
Abstract
Background
Telemedicine may facilitate the selection of stroke patients who require emergency transfer to a comprehensive stroke center to receive additional therapies other than intravenous tissue plasminogen activator.
Aims and/or hypothesis
We sought to analyze frequency, patient characteristics, and specific therapies among emergently transferred patients within the telemedical Stroke East Saxony Network.
Methods
We reviewed consecutive patients who were transferred emergently from remote spoke sites to hub sites. Certified stroke neurologists performed teleconsultations 24/7, with access to high-speed videoconferencing and transfer of brain images. Emergent transfers were initiated when considered necessary by the stroke neurologist.
Results
In 2009 and 2010, we conducted 1413 teleconsultations and subsequently recommended transfer in 339 (24%) patients [mean age 64 ± 14 years, 54% males, median National Institutes of Health Stroke Scale score 5 (interquartile range, IQR 12). The mean teleconsultation-to-arrival time was 1·7 ± 0·8 h (median 1·6 h). Sixty-eight (20%) transferred patients had a nonstroke diagnosis. The remaining 271 (80%) patients had stroke diagnoses [ischemic stroke, 114 (34%); transient ischemic attack, 8 (2%); and intracranial haemorrhage, 149 (44%)]. Forty (35%) ischemic stroke patients received tissue plasminogen activator at spoke sites (‘drip and ship’). Of the 240 stroke patients emergently transferred to the main hub site, 119 (49·6%) received at least one specific stroke therapy.
Conclusion
A remarkable number of stroke patients can be transferred within a telemedical network to enable the delivery of specific stroke therapies that require advanced multispecialty expertise. Whether associated logistic efforts and costs have an impact on patients' clinical outcomes needs to be evaluated.
Introduction
Although improvements in stroke care delivery maximize the chance for patients to receive specific stroke therapies, only a minority has access to potentially beneficial approaches due to logistic challenges and the lack of multispecialty expertise (1). Even intravenous tissue plasminogen activator (IV tPA) (2), which remains the only effective and approved therapy for ischemic stroke (3,4) available at any level stroke center, is underutilized, particularly in neurologically underserved areas (5). Most specific stroke therapies like endovascular and surgical procedures are invasive, labor- and resource-intensive, and predominantly applicable to comprehensive stroke centers. Consequently, overall treatment rates remain low (6–8).
This shortcoming can be overcome by telemedicine, which enhances the availability of acute stroke care in rural areas, where most of the primary hospitals are located (9,10). It has been shown that telemedicine in stroke constitutes a reliable method for initial neurological assessment, remote reading of brain images, and clinical decision making on IV tPA (11–13). Telemedicine in stroke can also be used for selection of patients potentially amenable to specific stroke therapies available at comprehensive stroke centers but not at primary hospitals. However, data on emergency transfers within a telemedicine stroke network in order to deliver specific stroke therapies to these patients have not been reported yet.
Aims and/or hypothesis
We sought to analyze frequency, patient characteristics, and specific therapies among emergently transferred patients within the telemedical Stroke East Saxony Network (SOS-NET; ‘East’ translates into the German Ost) in order to facilitate future transfer management of these patients.
Methods
SOS-NET
The SOS-NET has been established in 2007 utilizing the hub-and-spoke model, which constitutes the most common telemedicine facilitated system (14). The hub is usually an urban tertiary care facility or a comprehensive stroke center from where stroke neurologists connect through high-quality videoconferencing to a remote rural hospital – the spoke site. Within the SOS-NET, the Dresden University Stroke Center (DUSC) serves as the main hub and now co-operates with 14 spoke sites (in 2009, 9; in 2010, 13 spoke sites), covering an overall population of 1·7 million people in the eastern part of Saxony, Germany (Fig. 1). Currently, approximately 3·350 stroke patients present to these spoke sites each year (in 2009, 2·150; in 2010, 3·050 stroke patients). In 2010, two secondary care hospitals joined the SOS-NET, serving as additional hubs, with one of them conducting teleconsultations three-days per month. The other center exclusively delivers neurosurgical service to acute stroke patients but does not conduct teleconsultations. The distances between the DUSC and the rural spoke sites range from 15 km (about 10 mi) being the closest to 120 km (about 75 mi) being the furthest. One spoke site is located in the urban area about 1·5 km (about one-mile) away from the DUSC and mostly covers in-hospital strokes.
