
Abstract
Background
Aphasia affects up to a third of the stroke population and is associated with poor social participation and quality of life. Yet people with aphasia may be excluded from some types of stroke research due to challenges in informing, consenting, and conducting follow-up in this population.
Aims and/or hypothesis
We described the representation of those with aphasia in acute stroke clinical research, the level of inclusion across international trial sites, and whether there have been improvements in the inclusion of this population in recent clinical trials.
Methods
We conducted a retrospective analysis of clinical trial data from the Virtual International Stroke Trials Archive (VISTA), defining aphasia using the Best Language (item 9) domain of the National Institutes of Health Stroke Scale. We used proportional odds modeling, adjusting for age, gender, ethnicity, stroke severity, medical history, hemisphere affected by stroke, and trial eligibility criteria, to examine the associations between year, location of enrollment, inclusion, and attrition of those with aphasia.
Results
Data were available for 8904 patients from 10 trials; no trials listed aphasia as an exclusion criterion. At baseline, aphasia was present in 4039 (45·4%); severe/global aphasia was present in 2688 (30·2%). We observed no geographic or longitudinal disparity in the attrition of these patients at three-months. Centers in the Philippines recruited fewer people [P = 0·05, odds ratio = 0·5, 95% confidence interval (0·2, 1·0)], while centers in Central and South America included more people with severe/global aphasia [P = 0·0004, odds ratio = 2·4, 95% confidence interval (1·3, 4·3)], when compared with centers in the USA and Canada.
Conclusion
Acute stroke trials have demonstrated the feasibility of including people with aphasia in stroke research; we observed geographic variations that were not entirely explained by case mix or trial eligibility criteria. Similar levels of inclusion should be sought in nonemergency stroke trials to improve the applicability of research findings to this population.
Introduction
Informed consent for participation in a randomized controlled trial (RCT) is a basic tenet of research. However, establishing capacity to consent is complex. Aphasia occurs in 12–38% (1–4) of people following stroke and can form a barrier to the process of informed consent and data collection using standard methods (5–7). Aphasia can affect both language and comprehension (8). A person may be able to understand their diagnosis, the risks and benefits of the investigational treatment, and the implications of consenting to participation, but aphasia may prevent them from expressing their wishes (9,10). As this impairment has major implications for social participation, activities of daily living, length of hospitalization (1), depression (11), and poor quality of life (12), the inclusion of this population in clinical research has great value. Currently, trialists in the United Kingdom need to justify the inclusion of those with incapacity in clinical research; some trialists may consider it easier to exclude these patients (13). Similar issues arise with those who exhibit aphasia as a result of stroke; capacity to consent may be completely impeded or limited to certain domains such as a language, leaving comprehension intact (8).
Despite legislation (14) and guidelines to facilitate the process of consent in people with aphasia (10,15,16), practical issues can arise that delay the consent process (17). As a result, those who can readily demonstrate capacity and who are able to give full consent by themselves are often more likely to be included in clinical research. The exclusion of those with aphasia from some types of stroke research has been observed particularly in nonemergency settings (5,18). Intentional or unintentional exclusion affects the representativeness of the stroke trial population (19), which in turn impacts the validity and clinical applicability of research findings in relation to people with aphasia (20,21). However, research in the acute stroke setting has benefited from legislation in Europe and the USA, permitting those unable to consent for themselves to be included in Clinical Trials of Investigational Medicinal Products (CTIMPs) (22–25). Under the exemption from informed consent directive, a patient must be in a life-threatening situation, existing therapies must be ineffective, consent must be impracticable due to the patient's medical condition (such as in the case of severe aphasia), and the use of a surrogate to provide consent should be infeasible due to the acute setting and need for urgent care (24,25). Thus, under these guidelines, people with aphasia may be included in CTIMPs.
Aims
We sought to describe the representation of this important population in acute stroke clinical research, whether the level of inclusion is similar across international trial sites, and if there have been improvements in the inclusion of those with aphasia in recent clinical trials.
Methods
We conducted a retrospective analysis of pooled clinical trial data from the Virtual International Stroke Trials Archive (VISTA). This collaborative venture was established to collate and provide access to completed, anonymized, clinical trial data for novel exploratory analyses (26). We extracted data on patient age, gender, race-ethnicity, initial stroke severity [measured using the National Institutes of Health Stroke Scale (NIHSS)], medical history (atrial fibrillation, myocardial infarction, hypertension, diabetes, and prior stroke), year, and geographic location of enrollment. Aphasia was assessed using the Best Language domain (1 = mild to moderate aphasia, 2 = severe aphasia, and 3 = mute/global aphasia) of the NIHSS at baseline (day 0) and at final follow-up (three-months). Trials in our dataset typically included patients who were aged 18 or older, presented at hospital within six-hours of stroke onset, had a baseline NIHSS score of at least 5, were conscious at baseline, and displayed some limb weakness.
