
Abstract
Although several studies show that self–esteem varies according to neighborhood context, few have directly examined potential mediators of this association. In this paper, we use longitudinal survey data from the Welfare, Children, and Families project (1999, 2001) to examine the association between perceived neighborhood disorder and self–esteem among low–income urban women with children in Boston, Chicago, and San Antonio, testing for city heterogeneity. Building on social disorganization theory and previous research, we examine the mediating influence of social support. Our longitudinal models show that higher levels of disorder at baseline are associated with lower levels of social support and self–esteem. We also observe that increases in disorder over the study period are associated with concurrent losses in social support and self–esteem. Our mediation analyses suggest that perceived neighborhood disorder may undermine self–esteem by limiting opportunities for social support. Reducing signs and perceptions of disorder by improving the social and physical landscapes of neighborhoods may uniquely contribute to self–worth of low–income urban women with children.
Desorden, Apoyo Social y Auto–Estima en Barrios: Evidencia de una Muestra de Mujeres de Bajos Ingresos en Tres Ciudades
Resumen
Aunque varios estudios muestran que la auto–estima varía de acuerdo al contexto del barrio, pocos han examinado directamente los mecanismos o variables mediadoras potenciales en esta asociación. En este artículo usamos una encuesta longitudinal del proyecto Welfare, Children and Families (1999, 2001) para examinar la asociación entre la percepción de desorden en el barrio y la auto–estima en mujeres y niños de bajos ingresos en Boston, Chicago y San Antonio, tomando en cuenta la heterogeneidad de la ciudad. A partir de la teoría de la desorganización social y de investigación previa, examinamos el efecto mediador del apoyo social. Nuestros modelos longitudinales muestran que los niveles más altos de desorden en la línea de base están asociados con menores niveles de apoyo social y de auto–estima. También observamos que aumentos en desorden durante el periodo de estudio están asociados simultáneamente con reducción del apoyo social y de la auto–estima. Nuestro estudio de la mediación sugiere que la percepción de desorden en el barrio podría disminuir la auto–estima al limitar las oportunidades de apoyo social. La reducción de las señales y percepciones de desorden a través de la mejora del medio físico y social de los barrios podrían contribuir de manera importante a la mejora de la auto–estima de mujeres y niños de bajos ingresos en ciudades.
Introduction
Does self–esteem−the positive or negative evaluation of the self as an object−vary according to neighborhood context? Several cross–sectional studies (Bámaca et al. 2005; Behnke et al. 2011; Haney 2007; Paschall and Hubbard 1998; Prelow et al. 2006; Turley 2003; Wiltfang and Scarbecz 1990) and two longitudinal studies (McMahon et al. 2011; Pals and Kaplan 2013) suggests that it does. Overall, this body of work indicates that residents of more disadvantaged neighborhoods tend to report lower levels of self–esteem than residents of more advantaged communities (see Drukker et al. 2003; Ewart and Suchday 2002, and Turley 2002 for exceptions). This general pattern is remarkably consistent across objective and subjective indicators of neighborhood context, including Census–based measures of neighborhood social structure (neighborhood–level income and poverty) and residents’ perceptions of neighborhood disorder (physical and social problems in the neighborhood).
Although previous studies have made significant contributions to our understanding of neighborhood contextual variations in self–esteem, researchers have only begun to explain these patterns. If residents of disadvantaged neighborhoods tend to report lower levels of self–esteem, why do they? To the best of our knowledge, Haney (2007) is the first to empirically investigate this fundamental question. Using data collected from a sample of adults living in Los Angeles and Boston, Haney (2007) shows that the inverse association between neighborhood–level poverty and self–esteem is fully mediated by perceptions of neighborhood disorder (perceptions of problems with city services such as street cleaning or garbage collection, housing and property not being kept up, crime, and vandalism). Extending this process, Haney (2007) also finds that the inverse association between perceived neighborhood disorder and self–esteem is explained by poor physical health. According to Haney (2007:989), “…one of the channels by which this change in self–esteem may happen is through compounding health problems associated with the stress of residing in a blighted neighborhood.”
Although Haney's (2007) work is informative and important, he acknowledges that “…research should begin unraveling more of the mechanisms by which impoverished and deteriorating surroundings are internalized and incorporated into an individual's self–image” (p. 992). Aside from contributing to poor physical health, why might perceptions of neighborhood disorder undermine self–esteem? Prelow et al. (2006:514) offer one promising possibility: “…ecological risk may reduce self–esteem by disrupting relationships that could promote positive self–evaluations…” Following the suggestion of Prelow et al. (2006), we use longitudinal survey data collected from a sample of low–income women with children living in low–income neighborhoods in Boston, Chicago, and San Antonio to test whether the association between perceived neighborhood disorder and self–esteem is mediated by social support. To our knowledge, no studies have formally tested this model.
