
Abstract
Background and purpose
Heart failure is an independent risk factor for stroke. Anticoagulation is effective for prevention of cardio-embolic stroke secondary to atrial fibrillation or mechanical heart valves but is of uncertain benefit in heart failure patients. We performed this meta-analysis to obtain the best estimates of the efficacy and safety of warfarin as compared with antiplatelet therapy in patients with systolic heart failure who are in sinus rhythm.
Methods and results
A systematic search was performed using PubMed and Central Register of Controlled Trials databases for all randomized controlled trials, which compare warfarin with antiplatelet therapy given for at least one-month in heart failure patients with sinus rhythm and report at least one of the following outcomes: ischemic stroke, death, myocardial infarction, hospitalization due to worsening heart failure, intracranial hemorrhage, and major hemorrhage. Four randomized controlled trials involving adjusted-dose warfarin (4187 subjects) were included. When compared with antiplatelet therapy, warfarin reduced ischemic stroke by 0·74% per year (RR 0·49; 95% CI: 0·32–0·73: P = 0·0006; Number needed to treat = 135) but increased major hemorrhage by 0·99% per year (RR 2·15; 95% CI: 1·55–2·99: P < 0·00001; Number needed to harm = 101). Warfarin did not significantly affect the risk of death, myocardial infarction, hospitalization due to heart failure or intracranial hemorrhage as compared with antiplatelet therapy.
Conclusion
Warfarin as compared with antiplatelet therapy reduces risk of ischemic stroke, does not significantly affect death, myocardial infarction, hospitalization due to heart failure or intracranial hemorrhage and increases major hemorrhage in heart failure patients who are in sinus rhythm.
Introduction
Heart failure has been recognized as an independent risk factor for ischemic stroke. Its incidence is approximately 10 persons per 1000 population over 65 years of age and is increasing because of the ageing of the population and the increasing survival of patients with chronic cardiac conditions (1). More than 6 million adults over 18 years of age in the USA have heart failure and it is estimated that there will be a 25% increase in the prevalence of heart failure by 2030. Heart failure is also one of the most common causes of hospitalization and accounts for a substantial burden of mortality and morbidity (1). Heart failure is associated with formation of intracardiac thrombi as a result of stasis, endocardial dysfunction, and a systemic hypercoagulable state, and these thrombi can embolize to cause stroke. Patients with heart failure are at risk of developing atrial fibrillation, which predisposed them to increase risk of thromboembolic complications. Warfarin is highly effective for the prevention of cardio-embolic stroke associated with atrial fibrillation, but its role in patients with systolic heart failure who are in sinus rhythm remains uncertain.
Over the last decade, randomized controlled trials have evaluated the efficacy and safety of warfarin for the prevention of major cardiovascular events in systolic heart failure patients with sinus rhythm (2–5). We performed a meta-analysis of all these trials in order to obtain best estimates of the efficacy and safety of warfarin as compared with antiplatelet therapy, in patients with systolic heart failure who are in sinus rhythm.
Methods
We hypothesized that warfarin is more efficacious than antiplatelet therapy for primary prevention of cardiovascular events in patients with systolic heart failure and sinus rhythm. We also hypothesized that warfarin is associated with a higher risk of major hemorrhage, including intracranial hemorrhage, as compared with antiplatelet therapy. Our research questions were: In patients with systolic heart failure who are in sinus rhythm, does warfarin (International Normalized Ratio [INR] range of 2–3) compared with antiplatelet therapy including aspirin (81–325 mg od) or clopidogrel (75 mg od) result in lower rates of: (1) ischemic stroke, (2) death, (3) myocardial infarction (MI), and (4) hospitalization due to worsening heart failure? Furthermore, does this intervention also increase the rates of: (1) intracranial hemorrhage and (2) major hemorrhage?
Criteria for trial selection
To be included, trials had to meet all of the following criteria: (1) randomized studies, (2) inclusion of patients with heart failure, (3) comparison of warfarin with antiplatelet therapy given for at least one-month, and (4) report at least one of the following outcomes: ischemic stroke, death, MI, hospitalization due to worsening heart failure, intracranial hemorrhage, and major hemorrhage. Studies were excluded if they involved heart failure patients with atrial fibrillation, prosthetic cardiac valves or mitral stenosis, unless data were presented separately for patients without these features. However, studies that included heart failure patients with sinus rhythm on enrolment but subsequently developed atrial fibrillation will be included and were stated otherwise. Three physician reviewers determined whether trials met inclusion criteria, with disagreements resolved by joint review and consensus.
Selection of outcomes
The main outcome(s) of interest were (1) ischemic stroke; (2) death; (3) MI; (4) hospitalization due to worsening heart failure; (5) intracranial hemorrhage; and (6) major hemorrhage.
Data extraction
Unconfounded randomized trials testing long-term (⩾ one-month) use of warfarin as a primary prevention in patients with heart failure who were in sinus rhythm were identified by computerized search of the PubMed/Cochrane Central Register of Controlled Trials databases (from 1966 to June 2012, not restricted by language). Appendices 2 and 3 describe the search terms and strategies for each database.