We described the proportion of people who presented with aphasia at baseline as a percentage of the whole trial population, stratified by year and geographic location of trial enrollment. We described the proportion of people with aphasia who were lost to follow-up, stratified by the year of trial enrollment, to indicate whether there has been an improvement in the retention of those with aphasia in recent trials. Finally, we examined attrition by geographic location.
As people with mild to moderate aphasia may not face the same challenges during the consent process as those with more severe impairment, we conducted a sub-group analysis to examine the inclusion and attrition of people with severe or global aphasia (Best Language Score ⩾2 at baseline).
In order to maximize statistical power, we excluded observations from strata in which fewer than 100 patients were enrolled. We formally tested the association between geographic location of recruitment, inclusion, and attrition using proportional odds modeling, adjusting for age, gender, ethnicity, initial stroke severity, medical history variables, and hemisphere affected by stroke. As the presence of aphasia was assessed using the Best Language domain of the NIHSS, we omitted the individual score for this domain from the total NIHSS score when describing stroke severity to avoid confounding our analysis. Trial sources could not be revealed in accordance with VISTA regulations. Therefore, an anonymized sensitivity analysis was carried out to adjust for the effects of trial eligibility criteria.
Results
Analysis dataset
We extracted anonymized data on 8904 patients, for whom age, gender, ethnicity, medical history variables, and individual NIHSS domain scores were recorded. All patients had experienced an acute ischemic stroke. These patients were enrolled across 30 geographic regions between 1992 and 2008 (Table 1).
Patient demographic variables
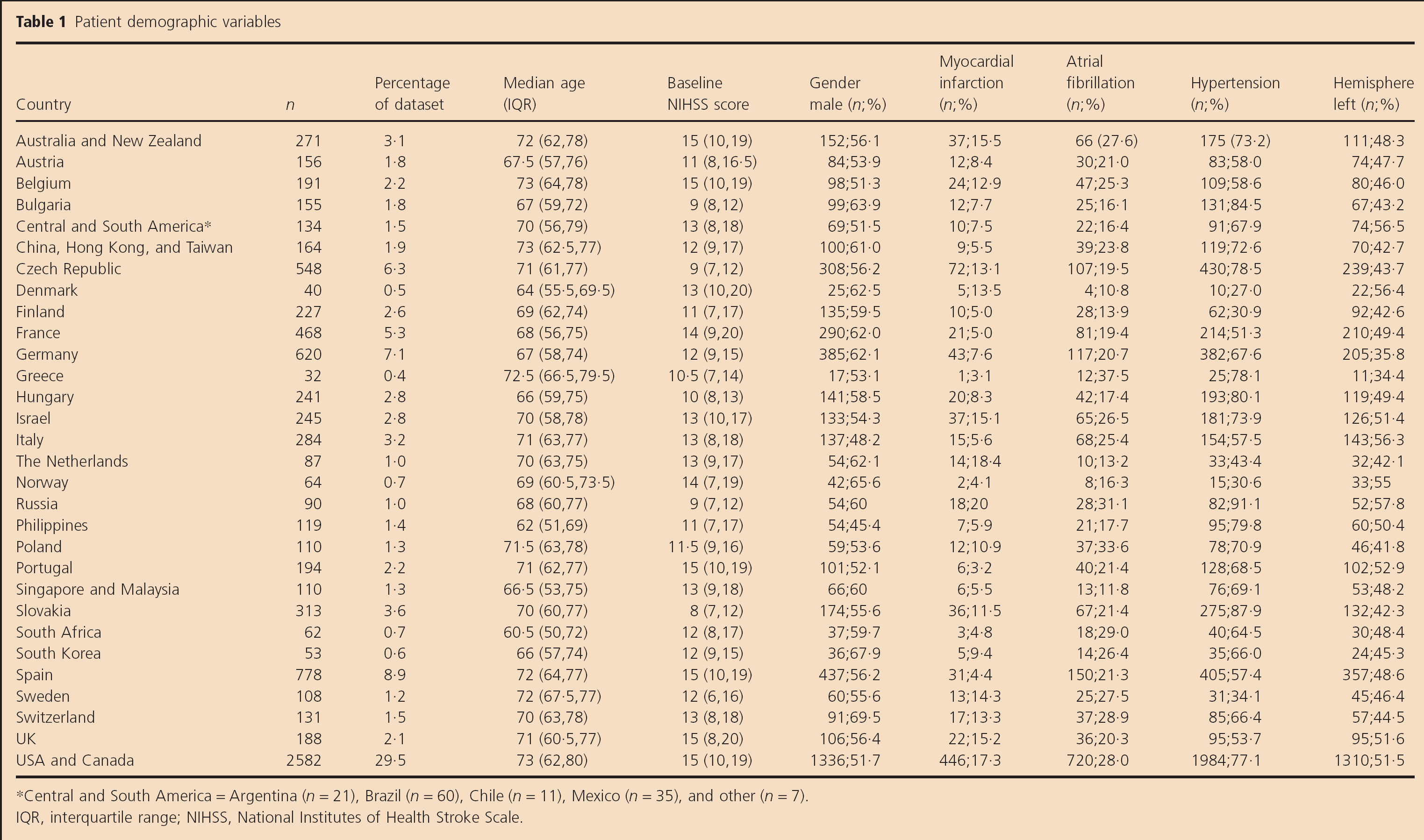
Central and South America = Argentina (n = 21), Brazil (n = 60), Chile (n = 11), Mexico (n = 35), and other (n = 7). IQR, interquartile range; NIHSS, National Institutes of Health Stroke Scale.