In the pages that follow, we present our rationale for focusing on low–income urban women with children, set our foundation in urban sociological theory, and develop each link in our theoretical model. After describing our data, measures, and statistical procedures, we summarize the key results of our mediation analyses. We end with a discussion of the implications and limitations of our work.
Theoretical Background
Low–Income Urban Women with Children
There are several reasons to focus on low–income urban women with children. The first reason is theoretical. In addition to the Welfare, Children, and Families (WCF) Project, a number of influential studies (e.g., The Urban Poverty and Family Life Study, The Multi–City Study of Urban Inequality, The Fragile Families and Child Well–Being Study, and Moving to Opportunity for Fair Housing) have recognized the unique vulnerabilities of low–income urban families. Because of their disadvantaged position within several systems of social stratification (e.g., gender, race, and class), low–income urban women are disproportionately exposed to impoverished neighborhoods and conditions of disorder (Ross and Mirowsky 2001; Skogan 1990). The presence of children may also multiply the fears and risks associated with living in a dangerous urban community (Skogan 1990). The second reason is methodological. Because most Americans are not exposed to neighborhoods where crime and decay are problems, we look to disadvantaged urban samples to maximize variation on the undesirable end of disorder scales (Hill et al. 2005). The third reason is related to policy. If we are going to solve the problems of urban poverty and neighborhood disadvantage, it makes sense to direct our attention to the lives of those who are most likely to experience and suffer from these conditions. In the end, neighborhood policy discussions must be based on actual studies of the urban poor.
Foundations in Urban Sociological Theory
The idea that perceptions of neighborhood disorder might somehow undermine social support flows from several urban sociological theories, including social disorganization, collective efficacy, and broken windows (Faris and Dunham 1939; Massey and Denton 1993; Sampson 2013; Shaw and McKay 1942; Skogan 1990; Wilson 1987; Wilson and Kelling 1982). For nearly three quarters of a century, these theories have described in great detail the processes through which disadvantaged urban neighborhoods might weaken or disrupt the social fabric of communities. In the language of these theorists, neighborhood characteristics like disorder and crime promote “social withdrawal,” “social isolation,” and the erosion of “social ties,” “social cohesion,” and “informal social control” by contributing to feelings of “fear,” “anger,” “distrust,” and “demoralization.” Although explicit connections are rare, indicators like “social ties” and “social cohesion” are at least conceptually related to social support (Cullen 1994).
Perceptions of Neighborhood Disorder
Neighborhood disorder refers to a range of social and physical conditions that indicate the breakdown of social control in the community (Hill and Maimon 2013; Ross and Mirowsky 1999; Sampson 2013; Skogan 1990). Signs of social disorder include people hanging around on the streets, open alcohol consumption and drug use, prostitution, and other forms of criminal activity. Indicators of physical disorder include the presence of abandoned buildings, vandalism, graffiti, garbage, and ambient noise. Although these conditions can be measured independently of neighborhood residents through, for example, systematic social observations (i.e., researchers traveling through neighborhoods, filming and recording social activities and physical features; Raudenbush 2003; Sampson 2013), we emphasize perceptions of neighborhood disorder to directly assess the ways in which residents interpret and experience their neighborhoods (Aneshensel and Sucoff 1996; Haney 2007; Hill and Maimon 2013; Ross and Mirowsky 1999). According to Haney (2007:989), “…one of the ways that residing in an impoverished neighborhood is internalized and translated into self–esteem is through the way a person perceives the physical and social disorder of their neighborhood.” It is our view that disadvantaged neighborhood environments are only relevant to the self–concept when residents perceive them to be unpredictable, disreputable, or dangerous. We will argue that it is precisely the perception of dilapidation and danger in the neighborhood that leads some residents to retreat from social relations and to infer that they are not as good as other people.
