
Abstract
Aims
To characterize the thematic foci, structure, and evolution of nursing research on clinical reasoning and judgment.
Design
Bibliometric analysis.
Methods
We used a bibliometric method to analyze 1528 articles.
Data source
We searched the Scopus bibliographic database on January 7, 2024.
Results
Through a keyword co-occurrence analysis, we found the most frequent keywords to be clinical judgment, clinical reasoning, nursing education, simulation, nursing, clinical decision-making, nursing students, nursing assessment, critical thinking, nursing diagnosis, patient safety, nurses, nursing process, clinical competence, and risk assessment. The focal themes, structure, and evolution of nursing research on clinical reasoning and judgment were revealed by keyword mapping, clustering, and time-tracking.
Conclusion
By assessing key nursing research areas, we extend the current discourse on clinical reasoning and clinical judgment for researchers, educators, and practitioners. Critical challenges must still be met by nursing professionals with regard to their use of clinical reasoning and judgment within their clinical practice. Further knowledge and comprehension of the clinical reasoning process and the development of clinical judgment must be successfully translated from research to nursing education and practice.
Implications for the profession
This study highlights the nursing knowledge gaps with regard to nurses’ use of clinical reasoning and judgment and encourages nursing educators and professionals to focus on developing nurses’ clinical reasoning and judgment with regard to their patients’ safety.
Impact
In addressing nurses’ use of clinical reasoning and judgment, and with regard to patient safety in particular, this study found that, in certain clinical settings, the use of clinical reasoning and judgment remains a challenge for nursing professionals. This study should thus have an effect on nursing academics’ research choices, on nursing educators’ teaching practices, and on nurses’ clinical practices.
Reporting method
Relevant EQUATOR guidelines have been adhered to by employing recognized bibliometric reporting methods.
Keywords
INTRODUCTION
Demonstrating clinical reasoning and clinical judgment has been acknowledged by nursing researchers, educators, and professionals to be essential competencies to be developed by nurses in facing the complexity of their work as clinicians (Itano, 1989; Jones, 1988) and as diagnosticians, especially (Ebright et al., 2003). This includes the ability of nurses to integrate foundational and advanced knowledge into their clinical reasoning and to base their clinical judgment on current and emerging evidence (American Association of Colleges of Nursing, 2020; Higgs, 2001). Clinical reasoning may be defined as a “complex process that uses cognition, metacognition, and discipline-specific knowledge to gather and analyze patient information, evaluate its significance, and weigh alternative actions” (Simmons, 2010, p. 1151). However, clinical judgment may be defined as “an interpretation or conclusion about a patient's needs, concerns, or health problems, and/or the decision to take action (or not), use or modify standard approaches, or improvise new ones as deemed appropriate by the patient's response” (Tanner, 2006, p. 204). As such, clinical judgment may be viewed as a result of clinical reasoning and may be equated to “thinking like a nurse” (Etheridge, 2007). In turn, the clinical decision-making of nurses, resulting from the soundness of their clinical judgment, has a direct effect on patient care outcomes (Manetti, 2019) and on patient safety, especially (Billings, 2019).
One may first note that the terms “clinical reasoning” and “clinical judgment” have often been used interchangeably by nursing researchers, thus generating ambiguity when cumulating and comparing research findings (Griffits et al., 2022; Victor-Chmil, 2013). Moreover, the term “critical thinking” has also been used interchangeably with both clinical reasoning and clinical judgment (Alfaro-LeFevre, 2020), thus generating even more ambiguity. One may also note that “critical thinking is an ‘umbrella term’ that includes reasoning both inside and outside of the clinical setting” (Alfaro-LeFevre, op. cit., p. 64). Thus, as our research interest lies in nurses’ reasoning inside the clinical setting, that is, in their clinical reasoning, our study excludes critical thinking at the outset.
Clinical reasoning and clinical judgment have been objects of study first and foremost in nursing education research (Calcagni et al., 2023; Mohammadi-Shahboulaghi et al., 2021; Thompson & Stapley, 2011). Indeed, researchers have sought to uncover the most effective educational interventions, techniques, and tools for developing nursing students’—and nurses’—clinical reasoning and clinical judgment (Kuiper, 2004; Lasater, 2007b; Maheu-Cadotte et al., 2023; Victor et al., 2017), including the ability to effectively monitor and surveil “at-risk” or deteriorating patients (Levett-Jones et al., 2010). In this regard, experiential learning through the use of simulation methods meant to replicate clinical scenarios has been the dominant educational approach (Decker et al., 2008; Kow, 2024; Lasater, 2007a; Reinhardt et al., 2019), often combined with debriefing techniques meant to structure and guide the students’ and nurses’ performance self-appraisal (Decker et al., 2013; Dreifuerst, 2012; Al Sabei & Lasater, 2016). Measurement scales have also been developed and validated by researchers as means to assess nursing students’ and nurses’ clinical reasoning and clinical judgment competencies and skills in various simulated or clinical care settings (Bae et al., 2023; Bambini et al., 2009; Facione et al., 1994).
