
Abstract
Background
In Germany, the financing of stroke unit care was implemented into the hospital reimbursement system in 2006. Since then, many acute care hospitals newly implemented stroke units. Simultaneous, in-hospital mortality for stroke declined.
Aims
The study aims to analyze the association of mortality trends for stroke with the increasing provision of stroke unit care in German hospitals.
Methods
Hospitalizations for acute stroke from 2005 to 2010 are identified in the nationwide German Diagnosis Related Groups statistics. Trends of risk-adjusted in-hospital mortality are studied stratified by existence of a stroke unit in the admitting hospital, as well as stratified by cohorts of hospitals defined by the respective period of stroke unit implementation.
Results
Overall, mortality in patients admitted to stroke unit hospitals is lower (crude 9·2%; adjusted 9·8%) compared to patients admitted to nonstroke unit hospitals (12·7%; 11·6%). The longitudinal analysis revealed a general secular trend of declining mortality in all cohorts of hospitals. However, while all stroke unit-providing hospital cohorts converge to a quite similar level of mortality in 2010, mortality in hospitals without stroke unit remains significantly higher. Reduction of mortality in hospitals with early provision of stroke unit care seems to be attributable to the secular trend. A reduction of mortality exceeding the secular trend was observed in hospitals with late stroke unit implementation.
Conclusions
The earlier stroke unit implementations might represent rather ‘formal’ inceptions in experienced hospitals with preexisting appropriate stroke care, whereas late implementations seem to have caused extra improvements. Overall, stroke patients are more likely to survive when admitted to an stroke unit-providing hospital. A more stringent assignment of acute stroke patients to stroke unit-providing hospitals could possibly further reduce stroke mortality in Germany.
Introduction
There is strong evidence for the benefit of specialized stroke unit (SU) care on patients experiencing acute stroke, demonstrated in randomized controlled clinical trials (1) as well as in observational studies (2). In Germany, the financing of SU care was implemented into the hospital reimbursement system in 2006. This has been triggering openings of new stroke units in acute care hospitals. In a previous study, one third of all German acute care hospitals were identified as providing SU care in the year 2010. The share of stroke patients receiving SU care rose from 15% in 2005 to more than 50% in 2010 (3).
SU care as reimbursed via the German Diagnosis Related Groups (G-DRG) relies on a sub-intensive-care concept for continuous monitoring and specialized treatment of stroke patients, which is being applied within the acute phase of stroke. Characterized by early admission and usually rapid discharge to a general ward after the acute phase, this concept is different to the British or Scandinavian nonintensive combined acute and rehabilitation SUs (4–6).
Preconditions for reimbursement are defined by the German procedure classification OPS (Operationen- und Prozedurenschlüssel). Among these, the most important requirements are treatment in a stroke-specialized sub-intensive ward with defined staffing (concerning qualification and presence), continuous monitoring, immediate execution of certain diagnostic measures, access to neurosurgery, and availability of therapeutic procedures, such as thrombolytic therapy. Compliance with these requirements is commonly being validated by health insurers.
Up to now, there has been no overall evaluation of the impact of SU care on outcome for stroke in the German population. Previous studies revealed considerable variation of volumes and in-hospital mortality for ischemic stroke among German hospitals (7), but also a continued decline of in-hospital mortality for stroke with a relative decrease of 20% from 2005 to 2010 (3). However, it is unclear to which extent this is attributable to the growing coverage of SU care within this time span.
Aims
The association of in-hospital mortality for stroke with the provision of SU care is studied within an observational study of nationwide German administrative hospital data from 2005 to 2010. Stratified by existence of a stroke unit in the admitting hospital trends of mortality are studied. Additionally it is investigated, if and how the opening of new stroke units influences mortality in the respective hospitals. These effects are analyzed for cohorts of hospitals classified by the respective period of SU implementation.
Methods
Data
The nationwide DRG statistics provided by the Research Data Centres of the Federal Statistical Office and the statistical offices of the Länder (federal states) contain discharge information on all in-hospital episodes of acute care hospitals that are reimbursed via DRG. As the DRG system in Germany is an all-patient/all-payer system, the DRG statistics cover 94% of all acute care hospital episodes in Germany. Not covered are episodes in psychiatric and psychosomatic hospitals, primarily. Therefore, the data are virtually complete with respect to acute care hospitalizations for stroke.