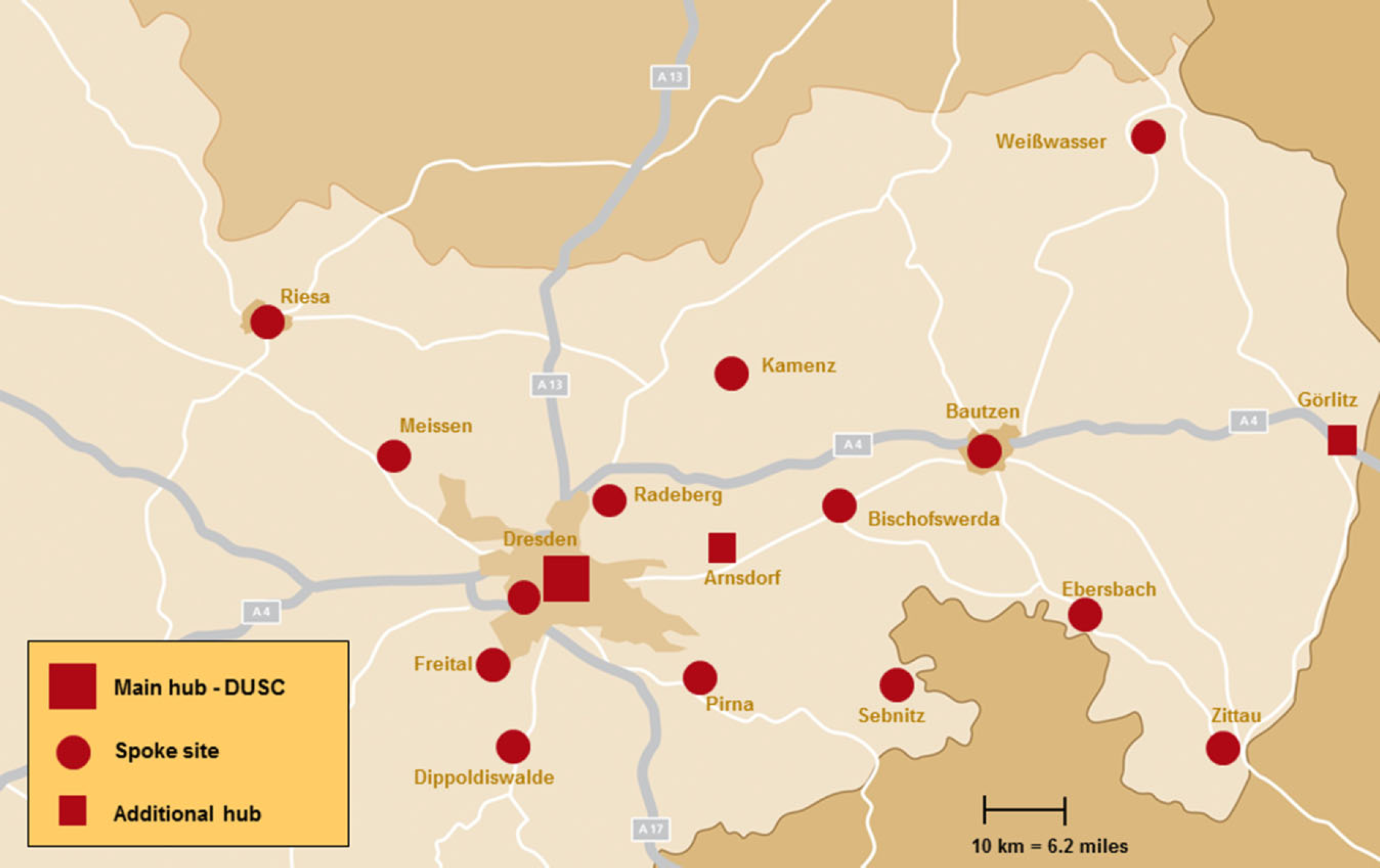
Map of the Stroke East Saxony Network region in the eastern part of Saxony, Germany (status as of March 2011). DUSC, Dresden University Stroke Center.
