globally, suicide was the fourth leading cause of death in the 15–29 age group in 2019, with more than 77% of all cases occurring in low- and middle-income countries (Pan American Health Organization, 2020). The geographical distribution of the highest suicide rates includes Slovenia, South Korea, and Lithuania, with figures in the range of 27 deaths/100,000 inhabitants. In contrast, countries such as Greece, Turkey, and South Africa have a rate of less than 4 deaths/100,000 population, with hanging and jumping being the most commonly selected methods (National Institute of Statistics, 2020).
The recently published WHO (2021) strategy for suicide prevention in all countries, “Live Life,” recommends the implementation of effective evidence-based interventions, including restricting access to the most commonly used means (pesticides, firearms, or certain medications), prevention in the general population, educating the media on the appropriate dissemination of information, developing socioemotional skills in adolescents, and early detection, follow-up, assessment and treatment of the at-risk population (World Health Organization, 2021).
Due to the multiple factors involved in the development of suicidal behavior, prevention requires the coordination and cooperation of different sectors of society, such as education, health, law enforcement, politics, and the media. Studies aimed at the prevention and treatment of suicidal behavior highlight the effectiveness of multilevel intervention in adults with significant results in reducing ideation and repetition of the behavior (Melia et al., 2020; Büscher et al., 2020; Briggs et al., 2019; Gøtzsche & Gøtzsche, 2017; Larsen et al., 2016). Cognitive behavioral therapy, individual and group support, brief contact, counseling, improved access to health services, support groups led by health professionals, education and information, mental health promotion, community awareness, coping support, stress management, and symptom detection training have all been proposed as effective interventions (Hofstra et al., 2020; Lai et al., 2014).
In relation to the most recent publications on the effect of interventions for the prevention and management of suicidal behavior, Hofstra et al. (2020), in their systematic review which includes a meta-analysis, highlight the effectiveness of interventions such as health education and training, telephone counseling and follow-up, promotion of gatekeeper figures, and cognitive behavioral therapy. In terms of brief and contact intervention as a skilled strategy for suicide prevention, the WHO indicates that suicide rates decrease with follow-up interventions, training, education and counseling, the administration of lithium in specific pathologies, group therapy, and cognitive behavioral therapy, with the latter emerging as one of the most effective therapies in routine treatment (Gøtzsche & Gøtzsche, 2017; Lai et al., 2014; Riblet et al., 2017). Several studies report a decrease in self-harming events, following brief contact interventions including telephone or postal mail follow-up (Milner et al., 2015). New technologies employed for the promotion of contact interventions offer promising and significant results in prevention, as well as a positive impact on the promotion of coping strategies in reducing depression, distress, and self-harm (Larsen et al., 2016; Melia et al., 2020).
Professional health intervention for the care of people at risk and/or with suicidal behavior is carried out by community care teams, hospitalization and emergency services and particularly by the different units that make up the mental health care networks of the health services. From these units, the nursing professional, as part of the multidisciplinary team, develops general and specific interventions on population, patient and/or user, health education, contact, follow-up and case management, cognitive behavioral therapy, problem-solving therapy, survivor interventions, interpersonal therapy, medication administration, and crisis intervention techniques, among others (Registered Nurse's Association of Ontario, 2009). These types of interventions carried out by nursing professionals are generally well received by the patient due to the availability, accessibility, and therapeutic relationship established between the patient and the professional (Silva et al., 2018). Nursing professionals contribute their knowledge and skills at the levels of care, management, education, and research (Galvis, 2015).
Nursing activity in relation to the intervention and prevention of suicidal behavior is fundamentally encapsulated by the ninth need described by Virginia Henderson in the Basic Needs nursing model, “Avoidance of environmental hazards,” which includes the assessment of the patient's knowledge of environmental hazards and their corresponding prevention and intervention (Gallego et al., 2015; Henderson, 1961). The NANDA-International (NANDA-I) nursing diagnosis on the risk of suicide (00150) is defined as the situation where there is a danger of self-inflicted life-threatening injury (Ackley et al., 2021).
This study will use the nursing diagnosis Risk for suicide (00150) as a reference to determine, according to current scientific evidence, which interventions are effective in nursing practice for the prevention and treatment of suicidal behavior, identifying these in the Nursing Interventions Classification (NIC) taxonomy (Butcher et al., 2018).