Neighborhood Disorder and Self–Esteem
Several studies show that perceptions of neighborhood disorder are associated with lower levels of self–esteem (Bámaca et al. 2005; Behnke et al. 2011; Haney 2007; McMahon et al. 2011; Pals and Kaplan 2013; Prelow et al. 2006; Wiltfang and Scarbecz 1990; but see Ewart and Suchday 2002 for an exception). Although the overwhelming majority of studies focus on adolescents (Bámaca et al. 2005; Behnke et al. 2011; McMahon et al. 2011; Prelow et al. 2006), there is at least some evidence to suggest that perceptions of neighborhood disorder can undermine self–esteem in adulthood (Haney 2007). The inverse association between perceived neighborhood disorder and self–esteem is also found across race and ethnic groups, including non–Hispanic whites (Prelow et al. 2006), non–Hispanic blacks (McMahon et al. 2011; Prelow et al. 2006), and Hispanics (Bámaca et al. 2005; Behnke et al. 2011). There is also striking consistency across indicators of self–esteem, including Rosenberg's Self–Esteem Scale (Bámaca et al. 2005; Behnke et al. 2011; Haney 2007; Pals and Kaplan 2013; Prelow et al. 2006; Wiltfang and Scarbecz 1990), the Coopersmith Self–Esteem Inventory (Wiltfang and Scarbecz 1990), and the self–worth subscale of the Self–Perception Profile for Children (McMahon et al. 2011). In accordance with these studies, we expect that perceptions of neighborhood disorder will be inversely associated with self–esteem (H1).
Neighborhood Disorder and Social Support
The first link in our proposed mediation model suggests that perceptions of neighborhood disorder undermine social support. People who live in disadvantaged neighborhoods may be reluctant to invite guests to visit because of safety concerns or the stigma associated with living in a substandard environment. Perceptions of disorder might also motivate residents to avoid social interaction and the formation of social ties by contributing to distressing emotional states (e.g., fear, depression, and hostility) and negative dispositions toward humanity (e.g., mistrust and misanthropy; Ewart and Suchday 2002; Fullilove et al. 1998; Hill and Maimon 2013; Ross and Mirowsky 2009; Wilson and Kelling 1982). For example, Wilson and Kelling (1982:31) suggest that, in the context of disorder, residents “…will use the streets less often, and when on the streets will stay apart from their fellows, moving with averted eyes, silent lips, and hurried steps.” Such restricted opportunities for social interaction would, by extension, limit the availability of social support. Even under the conditions of extensive social ties, distressing emotional states and negative dispositions toward humanity could undermine perceptions of the availability of social support (Hill and Maimon 2013; Ross and Mirowsky 2009). Consistent with these perspectives, studies show that living in a neighborhood that is characterized by disadvantage and disorder is associated with fewer social ties with neighbors (Geis and Ross 1998; Kim 2010) and lower levels of social support (Kim 2010; McMahon et al. 2011; Schieman 2005). Drawing on this body of work, we expect that perceptions of neighborhood disorder will be inversely associated with social support (H2).
Social Support and Self–Esteem
The second link in our proposed mediation model suggests that limitations in social support undermine self–esteem. The link between social support and self–esteem is fundamental. Nearly four decades ago, Cobb (1976:300) defined social support “… as information leading the subject to believe that he [sic] is cared for and loved, esteemed, and a member of a network of mutual obligations.” Cobb (1976:301) went on to argue that social support “…leads the individual to esteem himself [sic] and reaffirms his [sic] sense of personal worth.” Since the publication of this work, numerous empirical studies have confirmed the positive association between social support and self–esteem (Bámaca et al. 2005; Behnke et al. 2011; Dumont and Provost 1999; Hoffman et al. 1988; Kaplan et al. 1977; Krause 1987; McMahon et al. 2011; Whitbeck et al. 1991). Following this research and building on our first two hypotheses, we expect that the inverse association between perceived neighborhood disorder and self–esteem will be mediated by social support (H3).
Isolating Perceptions of Neighborhood Disorder
Although our mediation model is at least theoretically viable, it is important to isolate perceptions of neighborhood disorder from other difficult conditions that pervade the lives of low–income urban women with children. Along with the troubles associated with living in disadvantaged neighborhoods, the urban poor are regularly confronted with the trials of financial hardship, substandard housing, relationship violence, and poor health (Hill et al. 2007; Hill et al. 2009). The central question that is generally overlooked in previous research is whether low self–esteem is the result of actual or perceived neighborhood disorder per se or the collateral consequences of living in urban poverty. Another vital consideration in longitudinal studies of perceived disorder is the problem of disentangling the effects of changing perceptions from the effects of residential mobility. The question is whether we can attribute changes in support and self–esteem to changes in perceptions of disorder or to changes in social ties that are often associated with moving to a new neighborhood. In an effort to isolate the unique effects of neighborhood disorder, subsequent multivariate analyses control for financial hardship, housing disrepair, relationship violence, self–rated health, neighborhood change.