Each data row represents one in-hospital episode. Principal and secondary diagnoses are coded via the German version of ICD-10, procedures via the German procedure coding system OPS. Among others, information on age at admission, gender, type of residence (rural/urban), hours of mechanical ventilation, length of stay, source of admission, and discharge disposition are contained. Episodes can be assigned to the respective treating hospital via a pseudonymized hospital identifier. Because the data do not contain a patient identifier, multiple hospitalizations cannot be tagged.
Patients
Unit of analysis are patients hospitalized for all types of first-time and recurrent acute stroke. These are identified by a principal diagnosis of ischemic stroke (ICD-10 code I63), intracerebral hemorrhage (I61), subarachnoid hemorrhage (I60), or stroke of unspecified type (I64). Patients aged below 20 are excluded because of the different etiology.
To focus on the episode in the first admitting hospital, subsequent episodes of care are excluded (by excluding transfers from other acute care hospitals identified via the source-of-admission code). By these means, we avoid double counting of patients due to transfers.
Hospitals
Hospitals are classified by the provision of stroke unit care. Under the precondition of a principal diagnosis of stroke (I60, I61, I63, I64) or TIA (transient ischemic attack, G45), the number of episodes with documented SU care (OPS codes 8–981 or 8–98b) per hospital and year is calculated. The code 8–981 represents SU care within a neurological department (reimbursable since 2006), 8–98b within a medical department (reimbursable since 2009), both for a minimum duration of 24 h.
Existence of a stroke unit in the respective hospital is assumed when at least ten episodes with coded SU care are present within a calendar year. The limit is carefully chosen to avoid misclassification of hospitals with accidental or false coding (it is very unlikely that a hospital coding less than 10 SU treatments per year really provides an expensive facility like a stroke unit).
The analyzed episodes for stroke are then for a first analysis assigned to two groups: Patients admitted to SU hospitals, and patients admitted to non-SU hospitals.
A second classification of hospitals is based on the period of SU provision or implementation. Hospitals are assigned to cohorts based on the first year of SU existence, if they continued to provide SU services in the subsequent years. The investigated cohorts are: SU provision before 2007, SU implementation 2007 or 2008, SU implementation 2009 or 2010, no SU provision within the observation period, and a group of remainders where provision of SU care or treatment of stroke patients has occurred temporarily within the observation period.
Analysis
To evaluate risk-adjusted mortality, generalized estimating equations with a logit link function are used, accounting for clustering of patients within institutions. Besides age and gender, the model includes type of stroke in order to consider the poorer prognosis of patients with hemorrhagic stroke. As there is no present-on-admission flag for secondary diagnoses in the German data, only such comorbidities are included in the model, which are documented reliably and likely to have been present on admission (e.g., heart failure, atrial fibrillation). Furthermore, severe acute conditions, like cardiogenic shock, are included. Comorbidities that might represent possibly preventable complications (e.g., pneumonia) or conditions associated with stroke itself (e.g., paralysis) are not included. Model fitting was done upon the pooled data of the entire observation period. The final model includes age in years, gender, type of stroke (intracerebral and subarachnoid hemorrhage versus ischemic or unspecified type of stroke), and the secondary diagnoses of cardiogenic shock, atrial fibrillation, ventricular fibrillation, ventricular tachycardia, lower limb atherosclerosis, heart failure, COPD (chronic obstructive pulmonary disease), severe kidney disease, chronic renal failure, diabetes, coronary artery disease, congenital heart disease, malignancies, and dilated cardiomyopathy. Discrimination was assessed by the c statistic (8), which showed an acceptable value of 0·740.
Temporal trends are assessed via simple linear regression models, accounting for least square weighting by number of cases. The level of statistical significance is set on 0·05. All data analyses were conducted using SAS Version 9·1 (SAS Institute Inc., Cary, NC, USA).
