
Abstract
Purpose
Due to disability and reduced activities of daily living (ADL), older adult stroke survivors face difficulties deciding whether to receive care at home or move to a facility after discharge. The study aims to evaluate the impact of decision-aid (DA) use on decision-making participation and conflict regarding the selection of post-discharge care locations for older adult stroke survivors and their families.
Data sources
A randomized controlled trial will be conducted among older adult stroke survivors at a medical rehabilitation facility during their recovery period. Randomization units will be blinded and allocated according to the patient's room, and the intervention period will be approximately 2 months, from admission to discharge. The study participants will include (1) people over 65 years of age, (2) stroke survivors, and (3) those facing the need to make decisions regarding the location of post-discharge care. However, those who have difficulty making their own decisions due to severe dementia, aphasia, or altered consciousness will be excluded. In the intervention group, a DA will be provided with its utilization confirmed approximately 1 month after hospitalization. Similarly, the control group will be provided with an informative brochure, with the provision being confirmed approximately 1 month after hospitalization.
Data synthesis
The primary outcome (decision-making conflict) and secondary outcome (decision-making participation) will be evaluated using the decisional conflict scale (DCS) and revised control preference scale (CPS), respectively. Intergroup differences in DCS and CPS will be analyzed using two-way repeated measures analysis of variance and z-test, respectively.
Conclusions
Verification using randomized controlled trials is necessary to determine the effectiveness and versatility of DAs.
Implications for nursing practice
By deepening the knowledge of our priority research areas, the results of the proposed study will strengthen our fundamental knowledge by revealing older adult stroke survivors’ care preferences after discharge.
BACKGROUND
Strokes are the second leading cause of death worldwide (WHO, 2019), with high age-related rates of incidence and recurrence, and are a leading cause of care-dependent disability. As such, considering cognitive function, financial situations (Kashiwagi, 2011), activities of daily living (ADL), and family care capabilities (Kojima & Shiraishi, 2015), it is difficult to decide whether to continue living at home or to receive care elsewhere after discharge. However, in Japan, where older adults are often cared for by their families, post-discharge decisions are made between families and specialists without patient participation. This may be due to older adult patients’ difficulties in communicating their wishes (Iso & Iijima, 2016), or their participation is considered unnecessary. Hence, the most difficult task for hospitals is supporting post-discharge care decision-making and managing the “misalignment” between the wishes of older adult stroke survivors and families and/or medical professionals (Harada et al., 2014).
Currently, shared decision-making (SDM) (Hoffman et al., 2014), a joint decision-making process whereby patients and physicians are involved in medical decisions, is gradually being adopted. In SDM, patients and physicians carefully consider the patient's values and preferences and discuss the advantages and disadvantages of treatment options (Kon, 2010). Furthermore, the International Professional Shared Decision Making (IP-SDM) model, a decision-making tool between patients, doctors, families, and multidisciplinary professionals, was recently developed and is shown to be useful when applied to residence-related decision-making (Légaré et al., 2018).
One method of supporting decisions that are facilitated by the IP-SDM model is the use of a decision aid (DA). Unlike traditional information-based materials, DAs involve the comparison of the advantages and disadvantages of different options and promote selecting the option that matches one's values. Benefits include increased knowledge, reduced conflict and value uncertainty, and increased participation in decision-making (Stacey et al., 2017). It has also been proven effective for older adults (Moher et al., 2001). In Japan, the standard information-based post-discharge brochures contain large amounts of information, making the decision even more difficult. However, DAs for older adult stroke survivors and those reviewed by multidisciplinary professionals do not exist in Japan, and their effects are unclear.
Therefore, this study aims to evaluate the impact of using a DA based on the values of older adult stroke patients and their families on decision-making participation and conflict regarding potential discharge locations. We hypothesize that the group provided with a DA in selecting a discharge location will have significantly reduced decision-making conflict and increased decision-making participation compared with the nonintervention group.