Inclusion of people with aphasia
None of the trials in our analysis dataset specifically mentioned aphasia as an exclusion criterion; one trial required patients to present with either visual field deficit, neglect, or aphasia at baseline.
Aphasia affected 4039/8904 (45·4%) at baseline, with 2688/8904 (30·2%) experiencing severe or global aphasia. At baseline, 2833/4039 (70·1%) of those with aphasia were alert, 1025/4039 (25·4%) answered both NIHSS orientation questions correctly, and 2059/4039 (50·1%) responded to commands.
Variation in inclusion of people with aphasia by year of enrollment
After selecting strata, which contained more than 100 patients, our longitudinal analyses were based on patients who were enrolled between 1993 and 2006. During this period, the proportion of people who presented with aphasia at baseline ranged between 39·4% and 72·3%, while the proportion of people with severe or global aphasia ranged between 27·7% and 51·1%. Newer trials did not appear to enroll more people with aphasia when compared with older trials (Fig. 1a,b).
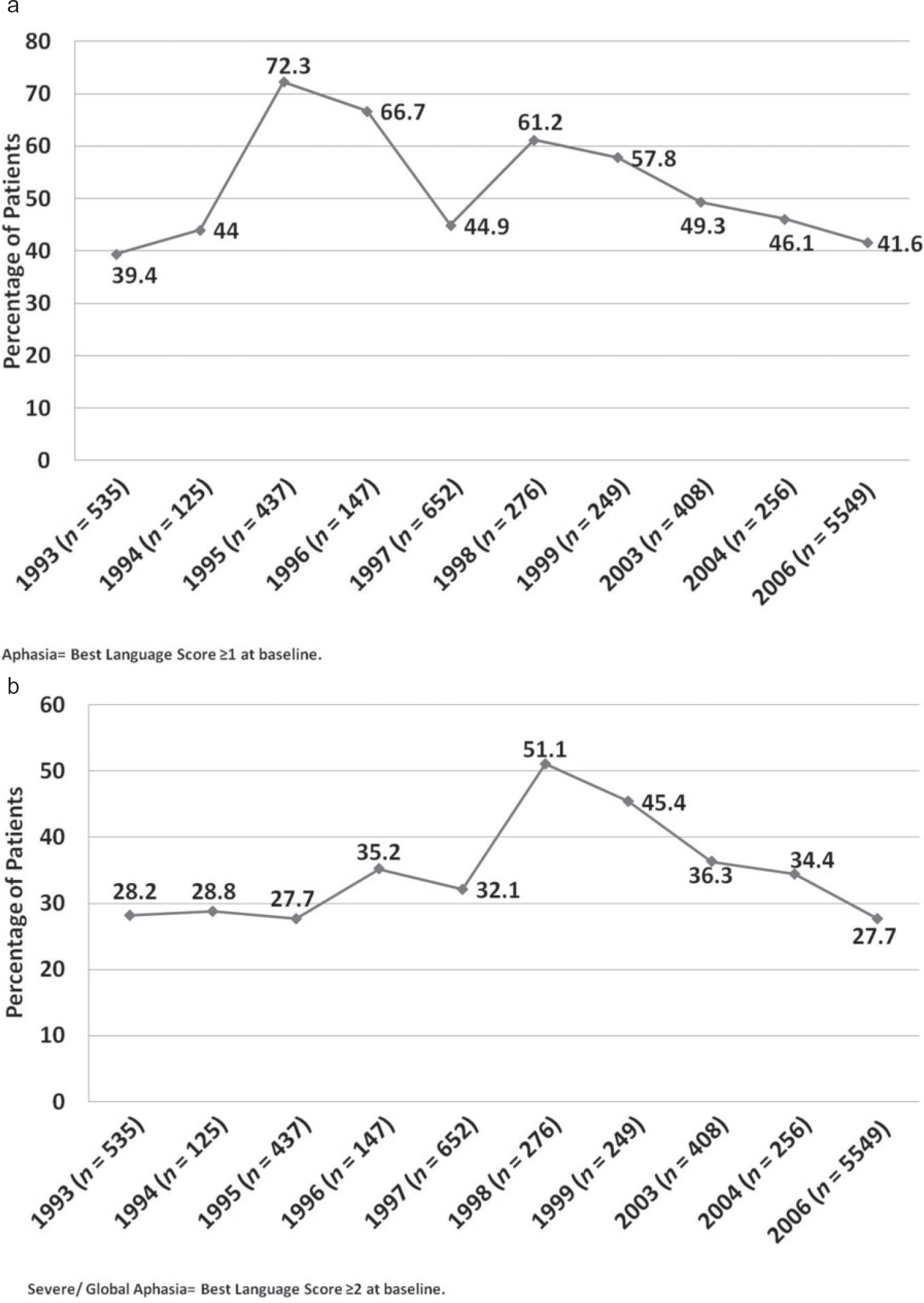
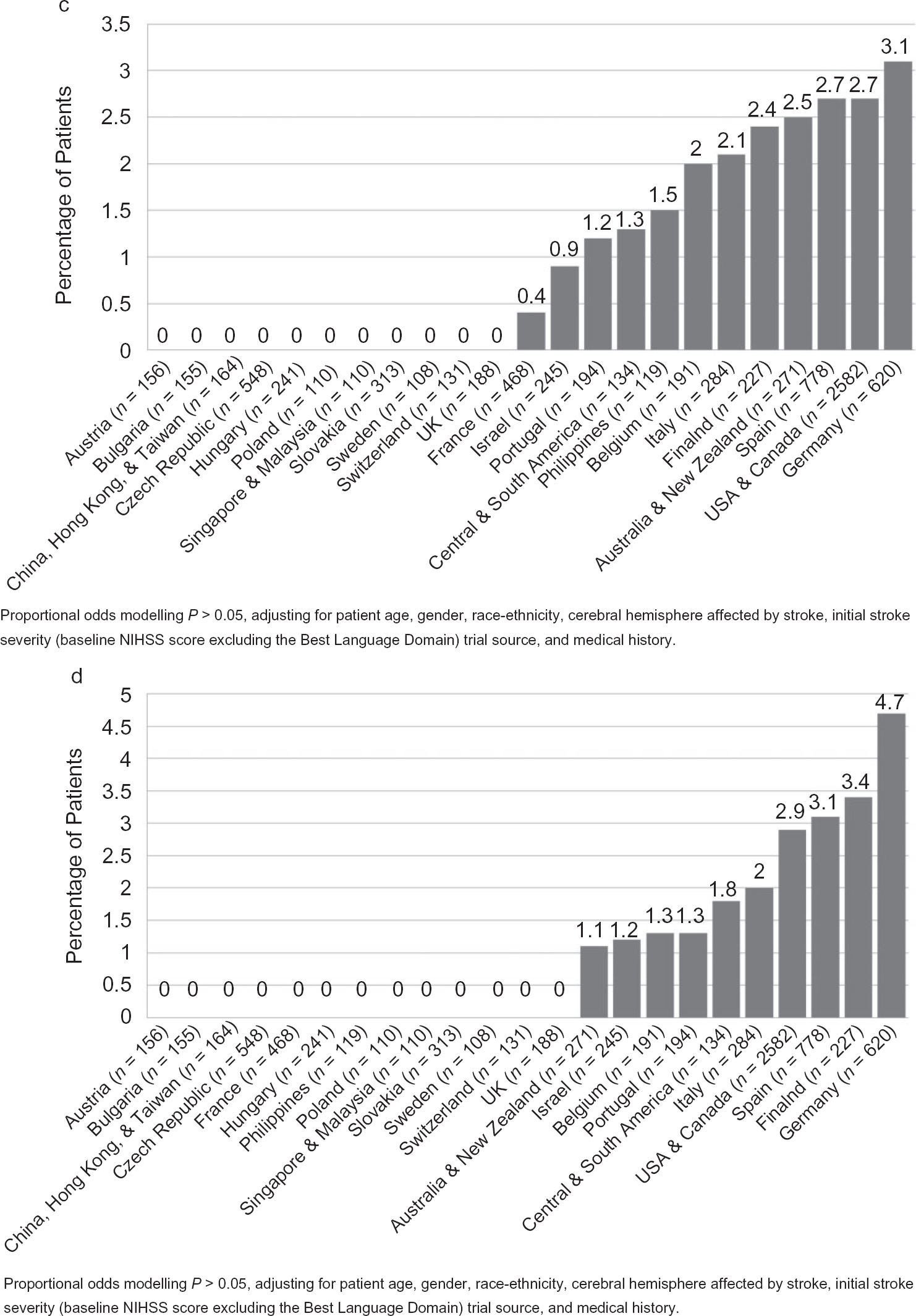
(a) Variation in the inclusion of patients with all types of aphasia in acute stroke RCTs, by year of enrollment. (b) Variation in the inclusion of patients with severe or global aphasia in acute stroke RCTs, by year of enrollment. (c) Geographic variation: odds ratios for inclusion of patients with all types of aphasia in acute stroke RCTs. (d) Geographic variation: odds ratios for inclusion of patients with severe or global aphasia in acute stroke RCTs. NIHSS, National Institutes of Health Stroke Scale; RCT, randomized controlled trial.