Three physician reviewers (AYLL, JWE, RGH) independently extracted data from published sources (regarding study design, number of patients, eligibility, method of randomization, interventions, blinding, quality of INR control, completeness of follow-up and outcomes. The following outcomes were included in the meta-analysis unless otherwise specified: ischemic stroke, death, MI: both fatal and nonfatal, hospitalization due to worsening heart failure, intracranial hemorrhage, and major hemorrhage. The number of participants with strokes that underwent neuroimaging or autopsy to reliably distinguish between ischemic or hemorrhagic stroke varied and was not consistently reported; consequently all strokes (ischemic and hemorrhagic) were included in the efficacy outcome. Undefined strokes without neuroimaging were counted as ischemic. Transient ischemic attacks were not included. We accepted each trial's definition of major hemorrhage. Data on all stroke (fatal and nonfatal stroke) or nonfatal stroke were included if the ischemic stroke outcome was not specifically provided in the trials. Data on nonfatal MI or unspecified MI were included if the composite fatal and nonfatal MI outcome was not specifically provided in the trials. Data on central nervous system (CNS) hemorrhage were included if intracranial hemorrhage outcome was not specifically provided in the trials. Similarly, if the trial did not include any data on intracranial or CNS hemorrhage and stated that all the major hemorrhage was not of CNS origin, the number of intracranial hemorrhage event in that trial was considered as zero by default. Data from trials that included subjects with subsequent development of atrial fibrillation during follow-up will be used only if data excluding subjects with atrial fibrillation were not available. Agreement was assessed using Cohen's unweighted kappa statistic. The quality of the randomized clinical trials was assessed using the Jadad scale (6). Disagreements were resolved by joint review and consensus.