Systematic reviews and meta-analyses describing interventions for the prevention and treatment of suicidal ideation and/or attempted suicidal behavior employ heterogeneous methodologies, which impede a joint perspective that would allow for the identification of the most effective interventions that nurses can implement. An umbrella review is a systematic review that synthesizes the highest level of evidence and contributes to a global and complete vision to respond to the objectives pursued, providing an assessment of the quality of the existing evidence (Aromataris et al., 2015; Biondi-Zoccai, 2016). One of the main utilities of this methodology is that a more holistic perspective on the available scientific evidence can be obtained from several systematic reviews answering the same question and with a more systematic and rigorous focus than an integrative review (Fusar-Poli & Radua, 2018). The creation of an umbrella review involves compiling the studies with the best evidence, in this case for the search for effective nursing interventions for the treatment and prevention of suicidal behavior, in order to generate a high-quality overview of the issue in question (Chambergo-Michilot et al., 2021).
OBJECTIVE
The aim of this umbrella review was to identify and gather scientific evidence on nursing interventions from the NIC taxonomy that have been shown to be effective in the prevention and treatment of suicidal behavior (Butcher et al., 2018).
The overarching review question for the study was as follows: What nursing interventions have been shown to be effective in the prevention and treatment of suicidal behavior in adults?
METHODS AND ANALYSIS
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The umbrella review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with registration code CRD42020221516.
Eligibility criteria
Systematic reviews with or without meta-analyses on the effectiveness of nursing interventions on suicidal behavior in men and women over 18 years of age, in Spanish and English, and less than 10 years old. To compile evidence on interventions that could be extrapolated to the general population, research was excluded if the sample consisted of specific population groups with particular idiosyncrasies, such as military authorities, armed forces personnel, war veterans, or the prison population.
Sources of information
A systematic search was conducted of papers published between January 1, 2011 and May 1, 2020 listed in the PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Database of Systematic Reviews (CDSR), Scopus, Institute for Scientific Information Web of Knowledge (ISI WoK), and the Joanna Briggs Institute (JBI) databases. In 2011, the European Community called on member states to include strategies focusing on the treatment and prevention of suicidal behavior in their health policies (Scheftlein, 2011). In the same year, the WHO published a protocol guide for the intervention and assessment of patients with suicidal behavior and mental disorders, among others (World Health Organization, 2011). Subsequently, at the World Health Assembly in 2013, an agreement was made to develop the “WHO Comprehensive Mental Health Action Plan 2013–2020,” one of the priority goals of which was to reduce the suicide rate by 10% by 2020 (World Health Organization, 2013).
The keywords used were suicide attempted, suicide, suicidal ideation, primary prevention, secondary prevention, tertiary prevention, risks, risk assessment, risk factors, risk reduction behavior, and systematic review. These were combined with the Boolean operators and adapted specifically to each database.
Search strategy
The search strategy is shown in the file “Supplementary 1.”
Selection process for studies
The inclusion of papers was assessed by two independent reviewers and they assessed the methodological quality of the included systematic reviews and meta-analyses and data extraction. Selection conflicts between reviewers were resolved by an independent third reviewer.
The process began with the initial search and exclusion of duplicate studies; the review of the title and abstract was conducted by two independent reviewers. Papers that were only selected by one reviewer were retrieved for full-text reanalysis by both reviewers. Conflict resolution was carried out by a third-party reviewer.
The search comprised a total of 3711 papers, obtained 575 from PubMed, 341 from CINAHL, 22 from CDSR, 1156 from Scopus, 1563 from WOS, and 54 from JBI. Duplicates were eliminated and 2302 results were included for analysis by title and abstract. After applying the defined inclusion and exclusion criteria, a total of 314 papers were critically analyzed. Following this analysis, 23 studies moved on to the next phase.
Data extraction procedure
The Covidence program was used as a tool for reviewing and selecting papers for review (Covidence, 2020). A form for data extraction was developed using an adapted version of the “JBI data-extraction tool.” The data extracted through the extraction form and based on the research question were analyzed in order to identify and summarize the nursing interventions represented in the selected studies.
