
Abstract
Objective
To identify the most relevant clinical characteristics of the nursing diagnosis frail elderly syndrome (FES) in hospitalized patients aged 65 or older and analyze their impact on 9-month mortality and hospital readmission.
Methods
A prospective and prognostic accuracy study was conducted in patients aged 65 or older, who were admitted to hospital more than 24 h. A consecutive convenience sampling process was used. Assessment included defining characteristics (DCs) of FES, clinical fraility scale (CFS), frail scale (FS), and 9-month mortality and hospital readmission. Statistical tests were used to verify associations between variables. Binary logistic regression analysis and area under the curve were used, to identify significant predictors for the outcomes and evaluate the prognostic accuracy of the DCs.
Findings
This study involved 150 patients. CFS scored 65 patients (43.3%, confidence interval 95% 35.2% a 51.6) as frail and proved a prognostic value of mortality at 9 month from pre-frail state (p = 0.020). The mean number of DCs for FES nursing diagnosis was 6.35 (SD = 3.14). Validated tools for measuring frailty were associated with all DCs, excepting nutritional imbalance: below body needs. The hospital readmission during the following 9 months was only statistically related to memory impairment (p = 0.07).
Conclusion
Clinical frailty scale showed good results as a predictor of mortality. The study suggests exploring including it, in clinical manifestations of elderly frail syndrome. This study found that only memory impairment defining characteristic was predictive of hospital readmission. Further research should identify other relevant and prognostic clinical manifestations.
Implication for nursing practice
These findings highlight the importance of being vigilant on cognitive decline during hospital admissions. The most prevalent and determinant DCs identified in this study indicate that clinical should focus on preserving functional and mental abilities as well as mobility.
Keywords
INTRODUCTION
As the elderly population continues to increase worldwide, it is apparent that we are entering into an era of an aging society (Ritchie & Roser, 2023). In 2020, in Spain, one of the most aged countries, the average age of hospital discharges was 59.8 years for men and 56.6 years for women. If discharges resulting from pregnancy, childbirth, and puerperium were excluded, the average age for women would rise to 61.6 years (National Institute of Statistics, 2022). In a few years, the patient profile in our hospitals will be that of individuals over the age of 65, and this trend will gradually extend worldwide. Adapting hospital protocols, procedures, and care to the needs of this patient profile will be crucial in the next decade.
In population over 65 years, the term “fraility” can be defined as a syndrome characterized by a decrease in reserve and resistance to stressors. We often use concepts that are closely related to fraility, such as vulnerability and disability, although they are not equivalent. Disability is a contextual limitation that all individuals can have throughout their lives, whereas fraility is a state of extreme vulnerability in which minimal stress can cause functional decline (Rodríguez-Mañas et al., 2013).
Detection and management of fraility constitute a pillar for health systems to care of older populations. The evidence from implementing different types of interventions for frailty suggests that it is possible to reduce its impact (Apóstolo et al., 2017). Screening frailty can provide crucial information for planning and implementing strategies to preserve functional ability and prevent adverse outcomes (Argenta et al., 2022; Lucena et al., 2019).
Regarding the detection of frailty, a systematic determination of the status, preferably conducted in community settings, emerges as the optimal approach. Nonetheless, in cases where such assessment is not accessible, its significance amplifies during hospital admission. This is because nursing professionals tailor patient care according to their distinct functional characteristics. Literature indicates the existence of over 20 diverse frailty screening measures, out of which 17 are utilized for assessing frailty within hospital settings. Each distinct assessment method is associated with a specific conceptualization of frailty (Apóstolo et al., 2017).
Frail elderly syndrome (FES) (00231) nursing diagnoses have been part of the NANDA taxonomy from 2013, and it is defined as: “A dynamic state of unstable equilibrium that affects older individuals who experience deterioration in one or more domains of health (physical, functional, psychological, or social) that increases susceptibility to adverse health effects, particularly disability” (Herdman et al., 2021). The approach from nursing to the construct of frailty emphasizes the multidimensionality of the concept and considers fraility as a pre-disability state, as it is an independent prognostic marker of mortality and poor health outcomes (Gregersen et al., 2020; Vermeiren et al., 2016).
Herdman et al. (2021) cautioned that it is critical to conduct research on which assessment indicators are more predictive for patients to present a nursing diagnosis. Given that frailty is essentially defined as a poor prognosis, particularly under further stressors, it is important to explore the predictive ability of the nursing diagnosis FES. Defining characteristics (DCs) of the nursing diagnosis FES should be able to distinguish between frailty and acute illness, that is, differentiate between older patients who are ill but have good physiological reserve and those who have poor reserve and are therefore frail.