METHODS
Study design
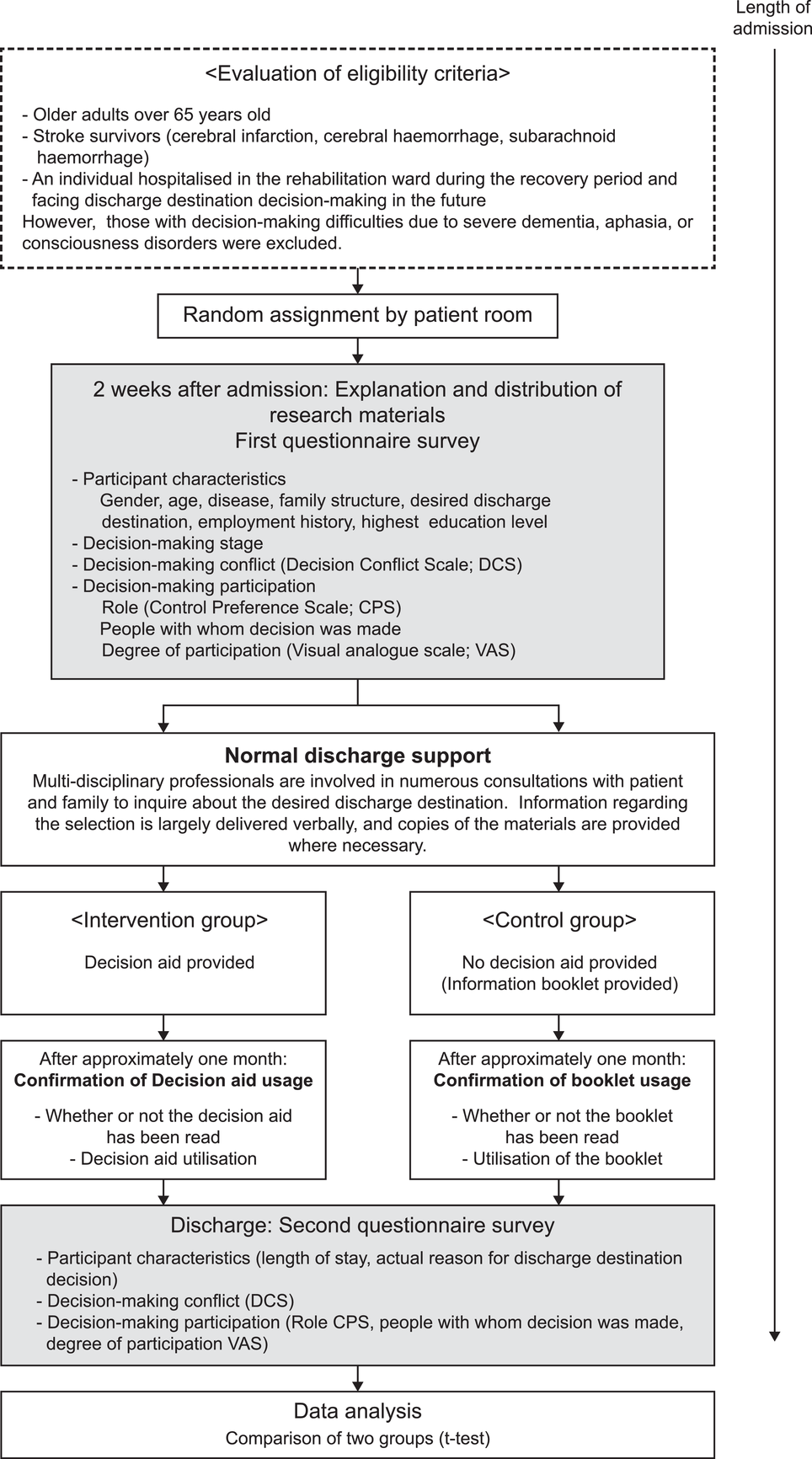
This is a comparative randomized controlled trial of older adult stroke survivors who will be allocated into a DA intervention group and a nonintervention group, who will receive an informative brochure instead (nonintervention). We expect to verify the effects of increased decision-making participation and reduced decision-making conflict. The trial will be conducted in accordance with Consolidated Standards of Reporting Trials (Moher et al., 2001; Tsutani et al., 2019), adapted for randomized trials. This protocol will be conducted in accordance with Standard Protocol Items: Recommendations for Interventional Trials (Chan et al., 2013, 2017). The study flowchart is shown in Figure 1.