Risk of bias assessment (quality of reviews)
As at all stages of the process, the assessment of the quality of the papers was carried out independently by two reviewers (TSS and ISA) and in case of disagreement, a third reviewer arbitrated the decision (FML). The tool used was the “JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses” (Joanna Briggs Institute, 2020). This instrument is based on 11 criteria that give each paper a quality rating ranging from “low” if the score is below 40%, “medium” if it scores 70%, and “high quality” if it scores above 70%. After two papers obtained a quality assessment of less than 40% (low quality), the research group decided to exclude them from the research, so a total of 21 reviews were finally selected (Figure 1). Regarding the results of the quality analysis, 14 documents were rated with a high-quality level, and seven with a medium-quality level. Lack of clarity in the exposition of the review question and the absence of methods to minimize errors in data extraction were the most frequent reports in the evaluation. The “Supplementary 2” document contains the complete quality analysis of the reviews included.
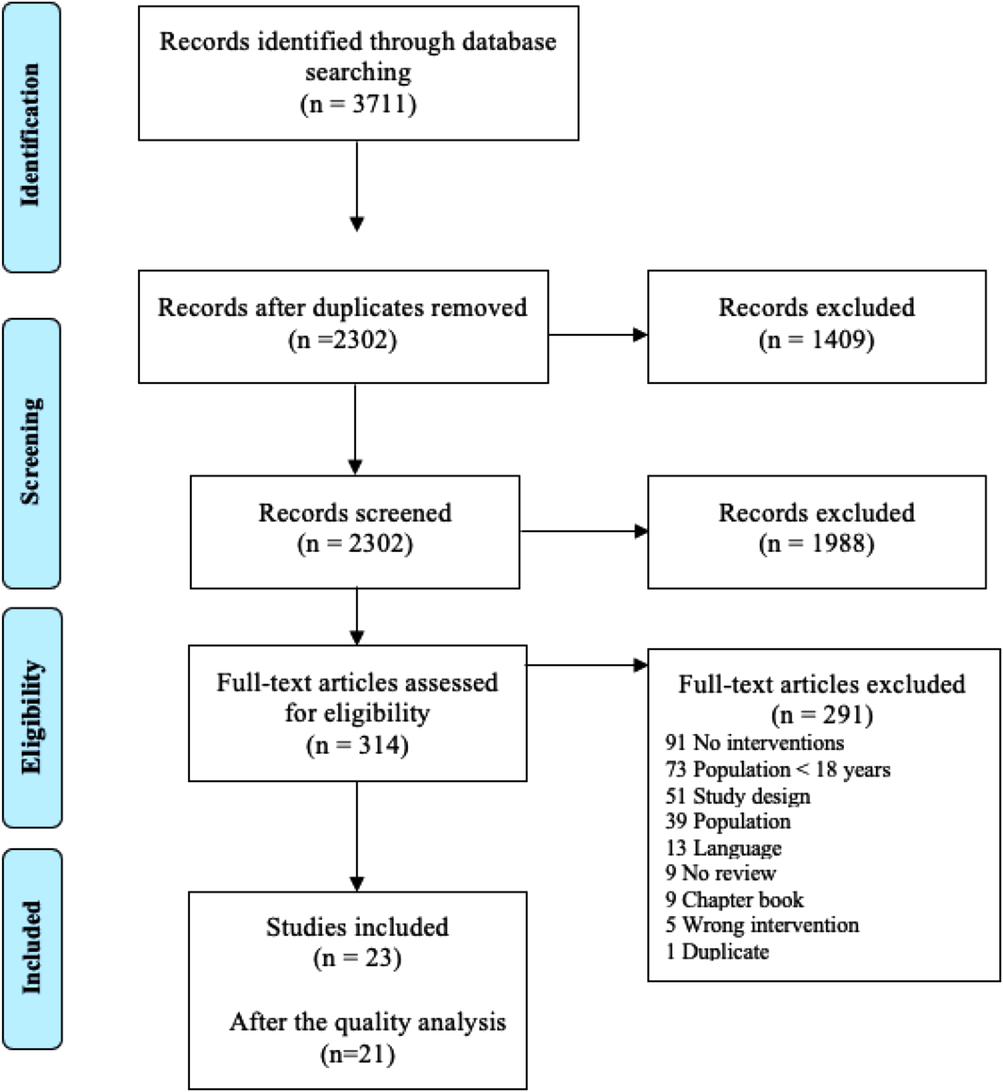
Adapted PRISMA flowchart
RESULTS
The results are presented as a narrative synthesis highlighting the main findings. The evaluated interventions were coded into categories: interventions based on psychological therapy, interventions related to pharmacotherapy, interventions related to the therapeutic relationship between health professionals and patients, and interventions aimed at the general population.