This study aims to determinate the critical DCs of the nursing diagnosis FES in hospitalized patients aged 65 or older and examine their relationship with the presence of frailty, as measured by validated instruments, as well as their impact on 9-month mortality and readmission rates.
METHODS
Design and sample
This is a prospective study of accuracy and prognostic capacity of the DCs of the FES nursing diagnosis, and was conducted at Santa Lucia University General Hospital in the southeast of Spain.
This study included patients aged 65 or older who were admitted to hospital more than 24 h. Exclusion criteria were as follows: patients who did not sign the informed consent, patients in terminal condition (life expectancy ≤6 months), patients admitted to the ICU, and patients who, due to their cognitive state or level of Spanish, were unable to respond the questionnaire. There were included patients whose primary caregiver answered the survey.
To determine the necessary sample size a significance level of α = 0.05 (two-tailed) was assumed, a power of β = 0.8, a disease prevalence of 41.4% (Gómez Jiménez et al., 2021), and a sensitivity of the reference test of 0.58 (Smith & Jones, 2019). To detect a range of sensitivity values for the FES DCs from 0.5 to 0.7, the required sample size calculated was 150 patients.
A consecutive convenience sampling process was used. Data collection was done between April 2021 and May 2022.
Data collection
During patients’ hospital admission, some data were collected by questionnaire and other by reviewing health records. The remaining data were collected, 9 months after hospital discharge, by extracting information from the patients’ digital clinical history.
The questionnaire used for data collection was composed of three different parts: (1) sociodemographic data (age and gender), (2) clinical data (hospitalization unit, weight, height, frail scale [FS], and clinical frailty scale [CFS]), (3) data on the DCs that characterize FES, the 13 DCs presented by the NANDA-I taxonomy II: self-care deficit bathing/hygiene, (00108), decreased activity tolerance (00298), decreased cardiac output (00029), self-care deficit in dress (00109), fatigue (00093), feeding self-care deficit (00102), hopelessness (00124), and nutritional imbalance: below body needs (00002), memory impairment (00131), impaired physical mobility (00085), ambulation impairment (00088), social isolation (00053), and self-care deficit in toilet use (00110). From personal interviews with patients and/or caregivers, the presence or absence of DCs was recorded, except for: decreased cardiac output and memory impairment (which were also corroborated through the digital health record), and nutritional imbalance: below body needs, also evaluated through (BMI and calf circumference measurement).
CFS is a measure of frailty that assesses an individual's overall health status and level of vulnerability to adverse outcomes. CFS is a global measure of frailty based on the clinical judgment of the professional using available clinical information. The scale is graded from 1 to 9 (1, very fit; 2, well; 3, managing well; 4, vulnerable; 5, mildly frail; 6, moderately frail; 7, severely frail; 8, very severely frail; 9, terminally ill). This scale classifies patients as: “non-frail” for a CFS score of 1–3, “pre-frail” for a CFS score of 4, and “frail” for a CFS score of ≥5 (Rockwood et al.,2005 ).
FS consists of five self-reported questions that ask about number of diseases, fatigue, ability to climb stairs and walk, and unintentional weight loss. The questions can be administered to patients or their caregivers, and each component of the assessment is worth one point. The score ranges from 0 to 5 points, and individuals are classified as “non-frail” (score 0), “pre-frail” (score 1–2), or “frail” (score 3–5) (Morley et al., 2012).
The choice of both scales (FS and CFS) is based on their predictive power of adverse events in specific environments. (Dent et al., ; Woo et al., 2012). Moreover, both scales have demonstrated excellent results in feasibility and time to complete aspects highly valued in acute patient care settings, where busy healthcare staff need a simple and quick tool to detect frailty (Oviedo-Briones et al., 2021, 2022).
Data analysis
Data were analyzed in SPSS version 22.0. Central tendency and dispersion tools were implemented for the descriptive analysis of quantitative variables. Categorical variables were described with frequency tables (number and percentage). The Kolmogorov–Smirnov test was used to determine normality in the distribution of quantitative variables. The chi-square test or Fisher's exact test was estimated, as appropriate, to verify the association between categorical variables. The Mann–Whitney U test was used to verify the relationship between quantitative and dichotomous categorical variables, and the Kruskal–Wallis test was developed for polytomous categorical variables if the distribution was non-normal. Binary logistic regression analysis was performed to determine which DCs were independently associated with mortality and hospital readmission. An analysis using area under the curve (AUC) curves was conducted to determine the best cut-off point (number of DCs) with the best discriminative power of frailty (measured through both the CFS and FS scales). In addition, 95% confidence intervals (95% CI) were calculated. Significant differences between variables will be considered when the level of significance (p) is less than 0.05.