Heterogeneity across Cities
In addition to explaining and isolating the association between neighborhood disorder and self–esteem, it is important to consider the possibility of heterogeneity across cities. Although some scholars (e.g., Small and Feldman 2012) argue that city–level heterogeneity in neighborhood processes “should be a starting assumption,” others (e.g., Sampson 2013) contend that neighborhood processes in cities like Chicago are “parallel to the national scene.” To formally address this issue, subsequent multivariate analyses test whether the effects of neighborhood disorder on social support and self–esteem are moderated by city of residence. We are especially interested in Small and Feldman's (2012:73) question of whether “…particular kinds of neighborhoods or cities—notably, Chicago—represent ideal laboratories to observe universal social processes…”
Data
To formally assess these expectations, we employ data from the WCF project (see http://www.jhu.edu/∼welfare/). The WCF project is a household–based, stratified random sample of 2,402 low–income women living in low–income neighborhoods in Boston, Chicago, and San Antonio. The WCF first sampled census blocks (or neighborhoods) with at least 20 percent of residents below the Federal Poverty line based on the 1990 census. Within these neighborhoods, households under 200 percent of the poverty line were sampled, with an over–sample of households below 100 percent of the poverty line. Because one of the goals of the WCF project is to assess the impact of welfare policy and work on children, households were screened for the presence of children. Households with at least one infant or child (aged 0–4) or young adolescent (aged 10–14) were sampled. The children's caregivers, all women, were interviewed face–to–face. We refer to the caregivers as “women with children” instead of “mothers” because some caretakers did not identify themselves as the child's parent. The data were collected in 1999 with a follow–up in 2001. The baseline response rate was 75 percent, and 89 percent of the original sample was re–interviewed. The overall respondent–level response rate is 75 percent, with city–specific response rates of 74 percent (Boston), 71 percent (Chicago), and 79 percent (San Antonio). Subsequent analyses are weighted to account for variations in sample sizes across cities.
Measures
Focal Variables
Self–esteem, the focal dependent variable, refers to a personal sense of competence and worthiness (Mruk 2006). Self–esteem is measured as the mean response to eight items (α = 0.74), which were developed by Rosenberg (1965). Respondents were asked to indicate the extent to which they agree or disagree with the following statements: (1) I take a positive attitude toward myself, (2) All in all, I am inclined to feel that I am a failure, (3) On the whole, I am satisfied with myself, (4) I feel I don't have much to be proud of, (5) I'm a person of worth, at least on an equal basis with others, (6) At times, I feel that I am no good at all, (7) I wish I could have more respect for myself, (8) I feel I am able to do things as well as most other people. Response categories for these items range from (1) strongly disagree to (4) strongly agree. These items have demonstrated adequate reliability and validity in previous research (Blascovich and Tomaka 1991; Mruk 2006). These particular items have demonstrated construct validity through associations with mental health, relationship violence, and attitudes toward parenting (Burdette et al. 2011; Hill et al. 2008, 2010).
Perceived neighborhood disorder, the focal predictor variable, refers to conditions and activities, major and minor, criminal and noncriminal, that residents perceive to be signs of the breakdown of social order (Ross and Mirowsky 1999). Neighborhood disorder is measured as the mean response to ten items (α = 0.89). Respondents were asked to rate their neighborhood environment in terms of (1) assaults and muggings, (2) drug dealing in the open, (3) gangs, (4) unsafe streets during the day, (5) burglaries and thefts, (6) teenage pregnancy, (7) abandoned houses, (8) police not being available, (9) unsupervised children, and (10) high unemployment. Response categories for these items are coded (1) not a problem, (2) somewhat of a problem, and (3) a big problem. These items have demonstrated adequate psychometric properties in previous research (Hill et al. 2005). This measure has shown construct validity through associations with social support, self–esteem, mental health, heavy drinking, and self–rated health (Hill et al. 2005; Hill and Angel 2005; Hill et al. 2010).
Social support is the proposed mediating variable. Although some researchers define social support as the actual receipt of resources, others classify it in cognitive terms, as individual perceptions of resource availability (Thoits 1995). In this study, social support refers to perceptions of emotional and instrumental support and is measured as the mean response to four items (α = 0.81). Respondents were asked to indicate how many people they could count on to (1) listen to their problems when they were feeling low, (2) take care of their children when they were not around, (3) help them with small favors, and (4) loan them money in case of an emergency. Response categories for all support items are coded as (0) no one, (1) too few people, and (2) enough people. These measures have demonstrated construct validity in previous research through associations with mental health and attitudes toward parenting (Durden et al. 2007; Hill et al. 2008; Hill et al. 2010).
