
Abstract
Rationale
In about 20% of acute ischemic stroke patients stroke occurs during sleep. These patients are generally excluded from intravenous thrombolysis. MRI can identify patients within the time-window for thrombolysis (≤4·5 h from symptom onset) by a mismatch between the acute ischemic lesion visible on diffusion weighted imaging (DWI) but not visible on fluid-attenuated inversion recovery (FLAIR) imaging. Aims and hypothesis The study aims to test the efficacy and safety of MRI-guided thrombolysis with tissue plasminogen activator (rtPA) in ischemic stroke patients with unknown time of symptom onset, e.g., waking up with stroke symptoms. We hypothesize that stroke patients with unknown time of symptom onset with a DWI-FLAIR-mismatch pattern on MRI will have improved outcome when treated with rtPA compared to placebo.
Design
WAKE-UP is an investigator initiated, European, multicentre, randomized, double-blind, placebo-controlled clinical trial. Patients with unknown time of symptom onset who fulfil clinical inclusion criteria (disabling neurological deficit, no contraindications against thrombolysis) will be studied by MRI. Patients with MRI findings of a DWI-FLAIR-mismatch will be randomised to either treatment with rtPA or placebo. Study outcome The primary efficacy endpoint will be favourable outcome defined by modified Rankin Scale 0–1 at day 90. The primary safety outcome measures will be mortality and death or dependency defined by modified Rankin Scale 4–6 at 90 days.
Discussion
If positive, WAKE-UP is expected to change clinical practice making effective and safe treatment available for a large group of acute stroke patients currently excluded from specific acute therapy.
Keywords
Introduction and rationale
Stroke is the second most common single cause of death and the most frequent cause of permanent disability in industrialized countries. The World Health Organization estimates that 15 million people suffer from stroke each year, and 5 million are left permanently disabled (1). Currently, intravenous (i.v.) thrombolysis with recombinant tissue plasminogen activator (rtPA, alteplase) represents the only effective and approved specific treatment for acute ischemic stroke and is recommended by international, European, and national guidelines (2). Given the recent proof of efficacy and safety of i.v. rtPA to 4·5 h, international guidelines have already modified the recommendations for thrombolysis (3), and 15 European countries have recently approved i.v. thrombolysis with rtPA for acute stroke up to 4·5 h of symptom onset. However, confirmed symptom onset within this time window is currently a prerequisite for treatment with i.v. thrombolysis, and an unknown time of onset usually represents a contraindication to thrombolysis in stroke.
Wake-up stroke
Up to 20% of strokes are estimated to occur during sleep (4,–6) adding up to an estimated 3 million strokes per year worldwide. Following current approval criteria and guideline recommendation, this large group of patients is predominantly excluded from thrombolysis. However, clinical and imaging observations suggest that in a large number of patients waking up with stroke symptoms, strokes may have occurred in the early morning hours so that they might still be eligible for thrombolysis. The frequency of early ischemic signs on computed tomography (CT) was reported to be similar in patients who woke up with stroke symptoms as compared with patients presenting within three-hours (7) or six-hours of symptom recognition (6). The proportion of patients showing a perfusion-diffusion mismatch pattern on magnetic resonance imaging (MRI) was also similar for wake-up strokes and patients within three-hours of symptom onset (4), a finding that was recently reproduced for the detection of ‘tissue at risk’ by perfusion CT in another case series of wake-up stroke patients (8). Together, these data suggest that a large number of patients with wake-up stroke might still be within a time window for thrombolysis when reaching the hospital.
Pilot studies of thrombolysis in wake-up stroke
There are several case reports or small uncontrolled case series that report on thrombolysis in patients with wake-up stroke. These studies used either plain CT, perfusion CT, or multiparametric stroke MRI (9,–12). There is, however, no evidence from any randomized controlled trial of thrombolysis in wake-up stroke.