Results
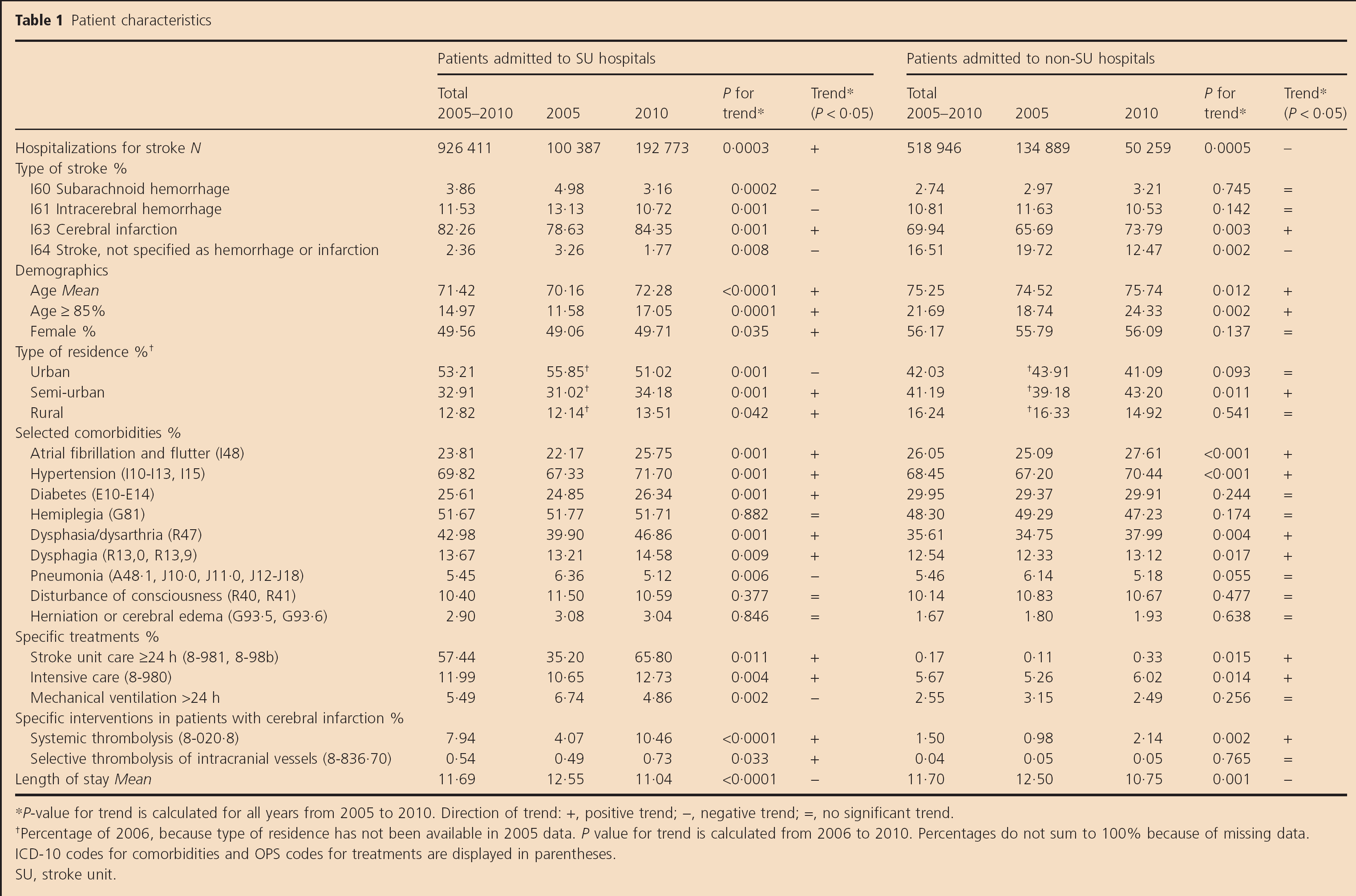
Characteristics of patients admitted to SU hospitals compared with those admitted to non-SU hospitals are displayed in Table 1. Within the observation period the share of admissions to SU hospitals rose, while admissions to non-SU hospitals fell, respectively. Regarding stroke type, the share of strokes coded as unspecified was higher in non-SU hospitals, although this proportion declined until 2010.