The umbrella review consists of 21 systematic reviews that were published between 2011 and 2020. The characteristics of the reviews included for analysis are shown arranged chronologically in Table 1.
Details of the included systematic reviews
Seven of the reviews included meta-analyses (Büscher et al., 2020; Hofstra et al., 2020; Briggs et al., 2019; Gøtzsche & Gøtzsche, 2017; Meerwijk et al., 2016; Milner et al., 2015; Winter et al., 2013), one paper focused on the working environment (Milner et al., 2014), and one was based on a population aged 60+ (Okolie et al., 2017). Several reviews examined the prevention of suicidal behavior through the use and employment of online tools, mobile apps, and social networks (Büscher et al., 2020; Melia et al., 2020; Larsen et al., 2016; Robinson et al., 2016; Christensen et al., 2014; Lai et al., 2014).
Six reviews examine which interventions are effective for the prevention of suicidal behavior (Hoffberg et al., 2019; Hofstra et al., 2020; D'Anci et al., 2019; Méndez-Bustos et al., 2019; Riblet et al., 2017; Lapierre et al., 2011) and more specifically, some work focused on evaluating the functionality of specific interventions in the prevention of suicidal behaviors such as the development of resilience in the adult population (Macedo et al., 2014), brief contact (Milner et al., 2015), or acceptance and commitment therapy (Tighe et al., 2018).
Interventions based on psychological therapies
Under the category of interventions based on psychological therapies, dialectical behavioral therapy, cognitive behavioral therapy, problem solving and adjustment therapy), psychodynamic therapy, psychoanalytic therapy, acceptance and commitment therapy, and family, interpersonal, or group therapy are observed as effective interventions (Hofstra et al., 2020; Briggs et al., 2019; D'Anci et al., 2019; Hoffberg et al., 2019; Méndez-Bustos et al., 2019; Tighe et al., 2018; Gøtzsche & Gøtzsche, 2017; Okolie et al., 2017; Riblet et al., 2017; Larsen et al., 2016; Meerjwijk et al., 2016; Milner et al., 2015; Winter et al., 2013; Lapierre et al., 2011).
Interventions focusing on pharmacological treatment
In the review, the health interventions focusing on pharmacological treatment that stand out for their effectiveness are education and training on the prescribed treatment; long-term control and monitoring of pharmacological guidelines; information and education on the most frequent side effects; adequate monitoring of the patient with prescriptions for ketamine and lithium; promotion of adherence to prescribed guidelines and pharmacological treatment for affective disorders (Okolie et al., 2017; Riblet et al., 2017; Meerjwijk et al., 2016; Lapierre et al., 2011).
Interventions related to the relationship between the health professional and the patient
Health interventions, related to the broader health professional–patient relationship, would include active patient follow-up and the establishment of follow-up meetings/consultations, brief intervention (via telephone, email, or mail), early detection and treatment of depression and its symptoms, training, and counseling in self-care, acceptance, social and coping skills training, mood monitoring and promotion of resilience (Hofstra et al., 2020; Melia et al., 2020; Briggs et al., 2019; Hoffberg et al., 2019; Méndez-Bustos et al., 2019; Okolie et al., 2017; Riblet et al., 2017). Stress management, strengthening protective factors, crisis contact and support, mood and emotion management, therapeutic alliance, support group membership, and the development of a personalized care plan are also reported as effective interventions (Larsen et al., 2016; Meerwijk et al., 2016; Robinson et al., 2016; Milner et al., 2015; Christensen et al., 2014; Lai et al., 2014; Macedo et al., 2014; Milner et al., 2014; Winter et al., 2013; Lapierre et al., 2011). For the implementation of these interventions, scheduled nursing consultations, telephone, and new technology-based follow-ups and consultations, and supportive home visits through assertive community therapies have been shown to be effective ( Büscher et al., 2020; Robinson et al., 2016; Christensen et al., 2014; Lai et al., 2014; Macedo et al., 2014). Because of the strong relationship between suicide and hopelessness (Ribeiro et al., 2018), interventions for more acute contexts may include providing hope, managing self-harming behavior, limit setting, and crisis intervention or even first aid (Butcher et al., 2018).