Confounding Variables
Financial hardship refers to the inability to meet essential material needs. Hardship is measured as the mean response to thirteen items (α = 0.83). For example, respondents were asked to indicate how often they had to “borrow money to pay bills.” Respondents were also asked to indicate whether they had enough money to “afford housing, food, and clothing,” and whether any adults or children in the household were “unable to eat for a whole day because there wasn't enough money for food.” Because original hardship items were measured with mixed question formats and responses, each of these items has been standardized to account for metric differences. This measure has shown construct validity through associations with heavy drinking and mental health (Hill and Angel 2005; Hill et al. 2007).
Housing disrepair refers to a range of potentially noxious housing conditions. Housing disrepair is measured as a summed response to eight items (α = 0.70). For example, respondents were asked to indicate whether any of the following conditions were present in their households: “a leaky roof, a toilet, hot water, or other plumbing that doesn't work,” “broken windows,” and “rats, mice, cockroaches, or other pests.” Responses to these individual items were dummy coded (0) no and (1) yes. This measure has demonstrated construct validity in previous research through associations with mental health and independent interviewer ratings of housing disrepair (Burdette et al. 2011; Hill et al. 2007).
Relationship violence in the past year is measured with several items drawn from the Revised Conflict Tactics Scales (CTS2) (Straus et al. 1996). In accordance with the work of Straus and colleagues (1996), we assess whether the respondent experienced any of four major types of relationship violence in the past year, including psychological aggression (e.g., a romantic partner had threatened to hit the respondent or use a weapon on them), minor physical assault (e.g., a romantic partner had thrown something at the respondent or pushed, grabbed, or shoved them), severe physical assault (e.g., a romantic partner had slapped, kicked, bit, or punched the respondent), and sexual coercion (i.e., a romantic partner had forced the respondent into any sexual activity). Respondents were assigned a value of (1) if they reported any experiences with relationship violence in the past year and (0) otherwise. The CTS2 has established reliability and validity (Straus et al. 1996). These particular measures have shown construct validity through associations with social support, self–esteem, heavy drinking, mental health, self–rated health, and criminal behavior (Hill et al. 2009; Hill et al. 2010; Hill et al. 2007; Hill et al. 2009; Schroeder et al. 2011).
Self–rated health is indicated by a single item. Respondents were asked, “In general how is your health?” Response categories for this item are coded as (1) poor, (2) fair, (3) good, (4) very good, or (5) excellent. This item is unique in that it measures a wide range of physical health problems, including diagnosed or known conditions and symptoms of undiagnosed or unknown conditions (Idler and Benyamini 1997). Self–rated health is widely used to measure general physical health status. It is strongly correlated with more objective measures of physical health, including physician diagnoses, various measures of morbidity, and all–cause mortality (Idler and Benyamini 1997).
Neighborhood move is also indicated by a single item. During the second wave of data collection, respondents were asked to indicate whether they had moved to a different neighborhood since the last interview. Responses to this item were dummy coded (0) no and (1) yes. Neighborhood mobility is only included in our longitudinal models because it was not assessed at baseline.
Background Variables
Our multivariate analyses also control for a range of background variables that are known correlates of neighborhood disorder, social support, and/or self–esteem (e.g., Haney 2007; Hill et al. 2010; Rosenberg 1981; Schieman and Pearlin 2006; Wiltfang and Scarbecz 1990). These factors include age (in years), race and ethnicity (four dummy variables capturing non–Hispanic Whites, Mexicans, other Hispanics, and Blacks—the reference category), education (in years), employment status (1 = currently employed, 0 = otherwise), welfare status (1 = currently receiving public assistance, 0 = otherwise), marital status (1 = currently married/spouse in house, 0 = otherwise), number of children (1 to 6 or more, top–coded continuous variable), and city of residence (three dummy variables capturing residence in Boston, San Antonio, and Chicago—the reference category).
Statistical Procedures
We use ordinary least squares (OLS) regression to model changes in self–esteem over the 2–year (1999 and 2001) study period (Table 1). In lieu of lagged endogenous dependent variable models, we employ change score models to assess 2–year self–esteem changes. A comparison of two–wave panel designs concluded that change score models are generally preferable to lagged endogenous dependent variable models (Johnson 2005). We computed change scores by subtracting baseline (1999) self–esteem scores from follow–up (2001) self–esteem scores. Change scores are continuous variables that range from some negative number to some positive number. Negative numbers indicate lower levels of self–esteem in 2001 than in 1999 (i.e., a loss of self–esteem). Positive numbers suggest higher levels of self–esteem in 2001 than in 1999 (i.e., improvements in self–esteem). Many respondents exhibit a change score of zero, which indicates no change in self–esteem across waves. Because change scores are continuous variables, we also use OLS regression to predict changes in self–esteem with neighborhood disorder. In this case, unstandardized coefficients are estimated to describe the difference in the expected change in self–esteem for each one–unit change in a predictor.