Teleconsultations
The hub site is equipped with a bidirectional high-speed audio-visual system and a teleradiology application allowing immediate transfer of brain images via a virtual private network for remote review. The teleconsultations are performed 24/7 by stroke neurologists who are experienced in the treatment of acute stroke patients and are trained and certified in stroke brain imaging interpretation by an expert neuroradiologist (R. v. K.). The stroke neurologist can rely on a 24/7 on-call service of board-certified neuroradiologists to discuss difficult differential diagnoses and the indication for neuroradiological interventions. The spoke site is equipped with a mobile telemedical system (Meytec™, Werneuchen, Germany) that is positioned in the emergency department. Calls from the spoke sites are made on the following indications: clinically suspected acute ischemic stroke (AIS) with potential eligibility for thrombolysis; decreased level of consciousness of unknown etiology; brain-stem symptoms; progressive stroke; and uncertainty about diagnostic or therapeutic procedures. The stroke neurologist performs a complete real-time neurological examination, including the National Institutes of Health Stroke Scale (NIHSS), by videoconference from a stationary workstation, which is located at the DUSC at daytimes and from a portable notebook using Universal Mobile Telecommunications System (UMTS) connection for wireless data transfer at night shifts. Brain computed tomography (CT) or magnetic resonance imaging (MRI) using the Picture Archiving and Communication System is reviewed.
Emergent transfers
Indications for emergent transfers were discussed during the teleconsultation and ultimately recommended at the discretion of the stroke neurologist or as a second decision after neurological worsening has occurred subsequently. The latter and patients with nonstroke diagnoses were excluded from teleconsultation-to-arrival-time calculations.
We reviewed patients who were transferred emergently from the remote spoke sites to the main hub site in 2009 and 2010 and to the two additional hub sites in 2010. Frequencies of teleconsultations and patient characteristics (including NIHSS) were collected prospectively as part of our quality telestroke assurance for all hub sites, whereas the teleconsultation-to-arrival time, specific stroke therapies, and clinical outcomes were analyzed exclusively for the main hub site due to missing data. Subsequent analyses were conducted retrospectively. Specific stroke therapies were defined as any endovascular and neurosurgical procedures, as well as adjuvant therapeutic hypothermia. We collected the modified Rankin Scale (mRS) score at discharge for each patient who was transferred to the main hub site as stated in our institutional quality assurance reports. Favorable outcome was defined as an mRS score of 0–2, and unfavorable outcome as an mRS score of 3–5 or death. Symptomatic intracerebral haemorrhage (sICH) following IV tPA was captured for all thrombolysed patients within the SOS-NET (including shipped and nonshipped patients). Symptomatic ICH was defined as any haemorrhage on CT or MRI associated with an increase of more than four points on the NIHSS score within 36 h. Our analysis was approved by the institutional review board.
Statistical analysis
All variables were entered into a Microsoft Excel spreadsheet (Microsoft Corporation, Redmond, WA, USA). Continuous variables are presented as mean (standard deviation) or median (range). Noncontinuous variables are presented as percentages. An unpaired t-test was performed for continuous data and a chi-squared test for categorical data using the STATA statistical package 12·1 (StataCorp LP, College Station, TX, USA). Statistical significance was achieved at a two-tailed P-value of <0·05.