Interventions targeting the general public
Interventions related to the general population (society/community) for the treatment and prevention of suicidal behavior include raising awareness and understanding of the problem, facilitating access to health services, reducing access to the most commonly used means, promoting the role of community gatekeepers, promoting mental health and reducing isolation. In addition, they encompass the production and distribution of standardized, nonsensationalized, truthful information through social networks, media, and websites, as well as the early identification of harmful content (Hofstra et al., 2020; Méndez-Bustos et al., 2019; Okolie et al., 2017; Christensen et al., 2014; Larsen et al., 2016; Lai et al., 2014; Macedo et al., 2014; Milner et al., 2014). In this context, the interventions of the NIC taxonomy that are related to the community aspects are as follows: environmental management – safety; health education in general and particularly in the prevention of substance abuse; establishment of consultations or visits that promote mental health; listening visits; exchange of health care information; improvement of access to health information; and training in first aid. In addition, and specifically in the community closest to the patient, increasing family and social support systems, and enhancing socialization are effective interventions (Butcher et al., 2018).
Table 2 shows specifically coded interventions from the NIC taxonomy that are most effective for the correct management of patients with suicidal behavior.
Interventions codified in the NIC taxonomy which are most effective for the proper management of patients exhibiting suicidal behavior
DISCUSSION
This review has identified and compiled the scientific evidence that addresses the prevention, management, and treatment of suicidal behavior using nursing interventions from the NIC taxonomy so that the objective set by the research team has been achieved.
Due to the magnitude of the serious public health problem of suicide, the reduction of suicidal behavior must become a priority in social, political, media and health agendas, where greater awareness and training of professionals are needed, through knowledge of evidence-based interventions. This article identifies the most effective interventions from the NIC taxonomy described for the prevention and treatment of patients presenting with suicidal ideation and behavior. In order to get a broad and comprehensive view of existing interventions supported by the best evidence, an extensive search was conducted, including systematic reviews and meta-analyses. An assessment of the methodological quality of the included systematic reviews and meta-analyses by two independent reviewers determined a high-quality rating for most of the studies. Taking into account the concepts that integrate the holistic nursing metaparadigm (person, health, environment, care), as well as the different integral models of nursing care such as the critical-holistic model of Miotto Wright (Wright, 2000), intervention against suicidal ideation and the prevention of suicidal behavior offers the nursing discipline a wide field of intervention. The results of this study confirm the efficacy of holistic (bio-psycho-social) interventions, based on psychological therapy, pharmacotherapy, interventions related to the relationship between the health professional and the patient, and interventions aimed at the general population.
NIC interventions based on psychological therapies for the management and reduction of suicide risk are prevalent in the scientific literature and are shown to be effective for patients with suicidal ideation or previous suicide attempts (D'Anci et al., 2019; Gøtzsche & Gøtzsche, 2017; Lai et al., 2014; Meerwijk et al., 2016; Méndez-Bustos et al., 2019; Milner et al., 2014). In this line, P. C. Gøtzsche and P. K. Gøtzsche associated interventions based on modifications of the patient's thought processes, improvement of self-confidence, and cognitive restructuring with a 50% reduction in the repetition of suicidal behavior. Interventions to build resilience, and improve self-awareness, self-esteem and coping have been shown to be effective in reducing suicidal risk (Pérez et al., 2021; Revuelta et al., 2016). After these interventions, patients' expression improved self-acceptance and were able to recognize some positive personal characteristics; several studies report a significant improvement in the Rosenberg Self-Esteem Scale after these NIC interventions (Rodríguez et al., 2014). The use of self-help interventions, aimed at working on self-esteem and coping strategies, based on new information technologies (chats, social networks, apps, email, and so on) are associated with significant reductions in suicidal ideation when developed on the basis of scientific evidence and best practices (Büscher et al., 2020; Christensen et al., 2014; Lai et al., 2014; Larsen et al., 2016; Melia et al., 2020; Robinson et al., 2016). In this area, some studies have shown the development of these techniques in online formats using new technologies and tools to be effective, including mobile applications, group chats, and social networks (Büscher et al., 2020; Robinson et al., 2016; Christensen et al., 2014; Lai et al., 2014; Macedo et al., 2014).