Study flowchart
Study setting
The study is being conducted in the Support Center for Children with Disabilities at Toyama Prefecture Rehabilitation Hospital, which has 100 beds, distributed equally between the third and fourth wards. The hospital has male and female rooms, with little movement of patients between the rooms. There are six one-person rooms and 11 four-person rooms per ward. Usual discharge support involves screening the patients, determining the discharge location in consultation with the patients and families, and coordinating the utilization of social security systems and welfare services. Doctors, nurses, physical therapists (PTs), occupational therapists (OTs), and medical social workers (MSWs) are the core members of the multidisciplinary team. Physicians manage treatment, while nurses monitor patients’ physical conditions, manage their daily lives (e.g., providing dietary care), and provide instructions on caregiving skills. PTs and OTs work to improve ADL, instruct patients and families on caregiving methods, evaluate the home environment, and coordinate the selection of necessary home care equipment and modifications advice. MSWs mediate between patients and families, as well as ensure the provision of social security programs and welfare services. Support from the team usually involves the central MSW asking the patient and families their post-discharge location wishes and then proposing a selection of two to three social welfare services and facility options based on the decisions made. Specifically, the information is provided over numerous meetings and explained mostly verbally, with copies of the necessary materials and sections of the city's pamphlets provided.
Eligibility criteria
Study participants will be (1) older adults >65 years, (2) stroke survivors (cerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage), and (3) admitted to the rehabilitation ward during their recovery period and facing discharge location decision-making. However, those with decision-making difficulties due to severe dementia, aphasia, and altered consciousness will be excluded.
Eligibility screening and recruitment
Enrollment
Patients will be referred by the nurse manager, who would have obtained referral consent from the patient. Patients who meet the study criteria will be enrolled approximately 2 weeks after admission, after adjusting to hospital life, and after the primary investigator has obtained written consent and explained the study verbally, using the research description document.
Allocation
Preliminary studies (Aoki & Nakayama, 2019) have indicated no significant differences in characteristics concerning the age, sex, and length of stay of inpatients in the two wards. According to the stipulated rehabilitation ward criteria, the nature of the ward, staff numbers, and types of professionals are similar in both wards and will be deemed equivalent at baseline. Ward allocation at admission is managed through daily meetings between the hospital director, nursing director, and clerical staff to ensure that the hospital staff workload is spread as evenly as possible across both wards. Moreover, the nurse manager determines the room distribution based on the severity of the patients’ condition and ADL status.
The group allocation will be randomly determined according to the patient's room. Specifically, research assistant A will first create a random number table by using computer-generated random numbers that give a 50/50 chance of assigning a patient to either the DA or control groups. In this study, research assistants will be nursing students or licensed nurses who will have been trained according to the manual. Next, the nurse manager will allocate the six private rooms in three stages, two rooms at a time. Regarding the 11 four-person rooms, three rooms with the highest case severity will be selected, and the remaining eight rooms will be allocated the same way as the six private rooms. In addition, the random number and allocation tables detailing the random assignment of patients will be prepared by the principal investigator, while the patients, family members, specialists, and research assistants will be blinded to the allocation. When a patient who meets the eligibility criteria is admitted, the principal investigator will enroll and allocate according to the allocation table.
Intervention
The intervention duration for both groups will be approximately 2 months, from admission to discharge. It was decided that variations in inpatient duration, which according to prior research (Aoki & Nakayama, 2019) is 86.1 ± 44.3 days, would not impact the intervention. Furthermore, termination of research participation criteria will comprise participants who request to be withdrawn from the study or withdraw their consent, participants who no longer meet the selection criteria after enrollment, or the primary physician determining that cessation is necessary due to increasing discharge anxiety or other reasons. Moreover, removal criteria for the study participants shall include those who cannot complete both admissions and discharge questionnaires as well as those who fail to read the DA during their inpatient period.
Intervention arm: Procedures for the intervention group will include the provision of the DA and confirmation of its utilization, in addition to normal discharge support, including standard information on discharge locations and the types of social welfare services available. At approximately 2 weeks post-admission, the principal researcher will distribute the DA to the research participants referred by the ward nurses as a specific intervention step. This intervention step will take place in a private meeting room to maintain privacy. Participants will be given a 15-min explanation of the purpose, content, use, and cautions regarding the DA.
DA content will be explained as a means of thinking through the following processes: (1) having knowledge of service types and characteristics, (2) knowledge of the strengths and weaknesses of the discharge destinations, (3) determining what is important, (4) establishing a discharge plan, and (5) deciding to leave the hospital when preparations have been made. Moreover, the principal investigator will explain that decision-making involves the comparison of the advantages and disadvantages of the following six important considerations: (1) lifestyle level, (2) service and cost, (3) emergencies, (4) family support, (5) environment, and (6) home modifications. The explanation about the DA utilization will include information regarding the flexibility of the time to use it, where patients can read it at any time in preparation for discharge, and will also explain the checklist, and if the participant is willing and capable, how he/she can use this with family and multidisciplinary professionals. Furthermore, an explanation will be provided regarding how to complete the two admissions and discharge questionnaires with the help of research assistant B. The principal investigator will then confirm whether the DA is utilized after approximately 1 month.