In clinical nursing research, the clinical reasoning and clinical judgment processes, characteristics, and performance of nurses have been observed, described, assessed, and compared in various clinical care settings (Callihan et al., 2023; Gerber et al., 2015; Hosseinzadeh et al., 2022; McCarthy, 2003; Wøien & Bjørk, 2013). This includes “think-aloud” studies done within patient monitoring and surveillance interventions (Johnsen et al., 2016; Lee et al., 2016). Researchers have especially examined the clinical reasoning and clinical judgment demonstrated by nurses in their clinical practice as it relates to adverse events and patient safety (Brier et al., 2015; Domm et al., 2021; Dresser et al., 2023; Lavoie et al., 2020; Rohde & Domm, 2018; Stannard et al., 1996; Wagner et al., 2020). Moreover, nurses’ clinical reasoning and clinical judgment in practice have been used by researchers as models, benchmarks, and baselines in nursing informatics studies of clinical decision-support systems, early warning systems, and other automated monitoring and surveillance systems, as well as artificial intelligence (AI)-based and machine learning–based predictive algorithms designed to support nurses in their patient monitoring and surveillance interventions (Chin-Yee & Upshur, 2019; der Cingel et al., 2021; Lovegrove et al., 2023; O'Neill et al., 2005; Seney et al., 2023; Yang et al., 2023). In particular, a number of intervention studies and field investigations have examined the extent to which and the manner by which health information technologies (HITs) and AI-based technologies may be mobilized in support of nursing students’ and practicing nurses’ clinical reasoning and clinical judgment (Hah & Goldin, 2021; Raymond et al., 2022; Saban & Dubovi, 2024; Von Gerich et al., 2022).
As nurses are deemed to be “the last line of defense” for their patients (Joy, 2009), and as they must face an “ever-widening experience-complexity gap” in acute and critical care settings (Delgado, 2021), we require further contextualization, characterization, and comprehension of the nature, extent, and effectiveness of nurses’ use of clinical reasoning and clinical judgment, and especially of the effects of such use on patient safety (Calcagni et al., 2023; Cappelletti et al., 2014; Connor et al., 2023; Cunha et al., 2022; Holder, 2018). An initial step in obtaining such comprehension may be taken by analyzing the corpus of nursing literature on clinical reasoning and clinical judgment and assessing the field's key areas to extend and enrich the discourse for researchers, educators, and practitioners (Sherwood et al., 2023). Given the preceding considerations, and by means of a bibliometric analysis, this study has the following objectives: identification and characterization of the most important articles, authors, journals, research institutions, and countries in nursing research with regard to clinical reasoning and clinical judgment; identification and characterization of the thematic structure of nursing research with regard to clinical reasoning and clinical judgment; identification and characterization of the thematic evolution of nursing research with regard to clinical reasoning and clinical judgment.
In attaining these objectives, we contribute to nursing research in three ways. First, we fill a knowledge gap in the nursing literature with regard to the current status and evolution of a nursing research domain that has important implications for nursing practice and for nursing professionals. Second, through an analysis of the bibliometric data, we provide a broader comprehension of nurses’ clinical reasoning and clinical judgment within their clinical practice and nursing process, and most importantly as this practice and process are meant to ensure their patients’ safety. Third, by providing nursing researchers with a more systemic, thematic, and dynamic perspective of clinical reasoning and clinical judgment over the last 35 years, the study's findings allow us to highlight, interrelate, and integrate key research areas and provide future research directions.
METHODS
By means of content and citation analyses of scientific publications, bibliometric methods aim to identify streams of research literature within a general or specialized subject area, such as the nursing research stream on clinical reasoning and clinical judgment in this case (Ellegaard & Wallin, 2015). Although literature review methods may be employed as an alternative to search, organize, and synthesize scientific publications in a particular research stream, the main advantage of bibliometric methods, in addition to their systematicity and their transparency, lies in their ability to unveil the structural, relational, and dynamic aspects of emerging or established subject areas (Unal & Teskereci, 2022). This type of study does not require ethical approval.
Identification and selection of the documents
The Scopus bibliographical database was queried on January 7, 2024, with the following keyword syntax to be found in the documents’ title, keywords, and/or abstract: (“nurse” OR “nurses” OR “nursing”) AND (“clinical reasoning” OR “clinical judgement” OR “clinical judgment”). This database encompasses all of the peer-reviewed nursing journals listed in the Journal Citation Report (Baas et al., 2020). Moreover, when compared to other databases such as PubMed, Web of Science, and Cinahl, Scopus is more comprehensive for subject areas related to health care (Pranckuté, 2021). As shown in Figure 1, the 2475 documents thus found were further limited to documents whose subject area is “nursing” and whose language is “English.” Documents were then selected on the basis of the document's type being either an “article” or a “review” (thus excluding “conference paper,” “book chapter,” and other types). A final selection was made by removing four documents whose years of publication ranged from 1973 to 1984. The selection process thus provided us with data for our bibliometric analysis from 1528 nursing research publications in total. In addition to the citation and bibliographical information, the data include the keywords, abstract, references, and funding details for each publication.