Patients with suicidal ideation and/or behavior often require pharmacological treatment, especially when suicidal ideation and/or behavior is related to the presence of a mental disorder (Barbero et al., 2010; Sansaloni et al., 2020; Rodríguez et al., 2014). NIC nursing interventions related to medication management, including patient education (teaching of prescribed medication) on the use of psychotropic drugs, appropriate follow-up by nursing professionals, adherence, and side effect management showed significant evidence for the prevention and treatment of suicidal behavior (D'Anci et al., 2019; Lapierre et al., 2011; Meerwijk et al., 2016; Okolie et al., 2017; Riblet et al., 2017). Mood regulators, such as lithium, are among the most commonly used drugs in these preventive programs (D'Anci et al., 2019).
Interventions related to the nurse/patient relationship should be singled out as high-quality preventive interventions by assessing the active follow-up of patients and enabling the nursing practice to develop NIC interventions such as health counseling and education, decision support, values clarification, emotional support, mood management, active listening, and contact. Several studies link brief contact interventions to a reduction in suicide attempts (Milner et al., 2015; Riblet et al., 2017). The effectiveness of these interventions has been demonstrated both for direct contact in consultation or at home, and for contact by telephone, email, or post (Büscher et al., 2020; Christensen et al., 2014; Melia et al., 2020; Riblet et al., 2017; Robinson et al., 2016; Consejería de Sanidad y Dependencia, 2008). The scientific literature has linked contact interventions where emotional support is provided to the reduction of self-harm related to suicidal ideation (Briggs et al., 2019; Hoffberg et al., 2019; Méndez-Bustos et al., 2019; Winter et al., 2013). The therapeutic nurse/patient relationship is a protective element against suicidal behavior (Briggs et al., 2019; Lapierre et al., 2011; Riblet et al., 2017); from this supportive relationship, it is possible to help maintain positive family processes and promote family integration. Some authors have emphasized the preventive role of the nuclear family. The family context can become a positive source in terms of self-control, verbal conflict resolution, counseling, emotional support, monitoring, and protection from self-destructive and risky behaviors (Becoña Iglesias, 2001; Sánchez et Carrillo, 2002; Barbero et al., 2010; Villa et Hermida, 2001).
In terms of community intervention, in the NIC taxonomy, we can highlight the identification and management of risks in the environment (environmental management). In this regard, restricting access to the most widely used lethal methods is one of the most prevalent preventive measures; however, efforts should be directed towards exploring new methods which could replace them, with the aim of working proactively (Méndez-Bustos et al., 2019; Okolie et al., 2017; Christensen et al., 2014; Larsen et al., 2016; Lai et al., 2014). Health education and improved access to health information are key preventive elements. It is a priority to “break the silence,” the traditional obscurantism, and to break with false myths, thinking and beliefs in relation to suicidal behavior, proposing actions to raise awareness and promote mental health from nursing consultations and advising the media in the dissemination of campaigns and news (Brito et al., 2020; Revuelta et al., 2016; Galán et al., 2010). New communication technologies, including social networks, chat rooms, online platforms, and mobile applications, are now key tools for community awareness raising. The reach, anonymity, instantaneity, and accessibility of these new information and communication technologies allow them to act as key elements alongside traditional media (Larsen et al., 2016; Macedo et al., 2014; Robinson et al., 2016).
Based on the latest edition of the NIC catalog of interventions (Butcher et al., 2018), this review identifies the various interventions that have been shown to be effective for individual and group work with the patient, family, and community. Prevention and treatment of suicidal behavior require comprehensive management in which patients, family, and community are provided with coping tools; behavioral interventions that directly address suicidal thoughts and behaviors; emotional management through psychological therapies; conventional therapies together with new information and communication technologies; support through therapeutic alliances and brief contact interventions; support for adherence to treatment, environmental management, and health education for patients and community.