Longitudinal Regressions of Changes in Social Support and Self–Esteem
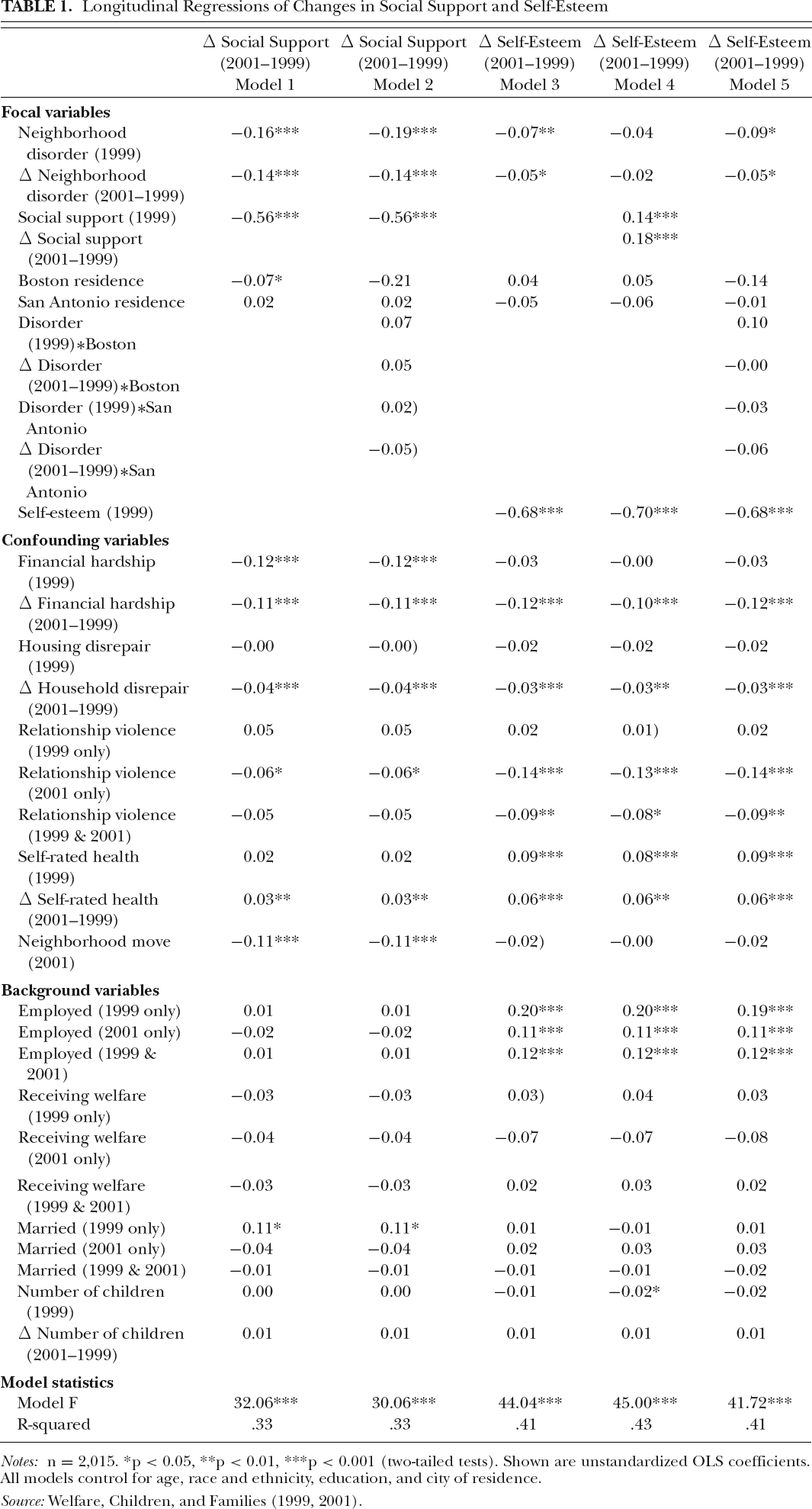
n = 2,015.
p < 0.05,
< 0.01,
p < 0.001 (two–tailed tests). Shown are unstandardized OLS coefficients. All models control for age, race and ethnicity, education, and city of residence.