Imaging surrogate markers of lesion age: the diffusion-weighted imaging–fluid-attenuated inversion recovery (DWI-FLAIR) mismatch
Magnetic resonance imaging findings change during the time course of acute cerebral ischemia reflecting the typical course of changes in tissue water in acute ischemia. The drop of cerebral blood flow below a critical threshold leads to a disruption of energy metabolism, resulting in cytotoxic edema, which can be depicted by a reduced apparent diffusion coefficient on DWI within minutes of stroke (13,14). During the following 1–4 h tissue osmolality increases, accompanied by a net increase of water and this absolute increase of water content can be detected by T2-weighted MRI (13,15). Fluid-attenuated inversion recovery imaging is characterized by strong T2 weighting together with suppression of cerebrospinal fluid signal (16). The pattern of a visible ischemic lesion on DWI together with normal T2-weighted imaging or FLAIR is a typical finding in human stroke if imaging is performed within the first hours of stroke. These observations have brought forward a new concept to identify patients likely to benefit from thrombolysis based on the assumed lesion age, the DWI-FLAIR mismatch (17). In contrast to the previously suggested concept of perfusion-diffusion mismatch that labels a mismatch between lesion volumes on two parameter maps, Diffusion-weighted imaging-fluid-attenuated inversion recovery mismatch refers to the mismatch between visibility of an ischemic lesion in one sequence (DWI), indicating the presence of acute ischemia, while it is not visible in the other sequence (FLAIR), indicating that the ischemic lesion is likely to be less than 4·5 h old. Other imaging approaches have been suggested to identify patients likely to respond to reperfusion treatment independent from time of symptom onset such as penumbral imaging using perfusion-diffusion mismatch as a marker of tissue at risk of infarction (18) or the presence of vessel occlusion (19). Moreover, tissue status as depicted by multiparametric MRI (20) or collateral flow (21) represent important determinants of treatment response in acute stroke. However, evidence for clinical efficacy of any of these approaches to select patient for thrombolysis is still lacking, while there is unequivocal evidence for efficacy of i.v. thrombolysis in acute stroke patient if started within 4·5 h of symptom onset. Thus, in contrast to perfusion-diffusion mismatch, which indicates tissue viability, DWI-FLAIR mismatch is a surrogate marker of lesion age, which is the essential piece of information missing in wake-up stroke.
Preparatory studies on DWI and FLAIR to estimate acute ischemic lesion age
In a series of single-center studies from different groups a clear time dependency of the visibility of acute ischemic lesions on FLAIR was demonstrated, increasing to almost 100% visibility after three- to six-hours (17,22,–24). Moreover, DWI-FLAIR mismatch was found to identify patients within a time window of three or 4·5 h with high specificity and positive predictive value (PPV) (17,22,–24). These findings were confirmed in a recent large multicenter study including 643 patients (PREFLAIR: PREdictive value of FLAIR and DWI for the identification of acute ischemic stroke patients ≤3 and ≤4·5 h of symptom onset – a multicenter study) (25). Within the assumed target population for thrombolysis, i.e. patients with stroke in the territory of the middle cerebral artery and a relevant neurological deficit, DWI-FLAIR mismatch identified patients within 4·5 h with a specificity of 0·81 and a PPV of 0·87 (25). This is similar to recent results of a Japanese group reporting a specificity of 0·83 and a PPV of 0·90 to identify patients with symptom onset <4·5 h from n = 214 patients with nonlacunar ischemic stroke (22). Together, these studies provide compelling evidence that the DWI-FLAIR mismatch allows identification of patients with stroke of unknown onset with a sufficiently high likelihood of being in a time window in which thrombolysis is proven effective and safe (i.e. within 4·5 h). The predictive values to identify patients within six-hours of symptom onset were even higher, with a PPV of 0·95 in PREFLAIR (25) and 0·98 in the Japanese sample (22). This appears noteworthy as both the pooled analysis of the clinical trials of rtPA in stroke and a Cochrane analysis indicate a possible beneficial effect of thrombolysis together with the absence of an increase in symptomatic intracranial hemorrhage (SICH) up to six-hours of symptom onset (26,27). Just recently, an observational study reported a high rate (44%) of DWI-FLAIR mismatch in patients with wake-up stroke (28).
On the basis of this evidence, the Efficacy and safety of MRI-based thrombolysis in wake-up stroke: a randomized, double-blind, placebo-controlled trial (WAKE-UP) will use the DWI-FLAIR-mismatch as the imaging criterion to select patients likely to benefit from thrombolysis based on the inferred time from symptom onset.
Aims
The objective of WAKE-UP is to test efficacy and safety of MRI-based i.v. thrombolysis with rtPA (alteplase) in patients with unknown symptom onset, e.g. patients waking up with stroke symptoms. WAKE-UP is aimed at changing clinical practice by providing evidence for an effective and safe treatment for a new large group of acute stroke patients currently excluded from specific acute treatment.
Methods
Study design
WAKE-UP is an investigator-initiated, interventional, randomized, double-blind, placebo-controlled, parallel-assignment, international, multicenter efficacy, and safety study. Patients will be randomized 1:1 to either treatment (alteplase, rtPA) or placebo. Infarct volume and intracranial hemorrhage will be assessed on follow-up MRI after 22–36 h. Final clinical outcome will be assessed 90 days after stroke. See Figure 1 for a flow chart of the study design.