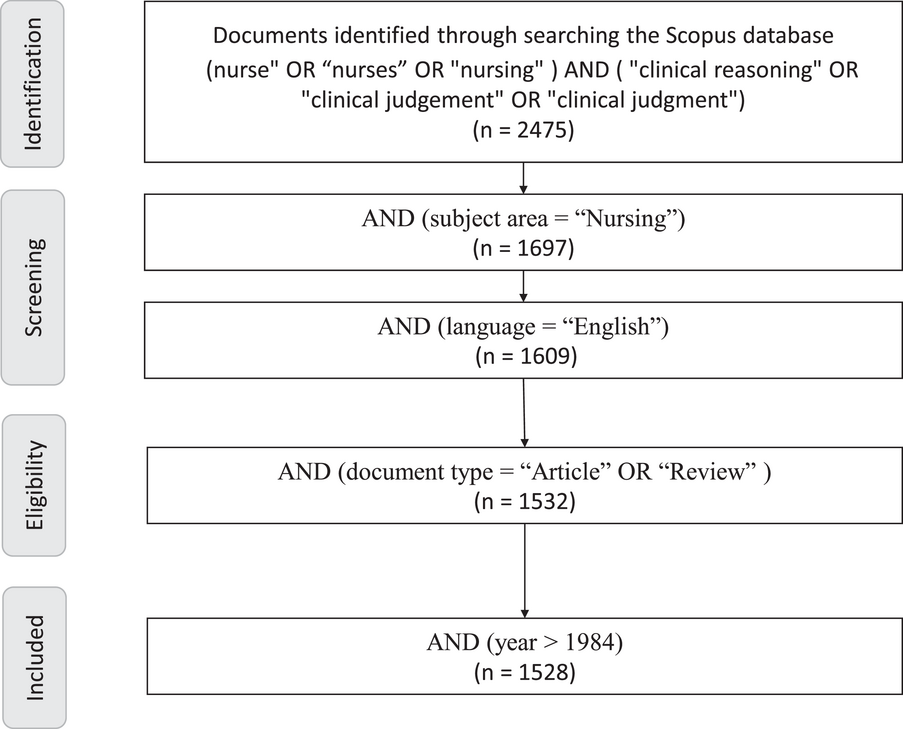
Flow diagram of the document selection process.
Bibliometric data analysis
The visualization and analysis of the collected bibliometric data were done by means of the VOSviewer (van Eck & Waltman, 2010) and Bibliometrix (Aria & Cuccurullo, 2017) application software. Note also that we employed the “author keywords” (rather than “keywords plus”) throughout the analysis, as author keywords represent a document's content in a more comprehensive manner and in a manner more unique to the nursing research stream and the nursing discipline (Tripathi et al., 2018).
RESULTS
A total of 1528 nursing research and review articles were analyzed. The articles were authored by 4023 different researchers, with 3 co-authors on average per article, 19% of the documents being single-authored, and 11% being international co-authorships. These documents comprise 2694 author keywords in total. There were a total of 41,009 references, with 19 citations on average per article. As shown in Figure 2, the number of articles published per year follows a rising trend over the past 35 years, that is, a 3% annual growth rate from 1985 (3 articles) to 2023 (166 articles). The breakdown of the articles in terms of research design is found in Table 1, a majority being either a simulation (24%), intervention (16%), survey (8%), or cross-sectional (7%) study.
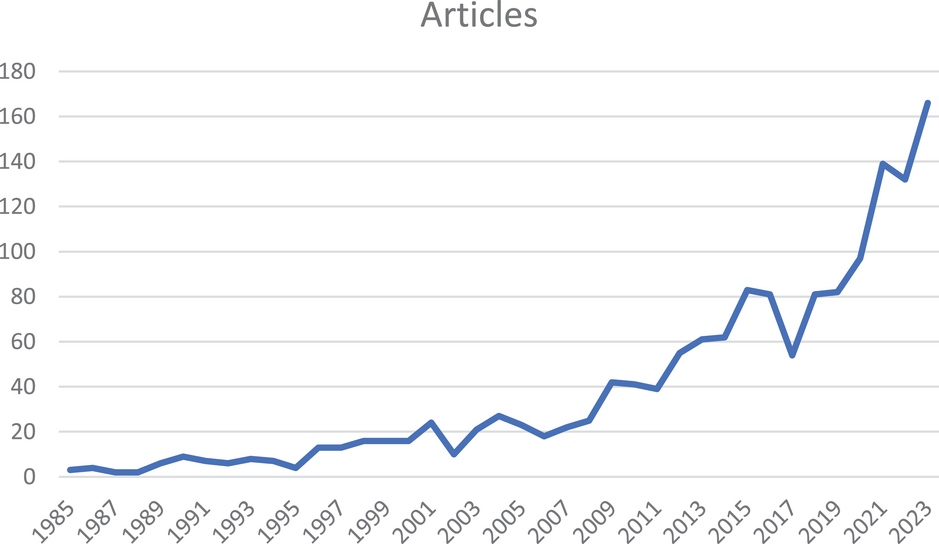
Number of articles published per year.
Breakdown of the 1528 articles by research design.
Descriptive analysis
The 20 most cited nursing research articles on clinical reasoning and clinical judgment are presented in Table 2, with the top 9 (with more than 250 citations) being Dreifuerst (2009), Facione et al. (1994), Gould et al. (2001), Pancorbo-Hidalgo et al. (2006), Lasater (2007a), Lasater (2007b), Tanner (2006), Tanner et al. (1993), and Levett-Jones et al. (2010). Also shown in Table 2 are the most cited journals, the top 7 (with more than 1000 citations) being the Journal of Advanced Nursing, Nurse Education Today, Journal of Clinical Nursing, Journal of Nursing Education, Clinical Simulation in Nursing, Nurse Education in Practice, and Nursing Education Perspectives. Most cited authors are presented in Table 3, with the top 5 (with more than 400 citations) being Lasater, Levett-Jones, Thompson, Nielsen, and Lavoie. Also presented in Table 3 are the most productive nursing research institutions with regard to clinical reasoning and clinical judgment, the top 5 (with 34 articles or more) being Université de Montréal, Oregon Health and Science University, Federal University of Ceára, Universidade de São Paulo, and Villanova University. As to the most productive countries, the top 5 (with more than 275 articles) are the United States, Australia, Brazil, the United Kingdom, and Canada.