As a precautionary measure, the principal investigator will explain that the effectiveness of the DA is currently unknown and that two types of DAs are currently being distributed to investigate its effectiveness. As such, participants will not be allowed to show the materials to other patients or their family members. If the study participant is in a four-person room, questionnaires will be administered in quiet spaces away from the patient room and other patients, such as in meeting rooms or canteens. Additionally, given that answering the questionnaire may prove difficult in some circumstances, research assistant B, who will be blinded to the participant allocation, will provide uniform responses to questionnaire administration issues in accordance with the manual.
Furthermore, to protect the personal information of participants, personal information will be communicated between the principal researcher and research assistant B in a communication file. This confidential information will be placed in secured lockers. Moreover, after participants complete the survey, research assistant B will contact the principal investigator to prevent the questionnaire from being leaked.
At approximately 1-month post-admission, the patient will discuss his/her future plans with the doctor, making concrete discharge decisions. Another 15-min meeting will be held with the participant in a private meeting room where DA use will be verified. The patient will be asked whether the DA was read, whether it was utilized with family or professionals, and whether they had any questions about the DA content or use. Finally, approximately 1–2 weeks before the date of discharge, research assistant B, who previously administered the admission questionnaire, will administer the discharge questionnaire following the same procedures as the initial questionnaire.
Control arm: Procedures for the control group will be the same as the intervention group, except that they will not receive a DA and will instead be provided with an informative brochure. Its use will be confirmed in addition to standard discharge support.
Multidisciplinary professionals: Two explanatory meetings detailing the research purpose, significance, method, content, and use of the DA will be held with the multidisciplinary professionals. These meetings will also detail precautions, such as the unproven effectiveness of the DA and the need to still provide standard discharge support to the intervention and control groups. We will ask patients to utilize the DA with families and professionals. Multidisciplinary professionals should consult with patients and families when they actively ask for help and not intervene while actively looking at or using the contents of the DA.
Research assistant B: A new user manual will be created to facilitate the provision of uniform responses to patient questions. Additionally, an explanatory meeting will be organized that details the distribution of the questionnaires at admission and discharge, confirms the method of contacting the principal investigator, and delineates the location of the communication file. Precautions to be explored will include not inquiring about group allocation and refraining from perusing the content of the DA or brochure.
Outcomes and measures
Primary outcome
Evidence from previous studies suggests that, amid the uncertainty of expected recovery, older adult stroke survivors experience conflict regarding the new self-image as someone with a disability and possibly rely on others to reconstruct their lives (Arayama, 2015). Here, the 16-item Japanese version (Kawaguchi et al., 2013; Légaré et al., 2010, 2012; Linder et al., 2011; O'Connor, 2010) of the decisional conflict scale (DCS) developed by O'Connor et al. will be used to evaluate decision-making conflict. This scale has been tested for reliability and validity and includes three sufficiently informed items, three value clarity, three support, three uncertainty, and four effective decision items. Each question is rated as follows: 0 points for “strongly agree,” 1 point for “agree,” 2 points for “neither agree nor disagree,” 3 points for “disagree,” or 4 points for “completely disagree.” A higher score indicates a higher level of decision-making conflict. Clinically significant differences in effect size are between 0.30 and 0.40, with scores of ≤25.0 related to decision implementation, while scores ≥37.5 are related to decision-making delays and feelings of uncertainty about implementation (O'Connor, 2010).
The Japanese version of the DCS contains the term “side-effects,” as it is typically used to measure whether or not one prefers to receive treatment. In our study, the use of DCS relates to choosing the post-discharge care location, so treatment-related terminology has been removed.
Secondary outcome
In Japan, discharge location decisions are often made between families and specialists without the participation of older adult stroke survivors. Therefore, three aspects of decision-making participation will be measured: (1) the role, (2) the participation level, and (3) with whom the decision is made. First, an item from the modified control preference scale (CPS) developed by Strull et al. (1984) and modified by Degner et al. (1997) will be used to evaluate the patients’ role in decision-making. This scale has been verified for reliability and consists of five questions. This study aims for families and multidisciplinary professionals to participate jointly with doctors in decision-making, so the scale has been modified, and certain terms have been replaced.