Source: Welfare, Children, and Families (1999, 2001).
Our change score analyses proceed in three steps. In the first step, we test whether neighborhood disorder at baseline (1999) and changes in neighborhood disorder (2001–1999) are associated with changes in social support, controlling for confounding variables, background variables, and baseline levels of social support. In the second step, we test whether neighborhood disorder at baseline and changes in neighborhood disorder are associated with changes in self–esteem, controlling for confounding variables, background variables, baseline levels of self–esteem and social support (baseline and change). In the third step, we add cross–product terms (disorder*city) to our unmediated regression models to test whether the effects of neighborhood disorder on social support and self–esteem are moderated by city of residence.
To formally assess mediation, we employ the Clogg statistic (see Clogg et al. 1995) to test for significant changes in the effects of neighborhood disorder across nested models (i.e., before and after adjusting for social support). A statistically significant reduction in the magnitude of a neighborhood disorder coefficient would suggest mediation.
When considering changes in outcomes over time, it is customary to examine the issue of bias because of sample attrition. The primary concern is whether or not there are any systematic changes in the sample across waves. To formally assess this issue, we estimated a binary logistic regression model predicting the log odds of sample attrition (results not shown, but available upon request). Approximately 13 percent of the sample was lost to follow–up, but our logistic regression results show very little evidence of bias because of sample attrition.
Results
Descriptive Analyses
The weighted descriptive statistics for the study sample, including minimum and maximum values, means, standard deviations, and alpha reliability estimates can be found online (Table 1). The average respondent reported a high level of self–esteem and a moderate level of neighborhood disorder. Respondents also reported high levels of social support. The change scores for these measures indicate that although self–esteem and social support increased over the study period, perceptions of neighborhood disorder decreased. The high levels of self–esteem are somewhat surprising given the disadvantaged nature of the sample, but this result is generally consistent with the high percentage of non–Hispanic black respondents in the sample. Although previous research shows that socioeconomic status is associated with lower levels of self–esteem, non–Hispanic blacks tend to exhibit high levels of self–esteem (e.g., Hughes and Demo 1989; Rosenberg and Pearlin 1978). The high average levels of social support in the sample may also contribute to such high levels of self–esteem. In any case, our observed distribution of self–esteem is generally consistent with other studies that focus on populations that include high percentages of low–income and minority respondents (e.g., Behnke et al. 2011; Haney 2007; McMahon et al. 2011; Paschall and Michael Hubbard 1998).
Longitudinal Analyses
Table 1 provides the results of our longitudinal change score analyses. Models 1 and 3, respectively, indicate that higher levels of perceived neighborhood disorder at baseline are associated with lower levels of social support and self–esteem from baseline to follow–up (i.e., lower levels of self–esteem in 2001 than in 1999), even with adjustments for a range of confounding variables, background variables, and baseline levels of social support and self–esteem. In other words, these results suggest that women who report high levels of neighborhood disorder are more vulnerable to losses in social support and self–esteem over the study period than those women who report more order in their neighborhoods. Models 1 and 3 also show that changes in perceived neighborhood disorder are associated with changes in social support and self–esteem. More specifically, those women who reported an increase in perceived neighborhood disorder from baseline to follow–up (i.e., more problems in the neighborhood in 2001 than in 1999) also tended to report concurrent losses in social support and self–esteem.
Model 4 in Table 1 presents tests of whether baseline levels of social support and changes in social support help to mediate or explain any of the effects of baseline levels of perceived neighborhood disorder and changes in disorder on changes in self–esteem. With the addition of social support in Model 4, the original association between baseline neighborhood disorder and the change in self–esteem is reduced by 43 percent, which is a statistically significant reduction (t = −6.87, p < 0.001). The original association between the change in neighborhood disorder and the change in self–esteem is also reduced by 60 percent, a statistically significant reduction (t = −5.63, p < 0.001). In Model 4, both neighborhood disorder variables are no longer statistically significant at conventional levels, and social support is associated with higher levels of self–esteem from baseline to follow–up. Taken together, these results suggest that neighborhood disorder may undermine self–esteem by restricting opportunities for social support.
Models 2 and 5, respectively, present tests of whether the effects of baseline levels of perceived neighborhood disorder and changes in disorder on changes in social support and self–esteem vary according to city of residence. Because none of the interaction terms reached conventional levels of statistical significance, we conclude that the effects of disorder on social support and self–esteem in Boston and San Antonio are comparable to those in Chicago.