Top 15 cited articles and journals.
Abbreviations: NA, number of articles; NC, number of citations.
Top 15 cited authors and 15 most productive research institutions and countries.
Abbreviations: NA, number of articles; NC, number of citations.
Thematic structure of nursing research on clinical reasoning and clinical judgment
The thematic structure of the nursing research stream on clinical reasoning and clinical judgment may be first uncovered through a co-occurrence analysis of the author keywords found in the 1145 articles. The 25 most frequently occurring keywords are as follows: clinical judgment (243 occurrences), clinical reasoning (218), nursing education (217), simulation (157), nursing (148), clinical decision-making (124), nursing students (123), nursing assessment (65), critical thinking (61), nursing diagnosis (51), patient safety (38), nurses (35), patient deterioration (27), nursing process (25), clinical competence (23), risk assessment (23), debriefing (22), qualitative research (21), pressure ulcer (19), reflection (18), high-fidelity simulation (17), learning (17), nursing practice (16), evidence-based practice (15), and systematic review (15). As shown in Figure 3, a network mapping of the author keywords provides a visualization of the strength of the co-occurrence links between keywords, that is, the extent to which the two keywords appear in the same articles. Furthermore, a clustering of the author keywords identifies distinct groups of keywords, wherein intragroup co-occurrences are stronger than intergroup co-occurrences. In Figure 3, the thickness of the connections between keywords is proportional to the number of co-occurrences between the two. Note also that VOSviewer combines networking and clustering algorithms to regroup author keywords into an optimal number of clusters. Each cluster is color-coded to identify keywords as being part of the same cluster. Here, the primary cluster (red) regroups nine keywords: clinical judgment, clinical decision-making, evidence-based practice, nursing, nursing assessment, nursing diagnosis, nursing process, pressure ulcer, and risk assessment. A second group (green) includes five keywords: clinical reasoning, learning, nursing education, nursing students, and systematic review. A third group (blue) also includes five keywords: debriefing, patient deterioration, patient safety, reflection, and simulation. A fourth cluster (yellow) regroups three keywords: clinical competence, nurses, and qualitative research. A fifth group (purple) includes two keywords: critical thinking and nursing practice.
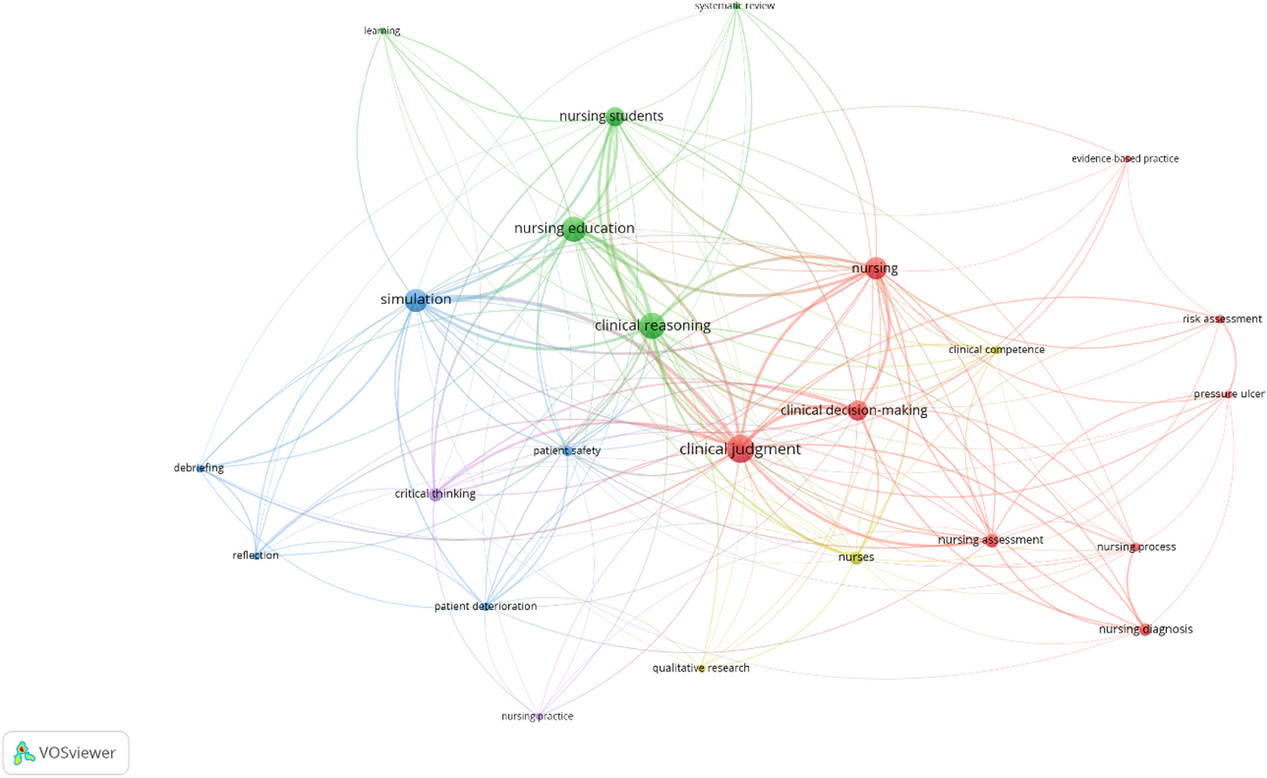
Co-occurrence analysis of most frequently occurring author keywords.