Geographic variation in the inclusion of people with aphasia
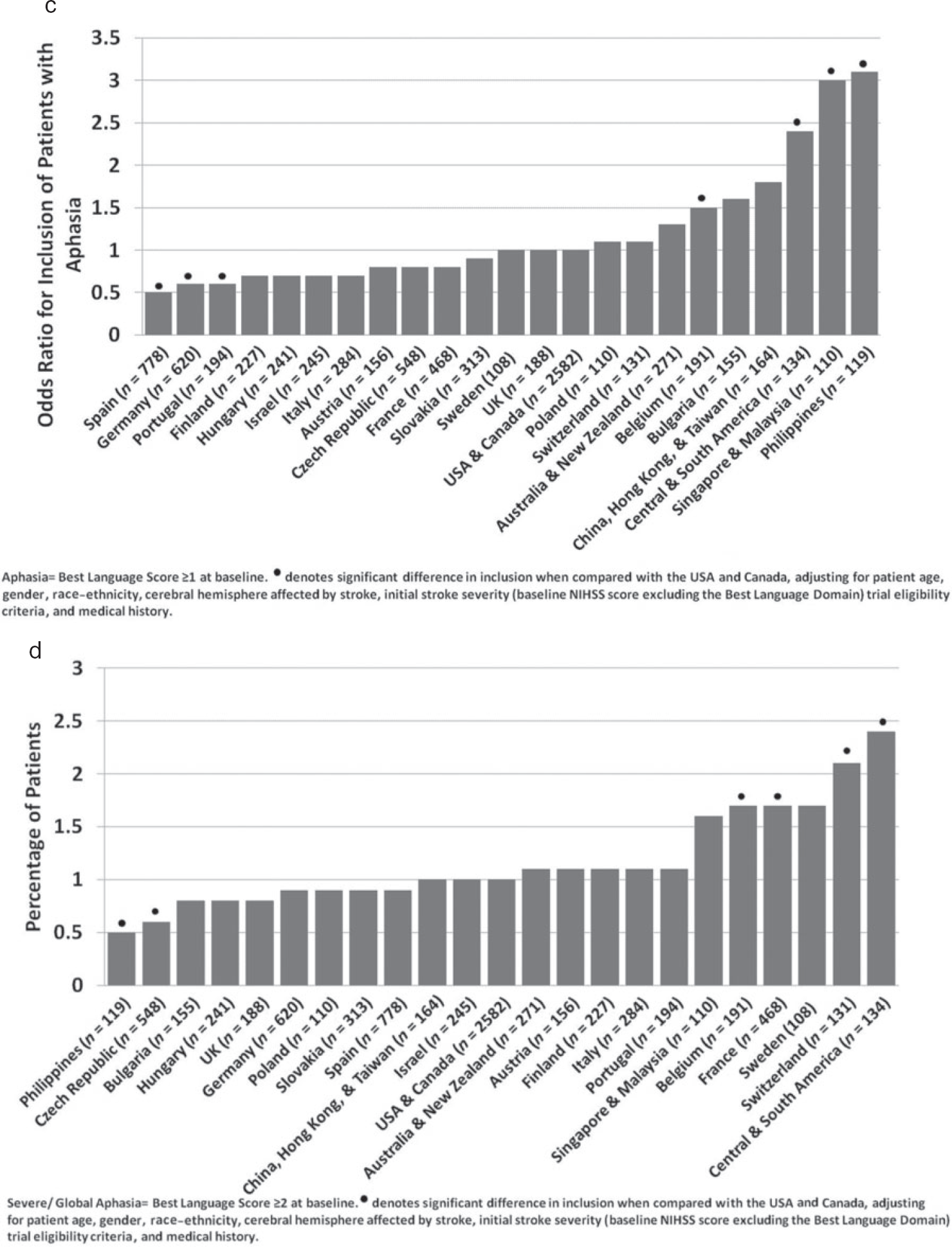
Geographic regions in which fewer than 100 patients were enrolled were omitted from this analysis. Proportional odds modeling adjusting for case mix and trial eligibility criteria revealed that compared with those who were enrolled in the USA and Canada, trial centers in Spain [P < 0·0001, odds ratio (OR) for inclusion = 0·5, 95% confidence interval (CI) (0·4, 0·7)], Portugal [P = 0·006, OR for inclusion = 0·6, 95% CI (0·4, 0·9)], and Germany [P = 0·003, OR for inclusion = 0·6, 95% CI (0·5, 0·9)] enrolled significantly fewer people with aphasia (Best Language score ⩾ 1). Centers in Belgium [P = 0·05, OR for inclusion = 1·5, 95% CI (1·0, 2·4)], Central and South America [P = 0·001, OR for inclusion = 2·4, 95% CI (1·4, 4·2)], Singapore and Malaysia [P = 0·001, OR for inclusion = 3·0, 95% CI (1·5, 6·1)], and the Philippines [P = 0·001, OR for inclusion = 3·1, 95% CI (1·5, 6·6)] included significantly more people with aphasia (Fig. 1c).