Patient characteristics
P-value for trend is calculated for all years from 2005 to 2010. Direction of trend: +, positive trend; -, negative trend; =, no significant trend.
Percentage of 2006, because type of residence has not been available in 2005 data. P value for trend is calculated from 2006 to 2010. Percentages do not sum to 100% because of missing data.
ICD-10 codes for comorbidities and OPS codes for treatments are displayed in parentheses.
SU, stroke unit.
Patients admitted to SU hospitals are younger and the share of females is lower than in non-SU hospitals. Urban type of patient's residence is more frequent in patients admitted to SU hospitals. However, during the observation period the percentage of patients admitted to SU hospitals with semi-urban or rural type of residence increased.
When focusing on selected comorbidities, a higher presence of atrial fibrillation and diabetes in non-SU hospitals is observed, while coding of manifestations of stroke like hemiplegia or dysphasia is more frequent in SU hospitals. As well, cerebral edema or herniation is more frequently coded in patients admitted to SU hospitals.
Patients admitted to SU hospitals more often received intensive care treatment and mechanical ventilation. The frequency of systemic or selective thrombolysis in ischemic stroke patients admitted to SU hospitals is higher. Within SU hospitals the share of stroke patients receiving SU care increased from 35% in 2005 to 66% in 2010. Also, in non-SU hospitals some occasional hospitalizations with coded SU care were observed.
Length of stay declined within the observation period in both groups, quite equally.
The crude relative risk (RR) of in-hospital death in patients admitted to SU hospitals is about 24% to 29% lower in comparison with patients admitted to non-SU hospitals. After risk adjustment, a 12% to 15% lower risk remains (see Table 2). Within the observation period there have been no significant changes of the RR.
Crude and adjusted relative risk (RR) of in-hospital death for patients admitted to SU hospitals (versus patients admitted to non-SU hospitals)
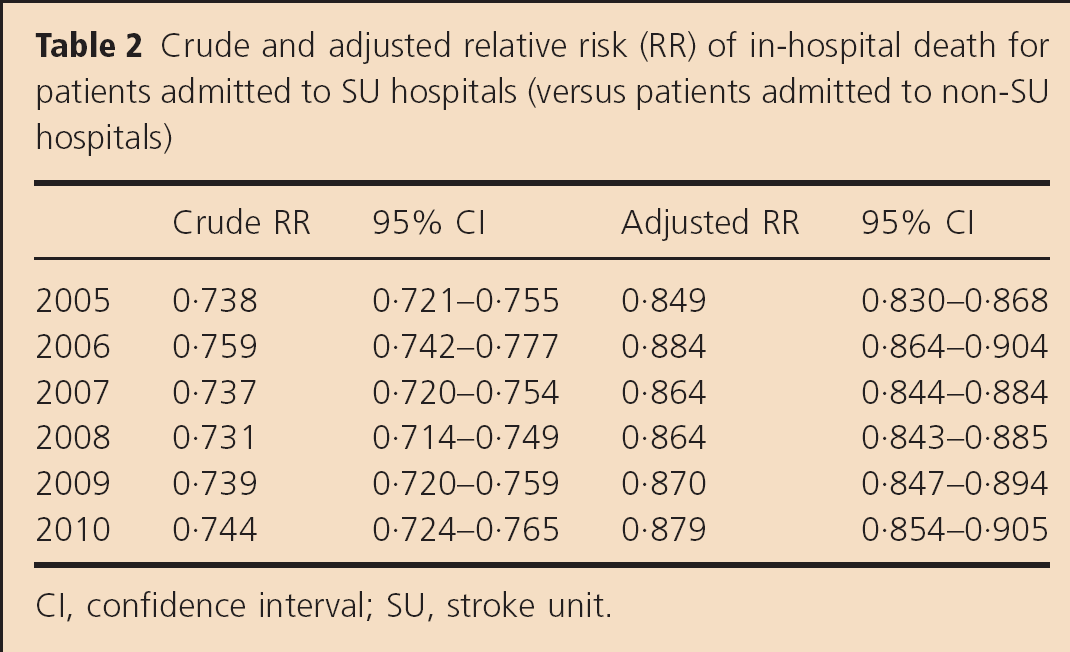
CI, confidence interval; SU, stroke unit.