Ethical aspects
Participants were informed about the research and all of them signed a consent form. The study protocol was approved by the Clinical Research Ethics Committee of Areas II and VIII of the Health Service of Murcia, Spanish National Health System, on March 2021. (Approval number EO 2021-19).
FINDINGS
The sample of 150 patients showed a mean age of 78.3 years (SD = 7.81, range = 65–94). Characteristics of the sample can be seen in Table 1.
Sample characteristics.
FS classified 68 patients (45.3%, IC 95% 37.2% a 53.7%), as frail, whereas with the CFS, 65 patients (43.3%, IC 95% 35.2% a 51.6) were classified as frail. CFS identified the two most prevalent profiles of frailty as vulnerable (24%) and managing well (22%). A chi-squared test was performed to investigate the relationship between the two scales. The results showed a significant association between the FS and the CFS scores (χ 2 = 37.629, df = 1, p < 0.001)
A significant relationship was observed between the CFS score, categorized as either vulnerable or more severe, and mortality within a span of 9 months (χ 2(1) = 5.39, p = 0.020); however, there was no significant association between FS score and mortality within 9-month period (χ 2(1) = 0.684, p = 0.408).
The mean number of DCs for FES nursing diagnosis was 6.35 (SD = 3.14). The dataset consisted of 150 cases, each indicating the presence or absence of 13 DCs. The range of the data was 12, with a minimum of 0. Overall, the results suggest that the SF and CFS are associated with a range of DCs, excepting nutritional imbalance: below body needs (Table 2). The AUC was in FS 0.898 (95% CI 0.820, 0.976) and 0.889 (95% CI 0.834, 0.944) in CFS. From the cut-off value of 5 DCs was obtained the best discriminative power for the FS (sensitivity 88.2% and specificity 76.2%) and CFS (sensitivity of 89.3% and specificity of 74.7% (Figure 1)).
Regression analysis of defining characteristics associated with mortality and hospital readmission in the 0–9-month period.
p-value Pearson´s chi-square test.
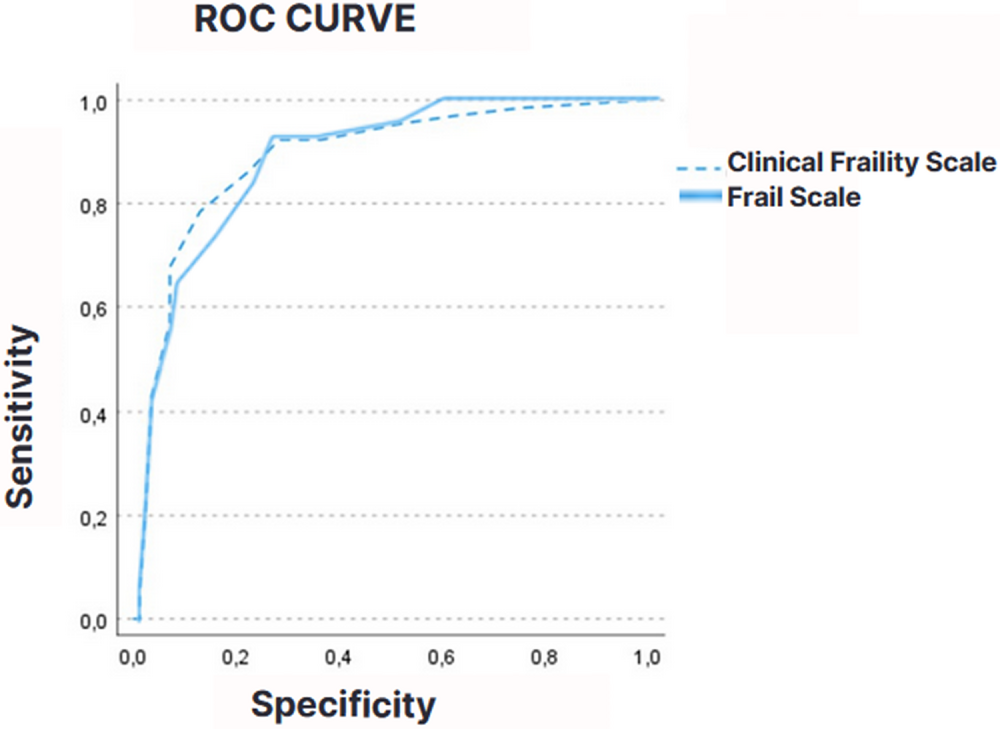
Comparing the Clinical Fraility Scale and Frail Scale through Receiver Operating Characteristics.