Results
Patients
In 2009 and 2010, we performed 1413 teleconsultations within the SOS-NET: mean age 71 ± 14 years, 50% male, median NIHSS 5 [range 0–41; interquartile range (IQR) 12], 81% acute strokes. Of these 1413 teleconsultations, 339 (24%) led to emergent transfers of patients to the main hub site (n = 300) and the two additional hub sites (n = 18 and n = 21, respectively). The mean age of all transferred patients was 64 ± 14 years, 54% were male, and the median NIHSS score was 5 (range 0–40; IQR 12). Ninety-three (27%) patients were less than 55 years old (as opposed to 14% of all teleconsultations). Within the SOS-NET, 698 patients had an AIS, of which 270 (39%) received IV tPA at spoke sites (= rate within the SOS-NET). Of these 270 AIS patients, 40 (15%) were subsequently transferred to the hub site in a ‘drip and ship’ approach, and 230/270 (85%) stayed at the spoke sites. Clinical characteristics and final clinical diagnoses of emergently transferred patients to hub sites are presented in Table 1.
Clinical characteristics and final diagnoses of all patients who were emergently transferred to the hub sites within the SOS-NET
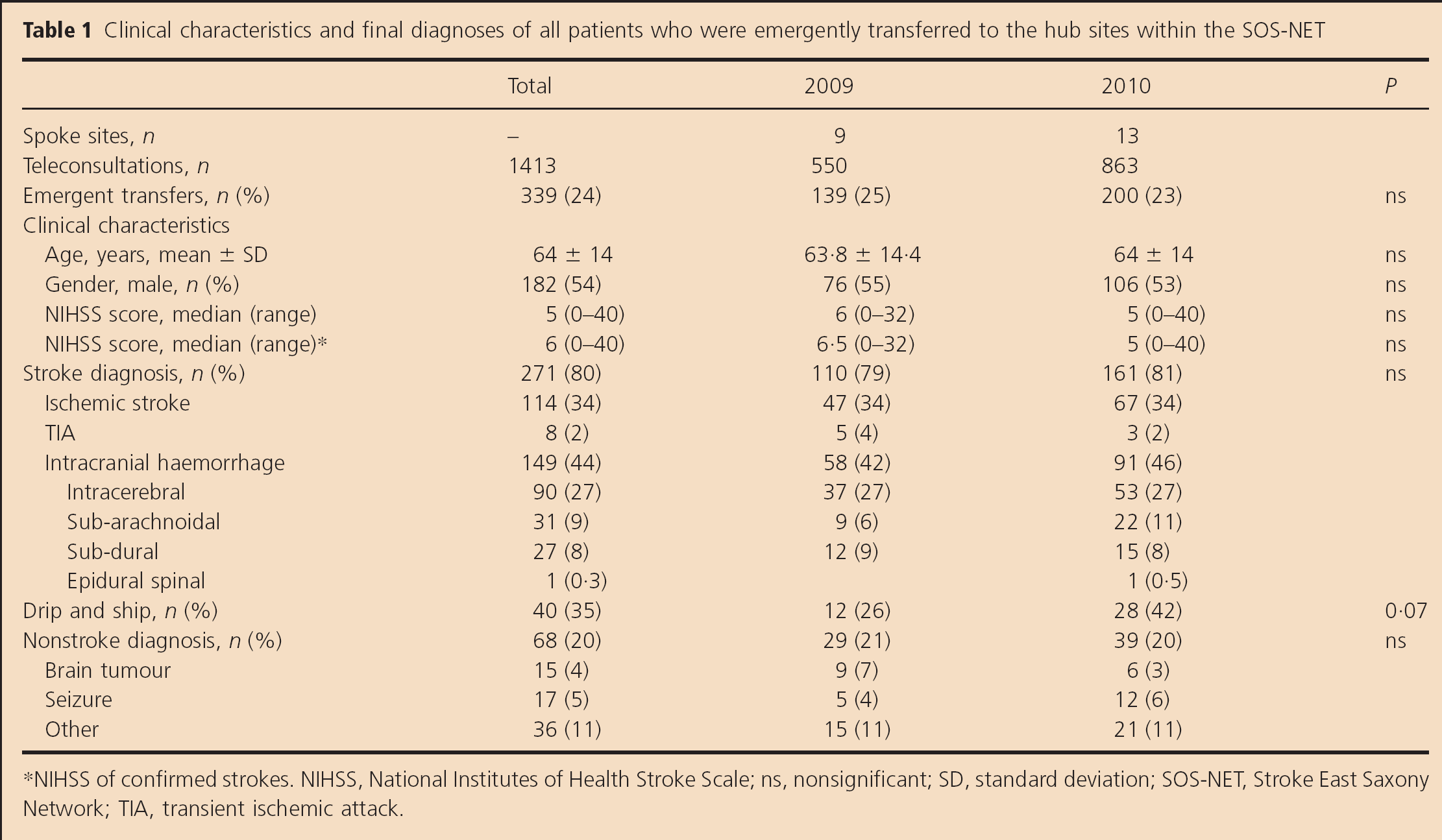
NIHSS of confirmed strokes. NIHSS, National Institutes of Health Stroke Scale; ns, nonsignificant; SD, standard deviation; SOS-NET, Stroke East Saxony Network; TIA, transient ischemic attack.