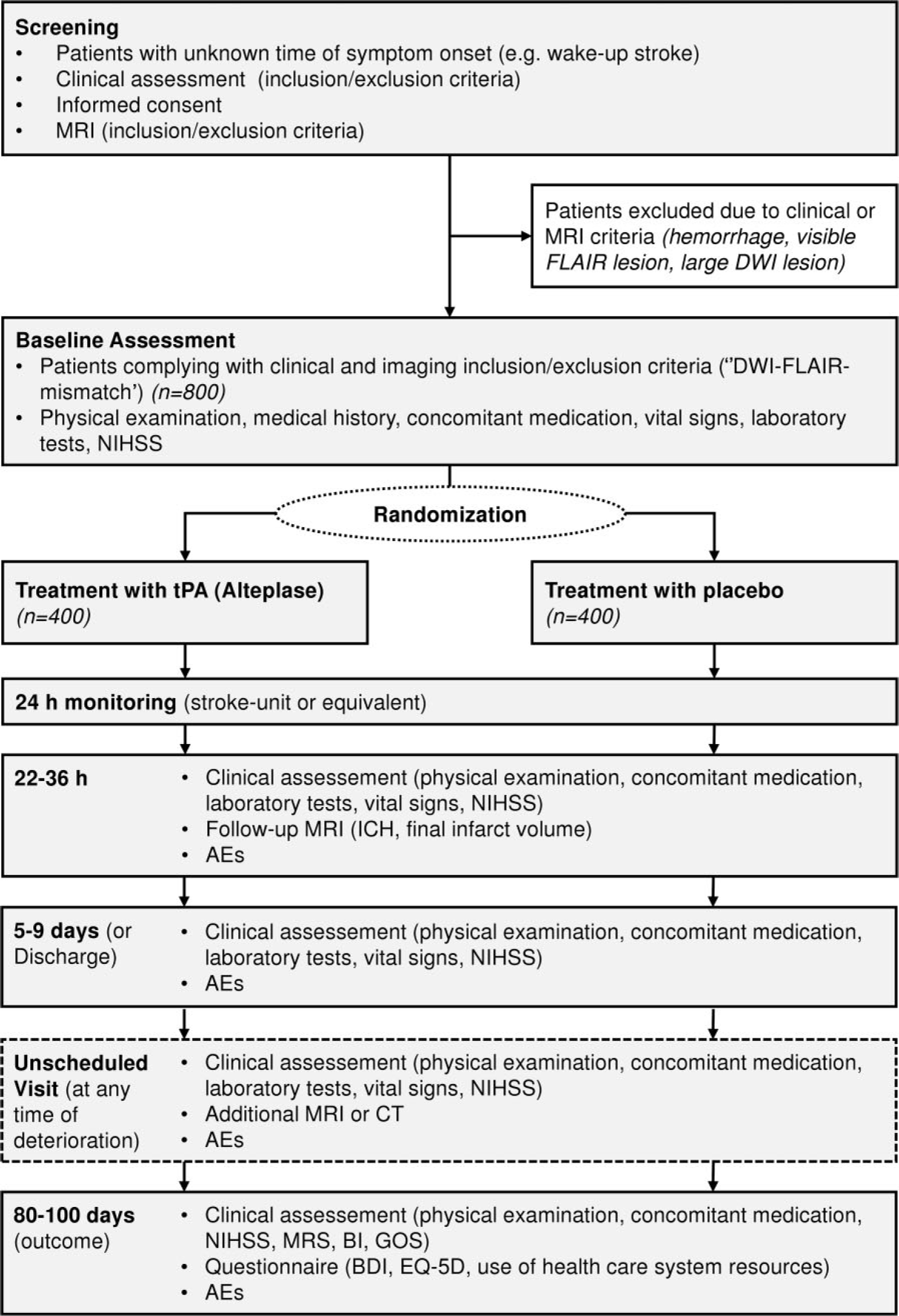
Efficacy and safety of MRI-based thrombolysis in wake-up stroke (WAKE-UP) study assessment flow chart. AE, adverse event; BDI, Beck Depression Inventory; BI, Barthel Index; CT, computed tomography; DWI, diffusion-weighted imaging; EQ-5D, EuroQol-5 dimensions, standardized measure of health status; FLAIR, fluid-attenuated inversion recovery; GOS, Glasgow Outcome Scale; ICH, intracranial hemorrhage; MRI, magnetic resonance imaging; MRS, modified Rankin scale; NIHSS, National Institutes of Health Stroke Scale; tPA, tissue plasminogen activator.