Study selection
The process of study selection is outlined in Fig. 1. The assessment of the reviewer agreement at the level of study selection from full text articles using Cohen's weighted kappa was 1 (SD = 0). Data on all stroke (fatal and nonfatal stroke) from the HELAS (Heart failure Long-term Anti-thrombotic Study) & WATCH (Warfarin and Anti-platelet Therapy in Chronic Heart Failure) trials and nonfatal stroke from the WASH (Warfarin/Aspirin Study in Heart failure) trial were included because the ischemic stroke outcome was not specifically provided in the trials. Data on nonfatal MI from WATCH trial or unspecified MI from the HELAS and WARCEF (Warfarin Aspirin in Reduced Cardiac Ejection Fraction) trials were included because the composite fatal and nonfatal MI outcome was not specifically provided in the trials. Data on CNS hemorrhage from WATCH trial was included because the intracranial hemorrhage outcome was not specifically provided in that trial. Since the WASH trial did not include any data on intracranial or CNS hemorrhage and stated that all the major hemorrhage was not of CNS origin, the number of intracranial hemorrhage event in that trial was considered as zero by default. Data from all the four trials were used for this meta-analysis. However, both the WATCH and WARCEF trials included patients who subsequently developed atrial fibrillation in their analysis, whereas the other two trials excluded them.
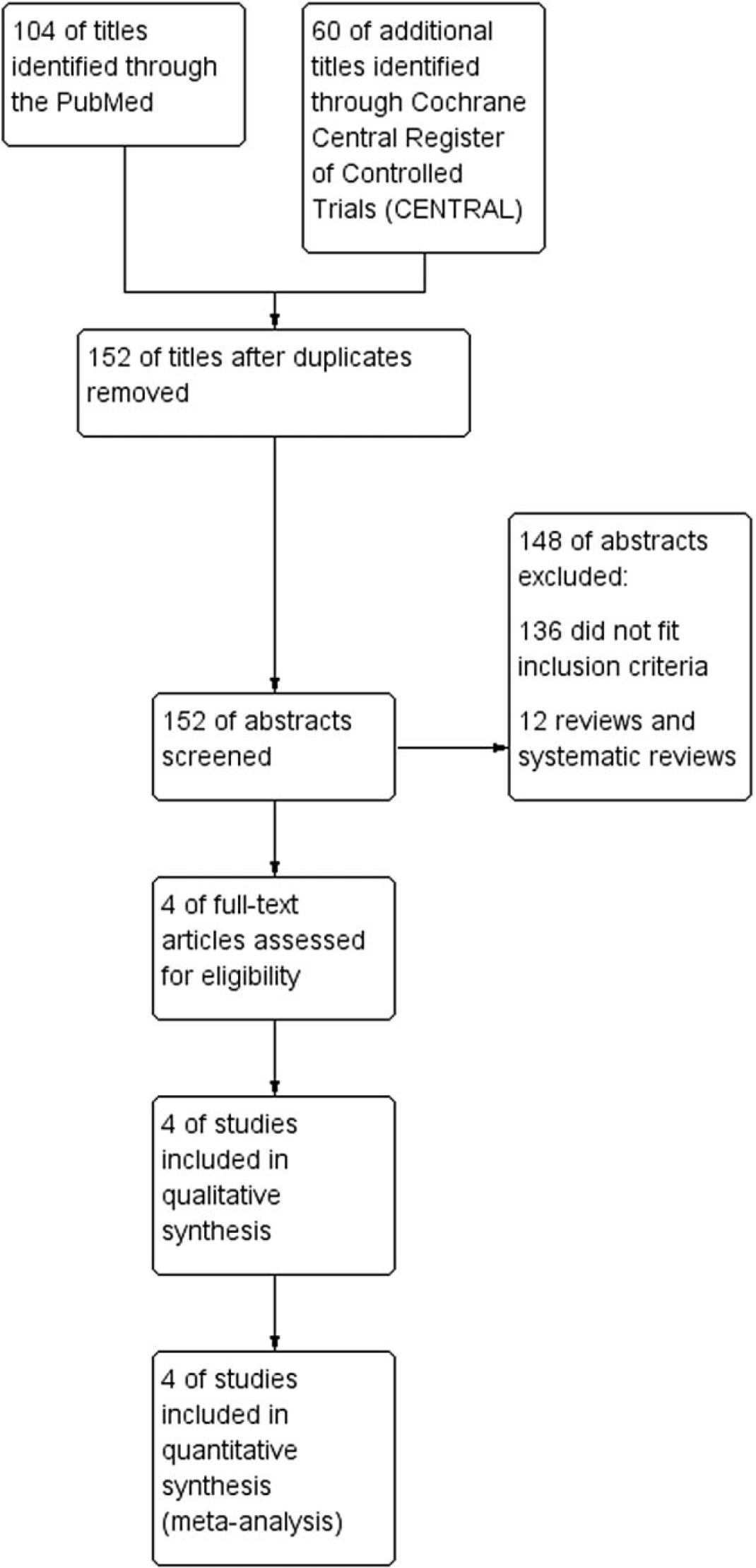
Process of study selection.
Statistical analysis