As seen in Figure 4, a bidimensional mapping of author keyword clusters by degree of relevance (centrality) and degree of development (density) provides us with a thematic typology of the nursing research stream as it concerns clinical reasoning and clinical judgment. Low-density/Low-centrality keyword clusters are typified as “declining or emerging” themes, high-density/high-centrality clusters as “motor” themes, high-density/low-centrality clusters as “niche” themes, and low-density/high-centrality clusters as “basic” themes. Here, the nursing research stream is structured into four themes. There first appears one emerging theme, focusing on nursing diagnosis, within the nursing process and nursing care. However, the lone niche theme concerns risk assessment and pressure ulcers in particular. There appears to be a single-motor theme centered on nursing education, nursing students, and simulation. However, the one basic theme relates clinical reasoning to clinical judgment, within nursing. Note also that the “patient safety” keyword does not appear in any of these research themes.
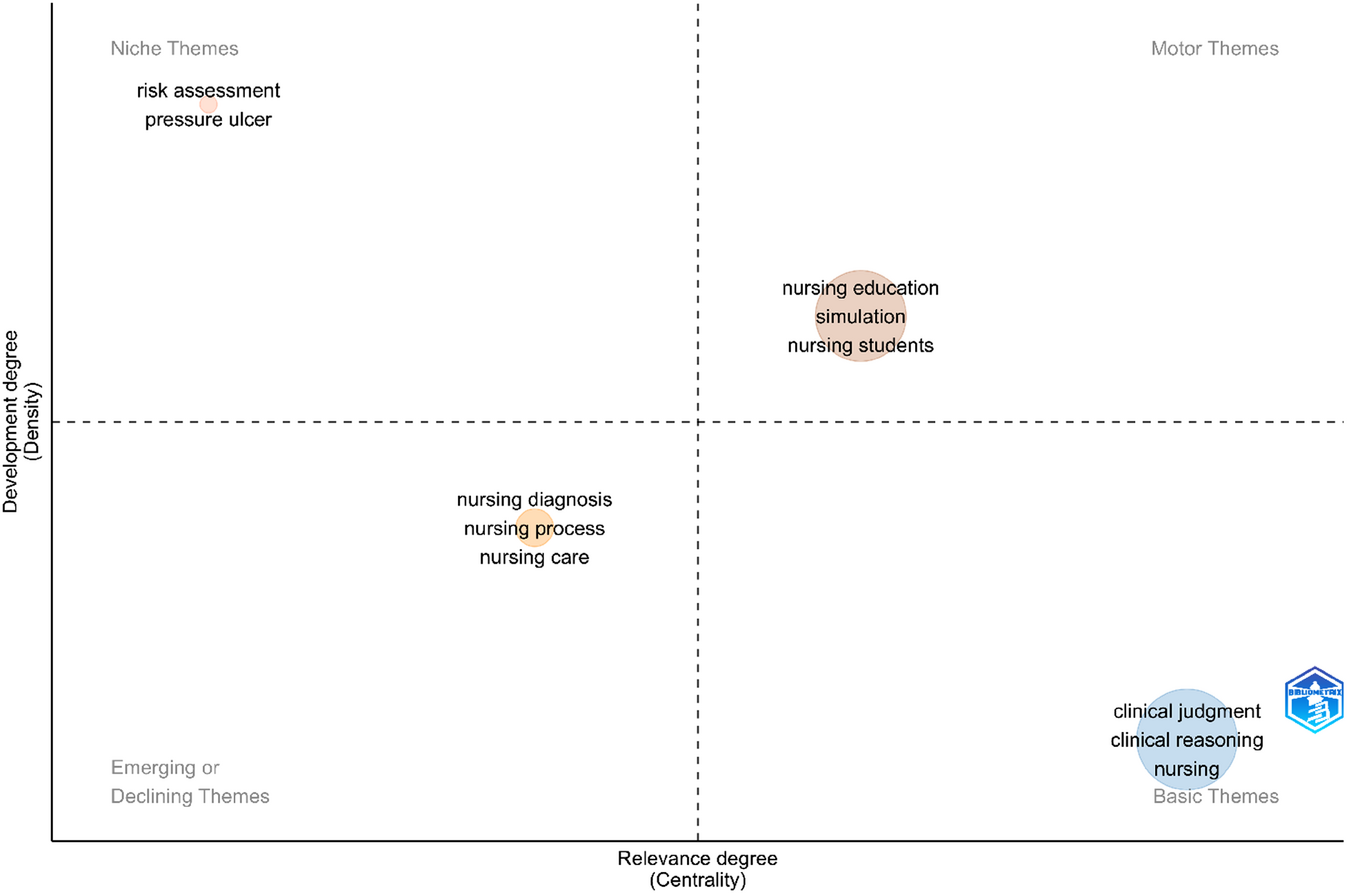
Thematic map of nursing research on clinical reasoning and clinical judgment.