LIMITATIONS
The research team worked within a time range of 10 years and used the latest published version of the NIC taxonomy, but the review focuses only on the most effective and specific NIC interventions for the prevention and treatment of suicidal behaviors, so there may be a bias of interventions available to the nurse that is not described in this paper, as there is also learning from negative results.
CONCLUSION
This paper offers a highly methodological synthesis that identifies the most effective NIC interventions for the treatment and prevention of suicidal behavior. It provides a thorough and comprehensive review of the best evidence-based therapeutic interventions and can serve as a basis for clinical intervention guidelines and protocols and specific suicide prevention plans. These results enable nursing professionals to use the evidence to make decisions in their daily practice.
IMPLICATIONS FOR NURSING PRACTICE, RESEARCH, AND EDUCATION
This umbrella review synthesizes the most up-to-date evidence on the most effective NIC interventions for the treatment and prevention of suicidal behavior. It provides nursing practice with a review of the therapeutic interventions with the best evidence, being useful for the development of guidelines and protocols in clinical and care settings, as well as providing the up-to-date and evidence-based documentation that is necessary for the development of health policies and plans focused on the prevention and management of suicidal behaviors.
The standardized nursing interventions that have been detailed in this work allow the care provided to the patient, family, and community to be recorded and evaluated in a universal way, and thus to assess the impact on the needs and health of the units to be treated. Nursing professionals working in the field of research use standardized nursing language that facilitates the study and analysis of the quality and efficacy of the care provided. Therefore, the results obtained in this review can be used as quality indicators and can easily be compared with interventions and care provided worldwide. In the same way, these results synthesize the most current and effective scientific evidence, making it a necessary tool in the educational field for training future nursing professionals.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
AUTHOR CONTRIBUTIONS
Conceptualization: Teresa Sufrate-Sorzano and María Elena Garrote-Cámara.
Methodology: Teresa Sufrate-Sorzano, Jesús Pérez, María Elena Garrote-Cámara. and Regina Ruiz de Viñaspre.
Software: Raúl Juárez-Vela and Fidel Molina-Luque.
Validation: Jesús Pérez, María Elena Garrote-Cámara, Iván Santolalla-Arnedo and Raúl Juárez-Vela.
Formal análisis: Teresa Sufrate Sorzano, Iván Santolalla-Arnedo, and Fidel Molina-Luque.
Investigation: Teresa Sufrate-Sorzano and María Elena Garrote-Cámara.
Resources: Jesús Pérez, Iván Santolalla-Arnedo, Raúl Juárez-Vela, Fidel Molina-Luque, and Regina Ruiz de Viñaspre.
Data curation: Iván Santolalla-Arnedo, Raúl Juárez-Vela, Fidel Molina-Luque ,and Regina Ruiz de Viñaspre.
Writing—original draft preparation: Teresa Sufrate-Sorzano, Jesús Pérez, and María Elena Garrote-Cámara.
Writing—review and editing: Iván Santolalla-Arnedo, Raúl Juárez-Vela, Fidel Molina-Luque, and Regina Ruiz de Viñaspre.
Visualization: Teresa Sufrate-Sorzano and María Elena Garrote-Cámara.
Supervision: Jesús Pérez, Iván Santolalla-Arnedo, Raúl Juárez-Vela, Fidel Molina-Luque, and Regina Ruiz de Viñaspre.
Project administration: Teresa Sufrate-Sorzano.
All authors have read and agreed to the published version of the manuscript.
ETHICS STATEMENT
Formal ethical approval is not required for this umbrella review under Spanish law, as no primary data are collected, and no patient intervention is involved.
PROSPERO Registration number: CRD42020221516.
Footnotes
ACKNOWLEDGMENTS
The research team would like to thank the Research Group on Care (GRUPAC) of the University of La Rioja and the Research Group on Sustainability of the Health System (GISOSS) of the Biomedical Research Centre of La Rioja (CIBIR) for their support and collaboration. There was no financial support for this article.