The five specific options are (1) “I will decide the discharge location,” (2) “I will decide the discharge location, having seriously considered the opinions of my family and hospital personnel,” (3) “Hospital personnel, my family, and I will decide the discharge location together,” (4) “Having seriously considered my opinion, the discharge location will be decided by my family and the hospital personnel,” and (5) “My family and the hospital personnel will decide the discharge destination.” Active decision-making roles (decision-making by the individual) are shown in options 1 and 2, a cooperative role (based on the SDM) is shown in option 3, and passive roles (decision-making by another party) are shown in options 4 and 5.
In addition, a 10-step visual analog scale will be used to assess the degree of participation, ranging from not wanting to participate/nonparticipation (0%) to wanting to participate/participation (100%). Furthermore, answers to the question “with whom did you make the decision?” will be assessed. Answers will include five options: (1) “by myself,” (2) “with family or a significant other,” (3) “with a healthcare professional,” (4) “with family or a significant other and a healthcare professional,” and (5) “I wanted to leave it to…/I left it to…(Whom?).” These measures will be added as secondary outcomes since the DCS only asks about the presence or absence of support or pressure from others in the context of decision-making participation.
Patient characteristics
Participant characteristics will include sex, age, disease (cerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage), family structure, and desired discharge location (i.e., “same location as before admission” or “different location from before admission”). Furthermore, the highest level of education, employment history, inpatient duration, and reason for the final decision regarding discharge location were included.
Statistical consideration
Sample size calculation
A prior location of care study (Légaré et al., 2015) reported a cluster randomized controlled trial protocol that required 186 participants across both groups, allowing for a loss to follow-up of 20%, a power of 0.80, an effect size of 0.5, and a significance level of a two-sided α = 0.05, to compare the difference in average values between the two groups. Prior DA studies were also reviewed in a Cochrane Library systematic review (Stacey et al., 2017), using DCS as an outcome. The case numbers for this study are thus based on a power of 0.80, an effect size of 0.5, and a significance level of a two-sided α = 0.05. According to the sample size calculation carried out using G*Power (3.1.9.2) software (Heinrich-Heine-Universität Düsseldorf, Germany), the number of cases required to investigate the differences in average values before and after the decision-making intervention will be 51 participants per group. In terms of the loss to follow-up in randomized controlled trials of older adult participants, Fleming et al. (2004) reported 38.9%, while Nagayama et al. (2016) reported 18.9%. Some patients are expected to fail to meet the eligibility criteria through acute hospital readmission or death due to worsening medical conditions, severe dementia, or altered consciousness. This is because the current study will involve participants who will be older adult stroke survivors, and the intervention period will be approximately 2 months long. However, research assistant B will administer the two questionnaires at admission and discharge, as outlined in the user manual, and the recovery rate is expected to be high. A follow-up loss of 20% for the total research is estimated; therefore, the target will be a total of 122 participants (61 per group). However, an interim analysis has not been planned, and the termination criteria have not been stipulated.
Analysis plan
Data will be entered by research assistant B and, after multiple checks, will be handled by the principal investigator. To investigate decision-making conflict as the primary outcome, an independent t-test will be used to test the differences in average values for each DCS item between the intervention and control groups at baseline (admission) and discharge. Moreover, variations between baseline and discharge will be calculated, and an independent t-test will be performed to investigate whether differences exist between the groups in terms of DCS subscale items. As differences in average DCS subscale items will reflect random variations within a level, a paired t-test will be conducted to determine whether differences in average values for DCS subscale items are determined by admission and discharge values within each group. Furthermore, since these differences indicate a variation based on factorial effects, a two-way repeated measures analysis of variance (ANOVA) will determine whether differences in average values for DCS subscale items are observed for group differences (intervention/nonintervention) or time (admission/discharge).
The secondary outcome, decision-making participation, will be investigated using a McNemar test to determine whether the discharge destination choice changes from admission to discharge within each group. In addition, if this determines the discharge location, with whom the decision was made, and whether there are ratio differences in decision-making role items (CPS). A paired t-test will determine the differences in the average participation rate. Furthermore, a z-test hypothesizing a normal distribution for pre-/post-intervention ratio difference will determine the intervention effects of the DA on discharge locations, decision-making roles, and decision participants. Repeated measures two-factor ANOVA will be performed for the participation rate. Statistical analysis will be carried out using SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, N.Y., USA), and the significance level will be set at < 5% (two-sided test).