Discussion
Although several previous studies show that self–esteem varies according to neighborhood context, few have directly examined potential mediators of this association. In this paper, we used longitudinal survey data to examine the association between perceived neighborhood disorder and self–esteem among low–income urban women with children. Building on previous research, we examined the potential mediating influence of social support. We also considered the possibility of heterogeneity across cities.
Research Implications
In agreement with our first hypothesis (H1), we found that (1) higher levels of disorder at baseline were associated with lower levels of self–esteem from baseline to follow–up and that (2) increases in disorder over the study period were associated with concurrent losses in self–esteem. Our results confirm that perceptions of neighborhood disorder can undermine the self–esteem of adult women (Haney 2007).
Consistent with our second hypothesis (H2), we showed that (a) higher levels of disorder at baseline were associated with lower levels of social support from baseline to follow–up and that (b) increases in disorder over the study period were associated with concurrent losses in social support. These results confirm previous studies showing that living in a disadvantaged neighborhood is associated with fewer social ties with neighbors (Geis and Ross 1998; Kim 2010) and lower levels of social support (Kim 2010; McMahon et al. 2011; Schieman 2005). Our findings are also generally consistent with urban sociological theories of the disconnectedness of American inner cities, including social disorganization, collective efficacy, and broken windows. Although the first link in our conceptual model (the link between perceived disorder and social support) clearly flows from these theories, it is important to note that we never directly test these theories in our analyses.
In accordance with our final hypothesis (H3), our results showed evidence of full mediation. As Prelow et al. (2006) suspected, perceived neighborhood disorder may indeed undermine self–esteem by restricting opportunities for social support and, by extension, positive appraisals from others. Our analysis adds social support to poor previous health (Haney 2007) as a second pathway by which perceptions of neighborhood disorder undermine self–esteem.
Although it is reasonable to begin with the assumption of heterogeneity in neighborhood processes (Small and Feldman 2012), we found that the effects of disorder on social support and self–esteem in Boston and San Antonio are comparable to those in Chicago. These results are more in line with the notion that neighborhood processes can be invariant across cities (Sampson 2012). However, our modest range of comparison is in no way intended to represent a universal social process.
Research Limitations
The primary limitation of this study is that the sample is restricted to predominantly black and Hispanic low–income urban women with children living in low–income neighborhoods in Boston, Chicago, and San Antonio. Although we have attempted to frame the unique characteristics of our sample as a strength, we cannot generalize our results beyond these specific population parameters. Because we have focused on such a potentially vulnerable population, we may have overestimated the associations among our focal variables. Given that our multivariate analyses are based on observational data, we must acknowledge the possibility of alternative causal models. Even though we assume that neighborhood disorder and social support shape self–esteem, it is plausible that self–esteem could also shape perceptions of the neighborhood and the formation and maintenance of social ties. Clearly, the veracity, specificity, and external validity of our theoretical model is contingent upon replication and further testing of data collected from men, higher income women, women living in nonpoor neighborhoods, women without children, and those living in other cities. Having said this, we are encouraged that our results conform to previous theoretical and empirical work, including studies of more diverse populations.
Conclusion
In this article, we examined the association between perceived neighborhood disorder and self–esteem. We also considered the potential mediating influence of social support. Despite the limitations of our study, our results demonstrate that perceptions of neighborhood disorder can undermine self–esteem by limiting social support among low–income urban women with children. More empirical research is needed to test additional mediators of the association between neighborhood context and self–esteem. The sense of mattering is one mechanism that is at least theoretically viable. The idea is that neighborhood disorder could undermine self–esteem by weakening one's perceived significance and importance to others. It is also important to think about extending our theoretical model beyond self–esteem to examine other important outcomes (e.g., mental health) and negative feedback processes (e.g., motivations related to civic involvement). For example, neighborhood disorder could discourage organization and volunteering in the community by pushing people to believe that they are “no good at all” or “not able to do things as well as most other people.” Research along these lines should provide a more thorough understanding of how living in a disadvantaged neighborhood environment might contribute to a low self–concept and other unfavorable social, psychological, and behavioral outcomes. Several studies of the Moving to Opportunity and Gautreaux programs have documented a range of benefits associated with moving residents of disadvantaged neighborhoods to more advantaged neighborhoods (e.g., Acevedo–Garcia et al. 2004; Leventhal and Brooks–Gunn 2003; Rosenbaum 1995). In terms of policy, our results suggest that reducing signs and perceptions of disorder in disadvantaged neighborhoods may also uniquely contribute to the self–worth of low–income urban women with children. Reductions in disorder could be achieved by improving the social and physical landscapes of neighborhoods as well as by moving residents to neighborhoods characterized by lower levels of disorder.