Thematic evolution of nursing research on clinical reasoning and clinical judgment
The bibliometric analysis allows us to visualize the thematic evolution of nursing research on clinical reasoning and clinical judgment during the last 35 years, and to do so through three time-periods (1985–2010, 2011–2017, and 2018–2024). As seen in Figure 5, the central themes for each period are identified; also identified are the thematic correlations between two time-periods. Here, the size of a keyword block is proportional to its importance (number of occurrences) within a time-period, whereas the position of the keyword reflects its thematic distance (number of co-occurrences) from other keywords within the same period. Moreover, the thickness of the gray lines that link two author keywords across consecutive time-periods is proportional to the strength of the correlation between the keywords’ importance.
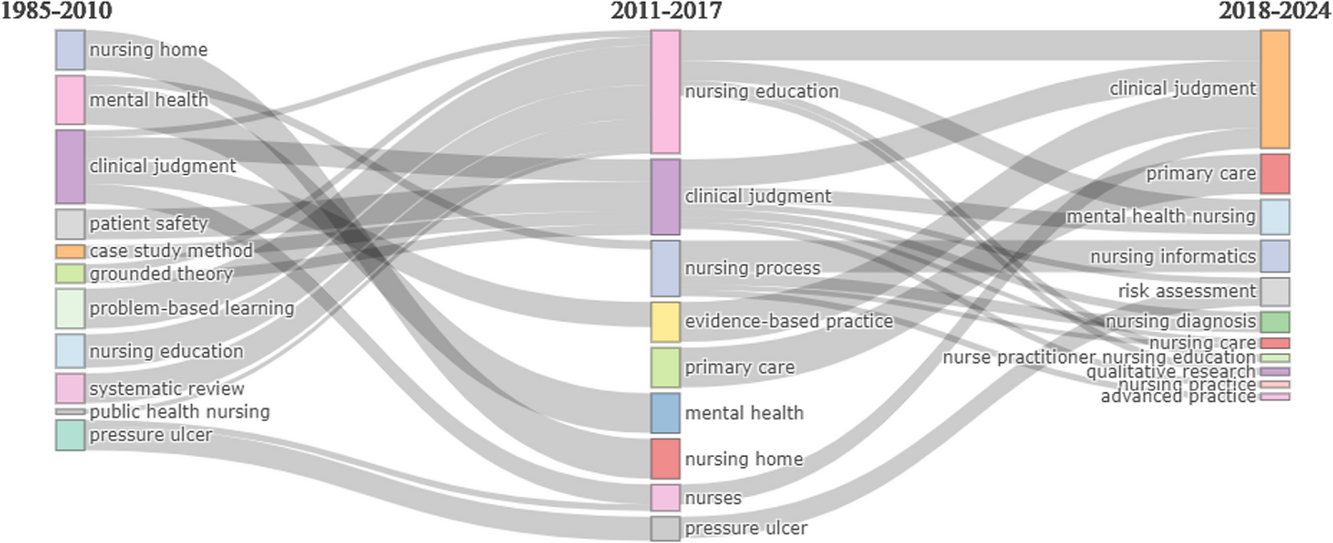
Thematic historiography of nursing research on clinical reasoning and clinical judgment.
Returning to Figure 5, one first notes that clinical judgment and nursing education, in relation to patient safety, clearly emerged as themes for nursing research in the initial period. Clinical judgment maintained its importance in the second time-period, whereas nursing education took greater importance. New themes that emerged during this period in relation to clinical judgment and nursing education include the nursing process, nursing homes, primary care, and evidence-based practice. Clinical judgment kept its most important place in the third time-period; however, the “nursing education” theme disappeared save for advanced nursing education. Furthermore, the more recently important themes to emerge in relation to clinical judgment, risk assessment, and nursing diagnosis included nursing informatics and mental health nursing. Finally, in contrast to the “clinical judgment” theme, the “clinical reasoning” theme did not surface in any of the three time-periods, even though it is found above to be a “basic” nursing research theme (cf., Figure 4). The same can be said for the absence of the “simulation” theme, although it is found above to be a “motor” theme.
To complement the preceding analysis, a visualization of the thematic “hotspots” of nursing research on clinical reasoning and clinical judgment may be obtained by examining the keyword “citation bursts” appearing in different time-periods over the last fifteen years. As seen in Figure 6, the top 15 keyword citation bursts are each characterized by their strength (frequency of occurrence of the keyword) and by their duration (time-period during which the keyword occurred most frequently). Thus, the most recent research hotspots to have emerged (in the 2019–2023 time-period) include, by order of importance, “clinical reasoning,” “nursing students,” and “nursing diagnosis.” In an earlier time-period (2017–2021), the nursing research themes to have emerged were “clinical judgment,” “nursing education,” “simulation,” “patient safety,” and “patient deterioration.” For the 2012–2018 time-period, the hotspots were “clinical decision-making” and “nursing assessment.” However, the earliest themes to emerge (2009–2016) were “critical thinking” and “risk assessment.” Finally, the appearance of the “clinical reasoning” and “simulation” themes as thematic hotspots only in more recent and shorter time-periods would explain their absence from the overall thematic evolution visualized above (cf., Figure 5).