Sixty-eight (20%) of all emergently transferred patients had a nonstroke diagnosis, with 15 (4%) being brain tumours, 17 (5%) being seizures, and 36 (11%) being other etiologies (e.g. migraine, meningitis, Guillain–Barré syndrome, non-ST-elevating myocardial infarction, and functional disorders). Of the remaining 271 transferred patients, 114 (34%) had an AIS, 8 (2%) had a transient ischemic attack, and 149 (44%) had an intracranial haemorrhage.
Transfer time and specific stroke therapies at the main hub site
The mean teleconsultation-to-arrival time to the main hub site was 1·7 ± 0·8 h (median 1·6 h; IQR 0·98). We observed a trend toward an improved teleconsultation-to-arrival time from 2009 to 2010 but is not statistically significant (2009: 1·8 ± 0·9 h; 2010: 1·7 ± 0·8 h; P = 0·6).
Of the 240 patients with a stroke diagnosis who were emergently transferred to the main hub site, 119 (49·6%) received at least one specific stroke therapy. Overall, 174 specific stroke therapies were performed during the two-years at the main hub site, with a trend toward an increased number of procedures per patient performed between 2009 and 2010 (procedures per patient; 2009: 0·66 ± 0·89; 2010: 0·77 ± 0·89; P = 0·3). Moreover, we found a nonsignificant increase in the number of stroke patients who received at least one specific stroke therapy from 2009 (46/105; 44%) to 2010 (73/135; 54%; P = 0·115). Table 2 demonstrates the specific stroke therapies. Of note, we enrolled 31 acute stroke patients (13%) in clinical multicenter trials after transferal to the main hub site.
Performed specific stroke therapies and clinical outcomes for stroke patients who were emergently transferred to the main hub site