A significant association was found between 9-month mortality and decreased cardiac output (χ 2 = 4343, df = 1, p = 0.037) (OR = 1768, 95% CI = 1033–3026) and hopelessness (χ 2 = 3.902, df = 1, p = 0.048) (OR = 1766, 95% CI = 1008–3098) (Table 2). The Mann–Whitney U test revealed no significant association between the number of DCs and 9-month mortality (U = 1611.500, z = −1789, p = 0.074, two-tailed). A Kruskal–Wallis test estimated the number of DCs was also not related to mortality at other periods (at 1 month, after 2–3 months, and after 4–9 months), (H(3) = 3637, p = 0.303). A logistic regression model was fit to explain 9-month mortality. The final model had a correct classification rate of 79.2% and explained 11.8% of the variance (R2 Nagelkerke). The model was not significant (χ 2(12) = 6566, df = 7, p = 0.475) (Table 3).
Inferential analysis between scales (frailty scale, clinical frailty scale) and adverse events (mortality and hospital readmission in the 0–9-month period).
Note: CD 5 fatigue (00093) was eliminated in the regression analysis in step 1.
The hospital readmission during the following 9 months was only statistically related to memory impairment (χ 2 = 7104, df = 1, p = 0.008) (OR = 2.13, 95% CI = 1.20–3.77) (Table 2). The Mann–Whitney U test showed no significant difference between the variables “hospital readmission” and the number of DCs (U = 2398.00, W = 6053.00, z = −1388, p = 0.165, two-tailed). The number of DCs was also not related to hospital readmission number (0 readmissions–5 readmissions) during the following 9 months (0–5) (H(5) = 10.103, p = 0.072). Moreover, a logistic regression model was appropriate to explain the relation between DCs and hospital readmission during the following 9 months. The logistic regression analysis showed that the model significantly predicted hospital readmission, χ 2(12) = 21.405, p = 0.045. The overall classification accuracy of the model was 63.8% and explained 16.9% of the variance (R2 Nagelkerke). None of the variables were significant at any step, except for memory impairment (B = 1241, SE = 0.458, Wald = 7343, p = 0.007, OR = 3460) (Table 3).
DISCUSSION
The prevalence of frailty in our study (45.3% using FS and 43.3% using CFS) aligns with reported prevalence rates in other studies (Gómez Jiménez et al., 2021). This underscores the importance of assessing frailty in older adults, as it is a common condition in hospitalized patients aged 65 or older.
The average number of DCs for the nursing diagnosis FES was 6.35 (SD = 3.14). In general, the results suggest that the FS and CFS are associated with a range of DCs, except for nutritional imbalance: below body needs. These findings highlight the importance of considering multiple factors when assessing frailty in older adults, as other studies have similarly reported the multifactorial nature of frailty (Fried et al., 2001).
The study also examined the relationship between DCs and 9-month mortality and hospital readmission rates. A significant association was found between 9-month mortality and decreased cardiac output and hopelessness, which is consistent with previous studies that have identified these factors in frail older adults (Afilalo et al., 2014; Ge et al., 2015; Newman et al., 2001; Park & Lee, 2019). However, the logistic regression model predicting 9-month mortality was not significant, so the influence of these two DCs was not significant when more variables were introduced in the analysis. Further research is needed to explore the factors contributing to mortality. In this respect, CFS predictive ability to detect adverse events makes it a good candidate. In this study, CFS proved a prognostic value of mortality at 9 months from pre-frail state (CFS score 4 or bigger). This supports previous findings regarding the characteristics of the scale (Church et al., 2020; Wallis et al., 2015), so it could be considered to include CFS positive result as one more DCs of FES nursing diagnosis.