Our sub-group analysis revealed that although centers in the Philippines had enrolled more people with all types of aphasia, these centers enrolled far fewer people with severe or global aphasia at baseline [P= 0·05, OR for inclusion = 0·5, 95% CI (0·2, 1·0)] compared with centers in the USA and Canada. Similarly, centers in the Czech Republic enrolled fewer people with severe or global aphasia [P = 0·001, OR for inclusion = 0·6, 95% CI (0·4, 0·9)] compared with centers in the USA and Canada. Trial centers in Belgium [P = 0·04, OR for inclusion = 1·7, 95% CI (1·0, 2·9)], France [P = 0·01, OR for inclusion = 1·7, 95% CI (1·1,2·5)], Switzerland [P = 0·02, OR for inclusion = 2·1, 95% CI (1·2, 3·8)], and Central and South America [P = 0·004, OR for inclusion = 2·4, 95%CI (1·3,4·3)] enrolled more people with severe or global aphasia, after adjusting for case mix and trial eligibility criteria (Fig. 1d).
(Continued)
Attrition of people with aphasia
By 90 days, 1530 (17·2%) of all patients in our dataset had died and 155 (1·7%) were lost to follow-up. Complete follow-up data were available for 3967 (98·2%) people with all types of aphasia. Similarly, few people with severe or global aphasia at baseline were lost to follow-up; three-month data were available for 2635/2688 (98%). Between 1993 and 2006, the proportion of people with aphasia who were lost to follow-up by 90 days ranged from 0% to 9·3% (Fig. 2a) and the proportion of people with severe or global aphasia who were lost to follow-up ranged from 0% to 10·2% (Fig. 2b).
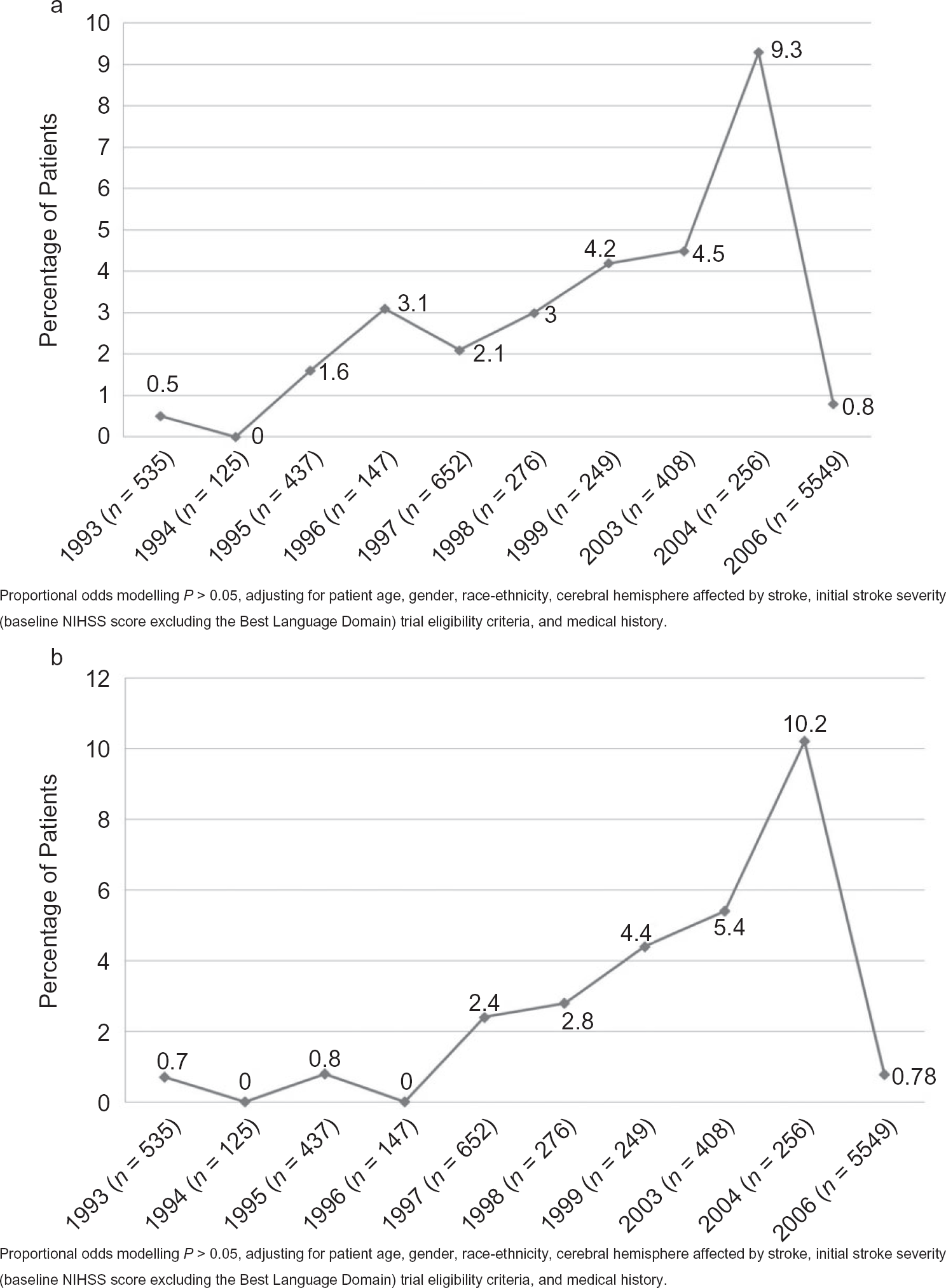
(a) Variation in the attrition of patients with all types of aphasia, by year of enrollment. (b) Variation in the attrition of patients with severe or global aphasia, by year of enrollment. (c) Geographic variation: attrition of patients with all types of aphasia. (d) Geographic variation: attrition of patients with severe or global aphasia. NIHSS, National Institutes of Health Stroke Scale.
Attrition of those with all types of aphasia, stratified by geographic region, ranged between 0% and 3·1% (Fig. 2c), while attrition of those with severe or global aphasia ranged from 0% to 4·7% (Fig. 2d). We observed no geographic disparity in the attrition of people with any type of aphasia.
(Continued).
Discussion
Our findings suggest that people with aphasia were well represented in acute stroke trials conducted between 1992 and 2008; typically less than 2% of patients were lost to follow-up at three-months, which was consistent with the proportion of patients who were lost to follow-up across the entire analysis dataset. We observed no significant change in the inclusion of those with aphasia in more recent trials. However, there were notable geographic differences in recruitment, which were not explained by case mix or trial eligibility criteria.