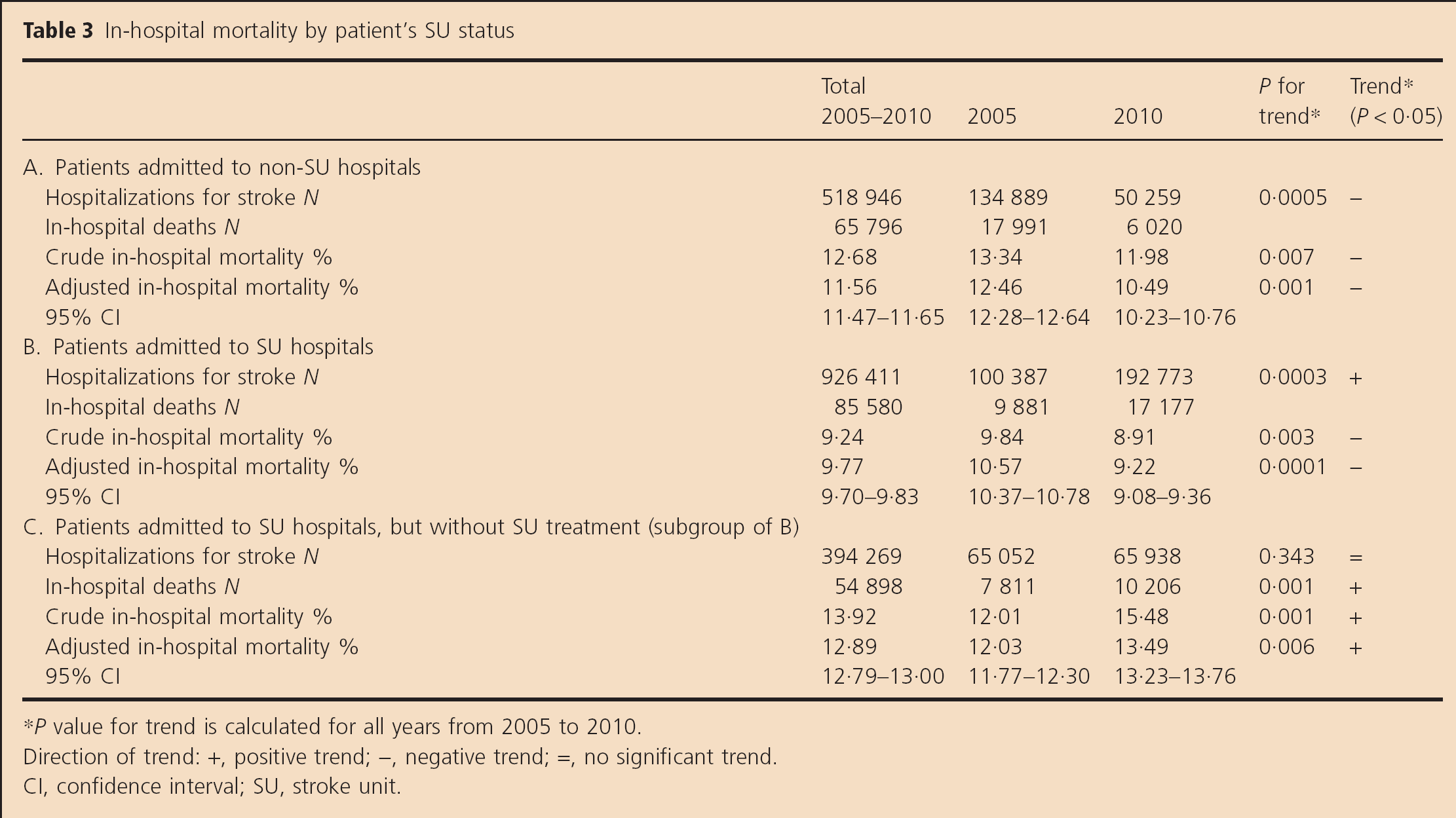
Table 3 displays in-hospital mortality in patients admitted to (a) non-SU hospitals and (b) SU hospitals. Both crude and adjusted mortality declined significantly within the observation period in both groups. In every period, as well as overall, adjusted mortality in patients admitted to non-SU hospitals is significantly higher.