Patient population
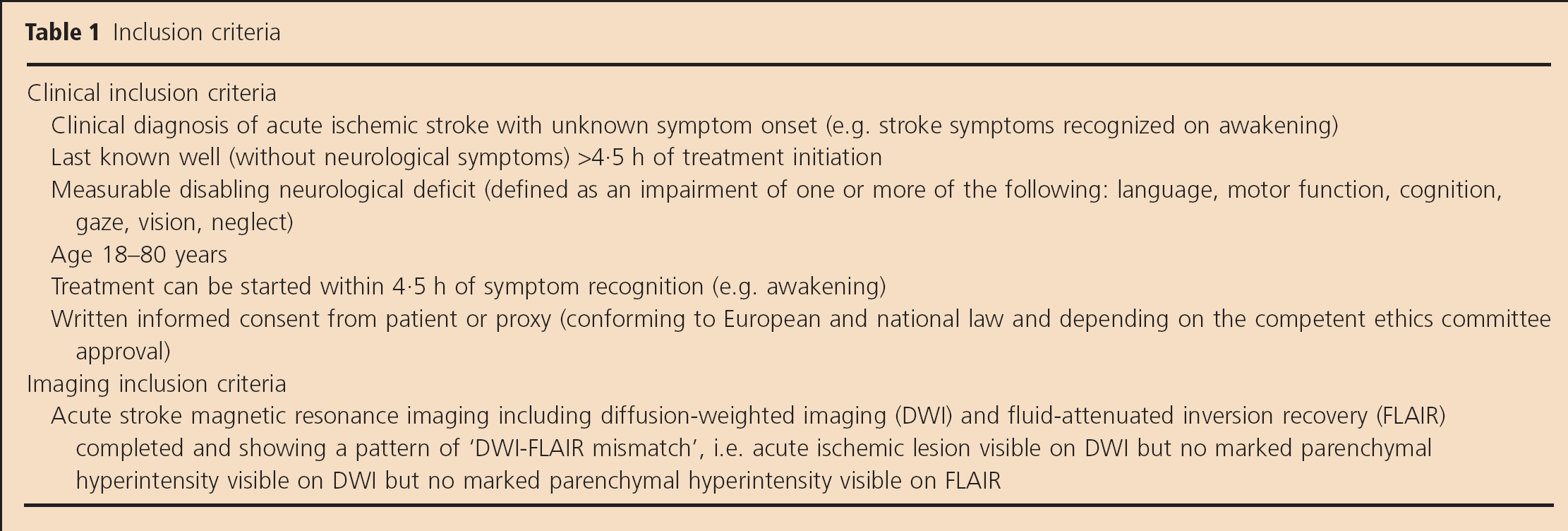
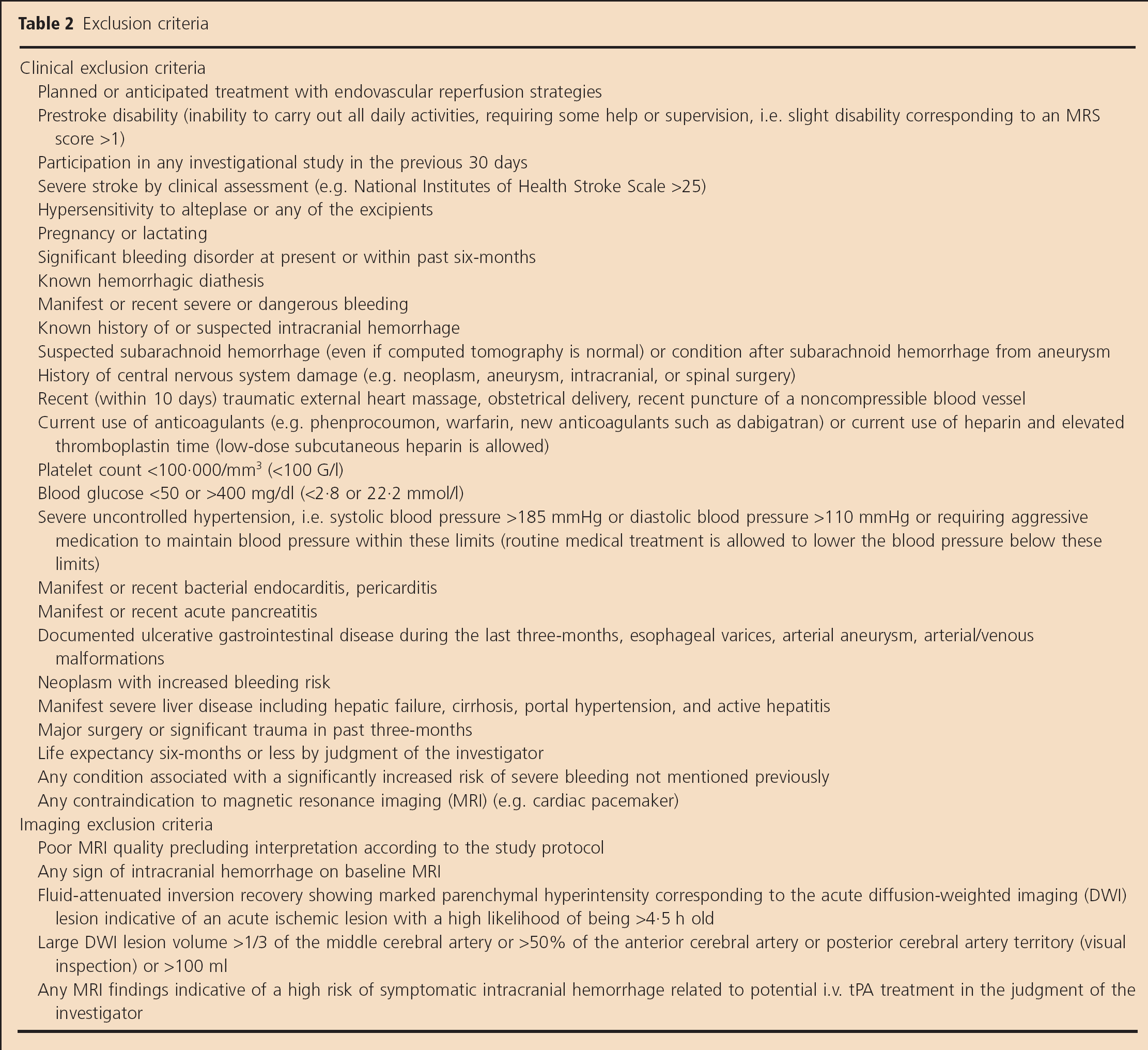
Patients with acute ischemic stroke confirmed by MRI and unknown time from symptom onset who otherwise fulfill the approval criteria for i.v. thrombolysis in acute stroke represent the target population for WAKE-UP. Inclusion and exclusion criteria mainly follow the license of alteplase in Europe except for specific criteria related to the clinical trial (e.g. unknown time of symptom onset and MRI criteria indicative of lesion age of less than 4·5 h). See Tables 1 and 2 for inclusion and exclusion criteria.
Inclusion criteria
Exclusion criteria
Clinical assessment
Trained investigators will perform clinical assessment at baseline, at 22–36 h, at five- to nine-days or at hospital discharge, and at 90 ± 10 days. Neurological deficit will be assessed using the National Institutes of Health Stroke Scale (NIHSS). At 90 ± 10 days, clinical outcome assessment will also comprise the Barthel Index (BI), modified Rankin scale (MRS), Glasgow Outcome Scale (GOS), Beck Depression Inventory (BDI), functional health status [EuroQol-5 dimensions (EQ-5D)], and a questionnaire on the use of health care system resources. Investigators will complete a training and certification program for the NIHSS and the MRS.
Imaging assessment – MRI protocol
The imaging inclusion criteria represent a crucial part of the trial. The presence of DWI-FLAIR mismatch identifies patients with ischemic lesions less than 4·5 h old (17,22,–25). This, in turn, assures the enrollment of patients that are likely to benefit from thrombolysis (26,29). Imaging inclusion criteria define DWI-FLAIR mismatch as an acute ischemic lesion visible on DWI but no marked parenchymal hyperintensity visible on FLAIR (see Fig. 2). Imaging exclusion criteria mainly aim at the reduction of the risk of symptomatic intracranial hemorrhage SICH and thus involve the exclusion of large DWI lesions that were found to be associated with increased risk of SICH in previous studies (30). A detailed imaging handbook will provide extensive examples illustrating inclusion and exclusion criteria. In addition, all investigators will pass a standardized training of image judgment according to imaging inclusion and exclusion criteria.