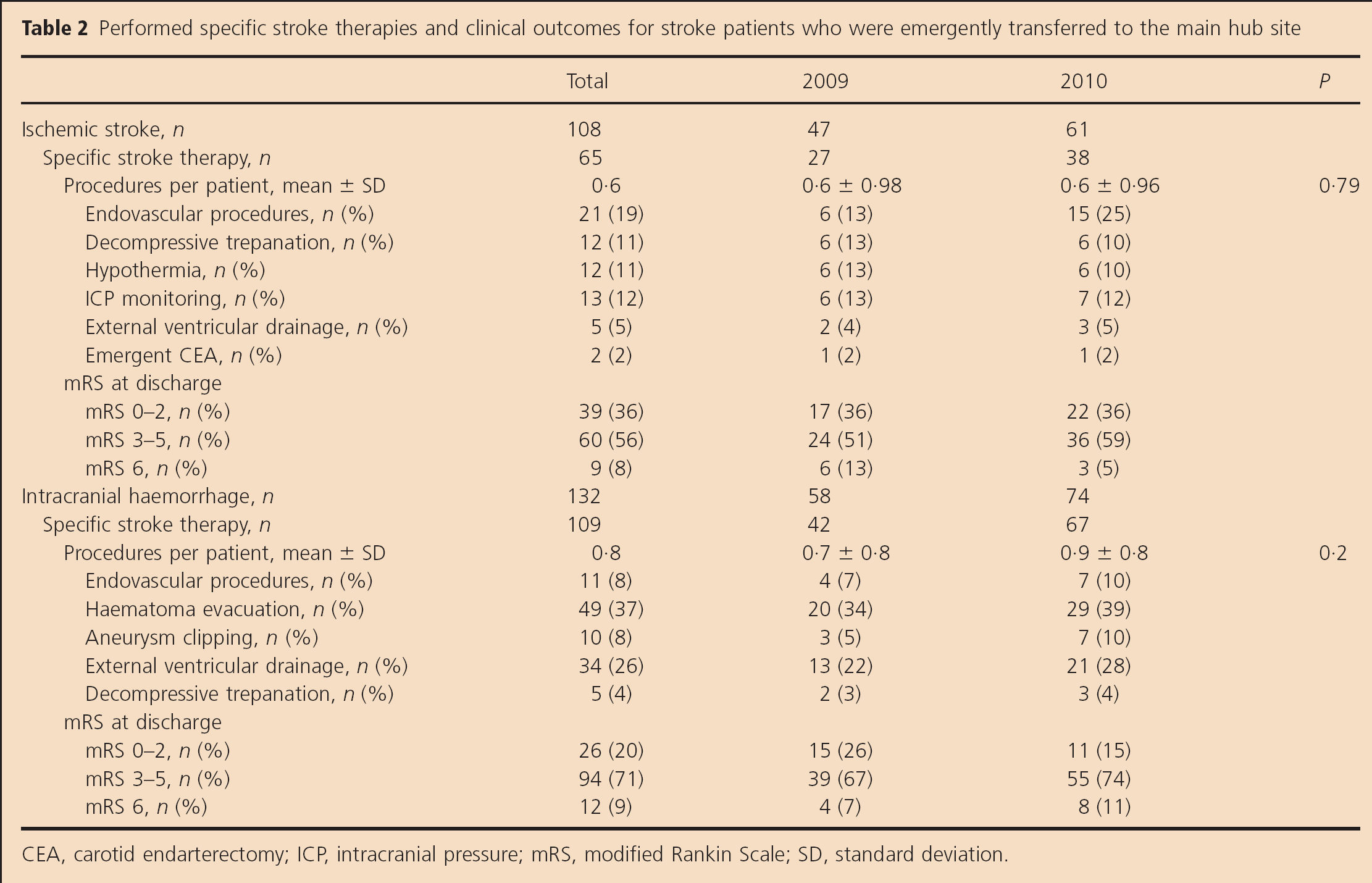
CEA, carotid endarterectomy; ICP, intracranial pressure; mRS, modified Rankin Scale; SD, standard deviation.
Clinical outcomes
At discharge, 65/240 (27%) stroke patients emergently transferred to the main hub site had a favorable outcome (mRS 0–2), 154/240 (64%) had an unfavorable outcome, and 21/240 (9%) patients were deceased. Of the 40 IV tPA patients who were emergently transferred in a ‘drip and ship’ approach, 12/40 (30%) had a favorable outcome, 22/40 (55%) had an unfavorable outcome, and 6/40 (15%) patients were deceased at discharge. Symptomatic ICH occurred in none of these patients [as opposed to a sICH rate of 7·8% (18/230) in nonshipped IV tPA patients]. Table 2 demonstrates functional outcomes for transferred stroke patients with regard to the ultimate diagnosis.
Discussion
Our two-year analysis of telemedicine in stroke demonstrated that a remarkable number of patients (one-fourth of all teleconsultations) were transferred to the hub sites and received specific stroke therapies not available at primary hospitals (half of the transferred stroke patients). In addition, one-third of the patients with AIS received IV tPA ‘drip’ at a spoke site before being ‘shipped’ to the hub site. The latter results are in line with previous observations that telemedical stroke services increase the utilization of IV tPA in primary hospitals (10,15,16). Moreover, the large proportion of patients with stroke mimics and of patients with primary intracranial haemorrhages underlines that our telemedicine service has helped identify ischemic stroke patients and facilitated diagnosis and treatment for other patients.