In-hospital mortality by patient's SU status
P value for trend is calculated for all years from 2005 to 2010.
Direction of trend: +, positive trend; -, negative trend; =, no significant trend.
CI, confidence interval; SU, stroke unit.
Separately displayed in Table 3 part C is mortality in the subgroup of patients that had been admitted to an SU hospital but did not receive SU treatment, that is, no SU coding is present in these episodes. While adjusted mortality in this subgroup was quite similar to patients admitted to non-SU hospitals in 2005, it increased continuously until 2010 and is overall higher than in patients admitted to non-SU hospitals.
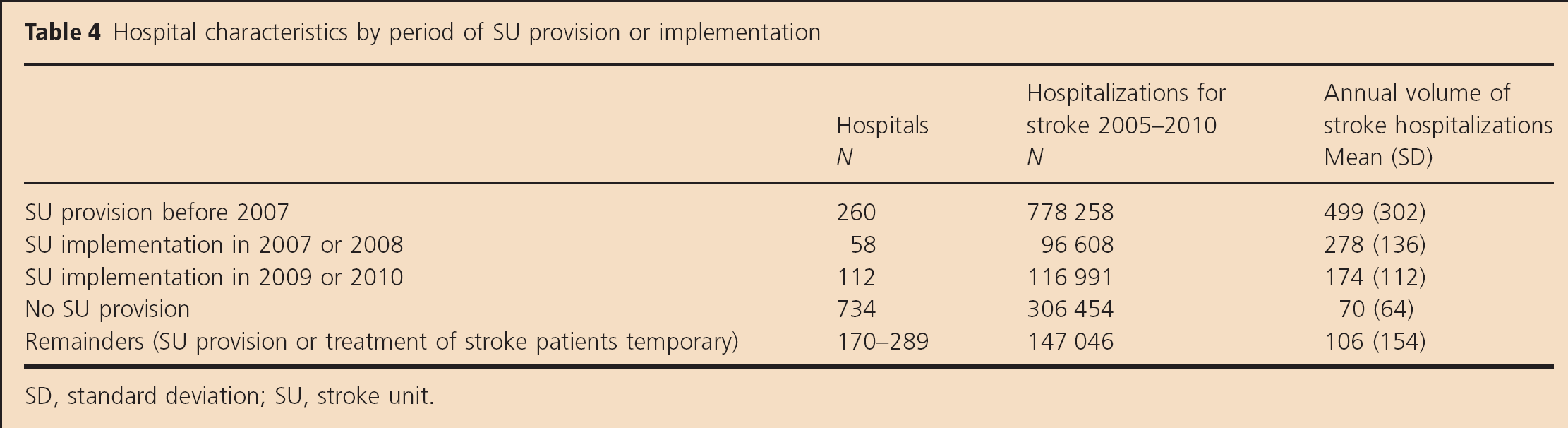
Characteristics of the analyzed hospital cohorts are displayed in Table 4. Two hundred sixty hospitals were identified as having been providing SU care already before 2007. New implementations of SU care between 2007 and 2009 were observed in 58 hospitals, and between 2009 and 2010 in 112 hospitals. Seven hundred thirty-four hospitals never provided SU care during the observation period. There were 289 (2005) to 170 (2010) hospitals which provided SU care or treated stroke patients temporarily but not continuously and were classified as remainders.
Hospital characteristics by period of SU provision or implementation
SD, standard deviation; SU, stroke unit.
The average annual volume of stroke hospitalizations in the different cohorts shows that especially hospitals with lower volumes implemented new stroke units after 2006. The lowest average annual volume is observed in hospitals that never provided SU care within the observation period.
Figure 1 illustrates the crude (part A) and adjusted (part B) trends of in-hospital mortality for the respective cohorts. In 2005, mortality was lowest in hospitals providing SU care before 2007, and highest in hospitals with no SU provision or late SU implementation. In all groups mortality declined until 2010. In those cohorts, which had SU in the beginning or which implemented SU within the observation period, mortality converges to a similar level in 2010. In hospitals without SU provision mortality remains significantly higher. A mortality reduction exceeding the secular trend is observable in the cohort of hospitals with late SU implementation only.