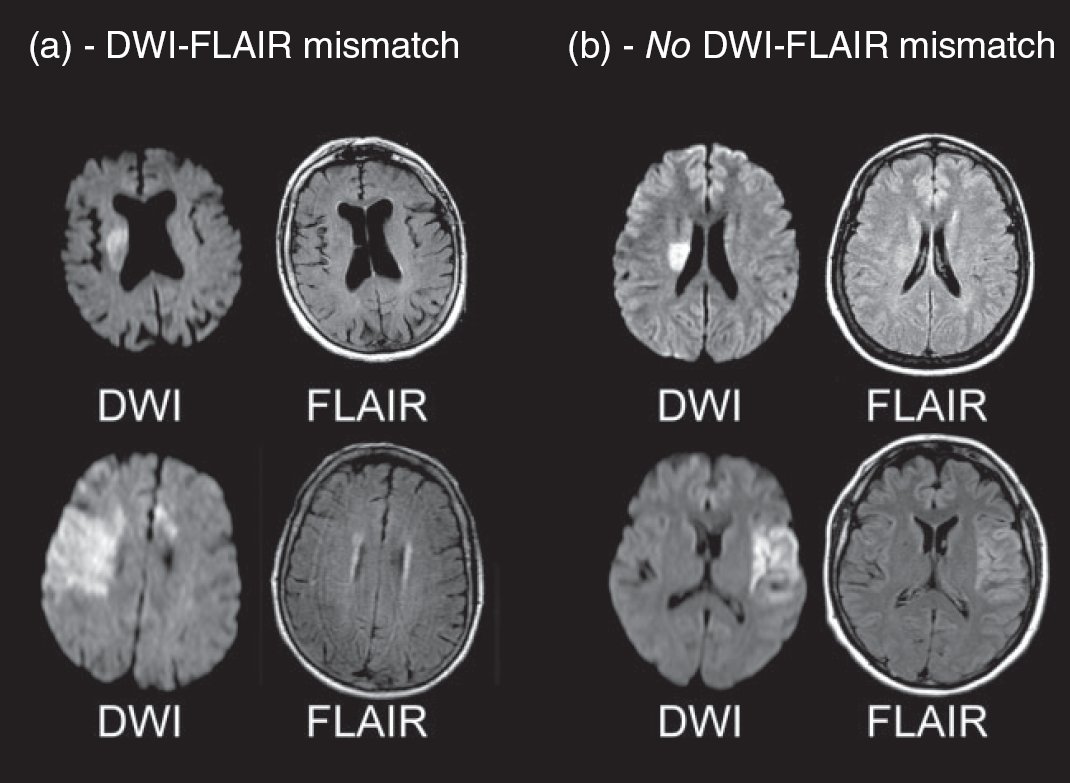
Examples of magnetic resonance imaging (MRI) inclusion and exclusion criteria. (a) Two examples of patients fulfilling the criterion of DWI-FLAIR mismatch: acute ischemic lesion clearly visible on diffusion-weighted imaging (DWI), but no clear parenchymal hyperintensity visible on fluid-attenuated inversion recovery (FLAIR) corresponding to the DWI lesion. (b) Two examples of patients not fulfilling the criterion of DWI-FLAIR mismatch: acute ischemic lesion clearly visible on DWI and clear parenchymal hyperintensity on FLAIR corresponding to the acute DWI lesion.
All patients will undergo a standardized MRI protocol. The following MRI sequences are mandatory: DWI, FLAIR, a sequence sensitive to hemorrhage, e.g. T2*-weighted gradientrecalled echo sequences, and time of flight magnetic resonance angiography covering the circle of Willis. Information on vessel occlusion or perfusion will not be used for patient enrollment but information on the vessel status will be used for secondary endpoint analysis and may be used by the data and safety monitoring board (DSMB) to weigh results of safety analyses. Only patients with completed MRI according to the study protocol are eligible. Contraindications to MRI as well as poor quality of MRI exclude patients from the trial. All images will be judged at the scanner by the local investigators. A central image reading board (CIRB) will continuously monitor the fulfillment of the prespecified MRI standards in each participating center and the compliance of patients randomized with the imaging inclusion and exclusion criteria. Follow-up MRI will be performed after 22–36 h to identify ICH and to delineate final infarct volume.
Randomization
Eligible patients are randomized to treatment with either alteplase or placebo (1:1). Randomization is stratified by center, age (≤60/>60 years), and severity of symptoms (NIHSS ≤10/>10). Age and severity of symptoms as measured by the NIHSS represent two major covariate predictors of outcome in acute stroke (31). The approach of stratified randomization helps to avoid imbalances between the groups that might affect outcome and bias results (32). Both patient and investigator are blinded to treatment allocation. The investigator will be provided with the options to selectively unblind an individual patient 24/7 if deemed necessary for any clinical reasons. The DSMB will have access to data that are grouped but not unblinded in terms of treatment allocation.