Analyses were based on the intention-to-treat principle. Pooled results are presented as relative risk and absolute risk reduction/increase with their respective 95% CIs. We calculated the pooled odds ratio using a random effects model (DerSimonian and Laird method) and compared these results with pooled odds ratios obtained using a Mantel–Haenszel fixed effects model (7). The absolute risk reduction is a weighted estimate of the difference in annualized event rates (7). Statistical homogeneity of the treatment effect (across trials and within a specific scenario) was tested using the QL statistic for the relative odds scale or the QW statistic with unequal weights for the absolute risk scale (7). Heterogeneity assessment was performed using the I2 index and chi-square test. Risk ratio and risk differences were calculated as alternative measures of association. We also reanalyzed the data by excluding low-quality trial (Jadad score < 3) to measure the strength of the association of the main analysis.
Publication bias was assessed using the Funnel plot regression. Estimates of relative risk reduction in individual trials were computed by subtracting the estimated odds ratio from 1. A two-sided P-value < 0·05 was considered as statistically significant. Calculations were done using RevMan version 5·1 (The Nordic Cochrane Centrem The Cochrane Collaboration 2011, Copenhagen, Denmark).
Results
Study characteristics
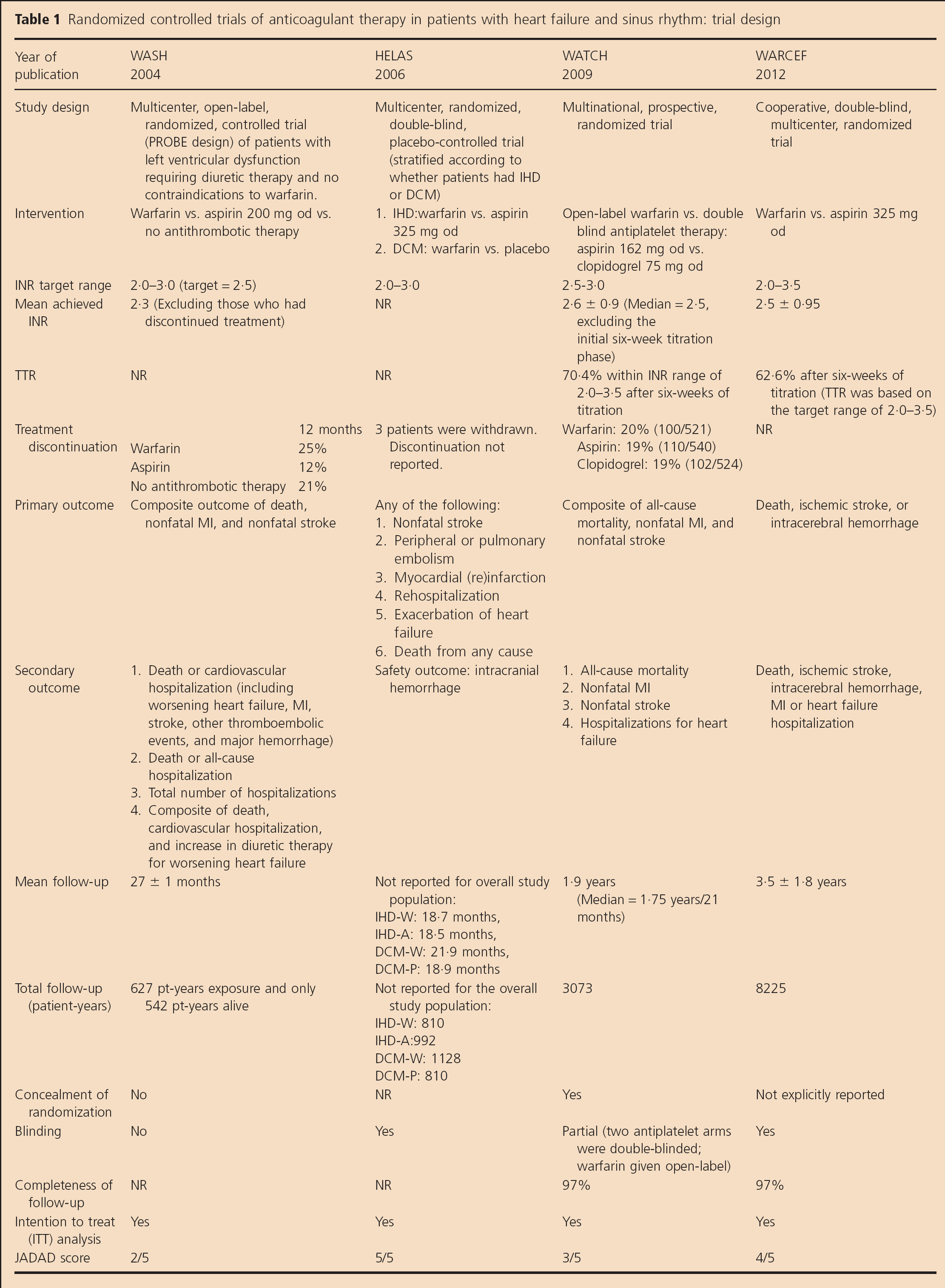
Four studies involving 4187 subjects were included. Two trials were double-blinded, whereas two others were open-label (Table 1). The mean patient age was 62 years, 82% were men, and the average left ventricular ejection fraction was 25% (Table 2). Follow-up averaged 2·3 ± 0·8years.
Randomized controlled trials of anticoagulant therapy in patients with heart failure and sinus rhythm: trial design
Randomized controlled trials of anticoagulant therapy in patients with heart failure and sinus rhythm: Patient characteristics
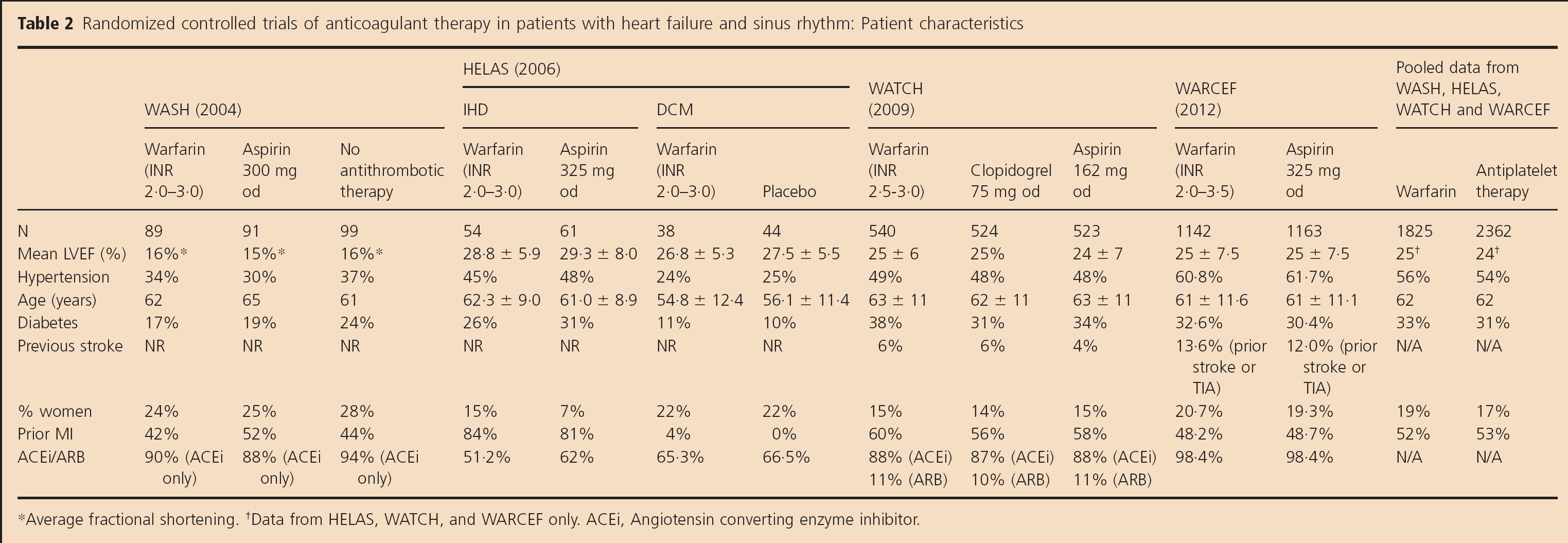
Average fractional shortening.