Although trial centers in the Philippines enrolled more people with all types of aphasia, closer examination revealed that this region included significantly fewer people with severe or global aphasia. Trial centers in Belgium, France, Switzerland, and Central and South America fared better, including more severely impaired patients. Thus, although the level of overall inclusion of people with aphasia appeared to be good in some regions, estimates were inflated by the presence of those with mild to moderate aphasia. In a clinical setting, these patients would not typically pose the same challenges to inform and consent. The representation of those with severe or global aphasia across different countries perhaps provides a more accurate estimate of the nature of inclusion. We observed that 30·2% presented with severe or global aphasia at baseline; this is consistent with prevalence estimates of poststroke aphasia in the literature (1–4).
To our knowledge, this is the first study describing the longitudinal and geographic differences in the inclusion and attrition of people with aphasia in acute stroke RCTs. As these RCTs form the evidence base for new interventions and as those with aphasia may form up to a third of stroke survivors (3,27), their inclusion in clinical research is of great value. Recruitment and retention of stroke patients in clinical research are challenging (28). Ethics boards require trialists to justify the inclusion of patients with incapacity in clinical research. However, people with aphasia may not necessarily have incapacity and should therefore be given the same opportunity to participate in clinical research as those with capacity; this is complicated when there is a loss of autonomy (29). Despite legislation permitting consent to be sought through a proxy or waived in the case of some types of emergency research, many patients deemed to lack capacity may not be included in important research. This is evident particularly in a stroke rehabilitation setting (18) where practical limitations may hinder timely consent by a proxy (17). This affects the reliability, validity, and generalizability of results (29). Furthermore, the collection of data on this population facilitates sub-group analyses, investigations of aspects of recovery that are unique to the population, and informs the investigations of future interventions.