Investigational product
The active study medication (rtPA) is supplied in glass vials containing 50 mg of rtPA as lyophilized powder to be reconstituted to obtain a solution. The matching placebo is supplied in a form of a lyophilized powder to be reconstituted in order to obtain a solution indistinguishable from the active drug. Labeling and packaging of study medication will be conducted according to good manufacturing practice, good clinical practice, and local and national regulatory requirements.
Treatment
Patients randomized to the active study drug will receive i.v. rtPA 0·9 mg/kg body weight up to a maximum of 90 mg, 10% as bolus, and 90% over one-hour as infusion. Accordingly, patients randomized to the placebo arm will receive i.v. placebo according to body weight, 10% as bolus, and 90% over one-hour as infusion. Treatment has to be initiated as soon as possible within 60 mins of the end of the MRI examination.
Outcome assessment
Primary efficacy end-point
‘Favorable outcome’ defined by a score of 0–1 on the (MRS) 90 (± 10) days after stroke
Primary safety end-points
Mortality 90 (±10) days after stroke
Death or dependency 90 (± 10) days after stroke (MRS 4–6)
Secondary efficacy end-points
Global Outcome Score (combination of MRS 0–1, NIHSS 0–1, BI 95–100, GOS 1) 90 (±10) days after stroke
Categorical shift in MRS 90 (± 10) days after stroke
Responder analysis relating MRS 90 (± 10) days after stroke to baseline NIHSS score (NIHSS <7: MRS 0; NIHSS 8–14: MRS 0–1; NIHSS >14: MRS 0–2)
Infarct volume after 22–36 h
Depressive symptoms 90 (±10) days after stroke (BDI)
Functional health status and quality of life 90 (± 10) days after stroke (EQ-5D)
Use of health care system resources
Secondary safety end-points
SICH as defined in SITS-MOST (Safe Implementation of Thrombolysis in Stroke-Monitoring Study)
SICH as defined ECASS II (Second European-Australasian Acute Stroke Study)
SICH as defined in NINDS (National Institute of Neurological Disorders and Stroke rt-PA Stroke Study)
Parenchymal hemorrhage type 2 (PH-2)
Statistical analysis
All analyses will be conducted on data from all randomly assigned patients, whether or not treated, according to the intention-to-treat principle. Sensitivity analyses based on different hypotheses about the pattern of missing data for the primary outcome will be performed to test for the robustness of the primary analysis. Analyses will also be repeated according to the per-protocol principle. The judgments of central image reading will be used to define the population for per-protocol analysis.
For the primary efficacy outcome measure, between-group differences will be tested using a chi-square test. An unconditional logistic regression model will be fitted to estimate the odds ratio associated with treatment effect, restricting the adjustment for the randomization stratified factors (age and symptom severity). One interim analysis of primary end-point is planned after the inclusion of 500 patients (250 in each group), with a statistical stopping guideline for an overwhelming benefit. Lan-DeMets alpha-spending function will be used to control for the overall alpha level, using O'Brian and Fleming boundaries (corresponding to alpha levels of 0·0132 and 0·0460 at the interim and final analysis, respectively). Secondary outcome analyses will be performed according to standard statistical principles for comparison of parametric or nonparametric distributions as appropriate.
Sample size calculation
Based on the reported pooled data of the stroke thrombolysis trials (26), we expect a 10·0% absolute difference in the proportion of patients reaching the primary efficacy end-point between patients treated with the active drug and placebo (expected rate of ‘favorable outcome’ 43·3% in patients treated with alteplase and 33·3% inpatients in the placebo group). In order to reject the null hypothesis of an identical proportion of favorable outcome in the two groups with a type 1 error alpha = 0·05 (two tailed), a power of 80% is achieved with a sample size of n = 740 patients (n = 370 per treatment group). Accounting for possible treatment failures, protocol violations, and dropouts, we plan to enroll n = 800 patients (n = 400 per treatment group).
Data and safety monitoring
An independent DSMB will oversee the conduct of the trial. The primary safety end-points mortality and death or dependency (MRS 4–6) 90 (±10) days after stroke will be analyzed sequentially after inclusion of 100, 200, 300, 500, and 800 patients. A Lan-DeMets alpha-spending function will be used to control for the overall alpha level, using Hwang-Shih-DeCani boundaries (parameter 1·2). The stopping rule proposed to the DSMB is to stop the trial after an interim analysis if the proportion of death, or the proportion of the combined end-point death or dependency in the alteplase group exceeds the proportion in the placebo group with a chi-square test value greater than the threshold defined by the alpha-spending function (one-sided test, overall alpha level of 0·10 for each end-point). The occurrence of SICH (as defined in SITS-MOST, ECASS II, NINDS) and PH-2 will also be compared between the test and the control arm but will not be used as end-points for formal stopping rules. Formally, these variables will not be considered as sequentially analyzed. In any case of concern about the safety of participants the DSMB will make a recommendation to the steering committee about continuing, stopping, or modifying the trial.