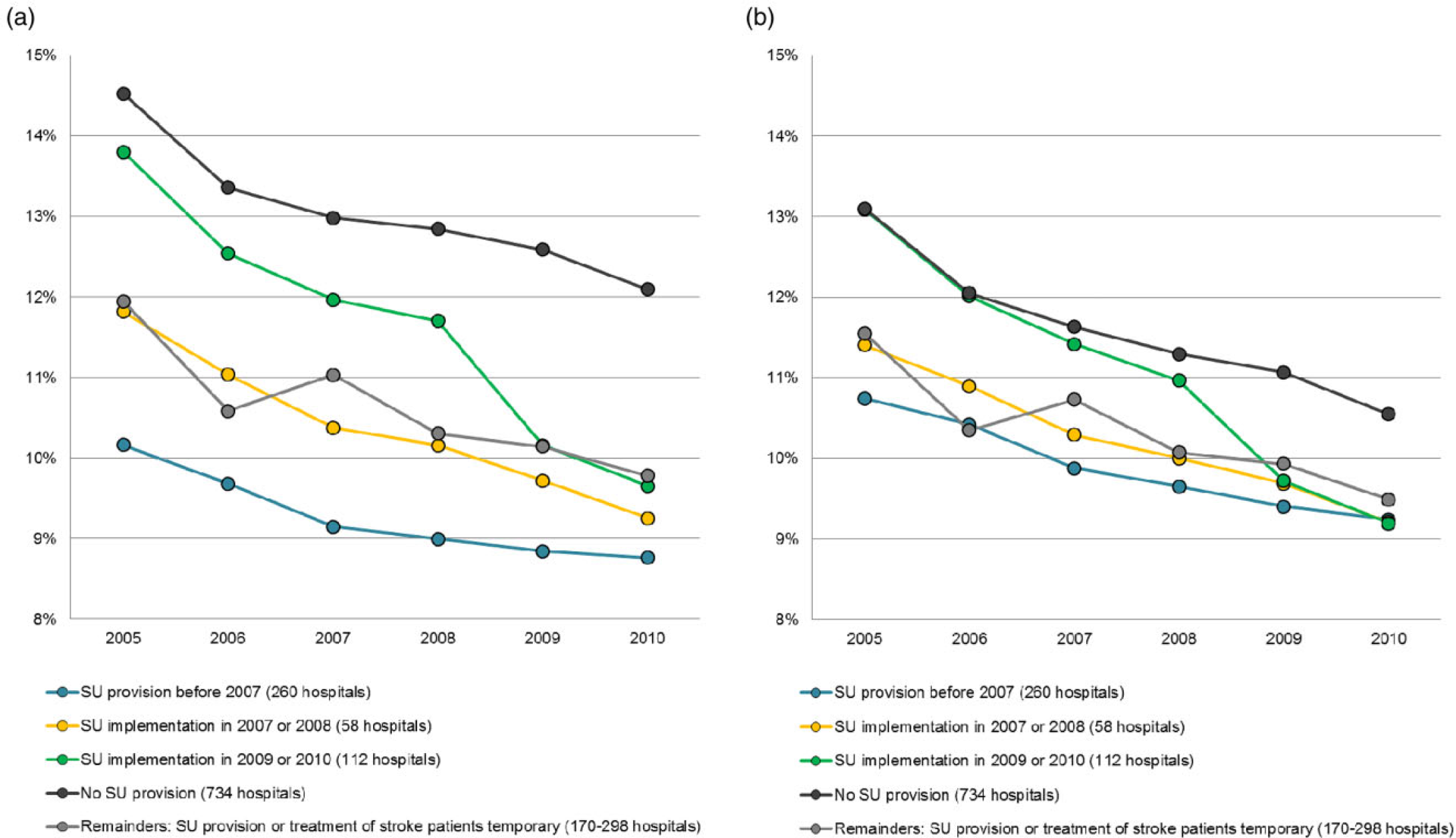
Trends of in-hospital mortality in groups of hospitals, classified by period of stroke unit (SU) provision or implementation. (a) Crude in-hospital mortality; (b) adjusted in-hospital mortality.