The composition of our analysis dataset was influenced by the eligibility criteria of contributed trials. Accordingly, trial source was included as an anonymized covariate in our analyses. The patients in our analysis dataset were representative of those typically enrolled in acute stroke CTIMPs. These patients typically presented at hospital within the first six-hours of stroke onset and in order to be eligible for inclusion in acute stroke intervention trials, they were usually conscious at baseline, demonstrated limb weakness, have possible higher cortical dysfunction, have visual field defects, have sensory or communication impairments, and typically scored greater than five points on the NIHSS at admission. These criteria therefore include a greater proportion of those with aphasia than might be anticipated within the general stroke population. We did not have access to screening data to describe the population of patients who were deemed to be ineligible for participation or in how many the level of language impairment hindered inclusion. Nevertheless, we found that those with aphasia were well represented in acute stroke clinical research and that valuable data on this patient population were generated.
All trials within VISTA required documented consent or waiver of consent after local institutional review board–approved procedure (26). For the vast majority of patients in our dataset, the method of consent (self vs. proxy) was not recorded in case report forms, from which we extracted our data. However, as legislation permits the inclusion of those with incapacity in emergency CTIMP research and as we observed that those with aphasia were well represented in our analysis dataset, we postulate that the method of consent would not have significantly affected the number of people with aphasia who were included.
Aphasia was assessed as part of the NIHSS, the recommended stroke severity assessment tool in acute stroke (30,31). Patients were asked to describe a picture, identify items on a naming card, and read standard sentences. However, this method of assessment may be perceived as lacking in sensitivity (32). Within the hyperacute stroke setting, the use of a formal aphasia battery, such as the Western Aphasia Battery or the Boston Diagnostic Aphasia Examination, could be confounded by rapidly changing language profiles, decreased levels of consciousness, and medical instability. Typically, more sensitive aphasia assessments are conducted within the first few days after stroke. None of the trials included in our analysis conducted specialized aphasia assessments at baseline or three-months. Nevertheless, the Best Language domain of the NIHSS examined elements of speech including repetition of words, phrases, and sentences, spontaneous speech, naming, reading, and comprehension. This was consistent with Lezak's recommendations (33) for assessments of communication impairments. Guidelines, training, and certification for use of the NIHSS are also widely available (34,35). Therefore, the use of NIHSS Best Language domain was deemed to be a good indicator of aphasia in the acute setting.
The presence of aphasia is related to index stroke severity, the location, and size of the stroke. These factors in turn are associated with patient demography such as age, the presence of hypertension, atrial fibrillation, and a history of prior stroke. Geographic differences in stroke severity can be explained by social status, poverty, and the population demographics of the country. As populations and social structures evolve over time, so too do the factors that contribute to stroke; the causes of stroke shift from those related to nutritional deficiencies and infections to chronic noncommunicable diseases such as cardiovascular disease and diabetes (36). Industrialization of a region has also been postulated as a mechanism for the transition from poverty-related stroke demographics toward increasing prevalence of cardiovascular disease and ischemic stroke (37–39). Case mix is therefore an important factor to consider when describing geographical variation in patient inclusion. We observed that after adjusting for patient age, gender, race-ethnicity, cerebral hemisphere affected by stroke, initial stroke severity, medical history variables, and trial source, the geographic disparity in the inclusion of people with aphasia remained. The reason for this is not known. However, we acknowledge that legislation and individual practice in each region may have contributed to the geographic variation in inclusion. For example, regulations for surrogate consent in the USA vary between states (29), with even greater variability in legislation and interpretation on a global level (40). Examination of geographic variations in stroke subtype, lesion volume, and location of stroke may yield further explanations. Participating centers may represent some of the more organized hospitals in their country. These trial centers could potentially be used in future international, multicenter trials and similar disparities in enrollment of certain patient subgroups may occur.
Our findings contrast with the level of inclusion of people with aphasia observed in other types of stroke research, particularly in poststroke depression studies (5). Legislation such as Section 32 of the UK Mental Capacity Act 2005 (14) provides guidance on the methods for securing consent from a suitable proxy for research in those with incapacity. This legislation is applicable for nonemergency research including stroke rehabilitation trials, yet people with aphasia may not be given an opportunity to be included in this type of research due to inadequate information provision or their objection to others making decisions on their behalf regarding participation (10). The time pressures that are seen in the acute stroke setting are not as severe in the rehabilitation setting (9). Additionally, numerous strategies have been identified to improve communication between trialists and people with aphasia to enhance information provision for participation in clinical research. These include simplifying language on trial information sheets, the use of repetition to enforce key messages, incorporating yes/no and open ended questions as necessary, and use of nonverbal communication such as gestures, diagrams, and models (10,15,16). Aphasia friendly consent documentation was utilized in the recent ACT NoW trial and aids such as Talking Mats™ (Stirling, UK) have been developed to facilitate communication. However, the use of such material remains inconsistent. Provisions are in place to facilitate the participation of those with aphasia in clinical research and our study findings indicate that the follow-up in this population is feasible and yields valuable information. Future research should identify and apply methods to facilitate inclusion and follow-up in those with aphasia; this could enhance inclusion in nonemergency trials and therefore the clinical applicability of research findings.