Interestingly, memory impairment was the only defining characteristic significantly associated with hospital readmission during the following 9 months. This finding supports the notion of a significant, negative effect of frailty on cognitive performance. This association between cognitive decline and frailty status appears to be consistent in older populations across the age spectrum (Miyamura et al., 2019; Robinson et al., 2022), affecting individual ability for health-promoting behaviors, and resulting in increased morbidity and higher hospital readmission rates among older adults (Yao et al., 2020).
In our study, the most prevalent DCs of the patients evaluated during hospitalization were those that affected the individual's mobility (decreased activity tolerance (00298), fatigue (00093), impaired physical mobility (00085), and ambulation impairment (00088)). Evidence suggests that an individualized, multicomponent exercise intervention during hospitalization could provide a significant benefit (Martínez-Velilla et al., 2019). Even simple walking stimulation enables patients to maintain their prehospitalization community mobility (Brown et al., 2016). The tandem “Exercise promotion (0200)—Exercise participation (1633)” (Argenta et al., 2022; Lucena et al., 2019) could preserve mobilization in frail older patients during acute hospitalization. The effects of these exercise transcend the area of mobility and demonstrate improvements in the functional capacity of the individual (activities of daily living) (Martínez-Velilla et al., 2019), improving results such as self-care: activities of daily living (0300), also proposed for care planning in this type of patients (Argenta et al., 2022; Lucena et al., 2019).
Cognitive decline, the only defining characteristic that was significantly associated with a negative health outcome in our sample, can be treated in hospital through interventions such as “Cognitive stimulation” (4720), but also through participation in physical exercise programs. Argenta et al. (2022) maintained that planning, adaptation to the new routine, attention, adherence, and the learning that participation in exercise programs requires, improved “Concentration (09.0004)” and other outcome measures related to the affective and cognitive areas (Martínez-Velilla et al., 2019).
Limitations
Limitations of this include the relatively small sample size and the fact that a study was conducted in a single hospital, which could limit the generalizability of the results. This study presents selection bias, as patients were not recruited randomly. The research focuses on frailty during hospitalization without taking into account the preadmission frailty classification. As a result, the study faces challenges in distinguishing between acute and chronic frail patients. The substantial number of DCs identified, which often relate more to the illness than to frailty, suggests that in a hospital setting, the diagnosis should be established using at least five DCs. This threshold limits the number of false positives and achieves acceptable specificity when the FS and CFS scales are used as a gold standard.
IMPLICATIONS FOR NURSING PRACTICE
The findings of this study have implications for nursing practice in the care of hospitalized older adults. Nursing professionals should prioritize the assessment of characteristics such as “memory impairment,” as it was associated with hospital readmission. This suggests that cognitive decline could be a crucial factor in the vulnerability of older adults and may influence their ability for self-care and adherence to medical instructions.
Early interventions during hospitalization focused on the preservation of functional competences, mobility, and mental capacities should be the focus of care management of hospitalized frail elderly.
Exercise programs appear to yield benefits across a wide range of clinical manifestations of frailty, including the most prevalent and determinant factors identified in this study.
CONCLUSIONS
The prevalence of frailty in hospitalized older adults identified in this study is significant and presumably will continue to increase in the coming years. It becomes essential to improve nursing perspective of the frailty phenomenon and the ways of identifying it.
Only one of the DCs of our sample predicts hospital readmission. Although the methodological deficiencies of this work may have led to this result, it is important to identify representative clinical indicators. The good results obtained in the CFS scale as a predictor of mortality indicate that it may be interesting to explore its inclusion as a clinical manifestation of FES nursing diagnosis, in future research.
The findings of this study support the notion that frailty and cognitive decline are closely related and may contribute to increased readmission rates in older adults. These results highlight the importance of being vigilant of key CDs in nursing diagnoses FES during hospital admissions.
Hospital care for acutely ill frail older adults should include well-dimensioned and evidence-based care strategies. Nursing taxonomies identify key interventions and outcomes for this type of patient, such as Exercise promotion (0200), Exercise participation (1633) and Cognitive stimulation (4720).
AUTHOR CONTRIBUTIONS
Conceptualization; methodology; formal analysis; data curation; writing (original draft); writing (review & editing); supervision; project administration: María T. Roldán-Chicano. Methodology; formal analysis; data curation; writing (original draft); writing (review & editing); supervision; project administration: María M. García-López, María del Carmen Martínez-Pacheco, and Javier Rodríguez-Tello.
CONFLICT OF INTEREST STATEMENT
The author declares no conflicts of interest.
FUNDING INFORMATION
The authors received no specific funding for this work.