Data from HELAS, WATCH, and WARCEF only. ACEi, Angiotensin converting enzyme inhibitor.
Risk of bias
All the four studies were terminated prematurely with poor recruitment as one of the issue. Both HELAS and WARCEF trials were double blinded. The WATCH trial was partially blinded (the antiplatelet arms were double blinded, but the warfarin was given open labeled). The WASH trial utilized an open-blinded end-point (PROBE) design whereby both the patients and physicians were aware of the treatment allocation (either with warfarin, aspirin or no treatment), and the outcome adjudicators were blinded. The completeness of follow-up was not reported in WASH trial. In both the WARCEF and WATCH trials, 97% of their patients completed the follow-up, whereas the other two trials did not explicitly report their completeness of follow-up (Table 1).
Outcomes
All four trials contributed to the analysis of ischemic stroke (117 events), death (877 events), and MI (118 events). All four trials (4187 patients) contributed to the analysis of hospitalization due to heart failure (798 events) and major hemorrhage (164 events). The WASH, WATCH, and WARCEF trials (4072 patients) contributed to the analysis of the intracranial hemorrhage (22 events).
Ischemic stroke
Warfarin was associated with a 51% reduction in ischemic stroke as compared with antiplatelet therapy (1·87% vs. 3·53%, RR 0·49; 95% CI, 0·32–0·73, P = 0·0006) with an absolute risk reduction of 0·74% per year (Table 3). There was no statistical evidence of heterogeneity among the studies for the ischemic stroke outcome (I2 = 0%, χ2 = 2·53, P = 0·47) (Fig. 2).
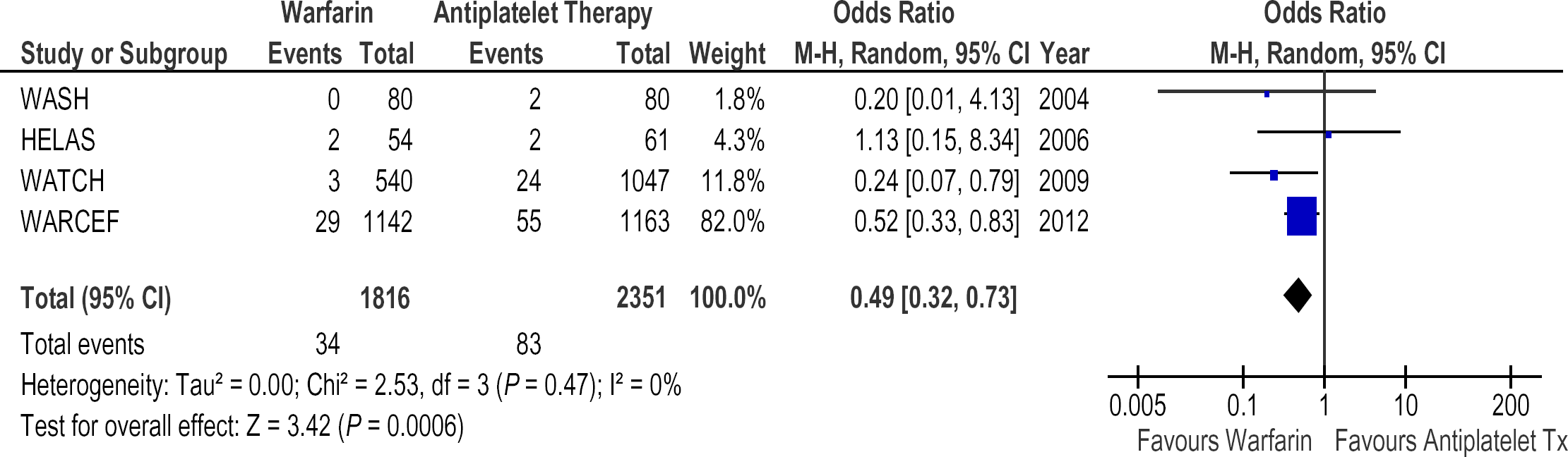
Relative risk of ischemic stroke in patients treated with warfarin vs. antiplatelet therapy (RE Model).
Death
There was no significant reduction in risk of death with warfarin as compared with antiplatelet therapy (21·53% vs. 20·67%, RR 1·00; 95% CI, 0·86–1·17, P = 0·96) (Table 3). There was no statistical evidence of heterogeneity among the studies for death outcome (I2 = 0%, χ2 = 1·66, P = 0·65) (Fig. 3).