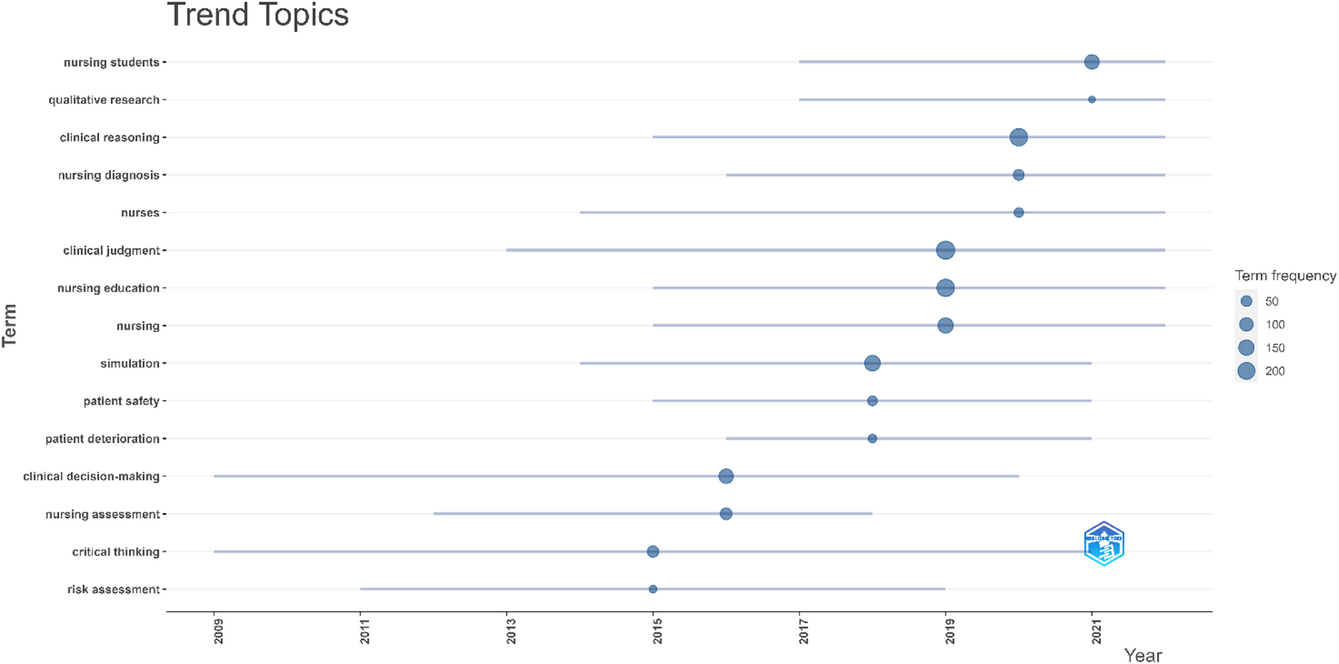
Top 15 keyword citation bursts from 2009 to 2023.
DISCUSSION
This study's findings are discussed in view of the research aims that guided the bibliometric analysis of nursing research on clinical reasoning and clinical judgment. The first finding is that both the development of nurses’ clinical reasoning and clinical judgment competencies and the use of these competencies in nursing practice have become foundational and enduring research themes of the nursing discipline over the last 35 years. Throughout this period, however, researchers have placed emphasis on clinical judgment rather than clinical reasoning and on developing the clinical judgment of nursing students rather than practicing nurses. Now, this remains somewhat paradoxical, given that clinical judgment was deemed early on to be the end-result of the clinical reasoning process (El Hussein et al., 2022). It is only in the last 10 years that clinical reasoning has come to the fore, as researchers seek to assess and explain nurses’ clinical performance through their clinical reasoning capacity. In turn, nursing educators seek to develop nursing students’ clinical reasoning capacity, particularly with regard to patient safety and mainly by simulating patient deterioration situations.
Another important finding is that nursing researchers have examined clinical reasoning and clinical judgment through an “evidence-based” view of nursing practice. That is, the clinical reasoning process has been observed and evaluated for effectiveness on the basis of the foundational and advanced knowledge mobilized (or not) by nursing students and nurses. In similar fashion, the clinical judgment of nursing students and nurses has been developed and assessed for soundness to the extent that their clinical decisions are based (or not) on current and emerging evidence. Thus, demonstrating clinical reasoning and clinical judgment may be viewed as “core” competencies for the practice of evidence-based nursing.
A third finding is that nursing research on clinical reasoning and clinical judgment has focused on two aspects of the nursing process and practice, both related to patient safety, namely, patient assessment and diagnosis. This confirms that effective clinical reasoning and sound clinical judgment enable nurses to fully assess their patients, and the risk of patient deterioration in particular, and to correctly diagnose their patients’ physical and mental condition in the course of their monitoring and surveillance interventions. Again, nurses’ use of clinical reasoning and clinical judgment is seen to be the key success factor for their clinical decision-making, as well as the main guarantor of their patients’ safety.
A last finding regards an emerging trend in nursing informatics research with regard to HIT, AI, and machine learning–based support of nursing students’ and nurses’ clinical reasoning process, and in their role as therapeutic experts (e.g., medication adjustment decisions) and as diagnosis experts (e.g., patient referral decisions). Moreover, this research has been reliant upon the clinical judgment, expertise, and experience of nurses as the foundation upon which HIT and AI-based nursing applications are developed and as the benchmark upon which these systems are evaluated.
In line with its research aims, this study allowed us to identify and characterize the key areas of the nursing research stream on clinical reasoning and clinical judgment, as well as the thematic structure and dynamics of this research corpus. This study thus contributes to nursing theory and practice by filling a knowledge gap in a subject area that is critical to the advancement of nursing as an academic discipline and as a profession. We have thus obtained results and generated findings from our bibliometric analysis that should be of importance and interest to nursing researchers, educators, and practitioners. Moreover, this study has certain implications for future nursing studies of clinical reasoning and clinical judgment.