Discussion
This is the first nationwide study in Germany evaluating the association of stroke unit care and in-hospital mortality. Similar to observational studies from other countries (2,9,10), a significantly lower in-hospital mortality in patients admitted to SU-providing hospitals was observed in Germany in cross-sectional comparisons within each observation year.
However, the findings become more differentiated in a longitudinal perspective. First, the proportion of hospitals providing SU care has increased. This development can be attributed to the inclusion of SU payments in the DRG reimbursement system in 2006, which resulted in financial incentives for German hospitals. Based on hospitals treating stroke patients, the share of hospitals with SU care increased from 14% to 35% (3).
The later SU care was implemented, the lower was the average case volume of the respective hospitals. We consider this to be caused by increasing competitive pressure due to excess capacities in the German hospital market (11). This forces even lower volume providers either to improve their services or to lose certain service areas to competitors.
The analysis of mortality trends for the cohorts of hospitals classified by the period of SU implementation basically revealed a secular trend of declining mortality in all groups. The reduction of mortality in those hospitals with early provision of SU care seems to be attributable to the secular mortality trend only. As one would not expect additional mortality reductions in hospitals that already provided SU care before the observation period, this finding seems to be plausible. In the intermediate cohort, which implemented SU care in 2007 or 2008, we also did not find additional mortality reductions. It could be possible, that the SU implementation in this cohort might represent some rather ‘formal’ changes in care according to the detailed requirements for reimbursement purposes in hospitals with already preexisting appropriate stroke care.
An additional effect of SU implementation on mortality could only be observed for the cohort of those hospitals which implemented SU care lately in 2009/2010. Considering the initially higher mortality in these hospitals, it seems that the implementation of SU care led to substantial improvements in this cohort.
Mortality in the three cohorts having implemented SU care before or within the observation period converges to a similar level in 2010. Also, the cohort of hospitals which did not implement SU care shows the secular trend toward lower mortality. However, mortality in this cohort remained higher than in SU hospitals throughout the whole observation period. It might be discussed, if mortality in these hospitals could be improved by SU introduction. Considering that these hospitals on average treat only 70 stroke patients per year, it is obvious that they cannot fulfill the requirements for stroke units in an economically meaningful way. Therefore, from a public health perspective it would make more sense to direct stroke patients more rigorously to SU hospitals, as far as possible. The evidence of beneficial effects of SU care for all acute stroke patients (12), independent from age (10,13), type of stroke (14,15), or severity (1), would support such policies.
The share of patients admitted to SU hospitals but not receiving SU care decreased within the observation period. This group shows a considerable higher mortality, which might be explained by internal selection effects, where end-stage patients intentionally are not admitted to the SU. On the other hand, for patients dying within the first 24 h after admission, SU care by definition cannot be coded.
The strength of this study is the use of complete national data, covering all hospitalized acute strokes in Germany. In contrast to data from other countries, the German DRG data allow the identification of SU providing hospitals as well as of patients receiving SU care. Limitations occur from the restricted information available in the administrative dataset (e.g., stroke severity cannot be assessed), and the limited time of patient observation covering the in-hospital episode only. Further research is needed to study the impact of SU care on long-term mortality and functional outcome in the German population, and to assess the cost-effectiveness within the German health care system.
Conclusion
Following the implementation of the DRG reimbursement system in Germany, a more formalized definition of stroke unit care has been introduced for reimbursement purposes. Those hospitals which participated in SU care from the beginning of observation or implemented SU care shortly after the introduction SU payment did not show improvements in mortality which exceeded the basic secular trend. In these hospitals the SU implementation might represent rather ‘formal’ inceptions which did not further improve the preexisting appropriate stroke care. In hospitals which introduced SU care later, this seems to have caused additional improvements. Overall, stroke patients are more likely to survive when admitted to SU-providing hospitals. From an economical point of view a further spread of stroke units to providers with lower volumes would not be reasonable due to heavily increasing per-patient cost. Therefore, a more stringent assignment of acute stroke patients to SU-providing hospitals, which could possibly further reduce stroke mortality rates in Germany, would politically be advisable.