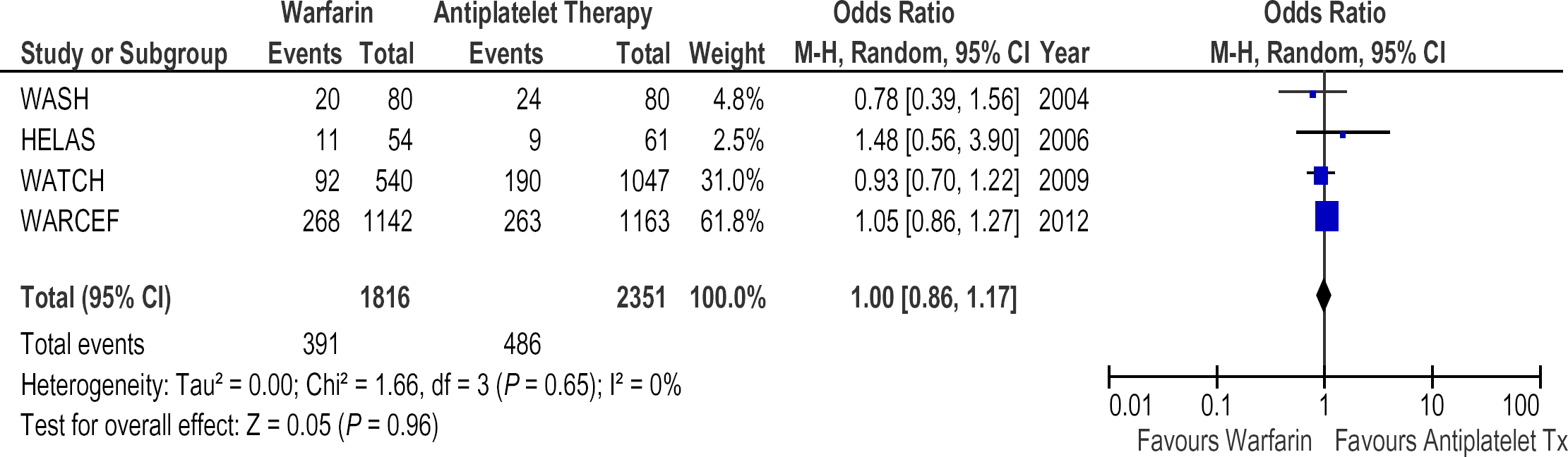
Relative risk of death in patients treated with warfarin vs. antiplatelet therapy (RE Model).
Pooled estimates of the risk and benefit of warfarin vs. antiplatelet therapy in patients with heart failure and sinus rhythm
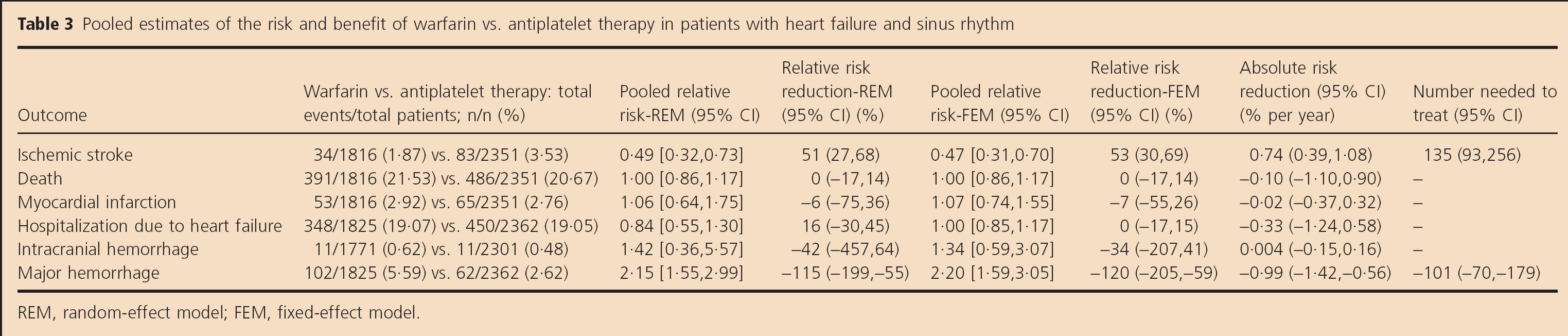
REM, random-effect model; FEM, fixed-effect model.
Myocardial infarction
There was no significant reduction in risk of MI with warfarin as compared with antiplatelet therapy (2·92% vs. 2·76%, RR 1·06; 95% CI, 0·64–1·75, P = 0·81) (Table 3). There was no statistical evidence of heterogeneity among the studies for MI (I2 = 28%, χ2 = 4·16, P = 0·24) (Fig. 4).