Implications for nursing research
Twenty years after the Institute of Medicine's report on Patient Safety: Achieving a New Standard for Care (Institute of Medicine, 2004), the threats to patient safety, and failure to rescue in particular, are still current issues in the clinical practice of nurses (Doyon & Raymond, 2024). Indeed, nursing failures with regard to patient are basically characterized as failure to recognize a patient's deteriorating condition, failure to relay information on such deterioration, and failure to react in timely and appropriate fashion (Burke et al., 2022). Now, the inability of nurses to make effective use of clinical reasoning and to make sound clinical judgments when assessing, monitoring, and surveilling their patients may be surmised as a root cause of these failures (Al-Moteri et al., 2019), given the patient safety aims of nursing education with regard to clinical reasoning and clinical judgment (Fisher & King, 2013). Thus appears a need to better evaluate the clinical reasoning and clinical judgment competencies of nurses as they affect patient safety outcomes, and a need to do so in the nursing practice context (in the “real world”) rather than only in the nursing education context (through simulation).
In facing these remaining research questions and challenges, nursing researchers may use our bibliometric analysis as a starting guide or map in their future investigations, conceptualization and operationalization of clinical reasoning, and clinical judgment. A first question that should be the subject of empirical investigation lies in translating our current knowledge of nurses’ actual use of clinical reasoning and clinical judgment within their clinical nursing practice, that is, in identifying the extent to which these practices are based on effective clinical reasoning and sound clinical judgment. And in doing so, researchers (as well as nursing educators) should put the emphasis on a clinical reasoning process founded upon the notion of vigilance, that is, upon nurses’ careful and mindful monitoring and surveillance of their patients (“what is”), upon their assessment of the risks and anticipation of the threats to their patients’ safety (“what might be”), and upon their readiness to respond appropriately to minimize such risks and counter such threats (Meyer & Lavin, 2005).
A second question lies in the enabling power of HIT and AI with regard to nurses’ clinical reasoning and clinical judgment competencies. However, technology is not a “substitute” for effective reasoning and sound judgment in nurses’ early recognition, communication, and reaction to complications and patient deterioration (McGaughey et al., 2017). Rather, the use of technology enhances nurses’ ability to integrate advanced clinical knowledge into their reasoning and to base their judgment on emerging clinical evidence. Thus, more empirical investigations are needed, including design science and simulation studies, of the extent to which and the manner in which HIT-based systems (such as early warning systems and clinical decision-support systems) as well as AI-based technologies (such as machine learning and computer vision) may enable nurses’ clinical reasoning process as well as improve their clinical judgment and decision-making.
A final research question pertains to care settings other than acute, emergency, and critical care in which the clinical reasoning and clinical judgment of nurses should be further investigated. Indeed, studies done in chronic care, nursing home care, and mental healthcare settings have begun to emerge. Nonetheless, given demographic and population healthcare trends as well as the recent Covid-19 pandemic and rising patient safety issues in these nursing care settings, more studies are needed in order to further contextualize and better anchor nurses’ and nursing students’ clinical reasoning and clinical judgment within the nursing care process.
Implications for nursing practice
Beyond its implications for nursing researchers and educators, this study may also have implications for practicing nurses. First, given the increasing importance of clinical reasoning and clinical judgment for patient safety outcomes, the challenge for experienced nurses is to continuously improve the effectiveness of their reasoning and the soundness of their judgment, and to do so as patient cases keep increasing in complexity (e.g., chronicity, multimorbidities, polypharmacy, and aging). Second, given the increasing shift to a more “evidence-based” nursing practice, notably the necessity to improve clinical assessment skills, to use recommended tools that improve clinical assessment, such as the EWS score, to develop analytical reasoning, and to be attentive to the presence of cognitive biases. Thus, nurses must realize that this shift necessitates the integration of evidence-based practices within their clinical reasoning process. Third, in order to enable the continuous improvement needed of their clinical reasoning and judgment, practicing nurses must prepare themselves to experiment with and use HIT and AI-based technologies in their clinical decision-making. In addition, this should include nursing care in settings other than acute, emergency, and critical care settings such as nursing home care.
LIMITATIONS AND CONCLUSION
This study shows two limitations that are common to bibliometric analyses. First, notwithstanding Scopus’ comprehensiveness with regard to nursing research, alternative bibliographic databases such as Web of Science could have been searched instead. Second, there is the possibility of a publication bias, as we only analyzed English-language articles published in recognized peer-reviewed scientific journals.
Despite these limitations, this bibliometric analysis allowed us to identify and characterize the thematic foci, structure, and evolution of the nursing research stream on clinical reasoning and clinical judgment. By assessing in such manner critical areas of the nursing research field, this study has extended and enriched the current discourse on clinical reasoning and clinical judgment for nursing researchers, educators, and practitioners. Critical challenges still have to be met by nurses, however, especially with regard to the consequences for patient safety of their effective use of clinical reasoning and the soundness of their clinical judgment. Thus, deeper knowledge and further understanding of nurses’ clinical reasoning and clinical judgment should eventually be translated from nursing research to nurses’ and nursing students’ clinical practice.
AUTHOR CONTRIBUTIONS
Both authors contributed equally to all phases of the study.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
FUNDING INFORMATION
None.
DATA AVAILABILITY STATEMENT
Bibliometric data are available from the authors upon reasonable request.
ETHICS STATEMENT
None.