Adherence
To improve intervention adherence, participants will be informed of the timing of the 1-month post-admission initial confirmation of DA utilization. Additionally, the front page of both the DA and the information brochure will feature the same design to prevent contamination if others in the same room are shown the brochures when patients move rooms. Moreover, as an adherence measure regarding the correct completion of the questionnaires, uniform responses will be provided by research assistant B according to the manual, and research assistant B will return the questionnaires to the principal investigator.
Loss to follow-up
Since only one rehabilitation facility will participate in the research, medical conditions are expected to remain stable. Minimal loss to follow-up is expected because close contact with the nurse manager will be maintained, and measures will be taken to minimize loss, such as having the questionnaires administered exclusively by research assistant B. Furthermore, because the study relies on random allocation for the analysis, all randomized data will be analyzed in the allocated groups, regardless of whether the study is completed or not (intention-to-treat analysis).
Data monitoring
Nurse researchers (Yoriko Aoki and Kazuhiro Nakayama) will hold regular meetings every six months to monitor the trial. Furthermore, progress reports will be submitted annually to each facility's Ethics Review Committee, with approvals expected.
Dissemination policy
All authors will contribute to the dissemination of the research results. The results of the research will be disseminated via publication: (1) at SDM and IP-SDM-themed academic conferences (scientific and professional), (2) on a website, and (3) as a paper in a peer-reviewed and specialist journal.
DISCUSSION
The purpose of this study is to evaluate the impact of DA utilization on discharge location decision-making participation and conflict, particularly when developed to assist in the selection based on the values of older adult stroke survivors and their families. In Japanese medical practice, older adult stroke survivors are confronted with large amounts of discharge location information, which increases decision-making difficulties. Therefore, establishing a decision-making support method is an urgent issue. It has been reported that patients whose discharge location has not been determined at the time of discharge are more likely to be readmitted or die after 30 days (Gilmore-Bykovskyi et al., 2018). DA may provide a foundation for older adult stroke survivors, families, and multidisciplinary professionals to work through the decision-making process together. Therefore, verification using randomized controlled trials is necessary to determine the effectiveness of DA use.
The results of the proposed study will strengthen our fundamental knowledge by revealing how older adult stroke survivors prefer to live after discharge. The knowledge gained from this study may contribute to the following areas: (1) improving evidence-based decision-making processes regarding the location of care post-discharge, (2) supporting family caregivers who are struggling with decision-making, (3) reducing decision-making conflict and increasing decision-making participation in older adult stroke survivors, (4) implementing patient-centered decision-making based on patient values, and (5) facilitating the development of decision-making support methods using the IP-SDM. As a potential limitation, the research facility is an intermediate, convalescent rehabilitation ward used between the acute-phase hospital stay and home or post-discharge facility. Therefore, it may be affected by facility standards and regional characteristics. It may also be necessary to consider increasing the number of research facilities for general standardization.
AUTHOR CONTRIBUTIONS
Yoriko Aoki designed the study and drafted the manuscript. Kazuhiro Nakayama provided advice on the analysis and study overall, as well as offering suggestions. Both authors have consented to publication and have checked the final document.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
TRIAL STATUS
Participant recruitment began in November 2018 and was halted in May 2020, when hospital entry was barred due to COVID-19 restrictions. Currently, the application period ended on March 31, 2021, as the prospects for the study are no longer available.
ETHICS STATEMENT
Consent to participate in the study will be obtained and confirmed by the participant's signature on a consent form after receiving an explanation about the study, both verbally and by provision of written documents. Furthermore, the research will be conducted with the approval of the Ethics Review Committee of St. Luke's International University (18-A010), Toyama University (C 30-60), and the Children's Support Centre of Toyama Prefecture Rehabilitation Hospital (No. 51) and comply with the CONSORT guidelines adapted to randomized controlled trials. UMIN registration number: UMIN000032623 (registered May 17, 2018).
Footnotes
ACKNOWLEDGMENTS
We would like to thank the members of the Nursing Informatics Laboratory at St. Luke's International University for their advice on the protocol. This research was supported by Grants-in-Aid for Scientific Research C (Task number: 19K11244) in the design of the study; collection, analysis, interpretation of data; and writing of the manuscript.