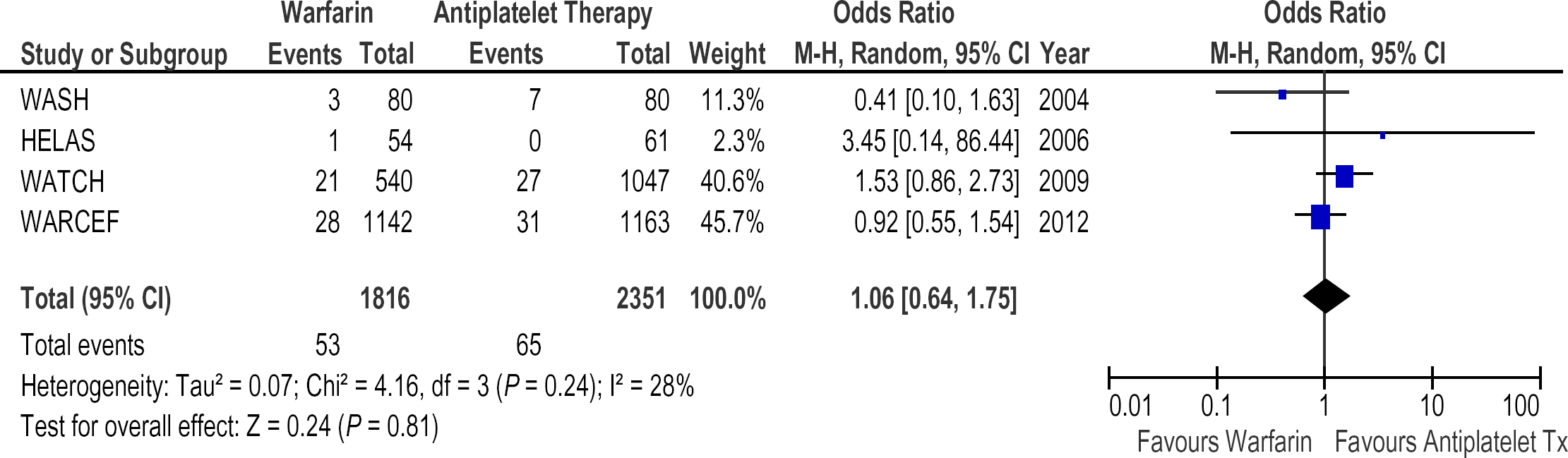
Relative risk of myocardial infarction in patients treated with warfarin vs. antiplatelet therapy (RE Model).
Hospitalization due to heart failure
There was no significant reduction in hospitalization due to worsening congestive heart failure with warfarin as compared with antiplatelet therapy (19·07% vs. 19·05%, RR 0·84; 95% CI, 0·55–1·30, P = 0·44) (Table 3). Both the WASH (OR 0·49; 95% CI, 0·25–0·96) and WATCH (OR 0·77; 95% CI, 0·59–1·01) studies showed a reduction in the rate of hospitalization due to worsening congestive heart failure with warfarin as compared with antiplatelet therapy. However, the WARCEF study, which contributed 442 of the combined total of 798 events from all the four studies, showed that warfarin compared with antiplatelet therapy was associated with an increase in hospitalization due to worsening heart failure (OR 1·25; 95% CI, 1·02–1·54). This may explain the reason for the significant heterogeneity among these four studies for this outcome (I2 = 76%, χ2 = 12·29, P = 0·006).
Major hemorrhage
The risk of major hemorrhage was doubled with warfarin as compared with antiplatelet therapy (5·59% vs. 2·62%, RR 2·15; 95% CI, 1·55–2·99, P < 0·00001) with an absolute risk increase of 0·99% per year (Table 3). This effect was driven by the results of the WARCEF trial (OR 2·24; 95% CI, 1·45–3·46), which contributed 59·1% of the events (97/164). There was no statistical evidence of heterogeneity among the studies for major bleeding (I2 = 0%, χ2 = 1·89, P = 0·59) (Fig. 5). On the other hand, there was no significant increase in intracranial hemorrhage with warfarin as compared with antiplatelet therapy (0·62% vs. 0·48%, RR 1·42; 95% CI, 0·36–5·57, P = 0·61) (Table 3). There was no statistical evidence of heterogeneity among the studies for intracranial hemorrhage (I2 = 61%, χ2 = 2·55, P = 0·11).
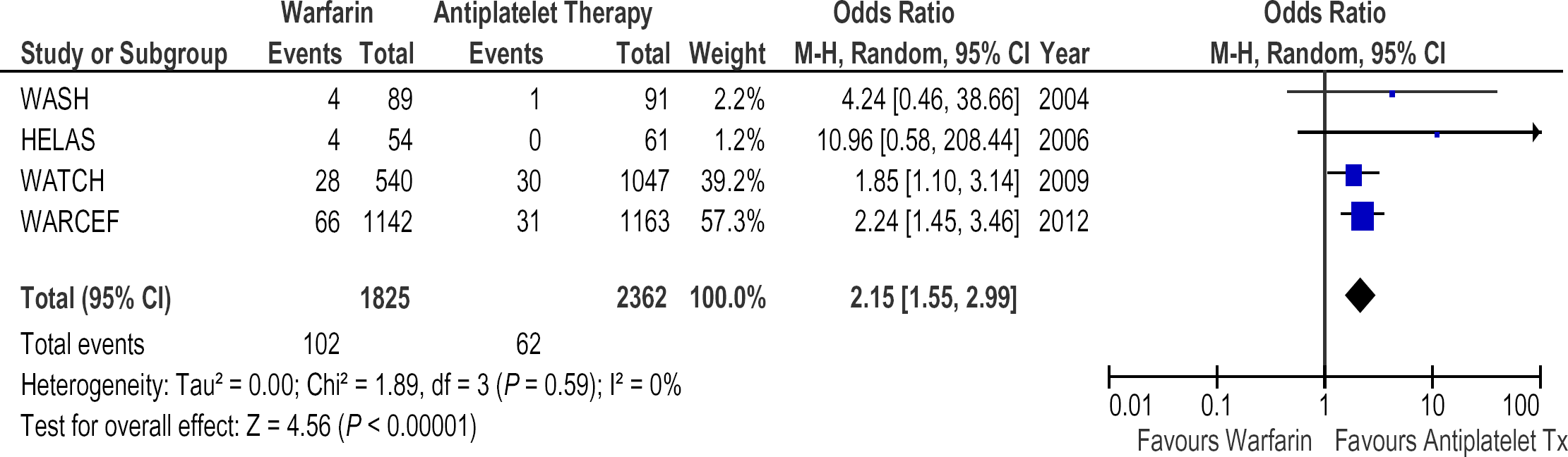
Relative risk of major hemorrhage in patients treated with warfarin vs. antiplatelet therapy (RE Model).