Implementation of stroke unit care in primary hospitals enables organized stroke care for standard stroke patients. Meanwhile, primary hospitals comprise multidisciplinary stroke teams available 24/7 and maintain tight co-operations with tertiary stroke centers in order to receive continuous medical education (e.g. stroke nurses and NIHSS training courses) and regular spoke site visits (17). This may be reflected in an observed slight increase in teleconsultations over the reported two-years, indicating that improved local expertise as an awareness of even subtle stroke-related symptoms and clinical constellations potentially amenable to specific stroke therapies grows. However, with evolving imaging modalities (18) and novel supplemental therapies, (1) stroke care became more than just basic therapy, making multispecialty stroke expertise essential. The fact that almost one out of two patients transferred to our tertiary stroke center received at least one specific stroke therapy underlines the importance of having multispecialized stroke centers attached to primary hospitals. Furthermore, specific stroke therapies performed at our center increased over the reported two-years (without being statistical significant), emphasizing that primary hospitals are less able to pursue recent progress in these therapies. Nevertheless, selecting the optimal patient to be transferred still remains a challenge, because enormous logistic efforts and costs need to be considered. As recently suggested, patients receiving IV tPA, particularly those with moderate to severe strokes, may benefit from transferring to the hub site within a stroke telemedical network, as post-IV tPA care at the spoke site has been identified as a predictor of poor outcome (19). Another potential approach could be stratification by age, as younger patients usually require more comprehensive investigations than the elderly and, therefore, are more likely to be transferred (almost one-third of the patients transferred to one of our hub sites were younger than 55 years). The latter might explain the low median NIHSS score in our patient population. Decision making for emergent transfer may follow a lower threshold in younger patients in order not to miss a potentially beneficial specific stroke therapy, even in those with minor strokes. Future studies need to address whether a specific transfer algorithm can be developed to simplify the triage of patients and spare hospital-linked resources within a stroke telemedical network, as recently shown for interhospital transfers in trauma patients (20).
Most of the specific stroke therapies provided by tertiary stroke centers are time sensitive (21–23). Therefore, transfer time is a crucial component within a stroke telemedical network, which can be significantly reduced by stroke transfer protocols (24). A recent study evaluating certain time intervals within a stroke telemedical network showed that a prolonged transfer time might contribute to additional patient harm (25). Our median teleconsultation-to-arrival time (96 min) appears short as compared with those reported by Audebert et al. (basilar thrombosis, 147 min; malignant infarcts, 161; and intracranial haemorrhages, 134), indicating a reasonable transfer management within our telemedical network. It should be mentioned that our teleconsultation-to-arrival times are of limited comparability with published studies on time intervals within stroke telemedical networks because distances between spoke and hub sites may differ significantly. Nonetheless, it appears clear that each of the time intervals is prone to potential improvement, mostly by increasing the awareness of stroke symptoms among non-neurologists in order to initiate teleconsultation immediately after primary admission and optimizing transport organization. Therefore, regular visits to the spoke sites and corresponding training courses should be carried out by the hub sites.
Interestingly, our data are in line with recent data that suggest that telemedicine may enhance the enrollment of patients into time-sensitive acute stroke trials (26). Thirteen percent of the patients transferred to the main hub site were enrolled into a clinical trial. This is an important observation because recruitment rates in large acute stroke trials are decreasing (27).
Our analysis has limitations. Although most of the data were collected prospectively as part of our quality assurance, some were gathered from various retrospective sources, leaving room for misclassification and information bias. In addition, we did not analyze teleconsultations from patients who were not emergently transferred to one of the hub sites, allowing no comparisons with our reported patient population. Nevertheless, in order to define a target population, which might have the most benefit from emergent transfers, we plan to conduct a prospective investigation, comparing transferred to nontransferred patients. Finally, our data may not be generalizable to other stroke telemedical networks.
In conclusion, our analysis shows that a remarkable number of stroke patients can be transferred within a telemedical network, enabling delivery of specific stroke therapies that require advanced multispecialty expertise to these patients. Whether associated logistic efforts and costs ultimately have an impact on patients' clinical outcomes needs to be further evaluated.