Study organization and funding
WAKE-UP is an investigator-initiated trial launched by a consortium of academic and enterprise partners. University Medical Center Hamburg-Eppendorf is the sponsor. The trial will be organized by a central coordinating center located at the sponsor and six national coordinating centers. WAKE-UP will be conducted in approximately 40–60 centers in six European countries. The steering committee manages the trial. WAKE-UP receives funding from the European Union (EU) Seventh Framework Programme (FP7/2007–2013) under grant agreement no. 278276 (WAKE-UP).
WAKE-UP is registered with the EU Clinical Trials Register (EudraCT no. 2011-005906-32) and ClinicalTrials.gov (Clinical-Trials.gov Identifier NCT01525290).
Conclusion
WAKE-UP is the first randomized, controlled trial of stroke thrombolysis dedicated specifically to the large group of patients with unknown time of symptom onset, e.g. wake-up stroke. Moreover, WAKE-UP is the first clinical trial to use the novel approach of DWI-FLAIR mismatch to prospectively identify patients likely to benefit from treatment with i.v. tPA. The imaging criteria used will ensure the enrollment of patients with ischemic lesions likely to be less than 4·5 h old who are likely to benefit from thrombolysis. If the trial is positive, it will be the first evidence that applying MRI criteria to select patients for thrombolysis in acute stroke is beneficial. This will represent a paradigm change and a scientific breakthrough toward an imaging-guided, individually tailored, acute stroke treatment. If positive, WAKE-UP is expected to change clinical practice and to make available effective and safe treatment for a large group of acute stroke patients currently excluded from specific acute treatment. By this, WAKE-UP will aid in reducing the overall burden of stroke.
WAKE-UP consortium
University Medical Center Hamburg-Eppendorf, Hamburg, Germany – Christian Gerloff (Coordinator), Götz Thomalla (Deputy Coordinator), Jens Fiehler, Saskia Borregard, Bastian Cheng, Celine Otten
Aarhus University Hospital, Aarhus, Denmark – Leif Østergaard, Claus Z. Simonsen, Grethe Andersen
Charité – Universitätsmedizin Berlin, Berlin, Germany – Jochen B. Fiebach, Martin Ebinger, Matthias Endres, Ivana Galinovic, Anna Kufner, Kati Jegzentis, Jan Jungehülsing
Institut d'Investgació Biomèdica de Girona, Girona, Spain – Salvador Pedraza, Joaquín Serena, Josep Puig, Gerard Blasco, Mar Castellanos, Jorge Guibernau
University of Leuven, Leuven, Belgium – Vincent Thijs, Stefan Sunaert, Robin Lemmens, Evelyn Marcelis
Hospices Civils de Lyon, Lyon, France – Norbert Nighoghossian, Tae-Hee Cho, Pascal Roy, Delphine Bertram, Florent Boutitie, Yves Berthezène, Laurent Derex
University of Glasgow, Glasgow, UK – Keith Muir, Krishna Dani Stroke Alliance for Europe, Brussels, Belgium – Markus Wagner, Clare Walton, Joanna Knight
Fraunhofer MEVIS, Bremen, Germany – Matthias Guenther, Jan Klein, Benjamin Geisler
Mediri GmbH, Heidelberg, Germany – Johannes Gregori, Andr, Bongers, Johannes Heitz
ZytoService Deutschland GmbH, Hamburg, Germany – Enno Scheel, Pia Sundermann, Alexander Schmitz, Mirco Schaecke GABO:mi Gesellschaft fuer Ablauforganisation: Milliarium mbH & Co. KG, Munich, Germany – Birgit Fuchs, Annina Sorgner
ORION Clinical Services Ltd, Berkshire, UK (ORION) – Paul Hunter, Fabrice Chartier, Jörg Rennecke
WAKE-UP boards and institutions
Steering committee: Christian Gerloff (Chair), Götz Thomalla (Coordinating Investigator), Jochen B. Fiebach, Claus Z. Simonsen, Salvador Pedraza, Vincent Thijs, Norbert Nighoghossian, Keith Muir, Matthias Endres, Ian Ford
CIRB: Salvador Pedraza (Chair), Jochen B. Fiebach, Jens Fiehler
Biostatistics: Pascal Roy, Florent Boutitie
Independent DSMB: Marc Hommel (Chair), Kennedy Lees, Karl Wegscheider