Results were consistent irrespective of whether warfarin was being compared with aspirin (n = 1838) or clopidogrel (n = 524) separately (data not shown). Similar results were obtained using random-effect and fixed-effect models and when the pooled data were summarized using risk ratios and risk differences (data not shown). Excluding the WASH trial, which has Jadad score of 2, did not alter the results (data not shown).
Discussion
Our meta-analysis of the four trials involving 4187 subjects with heart failure and sinus rhythm showed that warfarin as compared with antiplatelet therapy (1) reduces ischemic stroke events although the absolute rate reduction was small; (2) doubles the risk of major hemorrhage with a consistent pattern of increase in risk of intracranial hemorrhage; and (3) does not significantly reduce death, MI, or hospitalization due to heart failure. Of note, the narrow confidence interval around the neutral effect on mortality (RR 1·00; 95% CI, 0·86–1·17) excludes a clinically meaningful benefit of warfarin anticoagulation on death for patients with unselected etiology of heart failure.
Previous meta-analysis based on the WASH and WATCH trials showed no significant difference between warfarin and aspirin therapy on the risk of death, MI, and stroke (8). Our finding that warfarin reduces the risk of ischemic stroke is driven primarily by the results of the WARCEF trial, which accounted for 84 of the 105 ischemic strokes in our pooled analyses. Previous meta-analysis was based on two trials involving a combined total of 1767 patients, 29 events for ischemic stroke, and 63 events major hemorrhage. Publication of the WARCEF trial increased the number of patients by 2305, strokes by 84 events, and major hemorrhage by 97 events. Although the estimates were similar, the confidence intervals are much narrower, increasing our confidence in the accuracy of the estimates.
Significant heterogeneity existed among the four studies for the hospitalization due to heart failure outcome. Although there were differences among the trials in relation to baseline characteristics (e.g. the severity of heart failure at baseline, proportion with coronary artery disease or prior stroke) and the duration of study treatment, it is unclear how these differences could account for the observed heterogeneity. Aspirin has been reported to negatively interact with Angiotensin converting enzyme (ACE) inhibitor therapy, which may have differentially affected trials with higher rates of ACE/ARB used, but the importance of this interaction remains unproven (9).
Several possible explanations should be considered for the lack of effect of warfarin on cardiovascular events other than stroke. Warfarin is effective for prevention of recurrent MI (10), but only about half of the patients included in these studies had underlying coronary artery disease. Arrhythmias and pump failure are potentially competing risks of death in patients with heart failure and cannot be expected to be prevented by warfarin.
Current guidelines do not advocate the use of antithrombotic therapy for patients with heart failure and sinus rhythm (11–13). We believe that the results of our meta-analysis should not alter these recommendations because the small absolute benefits of stroke reduction appear to be outweighed by increased bleeding and there is no suggestion of a mortality benefit. However, warfarin might still be considered in heart failure patients with atrial fibrillation, major regional left ventricular wall motion abnormalities and those with aneurysm formation who may be at very high risk of thromboembolic complications. We believe that future research on the role of anticoagulants in heart failure should focus on those with underlying coronary heart disease. A strong argument can be made to evaluate one of the new oral anticoagulants, such as dabigatran, apixaban, or rivaroxaban, rather than warfarin in any future trials because they have a superior balance between efficacy and safety profile (14).
Limitation of the study
The most important limitation of our meta-analysis is the lack of individual participant-level data, which precluded exploration of the effects of warfarin compared with antiplatelet therapy in patients with or without underlying ischemic heart disease and previous stroke and in those with different severities of heart failure.
Conclusions
In conclusion, warfarin as compared with antiplatelet therapy reduces the risk of ischemic stroke in patients with systolic heart failure who are in sinus rhythm but increases the risk of major hemorrhage. The effects of warfarin vs. antiplatelet therapy on the rate of death, MI, hospitalization secondary to heart failure and intracranial hemorrhage were not statistically different. These results provide no support for the routine use of warfarin anticoagulation in heart failure patients who are in sinus rhythm.